CE Directed Reading - American Society of Radiologic ... · Johann Georg Wirsung reported the...
24
645CT CE Directed Reading This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference. RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6 After completing this article, the reader should be able to: Understand anatomy of the pancreas as well as its exocrine and endocrine functions. Compare and contrast the genetic and nongenetic risk factors for pancreatic cancers and acute and chronic pancreatitis. List symptoms of duct obstructions, pancreatitis, and pancreatic cancer. Describe computed tomography signs of duct obstructions, pancreatitis, and pancreatic cancer. Explain staging and prognostic scoring systems for pancreatitis and pancreatic cancer. Discuss the roles of contrast-enhanced multidetector computed tomography and other imaging modalities in the diagnosis, staging, and management of pancreatitis and pancreatic cancer. Computed Tomography of Pancreatitis and Pancreatic Cancer Bryant Furlow, BA Pancreatic disease often is asymptomatic until tissue damage and complications occur or until malignancies have reached advanced stages and have metastasized. Contrast-enhanced multidetector computed tomography plays a central role in diagnosing, staging, and treatment planning for pancreatitis and pancreatic cancer. This article introduces the functional anatomy of the pancreas and common bile duct and the epidemiology, pathobiology, and computed tomography imaging of pancreatitis, calculi, and pancreatic cancer. P ancreatitis and pancreatic can- cer are complex diseases associ- ated with profound effects on patient quality of life and poor prognosis, particularly if not detected and treated promptly. Contrast- enhanced computed tomography (CECT), usually undertaken with mul- tidetector equipment, has become the standard pancreatic imaging modality for diagnosing, staging, and planning treatment for these diseases. Carefully timed CECT scan acquisitions can maximize the utility of intravenous contrast agents to identify specific signs of pancreatitis, duct-obstructing calculi (stones), and tumors, as well as poten- tially life-threatening complications. Anatomy and Physiology The pancreas is the largest gland in the digestive system. It plays life- sustaining roles in the regulation of food digestion and blood glucose levels. It was first tentatively identified by the ancient Greeks, but its functions and even its existence as a discrete organ did not become clear until the 1500s, partly because of its visual similarity to mesenteric fat. 1,2 German anatomist Johann Georg Wirsung reported the anatomy of the main pancreatic duct in 1642, based on his dissection of an executed convict. 2 In the 1850s, French physiologist Claude Bernard reported on the organ’s exocrine roles in excret- ing digestive enzymes. 2 Essentially a glandular network of ducts, this heavily vascularized organ is situated in the upper abdomen against the left diaphragm, behind the stomach, and adjacent to the small intestine and the gallbladder, which stores liver bile. 3,4 The pancreas is both an endocrine and exocrine organ excreting hormones into the bloodstream and digestive enzymes
-
Upload
truongkhue -
Category
Documents
-
view
213 -
download
0
Transcript of CE Directed Reading - American Society of Radiologic ... · Johann Georg Wirsung reported the...
645CT
CEDirected Reading
This article is a Directed Reading. Your access to Directed Reading quizzes for continuing education credit is determined by your membership status and CE preference.
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
After completing this article, the reader should be able to:Understand anatomy of the pancreas as well as its exocrine and endocrine functions.Compare and contrast the genetic and nongenetic risk factors for pancreatic cancers
and acute and chronic pancreatitis.List symptoms of duct obstructions, pancreatitis, and pancreatic cancer.Describe computed tomography signs of duct obstructions, pancreatitis, and pancreatic
cancer.Explain staging and prognostic scoring systems for pancreatitis and pancreatic cancer.Discuss the roles of contrast-enhanced multidetector computed tomography and other
imaging modalities in the diagnosis, staging, and management of pancreatitis and pancreatic cancer.
Computed Tomography of Pancreatitis and Pancreatic Cancer
Bryant Furlow, BA
Pancreatic disease often is asymptomatic until tissue damage and complications occur or until malignancies have reached advanced stages and have metastasized. Contrast-enhanced multidetector computed tomography plays a central role in diagnosing, staging, and treatment planning for pancreatitis and pancreatic cancer. This article introduces the functional anatomy of the pancreas and common bile duct and the epidemiology, pathobiology, and computed tomography imaging of pancreatitis, calculi, and pancreatic cancer.
Pancreatitis and pancreatic can-cer are complex diseases associ-ated with profound effects on patient quality of life and poor
prognosis, particularly if not detected and treated promptly. Contrast-enhanced computed tomography (CECT), usually undertaken with mul-tidetector equipment, has become the standard pancreatic imaging modality for diagnosing, staging, and planning treatment for these diseases. Carefully timed CECT scan acquisitions can maximize the utility of intravenous contrast agents to identify specific signs of pancreatitis, duct-obstructing calculi (stones), and tumors, as well as poten-tially life-threatening complications.
Anatomy and PhysiologyThe pancreas is the largest gland
in the digestive system. It plays life-sustaining roles in the regulation of
food digestion and blood glucose levels. It was first tentatively identified by the ancient Greeks, but its functions and even its existence as a discrete organ did not become clear until the 1500s, partly because of its visual similarity to mesenteric fat.1,2 German anatomist Johann Georg Wirsung reported the anatomy of the main pancreatic duct in 1642, based on his dissection of an executed convict.2 In the 1850s, French physiologist Claude Bernard reported on the organ’s exocrine roles in excret-ing digestive enzymes.2
Essentially a glandular network of ducts, this heavily vascularized organ is situated in the upper abdomen against the left diaphragm, behind the stomach, and adjacent to the small intestine and the gallbladder, which stores liver bile.3,4 The pancreas is both an endocrine and exocrine organ excreting hormones into the bloodstream and digestive enzymes

646CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
into the upper duodenum (a C-shaped curve in the upper small intestine) at the major papilla.3,4 The major papilla also is known as the ampulla of Vater, hepatopancreatic ampulla, or hepatopancreatic duct.3,4 Partially digested food, called chyme, moves from the stomach into the duo-denum where enzymes break down chyme components for digestion or excretion as waste.
The surface of the pancreas is covered with lobes that contain endocrine cell clusters called islets of Langerhans and clusters of exocrine cells called acini. Acini secrete pancreatic f luids that drain into tiny intralobular duct-ules and then into the main and accessory pancreatic ducts, through which they reach the duodenum.3,4
The pancreatic blood supply comes from branches of the superior mesenteric, celiac, and splenic arter-ies (see Figure 1). The pancreas also is surrounded by a regional network of immune system lymph nodes (see Figure 2).
The pancreas is divided into 3 major regions: the pancreatic head, body, and tail.4 The head rests in the curve of the duodenum. It contains the major papilla and a structure known as the uncinate process, which is a wedge-shaped projection.3 The main pancreatic duct passes through the length of the tail and through the body and the head, terminating at the major papilla where it joins with the common bile duct.3,4 The com-mon bile duct originates in the liver and passes through the pancreatic head to deliver bile into the duodenum.3,4 The accessory pancreatic duct usually enters the duode-num slightly above (~2 cm) the major papilla.4
The anatomy of pancreatic ducts can vary consider-ably between individuals, reflecting prenatal develop-mental differences.4,5 In the most frequent arrangement of pancreatic ducts, seen in half of patients, the acces-sory and main ducts communicate. Pancreas divisum is a congenital variant in which the 2 ducts do not fuse to develop a connection. Divisum long was considered a cause of pancreatitis.6 However, despite its marked deviation from typical duct anatomy, pancreas divisum and other anatomic variants of the ducts usually do not affect pancreas function.5
Figure 1. Gross anatomy of the pancreas, its blood supply, and its relation to other internal organs. Figure 2. Lymph node locations surrounding the pancreas.
Liver
Spleen
Pancreas
Gallbladder
Duodenum
Common bile duct Head
Neck
Tail
Body
Splenic artery
Splenic vein
Portal vein
Uncinate process
Islet of Langerhans
Duct
Pancreatic acini
Gastric
Pancreaticosplenic
Celiac
Hepatic

647CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
Endocrine FunctionsThe pancreas plays a key endocrine role in blood glu-
cose regulation, releasing hormones such as insulin, glu-cagon, somatostatin (which helps regulate insulin and glucagon secretion), and appetite-suppressing pancre-atic polypeptide into the bloodstream.3 The pancreas’ endocrine tissues are composed of well-vascularized islets of Langerhans, which are situated between exo-crine cell acini and are particularly common in the pancreatic tail.4 The cells of the islets of Langerhans are in close physical association with capillaries, allowing access to the bloodstream, into which they release—and from which they receive—regulatory hormone signals.4 The 4 types of cells in the islets of Langerhans are4:
■ Alpha – secrete glucagon to upregulate glucose levels.
■ Beta – secrete insulin to downregulate glucose levels.
■ Delta – secrete somatostatin to regulate alpha and beta cell excretion.
■ Gamma – secrete the appetite-suppressing hor-mone pancreatic polypeptide.
Exocrine FunctionsThe pancreas plays a key role in digestion, produc-
ing alkaline bicarbonate ions that neutralize stomach acids and digestive enzymes that are used to break down foods within the small intestine.3 The exocrine activities of the pancreas are regulated by endocrine hormones at the islets of Langerhans within the pan-creas and by hormones secreted in the stomach and duodenum when food arrives in the stomach. These hormones are then delivered to the pancreas in the bloodstream.3 Pancreatic digestive enzymes include proteases, which break down proteins into amino acids, and lipases, which break down dietary fats.3,4 The pan-creas also is a source of amylase, which breaks down polysaccharide starches into glucose; amylase also is present in mouth saliva.3,4
These digestive enzymes are powerful and could damage and destroy pancreatic tissues. Therefore, they are produced in an inactive form as proenzymes that carry a protective trypsin inhibitor until they are released into the gastrointestinal tract at the major papilla, at which point they are released from the trypsin
and become activated enzymes.3 (Hereditary childhood-onset pancreatitis appears to be associated with a genetic mutation that prevents trypsin deactivation of digestive enzymes within the pancreas.7) Bile that breaks down dietary fats also enters the duodenum at the major papilla.3,4
Pathobiology The pathobiology of acute and chronic pancreatitis
and pancreatic cancer is complex, involving the interac-tion of genetic-molecular pathways, immune system responses, and toxic insults related to environmental and lifestyle factors. Acute and chronic pancreatitis have overlapping etiologies. Recurring acute pancreatitis can progress to become chronic pancreatitis. In turn, chron-ic pancreatitis increases the risk of pancreatic cancer, and type 2 diabetes appears to increase the risk of acute and chronic pancreatitis, calculi, and pancreatic cancer.
Biliary and Pancreatic CalculiHard and potentially obstructive biliary calculi can
develop in the gallbladder, the common bile duct, or the pancreatic ducts.8 These can range in size from sand-like grains to golf balls. Their chemical constituents can vary but usually include calcium and bilirubin, or cholesterol.8
Calculi can be classified by anatomy of origin and by their biochemical components.8 Anatomic classification separates primary gallbladder calculi from secondary gallbladder calculi that have migrated into the common bile duct and primary bile duct calculi. Primary com-mon bile duct calculi are made up mainly of bilirubin, for example, and gallstones are composed of choles-terol.8 The calculus’ color reflects its chemical composi-tion, with black calculi containing bilirubin and brown calculi (usually found in the common bile duct) con-taining calcium bilirubinate.8
Although biliary calculi are most frequently found in the gallbladder, they also can pass into the bile ducts, where they are sometimes called bile duct stones or secondary gallstones.8 Calculi also can develop in, and migrate down along, the bile ducts, including the com-mon bile duct, which passes from the liver through the pancreas.8 In the United States, primary common bile duct calculi occur less often than do gallstones; how-ever, secondary bile duct calculi that initially formed in

648CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
the gallbladder are sometimes seen in association with primary gallstones.8 Common bile duct calculi also occur frequently (70%) among patients who have bile duct calculi.8 Common bile duct calculi and pancreatic duct calculi can grow to obstruct ducts, contributing to pancreatitis.8,9
Calculi obstruction of ducts or the major papilla can be asymptomatic but commonly leads to pancreatitis.8 Without drainage of these structures, patients with this condition often develop jaundice and sometimes fever.8
Acute PancreatitisPancreatitis refers to the inflammation of the pancre-
as. It usually is a diffuse disease of the entire pancreas rather than a focal inflammation, except for cases asso-ciated with trauma, laceration, and hemorrhage.10 Acute pancreatitis has a sudden onset of symptoms and rep-resents a potentially life-threatening condition that can be painful; up to 20% of cases are clinically severe and associated with high morbidity and mortality rates.11,12 Inflammation occurs when pancreatic enzymes become active before they are delivered into the duodenum, resulting in autodigestion of pancreatic tissues.12 In up to 80% of cases, acute pancreatitis is not severe and will resolve over time.12 In severe cases, pancreatic tis-sue, or the tissue of organs around the pancreas, dies. Complications, primarily infection, associated with this necrosis can be localized or systemic and life threaten-ing.12 Mild and severe acute pancreatitis were tradition-ally termed interstitial (edematous) and necrotizing, respectively.13 More than 80% of deaths related to acute pancreatitis are associated with pancreatic necrosis and infection.10
Acute pancreatitis can be caused by a wide array of underlying factors, including heavy alcohol consump-tion and biliary calculi.12 It also can be triggered by mumps, infections, surgery, and endoscopy.12,14
Severe acute pancreatitis complications have been described as 2-phased, referring to an early toxicoen-zymatic phase that occurs during the first 2 weeks, followed in some cases by a subsequent necrotic infec-tion or septic phase usually emerging 3 weeks or more after onset.11 When f luids from the inflamed pancreas enter the bloodstream, pancreatic toxemia can ensue, potentially affecting organ function in the heart, lungs,
kidneys, and brain. Eventually, without timely and effective intervention, multiple organ failure and death can occur.11 The emergence of multidrug-resistant infections in severe acute pancreatitis represents an important management challenge.15
Chronic PancreatitisThe pathogenesis of chronic pancreatic inflamma-
tion is largely unclear.16 Generally speaking, it appears that chronic inflammation triggers progressive fibrotic scarring and tissue damage.16 Calculi can exacerbate inflammation and the loss of exocrine and endocrine tissue function when they obstruct the pancreatic ducts.9 Chronic pancreatitis associated with main pan-creatic duct calculi is sometimes called chronic calcific pancreatitis.
Recurring acute pancreatitis sometimes progresses to chronic pancreatitis.16 A necrosis-fibrosis pathway or sequence has been proposed for this progression, with sequential injuries to pancreatic tissues by alcohol or other insults leading to fibrotic scarring and chronic inflammation.16-18 Metabolic insults to pancreatic tis-sues, particularly in the presence of certain genetic polymorphisms (gene variants), can disrupt trypsin mechanisms and trigger early activation of enzymes within the pancreatic ducts, causing fibrotic scarring that can obstruct ducts.16 Repeated or chronic immune system activation and inflammation can lead to fibrosis and tissue metaplasia, potentially increasing the risk of tumor formation.16 Metaplastic pancreatic ducts are associated with pancreatitis and pancreatic cancer.19
Among patients with alcoholism, progression from acute to chronic pancreatitis is associated with the num-ber and severity of previous acute attacks.17,20 Cessation of alcohol consumption can prevent progression from acute to chronic pancreatitis.17
Pancreatic CancerAlmost all pancreatic cancers arise in the organ’s
exocrine tissue, and an estimated 70% to 78% of pan-creatic tumors occur in the pancreatic head region (see Figure 3).21,22 Approximately 11% of pancreatic cancers arise in the pancreatic body region, and 11% arise in the tail region.22 Because of the likelihood of bile duct obstruction by tumors growing in the

649CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
pancreatic head, tumors in this region often become symptomatic at a less advanced stage than is the case with tumors in the pancreatic body or tail.22 Pancreatic tumors are frequently inoperable after they have metas-tasized or have grown around key blood vessels such as the superior mesenteric vein (see Figure 4).
Of the different forms of pancreatic cancer, the most common is pancreatic adenocarcinoma, an aggressive malignancy arising in the organ’s exocrine enzyme-transporting ducts. Adenocarcinoma represents 85% of all pancreatic cancer diagnoses.22 It is commonly known as invasive adenocarcinoma or duct cell carcinoma.23
Nonadenocarcinoma pancreatic cancers include the exocrine acinar cell carcinoma of the pancreas, which arises in the cells that produce digestive enzymes rather than in the ductal cells that transport them. Acinar cell carcinomas represent the second most common form of pancreatic cancer but are rare.23 Less common forms of exocrine pancreatic cancers include23:
■ Adenosquamous carcinoma.■ Cystadenocarcinoma.■ Giant cell carcinoma.■ Mixed type carcinoma (ductal/endocrine or
acinar/endocrine).
■ Mucinous carcinoma.■ Pancreatoblastoma.■ Papillary cystic neoplasm (Frantz tumor).■ Papillary mucinous carcinoma.■ Signet ring carcinoma.■ Small cell carcinoma.■ Undifferentiated carcinomas.
Figure 3. This contrast-enhanced computed tomography (CECT) scan shows a large locally unresectable adenocarcinoma of the pancreatic head (arrow). Note the difference in attenuation between the tumor and the avidly enhancing normal pancreas. Figure used with permission from Darren DD, Brennan MB, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assessment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1656.
Figure 4. These CECT images show vascular involvement of a pancreatic tumor. A. Pancreatic mass (arrowhead) causing severe flattening of the superior mesenteric vein (white arrow). Note also the cuff of soft tissue (blue arrows) surrounding the celiac axis. B. The coronal reformatted image depicts the degree of venous deformity and the low-attenuation mass (arrow), which was found to be an unresectable pancreatic tumor. Figure used with permis-sion from Darren DD, Brennan MB, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assessment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1662.
A
B

650CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
Collectively, ductal pancreatic adenocarcinoma and acinar cell carcinoma make up nearly all of the newly diagnosed pancreatic cancers each year.23 However, rare neuroendocrine tumors arise in the islet cells and repre-sent 1% or less of pancreatic cancer diagnoses overall.24 Neuroendocrine tumors are sometimes called islet cell tumors.24 Neuroendocrine tumors sometimes result from the multiple endocrine neoplasia type-1 (MEN-1) syndrome, which is inherited and can cause cancer of the pancreas, pituitary gland, and parathyroid gland.23
Pancreatic AdenocarcinomaPancreatic adenocarcinoma tumorigenesis involves
the progressive accumulation of genetic mutations in premalignant cysts that evolve over time into malignant tumors. This process is similar to that seen with colon cancer, in which premalignant epithelial polyps become colon tumors. The continuing accumulation of gene mutations during treatment can limit treatment success because it facilitates the acquisition of resistance to par-ticular chemotherapies or targeted anticancer agents.25
Nonmalignant pancreatic cysts are important pre-cursors to pancreatic cancer.21 Such cysts are seen in an estimated 10% of elderly patients aged older than 75 years.22 Cysts that emerge under conditions of repeated or chronic pancreatic inflammation include intraductal papillary mucinous neoplasms (IPMNs), pancreatic intraepithelial neoplasias (PanIns), and mucinous cystic neoplasms. Under conditions of con-tinued or repeated inflammation and high levels of mutated KRAS gene activity, these cystic lesions can become increasingly dysplastic or disorganized and accumulate additional gene mutations. Over time, they can progress from low-grade type 1 neoplasias into high-grade type 3 precancerous neoplasias, and eventu-ally into malignant adenocarcinoma tumors.21,22 This process is sometimes referred to as acinar-to-ductal metaplasia.26
KRAS gene mutations affect the progression from precursor, or premalignant, cystic lesions into pancre-atic cancers.26 Both IPMN and PanIn cystic lesions are known to be precursors to pancreatic cancers.21 IPMN lesions are associated with a 25% overall risk of develop-ing invasive tumors; those found in the main pancreatic duct are the most likely to become cancerous.21 Although
KRAS mutations occur in up to 65% of nonmalignant IPMN cystic lesions, they occur in more than 90% of pancreatic duct adenocarcinoma cancers.21 More than 90% of PanIn lesions harbor KRAS mutations, possibly rendering them more cancer-prone and dangerous.21
In addition to KRAS mutations, pancreatic cancer frequently is associated with other genetic mutations in the tumor-suppressing p16, p53, CDK2NA, and SMAD4 (DPC4) genes.21,22 BRCA1 and BRCA2 mutations are well known as risk factors for heritable breast cancer; how-ever, these mutations also increase the risk of pancreatic adenocarcinoma, with BRCA2 mutations more than tri-pling the risk of this pancreatic malignancy.27 On average, pancreatic tumor cells harbor 63 genetic mutations in 12 distinct molecular gene pathways.28 Pancreatic adenocar-cinomas harboring SMAD4 (DPC4) mutations are more likely to be aggressively metastatic, meaning they more aggressively spread to regional lymph nodes and distant organs.21 Tumors with this mutation are associated with shorter patient survival times.21
EpidemiologyThe epidemiology of pancreatic disorders is com-
plex and varies between ethnic populations.29 African Americans suffer rates of pancreatic disease up to 3 times higher than other ethnicities in the United States.29 However, calculi—a risk factor for pancreatitis —are less prevalent among African Americans than among whites.8
Pancreatic diseases are complexly related to one another. For example, type 2 diabetes—an endocrine disorder of the pancreas—is associated with increased risks of pancreatitis, calculi, and pancreatic cancer.30
Acute pancreatitis is a leading gastrointestinal cause of hospitalization, with an annual incidence of up to 45 per 100 000 people.29 Reported rates have increased over the past decade, partly because of improved detec-tion of pancreatic enzymes in patients’ blood.29
The estimated annual incidence of chronic pan-creatitis is much lower at 4 per 100 000 people per year.31 As with acute pancreatitis, chronic pancreatitis rates and hospitalizations have increased around the world in recent years, possibly because of increasing levels of tobacco smoking and alcohol consumption.17 Chronic pancreatitis is believed to involve a sequential,

651CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
multiple-step etiology, with acute necrotic events trig-gering obstructive fibrotic scarring and inflammation.16
In 2014, the United States saw an estimated 46 420 patients newly diagnosed with some form of primary pancreatic cancer, and 39 590 pancreatic cancer patients died.23 Pancreatic cancer rates increase with age, par-ticularly after age 50 years. Pancreatic cancers rarely are seen before 40 years of age, and the median age at diagnosis is 71 years.21,22 Pancreatic adenocarcinoma is a highly lethal type of cancer. Although less common than many other types of cancer, it is the fourth-leading cause of cancer deaths in the United States, represent-ing 7% of cancer deaths overall.22,29 Pancreatic cancers typically are diagnosed only after they are advanced, symptomatic, and difficult to treat. More than 90% of patients with pancreatic cancers are diagnosed with metastatic disease.22 Therefore, the 5-year overall survival rates for patients diagnosed with pancreatic adenocarcinoma is 6% or less; more than half of patients die within 2 years of diagnosis.22,25 Pancreatic adenocar-cinoma’s dauntingly low survival rate has held for more than 50 years.22 In contrast, patients diagnosed with the rarer and less aggressive pancreatic neuroendocrine tumors have a 55% overall 5-year survival rate.23
Genetic FactorsGenetic polymorphisms appear to play a central role
in the pathobiology of pancreatic diseases, although these roles are only beginning to be identified and close-ly studied. For example, KRAS gene activity and muta-tions are involved in most pancreatic diseases.22 KRAS gene mutations also might mediate the association of acinar inflammation and pancreatic disease.22 Candidate gene polymorphisms that might be involved in biliary calculi include ApoB-100 polymorphisms.32
The total mutational load of pancreatic genomes increases dramatically between normal and chroni-cally or repeatedly inflamed pancreatic tissue, between chronic pancreatitis and pancreatic cancer, and between precancerous intraepithelial neoplasia and pancreatic adenocarcinoma tumors.22,33 Certain gene polymor-phisms also might increase the risk of acute pancreatitis and the progression of acute to chronic pancreatitis.18 These include mutations in the cystic fibrosis trans-membrane conductance regulator (CFTR) gene, PRSS1,
and SPINK1.7,18 CFTR mutations affect epithelial cells’ chloride channels in a way that can cause thicker pan-creatic exocrine f luids and chronic duct obstruction.7 PRSS1 mutations are seen in hereditary pancreatitis; these mutations lead to a failure to temporarily inacti-vate digestive enzymes with trypsin while the enzymes are still in the pancreas.7 SPINK1 mutations similarly disrupt the trypsin inactivation of digestive enzymes, albeit through a different molecular-genetic pathway than does PRSS1.7,18 Studies indicate that up to 23% of patients diagnosed with pancreatitis harbor SPINK1 mutations compared with approximately 2% of healthy controls.7,34
Genetic polymorphisms’ influence on pancreatic pathogenesis is not always simple. In most cases, poly-morphisms interact with other gene pathways and environmental, dietary, metabolic, and other factors.18 Regions of the PRSS1, PRSS2, and CLDN2 genes are now understood to play a role in alcohol-related pancre-atitis.18
Other Risk Factors Authors of a 2014 meta-analysis of data pooled from
51 studies concluded that heavy alcohol consumption, current tobacco use, and obesity are each strongly asso-ciated with pancreatic disease risk.35 Alcohol consump-tion is a leading causal risk factor for acute and chronic pancreatitis, contributing to up to 67% of chronic pan-creatitis diagnoses in North America and up to 95% of cases in the Asia-Pacific region.17,29,31,36 Tobacco smoking is associated with both acute and chronic pancreatitis, even after alcohol consumption and body mass index are statistically controlled.29,37 Cessation of tobacco and alcohol consumption appear to reduce the risk of acute pancreatitis progression and recurrence and to slow progression of chronic pancreatitis.29,38
PancreatitisIn addition to lifestyle risks, acute pancreatitis is
associated with calculi, particularly among non−African American patients.29 Type 2 diabetes, and possibly type 2 diabetes medication, also appear to be associated with an increased risk of acute pancreatitis.29
Autoimmune disorders appear to increase the risk of both acute and chronic pancreatitis.29 Such

652CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
associations have been reported for patients with inf lammatory bowel disease and systemic lupus erythematosus, for example.29 Autoimmune celiac disease has been estimated to more than double the risk of pancreatitis.39 Autoimmune pancreatitis is infrequent, representing fewer than 5% of pancreatitis diagnoses.16
Risk factors for chronic pancreatitis are most easily introduced by listing the precipitating risk factor eti-ologies, which are classified using the TIGAR-O clas-sification system.17,40 Despite a longstanding belief that pancreas divisum is a cause of pancreatitis, the evidence is mixed, and at least one recent study found no associa-tion between pancreas divisum and chronic pancreatitis or impaired pancreatic exocrine function.5
CalculiBiliary calculi afflicted the people of ancient Egypt
and China, as revealed by autopsies of mummies.41 Today, as much as 15% of the U.S. adult population is believed to have biliary calculi, leading to an estimated 622 000 hospitalizations annually.41
Cirrhosis of the liver and Crohn disease are each strongly correlated with biliary calculi.42 Central obe-sity (increased abdominal fat) and metabolic syndrome increase the risk of developing biliary and pancreatic duct calculi.42 Common bile duct calculi are a common cause of obstructive acute pancreatitis.29 Because obesi-ty is a risk factor for calculi, it is thought to be a possible cause of the increase in reported pancreatitis rates seen in recent years.29
African Americans are significantly less likely to develop calculi than are other ethnicities.8,42 In contrast, calculi appear to be more prevalent among Native Americans and Mexican Americans than in other ethnicities, possibly in part because of genetic factors.8,42
Risk factors also include sex and age. Calculi are unusual in children and are more common in women than in men.42 Risk increases with an increasing num-ber of pregnancies.42 Postmenopausal women tend to face a lower risk of developing calculi than do younger women, but estrogen replacement therapy increases the risk of calculi, suggesting that estrogen plays a role in biliary calculi development.42
Pancreatic CancerModifiable risk factors for pancreatic cancer include
tobacco smoking, obesity, high dietary consumption of animal fats, and type 2 diabetes mellitus.22 Patients with cystic fibrosis or a family history of pancreatic cancer also are at increased risk.22,23 Chronic pancre-atitis increases the risk of developing pancreatic can-cer, although it is important to note that the overall long-term (20-year) risk of this malignancy is only 5% among patients with chronic pancreatitis.22,23
Epidemiological studies of pancreatic cancer high-light the potential importance of public health preven-tion efforts. Researchers who reviewed 117 meta- analyses concluded that two-thirds of major risk fac-tors for pancreatic cancer are modifiable factors such as tobacco use, thereby “affording a unique opportunity for preventing one of our deadliest cancers.”36
Pancreatic cancer risk also has been connected with Helicobacter pylori infection, idiopathic thrombosis, and ABO group blood types other than O.29,36 In addition, taller adults have a moderately higher risk of developing pancreatic cancer.36
Type 2 diabetes is an important risk factor for pan-creatic cancer, increasing risk by 30% to 200%, accord-ing to different studies.29,30,43 Half of patients diagnosed with pancreatic cancer have diabetes; although some studies do not differentiate between type 1 and type 2 diabetes, the association appears to be clear for type 2 rather than type 1 diabetes.21 The association between recently diagnosed diabetes and pancreatic adenocarci-noma is stronger than the long-term risk of this malig-nancy among people with diabetes, suggesting a possi-ble causal modulation of cancer risk by diabetes disease processes, according to a meta-analysis of data pooled from 88 studies.43 The relationship between diabetes and pancreatic cancer also might be bidirectional, such that diabetes and pancreatic cancer might each increase the risk of the other disease.29 For example, in a small proportion ( 1%) of newly onset type 2 diabetes cases, diabetes appears to be caused by pancreatic cancer, and an estimated 40% of patients diagnosed with pancreatic cancer have prior diabetes diagnoses.29
Diabetes medication also might affect pancreatic cancer epidemiology.30 The diabetes drug metformin has been associated with a reduced risk of pancreatic

653CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
cancer, whereas findings about insulin’s role have been inconsistent across studies.30,44
Dietary risk factors have been proposed for pan-creatic cancer, although evidence remains weak.29 Increased fruit or folate intake appears to reduce the risk of pancreatic cancer,36 as does a Mediterranean dietary pattern (consumption of high levels of olive oil, legumes, fruits, and whole grains) when combined with other healthy behaviors like daily physical activity and not smoking.29,45
Other proposed protective factors have included aspirin and tea.22 Evidence for aspirin’s benefits have yet to be confirmed.22,46 Preliminary in vitro and laboratory animal studies had suggested that green tea or coffee might modulate pancreatic cancer risk, with green tea standing out as a promising chemoprotective agent.47,48 However, a meta-analysis of 8 studies found no over-all correlation between green tea consumption and pancreatic cancer risk. Similarly, the large European Prospective Investigation into Nutrition and Cancer found consumption levels of coffee, decaffeinated cof-fee, and tea neither increased nor decreased the risk of pancreatic cancer.47,48
Diagnosis and TreatmentMedical imaging plays a critical role in the diagnosis,
staging and characterization, treatment planning, and post-treatment monitoring of pancreatic diseases.49,50 Although ultrasonography is a noninvasive imag-ing modality option for initial assessment of acute abdominal pain and to confirm or exclude cholelithiasis (gallstones), CECT is the standard first-line modality for detailed abdominal and pancreatic imaging; it is preferred to confirm diagnoses of pancreatitis and pan-creatic cancer.10,13,49,50
CECT helps detect and stage pancreatic cancers.49,50 However, CT imaging has important limitations. For example, CT has not yet been shown to reliably detect early duct anatomy changes indicative of chronic pan-creatitis or to reliably detect the earliest stages of pan-creatic cancer.6
In some situations, other imaging modalities might be more informative. These modalities also are impor-tant in diagnostic pancreatic imaging algorithms. Despite relatively low spatial resolution, positron
emission tomography (PET)-CT functional imaging with 18-f luorodeoxyglucose is superior to MDCT in detection of pancreatic tumor recurrence after sur-gery.49 PET-CT also allows comprehensive whole-body visualization of the extent of metastatic tumors and, therefore, is potentially useful in staging cancers.49 Magnetic resonance (MR) imaging offers better soft-tissue contrast than does CT, and for applications such as detection of suspected small tumors or isoat-tenuating tumors in the pancreatic head, MR imaging might be superior to CT imaging.49 Current diagnostic imaging algorithms for suspected pancreatic tumors recommend initially imaging masses with CECT, but following up with MR imaging if findings from CECT for suspected tumors are ambiguous.51
Computed TomographyContrast-enhanced multidetector CT is a standard
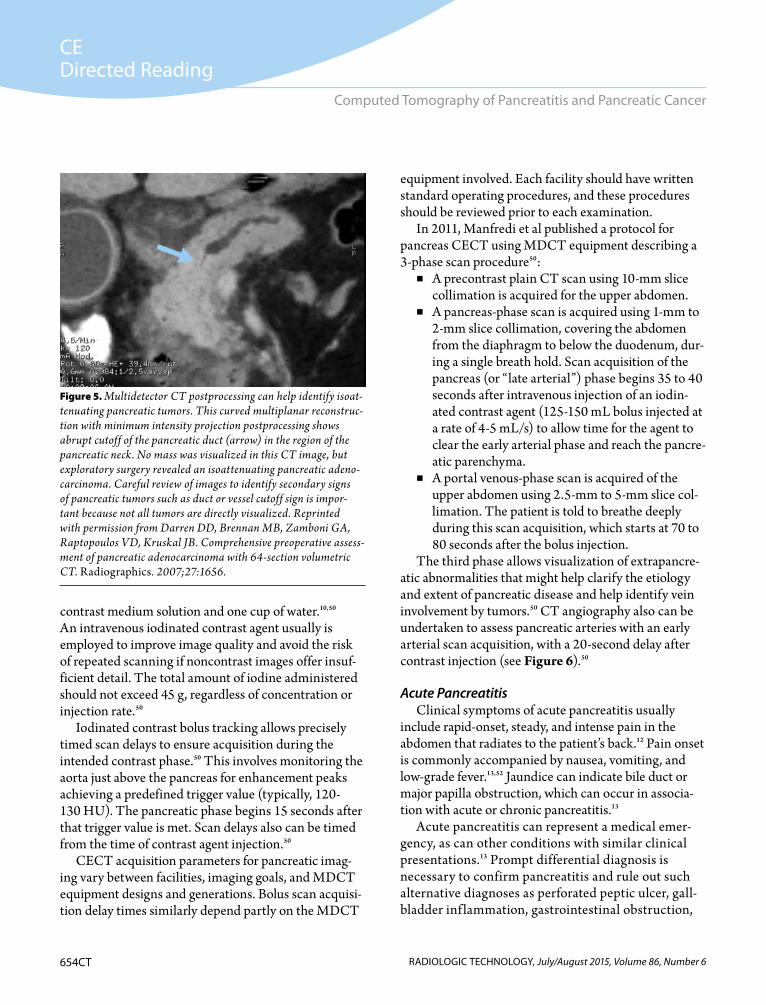
diagnostic imaging modality for rapidly evaluating patients with abdominal symptoms and suspected pan-creatic disease.50 The anatomic detail of CECT images and the versatility afforded by contemporary recon-struction and postprocessing software allow detailed differential diagnosis among disorders and etiologies (see Figure 5).
Pancreatic diseases usually affect older adults. Because of the relatively long latency period between irradiation and radiation-associated tumorigenesis, the long-term secondary cancer risk associated with ionizing radiation is relatively low compared with comparable radiation doses delivered to younger patients. Nevertheless, the ALARA (as low as reasonably achievable) principle is a central consideration for ensuring patient protection during any radiographic examination. Observing the ALARA prin-ciple means that every patient dose of medical radiation should be the lowest possible to achieve clinical goals. Pancreatic disease management can involve repeated CT examinations. Because of the long-term hazards posed by cumulative doses of ionizing radiation, unnecessary CT examinations should be avoided, and set-up and scan acquisitions should be carefully planned and executed to avoid errors that could require additional imaging exami-nations.
For pancreatic CECT imaging, the duodenum and stomach usually are distended with a negative oral
654CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
contrast medium solution and one cup of water.10,50 An intravenous iodinated contrast agent usually is employed to improve image quality and avoid the risk of repeated scanning if noncontrast images offer insuf-ficient detail. The total amount of iodine administered should not exceed 45 g, regardless of concentration or injection rate.50
Iodinated contrast bolus tracking allows precisely timed scan delays to ensure acquisition during the intended contrast phase.50 This involves monitoring the aorta just above the pancreas for enhancement peaks achieving a predefined trigger value (typically, 120-130 HU). The pancreatic phase begins 15 seconds after that trigger value is met. Scan delays also can be timed from the time of contrast agent injection.50
CECT acquisition parameters for pancreatic imag-ing vary between facilities, imaging goals, and MDCT equipment designs and generations. Bolus scan acquisi-tion delay times similarly depend partly on the MDCT
equipment involved. Each facility should have written standard operating procedures, and these procedures should be reviewed prior to each examination.
In 2011, Manfredi et al published a protocol for pancreas CECT using MDCT equipment describing a 3-phase scan procedure50:
■ A precontrast plain CT scan using 10-mm slice collimation is acquired for the upper abdomen.
■ A pancreas-phase scan is acquired using 1-mm to 2-mm slice collimation, covering the abdomen from the diaphragm to below the duodenum, dur-ing a single breath hold. Scan acquisition of the pancreas (or “late arterial”) phase begins 35 to 40 seconds after intravenous injection of an iodin-ated contrast agent (125-150 mL bolus injected at a rate of 4-5 mL/s) to allow time for the agent to clear the early arterial phase and reach the pancre-atic parenchyma.
■ A portal venous-phase scan is acquired of the upper abdomen using 2.5-mm to 5-mm slice col-limation. The patient is told to breathe deeply during this scan acquisition, which starts at 70 to 80 seconds after the bolus injection.
The third phase allows visualization of extrapancre-atic abnormalities that might help clarify the etiology and extent of pancreatic disease and help identify vein involvement by tumors.50 CT angiography also can be undertaken to assess pancreatic arteries with an early arterial scan acquisition, with a 20-second delay after contrast injection (see Figure 6).50
Acute PancreatitisClinical symptoms of acute pancreatitis usually
include rapid-onset, steady, and intense pain in the abdomen that radiates to the patient’s back.12 Pain onset is commonly accompanied by nausea, vomiting, and low-grade fever.13,52 Jaundice can indicate bile duct or major papilla obstruction, which can occur in associa-tion with acute or chronic pancreatitis.13
Acute pancreatitis can represent a medical emer-gency, as can other conditions with similar clinical presentations.13 Prompt differential diagnosis is necessary to confirm pancreatitis and rule out such alternative diagnoses as perforated peptic ulcer, gall-bladder inf lammation, gastrointestinal obstruction,
Figure 5. Multidetector CT postprocessing can help identify isoat-tenuating pancreatic tumors. This curved multiplanar reconstruc-tion with minimum intensity projection postprocessing shows abrupt cutoff of the pancreatic duct (arrow) in the region of the pancreatic neck. No mass was visualized in this CT image, but exploratory surgery revealed an isoattenuating pancreatic adeno-carcinoma. Careful review of images to identify secondary signs of pancreatic tumors such as duct or vessel cutoff sign is impor-tant because not all tumors are directly visualized. Reprinted with permission from Darren DD, Brennan MB, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assess-ment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1656.

655CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
appendicitis, and intestinal or myocardial (inferior wall) infarction.13
In cases of acute pancreatitis, lab tests typically reveal increased levels of pancreatic amylase and lipase; elevated amylase is a preferred method for acute pancre-atitis diagnosis.12,13 Onset of acute pancreatitis is defined as the time of onset of abdominal pain; the time since onset should be noted in patients’ medical records when tests and imaging are undertaken.53
Using the revised Atlanta classification system, diag-nosis of acute pancreatitis involves confirming at least 2 of the following53:
■ Abdominal pain or “acute onset of a persistent, severe, epigastric pain often radiating to the back.”
■ Serum lipase or amylase activity concentrations at least 3 times greater than the upper limit of normal.
■ Diagnostic imaging findings consistent with acute pancreatitis, obtained using CECT, transabdomi-nal ultrasonography, or MR imaging.
When pain and elevated serum lipase or amylase are confirmed, a diagnosis of acute pancreatitis might be made prior to imaging.53 However, imaging must be
undertaken for diagnosis if a patient presents with pain suggestive of acute pancreatitis but without elevated lipase or amylase levels.53
When enzyme-containing pancreatic f luids escape into general circulation, complications can be severe and include early shock, infection, multiple organ failure, enzyme damage to lung tissue, and systemic inflammation.52 Intra-abdominal hypertension and abdominal compartment syndrome commonly occur in severe acute pancreatitis and can lead to hemorrhage, severe edema, and intestinal obstruction.54 Late compli-cations can include potentially painful scar tissue-lined pockets of pancreatic f luids called pseudocysts that might bleed, rupture, or obstruct ducts.55,56 Acute bleed-ing also can indicate retroperitoneal hemorrhage or pseudoaneurysms, which can be confirmed with follow-up CT imaging.13
Acute Pancreatitis Computed TomographyCECT is the standard imaging examination for diag-
nosing, assessing, and monitoring patients with sus-pected acute pancreatitis.10 CT imaging also is used to assess prognosis and plan treatments.13 Serial or repeat-ed MDCT examinations allow close monitoring of the progression of acute pancreatitis and timely detection of potentially life-threatening complications.10
CT examinations have been incorporated into the revised Atlanta classification system’s 3 criteria for diag-nosis of acute pancreatitis, partly because CT images can reveal anatomic defects and irregularities with sufficient detail to allow for the differentiation of pancreatitis from other disorders that have similar signs and symptoms.10
MDCT imaging of acute pancreatitis can involve a 3-phase or a biphasic acquisition protocol (see Table).57 Postacquisition reconstruction of 2-D axial images or images in other planes, as needed, is possible with any standard MDCT workstation.10 In CECT, healthy pan-creas tissue has uniform morphologic texture and exhib-its homogeneous CT enhancement of 100 HU to 150 HU.10,57 Acute pancreatitis is associated with enlargement of the pancreas and CT enhancement heterogeneities, with the degree of inflammatory edema correlating with the degree of enhancement heterogeneity.10
Acute accumulations of enzyme-containing pan-creatic f luids might appear within or close to the
Figure 6. A pancreatic CT angiograph showing a large mass (arrows) arising from the pancreatic neck and invading the stomach (arrowhead), representing a T3 tumor that does not involve the celiac axis or superior mesenteric artery. This tumor was associated with distant metastases and deemed unresect-able. Reprinted with permission from Darren DD, Brennan MB, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assessment of pancreatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1659.

656CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
pancreas.57 If a f luid accumulation does not resolve, it could develop into an encapsulated acute pseudocyst or pancreatic abscess.57 A pseudocyst will appear on CECT images as a discrete, low-attenuation area with a thin but well-defined wall.57 Pancreatic abscesses usu-ally occur 4 weeks or later after onset of symptoms and appear on CECT images as discrete pus accumulations with a thick, irregular wall in contrast to pseudocysts’ thin and well-defined walls.57
CT images also are important in identifying the cause or etiology of confirmed cases of acute pancreatitis, such as gallstones or pancreatic calculi, and in identifying extra-pancreatic findings associated with acute pancreatitis, such as liver or gallbladder inflammation (which appear as enhanced regions on CECT).13,57
As previously noted, CT examination is not always needed to diagnose acute pancreatitis, and mild cases that resolve might not require CT imaging.57 CT signs of pancreatitis and necrosis might not be apparent in the first 12 hours after onset of symptoms.57
If acute pancreatitis does not resolve within 3 to 7 days of hospitalization, or worsens clinically, then CECT examinations are undertaken to determine whether pan-creatic necrosis has occurred.13 Pancreatic necrosis is visi-ble on CECT images 2 to 3 days after onset of symptoms; thus, contrast CT examinations undertaken between
48 and 72 hours after onset allow for severity assessment and detec-tion of pseudocysts and other complications.71 Necrosis can be focal or diffuse.57 In CECT images, necrotic tissue is nonenhancing unless it causes vascular hemor-rhage, which appears as increased attenuation.57
Usually, CECT can-not differentiate sterile from infected necrosis.13 However, the presence of small air bubbles is a sign of infection.13 CT-guided percutane-
ous fine-needle aspiration of necrotic fluids allows for lab-oratory culture testing for bacterial or fungal infection.13
Predicting the clinical severity of acute pancreatitis is possible using clinical and imaging criteria.13 Pleural effusion on a plain chest radiograph is predictive of severe acute pancreatitis. The condition is seen in only 8.6% of patients with mild pancreatitis, whereas in severe cases, pleural effusion is seen in 84% of patients.13,58
The CT Severity Index (CTSI) facilitates radiologic assessment of acute pancreatitis, associated f luid accu-mulations, and pancreatic necrosis.13 CTSI scores are based on observer assessments of 5 pancreatic anatomy observations and the percentage of pancreas that appears necrotic in reviews of CECT pancreas images.13
CT finding:■ Score 0 – normal pancreas (Grade A).■ Score 1 – pancreatic enlargement
(Grade B).■ Score 2 – pancreatic inflammation or peripancre-
atic fat changes (Grade C).■ Score 3 – single
collection of peripancreatic f luid (Grade D).
■ Score 4 – two or more collections of pancreatic f luid or retroperitoneal air (Grade E).
Table
MDCT Parameters for Acute Pancreatitis Biphasic Imaging57
Vascular Phase (40-45 s) Portal Venous Phase (65-70 s)
IV contrast injection rate 4-5 cm3/s 3 cm3/s
Imaging range Celiac through pancreas Dome of diaphragm to symphysis pubis
Bolus tracking 150 HU threshold in aorta at celiac artery level; 8- to 10-second delay
55 HU threshold in right lobe of liver at level of right portal vein
Slice thickness 1-3 mm 5 mm
Spacing 1-3 mm 5 mm
Peak kV 120-140 kV 120-140 kV
mA 240-280 mA 240-280 mA
Time 0.5-0.8 s 0.5-0.8 s
Field of view 28 Varies depending on size of patient
Abbreviations: HU, Hounsfield Units; kV, kilovoltage; mA, milliampere; MDCT, multidetector computed tomography. Reprinted with permission from Rebello AS, Sahani DV. Imaging of acute pancreatitis. In: Sahani DV, Samir AE, eds. Abdominal Imaging. Vol 1. Maryland Heights, MO: Saunders Elsevier; 2011:769.
657CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
Pancreatic necrosis:■ Score 0 – no necrosis noted.■ Score 2 – 30% necrosis.■ Score 4 – 30% to 50% necrosis.■ Score 6 – 50% necrosis.To calculate the CTSI score, the numerical scores
for CT findings (grades) and percent of necrosis are summed.13 Scores of 0 to 3 are predictive of mild acute pancreatitis, with a 3% risk of mortality, whereas scores of 7 to 10 are predictive of severe cases and are associ-ated with 17% mortality.13 CTSI scores higher than 5 are associated with an increased likelihood of surgical necrosectomy.13 The accuracy of CTSI staging of pan-creatitis depends on administration of an intravenous contrast agent, and CTSI should not be undertaken with plain radiographic images.10
In rare cases, pancreatitis affects only one segment or region of the pancreas, often the head.10 This is an indica-tion of biliary obstruction–associated pancreatitis and usu-ally is associated with recurrent and mild acute episodes.10
Prognostic Scoring and Classification of Acute PancreatitisPredicting the clinical course of acute pancreatitis
can be challenging, and severe acute pancreatitis is associated with high morbidity and mortality rates.59 Therefore, prognostic risk-stratification systems have been devised using clinical variables to differentiate patients with severe cases who require immediate and aggressive medical intervention and monitoring from those with nonsevere cases.52 Each system has its strengths and weaknesses.59
Single biochemical-marker systems have been pro-posed, including hematocrit, creatinine and blood urea nitrogen, and C-reactive protein levels.59 Produced by the liver, C-reactive protein is an inflammatory biomarker of acute pancreatitis.59 It sometimes is used to help differen-tiate between mild and severe acute pancreatitis.59
Clinical severity assessment instruments used in cases of acute pancreatitis include the revised Atlanta classification system,53 Ranson Criteria for Pancreatitis Mortality,60 the 12-item Acute Physiology and Chronic Health Evaluation (APACHE II)61 system, the Modified Glasgow (Imrie’s) Severity Criteria,62 and radiologic imaging-based or imaging/clinical-based scoring systems like the CTSI.63,64
Some of these systems have been modified from their original form to address the recently recognized prognostic significance of organ dysfunction outside of the pancreas, which might be even more important than infection status in predicting mortality.52 One example is the revised Atlanta classification system, which classifies cases of acute pancreatitis as mild, moderate, or severe52,53:
■ Mild – no organ failure, no local or systemic com-plications.
■ Moderate – transient ( 48 hours) organ function disruption (organ failure), local or systemic com-plications, or both.
■ Severe – persistent ( 48 hours) organ dysfunc-tion (organ failure).
Organ failure is defined as shock (systolic blood pressure 90 mm Hg), pulmonary insufficiency (PaO2 60 mm Hg), renal failure (serum creatinine 2 mg/dL following rehydration), or gastrointestinal bleeding (exceeding 500 mL in 24 hours).13 Under the revised Atlanta classification system, persistent organ failure also can be assessed using the modified Marshall score,52 which quantifies organ dysfunction of the lungs, heart, circulatory system, and kidneys.59 Assessed with-in 72 hours of hospitalization, the Marshall score com-pares well to the APACHE II score in predicting patient death.59 The alternative sequential organ failure assess-ment score also is used 48 hours after symptom onset to assess organ failure; it has a sensitivity of 86% and a specificity of 79% for predicting patient death, which is comparable to the Marshall score’s accuracy.59
A separate severity classification system for acute pancreatitis called determinant-based classification has been promulgated.52,65 This system adds a “critical” clas-sification to the risk-assessment categories of mild, mod-erate, and severe acute pancreatitis52,65:
■ Mild – no necrosis of pancreatic tissue and no organ dysfunction.
■ Moderate – sterile (uninfected) necrosis of pan-creas tissue, transient ( 48 hours) systemic organ dysfunction, or both.
■ Severe – infected necrosis of the pancreas or persis-tent ( 48 hours) systemic organ dysfunction.
■ Critical – infected necrosis of pancreas tissue and persistent ( 48 hours) systemic organ dysfunction.
658CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
Managing Acute PancreatitisPatients experiencing pancreatic necrosis must
be monitored for persisting organ failure, shock, and pancreatic or systemic infection. They might be hospi-talized for as long as 6 months.13 Aggressive f luid resus-citation, long considered necessary for treating severe acute pancreatitis, can worsen patients’ outcomes.52 Patients should be monitored for intra-abdominal hypertension.52
Acute pancreatitis complications include clinical evidence of heart, lung, or kidney dysfunction (usually within 2-3 days of onset); infection; abscesses and pseu-docysts; and metabolic disorders leading to coagulopa-thy, hyperglycemia, diabetes or diabetic coma, hypo-calcemia, thrombosis, or bleeding.10 Pancreatic necrosis affects up to 10% of patients and can become infected or remain sterile.66 Necrotic pancreatitis-associated infections can become systemic, and systemic infec-tions might become drug resistant if antibiotics are overused; therefore, prophylactic antibiotic therapy should not be undertaken.52 Percutaneous draining is undertaken for pancreatitis-associated infection; if the procedure is ineffective and abdominal organs begin to fail, surgery is indicated.52
Overall, less aggressive management offers bet-ter patient outcomes compared with more aggressive interventions. Thus, early surgery should be avoided if possible.52 Pancreatic necrosis should be managed with percutaneous drainage when possible. Fine-needle aspira-tion allows fluid collection for confirmation of infected necrotic tissue in the pancreas or adjacent organs.52 This allows for detection of drug-resistant infections and avoid-ance of unnecessary antibiotic treatment when tissue is determined not to be infected.52
Open surgery is associated with high morbidity and mortality rates and should be avoided if possible.52,66 Endoscopic and interventional radiologic approaches for drainage and debridement of necrotic tissue might be undertaken, but open abdominal surgery (necrosec-tomy) is sometimes necessary.66 Multiple endoscopic necrosectomy procedures can remove f luid accumula-tions and tissue necrosis and appear to be associated with a lower risk of postprocedural complications than open surgery.52 Another alternative to open sur-gery is minimally invasive retroperitoneal pancreatic
necrosectomy, which involves CT-guided placement of a percutaneous drain.52
Acute pancreatitis progression and recurrence can be slowed by tobacco and alcohol cessation.29 Patients diag-nosed with pancreatitis should be informed of cessation program resources and told that refraining from tobacco and alcohol use can help improve their prognosis.
Chronic PancreatitisChronic pancreatitis is sustained pancreatic inflam-
mation that has caused progressive and permanent loss of organ function.67 Clinical presentations for chronic pancreatitis involve abdominal pain in up to 85% of patients, associated with severe epigastric pain, or pain of the left or right quadrant of the abdomen radiating to the back.67 Patients often adopt a stooped posture because of abdominal pain.67 Chronic pancreatitis pain might involve either constant and severe pain or repeat-ed episodes of pain lasting up to several weeks followed by intervening periods of respite.67
Chronic pancreatitis etiologies are classified using the TIGAR-O system (see Box). Chronic pancreatitis is associated with progressive symptoms stemming from long-term inflammation and accumulated fibrotic scar-ring that diminishes endocrine and exocrine tissue func-tion.38 Therefore, complications can include malnutri-tion and weight loss caused by the loss of exocrine tissue
Box
The TIGAR-O System to Categorize Risk Factors for Developing Chronic Pancreatitis17
■ Toxic-metabolic − alcohol, tobacco, hyperlipidemia, chronic renal failure, toxins like organotin compounds, and medica-tion abuse (primarily involving the pain medication phenac-etin, which was banned in the United States in 1983).
■ Idiopathic − tropical calcific pancreatitis, fibrocalculous pan-creatic diabetes.
■ Genetic − dominant-allele disorders.■ Autoimmune − isolated autoimmune chronic pancreatitis,
autoimmune disease syndrome−associated pancreatitis.■ Recurring and severe acute pancreatitis progression − post-
necrotic, recurrent acute pancreatitis, ischemic vascular dis-ease, postirradiation.
■ Obstructive − duct obstruction by tumor, post-traumatic pancreatic duct scarring.

659CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
function and type 3c pancreatic diabetes caused by the loss of endocrine tissue function.16 Pancreatic enzyme insufficiency can cause malnutrition via impaired gut digestion and absorption, a sign of advanced chronic pancreatitis-associated loss of exocrine tissue.16 Fatty or oily loose stool is evidence of lipase insufficiency.16 Chronic pancreatitis also can cause osteoporosis because of the low vitamin D levels resulting from impaired fat absorption; this affects an estimated 25% of patients.16 Other complications include9,16:
■ Pancreatic duct calculi and pseudocysts.■ Bile duct obstructions.■ Fibrotic scarring of the duodenum.■ Bleeding in the gastrointestinal tract.■ Pancreatic fistula (pancreatic f luid leaking).■ Lung damage.■ Pleural effusion.■ Pancreatic cancer.Calculi and pseudocysts that obstruct ducts can act
as feedback mechanisms, worsening pancreatic inflam-mation and loss of endocrine and exocrine function.68 Biliary and pancreatic calculi commonly are discovered in the course of diagnostic workups for pancreatitis or pancreatic cancer. Endoscopic removal has limited suc-cess for pancreatic duct calculi, but even incomplete removal and relief of intraductal pressure can ease a patient’s pain.9 Extracorporeal shockwave lithotripsy can fragment remaining calculi from pancreatic and biliary ducts after endoscopic procedures, allowing natural passage into the gut or removal in follow-up endoscopy.68,69 When endoscopy approaches fail—or when pancreatic cancer also is suspected—calculi can be removed surgically via operations such as pancreato-duodenectomy, which is the most common technique for removing pancreatic tumors.9,69
Treatment of chronic pancreatitis focuses on manage-ment of complications, supportive therapy for abdomi-nal pain (including alcohol and tobacco abstinence), administration of nonsteroidal anti-inflammatory drugs, and management of maldigestion.38 As with acute pan-creatitis, smoking and alcohol cessation might slow the progression of disease, and patients should be provided with resources to help change their behavior.38
Pseudocysts are a common complication of pancre-atitis. They are pancreatic f luid-filled cysts contained
by fibrotic tissue that appear to result from downstream duct obstructions and are evidenced by upstream ductal dilatation.38 Pseudocysts can be associated with increased pain, vomiting, and duct obstructions, and they can be treated with endoscopic drainage. When bile duct obstruction or damage leads to jaundice, endoscopic or surgical decompression is indicated. Administration of exogenous pancreatic enzymes can improve maldigestion resulting from impaired pancreas exocrine function.38 When weight loss is pronounced, pancreatic cancer (which is associated with chronic pancreatitis) might be responsible.67 Lung damage, pleural effusion, and shortness of breath are indications for pulmonary imaging and consideration of endoscopic stent placement.38
Chronic Pancreatitis Computed TomographyCT imaging is useful for confirming chronic pan-
creatitis, detecting its complications, and identifying duct obstructions.6 Chronic pancreatitis usually causes the pancreas to atrophy, thereby appearing progres-sively smaller.6 Pancreatic duct calculi and other pan-creatic calcifications are common throughout chronic pancreatitis-affected pancreas tissues and can obstruct ducts.67 Calcifications are identified easily as hyper-dense foci that frequently are rounded when small or irregular when larger.6 Calculi can be seen readily even in nonenhanced CT imaging but can be confused with splenic artery calcifications when iodinated contrasts are not administered.6
CT images of chronic pancreatitis reveal an atro-phic pancreas and dilatation of the main pancreatic duct and, not infrequently, obstructions contributing to duct dilatation and pancreatic inflammation.6 As previously noted for acute pancreatitis, CT imaging can detect complications such as pseudocysts, which occur in 25% of patients with chronic pancreatitis.67 Pseudoaneurysms also can occur in the pancreatic, duodenal, and splenic arteries.67
Pancreatic CancerTypically, precursor cystic lesions and early-stage
pancreatic cancers are asymptomatic.22 These malig-nancies tend to be diagnosed only after they have pro-gressed to advanced stages and have already spread to

660CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
regional lymph nodes and distant organs, by which time they are difficult to manage.22
Common clinical signs and symptoms of pancreatic cancers include21:
■ Abdominal pain.■ Back pain.■ Nausea.■ Vomiting.■ Diarrhea.■ Anorexia and weight loss.■ Physical weakness.■ Dark urine.■ Itching.■ Type 2 diabetes. Clinical signs and symptoms can vary depending
on where the tumor is located in the pancreas.21,22 For example, jaundice is commonly associated with tumor obstruction of bile ducts passing through the pancreatic head and is less common when tumors occur in the pan-creatic body or tail regions.21,22 Tumors in the pancreatic head tend to become symptomatic at an earlier stage than do tumors in the pancreatic body or tail.22
Other signs include hepatomegaly, right upper quad-rant abdominal mass, and cachexia (muscle wasting).22 Cachexia is common but is not strongly associated with cancer stage or tumor burden.21 Large pancreatic tumors can encroach on the duodenum and stomach, obstructing the gastrointestinal tract and leading to nausea and loss of appetite.22
Pancreatic adenocarcinoma typically metastasizes to the liver, abdomen, and lungs.21 Pancreatic cancer test-ing is indicated for any patient aged older than 50 years newly diagnosed with diabetes and any of the signs or symptoms described above.22 Imaging and blood tests are undertaken and often initially include transabdomi-nal ultrasonography, a complete blood count, and liver enzyme and bilirubin tests.22 Endoscopic biopsy with ultrasonography allows confirmation and pathologic testing of the tumor.21
Pancreatic Cancer Computed TomographyDiagnostic CECT imaging of pancreatic ductal
adenocarcinoma is useful in confirming the presence of tumors, staging cancer (documenting tumor locations, sizes, and involvements with other organs and tissues),
and monitoring patients and restaging cancers after treatment.51
Biphasic pancreatic CECT is sensitive for diagnostic and staging imaging of adenocarcinoma, as well as for detection of metastatic tumors beyond the pancreas (eg, liver).51 The portal venous-phase scan acquisition image offers good visualization of veins and peripan-creatic organs such as the liver that might harbor meta-static pancreatic tumors.51
Adenocarcinoma tumors are visualized as low-enhancement regions that contrast with the enhancing normal tissues of the pancreas, making CECT an excel-lent modality for diagnostic imaging of these malignan-cies (see Figure 3).49,51,70 However, in approximately 10% of tumors, pancreatic adenocarcinomas are isoat-tenuating with surrounding nonmalignant pancreatic tissue.51 Therefore, images must be reviewed for evi-dence of duct or blood vessel encroachment or cutoff by tumors that are not otherwise evident (see Figure 5).70 Postprocessing techniques such as maximum intensity projections can improve visualization of duct and vas-cular deformation and dilatation, indirectly revealing the presence of isoattenuating tumors.70
Current diagnostic imaging algorithms for sus-pected pancreatic tumors recommend initially imag-ing pancreatic masses with CECT, but following up with MR or endoscopic ultrasound and biopsy if a suspected tumor is not visualized on the CT image.51 If CECT does detect pancreatic cancer, endoscopic ultrasound and biopsy are performed for pathologic confirmation as well as staging and assessment of tumor resectability.51
Adenocarcinomas of the uncinate process have distinct patterns from those of adenocarcinoma tumors elsewhere in the pancreatic head region.71 These include significantly less frequent pancreatic duct and common bile duct dila-tation and significantly more frequent mesenteric artery encasement by tumors in the uncinate process.71
Premalignant cystic neoplasms are at high risk of progressing to pancreatic adenocarcinoma tumors. Premalignant cystic neoplasms like intraductal papillary mucinous neoplasms (IPMNs) and mucinous cystic neo-plasms can be detected in diagnostic imaging examina-tions, but high-risk pancreatic intraepithelial neoplasm (PanIn) cysts are commonly missed.22 Small cysts of any

661CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
type can be difficult to characterize and might be mistak-en for pseudocysts, although a cystic wall is usually read-ily detectable in pseudocysts and is absent in IPMNs.51 IPMNs can cause CECT-detectable dilatation of the main pancreatic duct and bulging of the major papilla.51
Staging Pancreatic CancerTreatment options depend on tumor location and
tumor, node, and metastases (TNM) stage.22,72 The National Comprehensive Cancer Network regularly updates guidelines for pancreatic tumor staging.72,73 CT imaging plays a central role in the staging and assess-ment of surgical resectability of pancreatic tumors.22 Tumors also are restaged after systemic therapy.72
Managing Pancreatic CancerMost patients diagnosed with pancreatic cancer
already have metastatic disease. For these patients, supportive care is emphasized, and f luorouracil and gemcitabine-based chemotherapy regimens might be administered to modestly prolong the patient’s survival time.21,22,73 A combination chemotherapy regimen of f luorouracil, irinotecan, oxaliplatin, and leucovorin (FOLFIRINOX) is emerging as a standard option for metastatic pancreatic cancer.22,28,73 When localized, non-metastatic tumors are unresectable, radiation therapy or a combination of chemotherapy with gemcitabine and radiation therapy often is administered.21 Generally, T4-grade tumors are not resectable, but T1, T2, and T3 tumors are sometimes resectable.22,72
Vascular involvement is a key determinant of tumor resectability.21 Closely assessing tumor involvement of the celiac and superior mesenteric arteries and veins, the portal vein, and hepatic artery are crucial steps in deter-mining tumor resectability.21 Tumors without any arterial or superior mesenteric or portal vein involvement might be resectable. Tumors not eligible for surgery include those involving metastatic disease, including lymph nodes distant to the pancreas, or tumors that encase the superior mesenteric artery or celiac axis ( 180°).72 Resection also is not an option when tumor involvement or occlusion of major veins renders vascular reconstruction impossible.72
Resection of tumors in the pancreatic head or neck can involve open surgery (pancreaticoduodenectomy), distal pancreatectomy, or laparoscopic surgery to remove tumors of the pancreatic body or tail, or mini-mally invasive resections.21 Tumor resection usually is accompanied by adjuvant or neoadjuvant (presurgery) administration of chemotherapy and radiation therapy to kill remaining tumor cells in the surgical margins or in lymph node tissue.21 For example, FOLFIRINOX, gemcitabine, and paclitaxel albumin-stabilized nanoparticle formulation (nab-paclitaxel) are becom-ing more widely used as adjuvant therapies.21 Adjuvant immunotherapies also are undergoing clinical trial investigations.21
ConclusionCECT plays a central role in the diagnostic imag-
ing, disease staging, and monitoring of patients with pancreatitis and pancreatic cancer. As the contributions to pancreatic disease of molecular-genetic pathways become better understood, it might become possible to develop better prognostic biomarkers and targeted, etiology-specific therapeutic agents, reducing morbidity and improving survival rates associated with pancreati-tis and pancreatic cancer.18 Genetic biomarker tests that can reveal tumors harboring SMAD4 mutations might allow for better risk-stratification of patients to person-alize treatment plans.21
Some researchers expect routine genetic testing to soon become central to the management of pancreatic diseases.18 The development of increasingly sophisticated diagnostic imaging techniques and serum tumor biomark-ers might help realize the longstanding goal of detecting premalignant lesions and more readily curable early-stage pancreatic tumors.74 Indeed, although the role of CECT in cancer screening for early detection of adenocarcinoma is controversial, the detection of very early-stage tumors should become increasingly feasible as MDCT designs and postprocessing algorithms improve.51
New Mexico-based medical writer and journalist Bryant Furlow, BA, is a regular contributor to Radiologic Technology, The Lancet Oncology, Oncology Nurse Advisor’s “Radiation and Your Patient” column, and
Click here in the online version of this article to view the TNM staging for pancreatic cancer.
662CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
other publications. He reports on medical imaging, clinical oncology, radiation therapy, and respiratory medicine.
Reprint requests may be mailed to the American Society of Radiologic Technologists, Communications Department, 15000 Central Ave NE, Albuquerque, NM 87123-3909, or e-mailed to [email protected].
© 2015 American Society of Radiologic Technologists
References 1. Tsuckiya R, Kuroki T, Eguchi S. The pancreas from Aristotle
to Galen [published online ahead of print November 6, 2014]. Pancreatology. 2015;15(1):2-7. doi:10.1016/j.pan.2014.10.011.
2. Navarro S. A brief history of the anatomy and physiology of a mysterious and hidden gland called the pancreas. Gastroenterol Hepatol. 2014;37(9):527-534. doi:10.1016/j .gastrohep.2014.06.007.
3. Guyton AC, Hall JE. Secretory functions of the alimentary tract. Textbook of Medical Physiology. 10th ed. Philadelphia, PA: WB Saunders; 2000:738-753.
4. Ellis H. Anatomy of the pancreas and the spleen. Surgery. 2013;31(6):263-266.
5. Bülow R, Simon P, Thiel R, et al. Anatomic variants of the pancreatic duct and their clinical relevance: an MR-guided study in the general population. Eur Radiol. 2014;24:3142-3149. doi:10.1007/s00330-014-3359-7.
6. Graziani R, Cenci D, Franzoso F, Coser D, Neri M. The role of computed tomography. In: Balthazar EJ, Megibow AJ, Mucelli RP, eds. Imaging of the Pancreas: Acute and Chronic Pancreatitis. Berlin, Germany: Springer-Verlag; 2009:149-182.
7. Testoni PA. Acute recurrent pancreatitis: etiopathogenesis, diagnosis and treatment. World J Gastroenterol. 2014;20(45): 16891-16901.
8. Tazuma S. Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol. 2006;20(6):1075-1083.
9. Liu BN, Zhang TP, Zhao YP, Liao Q , Dai MH, Zhan HX. Pancreatic duct stones in patients with chronic pancreatitis: surgical outcomes. Hepatobil Pancreat Dis Int. 2010;9(4): 423-427.
10. Balthazar EJ. The role of computed tomography. In: Balthazar EJ, Megibow AJ, Mucelli RP, eds. Imaging of the Pancreas: Acute and Chronic Pancreatitis. Berlin, Germany: Springer-Verlag;2009:49-78.
11. Bassi C, Falconi M, Butturini G, et al. Early complications of severe acute pancreatitis. http://www.ncbi.nlm.nih.gov /books/NBK6932/?report=reader#!po=105.000. Accessed December 20, 2014.
12. Fagniez PL, Rotman N. Acute pancreatitis. http://www .ncbi.nlm.nih.gov/books/NBK6932/?report=reader#!po =105.000. Accessed December 20, 2014.
13. Kwon RZS, Mortele KJ, Banks PA. Clinical aspects of acute pancreatitis: features, prognosis and use of imaging findings in therapeutic decision making. In: Balthazar EJ, Megibow AJ, Mucelli RP, eds. Imaging of the Pancreas: Acute and Chronic Pancreatitis. Berlin, Germany: Springer-Verlag;2009:15-32.
14. Vanlioglu B, Chua TC. Presentation of mumps infection as acute pancreatitis without parotitis. Pancreas. 2011;40(1): 167-168. doi:10.1097/MPA.0b013e3181eabd3c.
15. Lee HS, Lee SK, Park DH, et al. Emergence of multidrug resistant infection in patients with severe acute pancreatitis. Pancreatology. 2014;14(6):450-453. doi:10.1016/j.pan.2014 .10.003.
16. Muniraj T, Aslanian HR, Farrell J, Jamidar PA. Chronic pan-creatitis: a comprehensive review and update: Part I: epide-miology, etiology, risk factors, genetics, pathophysiology, and clinical features. Disease-a-Month. 2014;60:530-550.
17. Jupp J, Fine D, Johnson CD. The epidemiology and socio-economic impact of chronic pancreatitis. Best Pract Res Clin Gastroenterol. 2010;24:219-231. doi:10.1016/j.bpg.2010 .03.005.
18. Whitcomb DC. Genetic risk factors for pancreatic disorders. Gastroenterology. 2013;144:1292-1302. doi:10.1053/j.gastro .2013.01.069.
19. Delgiorno KE, Hall JC, Takeuchi KK, et al. Identification and manipulation of biliary metaplasia in pancreatic tumors. Gastroenterology. 2014;146(1):233-244. doi:10.1053/j.gastro .2013.08.053.
20. Ammann RW, Muellhaupt B. Progression of alcoholic acute to chronic pancreatitis. Gut. 1994;35(4):552-556.
21. Ryan DP, Hong TS, Bardeesy N. Pancreatic adenocarcinoma. N Engl J Med. 2014;371(11):1039-1049. doi:10.1056/NEJMra 1404198.
22. Maniraj T, Jamidar PA, Aslanian HR. Pancreatic cancer: a comprehensive review. Disease-a-Month. 2013;59:368-402.
23. Pancreatic cancer. National Cancer Institute Web site. http://www.cancer.gov/cancertopics/types/pancreatic. Accessed November 19, 2014.
24. Pancreatic neuroendocrine tumors (islet cell tumors) treat-ment for health professionals (PDQ). National Cancer Institute Web site. http://www.cancer.gov/cancertopics/pdq /treatment/isletcell/HealthProfessional/page1. Accessed November 20, 2014.
25. Li J, Wientjes MG, Au JL. Pancreatic cancer: pathobi-ology, treatment options, and drug delivery. AAPS J. 2010;12(2):223-232. doi:10.1208/s12248-010-9181-5.
26. Seton-Rogers S. Pushing pancreatic cancer to take off. Nat Rev Cancer. 2012;12:739. doi:10.1038/nrc3383.
663CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Furlow
27. Vyas O, Leung K, Ledbetter L, et al. Clinical outcomes in pancreatic adenocarcinoma associated with BRCA-2 muta-tion. Anticancer Drugs. 2015;26(2):224-226. doi:10.1097 /CAD.0000000000000178.
28. Mohammed S, Van Buren G, Fisher WE. Pancreatic cancer: advances in treatment. World J Gastroenterol. 2014;20(28):9354-9360. doi:10.3748/wjg.v20.i28.9354.
29. Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology. 2013;144:1252-1261. doi:10.1053/j.gastro.2013.01.068.
30. Bosetti C, Rosato V, Li D, et al. Diabetes, antidiabetic medication, and pancreatic cancer risk: an analysis from the International Pancreatic Cancer Case-Control Consortium. Ann Oncol. 2014;25(10):2065-2072. doi:10.1093/annonc /mdu276.
31. Yadav D, Timmons LJ, Benson JT, Dierkhising RA, Vege SS, Chari ST. Incidence, prevalence and survival of chronic pancreatitis: a population-based study. Am J Gastroenterol. 2011;106(12):2209.
32. Gong Y, Zhang L, Bie P, Wang H. Roles of ApoB-100 gene polymorphisms and the risks of gallstones and gallbladder cancer: a meta-analysis. PLoS One. 2013;18:8(4):e61456. doi:10.1371/journal.pone.0061456.
33. Murphy SJ, Hart SN, Lima JF, et al. Genetic alterations associated with progression from pancreatic intraepithelial neoplasia to invasive pancreatic tumor. Gastroenterology. 2013;145(5):1098-1109. doi:10.1053/j.gastro.2013.07.049.
34. Witt H, Luck W, Hennies HC, et al. Mutations in the gene encoding the serine protease inhibitor, Kazal type 1 are asso-ciated with chronic pancreatitis. Nat Genet. 2000;25(2):213-216. doi:10.1038/76088.
35. Alsamarrai A, Das SL, Windsor JA, Petrov MS. Factors that affect risk for pancreatic disease in the general population: a systematic review and meta-analysis of prospective cohort studies. Clin Gastroenterol Hepatol. 2014;12(10):1635-1644. doi:10.1016/j.cgh.2014.01.038.
36. Maisonneuve P, Lowenfels AB. Risk factors for pancre-atic cancer: a summary review of meta-analytical studies [published online ahead of print December 14, 2014]. Int J Epidemiol. 2015;44(1):186-198. doi:10.1093/ije/dyu240.
37. Yuhara H, Ogawa M, Kawaguchi Y, Igarashi M, Mine T. Smoking and risk for acute pancreatitis: a systematic review and meta-analysis. Pancreas. 2014;43(8):1201-1207.
38. Chronic pancreatitis. Cleveland Clinic Web site. http:// www.clevelandclinicmeded.com/medicalpubs/disease management/gastroenterology/chronic-pancreatitis/. Accessed January 2, 2015.
39. Sadr-Azodi O, Sanders DS, Murray JA, et al. Patients with celiac disease have an increased risk of pancreatitis. Clin Gastroenterol Hepatol. 2012;10:1136-1142.
40. Etemad B, Whitcomb DC. Chronic pancreatitis: diag-nosis, classification, and new genetic developments. Gastroenterology. 2001;120(3):682-707.
41. Stinton LM, Myers RP, Shaffer EA. Epidemiology of gallstones. Gastroenterol Clin N Am. 2010;39:157-169. doi:10.1016/j.gtc.2010.02.003.
42. Shaffer EA. Epidemiology of gallbladder stone disease. Best Pract Res Clin Gastroenterol. 2006;20(6):981-996.
43. Batabyal P, Vander Hoorn S, Christophi C, Nikfarjam M. Association of diabetes mellitus and pancreatic adenocar-cinoma: a meta-analysis of 88 studies. Ann Surgic Oncol. 2014;21(7):2453-2462. doi:10.1245/s10434-014-3625-6.
44. Li D, Yeung SC, Hassan MM, et al. Antidiabetic therapies affect risk of pancreatic cancer. Gastroenterology. 2009;137 (2):482-488.
45. Jiao L, Mitrou PN, Reedy J, et al. A combined healthy lifestyle score and risk of pancreatic cancer in a large cohort study. Arch Intern Med. 2009;169:764-770.
46. Streicher SA, Yu H, Lu L, Kidd MS, Risch HA. Case-control study of aspirin use and risk of pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 2014;23(7):1254-1263. doi:10.1158/1055-9965.
47. Zeng JL, Li ZH, Wang ZC, Zhang HL. Green tea consump-tion and risk of pancreatic cancer: a meta-analysis. Nutrients. 2014;6:4640-4650. doi:10.3390/nu6114640.
48. Bhoo-Pathy N, Uitewaal CS, Dik VK, et al. Intake of coffee, decaffeinated coffee, or tea does not affect risk for pancreatic cancer: results from the European Prospective Investigation into Nutrition and Cancer Study. Clin Gastroenterol Hepatol. 2013;11(11):1486-1492. doi:10.1016/j.cgh.2013.05.029.
49. Lee ES, Lee JM. Imaging diagnosis of pancreatic cancer: a state-of-the-art review. World J Gastroenterology. 2014;20(24):7864-7877. doi:10.3748/wjg.v20.i24.7864.
50. Manfredi R, Motton M, D’Onofrio M, Graziani R, Carbognin G, Testoni M. Imaging of the pancreas. In: Sahani DV, Samir AE, eds. Abdominal Imaging. Vol 1. Maryland Heights, MO: Saunders Elsevier; 2011:691-704.
51. Catalano O, Sahani DV. Solid pancreatic masses. In: Sahani DV, Samir AE, eds. Abdominal Imaging. Vol 1. Maryland Heights, MO: Saunders Elsevier; 2011:721-746.
52. De Waele JJ. Acute pancreatitis. Curr Opin Crit Care. 2014;20:189-195. doi:10.1097/MCC.0000000000000068.
53. Banks PA, Bollen TL, Dervenis C, et al. Classification of acute pancreatitis—2012: revision of the Atlanta clas-sification and definitions by international consensus. Gut. 2013;62(1):102-111. doi:10.1136/gutjnl-2012-302779.
54. De Backer D. Abdominal compartment syndrome. Crit Care. 1999;3(6):R103-R104.

664CT
CEDirected Reading
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Computed Tomography of Pancreatitis and Pancreatic Cancer
55. Ng TS, Rochefort H, Czaplicki C, et al. Massive pancre-atic pseudocyst with portal vein fistula: case report and proposed treatment algorithm [published online ahead of print November 28, 2014]. Pancreatology. 2014;15(1):88-93. doi:10.1016/j.pan.2014.11.005.
56. Chiang KC, Chen TH, Hsu JT. Management of chronic pan-creatitis complicated with a bleeding pseudoaneurysm. World J Gastroenterol. 2014;20(43):16132-16137.
57. Rebello AS, Sahani DV. Imaging of acute pancreatitis. In: Sahani DV, Samir AE, eds. Abdominal Imaging. Vol 1. Maryland Heights, MO: Saunders Elsevier; 2011:768-780.
58. Heller SJ, Noordhoek E, Tenner SM, et al. Pleural effusion as a predictor of severity in acute pancreatitis. Pancreas. 1997;15(3):222-225.
59. Alfasser G, Rau BM, Klar E. Scoring of human acute pancre-atitis: state of the art. Langenbecks Arch Surg. 2013;398:789-797. doi:10.1007/s00423-013-1087-0.
60. Ranson JH. The timing of biliary surgery in acute pancreati-tis. Ann Surg. 1979;189:654-663.
61. Larvin M, McMahon MJ. APACHE-II score for assessment and monitoring of acute pancreatitis. Lancet. 1989;334 (8656):201-205. doi:10.1016/S0140-6736(89)90381-4.
62. Osborne DH, Imrie CW, Carter DC. Biliary surgery in the same admission for gallstone-associated acute pancreatitis. Br J Surg. 1981;68:758-761.
63. Park JY, Jeon TJ, Ha TH, et al. Bedside index for severity in acute pancreatitis: comparison with other scoring systems in predicting severity and organ failure. Hepatobil Pancreat Dis Int. 2013;12(6):645-650. doi:10.1016/S1499-3872(13)60101-0.
64. Bollen TL, Singh VK, Maurer R, et al. A comparative evalu-ation of radiologic and clinical scoring systems in the early prediction of severity in acute pancreatitis. Am J Gastroenterol. 2012;107:612-619.
65. Dellinger EP, Forsmark CE, Layer P, et al. Determinant-based classification of acute pancreatitis severity: an international multidisciplinary consultation. Ann Surg. 2012;256:875-880.
66. Karakayali FZ. Surgical and interventional management of complications caused by acute pancreatitis. World J Gastroenterol. 2014;20(37):13412-13423. doi:10.3748/wjg .v20.i37.13412.
67. Desai H, Kulkarni NM. Imaging of chronic pancreatitis. In: Sahani DV, Samir AE, eds. Abdominal Imaging. Vol 1. Maryland Heights, MO: Saunders Elsevier; 2011:781-791.
68. Guda NM, Freeman ML, Smith C. Role of extracorporeal shock wave lithotripsy in the treatment of pancreatic stones. Rev Gastroenterol Disord. 2005;5(2):73-81.
69. Kim YH, Jang SI, Rhee K, Lee DK. Endoscopic treatment of pancreatic calculi. Clin Endosc. 2014;47(3):227-235. doi:10.5946/ce.2014.47.3.227.
70. Darren DD, Brennan MB, Zamboni GA, Raptopoulos VD, Kruskal JB. Comprehensive preoperative assessment of pan-creatic adenocarcinoma with 64-section volumetric CT. Radiographics. 2007;27:1653-1666. doi:10.1148/rg.276 075034.
71. Padilla-Thornton AE, Willman JK, Jeffrey RB. Adenocarcinoma of the uncinated process of the pancreas: MDCT patterns of local invasion and clinical features at presentation. Eur Radiol. 2012;22:1067-1074. doi:10.1007 /s00330-011-2339-4.
72. National Comprehensive Cancer Network. Pancreatic adeno-carcinoma. Version I.2015. http://www.nccn.org/profession als/physician_gls/pdf/pancreatic.pdf. Accessed January 20, 2015.
73. Valsecchi ME, Díaz-Cantón E, de la Vega M, Littman SJ. Recent treatment advances and novel therapies in pancreas cancer: a review. J Gastrointest Canc. 2014;45:190-201. doi:10.1007/s12029-013-9561-z.
74. James TA, Gibbs JF. Pancreatic cancer screening: identifying premalignant disease. Future Oncol. 2005;1:191-195.
665CTRADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Directed Reading Quiz
continued on next page
Computed Tomography of Pancreatitis and Pancreatic Cancer
1. Which of the following statements regarding the pancreas is false?a. The pancreas helps regulate blood glucose levels.b. The pancreas was first tentatively identified by
the ancient Egyptians.c. The pancreas is essentially a glandular network
of ducts.d. The pancreas is heavily vascularized.
2. The pancreatic blood supply comes from branches of all of the following arteries except the ______ artery. a. femoralb. mesentericc. celiacd. splenic
3. The main pancreatic duct passes through which regions of the pancreas?
1. head2. body3. tail
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
4. The pancreas’ endocrine tissues are particularly common in which pancreatic region?a. body b. headc. taild. uncinate process
Read the preceding Directed Reading and choose the answer that is most correct based on the article.
Renewed through Sep. 1, 2020*
To earn continuing education credit: Take this Directed Reading quiz online at asrt.org/drquiz. Or, transfer your responses to the answer sheet on Page 670CT and mail to:
Processing Center, 2908 Stewart Creek Blvd., Charlotte, NC 28216.
New and rejoining members are ineligible to take DRs from journal issues published prior to their most recent join date unless they have purchased access to the quiz from the ASRT. To purchase access to other quizzes, go to asrt.org/store.
* Your answer sheet for this Directed Reading must be received in the ASRT office on or before this date. Some quizzes are renewed and the expiration date extended. Check online at asrt.org/drquiz or call Member Services at 800-444-2778.
15804-02 2.0 Category A+ credits Original Expiration Date: Aug. 31, 2017*Approved by MDCB.Check MDCB.org for details.
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Directed Reading Quiz
continued on next page
666
5. Type 2 diabetes appears to increase the risk of which of the following?
1. acute pancreatitis2. chronic pancreatitis3. pancreatic cancer
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
6. Which of the following is associated with calculi obstruction and undrained obstruction of the ducts or the major papilla?
1. pancreatitis2. jaundice3. fever
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
7. Which of the following can cause acute pancreatitis?1. pancreatic divisum2. heavy alcohol consumption3. mumps
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
8. A necrotic infection or septic phase usually emerges in how many weeks after onset of severe acute pancreatitis?a. 1b. 2c. 3d. 4
9. Metabolic insults to pancreatic tissues, particularly in the presence of certain genetic polymorphisms (gene variants), can disrupt ______ mechanisms and trigger early activation of enzymes.a. amylaseb. trypsinc. insulind. KRAS
10. Metaplastic pancreatic ducts are associated with pancreatic cancer but not with pancreatitis.a. true b. false
11. Pancreatic adenocarcinomas arise in the organ’s: a. islet cells.b. ducts.c. tail.d. uncinate process.
12. Ductal pancreatic adenocarcinoma and ______ carcinoma together make up nearly all of the pancreatic malignancies newly diagnosed each year.a. acinar cellb. neuroendocrinec. adenosquamousd. mucinous
13. Neuroendocrine tumors sometimes result from the multiple endocrine neoplasia type-1 (MEN-1) syndrome, which is inherited and also is associated with cancers of the:a. thyroid. b. pituitary.c. adrenals.d. tonsils.
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Directed Reading Quiz
continued on next page
667
14. Under conditions of continued or repeated inflammation and high levels of ______ activity, cystic lesions become increasing dysplastic.a. amylaseb. trypsinc. insulind. mutated KRAS gene
15. ______ people suffer a lower rate of calculi but higher rates of pancreatic disease overall.a. African Americanb. Whitec. Mexican Americand. Asian American
16. Which of the following gene polymorphisms might increase the risk of progression from acute to chronic pancreatitis?
1. CFTR2. PRSS13. SPINK1
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
17. Which of the following appears to reduce the risk of pancreatic cancer?a. coffeeb. green teac. fruitd. aspirin
18. Which imaging modality is superior to multidetector computed tomography (MDCT) in detection of pancreatic tumor recurrence after surgery?a. positron emission tomography (PET)-CT
functional imaging with 18-fluorodeoxyglucose b. single-photon emission computed tomography
(SPECT)c. magnetic resonance (MR) imagingd. transabdominal ultrasonography (US)
19. Total iodine administration for contrast-enhanced computed tomography (CECT) should not exceed ______ g, regardless of concentration or injection rate.a. 25b. 35c. 45d. 55
20. Which imaging modalities’ findings are included in the revised Atlanta classification system’s diagnostic criteria to confirm acute pancreatitis?
1. CECT2. PET-CT3. transabdominal US
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
21. ______ commonly occur(s) in severe acute pancreatitis and can lead to hemorrhage and intestinal obstruction.a. Intra-abdominal hypertensionb. Biliary duct rupturec. Pseudocystsd. Pleural effusion
RADIOLOGIC TECHNOLOGY, July/August 2015, Volume 86, Number 6
Directed Reading Quiz
668
27. Pancreatic necrosis should be managed with ______ if possible.a. surgeryb. percutaneous drainagec. prophylactic antibioticsd. fluid resuscitation
28. ______ appear to result from downstream duct obstructions and are evidenced by upstream ductal dilatation. a. Aneurysmsb. Pancreatic intraepithelial neoplasms c. Pseudocystsd. Fistulas
29. To which of the following does pancreatic adenocarcinoma typically metastasize?
1. liver2. brain3. lungs
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
30. In approximately ______% of tumors, pancreatic adenocarcinomas are isoattenuating with surrounding nonmalignant pancreatic tissue.a. 10b. 20c. 30d. 40
22. On pancreatic CECT images, healthy pancreas tissue exhibits CT enhancement values of 100 HU to ______ HU.a. 120b. 130c. 140d. 150
23. Pleural effusion on ______ can predict a patient’s eventual diagnosis with severe acute pancreatitis.a. a plain chest radiographb. MR imagingc. MDCTd. SPECT
24. A Computed Tomography Severity Index (CTSI) score higher than ______ is associated with an increased risk of surgical necrosectomy.a. 2b. 3c. 4d. 5
25. ______ categories describe the severity of acute pancreatitis.
1. Acute Physiology and Chronic Health Evaluation (APACHE-II)
2. TIGAR-O3. CTSI
a. 1 and 2b. 1 and 3c. 2 and 3d. 1, 2, and 3
26. Some clinical severity assessment instruments have been modified from their original forms to address the recently recognized prognostic significance of: a. infection status.b. ethnicity.c. organ dysfunction outside of the pancreas.d. C-reactive protein.