“Cauliflower Ear” in a Teenager: A Possible Sign of Child Abuse
2
hypersensitivity reaction to an inciting agent. Triggers include insect bites, medications, immunizations, hema- tologic disorders, infections, and association with solid tumors (2,4); however, half of all patients lack a known trigger (3), as was the case in our patient. The differential diagnoses include drug reaction, bacterial cellulitis, Churg–Strauss syndrome, idiopathic hypereosinophilic syndrome, and bullous pemphigoid. The disease may spontaneously remit, but treatment with topical corticosteroids can be used for limited dis- ease. However, our patient required the standard treat- ment of systemic corticosteroid therapy, slowly tapered over 1 month (5). When the disease is recurrent and widespread, alternative treatments have been employed including dapsone, antimalarial agents, cyclosporine, azathioprie, interferon alpha, and photochemotherapy (psoralen and ultraviolet A radiation ) (3,5). In conclusion, Wells’ syndrome is a rare disease that is even more obscure in childhood. The pediatric popula- tion does not typically present with bullae formation, as in our case, and can be mistaken for a drug eruption. Our patient illustrated that the extent of disease can be devastatingly widespread. It is therefore, imperative to consider Wells’ syndrome in patients with presumed cellulitis and eosinophila who fail antibiotic therapy. REFERENCES 1. Caputo R, Marzano AV, Vezzoli P et al. Wells syndrome in adults and children. Arch Dermatol 2006;142:1157– 1161. 2. Feliciani C, Motta A, Tortorella R et al. Bullous Wells syndrome. J Eur Acad Dermatol Venereol 2006;20:1021– 1022. 3. Gilliam AE, Bruckner AL, Howard RM et al. Bullous ‘‘cellulitis’’ with eosinophilia: case report and review of Wells’ syndrome in childhood. Pediatrics 2005;116:e149– e155. 4. Van der Straaten S, Wojciechowski M, Salgado R et al. Eosinophilic cellulitis or Wells’ syndrome in a 6-year-old child. Eur J Pediatr 2006;165:197–198. 5. Afsahi V, Kassabian C. Wells’ syndrome. Cutis 2003;72: 209–212. MARISSA SHAMS, M.D.* JEANNETTE HUDGENS, M.D. JACK L. LESHER, JR, M.D. FRANCES FLORENTINO, M.D. *Department of Medicine, Tulane University Health Sciences Center, New Orleans, Louisiana, Division of Dermatology, Medical College of Georgia, Augusta, Georgia ‘‘CAULIFLOWER EAR’’ IN A TEENAGER: A POSSIBLE SIGN OF CHILD ABUSE Abstract: ‘‘Cauliflower ear’’ is a perichondritis of the auricular pavilion, usually caused by infection or repeated trauma. In children, this entity is considered infrequent. We present the case of a 10-year-old girl living in a child care institution with ‘‘cauliflower ear’’ that was interpreted as a possible sign of child abuse. ‘‘Cauliflower ear’’ is an auricular perichondritis, usually caused by infection or trauma in the upper part of the ear. Repeated trauma is required for the development of this deformity. In children, it is infrequent, and few cases have been reported. We describe the case of a patient with ‘‘cauliflower ear’’ that was interpreted as an indirect sign of possible child abuse. A 10-year-old girl attended our dermatology surgery. She complained of a lump in the left ear of unknown evolution time that had to be evaluated. She was a healthy child with unremarkable patholog- ical history who had been living in a child care institution for the last few months. Her caretakers had observed a lump on the ear that was otherwise asymptomatic. The patient could not define accurately when it had first ap- peared. Clinical evaluation revealed a 2-cm asymptom- atic plaque (Fig. 1) located in the triangular cavity of the Figure 1. Bulky injury, elevated, folded, in the triangular cavity of the ear, of similar color to the normal skin, without swelling. Address correspondence to Jeannette Hudgens, M.D., 378 East Shoreline Dr., North Augusta, SC 29841, or e-mail: jennidawg@ yahoo.com. 226 Pediatric Dermatology Vol. 29 No. 2 March ⁄ April 2012
-
Upload
laura-cuesta -
Category
Documents
-
view
212 -
download
0
Transcript of “Cauliflower Ear” in a Teenager: A Possible Sign of Child Abuse

hypersensitivity reaction to an inciting agent. Triggersinclude insect bites, medications, immunizations, hema-tologic disorders, infections, and association with solidtumors (2,4); however, half of all patients lack a knowntrigger (3), as was the case in our patient. The differentialdiagnoses include drug reaction, bacterial cellulitis,Churg–Strauss syndrome, idiopathic hypereosinophilicsyndrome, and bullous pemphigoid.
The disease may spontaneously remit, but treatmentwith topical corticosteroids can be used for limited dis-ease. However, our patient required the standard treat-ment of systemic corticosteroid therapy, slowly taperedover 1 month (5). When the disease is recurrent andwidespread, alternative treatments have been employedincluding dapsone, antimalarial agents, cyclosporine,azathioprie, interferon alpha, and photochemotherapy(psoralen and ultraviolet A radiation ) (3,5).
In conclusion,Wells’ syndrome is a rare disease that iseven more obscure in childhood. The pediatric popula-tion does not typically present with bullae formation, asin our case, and can bemistaken for a drug eruption.Ourpatient illustrated that the extent of disease can bedevastatingly widespread. It is therefore, imperative toconsider Wells’ syndrome in patients with presumedcellulitis and eosinophila who fail antibiotic therapy.
REFERENCES
1. Caputo R, Marzano AV, Vezzoli P et al. Wells syndromein adults and children. Arch Dermatol 2006;142:1157–1161.
2. Feliciani C, Motta A, Tortorella R et al. Bullous Wellssyndrome. J Eur Acad Dermatol Venereol 2006;20:1021–1022.
3. Gilliam AE, Bruckner AL, Howard RM et al. Bullous‘‘cellulitis’’ with eosinophilia: case report and review ofWells’ syndrome in childhood. Pediatrics 2005;116:e149–e155.
4. Van der Straaten S, Wojciechowski M, Salgado R et al.Eosinophilic cellulitis or Wells’ syndrome in a 6-year-oldchild. Eur J Pediatr 2006;165:197–198.
5. Afsahi V, Kassabian C. Wells’ syndrome. Cutis 2003;72:209–212.
MARISSA SHAMS, M.D.*JEANNETTE HUDGENS, M.D.�JACK L. LESHER, JR, M.D.�FRANCES FLORENTINO, M.D.�*Department of Medicine, Tulane University HealthSciences Center, New Orleans, Louisiana, �Division ofDermatology, Medical College of Georgia, Augusta,Georgia
‘‘CAULIFLOWER EAR’’ IN A TEENAGER:
A POSSIBLE SIGN OF CHILD ABUSE
Abstract: ‘‘Cauliflower ear’’ is a perichondritis ofthe auricular pavilion, usually caused by infection orrepeated trauma. In children, this entity is consideredinfrequent. We present the case of a 10-year-old girlliving in a child care institution with ‘‘cauliflower ear’’that was interpreted as a possible sign of child abuse.
‘‘Cauliflower ear’’ is an auricular perichondritis, usuallycausedby infectionor trauma in theupperpart of the ear.Repeated trauma is required for the development of thisdeformity. In children, it is infrequent, and fewcaseshavebeen reported. We describe the case of a patient with‘‘cauliflower ear’’ that was interpreted as an indirect signof possible child abuse.
A 10-year-old girl attended our dermatology surgery.She complained of a lump in the left ear of unknownevolution time that had to be evaluated.
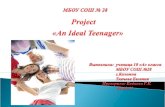
She was a healthy child with unremarkable patholog-ical historywho had been living in a child care institutionfor the last few months. Her caretakers had observed alump on the ear that was otherwise asymptomatic. Thepatient could not define accurately when it had first ap-peared. Clinical evaluation revealed a 2-cm asymptom-atic plaque (Fig. 1) located in the triangular cavity of the
Figure 1. Bulky injury, elevated, folded, in the triangularcavity of the ear, of similar color to the normal skin, withoutswelling.
Address correspondence to Jeannette Hudgens, M.D., 378 EastShoreline Dr., North Augusta, SC 29841, or e-mail: [email protected].
226 Pediatric Dermatology Vol. 29 No. 2 March ⁄April 2012

ear characterized by a bulky, irregular, hard surface withno inflammatory changes, fluctuation, or hair.
Our differential diagnosis included hamartoma,nevoid lesion, fibrocartilaginous tumor, ‘‘cauliflowerear,’’ and pseudocyst of the ear. A skin biopsy wasperformed that revealed hyperplasic epidermis and der-miswithfibrous repair tissue,without inflammatorysignsor hemorrhage. No hair or cartilaginous abortive struc-tures were observed. Such findings were interpreted asperichondritis following a possible previous trauma.
The patient was asked about the possibility of trau-matic history and admitted having suffered from strongear pulling and slapping by her father. According to thehistory taken fromthecaregiversof the institution thegirlhad been separated from her family because of suspicionofchildabuse.Uponherarrivalattheinstitution,theyhadnoticed strongevidenceof several ironburnsonherbody.Thepatientwas thoroughly examined, butnoevidenceofrecent injuries suggestive of child abuse was found.
‘‘Cauliflower ear’’ is an auricular perichondritis thatcan be caused by infection or trauma in the upper ormiddle third of the ear. It affects the auricular cartilageand as a result evolves into thickening of the ear, givingthe characteristic cauliflower appearance.
Repeated battering of the ear, strong enough to pro-duce a hematoma under the skin, is usually needed forthe development of the cauliflower-shaped deformity.The hematoma, which separates the skin from the car-tilage, results in an interruption of the vascular supply tothe cartilage (1,2).
‘‘Cauliflower ear’’ has also been described in relationto sports in which the ear is repeatedly traumatized, suchas football, baseball, hockey, boxing, and wrestling.Some cases have been reported as a result of piercings,opium smoking (3), or drug abuse (4).
‘‘Cauliflower ear’’ is not frequently seen in pediatricpatients. The majority of the described cases are relatedto hematomas associated with piercings and in the con-text of Munchausen’s syndrome (5). To our knowledge,‘‘cauliflower ear’’ as a result of child abuse has not so farbeen reported in the literature.
In our case, taking into account the high suspicion ofabuse by the family, in the absence of any other possiblecauses,weconsider thispathologyan indirect signofchildabuse, and we have informed the relevant authorities.
‘‘Cauliflower ear’’ is rare in children and adolescents.We believe it is necessary to consider this entity, partic-ularly given that it may be an indirect sign of child abuse.
REFERENCES
1. Ghanem T, Rasamny JK, Park SS. Rethinking auriculartrauma. Laryngoscope 2005;115:1251–1255.
2. Hanigan WC, Peterson RA, Njus G. Tin ear syndrome:rotational acceleration in pediatric head injuries. Pediatrics1987;80:618–622.
3. MuthusamyE.Opiumaddiction and cauliflower ears: a casereport. Singapore Med J 1991;32:90–91.
4. Kumar PD, Chandrasekharan KG. ‘Cauliflower ear’ in anIndian patient with drug abuse. J Assoc Physicians India1992;40:491.
5. GriffithsH,CuddihyPJ,MarnaneC.Bleeding ears: a caseofMunchausen syndrome by proxy. Int J Pediatr Otorhino-laryngol 2001;57:245–247.
LAURA CUESTA, M.D.ISABEL BETLLOCH, M.D.JOSE BANULS, M.D.FERNANDO TOLEDO, M.D.Department of Dermatology, Hospital GeneralUniversitario, Alicante, Spain
COMPLEX LIMBAL CHORISTOMA IN NEVUS
SEBACEOUS SYNDROME
Abstract: Excision of an epibulbar choristoma fol-lowed by amniotic membrane grafting was performedon a 3-month-old baby who presented with nevussebaceous syndrome. Upon histopathologic examina-tion, the excised mass was seen to be a complexchoristoma, a rare ocular tumor. Amniotic membranetransplantation is currently the most acceptablemodality of treatment of limbal choristoma, with goodcosmetic outcome.
Complex limbal choristoma is a rare epibulbar tumor ofchildhood. It consists of combinations of various dis-placed tissues not characteristic of that particular loca-tion. We report here a child with nevus sebaceoussyndrome who presented with an epibulbar tumor thatwas successfully managed by excision and amnioticmembrane transplantation (AMT). Histopathologicexamination of the lesion confirmed the diagnosis ofcomplex limbal choristoma.
CASE REPORT
A 3-month-old baby presented with a gradually enlarg-ing painless nodule in the left eye since birth. The childhad good fixation to light. Examination under generalanesthesia showed a round, firm lesion measuring
Address correspondence to Laura Cuesta Montero, M.D.,DepartmentofDermatology,HospitalGeneralUniversitario,PintorBaeza 12, 03010 Alicante, Spain, or e-mail: [email protected].
Brief Reports 227