
Central Adelaide Local Health Network - CPSU · 2020-02-11 · 2.3 Vision to deliver the Triple Aim...
55
Central Adelaide Local Health Network Organisational and Financial Recovery Plan November 2018 Liability limited by a scheme approved under Professional Standards Legislation
Transcript of Central Adelaide Local Health Network - CPSU · 2020-02-11 · 2.3 Vision to deliver the Triple Aim...

Central Adelaide Local Health Network
Organisational and Financial Recovery Plan
November 2018
Liability limited by a scheme approved under Professional Standards Legislation

Page 2
Table of contents
Covering letter ...................................................................................................................................... 3
Disclaimer ............................................................................................................................................. 4
1 Executive Summary ..................................................................................................................... 6
2 CALHN Recovery Plan | Guiding Principles and Initial Controls ............................................ 13
2.1 Primary objectives ........................................................................................................... 13
2.2 Key implementation principles ....................................................................................... 13
2.3 Vision to deliver the Triple Aim of Healthcare................................................................ 14
2.4 Workforce engagement principles ................................................................................. 15
2.5 Four key operational levers for recovery........................................................................ 16
2.6 High level recovery timeline ........................................................................................... 17
2.7 Proposed immediate controls ........................................................................................ 18
2.8 Monthly management reporting pack ............................................................................ 19
2.9 CEO Executive Management and Organisational On-boarding..................................... 20
2.10 Organisational design reset............................................................................................ 21
2.11 Governance and performance management reset ....................................................... 23
3 CALHN Recovery Plan | Implementation Approach ............................................................... 25
3.1 Context and overview...................................................................................................... 25
3.2 Indicative Recovery Plan organisational structure ........................................................ 26
3.3 Recovery Plan governance framework .......................................................................... 27
3.4 Recovery Plan risk assessment...................................................................................... 30
4 CALHN Recovery Plan | Target Financial Outcomes .............................................................. 32
4.1 Indicative 3-year financial recovery path ....................................................................... 32
4.2 Key financial performance drivers and sensitivities ..................................................... 33
5 CALHN Recovery Plan | Key Initiatives and Operating Levers ............................................... 36
5.1 Overview .......................................................................................................................... 36
5.2 Key initiatives for each operating lever over a three-year recovery period .................. 37
5.3 Recovery initiatives during Stabilise Phase ................................................................... 38
5.4 Recovery initiatives during CY2019 ............................................................................... 39
5.5 Recovery initiatives during CY2020 and CY2021 ......................................................... 40
List of Appendices
Appendix 1 – Recovery Plan - Indicative Timelines by Operating Lever
Appendix 2 – Recovery Plan – Risk Management Framework
Appendix 3 – CALHN – Current Organisation Structure
Appendix 4 – CALHN Administrator: Specific Actions & Performance Management Meetings
Appendix 5 – Glossary
Page 3
Covering letter
Ms. Jenny Richter
Chief Executive Officer
Central Adelaide Local Health Network
Royal Adelaide Hospital
Adelaide SA 5000
November 2018
Dear Jenny
Recovery Plan for Central Adelaide Local Health Network (‘CALHN’)
We refer to the contract of engagement between CALHN and KordaMentha Pty Ltd dated 6 August 2018.
Following the completion of the Phase 1 Diagnostic Review, we have now completed Phase 2 of our engagement, comprising
the development of a recovery plan to address the key issues identified in the Diagnostic Review.
In accordance with your instructions, we have developed a comprehensive recovery strategy and plan to deliver a step-change
in clinical, organisational and financial performance over a three-year horizon from 1 January 2019 to 31 December 2021,
preceded by an initial period of stabilisation during the remainder of 2018. Our recovery plan illustrates a clear road map to
ensuring CALHN is delivering improved patient outcomes and operating at or better than the National Efficient Price within a
three-year period.
It is anticipated that stabilisation activities will commence prior to 1 December 2018.
Should you have any queries, please do not hesitate to contact me.
Yours sincerely
Chris Martin
Partner

Page 4
Disclaimer
Issues considered
The issues considered during this review have been specifically limited to the matters set out in the engagement contract
dated 6 August 2018.
Sources of information
The information set forth in this review has been obtained from records provided by CALHN and SA Health and discussions with
the management and other relevant stakeholders of CALHN and SA Health and their advisers. In many instances, we have
relied on the representations of these parties and individuals.
The statements and opinions contained in this report are given in good faith. However, in the preparation of this report, we
have relied upon the accuracy and completion of information provided by the above parties.
Scope and limitations
The report has been prepared by KordaMentha with care and diligence. However, our work did not include the procedures
necessary to conduct an audit or to enable us to express an opinion as to whether the financial information contained in this
report present a true and fair view in accordance with applicable accounting standards and accordingly, no such opinion is
expressed.
The forecast information and the supporting assumptions are based on the best available information and, insofar as the
assumptions relate to the future or may be affected by unforeseen events, we can express no opinion on how closely the
forecasts will respond to actual results. While we have reviewed the assumptions underlying the forecast information, we do
not express an audit opinion or any other form of assurance on these forecasts or assumptions and our comments are based
on our evaluation.
We have no responsibility to update this report for events or circumstances occurring after the date of this report, apart from
any subsequent arrangement.
Any advice arising from this Engagement has been provided in our capacity as consultants.
Unless otherwise stated, all figures included in this report are expressed in Australian dollars and have not been adjusted for
the time value of money.
This report has been prepared solely for the use of CALHN and SA Health and must not be disclosed to or relied upon by any
other party without our prior consent.

Page 5
1. Executive Summary

Page 6
1 Executive Summary
Introduction
In September 2018, KordaMentha completed a Diagnostic Review of the Central Adelaide Local Health Network (‘CALHN’). The
Diagnostic Review identified a number of systemic issues impacting the network’s clinical, organisational and financial
performance. The Diagnostic Review also identified the need to undertake a robust planning process in order to properly
assess competing priorities and determine the optimal sequencing of turnaround activities. The CALHN Organisational and
Financial Recovery Plan (‘Recovery Plan’) has been developed as a result of this planning process and should be read in
conjunction with the Diagnostic Review.
Primary objectives and key implementation principles
The primary objective of the CALHN Organisational and Financial Recovery Plan is to ensure CALHN becomes a high performing
and accountable healthcare network that delivers world class healthcare and operates to Australian benchmark standards
across all domains. Underpinning this objective, we believe the aspiration of delivering the ‘Triple Aim of Healthcare’, an
internationally accepted and proven conceptual framework for optimising health system performance, should be the focus of
CALHN.
Triple aim System vision
• The health and wellbeing of the community served by CALHN will improve as a result of CALHN delivering health
prevention, intervention and treatments at scale in the community.
• CALHN will continue to develop alternative treatment pathways for patients, including through improving access
to the primary and community care sectors.
• More community-based treatment options will improve health outcomes while reducing emergency demand.
• CALHN will also focus on improving the health and wellbeing of staff and ensure that all staff work in an
environment where they are provided with the access to opportunity and appropriate training.
• CALHN will address unwarranted variation in clinical outcomes and effectiveness.
• CALHN will tackle long length of stay patients by identifying and addressing system and site process, procedure
and control inefficiencies.
• CALHN will ensure that outpatients are managed effectively and ensure that care is provided in the most
appropriate environment.
• Effectively manage clinical risk environments to achieve benchmark standards, including minimising
prevalence of hospital acquired infections and complications.
• Holding itself to account against a range of quality and value benchmarks such as the National Efficient Price
(‘NEP’) and Health Roundtable (‘HRT’), CALHN will deliver efficiencies and generate economies of scale across
the network.
• CALHN will think differently and creatively about meeting the rising demand implications for healthcare in the
community.
• CALHN will ensure that its risk management and control environment is fit for purpose and focuses on
achieving best practice.
• Sustainability does not just mean money – CALHN will consider the application of innovative technologies and
work practices to allow staff to work smarter and do more good for vulnerable patients.
• Ensure corporate and clinical risk environments are appropriate and deliver to benchmark standards.
The primary objectives that the CALHN Organisational and Financial Recovery Plan is intended to achieve, and which are
consistent with the Triple Aim of Healthcare performance framework, are outlined below.
Primary objectives
1. Ensure CALHN becomes a high performing and accountable healthcare network that operates to Australian benchmark
standards across all domains.
2. Maintain and improve community access to CALHN facilities and services.
3. Maintain and improve services to, and within, the community to support CALHN activities.
4. Support improvement of the quality of clinical outcomes delivered in all CALHN services.
5. Enable CALHN to build on the single-service, multi-site service concept, emphasising accountability at the local level.
6. Ensure CALHN develops and embeds a culture of continuous improvement and a commitment to improving healthcare
outcomes for the community it serves.
7. Create disciplined, repeatable and consistent processes and controls across CALHN.
1.Health and
wellbeing
2.Quality
of care
3.Sustainability

Page 7
Primary objectives
8. By December 2021, ensure that CALHN is delivering improved patient outcomes and performing at or better than the
NEP across all specialties and facilities.
9. Ensure external advisors assist in skills transfer to CALHN and SA Health staff and stakeholders.
The implementation of the CALHN Organisational and Financial Recovery Plan will be informed by a set of guiding principles
which we have summarised below.
Key implementation principles
• Patient care and health outcomes remain the primary focus of CALHN.
• Regular and meaningful input will be sought from stakeholders across CALHN.
• CALHN will:
− treat all individuals with respect and empathy
− act with honesty, integrity and transparency in all our dealings
− become an evidence-based decision-making organisation
− acknowledge that some current practices may not reflect contemporary standards and will need to change
− learn and adopt appropriate local, national and international best practices
− continue to maintain constructive relationships with workforce representative stakeholders
− provide appropriate training and professional development to the CALHN workforce
− develop and respect operational and financial controls
− acknowledge that developing a sustainable healthcare network is an acceptable organisational target
− acknowledge that succession planning is an important enabler of workforce management and organisational
sustainability
− not tolerate personal or departmental fiefdoms and agree that unacceptable behaviours should be ‘called out’
− work hard to develop stronger relationships with our internal and external suppliers
− clearly define individual responsibilities and hold people to account
− celebrate milestones and success along the way.
Key Operating Levers
The Recovery Plan has been developed around a set of four practical operational levers that will have meaningful impact and
align with the target end-state outcomes. The primary workstreams underpinning the implementation of the CALHN
Organisational and Financial Recovery Plan are then aligned with these key operating levers.
Intent
• Put patient outcomes at the centre
of decisions.
• Structure the delivery of services to
be efficient and well-planned.
• Recognise and manage towards
expectations of clinical performance.
Intent
• Create a culture of leadership
and accountability at all levels
of the organisation.
• Improve workforce
engagement.
Intent
• Improve the accuracy and provision
of relevant data and information.
• Focus reporting on key performance
indicators to enable evidence-based
decision making at all levels.
Intent
• Develop and enforce robust
financial decision making and
controls across the
organisation.
• Maximise available revenue.
Service Delivery
& Efficiency
01
People, Culture
& Governance
02
Information,
Evidence &
Insights
03
Finance, Cost &
Revenue
Management
04

Page 8
Initiatives to improve patient outcomes and healthcare service delivery form a key component of the comprehensive
Organisational and Financial Recovery Plan. However, the governance and provision of clinical care to patients will remain
under the direct control and oversight of the CALHN CEO.
Key initiatives
Recovery initiatives will be delivered under each operating lever/implementation workstream over the three-year recovery
period as follows:
Service Delivery & Efficiency People, Culture and
Governance
Information, Evidence and
Insights
Finance, Cost and Revenue
Management
1. Process and practice
improvement, including:
• Improve patient flow
• Improve patient
discharge practices
• Ensure integrated
operational planning
• Minimise unnecessary
hospital admissions
2. Improve staff
engagement and
capacity building
3. Achieve efficiencies and
cost savings in
infrastructure and
resource utilisation
4. Improve facility and IT
assets and their impact
on resource
effectiveness
5. Improve Departmental
efficiencies
1. Redesign the CALHN
organisational structure
and accountabilities
2. Strengthen the HR
function across CALHN
to develop and support
a strong workforce
3. Ensure relevant
leadership and
capability development
occurs
4. Establish project
governance structures
and protocols
5. Develop and implement
a fit for purpose Risk
Management framework
1. Define and establish an
effective Data and
Reporting Function
2. Develop a streamlined
data and reporting
framework
3. Develop revised
monthly management
reporting packs
4. Establishment of future
state reporting
structures, analytics
and education
programs
5. Optimise clinical coding
strategy and education
6. Establish best practice
clinical coding and
revenue management
team
1. Develop an activity-
based budget
2. Improve accounting for
and management of
block funding
3. Optimise public and
private patient revenue
4. Improve contract
management controls
5. Improve cost
management controls
6. Optimise management
of non-clinical services
7. Review Statewide
Clinical Support Services
(‘SCSS’) service costs to
CALHN
8. Optimisation of Shared
Services (payroll,
accounts payable etc)
Program Governance - Stakeholder Change and Communications - IR Engagement
The Recovery Plan initiatives, priorities, risks and timeframes documented in this report reflect our initial planning response.
Whilst we are confident that this reflects a comprehensive and achievable roadmap for CALHN’s organisational and financial
recovery, we fully expect the Recovery Plan to be dynamic and to continue to evolve during the course of implementation.
Whilst target outcomes and guiding principles will remain constant, we will closely monitor progress on individual workstreams
and change initiatives, re-prioritising the forward work program as necessary to maintain operational flexibility and momentum.

Page 9
Financial Overview
CALHN needs to transition from an unfavourable forecast variance to budget of $274 million to a balanced budget by 2021.
The streams of activity in the Recovery Plan will provide a framework for actionable implementation of cost reduction and
financial performance improvement. We estimate that, based on the assumptions outlined in this report, CALHN’s
unfavourable variance to budget will be eliminated over the next three years.
The Recovery Plan will drive cost reduction and financial
performance improvement across four key areas:
1. Reducing Length of Stay (‘LOS’) to national
benchmarks.
2. Undertaking all activity efficiently and ensuring
unfunded activities are identified and appropriately
managed.
3. Improving management of CALHN workforce to
maximise patient facing time.
4. Other improvements (including medical coding,
revenue collection, outpatients and corporate
efficiency gains).
Governance and oversight
The CALHN Transition Board will provide governance and oversight during the period of the Recovery Plan. The proposed
governance framework is driven by the urgent need to improve the quality of services for patients and ensure consistent
delivery of improved performance. The Minister for Health and Wellbeing is the responsible minister. Regular reports and
updates will also be provided to the Treasurer.
Budget variance – historical and forecast (excluding SCSS) ($million)
Recovery period
Organisational and
Financial Operating levers
Minister/s
Operational oversight
Government
Operational detail
CALHN functional delegation
Minister for Health and Wellbeing
SA Health – Chief Executive
Governing Board or Steering
Committee
Clinical care
CALHN CEO
Administrators
0402 0301
Treasurer
CALHN Transition Board/
Governing Board

Page 10
Key Risks
Several key risks have been identified that could influence the successful delivery of the Recovery Plan. Each of these has
been assessed, and appropriate treatment strategies developed to minimise the probability and/or consequence if the risk
was to be realised. The top six program risks are summarised below, with corresponding mitigation strategies outlined in the
body of this report:
Ref Risk description
1
Political commitment to the turnaround is not
maintained for the required three-year period which
leads to the recovery being deprioritised or stopped.
2
Workforce representatives attempt to block
employee-related changes that are necessary to
achieve forecast turnaround outcomes.
3 Individual disgruntled clinicians seek political
interference to resolve individual issues.
4
Other important priorities e.g. The Queen Elizabeth
Hospital (‘TQEH’) redevelopment, start diverting
resources and executive attention from the Recovery
activities.
5
An integrated electronic records system for CALHN is
significantly delayed or not implemented, impacting
the quality and usefulness of data available for
clinical and operational insights
6 Planned initiatives fail to achieve the projected
outcomes required to realise financial benefits.
Activities and timelines
Following below is the high-level timeline and key outcomes for the CALHN organisational and financial Recovery Plan.
Note: the indicative timeline represented above reflects a recovery plan over three calendar years based on the anticipated recovery plan implementation start
date in late 2018. During the course of the implementation phase, interim performance targets and milestones will also align with corresponding financial years for
reporting purposes.
Consequence
Insignificant Minor Moderate Major Severe
Lik
eli
ho
od
Almost
certain
Likely
Possible
Unlikely
Rare
16
2 3
4
5
Aug 18 Sep 18 Oct 18 Nov 18 Dec 18 CY19 CY20 CY21
Diagnostic
Recovery Program Launch/Stabilisation Recovery
Phase Recovery Phase Recovery
Phase
Key outcomes:
• Understand organisation and
stakeholders.
• Determine source of financial
and clinical problems.
• Identify range of options to
address problems.
• Prioritise and plan recovery
roadmap and target
initiatives.
• Identify stakeholders and
determine key contacts who
can lead and influence
change.
• Prepare diagnostic report.
• Hold staff meetings and
briefings outlining plan and
forward path.
• Implement new controls and
reporting frameworks.
• Implement new governance
framework.
• Develop a new
organisational structure.
• Agree priorities to action in
respect of improving patient
flow.
• Establish Project
Management office.
• Establish a clinical leaders
change program.
• Restructure the organisation and build a strong
accountability and governance structure.
• Improve staff engagement and leadership
capability.
• Establish a central data, insights and reporting
capability to guide and inform decision making.
• Build the tools and capability to enable strong
financial management across all departments.
• Achieve interim performance targets and
milestones.
• Improve service delivery efficiency and clinical
outcomes.
Planning
• Prioritise and
plan recovery
roadmap and
target initiatives.
• Commence staff
engagement and
communications.
• Prepare planning
report.

Page 11
The overarching program is supported by the following:
• A program governance structure to ensure that initiatives are delivered with reference to a control environment and with
an overarching steering committee to make decisions on program direction and benefits.
• An integrated stakeholder change and communications strategy to manage the impacts to stakeholders, and ensure
clear communication and engagement throughout the recovery project.
• An overarching IR engagement strategy to engage with workforce industrial representatives and manage the delivery of
changes impacting the workforce.
‘Day Zero’ activities
‘Day Zero’ (Monday 26th November 2018) will launch the Stabilise phase with a focus on regaining the stability of the
organisation through a series of control mechanisms. These include:
• Introducing procurement controls using existing systems.
• Implementing controls over recruitment and backfilling of roles, and approval of overtime.
• Launching a new monthly management reporting pack to focus operational management attention on critical data.
• Executive team self-assessments.
Conclusion
Whilst the organisational and financial recovery of CALHN will be a complex and, at times, challenging undertaking, we are
confident that with the appropriate leadership, resourcing and stakeholder commitment, the target outcomes can be achieved
within a three-year timeframe.
We expect to complete the organisational and financial recovery described in this Recovery Plan within CALHN’s existing
funding envelope.

Page 12
2. CALHN Recovery Plan
| Guiding Principles and Initial Controls

Page 13
2 CALHN Recovery Plan | Guiding Principles and Initial Controls
2.1 Primary objectives
The primary objectives of the CALHN Organisational and Financial Recovery Plan are to:
1. Ensure CALHN becomes a high performing and accountable healthcare network that operates to Australian benchmark
standards across all domains;
2. Maintain and improve community access to CALHN facilities and services;
3. Maintain and improve services to, and within, the community to support CALHN activities;
4. Support improvement of the quality of clinical outcomes delivered in all CALHN services;
5. Enable CALHN to build on the single-service, multi-site service planning, emphasising accountability at the local level;
6. Ensure CALHN develops and embeds a culture of continuous improvement and a commitment to improving healthcare
outcomes for the community it serves;
7. Create disciplined, repeatable and consistent processes and controls across CALHN;
8. By December 2021, ensure that CALHN is delivering improved patient outcomes and performing at or better than the NEP
across all specialties and facilities;
9. Ensure external advisors assist in skills transfer to CALHN and SA Health staff and stakeholders.
2.2 Key implementation principles
The following principles will guide the implementation of the Organisational and Financial Recovery Plan for CALHN:
• Patient care and health outcomes remain the primary focus of CALHN;
• Regular and meaningful input will be sought from all CALHN workforce stakeholders;
• CALHN will:
− treat all individuals with respect and empathy;
− act with honesty, integrity and transparency in all our dealings;
− become an evidence-based decision-making organisation;
− acknowledge that some current practices may not reflect contemporary standards and will need to change;
− learn and adopt appropriate local, national and international best practices;
− continue to maintain constructive relationships with workforce representative stakeholders;
− provide appropriate training and professional development to the CALHN workforce;
− develop and respect operational and financial controls;
− acknowledge that developing a sustainable healthcare network is an acceptable organisational target;
− acknowledge that succession planning is an important enabler of workforce management and organisational
sustainability;
− not tolerate personal or departmental fiefdoms and agree that unacceptable behaviours should be ‘called out’;
− work hard to develop stronger relationships with our internal and external suppliers;
− clearly define individual responsibilities and hold people to account;
− celebrate milestones and success along the way.

Page 14
2.3 Vision to deliver the Triple Aim of Healthcare
Various existing planning documents at CALHN refer to the aspiration of delivering the Triple Aim of Healthcare,
an internationally accepted and proven conceptual framework for optimising health system performance. We
believe this Triple Aim should continue to be the focus of CALHN.
Triple aim System vision
• The health and wellbeing of the community served by CALHN will improve as a result of CALHN delivering
coordinated and integrated health prevention, intervention and treatments at scale in the community.
• CALHN will continue to develop alternative treatment pathways for patients, including through improving
access to the primary and community care sectors.
• More community-based treatment options will improve health outcomes while reducing emergency
demand.
• CALHN will also focus on improving the health and wellbeing of staff and ensure that all staff work in an
environment where they are provided with the access to opportunity and appropriate training.
• CALHN will address unwarranted variation in clinical outcomes and effectiveness.
• CALHN will tackle long length of stay patients by identifying and addressing system and site process,
procedure and control inefficiencies.
• CALHN will ensure that outpatients are managed effectively and ensure that care is provided in the most
appropriate environment.
• Effectively manage clinical risk environments to achieve benchmark standards, including minimising
prevalence of hospital acquired infections and complications.
• Holding itself to account against a range of quality and value benchmarks like the NEP and HRT, CALHN
will deliver efficiencies and generate economies of scale across the network.
• CALHN will think differently and creatively about meeting the rising demand implications for healthcare in
the community.
• CALHN will ensure that its’ risk management and control environment is fit for purpose and focuses on
achieving best practice.
• Sustainability does not just mean money – CALHN will consider the application of innovative technologies
and work practices to allow staff to work smarter and do more good for vulnerable patients.
• Ensure corporate and clinical risk environments are appropriate and deliver to benchmark standards.
1.Health and
wellbeing
2.Quality
of care
3.Sustainability

Page 15
2.4 Workforce engagement principles
A key enabler of the organisational and financial recovery of CALHN will be the engagement of the entire
CALHN workforce. We outline below the workforce engagement principles we propose to adopt. For the
avoidance of doubt, these are intended more as a set of principles to be applied in parallel throughout the
Implementation Phase, rather than sequential steps.
Intent
Review activity occurring across the
organisation and be willing to stop
activities and focus limited resources.
Approach
• Review all existing improvement activities and initiatives
occurring across CALHN.
• Assess which activities, programs and committees are
ineffective.
• Redirect limited resources to high-return activities.
• Identify all unfunded activity and manage appropriately.
Intent
Provide visibility of performance and
arm the managers with timely,
accurate and relevant information to
make decisions. Support quality
leaders to advocate and make
change.
Approach
• Acknowledge and communicate performance issues and
expectations.
• Clarify decision rights and identify and empower leaders
across the organisation.
• Champion data transparency and focus reporting on what
managers need to make informed decisions.
• Establish a clinical leaders’ change program.
Intent
Let managers manage and begin
making evidence-based decisions.
Approach
• Develop targeted, clear performance plans and assign owners
at the level needed to effect change.
• Establish reporting process, monitor progress and remediate
things that are not working as they happen.
• Manage utilising a single source of truth.
Intent
Expect results. Hold leaders to
account, consistently track outcomes
and continually remediate issues.
Approach
• Work towards NEP benchmarks.
• Improve clinical outcomes, staff and patient experience.
• Hold individuals and departments to budgets and
performance outcomes.
Stop
Empower
Manage
Perform

Page 16
2.5 Four key operational levers for recovery
The Recovery Plan will employ a set of four key operational levers that are aligned with the target end-state
outcomes and will inform the Recovery Plan workstreams. In addition to a range of service delivery initiatives,
improved clinical care and outcomes will be a key focus area informing decision making across all
workstreams.
Intent
• Put patient outcomes at the
centre of decisions.
• Structure the delivery of services
to be efficient and well-planned.
• Recognise and manage towards
expectations of clinical
performance.
Approach
• Procedural efficiencies and appropriate management tools
• Streamlined patient flow
• Improve patient discharge practices
• Support for hospital avoidance strategies
• Integrated operational planning and management
Intent
• Create a culture of leadership and
accountability at all levels of the
organisation.
• Improve workforce engagement.
Approach
• Workforce engagement
• Redesign organisational structure and accountabilities
• Strengthen HR functions and controls
• Leadership and capability development
• Establish project governance structures and protocols
• Develop and implement a Risk Management framework
• Review OH&S protocols and approach
Intent
• Improve the accuracy and
provision of relevant data and
information.
• Focus reporting on key
performance indicators to enable
evidence-based decision making
at all levels.
Approach
• Ensure single source of truth
• Concise, insightful and visual data reporting
• Clinical coding strategy and education
• Internal and external benchmarking
• Consistent, timely performance reports
• Undertake mini-audits in respect of underperforming activities
• Explore available best practice technology service providers
Intent
• Develop and enforce robust
financial decision making and
controls across the organisation.
• Maximise available revenue.
Approach
• Activity based budget
• Block funding management
• Optimise public and private patient revenue
• Contract management controls
• Cost management controls
• Control of clinical and non-clinical services to CALHN
• Optimisation of Shared Services
Service Delivery
& Efficiency
01
People, Culture
& Governance
02
Information,
Evidence &
Insights
03
Finance, Cost &
Revenue
Management
04

Page 17
2.6 High level recovery timeline
We outline below the high-level timeline for the launch and completion of the CALHN organisational and financial Recovery
Plan.
Note: the indicative timeline represented above reflects a recovery plan over three calendar years based on the anticipated recovery plan implementation start
date in late 2018. During the course of the implementation phase, interim performance targets and milestones will also align with corresponding financial years for
reporting purposes.
Aug 18 Sep 18 Oct 18 Nov 18 Dec 18 CY19 CY20 CY21
Diagnostic
Recovery Program Launch/Stabilisation Recovery
Phase Recovery Phase Recovery
Phase
Key outcomes:
• Understand organisation and
stakeholders.
• Determine source of financial
and clinical problems.
• Identify range of options to
address problems.
• Prioritise and plan recovery
roadmap and target
initiatives.
• Identify stakeholders and
determine key contacts who
can lead and influence
change.
• Prepare diagnostic report.
• Hold staff meetings and
briefings outlining plan and
forward path.
• Implement new controls and
reporting frameworks.
• Implement new governance
framework.
• Develop a new
organisational structure.
• Agree priorities to action in
respect of improving patient
flow.
• Establish Project
Management office.
• Establish a clinical leaders
change program.
• Restructure the organisation and build a strong
accountability and governance structure.
• Improve staff engagement and leadership
capability.
• Establish a central data, insights and reporting
capability to guide and inform decision making.
• Build the tools and capability to enable strong
financial management across all departments.
• Achieve interim performance targets and
milestones.
• Improve service delivery efficiency and clinical
outcomes.
Planning
• Prioritise and
plan recovery
roadmap and
target initiatives.
• Commence staff
engagement and
communications.
• Prepare planning
report.

Page 18
2.7 Proposed immediate controls
CALHN’s spends around $600 million per annum on supplies and other services. Under current protocols and
practices there are limited effective controls over who orders what and, in many instances, purchases are
made outside of the normal purchasing guidelines. Similarly, CALHN continues to expand Full Time Equivalent
(‘FTE’) well in excess of commissioned and budgeted levels, with a more effective control environment for
recruitment, rostering and overtime urgently required.
2.7.1 Procurement controls
2.7.2 Workforce controls
01
02
03
04
05
Amend policy to state all purchases require Purchase Orders.
No payments made without Purchase Orders.
Ordering of uncatalogued items to require Administrators approval.
Purchases over $110,000 to require Administrator approval.
Agency nurse invoices to be reconciled against ProAct.
01
02
03
04
06
Administrator representatives to be on the CALHN Appointment Committee.
Administrator representative approval required in E-Recruit for backfilling.
Restrict E-Recruitment Panel Members selection.
Update E-Recruitment requisition form to ensure clear justification.
Expedite rollout of a Workforce Analytics, Modelling and Optimisation Tool.
05 Unplanned overtime in ProAct to be approved by Nursing Director.

Page 19
2.8 Monthly management reporting pack
As an essential management tool and to focus operational management attention on critical data we are developing a monthly
management reporting pack.
The management reporting pack will provide a visual, intuitive and network-wide representation of CALHN’s performance
against key measurable, actionable and accountable metrics in the following three areas: Patient Flow, People and Culture
and Financial Performance.
These features will empower CALHN staff to monitor not only CALHN’s current performance but monitor the change on an on-
going basis. This performance visibility will help drive accountability and ownership of CALHN performance throughout the
network.
2.8.1 Management reporting development, deployment and monitoring
We envisage that the management reporting pack will evolve through three primary stages, comprising: Development,
Deployment and Monitoring, depicted below along with the associated interactions and summary communications.
The table below details the interaction and involvement with stakeholders at each of the three stages in further detail:
Stage Time frame Stakeholders Interaction/involvement
Development
Identification and
incorporation of key
metrics, data sources
and reporting pack
development
Planning • CALHN executive team (i.e. CEO, CFO etc)
• Key senior leaders and stakeholder
(i.e. Clinical Service Directors)
• Overall impact and interoperability of the reporting
pack
• Suitability and validity of metrics and data
represented in the reporting pack
• Assignment and association of metric accountability
throughout the CALHN leadership team
Deployment
Initial top-down
deployment of the
reporting pack and
metric accountability
Stabilise
(pre-Day
Zero)
• Senior leaders and stakeholders including:
− Executive team (incl. Clinical Service
Directors)
− Clinical Directors
− Nursing Co-Directors
− Business Operation Managers
− Heads of Unit
• Intent and interoperability of the reporting pack and
metrics
• Availability and timeliness of management reporting
data
• Communication of metric ownership and
accountabilities
Stabilise
(post Day
Zero)
• CALHN employees • Intent and interoperability of the reporting pack and
metrics
• Availability and timeliness of management reporting
data
Monitoring Stabilise and
future • CALHN executive team
• Senior leaders and stakeholders
• Periodic key metric reporting and performance
justifications through workgroup or committee
meetings
• Review and evaluation of proposed management
reporting, metrics and data source enhancements
• Review data validity/timeliness and management
reporting delivery effectiveness
Development
Including: • Collaborative
involvement/input from senior CALHN executives and leaders.
Deployment
Including: • Initial top down
deployment and communications with senior leaders and stakeholders.
• Relevant CALHN wide delivery. communications.
Monitoring
Including on-going: • Stakeholder monitoring
and metric performance reviews.
• Metric, data and visual enhancements.
• Periodic and timely reporting deliveries.

Page 20
2.9 CEO Executive Management and Organisational On-boarding
In order to effectively support the newly appointed CEO it will be a timely and important step to commence an on-boarding
process encompassing both the organisational performance of CALHN and a self-assessment by individual CALHN executives.
2.9.1 Individual self-assessment by Executive Management Team
Each member of the CALHN Executive Management Team will take stock and reflect on the professional challenges and
opportunities that lie ahead.
We will ask each individual in the CALHN Executive Management Team to complete a self-assessment in anticipation of the
responses being discussed with the new CEO.
2.9.2 Organisational On-boarding
The organisational assessment will take the form of a proven Performance Assessment Audit template to be completed by
each member of the CALHN Executive Management Team, assessing the current status of the organisation in relation to a
range of key factors associated with each of a set of four important themes, as summarised below.
Response driven scores (0 - 10) are then aggregated to develop a composite view of the organisation’s current perceived
performance as well providing a baseline for benchmarking against peer organisations, the degree of variance between
executives internally and monitoring of change over time.
Part 1:
Strategic Clarity
Part 2:
Process Management
Part 3:
Healthcare Improvement
Methods & Techniques
Part 4:
Value Stream Stakeholder
Integration
1. Strategic Focus
2. Strategic Focus Deployment
3. Communication
4. Strategic Top-Level Metrics
5. Metric Deployment
6. Strategic Targeting
7. Targeting Deployment
8. “Catch-balling”
(management review
checking alignment to
strategy and targets)
9. Catch-balling by Time Period
1. Key Business Processes
2. Management Control
3. Reporting Structure
4. Cross-Functional/Multi-
disciplinary teamwork
5. Treatment/Service Value
6. “Waste” – non-value adding
time, effort, duplication, re-
work, errors etc
7. Process integration
8. Measures of Process
Capability
9. Continuous Improvement
1. Forward demand/capacity
alignment planning
2. Levelled Work Flow
3. Manage by Fact
4. Flow
5. Pull
6. Quality
7. Standards
8. Plan-Do-Check-Act
9. Equipment Effectiveness &
Reliability
10. Workplace Organisation
(5S)
1. Planning Horizon
2. Manage by Fact
3. Relationship and Trust
4. Connection between value
stream stakeholders
5. Quality from a patient’s
perspective
6. Inter-organisation Waste
7. Intra-organisation Waste
8. Schedule Stability
9. Learning Curve
Source: Bernie Kelly, Reliable Excellence in Care Research, adapted from material developed by Professor Peter Hines, Cardiff University.

Page 21
2.10 Organisational design reset
2.10.1 Overview
CALHN’s current organisational design is not fit for current needs. Reporting lines and responsibilities are not clear, spans of
control are too large. Further, there is no single, clearly documented, organisation chart of positions or people. A summary of
CALHN’s current executive organisation structure is provided in Appendix 3.
Despite the prevailing organisational dysfunction, the scale and complexity of the CALHN organisation is such that any revised
structure must necessarily be designed to accommodate the ‘now’ – incorporating existing systems and infrastructure. Given
the breakdown in operational and financial control and oversight it is critical that each site within CALHN receives more
immediate and focused management at the site level. Organisational design refinement may then evolve in time once effective
systems and controls are embedded.
It is also important that the incoming CALHN CEO, Lesley Dwyer, plays a key role in defining the future organisational structure.
We will also work with the CALHN Governing Board to establish a robust framework for effective board committees, controls
and delegations, including appropriate terms of reference and resourcing and skillsets. There are a range of proven models
which can be adopted from other well-functioning health networks and we would anticipate having an appropriate Governing
Board infrastructure in place by the time the Board becomes fully operational.
2.10.2 Organisational design principles
There are a wide range of important characteristics and interdependencies to consider in developing an effective new
organisational structure for CALHN. Our high-level guiding principles for the organisational redesign can be summarised in the
diagram below, with further detail outlined following.
More specifically, CALHN’s future organisational structure should support an enterprise which is:
Locally
Accountable
Local accountability at a site level. Communities identify with their local hospital and expect decisions
affecting patient care to be made and implemented at the local site level.
Clinically Multi-
disciplined
Recognise that old professional boundaries have blurred, and modern healthcare professionals need
to work in multi-disciplinary teams to provide holistic and high-quality care.
Leveraging Scale
Leveraging the benefits of scale effectively. This requires working out where and how CALHN facilities
can be most efficient and effective, using all the resources at CALHN’s disposal. It also means CALHN
needs to be able to coordinate and integrate its efforts across the various sites and services.
Administratively
Lean
The scale of CALHN’s network executive functions should reflect its position in the context of a
decentralised Metropolitan healthcare network, with an emphasis on ensuring local accountability
wherever possible. Network senior executive roles should be primarily strategic/policy focused except
for those limited transactional areas where it is best to run a service at Group rather than local facility
level. Most transactional services for CALHN are at present provided by SA Health e.g. procurement.
Clear in Purpose Just as CALHN needs to be clear on its purpose at a Group level, each of its sites needs to be clear on
its purpose or reason for existence.
Patient focussed Clear lines of
accountability
Site based
and logical
Appropriate
spans of control
01 02 03 0401 02 03 04

Page 22
Data-driven The structure should support a strong focus on data analytics and informatics as core components of
a highly performing health network in terms of quality and efficiency of services.
Innovative The structure should support a strong focus on innovation, including through use of technology and
digital platforms (IT and medical/surgical).
Empowering
Research &
Education
Including education of healthcare professionals for its own purposes and the broader State, as well
as education for stakeholders such as General Practitioners, patients and their families.
Responsible Active, timely and appropriate decision making. Give people authority and responsibility, and hold
people to account for their performance.
Adaptable The organisational structure should support CALHN’s group strategy and be able to adapt as the
strategy changes.

Page 23
2.11 Governance and performance management reset
2.11.1 Overview
Current shortcomings in organisational governance and performance management, together with proposed responses are
summarised in the table following:
Priority issues Impact Response
1 Lack of role and expectation
clarity • Leaders, managers and staff are not aware
of their roles, what is expected of them and
what they will be held accountable for.
• Role descriptions in place for all staff.
• All Committees have a charter.
• All Key Performance Indicators (‘KPIs’) have a
CALHN executive allocated to them.
• Documentation and implementation of decision-
making and issues-management hierarchy.
2 Lack of accountability • Decision-making is devolved to committees
with individuals not held accountable for
performance.
• All plans are to be documented.
• Actions to be taken are documented, with follow
up on progress and outstanding items.
• KPIs are allocated to individual owners.
3 Decisions are not driven by
consistent data • Time and focus is wasted debating sources
and accuracy of data.
• Decisions are not made.
• Agreed single source of truth forms basis of
reports used for decisions.
4 Performance is not managed
in an integrated manner which
considers clinical, people, and
financial outcomes
• Performance is managed in silos.
• Decisions are made which do not consider
all clinical, people and financial outcomes.
• Design and implementation of an Integrated
Management Systems incorporating a planning
and decision-making structure that considers all
clinical, people and financial outcomes.
2.11.2 Key principles
In addition to the proposed initiatives outlined above, a set of key performance governance and management principles will be
developed which govern all performance management activities.
Clarity People know what their role is, what is expected from them, and for what they will be held
accountable.
Accountability People are held to account for what they say they will do, and deadlines relating to those activities.
Timeliness Actions are given deadlines.
Data-driven Decisions and actions are driven by data and insights, and data issues (including lack of data) are not
a reason/excuse to not make decisions or take actions.
Action-oriented There is a focus throughout the organisation on making decisions and acting quickly. “Don’t let
perfect be the enemy of good.”
Aligned Decisions and actions must align to the overall CALHN strategy, and other decisions and actions that
are being made. Everyone must be pulling in the same direction.
Integrated Performance and decisions are viewed holistically in terms of clinical outcomes, people and culture
outcomes, and financial outcomes.

Page 24
3. CALHN Recovery Plan
| Implementation Approach

Page 25
3 CALHN Recovery Plan | Implementation Approach
As an essential element of improved governance and oversight, the CALHN Transition Board has been
immediately stood-up in advance of the Governing Board formally being constituted.
3.1 Context and overview
3.1.1 Appointment and role of Administrators
In light of the current performance and future outlook, it is proposed that Administrators be appointed to lead the Recovery
Plan for a period of up to three years.
We envisage that key responsibilities of the Administrator role will comprise:
1. Serving as the principal architects of the Organisational and Financial Recovery Plan of CALHN and ensure its effective
implementation
2. Serve as a catalyst to constantly energize the organisational and financial recovery process and to maintain the
momentum
3. Provide overall leadership for and specific management of the organisational and financial recovery process as it
progresses over a three year period, noting the bespoke Administrator role may cease in that time and revert to
management support as required
4. Create and maintain a supportive organisational climate for successful change and effective transition to the renewed
organisation following completion of the program
5. Identify any activities or programs at CALHN that have SA Health system benefit or impact and actively engage with SA
Health representatives on these matters.
The Administrators will work closely with the CEO and Group Executive of CALHN who will retain overall responsibility and
primary responsibility for patient care and clinical outcomes.
A summary operational structure chart is provided in Section 3.2 following.
3.1.2 Outcomes to be achieved by Administrators
The proposed Administrator governance framework is driven by the need to improve the quality of services for patients and
ensure consistent delivery of improved performance, and includes:
• Rapid roll out of extra controls to immediately strengthen financial control
• Rapid implementation of an Organisational and Financial Recovery Plan
• Plan to achieve National Efficient Price within three years
• Buy-in from key stakeholders and quality-assurance measures
• Consistent improvement in quality and patient safety indicators as a direct result of actions taken as part of the financial
recovery
• Addressing significant financial governance failures, with necessary actions to ensure stability into the future
• Robust management systems in place to deliver the organisational financial recovery plan.
A more detailed summary of the specific actions the Administrators may take to establish and maintain an effective control
and accountability environment, together with a rigourous performance review programme, is provided in Appendix 4.

Page 26
3.2 Indicative Recovery Plan organisational structure
Minister for Health and WellbeingMinister/s
SA Health – CE
Steering Committee Governing Board Operational
Oversight
Clinical
• Day to day clinical functionality
• Patient care and outcomes
Government
Statutory Body to
provide formal
approval of plans,
liaison to
Government
Provide Governance and
oversight during the Recovery
Program and support the work
of the Administrators
CALHN CEO
Operational
Detail
Day to Day operationAdministrators
CALHN
Functional
Delegation
04Finance, Cost &
Revenue Management
02People, Culture
& Governance
03Information, Evidence
& Insights
01Service Delivery &
Efficiency
Treasurer
CALHN Transition Board/Governing Board

Page 27
3.3 Recovery Plan governance framework
Practically, to deliver the Recovery Plan, the Administrators should be provided with Standard Level 1 Delegated Authority (in a
manner similar to the incumbent CALHN CEO derives authority from “Delegation for Financial Authorisations - Updated for
approvals by the CEO, CALHN as at 31 January 2018”).
The remaining key points for the Recovery Plan governace framework will be:
• Financial and procurement authorisation levels for Administrators – to Standard Level 1 (max: $550,000 incl GST with
limitations). Additional approvals above this value will require approval in the normal course (i.e. SA Health CE approval,
etc.) with reference to the Board – the delegation mapping is currently being developed.
• The CEO will retain delegated authority to Standard Level 1.
• All other existing delegations (specifically including CFO and COO) will be subordinated to Standard Level 4 (max: $55,000
including GST with limitations).
• Any additional employees will be subject to the rules of the Appointments Committee as set out in this document. For
clarity however, any appointment will require Appointments Committee approval and, separately, specific approval from
one of the Administrators representatives.
Specific delegation mechanics and relevant indemnities to be provided to Administrators are yet to be resolved.
3.3.1 Administrators Organisational and Financial Recovery Plan
The Administrators would implement a detailed implementation plan which demonstrates a road map to achieve an
organisatonal and financial recovery over a three year period, the CALHN Organisational and Financial Recovery Plan.
3.3.2 Ministerial Oversight of Administrators
While CALHN is the responsibility of the Health Minister it is not unusual in circumstances of organisational and financial
distress for oversight of the turnaround process to be shared between the responsible Minister and either the Treasurer (or
Finance Minister). We propose that the Minister for Health and Wellbeing retain day to day oversight with regular reports
provided to the Treasurer.
It is currently anticipated that the Administrators will be engaged with delegated authority from the CEO of CALHN.
3.3.3 Governance & Oversight
The CALHN Transition Board and Governing Board will provide governance and oversight during the period of the Recovery
Plan.
It is intended that the Governing Board will meet at least monthly.
The CALHN Transition Board and Governing Board may seek advice from other specialist advisors from time to time, for
example legal and industrial relations advisors.
3.3.4 CALHN CEO Role and Authority
The Chief Executive Officer (‘CEO’) provides leadership to the Local Health Network (‘LHN’) and is responsible for the sound
governance and management of the LHN to ensure that:
• The LHN fulfils its purpose, effectively exercises its functions and complies with its financial and policy obligations
• The LHN meets its obligations to deliver agreed services within an agreed budget and which meet specified performance
standards, under its annual LHN Service Agreement with SA Health
• The LHN implements SA Health service plans and policy
• An annual report in respect of the LHN’s finances and activities is produced which is compliant with State statutory,
financial accountability and audit requirements
• Effective communication and consultation mechanisms with SA Health entities and services, other State entities and local
stakeholders, including clinicians and the community, are established and maintained.
The CALHN CEO will retain day to day responsibility for the management of clinical and patient interactions and outcomes.

Page 28
3.3.5 Administration team structure
The proposed structure and key responsibilities of the Administration team are summarised overleaf, with the Administrators
having select delegated authorities from the CALHN CEO to plan and implement an organisational and financial recovery
strategy for the organisation in accordance with agreed principles.
Again, the CALHN CEO will retain day to day responsibility for the management of clinical and patient interactions and
outcomes across the organisation, with coordinated support from the Recovery Plan in terms of improving service delivery and
the improved patient outcomes this will facilitate.

Page 29
Proposed Administration team structure
The Royal Adelaide Hospital (‘RAH’) Public Private Partnership (‘PPP’) contract, the operations of SCSS (other than as a major
supplier to CALHN), various whole-of-government shared services (accounts payable/receivable) and SA Health provided
services (IT, payroll) are outside the direct scope of the Recovery Plan.
However, the various contracts and counterparties remain operationally significant to CALHN and accordingly we anticipate
maintaining regular engagement with these stakeholders on an ongoing basis, including providing relevant feedback to
SA Health.
03Information, Evidence and
Insights
04Finance, Cost and Revenue
Management
01aService Delivery &
EfficiencyInpatient activity improvement
and turnaround
01bService Delivery &
EfficiencyNon-inpatient activity
improvement and turnaround
Key responsibilities
• Program management and reporting
• Communications program
• Stakeholder management and reporting
• Media management
• Daily, weekly, monthly dash boards
• SA Health information interface
• HRT benchmarking
• CAHLN internal benchmarking
• Activity based budget by facility
• Financial controls and contract
management
• Patient coding
• IR framework and legal response
• FTE and HR approvals and controls
• Enterprise and program risk identification
and management
• Integrated operating plan
• Patient flow
• Average length of stay
• Workforce efficiency/rostering
• Facility activity planning
• Unfunded activity management
• Outpatients
• Emergency Department
• Commonwealth funded initiatives
• Statewide Services (as supplier)
• Community Care
• Private practice arrangements
RAH PPP
Statewide Services
• Not Administrators responsibility
• Not Administrators responsibility(Including Statewide Clinical Support Services
and SA Government Shared Services)
02People, Culture &
Governance
• Organisational design
• Capability building and training
• Workforce management and planning
• Performance management
• Governance framework and structure
Administrators
Program Administration,
Communications and
Reporting
CALHN CEO
Clinical Care

Page 30
3.4 Recovery Plan risk assessment
In the following section, we summarise the key risks assessed at the program level. A similar, workstream specific, assessment
for each of the primary operating levers is also being developed for adoption during the Implementation Phase. Our approach
to identifying and assessing risk, together with a Risk Consequence Assessment Framework are summarised in Appendix 2.
3.4.1 Key Risks – Program level
A number of key risks have been identified that could influence the successful delivery of the Recovery Plan. Each of these has
been assessed, and appropriate treatment strategies developed to minimise the probability and/or the consequence if the risk
was to be realised. The program risks relate to the uncertainty of the external environment, the need for commitment to the
Recovery Plan, and the potential impact of the changes to the organisation’s workforce and patients. The Top 10 program-level
risks are detailed below.
Ref Risk description
Risk
Rating Risk treatment
1
Political commitment to the turnaround is not
maintained for the required three-year period which
leads to the recovery being deprioritised or stopped.
Extreme
Maintain close engagement with key stakeholders. Deliver regular
updates to illustrate progress/momentum.
2
Workforce representatives attempt to block employee-
related changes that are necessary to achieve forecast
turnaround outcomes.
High
Develop a proactive engagement strategy with each of the impacted
unions with clear negotiation position for each desired change.
Obtain timely legal advice where required.
3 Individual disgruntled clinicians seek political
interference to resolve individual issues. High
Early identification of delegated authority and commitment by key
stakeholders not to get involved in local activities or issues.
4
Other important priorities eg: the TQEH redevelopment,
start diverting resources and executive attention from
the Recovery activities.
High
Ensure that adequate executive resourcing and support exists for
business as usual operations, the Recovery Plan and other high-
priority projects.
5
An integrated electronic records system for CALHN is
significantly delayed or not implemented, impacting the
quality and usefulness of data available for clinical and
operational insights.
High
Liaise with SA Health to ensure the timely delivery of an electronic
record system following completion of the Enterprise Patient
Administration System (‘EPAS’) Independent Review.
6
Planned initiatives fail to achieve the projected
outcomes required to realise financial benefits. High
Closely align individual initiatives to planned financial benefits and
track progress closely. Fail fast on ‘no/low benefit’ initiatives.
Reassess planned benefits if schedule or quality changes.
7
Workforce uncertainty around recovery activities and
staffing impacts leading to further disengagement and
disruption, including increasing IR activity.
High
Plan and deliver a communications strategy that keeps all staff
regularly informed about the roadmap and progress against targets.
8
Changes to the organisational structure have an adverse
impact on the clinical performance of the organisation. Medium
Identify risks and probable impacts of individual projects. Utilise
pilots and 'test and learn' approaches where the clinical impact is
unknown. Closely monitor the delivery of initiatives.
9
Unexpected and significant increases in service demand
(i.e. Public demand for ED) create a diversion of
attention and/or resources from the Recovery Plan
Medium
Monitor demand for hospital and other network services. Address
unexpected demand through macro solutions.
10
Patients are negatively impacted by the turnaround
program. Medium
Ensure patients are considered as the key impacted stakeholder
group and appropriate planning and communications are
undertaken to minimise impact and ensure continuity of care.
Consequence
Insignificant Minor Moderate Major Severe
Lik
eli
ho
od
Almost
certain
Likely
Possible
Unlikely
Rare
16
2
8
9
3
10
4
7
5

Page 31
4. CALHN Recovery Plan
| Target Financial Outcomes
Page 32
4 CALHN Recovery Plan | Target Financial Outcomes
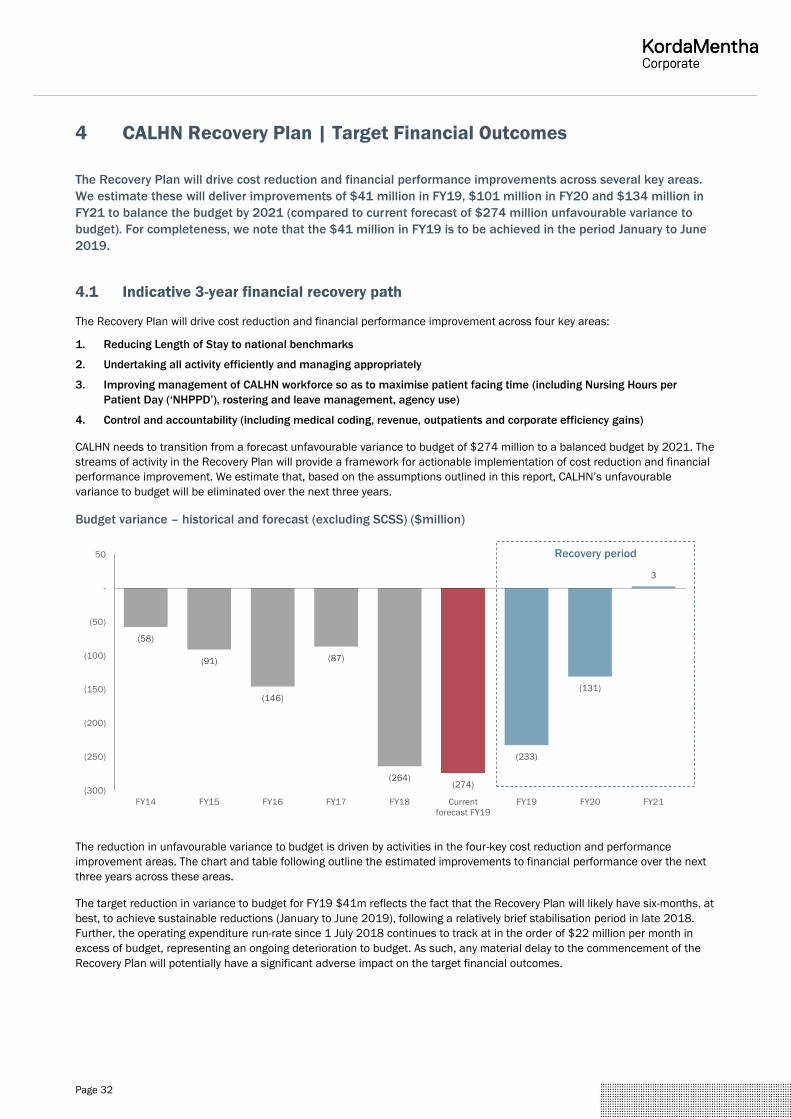
The Recovery Plan will drive cost reduction and financial performance improvements across several key areas.
We estimate these will deliver improvements of $41 million in FY19, $101 million in FY20 and $134 million in
FY21 to balance the budget by 2021 (compared to current forecast of $274 million unfavourable variance to
budget). For completeness, we note that the $41 million in FY19 is to be achieved in the period January to June
2019.
4.1 Indicative 3-year financial recovery path
The Recovery Plan will drive cost reduction and financial performance improvement across four key areas:
1. Reducing Length of Stay to national benchmarks
2. Undertaking all activity efficiently and managing appropriately
3. Improving management of CALHN workforce so as to maximise patient facing time (including Nursing Hours per
Patient Day (‘NHPPD’), rostering and leave management, agency use)
4. Control and accountability (including medical coding, revenue, outpatients and corporate efficiency gains)
CALHN needs to transition from a forecast unfavourable variance to budget of $274 million to a balanced budget by 2021. The
streams of activity in the Recovery Plan will provide a framework for actionable implementation of cost reduction and financial
performance improvement. We estimate that, based on the assumptions outlined in this report, CALHN’s unfavourable
variance to budget will be eliminated over the next three years.
Budget variance – historical and forecast (excluding SCSS) ($million)
The reduction in unfavourable variance to budget is driven by activities in the four-key cost reduction and performance
improvement areas. The chart and table following outline the estimated improvements to financial performance over the next
three years across these areas.
The target reduction in variance to budget for FY19 $41m reflects the fact that the Recovery Plan will likely have six-months, at
best, to achieve sustainable reductions (January to June 2019), following a relatively brief stabilisation period in late 2018.
Further, the operating expenditure run-rate since 1 July 2018 continues to track at in the order of $22 million per month in
excess of budget, representing an ongoing deterioration to budget. As such, any material delay to the commencement of the
Recovery Plan will potentially have a significant adverse impact on the target financial outcomes.
(58)
(91)
(146)
(87)
(264)(274)
(233)
(131)
3
(300)
(250)
(200)
(150)
(100)
(50)
-
50
FY14 FY15 FY16 FY17 FY18 Current
forecast FY19
FY19 FY20 FY21
Recovery period

Page 33
Estimated cost reduction and performance improvement ($million)
Key areas FY19 FY20 FY21 Total
$m % of total $m % of total $m % of total $m % of total
Length of stay 8 19% 44 43% 78 58% 130 47%
Activity levels and efficiency 12 28% 34 34% 25 19% 71 26%
Workforce management 9 21% 15 15% 17 13% 41 15%
Controls and accountability 13 31% 8 8% 14 11% 35 13%
Total 41 100% 101 100% 134 100% 277 100%
Note: Estimated FY19 savings will be achieved in a six-month period between January and June 2019. Totals subject to rounding.
4.2 Key financial performance drivers and sensitivities
There are a number of performance drivers for each of the four categories included above. The table following overleaf outlines
the high-level variance drivers and the assumptions underpinning the cost reduction and performance improvements.
Potential budget variance improvements related to length of stay are primarily based on reducing CALHN’s Relative Stay Index
(‘RSI’) to the median peer RSI, which is a key enabler in achieving NEP across CALHN’s activity. The associated reduction in
occupied bed days will also free up bed capacity and create optionality in bed management, including minimising access
blocks out of EDs, utilising beds for their intended use e.g. recovery vs inpatient, or periodically managing beds down to
commissioned levels where demand allows.
The actual savings achieved in respect of each key area may differ to the estimates depending on a range of variations,
sequencing decisions and organisational priorities. There are clearly significant elements of interdependency between the
primary variance drivers and we have sought to minimise the risk of double counting in estimated savings where possible.
Variance drivers
Category Variance driver Assumptions
Length of stay High average length of
stay of inpatients • Reducing the Relative Stay Index (‘RSI’) for RAH and TQEH to the median peer of RSI of
88% would generate potential cost efficiencies of approximately $130 million.
• This equates to an estimated reduction in the average length of stay of 1.5 days, which
would free-up approximately 65,000 Occupied Bed Days (‘OBD’) per annum to improve
bed management optionality (for intended use, alternative use, reserved for peak flex
etc, all subject to ongoing demand requirements).
• Impacts to length of stay require systemic improvements to multiple areas of the
network’s operations. Accordingly, we have assumed modest reductions in the average
length of stay of FY19 (4,000 OBD), improved reductions in average length of stay of
FY20 (22,000 OBD) and the largest portion of reductions average length of stay in FY21
(39,000 OBD) as a culmination of the work completed in the first 18 months of the
Recovery Plan.
8
44
78
12
34
25
9
15
17
13
8
14
-
20
40
60
80
100
120
140
FY19 FY20 FY21
Length of stay Activity levels & efficiency Workforce management Controls & accountability
$101m
$134m
$41m

Page 34
Category Variance driver Assumptions
Activity levels &
efficiency
Inpatient National
Weighted Activity Unit
(‘NWAU’) activity above
commissioned caps
• Management estimate that inpatient activity was 18,000 NWAU above cap in FY18.
• The additional cost associated with NWAU being delivered in excess of commissioned
levels equates to approximately $71 million. This assumes the estimated cost of the
additional activity is only at the current NEP of $4,503 (minus a discount applied to
account for indirect costs), excluding the actual CALHN cost above NEP to ensure no
double counting with other efficiency improvements.
• It is assumed that inpatient NWAU activity in excess of commissioned levels, including
elective surgeries, can be more effectively managed. Ensuring clinical coding is timely
and accurate will also help inform future activity commissioning and funding cycles.
• We have estimated that 20% of the inpatient NWAU activity above commissioned caps
can be addressed in FY19 (3,600 NWAU) with an increased improvement in FY20 (8,100
NWAU) and the remainder in FY21 (6,300 NWAU).
Workforce
management
Nursing hours per
patient day • Nursing hours per patient day in the period July to September 2018 has consistently
been above target, contributing to $2.8 million higher cost in this period, or around $11
million annualised. Target levels reflect the benchmarks set out in EAs.
• The cost reduction estimate is that 25% of this total cost ($2.8 million) will be recovered
in FY19 and FY20 respectively, with the final 50% ($5.5 million) recovered in FY21.
Nursing sick leave • Nursing sick leave hours as a proportion of total nursing hours for CALHN is significantly
higher than peers (12.9% at RAH and 11.3% at TQEH versus 5.4% at Flinders Medical
Centre (‘FMC’) and 4.3% at the Alfred).
• If CALHN can reduce its nursing sick leave hours at RAH to the levels achieved at the
Alfred this would result in an estimated cost saving of $9.7 million.
• Achieving this will involve cultural improvements and will be an output factor of other
recovery achievements. Accordingly, we have assumed that 15% ($1.4 million) of this
overall target is recovered in FY19, with an additional 35% ($3.4 million) recovered in
FY20 and half of the overall target is achieved in FY21 ($4.8 million).
Agency use • Agency use at CALHN is significantly higher than peers (5% of total nursing hours at RAH
and TQEH versus 2.2% at Melbourne Health, 1.4% at Princess Alexandra and 0.9% at
Alfred). Agency costs are forecast to be greater than $50 million in FY19.
• We have assumed that agency use can be halved through conversion of excess agency
use to permanent employees. Management advise that the agency premium is
approximately 40%. Accordingly, we estimate savings potential of $10 million.
• We have assumed 35% of this will be realised in FY19 ($3.5 million), with 50%
($5 million) recovered in FY20 and a further 15% ($1.5 million) in FY20.
Medical rostering • Management estimate that there are efficiency gains of approximately $10 million.
• The Recovery Plan will have a strong focus on improving operational efficiency including
rostering and workforce management. We estimate that, in-line with the roll out of these
initiatives throughout early 2019, 10% ($1 million) of the medical rostering efficiency
gains will be realised in FY19, 40% ($4 million) in FY20 and 50% in FY21 ($5 million).
Controls &
accountability
Private inpatient
revenue recovery • CALHN currently has in place a plan to increase private inpatient revenue by $16 million.
Management advise this will bring private inpatient revenue in-line with previous levels.
• We estimate that 75% ($12 million) of this revenue increase will be generated in FY19,
with a further 25% ($4 million) in FY20.
Outpatients efficiency
gains • Outpatients is funded for approximately $192 million per annum. CALHN are working
through a range of initiatives to improve the performance of the Outpatients Department.
• We assume that 5% ($9.6 million) of total funding can be realised as cost reductions.
• These initiatives will primarily improve throughput and manage activity levels. Additional
benefits to the network are likely to include decreased ED presentations, lower inpatient
admission rates from outpatients and improved information.
• Initiatives are anticipated to commence by FY20 and accordingly, 25% ($2.4 million) of
the savings target will be gained in FY20 and increase in FY21 (75% / $7.2 million).
Corporate efficiency
gains • Efficiency gains should be realised in corporate overhead costs in-line with activity
efficiencies and improved length of stay. We assume cost reductions of 5% will be found
in corporate efficiency gains for an approximate saving of $9.9 million.
• We expect that 10% ($1 million) of the corporate efficiency gain will be achieved in FY19,
a further 20% ($2 million) will be realised in FY20 and 70% ($6.9 million) in FY21.
Note: The actual savings achieved in respect of each key area may differ to the estimates depending on a range of variations, sequencing decisions and
organisational priorities.

Page 35
5. CALHN Recovery Plan
| Key Initiatives and Operating Levers

Page 36
5 CALHN Recovery Plan | Key Initiatives and Operating Levers
5.1 Overview
The initiatives of the CALHN Recovery Plan have been developed to address the key findings of the Diagnostic phase. During
the Planning phase, the initiatives have been scoped and prioritised based on those that will have the greatest impact on the
financial and clinical performance of the organisation or are essential enablers of change across the organisation. Where
possible, the program seeks to minimise the negative impact on stakeholders.
The roadmap for delivery of initiatives is planned around a series of phases:
Phase Purpose
Stabilise phase
(to end 2018)
Stabilise the organisation, engage the workforce, deliver priority changes with minimal roadblocks.
The Stabilise phase may stretch into early 2019 depending on the timing of the commencement of implementation.
CY2019 Deliver initiatives to empower leaders and address financial and clinical performance accountability.
CY2020 Build organisational capability and accountability to sustain change, commence work with longer term change timelines.
CY2021 Finalise changes; embed performance culture.
The sequencing of different initiatives is based on the level of impact, the ease of delivery, and sequencing change to build
capability and embed change. The sequencing also respects the multiple interdependencies within the program, as well as the
imperative to stabilise the organisation as quickly as possible.
The overarching program is supported by the following:
• A program governance structure to ensure that initiatives are delivered with reference to a control environment and with
an overarching steering committee to make decisions on program direction and benefits.
• An integrated stakeholder change and communications strategy to manage the impacts to stakeholders, and ensure clear
communication and engagement throughout the project.
• An overarching IR engagement strategy to engage with workforce industrial representatives and manage the delivery of
changes impacting the workforce.
The accompanying table overleaf summarises the key activities in each Operating Lever that are planned to be undertaken
across the delivery phases.
The Recovery Plan initiatives, priorities, risks and timeframes documented in this report reflect our initial planning response.
Whilst we are confident that this reflects a comprehensive and achievable roadmap for CALHN’s organisational and financial
recovery, we fully expect the Recovery Plan to be dynamic and to continue to evolve during the course of implementation.
Whilst target outcomes and guiding principles will remain constant, we will closely monitor progress on individual workstreams
and change initiatives, re-prioritising the forward work program as necessary to maintain operational flexibility and momentum.

Page 37
5.2 Key initiatives for each operating lever over a three-year recovery period
Service Delivery & Efficiency People, Culture &
Governance
Information, Evidence &
Insights
Finance, Cost & Revenue
Management
1. Process and practice
improvement, including:
• Improve patient flow
• Improve patient
discharge practices
• Ensure integrated
operational planning
• Minimise unnecessary
hospital admissions
2. Improve staff
engagement and
capacity building
3. Achieve efficiencies
and cost savings in
infrastructure and
resource utilisation
4. Improve facility and IT
assets and their
impact on resource
effectiveness
5. Improve Departmental
efficiencies
1. Redesign the CALHN
organisational structure
and accountabilities
2. Strengthen the HR
function across CALHN
to develop and support
a strong workforce
3. Ensure relevant
leadership and
capability development
occurs
4. Establish project
governance structures
and protocols
5. Develop and implement
a fit for purpose Risk
Management
framework
1. Define and establish
an effective Data and
Reporting Function
2. Develop a streamlined
data and reporting
framework
3. Develop revised
monthly management
reporting pack
4. Establishment of future
state reporting
structures, analytics
and education
programs
5. Optimise clinical coding
strategy and education
6. Establish best practice
clinical coding and
revenue management
team
1. Develop an activity-
based budget
2. Improve accounting for
and management of
block funding
3. Optimise public and
private patient revenue
4. Improve contract
management controls
5. Improve cost
management controls
6. Optimise management
of non-clinical services
7. Review SCSS service
costs to CALHN
8. Optimisation of Shared
Services (payroll,
accounts payable etc)
Program Governance
Stakeholder Change and Communications
IR Engagement

Page 38
5.3 Recovery initiatives during Stabilise Phase
The following tables illustrate the initiatives that are planned to be undertaken in each of the delivery phases – Stabilise,
CY2019, CY2020 and CY2021. This is intended to represent a roadmap and as such, the timing of some initiatives may be
brought forward or delayed to facilitate a cohesive program delivery. The planned approach and sequencing of key activities
under each operating lever will continue to be developed in more detail as implementation tools in advance of ‘Day Zero’.
We have also depicted the proposed recovery initiatives in the form of Gantt charts in Appendix 1.
Recovery initiatives during Stabilise Phase (to end of 2018*)
Operating Lever Key initiatives and focus activities
Service Delivery &
Efficiency
Explore efficiencies and cost
savings in resource utilisation.
Mental Health care and efficiency
improvement:
• Support resolution of issues
with duress alarms
Staff engagement and capacity
building to enable realisation of
patient care outcomes:
• Implement scenario taskforce
across clinical, nursing and
support staff
• Commence development of
workshops on operational
planning and forecasting for
accountable staff
• Implement an accountability
cycle for key stakeholders
Commence improvement of
patient flow throughout the
hospital:
• Agree priorities to action,
based on top causes of
process delays and top causes
of variations
Patient care efficiencies in ED:
• Identify improvements to
inefficient ED practices
Improve patient discharge
practices:
• Obtain benchmark data and
target discharge standards
• Improve linkages to existing
community facilities
Integrated operational planning to
reset business units:
• Commence implementation of
roster-based dashboards to
improve NUM planning
accountability
• Implement nursing structure
around the Christmas wind
down
• Plan efficient staff coverage of
wards
Identify and improve resource
efficiencies through bed
realignment:
• Support implementation of
Christmas period ramp down
People, Culture &
Governance
Redesign the CALHN
organisational structure and
accountabilities:
• Develop and implement a new
organisational structure
Develop an HR strategy and
workforce plans that support
CALHN's vision and purpose
• Establish workforce planning
practices across CALHN
• Manage to existing EAs
Establish project governance
structures and protocols:
• Assess current projects and
related business case
information
Information, Evidence &
Insights
CALHN data custodianship and
strategy:
• Identification of sources of
existing key data within CALHN
• Streamlined data and
reporting framework
• Identify and assess present
key data reports (both clinical
and financial)
Focused and insightful interim
reporting:
• Develop interim management
reporting pack for CALHN use
• Define, validate and
communicate interim key
metrics
Clinical coding strategy and
education:
• Develop a Clinical Coding
Strategy
• Repurpose the Clinical Coding
Committee
• Clinical Coding Audits and
follow-up
• Co-ordinate activity to clear
coding backlog
Finance, Cost & Revenue
Management
Budgeting and cost allocation:
• Commence development of
FY19 activity-based budget
aligned with commissioned
activity levels based on FY17 &
FY18 coding data
• Segregate costs and revenue
for block funded activities and
commence monthly reporting
to management
Stop leakage relating to private
patient revenue:
• Increase collection of private
patient and other sundry
revenue
Reduce expenditure on staff costs
to directly align with funded
activity.
• Immediate controls on
recruitment, rostering and
payroll management
Cost management
• Improve control over local
overspending
• Non-clinical costs - Expedite
existing modification requests
under the PPP contract
• Shared Services – start
seeking clarity on
responsibilities internally and
with Shared Services South
Australia (‘SSSA’)
* Stabilise Phase (60 days) may extend into early 2019 depending on the timing of the commencement of the Implementation Phase. The timing of individual initiatives may
be brought forward or pushed back to facilitate a cohesive program delivery.

Page 39
5.4 Recovery initiatives during CY2019
Operating Lever Key initiatives and focus activities
Service Delivery & Efficiency Streamline patient flow
throughout the hospital:
• Implement measures to
improve patient flow
• Redesign patient flow and
simulate new patient design
Improve patient discharge
practices
• Test and expand procedural
changes to improve
discharge planning and
execution
Improve resource efficiencies
through bed realignment:
• Design bed plan procedures
that provide flexibility in peak
periods
Efficiencies and cost savings
in infrastructure and resource
utilisation:
• Implement equipment
efficiencies
• Improve and streamline
Central Sterile Supplies
Department (‘CSSD’)
requests and requirements
Improve facility and IT assets
and their impact on resource
effectiveness:
• Determine current state of
IT assets and map to
digital hospital plan
• Agree a strategy to move
forward with an Electronic
Records system
Continuation of improvements to
ED practices
Mental Health care and efficiency
improvement:
• Staff recruitment/retention
strategy
• Procedural efficiency
improvements
Detailed review of outpatient
services and implementation of
changes
Integrated operational planning
• Quantify the variation in daily
patient arrivals and identify
staff that can be flexed
People, Culture & Governance Redesign the CALHN
organisational structure and
accountabilities:
• Establish an operating
tempo for meetings,
committees and forums
Establish project governance
structures and protocols
• Provide training and support
to project staff
Implement a fit for purpose Risk
Management framework
Strengthen the HR function
across CALHN to develop and
support a strong workforce:
• Establish workforce
planning practices across
CALHN
• Develop an HR strategy
that supports CALHN's
vision and purpose
• Develop recruitment and
retention strategies
• Build HR capability
Leadership and Capability
development:
• Implement talent management
and succession planning
• Grow the leadership capability
of managers
• Improve the financial/business
acumen of leaders
Information, Evidence &
Insights
CALHN data custodianship and
strategy:
• Develop and communicate a
strategy for the Data
Management and Delivery
Function
• Define the Data Function
structure, skills and
capabilities
Streamlined data and reporting
framework:
• Restructure CALHN reporting
preparation and delivery
Optimised reporting and
analytics capabilities:
• Future state management
reporting structure
• Education campaign for
decision-makers
Clinical coding strategy and
education
• Education and training to
upskill clinicians and nurses
• Clinical Coding Audits and
follow-up
Finance, Cost & Revenue
Management
Develop an activity-based
budget for FY20:
• Improve private patient
revenue
• Review the Rights of Private
Practice (‘ROPP’)
administration fee
Reduce unfunded expenditure
on staff costs:
• Streamline payroll processes
and controls
• Provide useful information to
inform planning
Contract management
controls:
• Internal controls over staff
recruitment
• Rationalise selection of
goods available under
contract management
• Increase goods under
central contract
management
SCSS cost to CALHN:
• Consider future service needs
in respect of Imaging,
Pharmacy and Pathology
• Review overhead costs
• Consider findings relevant to
CALHN from the independent
efficiency review of SCSS
Shared Services optimisation:
• Review shared services
contract terms for all sites
• Benchmark back office costs.
Review contract with SSSA
• Address utilities/overhead
costs where possible
Note: The timing of individual initiatives may be brought forward or pushed back to facilitate a cohesive program delivery.

Page 40
5.5 Recovery initiatives during CY2020 and CY2021
Operating Lever Key initiatives and focus activities
Service Delivery & Efficiency Minimise unnecessary hospital
admissions
• Work with SA Health to
implement Hospital
Avoidance Strategy
Streamline patient flow
throughout the hospital:
• Effective procedures to
ensure continuity of care and
decision-making across a 7-
day week
Improve patient discharge
practices:
• Increase home and
community services
available to support step-
down discharge
Support implementation of
Models of Care that reflect best
practice
People, Culture & Governance Redesign the CALHN
organisational structure and
accountabilities:
• Manage to performance of
KPIs
Information, Evidence &
Insights
Optimised reporting and
analytics capabilities:
• Refine Future state
management reporting
structure
• Develop strong analytic
function and capability to
drive insights and modelling
Clinical coding strategy and
education:
• Education and training to
upskill clinicians and nurses
• Clinical Coding Audits and
follow-up
Finance, Cost & Revenue
Management
Private Patient revenue:
• Review the
administration/resource fee
for ROPP
Contract management controls:
• Increase goods under central
contract management
Note: The timing of individual initiatives may be brought forward or pushed back to facilitate a cohesive program delivery.

Page 41
Appendices

Page 42
Appendix 1 – Recovery Plan - Indicative Timelines by Operating Lever
Operating Lever 1 | Service Delivery & Efficiency | Recovery timeline
Planning
(Oct 2018)
Stabilise
(Day 0 -31 Dec 18) CY 2019 CY 2020 CY 2021
M1 M2 Q1 Q2 Q3 Q4 H1 H2 H1 H2
Nov-18 Dec-18 Mar-19 Jun-19 Sep-19 Dec-19 Jun-20 Dec-20 Jun-21 Dec-21
1. Service Delivery & Efficiency
1.1 Minimise unnecessary
admissions
Implement initiatives that reduce the demand for hospital services where more appropriate
care can be provided elsewhere
1.2 Resource Efficiencies Review of the key assets to prioritise key business opportunity and savings
1.3 Identify and improve facility and
IT assets
Determine current state of IT assets and gap to digital hospital expectations.
Agree a strategy to move forward with an Electronic Records system post independent EPAS
review.
1.4 Streamline patient flow
throughout the hospital
Map and Identify the key patient delays through the systems
Agree priorities to action, based on top causes of process delays and unnecessary variations
Implement interim measures to improve patient flow
Redesign patient flow and simulate new patient design
Effective procedures to ensure care and decision-making across a 7-day week
1.5 Improve patient discharge
practices
Obtain benchmark data and target discharge standards for each facility/procedure.
Test and expand procedural changes to improve discharge planning and execution
Improve linkages to existing home and community facilities to facilitate discharge;
Increase home and community services available to support step-down discharge
1.6 Identify and improve resource
efficiencies through bed
realignment
Review bed profile of RAH to determine capacity constraints/overflow issues in peak periods
Review and redesign Christmas period ramp down
Design bed plan procedures that provide flexibility around known peak periods
1.7 Improve Departmental
efficiencies
Identify improvements to inefficient practices
Implement improvements to inefficient practices
1.8 Staff engagement Upskill accountable and responsible managers operational planning and forecasting
1.9 Integrated operational planning Implement roster dashboards to improve nurse unit manager planning accountability
Review appropriate nursing structure around the Christmas period wind down
Quantify demand variations and identify staff flex sources
Replan efficient staff coverage of wards
(Note: Timeline is indicative and subject to revision. Some individual initiatives have been rolled-up / grouped for presentation purposes in the body of this report)

Page 43
Operating Lever 2 | People, Culture & Governance | Recovery timeline
Planning Stabilise CY 2019 CY 2020 CY 2021
(Oct 2018) (Day Zero– 31 Dec 18)
M1 M2 Q1 Q2 Q3 Q4 H1 H2 H1 H2
Nov-18 Dec-18 Mar-19 Jun-19 Sep-19 Dec-19 Jun-20 Dec-20 Jun-21 Dec-21
2. People, Culture & Governance
2.1 Improve staff engagement Develop and communicate a clear vision for CALHN
2.2 Redesign the CALHN
organisational structure and
accountabilities
Develop and implement a new organisational structure
Establish an operating tempo for meetings, committee’s and forums
Manage to performance of KPIs
2.3 Strengthen the HR function
across CALHN to develop
and support a strong
workforce
Develop an HR strategy that supports CALHN's vision and purpose.
Establish workforce planning practices across CALHN
Develop recruitment and retention strategies
Build the capability of the HR team.
2.4 Leadership and Capability
development
Implement talent management and succession planning
Grow the leadership capability of managers
Improve the financial/business acumen of leaders
2.5 Establish project governance
structures and protocols
Assess current projects and related business case information (cost, benefits, impacts, etc)
Establish future state Project office and protocols
Provide training and support to project personnel
2.6 Implement a fit for purpose
Risk Management framework
Establish a framework that meets the needs of the organisation
Provide training and support to implement the structure
(Note: Timeline is indicative and subject to revision. Some individual initiatives have been rolled-up / grouped for presentation purposes in the body of this report)

Page 44
Operating Lever 3 | Information, Evidence & Insights | Recovery timeline
Planning Stabilise CY 2019 CY 2020 CY 2021
(Oct 2018)
(Day Zero–
31 Dec 18)
M1 M2 Q1 Q2 Q3 Q4 H1 H2 H1 H2
Nov-18 Dec-18 Mar-19 Jun-19 Sep-19 Dec-19 Jun-20 Dec-20 Jun-21 Dec-21
3. Information, Evidence and Insights
3.1 CALHN data custodianship and
strategy
Strategy for Data Management and Delivery Function
Identification of sources of existing key data within CALHN
Define the Data Function structure, skills and capabilities
Communicate new Data Management and Delivery function
3.2 Streamlined data and reporting
framework and improved data flow
from SA Health
Identify and assess present key data reports (both clinical and financial)
Restructure CALHN reporting preparation and delivery
Improve current reporting arrangements
Build collaborative relationship with SA Health
3.3 Focused and insightful interim
reporting
Define, validate and communicate interim key metrics
Develop interim management reporting pack for CALHN use
Facilitate information requests by Recovery team.
3.4 Optimised reporting and analytics
capabilities
Future state management reporting structure
Develop strong analytic function and capability to drive insights and modelling
Education campaign for decision-makers
3.5 Clinical coding strategy and
education
Develop a Clinical Coding Strategy
Repurpose the Clinical Coding Committee
Education and training to upskill clinicians and nurses
Clinical Coding Audits and follow-up
3.6 Clinical coding backlog management Co-ordinate activity to clear coding backlog by December 2018.
(Note: Timeline is indicative and subject to revision. Some individual initiatives have been rolled-up / grouped for presentation purposes in the body of this report)

Page 45
Operating Lever 4 | Finance, Cost & Revenue Management | Recovery timeline
Planning Stabilise CY 2019 CY 2020 CY 2021
(Oct 2018)
(Day Zero–31 Dec
18)
M1 M2 Q1 Q2 Q3 Q4 H1 H2 H1 H2
Nov-18 Dec-18 Mar-19 Jun-19 Sep-19 Dec-19 Jun-20 Dec-20 Jun-21 Dec-21
4. Finance, Cost and Revenue Management
4.1 Rebuild and re-tool financial reporting
infrastructure and responsibilities
Move to activity-based budget FY19
Develop activity-based budget for FY20
4.2 Control and accounting for block funded
activities
Block funded activities accounting and reporting
4.3 Private patient and sundry revenue Improve private patient and sundry revenue collection
Review the administration/resource fee for ROPP
4.4 Recruitment rostering & payroll controls Internal controls over staff recruitment
Internal controls over nursing staff rostering and payroll
Internal controls over staff payroll processes and systems
4.5 Rationalise selection of goods Rationalise selection of goods available under contract management
4.6 Increase goods under contract Increase volume of goods under central contract management
4.7 Non-clinical contract management Bring non-clinical services under PSCM contract management
4.8 Cost management controls Control local overspending on consumables and support services
4.9 Improve management of PPP contract Work with SA Health to manage service provision under the PPP contract
4.10 Management of non-clinical services Minimise modifications under the PPP contract
4.11 SCSS cost to CALHN Consider outcome of SCSS efficiency review, consider opportunities to reduce
service cost to CALHN
Consider unrecovered overhead costs that relate to SCSS
4.12 Optimisation of Shared Services Review terms of shared services contract with the inclusion of all CALHN sites.
Clarify responsibilities both internally and with shared services
Benchmark back office costs. Review contract with SSSA.
4.13 Overhead costs Review Utilities/ overhead costs
(Note: Timeline is indicative and subject to revision. Some individual initiatives have been rolled-up / grouped for presentation purposes in the body of this report)

Page 46
Appendix 2 – Recovery Plan – Risk Management Framework
Implementation Risk Management Approach
Risk Identification
New risks will be identified and captured through project delivery or through discussion at Program Team meetings, Steering
Committee meetings and stakeholder working group meetings. To facilitate the identification of risks, a Risk Management item
will be on the agenda of each Stream Leads meeting and each Program Team meeting.
Each new risk will be assessed and have a treatment plan developed, in consultation with the Program Manager and the
CALHN Risk Manager, and a risk owner assigned.
Risk Assessment
Risks will be assessed via the following framework:
Risk Rating
For each of the identified risks, a risk rating based on likelihood and consequence should be applied. This rating results in risks
being prioritised and limited risk management resources allocated appropriately.
Likelihood
Assess the likelihood of the risk occurring if no treatment was undertaken:
Almost Certain »Risk is expected to occur during the life of the project or phase (95+% certainty)
Likely »Risk will probably occur in most circumstances during the life of the project or phase (>50% probability)
Possible »Risk might not but likely to occur at some time during the life of the project or phase (>20% probability)
Unlikely »Risk not generally expected but could occur during the life of the project or phase (>5% probability)
Rare »Risk may occur only in exceptional circumstances during the life of the project or phase (<5% probability)
Consequence
For all risks, the consequence to the project of the risk occurring (if no treatment was undertaken) is assessed against the risk
framework described following.
Rating
For each of the identified risks, a risk rating based on likelihood and consequence will be applied. This rating results in risks
being prioritised and limited risk management resources allocated appropriately.
More detailed risk rating information follows overleaf, however the broad calculation is:
Likelihood
Rare
Unlikely
Possible
Likely
Definitely
=
Consequence
Insignificant
Minor
Moderate
Major
Catastrophic
Rating
Low
Moderate
High
Extreme

Page 47
Risk Response
Based on the risk rating, a risk response will be developed for each risk as follows:
Treat Implement additional processes and controls to reduce the risk.
Tolerate Accept the risk and take no further action to reduce it (e.g. within risk appetite, ability to reduce the risk is
limited, or cost to reduce is disproportionate to the potential benefit gained).
Transfer Outsource or insure against the risk. It is noted that reputation risk cannot be transferred.
Terminate Eliminate the risk altogether by avoiding the course of action or stopping an activity.
Once a response has been agreed and documented, the risk will be assessed based on the likelihood and consequence of the
risk occurring once the treatment is applied. This will determine the appropriateness of the treatment.
Risk Management
Risks will be monitored by the Program Manager and the Stream Leads who will advise the Program stakeholders and Steering
Committee (via status reports) of any new risks that have been identified as a ‘High’ or ‘Severe’ rating, and any risks that have
increased their rating. As a minimum, risks will be reviewed monthly and at the end of each project stage.
Risk consequence assessment framework
For all risks, the consequence to the organisation of the risk occurring (if no treatment was undertaken) is assessed against
the following framework:
Insignificant Minor Medium/Moderate Major Critical/ Severe
Clinical Negligible clinical event
resolved without impact
on Consumer or
organisation
Clinical event resolved
with minimal short-term
impact on Consumer or
organisation
Clinical event resulting in
temporary injury or
impact with considerable
effect on Consumer or
organisation. Internal
investigation required.
May require external
mediation
Clinical event resulting in
serious permanent injury,
requiring internal and
medico legal
investigation, external
mediation, major
penalties or
compensation payments
Failure in clinical
governance processes/
systems resulting in
fatality requiring
extensive internal and
medico legal
investigation, coroner’s
notification, significant
penalties or
compensation payments
Financial Financial loss of either
less than $250,000 or
0.05% of budget
Financial loss of either
between $250,000 to $1
million or between 0.05%
to 0.2% of budget
Financial loss of either
between $1 to $5 million
or between 0.2% to 1% of
budget
Financial loss of either
between $5 to $10
million or between 1% to
2% of budget
Financial loss of either
greater than $10 million
or 2% of budget
Our People Negligible staff injury or
near miss accident.
Insignificant industrial
grievance
Staff lost time injury.
Local temporary poor
engagement. Industrial
grievance resolved
internally
Temporary injury to staff.
Ongoing widespread
engagement issues.
Industrial disputation
mediated with no major
penalty
Serious permanent injury
to staff. Entrenched
engagement problems.
Inability to recruit staff
with necessary skills in
key areas. Staff walkout
and Industrial stoppages
Staff fatality.
Simultaneous loss of
several critical staff (e.g.
Executive)
Legal, Policy &
regulatory
Immaterial legal,
regulatory or internal
policy failure without
penalty implication
One-off minor legal,
regulatory or internal
policy failure resolved
without penalty
Repeated legal,
regulatory or internal
policy failure with penalty
implications requiring
internal investigation
Systemic legal, regulatory
or internal policy failure
with major penalty
requiring extensive
internal inquiry and
external review
Substantial failure in
internal governance and
control structures
resulting in Royal
Commission and
significant penalty
Organisation/
Consumer
Event with negligible
impact on delivery of
services to Consumers.
Internal inconvenience
only
Event with short term
impact on delivery of
services. Some impact on
Consumers or Partners
Event requiring
considerable remedial
action with moderate
impact on Consumers or
Partners. Temporary loss
of important information
Event with major impact
on delivery of services.
Major impact on
Consumers or Partners.
Temporary loss of critical
information
Event with significant
impact on delivery of
services across SA Health
for an extended period.
Significant impact on
Consumers or Partners.
Permanent loss of critical
information

Page 48
Insignificant Minor Medium/Moderate Major Critical/ Severe
Corporate
reputation and
image
One off negative media
coverage only and no
reputation impact
Isolated adverse media
exposure. Temporary
minor negative impact on
reputation
Repeated isolated
negative reporting in
media. Temporary
breakdown in key
relationship. Short term
reputation damage
Widespread negative
reporting in media
leading to high-level
independent
investigation with
adverse findings and
longer-term reputation
damage. Premier or
Ministerial involvement
/intervention by Cabinet.
Breakdown in key
relationship(s)
Sustained adverse media
exposure. Total loss of
confidence within
community and with the
Government.
Parliamentary enquiry.
Serious long-term impact
on reputation
Program Delivery Minor variation to quality
of deliverable; does not
impact target benefits
Deliverable does not
meet quality
expectations; does not
impact target benefits
Minor impact to business
case & target benefit
One or more benefits will
not be achieved
Severe impact to
business case & target
benefit
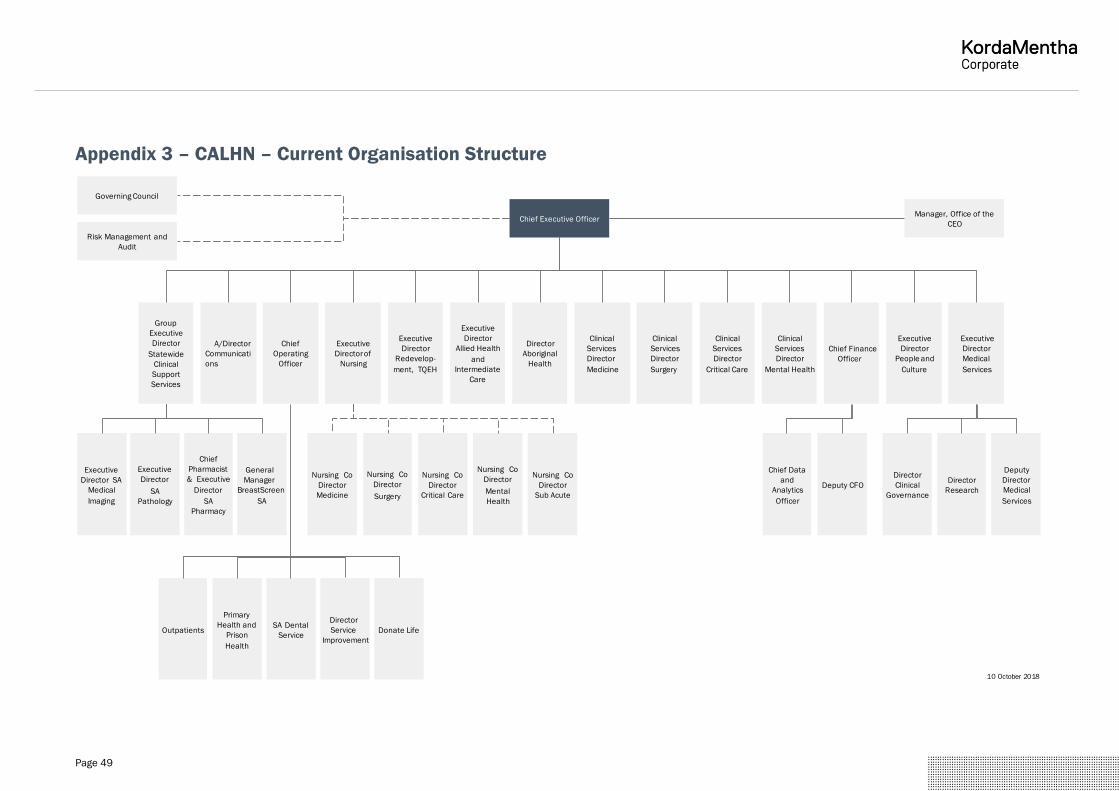
Page 49
Appendix 3 – CALHN – Current Organisation Structure
Chief Executive Officer
Governing Council
Executive
Director
Medical
Services
Executive
Director
Allied Health
and
Intermediate
Care
Chief Finance
Officer
Chief
Operating
Officer
Executive
Directorof
Nursing
Executive
Director
People and
Culture
Executive
Director SA
Medical
Imaging
Chief
Pharmacist
& Executive
Director
SA
Pharmacy
Executive
Director
SA
Pathology
Group
Executive
Director
Statewide
Clinical
Support
Services
A/Director
Communicati
ons
Manager, Office of the
CEO
Executive
Director
Redevelop-
ment, TQEH
Outpatients Donate Life
Primary
Health and
Prison
Health
Director
Clinical
Governance
Director
Research
Director
Service
Improvement
Deputy
Director
Medical
Services
Risk Management and
Audit
10 October 2018
SA Dental
Service
Deputy CFO
Nursing Co
Director
Medicine
General
Manager
BreastScreen
SA
Nursing Co
Director
Surgery
Nursing Co
Director
Critical Care
Nursing Co
Director
Mental
Health
Nursing Co
Director
Sub Acute
Chief Data
and
Analytics
Officer
Clinical
Services
Director
Medicine
Clinical
Services
Director
Surgery
Director
Aboriginal
Health
Clinical
Services
Director
Critical Care
Clinical
Services
Director
Mental Health

Page 50
Appendix 4 – CALHN Administrator: Specific Actions & Performance
Management Meetings
We outline below a number of the specific initiatives the Administrator should introduce in respect of the four key drivers of
financial improvement.
We also outline the performance management meeting approach and framework we will implement.
1 Specific initiatives to achieve target financial outcomes
The Recovery Plan will drive financial performance improvement across four key areas:
1. Control &
Accountability
2. Activity Levels &
Efficiency
3. Workforce
Management 4. Length of Stay
Key areas Specific actions
1. Control &
Accountability
Background: The introduction of a range of controls and improved accountability will deliver a significant
improvement in financial performance. The improved framework will deliver no less than $35 million
over the 3-year period, recurring at a minimum of $35 million per annum thereafter.
Specific actions:
1. Establish effective controls on procurement, including:
‒ No supplier payments without Purchase Orders, advise all suppliers
‒ Rationalise the number of category items available within Oracle
‒ Specific approvals required for uncatalogued items
‒ Specific approvals required for all items >$110,000
‒ Realign all financial controls and accountability in line with amended policies and procedures
‒ Implement a dual approval process external to specific directorates
‒ Align the PSCM team to facilitate more direct roles, responsibility and accountability of CALHN
‒ Identify what purchases would be best managed through a central procurement contract
2. Immediately commence initiatives to establish activity-based budgeting across CALHN, including:
‒ Recut FY19 Budget based on historic, and commissioned activity levels through to directorate
level via periodic monthly reporting
‒ Recut chart of accounts with appropriate site and directorate cost allocations
‒ Engage staff at directorate level in development of the recut FY19 budget
‒ Redefine responsibilities for expenditure and cost control within CALHN and align delegations
and system access accordingly
‒ Roll-out relevant financial benchmarks to be included in regular reporting
‒ Commence process for developing activity-based budget in January 2019 to ensure sources of
information are available
‒ Full move to Activity Based Budgeting for development of FY20 budget
3. Immediately restructure the delivery, accountability and validation of reporting throughout CALHN,
including:
‒ Develop improved monthly management reporting pack to provide high level visibility of clinical,
people and financial performance across CALHN
‒ Eliminate ineffective reporting and ensure reported key metrics are concise, measurable, action-
driving, and include lead and lag indicators, and cover clinical, people and financial performance
4. Expedite current activity and programs to increase private inpatient revenue by $16 million per
annum
5. Identify projects and committees to stop/pause/redirect resources

Page 51
Key areas Specific actions
2. Activity levels &
efficiency
Background: CALHN Management estimate that activity levels for inpatients were 18,000 NWAU above
commissioning cap in FY18. More effective management of activity in excess of currently commissioned
levels where possible would generate potential cost efficiencies of approximately $71 million over the 3-
year period, recurring at $71 million pa thereafter.
Specific actions:
1. Finalise and implement an effective clinical coding optimisation program
2. Reduce time for bed turnover through improved management of Spotless to deliver savings
3. Review and redesign Christmas period ramp down to meet needs
4. Implement changes to outpatient services that will improve efficiency, improve patient experience,
and reduce operational costs
3. Workforce
management
Background: More effective management and utilisation of CALHN’s existing workforce has the potential
to generate significant financial benefits.
Nurse agency use at CALHN is significantly higher than peers, with an approximate cost premium of 40%
and agency costs forecast to be greater than $50 million in FY19. Agency costs can potentially be
halved by improved rostering and more effective use of the existing workforce.
In addition, CALHN Management estimate that there are efficiency gains of approximately $10 million in
more effective medical rostering and reduced locum use.
Reducing nursing hours per patient day from prevailing levels to target levels would generate savings of
approximately $11 million on an annualised basis.
Specific actions:
1. Immediately take steps to improve workforce rostering and minimise the use of expensive nurse
agency and locum staffing, including:
‒ Empower nursing staff to take immediate control of the rostering process to ensure appropriate
allocation of resources
‒ Identify weaknesses in processes for rostering, approving rosters and updating for actual hours
worked, implementing internal controls to rectify
‒ Implement checks and reporting lines to ensure any discrepancies are identified and dealt with
in a timely manner.
‒ Implement processes to increase the reliability of information in CHRIS21 and ProAct to provide
accurate and timely information to decision makers.
‒ Improve roster forecasting to meeting financial budgets and implement roster-based
dashboards to improve nurse unit manager accountability with forward planning.
2. Immediately take effective control over hiring and recruitment practices to start managing back to
appropriate levels, including:
‒ Establish Appointments Committee
‒ Stop practice of ‘approval shopping’
‒ Require specific approval for backfill roles
‒ Require specific sign-offs for unplanned overtime (consistent with approach to planned
overtime)
3. Take immediate steps to improve the financial/business acumen of leaders
4. Immediately cease unnecessary committees and projects
5. Replan and implement efficient staff coverage of wards
6. Expedite rollout of currently stalled workforce analytics and optimisation software tools
7. Reducing CALHN’s comparatively high nursing sick leave by improving the internal culture and
environment to peer levels would generate estimated cost savings of approximately $10 million
8. Restructure organisation design to ensure more effective and accountable management at a site-
specific level

Page 52
Key areas Specific actions
4. Length of Stay Background: Reducing the Relative Stay Index (‘RSI’) for RAH and TQEH to the median peer of RSI of
88% would generate potential cost efficiencies of approximately $130 million over the 3-year period
recurring at $130 million per annum thereafter. This equates to an estimated reduction in the average
length of stay of 1.5 days, which would free-up approximately 65,000 Occupied Bed Days (‘OBD’) per
annum to improve bed management optionality (for intended use, alternative use, reserved for peak flex
etc, all subject to ongoing demand requirements).
Specific actions:
1. Establish NHS style Red/Green reporting across all relevant CALHN facilities to identify daily patient
flow road-blocks in respect of individual patients and act to resolve
2. Enforce current discharge planning and implementation activities over 7 days
3. Implement a range of clinical interventions in ED to diagnose, treat and discharge patients earlier
(ie: increased use of geriatricians, allied health)
4. Roll-out new, effective, procedures and policies to ensure continuity of care and decision making
across a 7-day week
5. Hold nurses and doctors to account for managing patient discharge dates to the estimated date for
discharge adopted at admittance
2 Performance Management Meeting
The Administrators will establish a rigorous performance review programme, which will include:
2.1 Setting expectations of leadership in managing performance
Clarify with Individual leaders what is required from them in relation to performance management. We anticipate that this will
include resetting expectations to include an emphasis on leaders demonstrating that they:
• Provide strong, visible leadership, modelling the highest standards of service delivery and patient care across the
Directorate
• Actively manage their Directorates to continually review services and objectives and achieve optimal fit between clinical
service delivery and sound financial management
• Challenge conventional approaches and drive forward change when needed, demonstrating a commitment to creating a
culture of continuous improvement and quality
• Take accountability for the performance of directly managed staff
• Effectively manage budgets and are accountable for the effective use of resources
2.2 Establishing and running performance reporting, review meetings and performance remediation
Establish reporting tools, a schedule of meetings and the required governance to consistently review operational and financial
performance by Directorate. It is envisaged that Directorate and Unit leadership will be required to:
• Complete regular reporting across several performance domains including operational, financial, workforce, risk and
complaints
• Attend routine performance review meetings chaired by the Administrator (e.g. fortnightly), with more frequent attendance
(e.g. weekly or daily) required for areas of poor operational and financial performance
• Where insufficient assurance of performance is provided, develop and implement a 30-day improvement plan with clear
milestones and actions. If this is not achieved, a number of interventions may be invoked including removal of
authorisation rights, reviews with the Chief Executive and more frequent performance reviews

Page 53
2.3 Strategic change management support to foster improvement across the organisation
During performance turnaround initiatives, significant change is often faced by leadership and their Directorates. We have
positioned experienced strategic change management capability to complement and support performance improvement
across CALHN. It is anticipated that the change management focus would be to:
• Establishing a relationship with key stakeholders, individually and collectively, as a Change Network or Design Reference
Group
• For improvement initiatives requiring design work, use a mixture of interviews and collaborative methods (e.g. workshops)
to get stakeholders to provide input, feedback, and validation of proposed changes to enhance buy-in
• Build early engagement and buy-in to the vision of the turnaround across the organisation, as well as the case for any
changes
• Develop communications and other engagement materials in collaboration with those stakeholders, to resonate with the
intended audience
• Recognise that the health setting is one where ultimately the determining factor is the patient outcome and restate or
translate commercial or operational issues into patient outcome terms across communications and learning materials

Page 54
Appendix 5 – Glossary
CALHN Central Adelaide Local Health Network
CEO Chief Executive Officer
CFO Chief Financial Officer
COO Chief Operating Officer
CSSD Central Sterile Supplies Department
ED Emergency Department
EPAS Enterprise Patient Administration System
FMC Flinders Medical Centre
FTE Full Time Equivalent
HRT Health Roundtable
KPI Key Performance Indicator
LHN Local Health Network
LOS Length of Stay
NEP National Efficient Price
NHPPD Nursing Hours per Patient Day
NWAU National Weighted Activity Unit
OBD Occupied Bed Day
OPD Outpatients Directorate
PPP Public Private Partnership
ProAct Nurse rostering system
RAH Royal Adelaide Hospital
ROPP Rights of Private Practice
RSI Relative Stay Index
SA South Australia
SCSS Statewide Clinical Support Services
SSSA Shared Services South Australia (Payroll, AP/AR, etc)
TQEH The Queen Elizabeth Hospital



















