
CCEB Modeling Quality of Life Data with Missing Values Andrea B. Troxel, Sc.D. Assistant Professor...
29
CCEB Modeling Quality of Life Data with Missing Values Andrea B. Troxel, Sc.D. Assistant Professor of Biostatistics Center for Clinical Epidemiology and Biostatistics University of Pennsylvania School of Medicine
-
Upload
milo-norris -
Category
Documents
-
view
215 -
download
1
Transcript of CCEB Modeling Quality of Life Data with Missing Values Andrea B. Troxel, Sc.D. Assistant Professor...

CCEB
Modeling Quality of Life Datawith Missing Values
Andrea B. Troxel, Sc.D.Assistant Professor of
BiostatisticsCenter for Clinical Epidemiology
and BiostatisticsUniversity of Pennsylvania
School of Medicine

CCEB
Outline
• Why measure QOL in oncology?
• Types of missing data
• Possible modeling approaches
• Example: SWOG study of QOL in colorectal cancer
CCEB
QOL in Oncology
• Potentially debilitating effects of treatment
• Tradeoff between quantity and quality of life
• An increasingly chronic disease
• Important focus on survivorship
• Longitudinal measurements

CCEB
Missing Data - Examples
• Subject moves out of town• Researcher forgets to administer
questionnaire• Subject returns incomplete
questionnaire• Subject’s family refuses questionnaire• Subject is too sick to fill out
questionnaire• Subject dies

CCEB
Missing Data - Definitions
• Missing completely at random
• Missing at random
• Nonignorable
CCEB
Modeling Approaches
• Complete case approaches• Models for MAR data• Models for NI data• Sensitivity analyses• Extensions of failure-time
models• Imputation methods

CCEB
Models for MAR data
• Generalized linear models
• Generalized estimating equations
• Weighted methods

CCEB
Models for NI data
• Fully parametric models–Directly model the missingness
mechanism
–Estimate a nonignorability parameter
–Computationally difficult
–Untestable assumptions
CCEB
Sensitivity Analyses
• Vary aspects of model and determine effects on inference
• Local sensitivity analysis– ISNI (Troxel, Ma, and Heitjan, 2005)
–Assess sensitivity in the neighborhood of the MAR assumption
–Easy to compute and interpret

CCEB
Failure-time Models
• Take advantage of bivariate survival methods• Integrate clinical and QOL
data• Avoid primacy of one outcome
over the other• Partially handle missing data
due to death

CCEB
Multiple Imputation
• Use an appropriate method to create a series of “complete” data sets
• Use any appropriate method of analysis on each data set
• Combine the analyses to achieve one reportable result
CCEB
SWOG 9045
• Companion study to SWOG 8905– 599 subjects with advanced colorectal
cancer
–Seven arms (!) assessing effectiveness of 5-FU

CCEB
SWOG 8905
• Variations in–Route of administration
» Bolus injection (arms 1-3)
» Protracted 28-day continuous infusion (arms 4-5)
» Four weekly 24-hour infusions (arms 6-7)
–Biochemical modulation» None (arms 1, 4, 6)
» Low dose leucovorin (arms 2, 5)
» High dose leucovorin (arm 3)
» PALA (arm 7)

CCEB
SWOG 9045
• Five primary outcomes–Mouth pain–Diarrhea–Hand/foot sensitivity–Emotional functioning (SF-36)–Physical functioning (SF-36)
• Secondary outcome–Symptom distress scale (high scores = more distress)

CCEB
SWOG 9045
• 4 assessments–Randomization– 6 weeks– 11 weeks– 21 weeks
• 287 patients registered• 272 (95%) submitted baseline
questionnaire

CCEB
QOL Submission Rates
Week
0 6 11 21n 272 230 207 182
% of total 95 80 72 63
% of 272 100 83 76 65
% of alive 100 85 79 78
CCEB
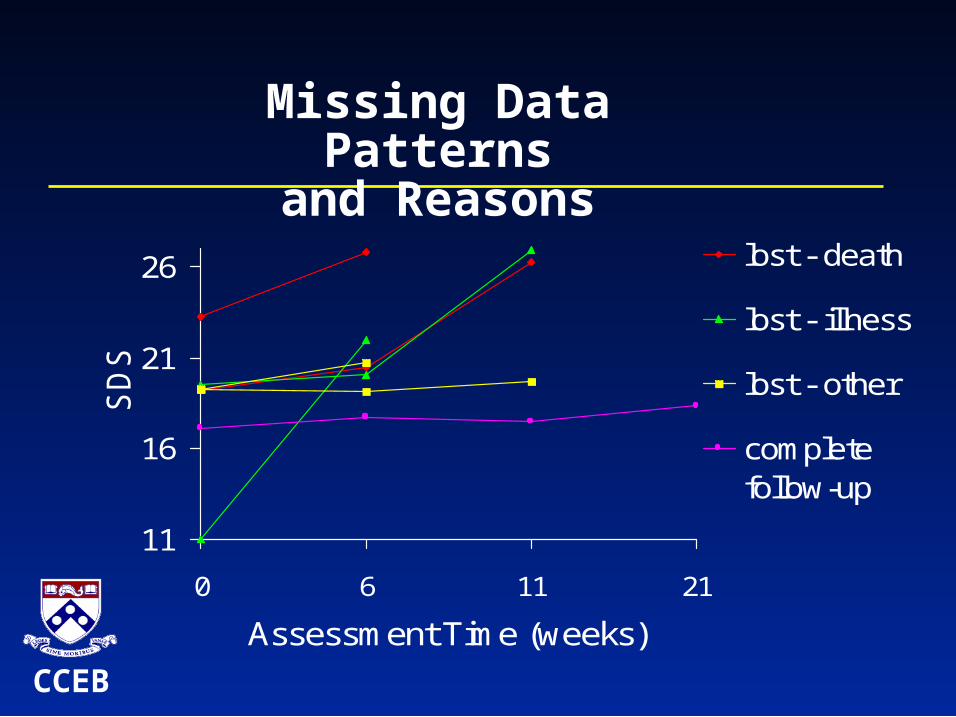
Missing Data Patterns
and Reasons
11
16
21
26
0 6 11 21
Assessment Time (weeks)
SD
S
lost - death
lost - illness
lost - other
completefollow-up

CCEB
Submission Rates
• Restrict analysis to subjects who survived for 21 weeks
• N=227
Week
0 6 11 21
N 227 197 187 172% 100 87 82 76

CCEB
Missing Data Patterns
Time Pattern ( 1=submitted, 0=missing) Total
0 1 1 1 1 1 1 1 1 2276 1 1 1 1 0 0 0 0 197
11 1 1 0 0 1 1 0 0 187
21 1 0 1 0 1 0 1 0 172
n 150 26 8 13 9 2 5 14 227

CCEB
Models - SDS
• Normal GLM–Complete cases
–All available data, unweighted
–All available data, weighted
• NI model–Normal component for SDS data
– Logistic model for missingness probs.
0 1logit 0 1, 2,3it t t itP R Y t

CCEB
Results - SDS
12
14
16
18
20
22
24
0 6 11 21
Time (weeks)
SD
S s
core
NI
Wtd MAR
MAR
CC
CCEB
Sensitivity Analysis
• Assess sensitivity to nonignorability in the neighborhood of the MAR model
• Sensitivity of parameters depends on how the model is parameterized

CCEB
Sensitivity - SDS
Estimate SE ISNI*
T0(single) 17.0 .51 14.29
T6(single) 17.4 .53 1.24
T11(single) 17.3 .56 0.87
T21(single) 18.1 .59 0.73
T0(comb) 18.5 .57 4.26
T6(comb) 19.0 .60 1.10
T11(comb) 18.8 .62 1.21
T21(comb) 19.6 .64 1.02
CCEB
Frailty Model - SDS
• SDS>24 SDS “event”• Jointly assess survival and
SDS events• Estimate correlation• Estimate covariate effects• No special programming
required

CCEB
Frailty Model – SDS
• No significant effect of combination therapy
• Frailty variance estimated to be 0.54
• 95%CI (0.28, 0.92)
• Significant random subject effect (p < .0001)
CCEB
Models – Hand/Foot Sensitivity
0 1 2 3 4logit 6 11 21it iE Y I t I t I t X
• Yit is a binary indicator of bothersome or worse symptoms
• Xi is an indicator of continuous infusion vs bolus injection (arms 4,5 vs arms 1-3)
• N=154 (arms 1-5, alive for 21 weeks)

CCEB
Results – Hand/Foot Sensitivity
0
5
10
15
20
25
30
0 6 11 21
Time (weeks)
Est
imat
ed %
CC
Unwtd GEE
Wtd GEE

CCEB
Models – Hand/Foot Sensitivity
• Treatment effect OR estimates–CC: 3.1 (1.4 – 7.0)
–MAR: 2.5 (1.2 – 5.3)
–Wtd MAR: 2.5 (1.2 – 4.8)

CCEB
Conclusions
• Missing data is a pervasive problem• Standard approaches can lead
to misleading inferences• Sensitivity analysis is a key
component• Certain comparisons are more
susceptible than others


















