CDX2 Polymorphisms, RNA Expression, And Risk
5
CDX2 Polymorphisms, RNA Expression, and Risk of Colorectal Cancer Laura S. Rozek, 1,5 Steven M. Lipkin, 7 Eric R. Fearon, 1,2,3 Samir Hanash, 4 Thomas J. Giordano, 3 Joel K. Greenson, 3 Rork Kuick, 4 David E. Misek, 4 Jeremy M.G. Taylor, 6 Julie A. Douglas, 2 Gad Rennert, 8,9 and Stephen B. Gruber 1,2,5 Departments of 1 Internal Medicine, 2 Human Genetics, 3 Pathology, and 4 Pediatrics, University of Michigan Medical School; Departments of 5 Epidemiology and 6 Biostatistics, University of Michigan School of Public Health, Ann Arbor, Michigan; 7 Division of Hematology-Oncology, Department of Medicine, University of California, Irvine, California; 8 Department of Community Medicine and Epidemiology, Carmel Medical Center and Technion Faculty of Medicine; and 9 CHS National Cancer Control Center, Haifa, Israel Abstract In adult mammals, CDX2 acts as a transcription factor and is expressed in intestinal epithelial cells. Down-regulation of CDX2 is frequently observed in colorectal cancer, suggesting its loss may cause dedifferentiation of gastrointestinal epithelial cells. However, it is not clear whether inherited variants of CDX2 are associated with risk of colorectal cancer. Using epidemiologic data and tumors from a population- based case-control study in Israel, we identified novel single nucleotide polymorphisms (SNPs) by resequencing 35 cases, compared genotype and haplotype frequencies in 455 matched pairs, and characterized the tumor characteristics of all 455 cases by microsatellite instability analysis, in addition to a partially overlapping set of 201 frozen tumors with expression profiling data (82/201) from the same study. Nine poly- morphisms were identified in the 35 cases, and none of the SNPs or haplotypes were associated with risk of colorectal cancer in the 455 matched pairs. These variants were not associated with CDX2 expression in the 83 subjects with expression data. We evaluated subject and tumor character- istics in the 201 subjects with CDX2 tumor expression data. Reduced CDX2 expression was associated with tumor location (right sided), poor differentiation, high microsatellite insta- bility status, and a positive first-degree family history. We conclude that it is unlikely that common CDX2 variants account for a measurable fraction of susceptibility to colorectal cancer in this population. However, CDX2 expres- sion levels were strongly associated with microsatellite instability and tumor location in the gastrointestinal tract, consistent with a possible role in the specification of gastrointestinal epithelial cell fate in humans. (Cancer Res 2005; 65(13): 5488-92) Introduction Colorectal carcinogenesis is defined by a complex multistep process that involves genetic, epigenetic, and environmental factors (1). Despite the identification of several important genes and the 2-fold increase in risk of colorectal cancer in first-degree relatives of colorectal cancer patients, the genetic basis of the majority of sporadic colorectal cancers is unknown. A candidate gene for colorectal cancer is the caudal-type homeobox gene CDX2 (13q12-13), which is exclusively expressed in adults in intestinal epithelium cells and plays an important role in epithelial cell proliferation, differentiation, and determination of cell fate in different organs along the lower gastrointestinal tract (2, 3). There are multiple lines of evidence that implicate CDX2 in colorectal carcinogenesis. Whereas mouse Cdx2 homozygote null mutants die between 3.5 and 5.5 days post coitum, mice heterozygous for Cdx2 null mutations have a variable phenotype including the develop- ment of multiple intestinal adenomatous polyps in the proximal colon, some of which contain areas of true neoplasia (4). CDX2 expression is reduced in colorectal cancers from rats and humans (5–7) and may define a distinct set of minimally differentiated colorectal cancers (7). A few studies have evaluated somatic and germ line variants in CDX2 . No pathogenic mutations of CDX2 were found in 49 colorectal cancer cell lines (8) or in 51 sporadic colorectal cancer tumors (9). Single nucleotide polymorphism (SNP) discovery in the Sivagnanasundaram study (9) identified six polymorphisms in 51 sporadic British colorectal cancer cases (47 Caucasian, 4 Asian). The frequency of these polymorphisms did not differ between these cases and 60 unrelated Centre d’Etude du Polymorphisme Humain controls and 50 unrelated British controls. However, there has been no thorough evaluation of population risk associated with germ line CDX2 variants in a population-based case-control study. Here, we did SNP discovery in 35 Ashkenazi Jewish colorectal cancer subjects with a family history of colorectal cancer and typed the discovery variants in 455 matched Ashkenazi Jewish cases and controls. We considered both allelic and haplotype associations with colorectal cancer in these subjects, as haplotype analysis may be useful for detecting putative variants in this founder population. CDX2 expression was evaluated with respect to the SNPs and histopathologic characteristics of the tumors in a subset of the colorectal cancer subjects. Subjects and Methods Subjects. The Molecular Epidemiology of Colorectal Cancer study is a population-based, matched case-control study that includes 1,947 incident colorectal cancer cases and 1,947 matched controls. A sequentially selected subset of the first 455 Ashkenazi Jewish cases and 455 Ashkenazi Jewish population-based controls were used for these analyses, as power calculations indicated that we had 86.3% power to detect an odds ratio of 1.5 using the same test set of cases and controls we used for a previous analysis (10). The Molecular Epidemiology of Colorectal Cancer study participants have previously been described (10, 11). Eligible cases include any person newly diagnosed with colorectal cancer between March 31, 1998 and April 1, 2004 in Northern Israel. Cases were identified through rapid case ascertainment in the hospitals and Kupat Holim Clalit National Center for Requests for reprints: Stephen B. Gruber, Division of Molecular Medicine and Genetics, University of Michigan, 4301 MSRB III, Box 0638, 1150 West Medical Center Drive, Ann Arbor, MI 48109-0638. Phone: 734-615-9712; Fax: 734-763-7672; E-mail: [email protected]. I2005 American Association for Cancer Research. Cancer Res 2005; 65: (13). July 1, 2005 5488 www.aacrjournals.org Priority Report
-
Upload
franciscrick69 -
Category
Documents
-
view
228 -
download
3
Transcript of CDX2 Polymorphisms, RNA Expression, And Risk

CDX2 Polymorphisms, RNA Expression, and Risk
of Colorectal Cancer
Laura S. Rozek,1,5Steven M. Lipkin,
7Eric R. Fearon,
1,2,3Samir Hanash,
4
Thomas J. Giordano,3Joel K. Greenson,
3Rork Kuick,
4David E. Misek,
4
Jeremy M.G. Taylor,6Julie A. Douglas,
2Gad Rennert,
8,9and Stephen B. Gruber
1,2,5
Departments of 1Internal Medicine, 2Human Genetics, 3Pathology, and 4Pediatrics, University of Michigan Medical School;Departments of 5Epidemiology and 6Biostatistics, University of Michigan School of Public Health, Ann Arbor, Michigan; 7Division ofHematology-Oncology, Department of Medicine, University of California, Irvine, California; 8Department of Community Medicine andEpidemiology, Carmel Medical Center and Technion Faculty of Medicine; and 9CHS National Cancer Control Center, Haifa, Israel
Abstract
In adult mammals, CDX2 acts as a transcription factor and isexpressed in intestinal epithelial cells. Down-regulation ofCDX2 is frequently observed in colorectal cancer, suggestingits loss may cause dedifferentiation of gastrointestinalepithelial cells. However, it is not clear whether inheritedvariants of CDX2 are associated with risk of colorectal cancer.Using epidemiologic data and tumors from a population-based case-control study in Israel, we identified novel singlenucleotide polymorphisms (SNPs) by resequencing 35 cases,compared genotype and haplotype frequencies in 455 matchedpairs, and characterized the tumor characteristics of all 455cases by microsatellite instability analysis, in addition to apartially overlapping set of 201 frozen tumors with expressionprofiling data (82/201) from the same study. Nine poly-morphisms were identified in the 35 cases, and none of theSNPs or haplotypes were associated with risk of colorectalcancer in the 455 matched pairs. These variants were notassociated with CDX2 expression in the 83 subjects withexpression data. We evaluated subject and tumor character-istics in the 201 subjects with CDX2 tumor expression data.Reduced CDX2 expression was associated with tumor location(right sided), poor differentiation, high microsatellite insta-bility status, and a positive first-degree family history. Weconclude that it is unlikely that common CDX2 variantsaccount for a measurable fraction of susceptibility tocolorectal cancer in this population. However, CDX2 expres-sion levels were strongly associated with microsatelliteinstability and tumor location in the gastrointestinal tract,consistent with a possible role in the specification ofgastrointestinal epithelial cell fate in humans. (Cancer Res2005; 65(13): 5488-92)
Introduction
Colorectal carcinogenesis is defined by a complex multistepprocess that involves genetic, epigenetic, and environmentalfactors (1). Despite the identification of several important genesand the 2-fold increase in risk of colorectal cancer in first-degreerelatives of colorectal cancer patients, the genetic basis of themajority of sporadic colorectal cancers is unknown. A candidate
gene for colorectal cancer is the caudal-type homeobox gene CDX2(13q12-13), which is exclusively expressed in adults in intestinalepithelium cells and plays an important role in epithelial cellproliferation, differentiation, and determination of cell fate indifferent organs along the lower gastrointestinal tract (2, 3). Thereare multiple lines of evidence that implicate CDX2 in colorectalcarcinogenesis. Whereas mouse Cdx2 homozygote null mutants diebetween 3.5 and 5.5 days post coitum, mice heterozygous for Cdx2null mutations have a variable phenotype including the develop-ment of multiple intestinal adenomatous polyps in the proximalcolon, some of which contain areas of true neoplasia (4). CDX2expression is reduced in colorectal cancers from rats and humans(5–7) and may define a distinct set of minimally differentiatedcolorectal cancers (7). A few studies have evaluated somatic andgerm line variants in CDX2 . No pathogenic mutations of CDX2were found in 49 colorectal cancer cell lines (8) or in 51 sporadiccolorectal cancer tumors (9). Single nucleotide polymorphism(SNP) discovery in the Sivagnanasundaram study (9) identified sixpolymorphisms in 51 sporadic British colorectal cancer cases(47 Caucasian, 4 Asian). The frequency of these polymorphisms didnot differ between these cases and 60 unrelated Centre d’Etude duPolymorphisme Humain controls and 50 unrelated British controls.However, there has been no thorough evaluation of population riskassociated with germ line CDX2 variants in a population-basedcase-control study. Here, we did SNP discovery in 35 AshkenaziJewish colorectal cancer subjects with a family history of colorectalcancer and typed the discovery variants in 455 matched AshkenaziJewish cases and controls. We considered both allelic andhaplotype associations with colorectal cancer in these subjects,as haplotype analysis may be useful for detecting putative variantsin this founder population. CDX2 expression was evaluated withrespect to the SNPs and histopathologic characteristics of thetumors in a subset of the colorectal cancer subjects.
Subjects and Methods
Subjects. The Molecular Epidemiology of Colorectal Cancer study is a
population-based, matched case-control study that includes 1,947 incident
colorectal cancer cases and 1,947 matched controls. A sequentially selectedsubset of the first 455 Ashkenazi Jewish cases and 455 Ashkenazi Jewish
population-based controls were used for these analyses, as power
calculations indicated that we had 86.3% power to detect an odds ratio of1.5 using the same test set of cases and controls we used for a previous
analysis (10). The Molecular Epidemiology of Colorectal Cancer study
participants have previously been described (10, 11). Eligible cases include
any person newly diagnosed with colorectal cancer between March 31, 1998
and April 1, 2004 in Northern Israel. Cases were identified through rapid case
ascertainment in the hospitals and Kupat Holim Clalit National Center for
Requests for reprints: Stephen B. Gruber, Division of Molecular Medicine andGenetics, University of Michigan, 4301 MSRB III, Box 0638, 1150 West Medical CenterDrive, Ann Arbor, MI 48109-0638. Phone: 734-615-9712; Fax: 734-763-7672; E-mail:[email protected].
I2005 American Association for Cancer Research.
Cancer Res 2005; 65: (13). July 1, 2005 5488 www.aacrjournals.org
Priority Report

Cancer Control tumor registry by International Classification of Diseases
code for cancer of the colon or rectum and were invited to participate and
interviewed. Potential controls were matched for exact year of birth, sex, and
primary-care clinic code. Structured interviews assessed demographic
information, personal and family history of cancer, reproductive history
and medical history, medication use, health habits, and a food-frequency
questionnaire. Individuals previously diagnosed with cancer of the color-
ectum were not eligible to participate. Overall, 3,181 potentially eligible cases
of colorectal cancer were ascertained in the study period before this analysis.
Of them, 618 (19.4%) could not be located or approached, including 275
(8.6%) who died before being approached. Thus 2,563 were approached and
invited to participate. Forty-two were subsequently excluded as too sick to
participate or unable to communicate in Hebrew, Russian, Arabic, or
English. Of the 2,521 remaining eligible cases, 335 declined to participate
(13.3%). Therefore, 2,186 cases were eligible and consented, and 2,146
completed the in-person interview, which corresponds to a response rate of
67% of all eligible cases. In addition, 2,162 consented matched controls were
interviewed. Among the matched controls who were first approached, 52.1%
participated in the study. The study was approved by the Institutional
Review Boards at the University of Michigan and Carmel Medical Center in
Haifa. Written informed consent was required for eligibility.
Study design. The SNP study was done in two stages: SNP discovery and
SNP screening. SNP discovery was done on 35 Molecular Epidemiology of
Colorectal Cancer colorectal cancer patients with at least one first-degree
relative with a history of colorectal cancer through resequencing of all exons
and overlapping intron boundaries. All variant alleles identified in the SNP
discovery stage were screened in the matched sample of 455 Ashkenazi cases
and 455 Ashkenazi controls. A partially overlapping set of 201 frozen tumors
with expression profiling data from the same study permitted joint
evaluation of CDX2 expression and CDX2 SNPs for 82 Molecular
Epidemiology of Colorectal Cancer cases.
Single nucleotide polymorphism genotyping. SNP genotyping was
done using Masscode Technology (Qiagen GmbH, Valencia, CA), which uses
highly multiplexed detection of low molecular weight photocleavable Mass
Tags in a single quadrupole mass spectrometer. Briefly, the assay used a
two-step PCR process for signal amplification and SNP discrimination.
Allele-specific incorporation of the Mass Tags occurs during the second
amplification step as previously described (12). SNP assays were carried out
using 4 ng of genomic DNA. Positive and negative (no DNA) controls were
included on every 96-well plate analyzed.
Microsatellite instability analyses. Microsatellite instability (MSI)
analyses were done as previously described (13). Normal and tumor DNA
were extracted from microdissected DNA and analyzed for the consensus
panel of five markers (14). Briefly, forward primers for BAT25, BAT26,
D2S123, and D5S346 and reverse primers for D17S250 were labeled with
[g-32P]ATP, and included in a 20 AL PCR reaction that included 1 AL of
microdissected DNA. PCR products were run on 6% polyacrylamide gels for
f3 hours at 65 W, and exposed to film at �80jC for 12 to 20 hours. Films
were double scored and entered as stable, unstable, or loss of
heterozygosity. Tumors were designated as MSI-high if there was instability
at two or more markers. For uninformative markers, a sixth marker from
the consensus panel was substituted.
CDX2 RNA expression. Primary tumors for expression analysis wereobtained at the time of surgical resection and snap frozen, embedded in
optimum cutting temperature freezing media (Miles Scientific, Naperville, IL),
cryotome sectioned, stained with H&E, and evaluated by a single surgical
pathologist (T.J.G.) as previously described (15). Areas with >70% tumorcellularity were identified for RNA isolation. Selected sections of tumor
samples were homogenized in Trizol (Life Technologies, Gaithersburg, MD),
and total cellular RNA was purified according the instructions of themanufacturer, with additional purification using RNeasy spin columns
(Qiagen). RNA quality was assessed by 1% agarose gel electrophoresis, and
samples were included only if the 18S and 28S bands were discrete and
approximately equal.
Expression levels were measured using commercially available Affymetrix
high-density microarrays (Affymetrix, Santa Clara, CA), with sample
preparation of cRNA, hybridization, and scanning all done according tothe protocols of the manufacturer. Tumors were evaluated on either
HuGeneFL or U133 chips.
Statistical analyses. Matched univariate analyses were done on eachindividual SNP using conditional logistic regression as implemented in SAS
version 8.2 (SAS Institute, Cary, NC, 1999). Each SNP was analyzed using
both additive and dominant models. T tests, ANOVA, and generalized linearmodels as implemented in SAS were used to compare the distribution of
CDX2 expression between subjects with and without a minor allele, and
with and without histopathologic characteristics. PHASE version 2.0.1 (16)
was used to infer haplotypes for individual subjects. Linkage disequilibriumbetween SNP pairs was calculated as DV and D2 using the GOLD program
(17). Haplotypes were also inferred using the EM algorithm, and
associations between haplotypes and colorectal cancer and CDX2
expression were determined using the haplo_score program in Splus (18).Family history of colorectal cancer was self-reported and coded as
‘‘colorectal cancer reported in any first-degree relative’’ or ‘‘colorectal
cancer reported in any relative.’’
Expression analysis was done as previously described (15). In brief, we
subtracted the mismatch probe values from the perfect match values andaveraged the middle 50% of these differences as the expression measure for
the CDX2 probe set. The data were quantile normalized to adjust for
intensity differences across chips. A monotone linear spline was applied to
each chip that mapped quantiles 0.02 up to 0.98 (in increments of 0.02)exactly to the corresponding median quartiles for all samples. The data
were then transformed for each chip, using log(100 + max(X + 100;0)).
Results and Discussion
Nine unique SNPs were identified in the 35 colorectal cancercases with a first-degree family history of colorectal cancer. Incomparison to the Sivagnanasundaram study which also looked atall exon/intron boundaries of CDX2 , the majority of the SNPsidentified were in the intronic regions: eight in noncoding regionsand one in exon 3 (Table 1). The T877C change results in serine(uncharged polar) to proline (nonpolar) substitution in exon 3.Two of the SNPs, IVS1 �33T>A and IVS1 �34T>C, are very simi-lar to polymorphisms described in the Sivagnanasundaram et al.study (IVS1 �31A>T, IVS1 �32C>T). Although it is not possible torecognize whether these polymorphisms represent the exact samepolymorphisms previously reported by Sivagnanasundaram fromthe published report, this possibility seems highly likely. The data
Table 1. SNP allele frequencies in controls and associa-tion with colorectal cancer in 455 matched pairs
SNP Control
minor allele
frequency
Odds ratio
(95% confidence
interval)
IVS1 +1020C!A 0.177 1.02 (0.76-1.40)
IVS1 +1476A!G 0.181 0.94 (0.70-1.25)IVS1 �1575T!G 0.448 0.98 (0.67-1.20)IVS1 �1042C!G 0.175 1.06 (0.79-1.42)
IVS1 �34T!C 0.266 0.99 (0.75-1.30)IVS1 �33T!A 0.184 1.04 (0.78-1.39)IVS2 �429C!A 0.176 1.05 (0.78 – 1.40)
T877C exon 3 0.170 1.03 (0.73-1.45)3V Untranslated region+10G!C
0.176 0.98 (0.73-1.31)
NOTE: Tag SNPs are in boldface.
CDX2 Variants and Expression in Colorectal Cancer
www.aacrjournals.org 5489 Cancer Res 2005; 65: (13). July 1, 2005

we report here find no evidence of a significant association withcolorectal cancer for these two polymorphisms, and thisinterpretation is entirely consistent with the conclusions drawnby Sivagnanasundaram et al. None of the other SNPs wereidentified in previous studies, which is likely due to populationdifferences between Ashkenazi Jews and the other groups studied.All identified SNPs were typed in the screening population of 455matched cases and controls. The observed genotype data wereconsistent with Hardy-Weinberg equilibrium as measured incontrol subjects. The mean age was similar between cases andcontrols by design, where the mean age of cases was 73.7 (SD =9.7) versus 74.4 (SD = 9.7) for controls. Slightly more than half(55.6% of cases and 55.1% of controls) of the subjects were male.The SNPs were highly frequent, with the least frequent minorallele found in 17% of the subjects (Table 1). All SNPs were seenequally frequently in cases and controls. Odds ratios for theseSNP associations with colorectal cancer from matched analysesranged from 0.94 to 1.06 (modeling presence or absence of theminor allele and risk of colorectal cancer), indicating that none ofthese SNPs were associated with risk of colorectal cancer in thispopulation. This result did not change when modeling an additivegenetic model and risk of colorectal cancer (data not shown).Although there were no putative SNP-colorectal cancer associ-
ations, we also tested whether haplotypes were associated withcolorectal cancer. Specifically, we evaluated haplotypes of SNPs byincluding only a single SNP from any set of associated SNPs,defined as D2 > 0.90. The SNPs in this gene were in strong linkagedisequilibrium, implying that there was very little historicalrecombination in this gene in the Ashkenazi Jewish population(DV = 1 for 27 of the 36 pairs of SNPs). IVS1 �1575 and IVS1 �34had pairwise measures of D2 ranging from 0.059 to 0.423 with eachof the other SNPs and each other, and T877C exon 3 had measuresof D2 of 0.250 and 0.082 with IVS1 �1575 and IVS1 �34,respectively, and a minimum D2 of 0.955 with each of theremaining SNPs. The remaining six SNPs were in very stronglinkage disequilibrium with each other (D2 > 0.91). The PHASEprogram inferred three common haplotypes of the nine SNPs withrelative frequencies of 55%, 25%, and 17% (Table 2). The three SNPseffectively distinguish or tag these three haplotypes, which accountfor 97% of the predicted haplotypes in our sample. Score statisticswere used to compare haplotype frequencies between cases andcontrols for all combinations of these three SNPs to determine ifthere was any association between haplotypes and colorectalcancer. Although there were a limited number of significantdifferences in haplotype frequencies between cases and controls,
there were no discernable patterns and these differences werelikely due to chance (data not shown).It is possible that variants in CDX2 that are not associated with
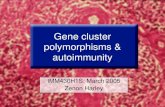
an increased risk of colorectal cancer may have a functional effecton CDX2 expression. Global gene expression derived from micro-arrays of CDX2 correlates well with CDX2 protein expression (19).We analyzed these variants with respect to differences in CDX2expression in an overlapping subset of 82 colorectal cancer casesubjects with both expression and CDX2 variant data available.None of the SNPs or derived haplotypes of the three tag SNPspredicted significant differences in CDX2 expression in thesesubjects. Previously, Hinoi et al. (7) reported reduced CDX2expression in large-cell minimally differentiated carcinomas, whichare predominantly right sided. Data on specific tumor location wasavailable for 65 of the 82 colorectal cancer cases with expressiondata, 28 of which were left-sided and 37 right-sided tumors.Right-sided tumors showed significantly lower mean CDX2expression (27% decrease, P = 0.018) than left-sided tumors. Inaddition, the larger data set of 201 tumors with CDX2 expressiondata (only 82 of which were genotyped for CDX2 variants) wereanalyzed to evaluate the expression with respect to histopathologiccharacteristics. These analyses show that CDX2 is underexpressedin right-sided, poorly differentiated tumors, consistent withprevious reports (Table 3). It is clear that, whereas overall levelsseem to be highest in the sigmoid colon, rectosigmoid junction,and rectum, some tumors in these areas have low expression levelscomparable to those found in the cecum and other right-sidedareas (Fig. 1A and B). As an expected consequence of tumorheterogeneity, a small number of right-sided tumors have highexpression levels, with low levels of expression found in some left-sided tumors.Twelve (6.0%) of the 199 cases with both CDX2 expression data
and family history data from Molecular Epidemiology ofColorectal Cancer interviews reported a first-degree relative witha history of colorectal cancer, and these subjects had significantlylower CDX2 expression (817.1 versus 1,283.6, P = 0.019; Table 2).
Table 2. Reconstructed haplotypes z1% for nine SNPs,all subjects (n = 910)
Haplotype Relative frequency
C-G-T-C-C-T-C-T-G 0.55
C-G-T-C-T-T-A-T-G 0.25A-A-G-G-C-A-A-C-C 0.17
C-G-T-G-C-T-A-T-G 0.01
C-G-T-C-C-T-A-T-G 0.01
NOTE: Tag SNPs are in boldface. These three SNPs distinguish the first
three haplotypes, which account for 97% of all predicted haplotypes.
Table 3. CDX2 expression by tumor characteristics (allsamples)
n Mean SD P
Location
Right 100 1,116.6 616.9
Left 97 1,395.0 691.5 0.003Grade
Poor 17 979.6 623.4
Moderate 144 1,319.3 658.7
Well 18 1,299.9 615.1 0.129Stage
A 7 1,245.3 461.0
B 116 1,261.3 655.8
C 77 1,251.8 713.2 0.99MSI status
MSI-high 28 737.5 491.7
Microsatellite stable 134 1,343.6 652.7 <0.001
Family historyFirst-degree family history 12 817.1 744.9
No first-degree family history 187 1,283.6 656.2 0.019
Any relative 18 1,008.4 760.1No family history 181 1,280.0 656.7 0.101
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5490 www.aacrjournals.org

Figure 1. Relative CDX2 expression levels by location (A and B ) and microsatellite instability status (C ).
CDX2 Variants and Expression in Colorectal Cancer
www.aacrjournals.org 5491 Cancer Res 2005; 65: (13). July 1, 2005

The 18 (9.0%) subjects who reported any relative with a familyhistory of colorectal cancer had lower CDX2 expression thanthose who did not report a relative with colorectal cancer (1,008.4versus 1,280.0), but this result was not statistically significant (P =0.101; Table 2).Microsatellite unstable (MSI) tumors have significantly lower
expression than microsatellite stable tumors (737.5 versus 1,343.6,P < 0.001; Table 2; Fig. 1C), which is consistent with the Hinoi et al.study that reported a high frequency of the MSI phenotype (60%) in alimited panel of tumors with reduced CDX2 expression (7). In amultivariatemodel that included bothMSI status and tumor location,MSI status is more strongly associated with CDX2 expression (P <0.001) than location (P = 0.192), suggesting loss of CDX2 expressionthrough somatic alterations in MSI-high tumors.The nature and implications of CDX2 alterations in colorectal
cancer are not clearly defined. Here, we investigated germ linevariants found in colorectal cancer cases with a family history ofcolorectal cancer to determine if these are associated withsusceptibility to sporadic colorectal cancer in this population.However, no variants or combination of variants were associatedwith risk of colorectal cancer in this population. Furthermore, wedid not identify any germ line variants that predicted CDX2expression levels, but confirmed the previously described patternsof CDX2 expression observed in poorly differentiated, right-sidedtumors. However, reduced CDX2 expression is not limited toright-sided tumors, and further molecular studies are needed to
clarify the nature and extent of CDX2 alterations in colorectaltumorigenesis. We provide additional evidence here that MSIstatus may be more strongly associated with CDX2 expressionthan tumor location. Hinoi et al. (20) propose a dominantrepressor pathway, where reduced or absent CDX2 expression inMSI tumors is due to repression of a transcription factor orprotein required for CDX2 expression commonly altered in MSIcolorectal cancers. This same study showed that demethylatingagents were not sufficient to reactivate CDX2 expression, showingthat CDX2 is unlikely, in these colorectal cancers, to be silencedby methylation. Here, we show that it is also unlikely that germline variants play a role in reduced CDX2 expression in sporadiccolorectal cancers and there is little genetic diversity in CDX2 inthis population. To our knowledge, this is the only population-based study of CDX2 germ line variants published to date. Giventhe number of subjects in this study, germ line variants in CDX2are unlikely to be associated with risk of colorectal cancer in thispopulation.
Acknowledgments
Received 10/11/2004; revised 1/25/2005; accepted 3/1/2005.Grant support: A grant (1R01CA81488) from the National Cancer Institute and a
gift from the Weinstein Foundation, a non profit charitable organization.The costs of publication of this article were defrayed in part by the payment of page
charges. This article must therefore be hereby marked advertisement in accordancewith 18 U.S.C. Section 1734 solely to indicate this fact.
Cancer Research
Cancer Res 2005; 65: (13). July 1, 2005 5492 www.aacrjournals.org
References1. Vogelstein B, Kinzler KW. The multistep nature ofcancer. Trends Genet 1993;9:138–41.
2. Drummond F, Putt W, Fox M, Edwards YH. Cloningand chromosome assignment of the human CDX2 gene.Ann Hum Genet 1997;61:393–400.
3. Lorentz O, Duluc I, Arcangelis AD, Simon-Assmann P,Kedinger M, Freund JN. Key role of the Cdx2 homeoboxgene in extracellular matrix-mediated intestinal celldifferentiation. J Cell Biol 1997;139:1553–65.
4. Chawengsaksophak K, James R, Hammond VE,Kontgen F, Beck F. Homeosis and intestinal tumoursin Cdx2 mutant mice. Nature 1997;386:84–7.
5. Ee HC, Erler T, Bhathal PS, Young GP, James RJ. Cdx-2homeodomain protein expression in human and ratcolorectal adenoma and carcinoma. Am J Pathol 1995;147:586–92.
6. Mallo GV, Rechreche H, Frigerio JM, et al. Molecularcloning, sequencing and expression of the mRNAencoding human Cdx1 and Cdx2 homeobox. Down-regulation of Cdx1 and Cdx2 mRNA expression duringcolorectal carcinogenesis. Int J Cancer 1997;74:35–44.
7. Hinoi T, Tani M, Lucas PC, et al. Loss of CDX2expression and microsatellite instability are prominentfeatures of large cell minimally differentiated carcino-mas of the colon. Am J Pathol 2001;159:2239–48.
8. Woodford-Richens KL, Halford S, Rowan A, et al.CDX2 mutations do not account for juvenile poly-posis or Peutz-Jeghers syndrome and occur infre-quently in sporadic colorectal cancers. Br J Cancer2001;84:1314–6.
9. Sivagnanasundaram S, Islam I, Talbot I, Drummond F,Walters JR, Edwards YH. The homeobox gene CDX2 incolorectal carcinoma: a genetic analysis. Br J Cancer2001;84:218–25.
10. Lipkin SM, Rozek LS, Rennert G, et al. TheMLH1 D132H variant is associated with susceptibilityto sporadic colorectal cancer. Nat Genet 2004;36:694–9.
11. Niell BL, Rennert G, Bonner JD, Almog R, Tomsho LP,Gruber SB. BRCA1 and BRCA2 founder mutations andthe risk of colorectal cancer. J Natl Cancer Inst 2004;96:15–21.
12. Kokoris M, Dix K, Moynihan K, et al. High-throughput SNP genotyping with the Masscode system.Mol Diagn 2000;5:329–40.
13. Greenson JK, Bonner JD, Ben Yzhak O, et al.Phenotype of microsatellite unstable colorectal carcino-mas: well-differentiated and focally mucinous tumorsand the absence of dirty necrosis correlate withmicrosatellite instability. Am J Surg Pathol 2003;27:563–70.
14. Boland CR, Thibodeau SN, Hamilton SR, et al. A
National Cancer Institute Workshop on microsatelliteinstability for cancer detection and familial predisposi-tion: development of international criteria for thedetermination of microsatellite instability in colorectalcancer. Cancer Res 1998;58:5248–57.
15. Giordano TJ, Shedden KA, Schwartz DR, et al. Organ-specific molecular classification of primary lung, colon,and ovarian adenocarcinomas using gene expressionprofiles. Am J Pathol 2001;159:1231–8.
16. Stephens M, Smith NJ, Donnelly P. A new statisticalmethod for haplotype reconstruction from populationdata. Am J Hum Genet 2001;68:978–89.
17. Abecasis GR, Cookson WO. GOLD—graphical over-view of linkage disequilibrium. Bioinformatics 2000;16:182–3.
18. Schaid DJ, Rowland CM, Tines DE, Jacobson RM,Poland GA. Score tests for association between traitsand haplotypes when linkage phase is ambiguous. Am JHum Genet 2002;70:425–34.
19. Moskaluk CA, Zhang H, Powell SM, Cerilli LA,Hampton GM, Frierson HF Jr. Cdx2 protein expressionin normal and malignant human tissues: an immuno-histochemical survey using tissue microarrays. ModPathol 2003;16:913–9.
20. Hinoi T, Loda M, Fearon ER. Silencing of CDX2expression in colon cancer via a dominant repressionpathway. J Biol Chem 2003;278:44608–16.