CBD in children with treatment-resistant epilepsies ... · PDF filetreatment-resistant...
33
CBD in children with treatment-resistant epilepsies: initial results and planned trials Maria Roberta Cilio, MD, PhD Professor Neurology & Pediatrics Director, Pediatric Epilepsy Research University of California, San Francisco
Transcript of CBD in children with treatment-resistant epilepsies ... · PDF filetreatment-resistant...

CBD in children with treatment-resistant
epilepsies: initial results and planned trials
Maria Roberta Cilio, MD, PhD Professor Neurology & Pediatrics
Director, Pediatric Epilepsy Research University of California, San Francisco

Disclosure
Nothing to disclose

US survey of 19 parents using artisanal preparations of CBD-enriched cannabis to treat their children with treatment-resistant epilepsy aged 2-16 years
12/19 had Dravet syndrome 4 patients had Doose syndrome 1 had Epilepsy in Females with Mental Retardation 1 had Lennox-Gastaut Syndrome 1 had idiopathic epilepsy

Large variety of seizure types Seizure frequency ranged between 2/week to 250/day Estimated doses of cannabidiol between 0.5 mg/kg/day
and 28 mg/kg/day Duration of treatment ranged between two weeks to > 1
year 16/19 parents reported a reduction in seizure
frequency
2 patients were reported to be seizure-free (1 Doose, 1 DS)
8 had a reduction in seizure frequency > 80% (5/12 patients with DS)
3 had a reduction > 50% (DS) 3 had a reduction > 25% 3 patients experience no change (2 DS, 1 Doose)

Up to 80% reported positive side-effects (better mood, increased alertness, better sleep)
Less than 1/3 reported negative side effects (drowsiness, fatigue, appetite decrease)
Severe side effects were not reported

The case for medical marijuana in epilepsy
Anecdotal reports Neither the doses nor the exact composition of the
different artisanal compounds can be determined The impact of the percentages of THC on effects and
side effects cannot be assessed Impact of placebo effect in this very selected
population
Scientific support of efficacy very slim Absolutely no data on drug-drug interaction No or little data on long-term safety and tolerability
The Myth It is natural – and organic! It must be good.
Not perceived as a drug but a natural remedy – requested as a first drug in children with childhood absences
CBD works better alone: let’s stop the other antiepileptic drugs
The use of pharmacological compounds derived from cannabis sativa = free marijuana

The context This is a very sensitive issue for epileptologists and
child neurologist practicing in Colorado as kids are streaming in from all over the country whose parents bring them here to get “Charlotte’s web”. There are likely more kids who have not responded than the few who have and made CNN.
Children may being given cannabis-based preparations in an uncontrolled and in my opinion unsafe fashion by people with no knowledge or experience in care of epilepsy patients.

The case and the challenges for assessing cannabidiol in
epilepsy CBD ≠ Marijuana DEA Schedule 1 substance – license and safe Children FDA approval Internal approval Import from the UK Traveling within the US Foundations have expressed “legal” concerns – study is unfunded

Open-label observational study
Pharmaceutical preparation of pure CBD Children with intractable seizures and well-defined epilepsies Overall responder rate Seizure-free patients Responder rate in specific seizure type Responder rate in specific syndromes Age of responders Adverse events Pharmacokinetic interactions Negative associations Possible synergies tested in a wide range of AEDs Trigger the design of a trial focused on a specific syndrome

Open-label observational study
Accuracy of diagnosis in terms of epilepsy type/syndrome and seizure type i.e. mutation in SCN1A gene ≠ Dravet syndrome
Prospective and non retrospective

Open-label trial of CBD in add-on for children with intractable
epilepsy Pediatric age: 1-18 years Accurate electroclinical diagnosis of epilepsy type/syndrome Video-EEG confirmed seizure type (s) Drug-resistant epilepsy despite trial with 2 or more gold standard
AEDs at therapeutic doses At least 2 seizures/week during 4-week baseline
Generalized tonic-clonic Myoclonic absences Clonic Tonic Tonic-atonic
§ 1-3 AEDs Stable concomitant AEDs during 4-week baseline – stable settings
of VNS and stable ketogenic diet for 3 months Informed consent

The importance of seizure characterization
A majority of patients with idiopathic generalized epilepsy had received inappropriate AEDs treatment (Benbadis et al. 2003)
Children with generalized spike-wave discharges whose staring spells have been misinterpreted as temporal lobe seizures (Hussain & Sankar, 2011)
The poor response to initial therapy in such cases is clearly not of prognostic significance
The precise characterization of seizures provide a basis for accurate diagnosis and therapy
Some patients with non-epileptic paroxysmal events are treated for epilepsy and clearly do not respond to treatment
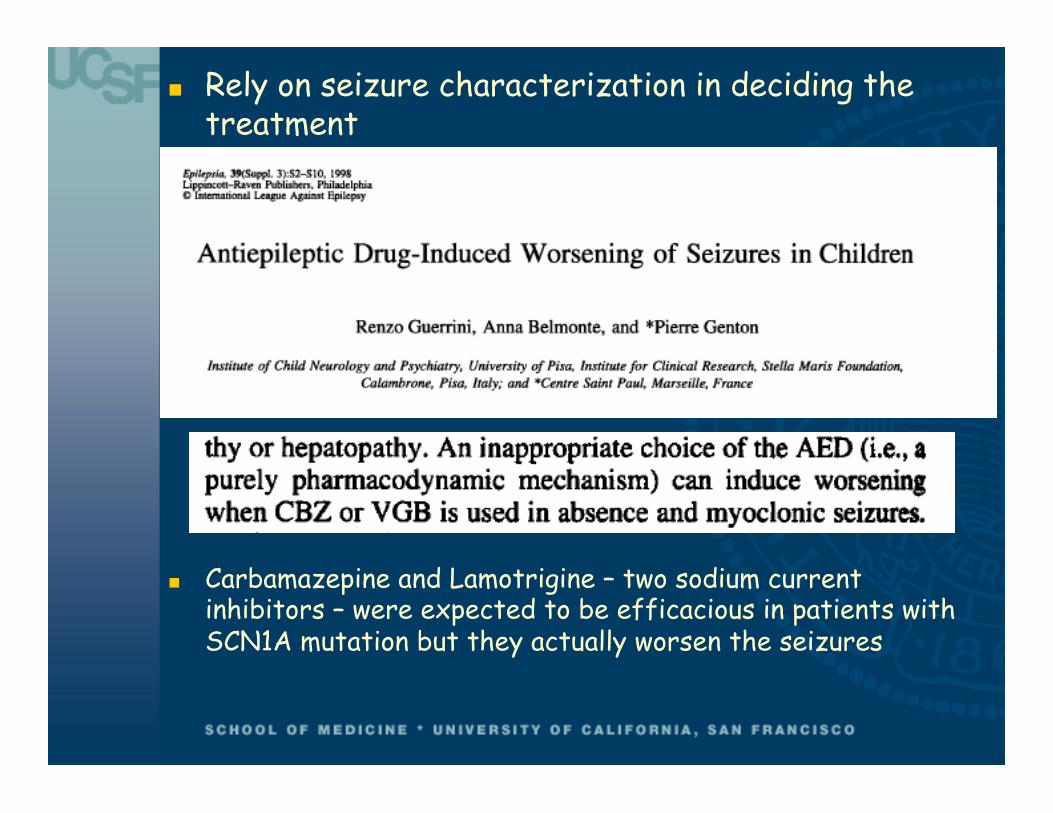
Rely on seizure characterization in deciding the treatment
Carbamazepine and Lamotrigine – two sodium current inhibitors – were expected to be efficacious in patients with SCN1A mutation but they actually worsen the seizures

Exclusion criteria Neurodegenerative diseases Inborn error of metabolism Tumors Non- well defined epilepsies Use of cannabis-derived compound in the preceding two
months Felbamate initiated within the past 18 months

Acknowledgements Geoffrey Guy Stephen Wright Alice Mead Michelle Welborn Terry Woodworth
Joe Sullivan - UCSF Orrin Devinsky -NYU Elisabeth Thiele – MGH/Harvard Helen Cross – Great Ormond Street, London Eric Marsh – Children’s Hospital Philadelphia Linda Laux – Children’s Hospital Chicago

Acknowledgements UCSF Yelena Belkin and Diana Wong – Investigational
Pharmacy Parents Children

Limitations Results are preliminary Numbers are small No statistical analysis No conclusions

9 patients Well-defined epilepsies and video-EEG confirmed
seizure types Genetic testing MRI Extensive metabolic testing All patients followed at UCSF Pediatric Epilepsy Center All fulfilled the inclusion criteria Seizure frequency evaluated by seizure diary during
baseline and during treatment Concomitant AEDs remained unchanged during the first
three months of treatment
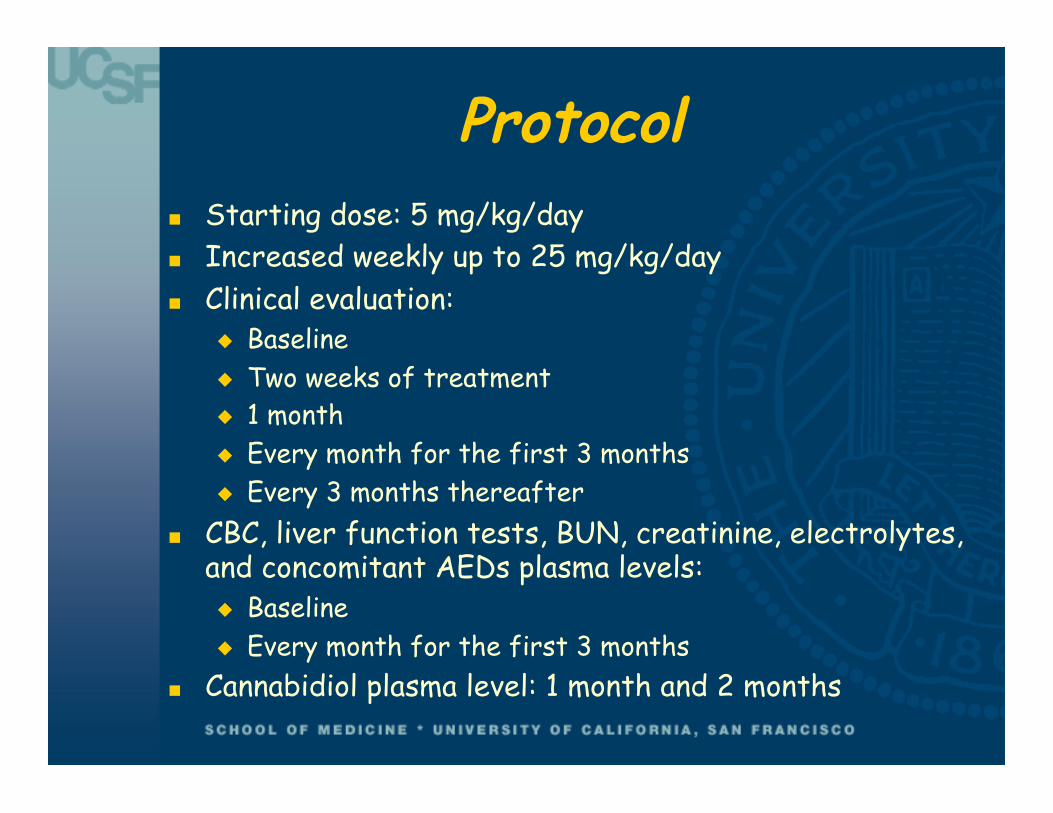
Protocol Starting dose: 5 mg/kg/day Increased weekly up to 25 mg/kg/day Clinical evaluation:
Baseline Two weeks of treatment 1 month Every month for the first 3 months Every 3 months thereafter
CBC, liver function tests, BUN, creatinine, electrolytes, and concomitant AEDs plasma levels: Baseline Every month for the first 3 months
Cannabidiol plasma level: 1 month and 2 months

9 patients Follow-up: 2 months – 1 year Age range: 3 – 17 years
3 patients: Dravet syndrome – SCN1A positive 4 patients: Epilepsy with myoclonic absences 1 patient: Generalized epilepsy with generalized tonic-
clonic seizures – MRI, extensive genetic and metabolic testing negative
1 patient: Epilepsy due to bilateral polymicrogyria and focal seizures evolving into bilateral clonic seizure

Concomitant AEDs Patients with Dravet:
Clobazam Levetiracetam Topiramate Stiripentol Phenobarbital Clonazepam
Patients with Epilepsy with myoclonic absences Clobazam Clonazepam Lamotrigine Levetiracetam Felbatol Acetazolamide

Concomitant AEDs 1 patient with Generalized epilepsy
Clobazam Prednisolone
1 patient with Epilepsy due to bilateral polymicrogyria: Phenobarbital Carbamazepine

Preliminary results 3 patients with Dravet
2 patients: seizure-free 1 patient: increased seizure frequency – started weaning
of CBD 4 patients with Epilepsy with myoclonic absences
2 patients: 75% and 90% reduction in seizure frequency – 1 patient on CBD monotherapy
2 patients: no changes in seizure frequency – 1 started weaning after > 3 months of treatment
1 patient with Generalized epilepsy 75% seizure reduction
1 patient with Epilepsy due to bilateral polymicrogyria: No changes in seizure frequency – CBD weaned after 6
month of treatment

Preliminary side-effects No significant changes in CBC, LFTs, BUN, Creatinine,
electrolytes Increased clobazam level 3 patients: appetite loss, food aversion, nausea and
occasional vomiting 1 patient: weight loss of 20% Dose was decreased in 2/3 patients from 25 to 20 mg/kg/
day with amelioration of symptoms 3 patients: loose stool/diarrhea 1 patient: fatigue

Next step All open-label studies are biased. This is particularly
true for CBD. We lack blinded data on safety and efficacy Company-sponsored randomized double-blind controlled
trials Dravet syndrome and Lennox-Gastaut syndrome

Placebo-controlled, syndrome- dedicated trial
Accurate selection of homogenous populations Small samples of patients may be sufficient to conclude
superiority of CBD Accurate definition of gold standard treatment for a
specific syndrome – restricted number of co-medication per syndrome
Better defined targets based on natural history Based on the known natural history, CBD may be
associated earlier

Dravet syndrome Stiripentol is the only compound that proved its efficacy in
DS through the methodology of randomized placebo-controlled trial (combined with Valprate and Clobazam)
Topiramate, Levetiracetam, Potassium Bromide, Ketogenic diet are useful (based on open studies and daily practice)
Lamotrigine and Carbamazepine should be avoided
Complete seizure control is rarely obtained particularly on the long-term
Can seizure reduction improve long-term cognitive outcome?
Chiron et al. Lancet 2001; Chiron and Dulac Epilepsia 2011

Lennox-Gastaut syndrome Electroclinical syndrome with childhood onset Onset between 1 and 4 years of age Many patients experience more than 90 seizures a
month (Glauser 2008) 60 to 80% of patients are refractory Normal psychomotor development at onset but mostly
global delay Etiology: genetic, structural/metabolic, and of unknown
origin 22% had neonatal seizures and 40% had West syndrome
(Trevathan et al. 1997)
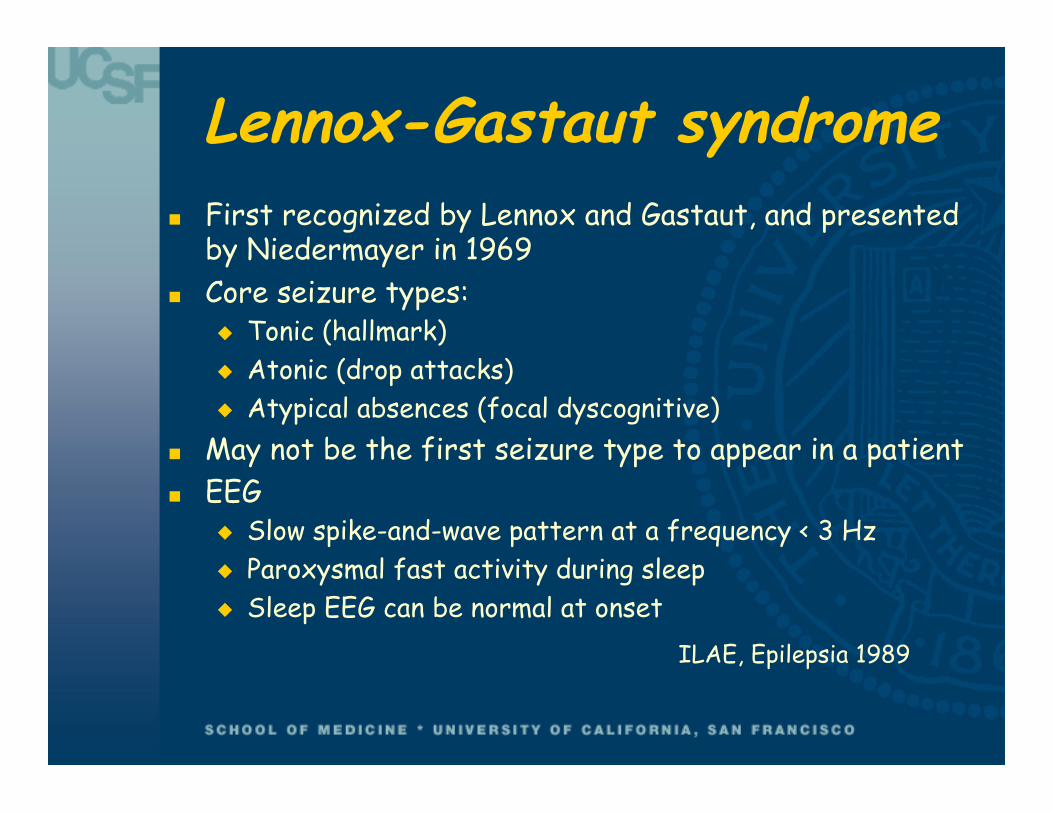
Lennox-Gastaut syndrome First recognized by Lennox and Gastaut, and presented
by Niedermayer in 1969 Core seizure types:
Tonic (hallmark) Atonic (drop attacks) Atypical absences (focal dyscognitive)
May not be the first seizure type to appear in a patient EEG
Slow spike-and-wave pattern at a frequency < 3 Hz Paroxysmal fast activity during sleep Sleep EEG can be normal at onset
ILAE, Epilepsia 1989

LGS current treatment Valproic acid – efficacy on myoclonic, atypical absences
and atonic seizures Several drugs proven effective on randomized placebo
controlled trials as adjuctive: Felbamate, Lamotrigine, Topiramate, Rufinamide, Clobazam (children and adults)
Ketogenic Diet VNS Corpus callosotomy Avoid medications known to worsen specific seizure
type i.e. i.v. benzodiazepines – worsening of tonic seizures