Plasmablastic Extramedullary Plasmacytoma Associated with ...

1801
□ CASE REPORT □
CD3- and CD4-Positive Plasmablastic Lymphoma:A Literature Review of Japanese Plasmablastic
Lymphoma Cases
Yuhko Suzuki 1,2, Tsutomu Yoshida 3, Naoya Nakamura 6, Hirotoshi Kamata 1, Shouko Kotani 4,
Manabu Ohsaka 1, Sabine Kajita 3, Koji Miyazaki 1, Shinichi Ohtani 2, Meijin Nakayama 5,
Ryouichi Horie 1, Kazushige Hayakawa 4, Nozomi Niitsu 7 and Masaaki Higashihara 1
Abstract
Plasmablastic lymphoma (PBL) is a very rare and recently-described subtype of diffuse large B-cell lym-
phoma. A maxillary tumor in an 84-year-old HIV-negative Japanese-man was referred. The biopsied speci-
men showed a diffuse proliferation of mature plasma cells, expressing CD3 (+), CD4 (+), CD20 (-), CD138
(+) and EBER (+) by immunohistochemistry. He was diagnosed as a plasmablastic lymphoma; radiation ther-
apy (RT) was started, but the response to the RT was only a partial response. To our knowledge, this is the
first report of a patient with PBL expressing CD3 and CD4.
Key words: plasmablastic lymphoma, Japanese, CD3
(Inter Med 49: 1801-1805, 2010)(DOI: 10.2169/internalmedicine.49.3164)
Introduction
Plasmablastic lymphoma (PBL) is a recently-described
subtype of diffuse large B-cell lymphoma. It has its highest
incidence in HIV-positive individuals, predominantly males.
PBL may also be associated with other immunodeficiency
states, including advanced age and post-transplant lym-
phoproliferative disorders (1-6).
PBL is characterized by diffuse growth of large tumor
cells with a high MIB-1 proliferation index, the presence of
immunoglobulin heavy (IgH)-chain gene rearrangement, and
expression of the plasma cell-associated antigens CD38 and
CD138. Typically, PBL lacks expression of leukocyte com-
mon antigen, CD19, and CD20. Positivity for Epstein-Barr
virus (EBV)-encoded RNA (EBER) is frequently ob-
served (1).
We describe the case of PBL, which interestingly ex-
pressed CD3 and CD4, and review the literature of Japanese
cases.
Case Report
An 84-year-old Japanese man was referred to our hospital
in 2008 due to a two-month history of left face pain and
inadaptation of a denture. On physical examination, the left
paranasal area of his face was swollen and his left upper
gingiva was partially swollen with a tumor. His peripheral
blood count was within normal range. Biochemical analysis
revealed the following: C-reactive protein 2.70 mg/dL, lac-
tate dehydrogenase 167 IU/L, BUN 41 mg/dL, and cre-
atinine 2.33 mg/dL. Hypergammopathy and monoclonal
gammopathy were detected neither in urine nor in serum.
The patient was HIV negative. Even though the tumor cells
1Department of Hematology, Kitasato University School of Medicine, Sagamihara, 2Department of Transfusion and Cell Transplantation, Ki-
tasato University School of Medicine, Sagamihara, 3Department of Pathology, Kitasato University School of Medicine, Sagamihara, 4Department
of Radiology, Kitasato University School of Medicine, Sagamihara, 5Department of Otolaryngology, Kitasato University School of Medicine,
Sagamihara, 6Department of Pathology, Tokai University School of Medicine, Isehara and 7Department of Hematology, Comprehensive Cancer
Center, International Medical Center, Saitama Medical University, Hidaka
Received for publication November 19, 2009; Accepted for publication April 26, 2010
Correspondence to Dr. Yuhko Suzuki, [email protected]

Inter Med 49: 1801-1805, 2010 DOI: 10.2169/internalmedicine.49.3164
1802
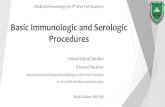
Figure 1. a. Head non-contrast-enhanced CT scan showed that the left paranasal sinus was occu-pied by a tumor and the tumor infiltrated the oral cavity. b. The tumor infiltrated the nasal cavity.
a b
expressed the T cell markers, CD3 and CD4 by IHC, results
of IgH rearrangement indicated B cell lymphoma, and the
diagnosis of PBL was established.
Computed tomography (CT) showed a soft tissue mass
that infiltrated the left nasal cavity and upper oral cavity
(Fig. 1). Bone marrow aspiration and biopsy were negative
for infiltration of lymphoma cells by light microscopy and
flow cytometry. He was Stage IIA and the international
prognostic index was low-intermediate. After informed con-
sent, the patient chose to receive involved-field radiation
therapy (RT) of 30 Gy/20 fractions and limited local field
RT of 20 Gy/10 fractions (total 50 Gy) and had a partial re-
sponse to the RT. Three months after the completion of RT,
a right chest wall tumor was newly found, suggesting lym-
phoma infiltration.
Histopathology, immunohistology, in situ hybridiza-
tion, and flow cytometry
Histopathological analysis revealed diffuse proliferation of
mature plasma cells having a round nucleus, intermingled
with large-sized cells with higher nuclear to cytoplasmic (N/
C) ratio were intermingled (Fig. 2a, b). On immunohisto-
chemistry (IHC), the tumor cells were negative for B cell
markers including CD10, CD20 (Fig. 2e), CD38, CD79a,
and PAX-5, but were positive for the T cell markers, CD3
(Fig. 2c) and CD4 (Fig. 2d). They were also positive for
plasma cell markers, CD138 (Fig. 2f) and MUM-1. As other
markers that are often used for IHC to diagnose lymphoma,
Bcl-2, CD56, and TdT were negative, but Bcl-6 was posi-
tive. The MIB-1 labeling index was high, and the tumor
cells were strongly positive on in situ hybridization with an
EBER probe (Fig. 2g). The flow cytometric study of the bi-
opsied specimen did not reflect the actual lymphoma cells.
PCR
At first, clonality analysis of IgH chain was performed
with primer recognizing not only FR2 but also FR3 region;
semi-nested PCR using FR3A and LJH for the first PCR
and FR3A and VLJH for the second PCR, as described pre-
viously (7, 8). To analyze clonality of T cell receptor βchain, multiplex PCR assays were performed, as described
previously (9).
PCR of the IgH chain showed a discrete band, indicating
IgH rearrangement (Fig. 3), but PCR of T cell receptor
(TCR) beta (V beta/J beta 1, 2, V beta/J beta 2, D beta/J
beta) showed no amplification, indicating no rearrangement.
Discussion
We reported the first Japanese patient with PBL, and it
expressed CD3 and CD4, and it arose in an 84-year-old,
HIV-negative Japanese patient. Interestingly, this case het-
erotropically expressed CD3 and CD4. The pathological
findings of the present case seemed to resemble pyothorax-
associated lymphoma (PAL), which usually arises from
chronic inflammation (10, 11). PAL is often associated with
EBV infection, and it also frequently expresses T-cell anti-
gen. However, the present patient did not have a medical
history of chronic inflammation of sinusoids. Heterotropic
expression of T-cell antigen in B-cell lymphoma is fre-
quently associated with EBV infection with or without
chronic inflammation.
Our case was interesting and difficult to diagnose because
it expressed pan-T cell antigens, CD3 and CD4, as detected
by IHC. And this case is the first report of CD3 and CD4
positive PBL. CD3 positivity by IHC is used as a pan-
T (12) and pan-thymic marker, namely, CD3-positive lym-
phoma generally means T-cell lymphoma. The monoclonal
antibody for CD3, clone F7.2.38 (DAKO), which we use,
recognizes the cytoplasmic domain of the epsilon chain, and
stained at least membrane and cytoplasm of lymphoma cells
in this case.
Several studies on aggressive CD3-positive B-cell lym-
phoma were reported (11, 13-18). PAL has peculiar clinico-
pathological features, and some cases express CD3 and
other T cell antigens (11). Aggressive CD3-positive B cell
lymphoma cases are often EBER-positive (11, 16, 17) as in
the present case. EBV may interfere with the PAX-5 gene,

Inter Med 49: 1801-1805, 2010 DOI: 10.2169/internalmedicine.49.3164
1803
Figure 2. Histological and immunohistochemical photographs of the biopsied tumor. a. Hematox-ylin and Eosin staining, original magnification×100. b. Hematoxylin and Eosin staining, original magnification×400. c. Anti-CD3 (original magnification×400). d. Anti-CD4 (original magnifica-tion×400). e. Anti-CD20 (original magnification×400). f. Anti-CD138 (original magnification×400). g. EBER (original magnification×400). Photographs show diffuse proliferation of large cells that are positive for CD3, CD4 (weak), CD138, and EBER and negative for CD20, which indicates a plasmablastic lymphoma. In figure 1-c, d, arrows indicate epithelial cells( → ) and normal T cells( ⇒ ). CD3 and CD4 are stained in the serial section, and CD3 and CD4 coexist on the same lymphoma cells. Compared to the normal T cells, positivities for CD3 and CD4 of lymphoma cells are weaker than normal T cells. And epithelial cells are negative for CD3 and CD4.
a b
c d
e f
g

Inter Med 49: 1801-1805, 2010 DOI: 10.2169/internalmedicine.49.3164
1804
Figure 3. PCR of the IgH chain. It showed a discrete band, indicating IgH rearrangement.
Table 1. PBL Cases in the Japanese Literature
NR: not reported, CRF: chronic renal failure, PNS: Paranasal sinus, PE: pleural effusion, LN: lymph node, Cx: chemotherapy, RT: radiation therapy, S: surgery
which is the master gene throughout B cell development
from pro-B to the mature B cell stage. PAX-5 expression
was negative in our case. Loss of PAX-5 may cause de-
differentiation to the immature lymphoid cell and lead to the
development of lymphoid malignancy (19, 20).
The possibility of extraosseous plasmacytoma (21) was
also considered. As a differential diagnosis, plasmacytoma is
the most difficult to distinguish from our case. EBV is not
normally harbored in normal plasma cells and neoplastic
plasma cells in immunocompetent individuals (22). Thus,
plasmacytomas do not express EBER, and therefore plasma-
cytoma was ruled out in this case. However, recently,
EBER-positive plasmacytoma was reported (22). The defini-
tion of PBL is still confusing. The clinical course of the
present case followed the typical clinical course of lym-
phoma, but not plasmacytoma.
From the results of a literature review, we found 9 Japa-
nese cases with PBL among the studies published in Japa-
nese (23-31) (Table 1). Considering these patients along
with the present patient, their ages ranged from 33 to 84
years (median, 59 years) with male dominance. As to the
background disease of PBL, only one patient (10%) was
HIV-positive. However, in Western countries the majority
(81%) of cases arise in the setting of HIV infection (6).
Prognoses were also reported in nine cases; three cases
were alive with complete response (CR) and the other six
died or had refractory cases. PBL is considered to be a
highly aggressive lymphoma and the prevalence of disease-
related death was 59.6% over a mean period of 10.4 months
from diagnosis (6, 32). Interestingly, case 9 underwent sur-
gery only but has survived without recurrence for more than
two years. The clinical course of PBL varies and standard
therapies for PBL have not yet been developed.
We reported CD3- and CD4-positive PBL arising in an
HIV-negative patient. Its clinicopathological features were
very unique. To our knowledge, this is the first report of pa-
tient with PBL expressing CD3 and CD4. We hope that,
with the accumulation of clinicopathologic data of PBL
cases, we will be able to elucidate the mechanism(s) in-
volved in the development of PBL, to confirm the most suit-
able treatment.
AcknowledgementWe would like to thank all of our colleagues, especially Mr.
Kusaba, who assisted PCR of IgH rearrangement assays.
We obtained no financial support from any company.

Inter Med 49: 1801-1805, 2010 DOI: 10.2169/internalmedicine.49.3164
1805
References
1. WHO Classification of Tumours of Haematopoietic and Lymphoid
Tissues. Swerdlow SH, Campo E, Harris NL, et al, Eds. WHO
Press, Geneva, 2008.
2. Borenstein J, Pezzella F, Gatter KC. Plasmablastic lymphomas
may occur as post-transplant lymphoproliferative disorders. Histo-
pathology 51: 774-777, 2007.
3. Scheper MA, Nikitakis NG, Fernandes R, Gocke CD, Ord RA,
Sauk JJ. Oral plasmablastic lymphoma in an HIV-negative patient:
a case report and review of the literature. Oral Surg Oral Med
Oral Pathol Oral Radiol Endod 100: 198-206, 2005.
4. Castillo J, Pantanowitz L, Dezube BJ. HIV-associated plasmablas-
tic lymphoma: lessons learned from 112 published cases. Am J
Hematol 83: 804-809, 2008.
5. Colomo L, Loong F, Rives S, et al. Diffuse large B-cell lympho-
mas with plasmablastic differentiation represent a heterogeneous
group of disease entities. Am J Surg Pathol 28: 736-747, 2004.
6. Rafaniello Raviele P, Pruneri G, Maiorano E. Plasmablastic lym-
phoma: a review. Oral Dis 15: 38-45, 2009.
7. Wan JH, Trainor KJ, Brisco MJ, Morley AA. Monoclonality in B
cell lymphoma detected in paraffin wax embedded sections using
the polymerase chain reaction. J Clin Pathol 43: 888-890, 1990.
8. Yamashita K, Tatebayashi T, Shinoda H, Okayasu I. Simplified
rapid non-radioactive PCR-SSCP method applied to K-ras muta-
tion analysis. Pathol Int 46: 801-804, 1996.
9. van Dongen JJ, Langerak AW, Bruggemann M, et al. Design and
standardization of PCR primers and protocols for detection of
clonal-immunoglobulin and T-cell receptor gene recombinations in
suspect lymphoproliferations: report of the BIOMED-2 Concerted
Action BMH4-CT98-3936. Leukemia 17: 2257-2317, 2003.
10. Aozasa K. Pyothorax-associated lymphoma. J Clin Exp Hematop
46: 5-10, 2006.
11. Petitjean B, Jardin F, Joly B, et al. Pyothorax-associated lym-
phoma: a peculiar clinicopathologic entity derived from B cells at
late stage of differentiation and with occasional aberrant dual B-
and T-cell phenotype. Am J Surg Pathol 26: 724-732, 2002.
12. Mason DY, Cordell J, Brown M, et al. Detection of T cells in par-
affin wax embedded tissue using antibodies against a peptide se-
quence from the CD3 antigen. J Clin Pathol 42: 1194-1200, 1989.
13. Inaba T, Shimazaki C, Sumikuma T, et al. Expression of T-cell-
associated antigens in B-cell non-Hodgkin’s lymphoma. Br J Hae-
matol 109: 592-599, 2000.
14. Kaleem Z, White G, Zutter MM. Aberrant expression of T-cell-
associated antigens on B-cell non-Hodgkin lymphomas. Am J Clin
Pathol 115: 396-403, 2001.
15. Inaba T, Shimazaki C, Sumikuma T, Nakagawa M. T-cell associ-
ated antigen-positive B-cell lymphoma. Leuk Lymphoma 42:
1161-1171, 2001.
16. Wang J, Chen C, Lau S, et al. CD3-positive large B-cell lym-
phoma. Am J Surg Pathol 33: 505-512, 2009.
17. Porter SR, Diz Dios P, Kumar N, Stock C, Barrett AW, Scully C.
Oral plasmablastic lymphoma in previously undiagnosed HIV dis-
ease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 87: 730-
734, 1999.
18. Wallentine JC, Perkins SL, Tripp SR, Bruggman RD, Bayerl MG.
Diffuse large B-cell lymphoma with coexpression of CD3 in a pe-
diatric patient: a case report, review of the literature, and tissue
microarray study. J Pediatr Hematol Oncol 31: 124-127, 2009.
19. Carotta S, Nutt SL. Losing B cell identity. Bioessays 30: 203-207,
2008.
20. Cobaleda C, Schebesta A, Delogu A, Busslinger M. Pax5: the
guardian of B cell identity and function. Nat Immunol 8: 463-470,
2007.
21. Alexiou C, Kau RJ, Dietzfelbinger H, et al. Extramedullary plas-
macytoma: tumor occurrence and therapeutic concepts. Cancer 85:
2305-2314, 1999.
22. Chang ST, Liao YL, Lu CL, Chuang SS, Li CY. Plasmablastic cy-
tomorphologic features in plasma cell neoplasms in immunocom-
petent patients are significantly associated with EBV. Am J Clin
Pathol 128: 339-344, 2007.
23. Hasegawa Y, Shimizu S, Katsura Y, et al. A case of plasmablastic
lymphoma, which occurs in protein losing enterogastorpathy (Ab-
stract). Rinsho Ketsueki 42: 1002, 2001 (in Japanese).
24. Iriyama C, Kasai M, Oyama T, Uchida T, Ogura M. A HIV nega-
tive plasmablastic lymphoma patient successfully treated by THP-
COP therapy (Abstract). Rinsho Ketsueki 58: 1193, 2007 (in Japa-
nese).
25. Katoh Y, Ishii Y, Hirabayashi K, Nakamura N, Osamura R. A case
of plasmablastic lymphoma, which was found as a rt maxillary tu-
mor (Abstract). Proceeding of the Japanese Society of Pathology
97: 359, 2008 (in Japanese).
26. Kobayashi A, Kobayashi S, Sato K, et al. A case of HIV negative
plasmablastic lymphoma (Abstract). Rinsho Ketsueki 45: 84, 2004
(in Japanese).
27. Matsuki E, Miyakawa Y, Tsukada Y, et al. Pathogensis of CD138
positive, TCR, IgH rearrangement negative plasmablastic lym-
phoma of the uterus (Abstract). Rinsho Ketsueki 49: 1117, 2008
(in Japanese).
28. Miyazaki Y, Shimizu S. A case of pancreatic plasmablastic lym-
phoma arising from SLE patient (Abstract). Nishinihon Journal of
Dermatology 70: 354, 2008 (in Japanese).
29. Ohno T, Hiraga J, Kinoshita T, Naoe T, Sakakibara A, Nakamura
S. A case of plasmablastic lymphoma arising from paranasal sinus
of HIV negative patient (Abstract). J Clin Exp Hematop 46: 84,
2006 (in Japanese).
30. Sakamoto I, Hishima T, Hayashi Y, et al. A case of HHV-8 associ-
ated plasmablastic lymphoma arising from multicentric Castle-
man’s disease patient (Abstract). Proceeding of the Japanese Soci-
ety of Pathology 95: 346, 2006 (in Japanese).
31. Toyonaga M, Numata A, Nagafuji K, et al. A case of HIV nega-
tive plasmablastic lymphoma with myelofiblosis (Abstract). J Clin
Exp Hematop 45: 91, 2005 (in Japanese).
32. Lin Y, Rodrigues GD, Turner JF, Vasef MA. Plasmablastic lym-
phoma of the lung: report of a unique case and review of the lit-
erature. Arch Pathol Lab Med 125: 282-285, 2001.
Ⓒ 2010 The Japanese Society of Internal Medicine
http://www.naika.or.jp/imindex.html