
CASES IN PRIMARY CARE - The New England Journal of Medicine · The New England Journal of Medicine...
60
CASES IN PRIMARY CARE Best practice in clinical diagnosis, treatment, and management
Transcript of CASES IN PRIMARY CARE - The New England Journal of Medicine · The New England Journal of Medicine...
CASES IN PRIMARY CAREBest practice in clinical diagnosis, treatment, and management

800.843.6356 | f: 781.891.1995 | [email protected] winter street, waltham, ma 02451-1413
nejmgroup.org
July 2017
CASES IN PRIMARY CARE
The presentation of interesting cases has a long tradition as an educational tool and contributes to lifelong learning. Discussing the clinical course and management of individual patients enhances our understanding of disease and provides a framework for learning about medical advances.
The New England Journal of Medicine publishes several case-based series including Case Records of the Massachusetts General Hospital, Clinical Problem-Solving, and Clinical Practice, plus our online Interactive Medical Cases. We have chosen the cases in this collection based on their clinical relevance to primary care. We hope you find this collection engaging and instructive.
Edward W. Campion, MDExecutive Editor and Online Editor The New England Journal of Medicine

3
Cases in Primary Care NEJM.org
Table of Contents
CASE RECORDS OF THE MASSACHUSETTS GENERAL HOSPITAL 5 Case10-2017—A6-Month-OldBoywithGastrointestinalBleedingandAbdominalPain L.M. Allister and Others Mar 30, 2017
14 Case2-2017—An18-Year-OldWomanwithAcuteLiverFailure K.R. Olson and Others Jan 19, 2017
CLINICAL PROBLEM-SOLVING 26 MakingtheConnection A.R. Schulman and Others Feb 2, 2017
33 BacktotheHistory M.W. Montgomery and Others May 4, 2017
CLINICAL PRACTICE
40 ScreeningforColorectalNeoplasia J.M. Inadomi Jan 12, 2017
48 HeartFailurewithPreservedEjectionFraction M.M. Redfield Nov 10, 2016
INTERACTIVE MEDICAL CASES
59 UnderPressure E.M. DeFilippis and Others Mar 30, 2017
60 DissectingaCaseofAbdominalPain J. Casey and Others Oct 27, 2016
© 2017 Copyright Massachusetts Medical Society. NEJM Group is a division of the Massachusetts Medical Society. All rights reserved.

4
BacktoTableofContents
Cases in Primary Care NEJM.org
CASE RECORDS OF THE MASSACHUSETTS GENERAL HOSPITALThe Journal has been publishing Case Records of the Massachusetts General Hospital since 1923. These reports of clinicopathological conferences are one of the most popular medical teaching tools in the world. They describe actual cases that expose the process of medical decision making, and range in focus from common conditions to medical mysteries, exploring advances in challenging differential diagnosis and treatment.

5
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 2017 1269
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Pr esen tation of C a se
Dr. Akash Gupta (Medicine and Pediatrics): A 6-month-old boy was seen in the emer-gency department of this hospital because of gastrointestinal bleeding and ab-dominal pain.
The patient had been in his usual state of health until 2 days before presenta-tion, when his parents noted that he began to have intermittent episodes of ab-dominal pain. During these episodes, some of which woke the patient from sleep, he cried and pulled his legs up toward his chest while lying on his back. His parents reported that they palpated his abdomen during some of the episodes and it felt rigid; they suspected that he might be having discomfort related to excessive intestinal gas. He continued to eat and drink normally without vomiting. The next day, the patient had two bowel movements, and the stools had reddish discolor-ation. With the first bowel movement, the redness seemed to be present in a small amount and only on the outside of the stool; with the second bowel movement, the amount of redness increased. The patient’s mother attributed the stool discolor-ation to beet consumption, since bowel movements with reddish stools had also occurred in the past after the patient had eaten beets. Intermittent episodes of apparent abdominal pain continued, and between the episodes, the patient be-haved normally. On the morning of presentation, he had a third bowel movement with reddish stools. His parents took him to day care, where he continued to have occasional periods of crying and pain, followed by a bowel movement that ap-peared to consist almost entirely of blood, including a large clot. After this bowel movement, he was reportedly pale and diaphoretic. The day care provider called the patient’s mother, who picked him up and took him to the emergency depart-ment of another hospital.
On examination at the other hospital, the temperature was 36.5°C, the pulse 178 beats per minute, the blood pressure 95/52 mm Hg, the respiratory rate 24 breaths per minute, and the oxygen saturation 100% while the patient was breathing am-
From the Departments of Emergency Medicine (L.M.A.), Radiology (R.L.), Sur‑gery (A.M.G.), and Pathology (J.K.L.), Massachusetts General Hospital, and the Departments of Emergency Medicine (L.M.A.), Radiology (R.L.), Surgery (A.M.G.), and Pathology (J.K.L.), Harvard Medical School — both in Boston.
N Engl J Med 2017;376:1269-77.DOI: 10.1056/NEJMcpc1616020Copyright © 2017 Massachusetts Medical Society.
Founded by Richard C. Cabot Eric S. Rosenberg, M.D., Nancy Lee Harris, M.D., Editors
Virginia M. Pierce, M.D., David M. Dudzinski, M.D., Meridale V. Baggett, M.D., Dennis C. Sgroi, M.D., Jo‑Anne O. Shepard, M.D., Associate Editors
Emily K. McDonald, Sally H. Ebeling, Production Editors
Case 10-2017: A 6-Month-Old Boy with Gastrointestinal Bleeding
and Abdominal PainLauren M. Allister, M.D., Ruth Lim, M.D., Allan M. Goldstein, M.D.,
and Jochen K. Lennerz, M.D.
Case Records of the Massachusetts General Hospital
Cases in Primary Care NEJM.org

6
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 20171270
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
bient air. The weight was 9.1 kg. On palpation of the abdomen, there was diffuse tenderness, which was greater on the right side than on the left, and no masses. There were no external anal fissures, and the remainder of the physi-cal examination was normal. Two hours after arrival at the other hospital, the patient passed a dark-red stool that was described as resem-bling currant jelly. Intravenous normal saline (5 ml per kilogram) was administered, and he was brought by ambulance to the emergency depart-ment of this hospital for further evaluation and treatment.
The patient had a history of infantile colic and gastroesophageal reflux, which had previously been treated with ranitidine. He received a low-lactose cow milk–based formula. Pureed fruits and vegetables had recently been introduced into his diet, after which constipation developed, his
stools became more firm, and daily bowel move-ments were associated with straining. He received cholecalciferol, and he had begun using an unspecified over-the-counter teething gel and unspecified homeopathic teething tablets 1 week earlier. Immunizations were current through 4 months of age; vaccines (including the second dose of live, oral human–bovine reassortant pentavalent rotavirus vaccine) had been adminis-tered 6 weeks earlier. There were no known aller-gies. The patient lived with his parents, attended day care, and had no known sick contacts. His parents were from Brazil; he was born in the United States and had not traveled outside the country. There was no family history of bleeding disorders.
On examination, the temperature was 36.3°C, the pulse 160 beats per minute, the blood pres-sure 98/47 mm Hg, the respiratory rate 32 breaths per minute, and the oxygen saturation 99% while the patient was breathing ambient air. He appeared well. Bowel sounds were pres-ent; the abdominal examination was otherwise limited because the patient was crying. The dia-per contained melena and a small amount of stool. The remainder of the examination was normal.
Dr. Ruth Lim: Thirty-five minutes after the pa-tient’s arrival in the emergency department, an ultrasound examination of the abdomen was performed. There was no evidence of intussus-ception, appendicitis, a focal lesion, or abnor-mally dilated bowel loops. Bowel peristalsis was present.
Dr. Gupta: On examination after ultrasonogra-phy, the pulse was 168 beats per minute, and the blood pressure 94/36 mm Hg. The patient ap-peared pale. The abdomen was soft, without distention, tenderness, or masses, and bowel sounds were present. Results of the physical examination were otherwise unchanged. Blood levels of electrolytes, glucose, aspartate amino-transferase, alanine aminotransferase, alkaline phosphatase, total bilirubin, direct bilirubin, and C-reactive protein were normal, as were the anion gap, platelet count, red-cell indexes, and results of renal-function tests. The results of other laboratory tests are shown in Table 1. Packed red cells were transfused, and pantopra-zole and famotidine were administered intrave-nously.
A diagnosis was made.
VariableReference Range,
Age-Adjusted†On Presentation,
This Hospital
Hematocrit (%) 33.0–39.0 17.5
Hemoglobin (g/dl) 10.5–13.5 5.7
Reticulocyte count (%) 0.5–2.5 7.6
White‑cell count (per mm3) 6000–17,500 22,200
Differential count (%)
Neutrophils 17–49 38
Lymphocytes 67–77 59
Monocytes 4–11 3
Red‑cell count (per mm3) 3,700,000–5,300,000 2,070,000
Prothrombin time (sec) 11.0–14.0 12.4
Prothrombin‑time international normalized ratio
0.9–1.1 1.0
Activated partial thromboplastin time (sec)
22.1–37.0 19.4
Total protein (g/dl) 6.0–8.3 5.4
Albumin (g/dl) 3.3–5.0 4.1
Globulin (g/dl) 1.9–4.1 1.3
Iron (μg/dl) 45–160 19
Iron‑binding capacity (μg/dl) 230–404 351
* To convert the values for iron and iron‑binding capacity to micromoles per liter, multiply by 0.1791.
† Reference values are affected by many variables, including the patient popula‑tion and the laboratory methods used. The ranges used at Massachusetts General Hospital are age‑adjusted, for patients who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be ap‑propriate for all patients.
Table 1. Laboratory Data.*
Cases in Primary Care NEJM.org

7
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 2017 1271
Case Records of the Massachusetts Gener al Hospital
Differ en ti a l Di agnosis
Dr. Lauren M. Allister: This 6-month-old boy pre-sented with gastrointestinal bleeding manifested by hematochezia, along with intermittent ab-dominal pain and one episode of melena. He appeared ill and had tachycardia. Pertinent fea-tures of the history include gastroesophageal reflux, a possible milk-protein allergy (since he was receiving a low-lactose formula), and expo-sure to unspecified teething tablets and a homeo-pathic teething medication. It is important to note the absence of fever, forceful vomiting, and hematemesis. Because care in the emergency department is more process-driven than outcome-driven, the evaluation in this case can be con-densed into the following steps: rapid assess-ment, stabilization, and diagnostic evaluation.
Rapid Assessment
This ill patient had tachycardia, pallor, profound anemia with ongoing blood loss, and intermit-tently abnormal findings on abdominal examina-tion. He presented with gastrointestinal bleed-ing manifested by hematochezia and melena. My initial diagnostic considerations include causes of lower gastrointestinal bleeding, although the description of melena gives me reason to think that this patient could have bleeding from both upper and lower gastrointestinal sources. Less likely is an isolated, massive upper gastrointesti-nal bleed with rapid transit time through the infant’s gastrointestinal tract.
Stabilization
The patient’s airway was intact, and his breath-ing was unlabored. However, his circulation was compromised; he was pale and had tachycardia, and the hematocrit was 17.5% with ongoing blood loss. He required volume resuscitation with the administration of isotonic f luids and the transfusion of packed red cells, which was performed in the emergency department.
The patient was neurologically intact. A bed-side glucose measurement may have been useful in determining whether poor feeding with resul-tant hypoglycemia contributed to his unwell appearance. The reported use of homeopathic and unspecified teething medications raises con-cerns about an unintentional toxic exposure. Could the teething tablets or medications have contained acetaminophen, which can cause an
overdose that leads to liver failure and gastroin-testinal bleeding, or nonsteroidal antiinflamma-tory drugs, which can cause irritation of the gastric mucosa and subsequent gastrointestinal bleeding? Although these exposures are unlikely underlying causes of this patient’s illness, they warrant further consideration and, possibly, toxi-cologic testing.
Diagnostic Evaluation
My diagnostic considerations fall into three broad categories: common, less common, and poten-tially life-threatening. Among the common diag-noses, ileocolic intussusception seems to be the most likely possibility; the patient presented at a typical age (since intussusception most com-monly occurs during infancy or early childhood) and had colicky abdominal pain and worsening gastrointestinal bleeding, with stool described as resembling currant jelly. Meckel’s diverticulum is the most common congenital malformation of the gastrointestinal tract, and if the diverticu-lum contains ectopic or heterotopic mucosa, it can cause gastrointestinal bleeding.1,2 Of the clinical findings associated with Meckel’s diverticulum, bleeding is one of the most common in chil-dren.1,3,4 Since Meckel’s diverticulum is classically associated with painless bleeding, this patient’s apparent abdominal pain is difficult to reconcile with this diagnosis.5,6 However, if Meckel’s diver-ticulum is associated with obstruction caused by intussusception, volvulus, or perforation, then pain can be a complicating feature.3 I would also consider an inflammatory or allergic gastritis or colitis, because these are common causes of lower gastrointestinal bleeding among children who present to the emergency department.7 The presence of mild gastritis plus colitis related to a milk-protein allergy could explain both the hematochezia and melena (mixed upper and lower gastrointestinal bleeding), as well as the associated pain. Infectious colitis seems unlike-ly, given the absence of fever, sick contacts, and travel. Other common causes of lower gastro-intestinal bleeding, such as a fissure or polyp, are not typically associated with such a severe presentation, so these diagnoses are easily ruled out in this case.
In a 6-month-old infant, the less common diagnoses that cause lower gastrointestinal bleed-ing include vascular malformations of the gastro-intestinal tract, atypical lymphonodular hyperpla-
Cases in Primary Care NEJM.org

8
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 20171272
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
sia, the hemolytic–uremic syndrome, inflammatory bowel disease, toxin-mediated processes, and underlying bleeding diatheses. I would give these causes careful consideration only after the com-mon diagnoses have been ruled out.
In this case, several diagnoses must be con-sidered because they are potentially life-threat-ening if missed. These diagnoses can be con-sequences of either the common or the less common conditions and include a perforated viscus, an acute abdomen, obstruction, hemor-rhagic shock, septic shock, and the presence of associated upper gastrointestinal bleeding while the patient is being evaluated for lower gastroin-testinal bleeding. Serial physical examinations and diagnostic testing are critical in identifying any of these potentially life-threatening pro-cesses.
Diagnostic Testing
The findings ascertained through diagnostic test-ing that are the most important in developing a differential diagnosis in this case are the hema-tocrit of 17.5%, the elevated white-cell count of 22,200 per cubic millimeter (which is nonspe-cific but worrisome), and the absence of intus-susception and other notable findings on ultra-sonography. The normal electrolyte levels, liver profile, and coagulation indexes are reassuring, and they argue against some systemic disease processes that would typically be associated with abnormalities in one or more of these mea-sures. However, a few additional studies would help to narrow the differential diagnosis. Be-cause of the possibility of a toxic exposure, I would perform a serum toxicology screen. In addition, I would perform blood and stool cul-tures to evaluate for infection, as well as abdomi-nal radiography to assess for bowel perforation, given the multiple days of gastrointestinal symp-toms and the worsening clinical appearance. To rule out upper gastrointestinal bleeding, I would consider performing gastric aspiration.
In view of the available test results, the ab-sence of intussusception on abdominal ultraso-nography, and the patient’s ongoing blood loss, two diagnoses from my list of common diagno-ses remain most likely: Meckel’s diverticulum and gastritis plus allergic colitis. Many other diagno-ses have been effectively ruled out through diag-nostic testing, and several less common causes would not be seriously considered until these
two common diagnoses are ruled out. In addi-tion, I am worried about the possibility of poten-tially life-threatening hemorrhagic shock, given the patient’s continued blood loss and profound anemia.
In the emergency department, emphasis is placed on providing the best possible systematic care during the period leading up to the diagno-sis rather than conclusively determining the diag-nosis; nevertheless, I think the diagnosis in this case is Meckel’s diverticulum. In an infant who has massive lower gastrointestinal bleeding with resultant hemodynamic compromise and for whom intussusception has been ruled out on the basis of ultrasonographic findings, the most likely diagnosis is Meckel’s diverticulum, and this possibility needs to be investigated before other diagnoses can be considered.7 The abdominal pain is one aspect of this patient’s clinical pre-sentation that does not totally fit with the diag-nosis of Meckel’s diverticulum, although an ob-struction or perforation could introduce pain into the clinical picture. The description of me-lena is not consistent with Meckel’s diverticulum but could be explained if the bleeding mucosa from the diverticulum was proximal enough for resultant blood to undergo partial digestion.6 It is also possible that the single stool described as melena was not truly melena but stool with darker or maroon blood that originated from a lower, rather than an upper, gastrointestinal source. Mixed gastritis and colitis is less likely than Meckel’s diverticulum overall, and bleeding related to allergic gastrointestinal disease is un-likely to be as acute and severe as the bleeding seen in this case.8 In the emergency department, it is more straightforward to obtain a scan to assess for Meckel’s diverticulum than to perform upper and lower endoscopy; the scan mandates coordination of fewer hospital resources, does not require the administration of anesthesia, and is noninvasive. If a scan were nondiagnostic, I would consider other studies, such as endoscopy or abdominal computed tomography.
Dr. Virginia M. Pierce (Pathology): Dr. Baldwin, what was your impression when you evaluated this patient?
Dr. Katherine R. Baldwin (Pediatric Gastroenter-ology): Our first step was to localize the source of blood loss. Melena is classically thought to reflect upper gastrointestinal bleeding (proximal to the ligament of Treitz), but it can also be
Cases in Primary Care NEJM.org

9
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 2017 1273
Case Records of the Massachusetts Gener al Hospital
caused by more distal lesions, such as lesions in the small bowel and right colon.9 We considered both upper gastrointestinal sources (including variceal bleeding, vascular malformations, and ulcer) and lower gastrointestinal sources (includ-ing colitis, Meckel’s diverticulum, and vascular malformations). We thought that the subacute tempo of this patient’s clinical presentation, the large volume of blood loss, and his age were most consistent with Meckel’s diverticulum. Although Meckel’s diverticulum is commonly thought to be a painless lesion, pain can result from intussusception (with the diverticulum serv-ing as the lead point), intermittent volvulus around associated fibrous bands, or torsion.
We recommended that the patient undergo prompt evaluation by a pediatric surgeon and that a scan to assess for Meckel’s diverticulum be obtained after the administration of a hista-mine H2-receptor antagonist to help retain radio-tracer in the gastric mucosa. We did not think that endoscopy would be immediately useful; although the performance of upper gastrointes-tinal endoscopy is standard for a large volume of blood loss because of the potential for diagnos-tic and therapeutic intervention, most causes of lower gastrointestinal bleeding do not require colonoscopy. Furthermore, colonoscopy in a pa-tient with acute severe bleeding may be techni-cally challenging because of difficulty with visu-alization.10
Clinic a l Di agnosis
Gastrointestinal bleeding due to Meckel’s diver-ticulum.
Dr . L aur en M. A llis ter’s Di agnosis
Gastrointestinal bleeding due to Meckel’s diver-ticulum.
Im aging S t udies
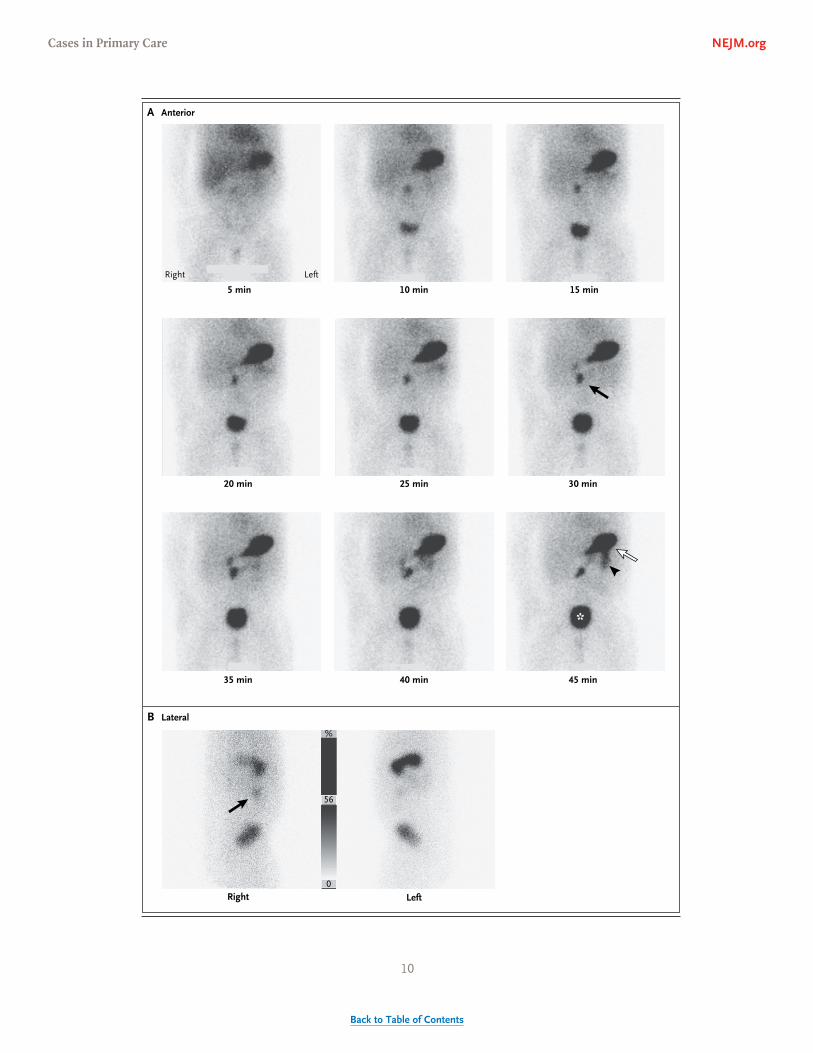
Dr. Lim: After the patient received premedication with intravenous famotidine, a technetium-99m pertechnetate scan was obtained to assess for the presence of a Meckel’s diverticulum. Immedi-ately after the intravenous injection of 0.97 mCi of radiotracer, anterior planar imaging was per-formed continuously for 1 hour. Additional imag-
ing was performed in a lateral view. An abnor-mal focus of radiotracer accumulation was seen in the right paramedian region of the abdomen that gradually increased in intensity over time (Fig. 1); this finding is consistent with ectopic gastric mucosa in a Meckel’s diverticulum.
Technetium-99m pertechnetate normally accu-mulates in any gastric mucosa, including ectopic gastric mucosa; therefore, this radiotracer is use-ful in the evaluation of a suspected Meckel’s di-verticulum. False positive scans can occur. Tech-netium-99m pertechnetate is excreted by the urinary system, and activity is normally seen in the bladder and kidneys. Radiotracer activity in the stomach can pass distally into the duodenum and small bowel. Premedication with a histamine H2-receptor antagonist can reduce the release of radiotracer from the stomach. Bowel or urinary activity is suggested by movement of focal radio-tracer activity over time, whereas focal accumu-lation in a Meckel’s diverticulum should remain fixed in position. A lateral view of the abdomen can be helpful in distinguishing urinary activity in the ureters, which are located in a posterior position. A false positive scan can also result from inflammation, intussusception, bowel ob-struction, or vascular lesions.
A false negative scan can result from the presence of too little or no gastric mucosa in a Meckel’s diverticulum; approximately 20% of Meckel’s diverticula do not contain gastric mu-cosa. Other causes of false negative scans include recent ingestion of barium or perchlorate, move-ment of the Meckel’s diverticulum, and brisk gastrointestinal bleeding.11
Discussion of M a nagemen t
Dr. Allan M. Goldstein: As a result of the clinical presentation and the findings on the scan, the infant was brought to the operating room. A short transverse incision was made in the right lower quadrant, and the diverticulum was identi-fied (Fig. 2). Inflammation and scarring were present at its base; these findings are consistent with ulceration in the small intestine, at its junc-tion with the diverticulum. A segmental small-bowel resection, which included the diverticu-lum and the presumed area of ulceration, was performed, followed by a hand-sewn end-to-end anastomosis.
A variety of operations can be performed to
Cases in Primary Care NEJM.org
10
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 20171274
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
A Anterior
LeftRight
10 min5 min 15 min
20 min 25 min 30 min
35 min 40 min 45 min
*
Right
%
56
0
Left
B Lateral
Cases in Primary Care NEJM.org

11
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 2017 1275
Case Records of the Massachusetts Gener al Hospital
treat a Meckel’s diverticulum that causes gastro-intestinal bleeding. These include simple diver-ticulectomy, wedge resection of the diverticulum and the small cuff of adjacent ileum at its base, and segmental small-bowel resection, which was done in this case. The primary cause of bleeding is the presence of acid-producing ectopic gastric mucosa in the diverticulum, which leads to the development of an ulcer in adjacent normal mu-cosa. The ulcer can be present in the diverticu-lum itself but is usually located at the junction of the diverticulum and the ileum,12 as appeared to be the case in this patient. Although remov-ing both the ectopic mucosa and the ulcer would seem to be the best approach, removing the ec-topic mucosa alone may be sufficient, since the ulcer would probably then heal. However, it is essential to remove all ectopic gastric mucosa, which cannot be reliably detected from the out-side. Therefore, a reasonable approach is to per-form a simple diverticulectomy for a diverticu-lum with a narrow base but to perform a wedge or segmental resection for a diverticulum with a broad base, since ectopic tissue may be left be-hind if the diverticular base is not fully excised. If the area of ulceration is apparent, as in this case, then resecting it with the diverticulum is also reasonable.
An important scenario to consider is whether this patient would have received different treat-ment if the scan had been negative, which could have easily occurred, given the imperfect sensi-tivity of the test.13,14 Meckel’s diverticulum needs to be included in the differential diagnosis for any child being evaluated for hematochezia. If a technetium-99m pertechnetate scan is negative
and other causes of bleeding have been ruled out, laparoscopy should be considered to assess for Meckel’s diverticulum.
Pathol o gic a l Discussion
Dr. Jochen K. Lennerz: We received a segment of small bowel (1.7 cm by 1.5 cm by 1.5 cm) with an attached intact, blind-ending diverticulum (2.5 cm by 0.8 cm by 0.8 cm) for pathological examination. The serosa near the small intestine showed patchy fibrinous inflammation (Fig. 2) and was otherwise mildly hyperemic; the tip of the diverticulum had no attached bands. The sections showed an average wall thickness of 0.2 cm and normally folded mucosa with red discoloration toward the small bowel. In con-trast to the mucosal herniation through the bowel wall that is present in diverticular disease, this diverticulum contained all three layers of bowel wall. Given the anatomical location of the diverticulum on the antimesenteric surface of the mid-ileum, these findings represent per-sistence of a proximal part of the vitelline duct (omphalomesenteric duct), or Meckel’s diver-ticulum.
A histotopogram allowed us to perform a
Figure 2. Intraoperative Photograph.
After a short transverse incision was made in the right lower quadrant, the diverticulum was identified. Inflam‑mation and scarring are present at the base of the diver‑ticulum; these findings are consistent with ulceration in the small intestine, at its junction with the diverticu‑lum. Photograph courtesy of Dr. David Lawlor.
Figure 1 (facing page). Technetium-99m Pertechnetate Scan of the Abdomen.
A technetium‑99m pertechnetate scan of the abdomen was performed to assess for Meckel’s diverticulum. Anterior planar images (Panel A), which were obtained continuously for 1 hour, show an abnormal focus of ra‑diotracer accumulation in the right paramedian region of the abdomen that gradually increases in intensity over time (black arrow). Physiological radiotracer accu‑mulation is present in the stomach (white arrow), bow‑el (arrowhead), and bladder (asterisk). Lateral planar images (Panel B) confirm that the abnormal focus of radiotracer accumulation (arrow) is in a location that is compatible with bowel activity and is not consistent with urinary activity, which would be more posterior.
Cases in Primary Care NEJM.org
12
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 20171276
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
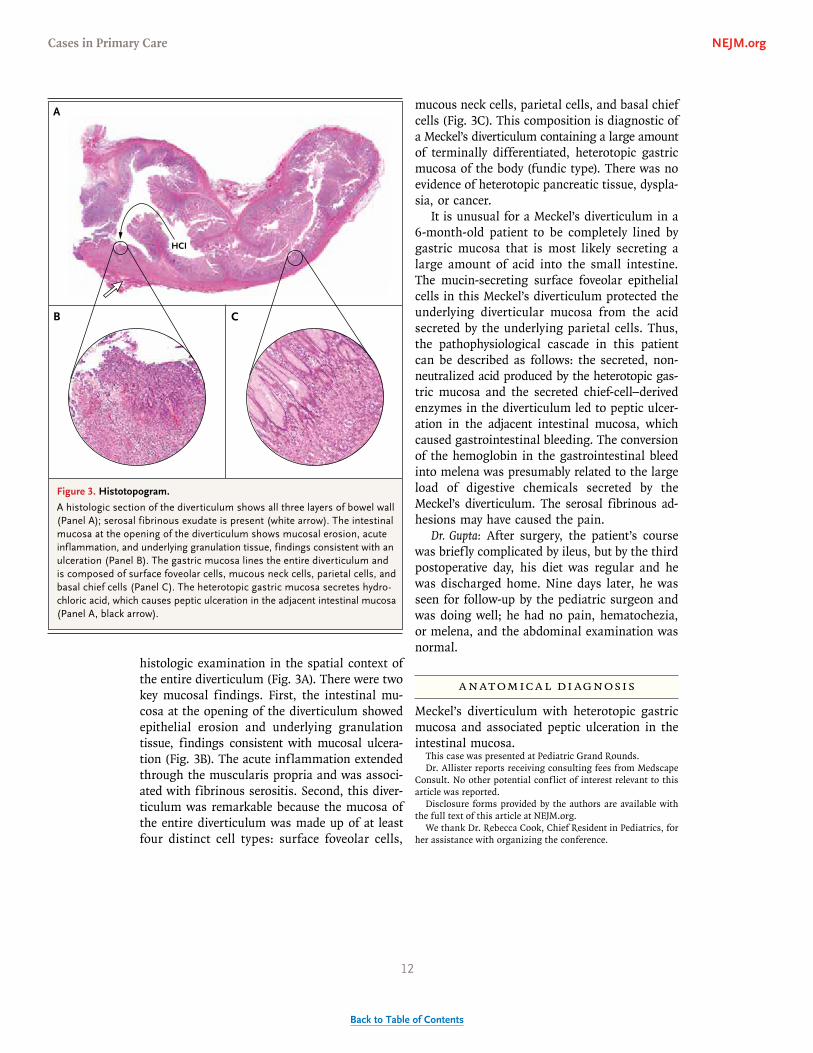
histologic examination in the spatial context of the entire diverticulum (Fig. 3A). There were two key mucosal findings. First, the intestinal mu-cosa at the opening of the diverticulum showed epithelial erosion and underlying granulation tissue, findings consistent with mucosal ulcera-tion (Fig. 3B). The acute inflammation extended through the muscularis propria and was associ-ated with fibrinous serositis. Second, this diver-ticulum was remarkable because the mucosa of the entire diverticulum was made up of at least four distinct cell types: surface foveolar cells,
mucous neck cells, parietal cells, and basal chief cells (Fig. 3C). This composition is diagnostic of a Meckel’s diverticulum containing a large amount of terminally differentiated, heterotopic gastric mucosa of the body (fundic type). There was no evidence of heterotopic pancreatic tissue, dyspla-sia, or cancer.
It is unusual for a Meckel’s diverticulum in a 6-month-old patient to be completely lined by gastric mucosa that is most likely secreting a large amount of acid into the small intestine. The mucin-secreting surface foveolar epithelial cells in this Meckel’s diverticulum protected the underlying diverticular mucosa from the acid secreted by the underlying parietal cells. Thus, the pathophysiological cascade in this patient can be described as follows: the secreted, non-neutralized acid produced by the heterotopic gas-tric mucosa and the secreted chief-cell–derived enzymes in the diverticulum led to peptic ulcer-ation in the adjacent intestinal mucosa, which caused gastrointestinal bleeding. The conversion of the hemoglobin in the gastrointestinal bleed into melena was presumably related to the large load of digestive chemicals secreted by the Meckel’s diverticulum. The serosal fibrinous ad-hesions may have caused the pain.
Dr. Gupta: After surgery, the patient’s course was briefly complicated by ileus, but by the third postoperative day, his diet was regular and he was discharged home. Nine days later, he was seen for follow-up by the pediatric surgeon and was doing well; he had no pain, hematochezia, or melena, and the abdominal examination was normal.
A nat omic a l Di agnosis
Meckel’s diverticulum with heterotopic gastric mucosa and associated peptic ulceration in the intestinal mucosa.
This case was presented at Pediatric Grand Rounds.Dr. Allister reports receiving consulting fees from Medscape
Consult. No other potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
We thank Dr. Rebecca Cook, Chief Resident in Pediatrics, for her assistance with organizing the conference.
References1. Sagar J, Kumar V, Shah DK. Meckel’s diverticulum: a systematic review. J R Soc Med 2006; 99: 501-5.
2. Pepper VK, Stanfill AB, Pearl RH. Di-agnosis and management of pediatric ap-pendicitis, intussusception, and Meckel
diverticulum. Surg Clin North Am 2012; 92: 505-26.3. Park JJ, Wolff BG, Tollefson MK, Walsh
Figure 3. Histotopogram.
A histologic section of the diverticulum shows all three layers of bowel wall (Panel A); serosal fibrinous exudate is present (white arrow). The intestinal mucosa at the opening of the diverticulum shows mucosal erosion, acute inflammation, and underlying granulation tissue, findings consistent with an ulceration (Panel B). The gastric mucosa lines the entire diverticulum and is composed of surface foveolar cells, mucous neck cells, parietal cells, and basal chief cells (Panel C). The heterotopic gastric mucosa secretes hydro‑chloric acid, which causes peptic ulceration in the adjacent intestinal mucosa (Panel A, black arrow).
B C
A
HCI
Cases in Primary Care NEJM.org

13
BacktoTableofContents
n engl j med 376;13 nejm.org March 30, 2017 1277
Case Records of the Massachusetts Gener al Hospital
EE, Larson DR. Meckel diverticulum: the Mayo Clinic experience with 1476 patients (1950-2002). Ann Surg 2005; 241: 529-33.4. Yahchouchy EK, Marano AF, Etienne JC, Fingerhut AL. Meckel’s diverticulum. J Am Coll Surg 2001; 192: 658-62.5. Itriyeva K, Harris M, Rocker J, Goch-man R. Not just painless bleeding: Meck-el’s diverticulum as a cause of small bowel obstruction in children — two cases and a review of the literature. Case Rep Emerg Med 2015; 2015: 938346.6. Poley JR, Thielen TE, Pence JC. Bleed-ing Meckel’s diverticulum in a 4-month-old infant: treatment with laparoscopic diverticulectomy — a case report and re-view of the literature. Clin Exp Gastroen-terol 2009; 2: 37-40.
7. Teach SJ, Fleisher GR. Rectal bleeding in the pediatric emergency department. Ann Emerg Med 1994; 23: 1252-8.8. Arvola T, Ruuska T, Keränen J, Hyöty H, Salminen S, Isolauri E. Rectal bleeding in infancy: clinical, allergological, and mi-crobiological examination. Pediatrics 2006; 117(4): e760-e768.9. Zuckerman GR, Trellis DR, Sherman TM, Clouse RE. An objective measure of stool color for differentiating upper from lower gastrointestinal bleeding. Dig Dis Sci 1995; 40: 1614-21.10. Thomson M, Tringali A, Dumonceau JM, et al. Paediatric gastrointestinal endos-copy: European Society for Paediatric Gastroenterology, Hepatology, and Nutri-tion and European Society of Gastrointes-
tinal Endoscopy guidelines. J Pediatr Gas-troenterol Nutr 2017; 64: 133-53.11. Spottswood SE, Pfluger T, Bartold SP, et al. SNMMI and EANM practice guide-line for Meckel diverticulum scintigraphy 2.0. J Nucl Med Technol 2014; 42: 163-9.12. Cobb DB. Meckel’s diverticulum with peptic ulcer. Ann Surg 1936; 103: 747-68.13. Al Janabi M, Samuel M, Kahlenberg A, Kumar S, Al-Janabi M. Symptomatic pae-diatric Meckel’s diverticulum: stratified diagnostic indicators and accuracy of Meckel’s scan. Nucl Med Commun 2014; 35: 1162-6.14. Tseng YY, Yang YJ. Clinical and diag-nostic relevance of Meckel’s diverticulum in children. Eur J Pediatr 2009; 168: 1519-23.Copyright © 2017 Massachusetts Medical Society.
Lantern SLideS Updated: CompLete powerpoint SLide SetS from the CLiniCopathoLogiCaL ConferenCeS
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
Cases in Primary Care NEJM.org

14
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017268
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Pr esen tation of C a se
Dr. Carolyn A. Boscia (Medicine and Pediatrics): An 18-year-old woman was seen in the emergency department of this hospital 11 weeks after the birth of her first child because of acute liver failure.
The patient had been well until 1 week before this presentation, when rhinor-rhea, sore throat, and cough developed. On the fourth day of illness, she was seen in an urgent care clinic because of worsening cough, wheezing, and dyspnea. Bronchitis was diagnosed, and promethazine–dextromethorphan syrup and a 5-day course of oral azithromycin were prescribed. The patient returned home.
Over the next 3 days, abdominal discomfort, nausea, vomiting, diarrhea, and vaginal bleeding developed. The patient also noted progressive yellowing of her skin and eyes. When she woke up on the morning of the current presentation, she felt light-headed. When she arose from bed, syncope occurred; the patient fell and had a laceration of the chin. Her boyfriend called emergency medical services (EMS), and a team was dispatched to the patient’s home.
On assessment by EMS personnel, the patient had jaundice and diaphoresis. She appeared fatigued. The pulse was 120 beats per minute, the blood pressure 82/56 mm Hg, the respiratory rate 22 breaths per minute, and the oxygen satura-tion 100% while she was breathing ambient air. Nystagmus occurred on right lateral gaze. The abdomen was distended, and tenderness was present in the right lower quadrant. The capillary blood glucose level was 121 mg per deciliter (6.7 mmol per liter), and an electrocardiogram showed sinus tachycardia. Intravenous fluids and supplemental oxygen (through a nasal cannula at a rate of 2 liters per minute) were administered, and the patient was transported to the emergency department of another hospital.
On arrival at the other hospital, the patient reported burning abdominal pain, which she rated at 10 on a scale of 0 to 10, with 10 indicating the most severe pain. The temperature was 37.0°C, the pulse 88 beats per minute, the blood pres-
From the Departments of Medicine (K.R.O., E.A.S.), Pediatrics (K.R.O.), Radi-ology (A.H.D.), Surgery (N.E.), and Pathol-ogy (J.M.), Massachusetts General Hos-pital, and the Departments of Medicine (K.R.O., E.A.S.), Pediatrics (K.R.O.), Radi-ology (A.H.D.), Surgery (N.E.), and Pathol-ogy (J.M.), Harvard Medical School — both in Boston.
N Engl J Med 2017;376:268-78.DOI: 10.1056/NEJMcpc1613467Copyright © 2017 Massachusetts Medical Society.
Founded by Richard C. Cabot
Eric S. Rosenberg, M.D., Nancy Lee Harris, M.D., Editors Virginia M. Pierce, M.D., David M. Dudzinski, M.D., Meridale V. Baggett, M.D.,
Dennis C. Sgroi, M.D., Jo-Anne O. Shepard, M.D., Associate EditorsEmily K. McDonald, Sally H. Ebeling, Production Editors
Case 2-2017: An 18-Year-Old Woman with Acute Liver Failure
Kristian R. Olson, M.D., Amir H. Davarpanah, M.D., Esperance A. Schaefer, M.D., M.P.H., Nahel Elias, M.D.,
and Joseph Misdraji, M.D.
Case Records of the Massachusetts General Hospital
Cases in Primary Care NEJM.org

15
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017 269
Case Records of the Massachusetts Gener al Hospital
sure 107/42 mm Hg, the respiratory rate 24 breaths per minute, and the oxygen saturation 100% while she was breathing ambient air. The abdo-men was soft, with tenderness on the right side, and there was trace edema of the legs. The results of the examination were otherwise un-changed. The blood carbon dioxide level was 21 mmol per liter (reference range, 24 to 34), and the blood glucose level was 104 mg per deciliter (5.8 mmol per liter; reference range, 70 to 100 mg per deciliter [3.9 to 5.6 mmol per liter]). The anion gap and blood levels of sodium, potassium, and chloride were normal, as were the results of renal-function tests and a serum toxicology screen, which included a test for acetaminophen. Other laboratory test results are shown in Table 1.
Dr. Amir H. Davarpanah: A chest radiograph and a computed tomographic (CT) scan of the head (obtained without the administration of intrave-nous contrast material) were normal. Ultrasonog-raphy of the abdomen revealed mildly increased hepatic parenchymal echogenicity (Fig. 1A). This finding, although nonspecific, could reflect he-patic steatosis or diffuse parenchymal disease. No focal liver lesions were identified. The gall-bladder was distended, with apparent wall ede-ma, a small amount of pericholecystic fluid, and layering sludge (Fig. 1B). The common bile duct was normal in diameter, with no intrahepatic biliary ductal dilatation (Fig. 1C). The spleen was mildly enlarged, to a greatest longitudinal diam-eter of 13 cm (normal, ≤12).
Dr. Boscia: Intravenous fluids, piperacillin–tazo-bactam, morphine, ondansetron, and N-acetyl-cysteine were administered, and packed red cells were transfused. Five hours after arrival at the other hospital, the patient was transferred to the emergency department of this hospital.
In the emergency department, the patient re-ported that the abdominal pain and light-headed-ness had resolved and the nausea had decreased. She recalled that during the past several days, her gums had bled easily when she brushed her teeth and her urine had been tea-colored. She had a history of mild asthma. Eleven weeks ear-lier, she had given birth to her first child; after an otherwise uncomplicated pregnancy, preterm labor developed and was complicated by placen-tal abruption, and vaginal delivery occurred at 32 weeks of gestation. The patient reported that she had remained in the hospital for 1 week af-
ter delivery because of unspecified abnormal laboratory test results. Her medications were albuterol as needed, azithromycin, and prometha-zine–dextromethorphan syrup; she did not take herbal remedies or supplements and had no known allergies. Immunizations were reportedly current.
Six weeks before this presentation, the patient had moved to an urban area of New England where she currently lived with her daughter, boy-friend, and boyfriend’s parents. She was of South-east Asian descent and had been born in the United States. She did not smoke tobacco, use illicit drugs, or drink alcohol. A grandmother had unspecified liver disease.
On examination, the patient appeared tired and had marked jaundice. The temperature was 37.6°C, the pulse 90 beats per minute, the blood pressure 100/58 mm Hg, the respiratory rate 18 breaths per minute, and the oxygen saturation 100% while she was breathing ambient air. Con-junctival icterus was present. The abdomen was soft, with mild epigastric tenderness; abdominal guarding, rebound tenderness, and Murphy’s sign were absent. There was a 1.5-cm laceration on the chin. The remainder of the physical exami-nation was normal. Examination of a peripheral-blood smear revealed smudge cells, burr cells, basophilic stippling, rouleaux formation, dysplas-tic neutrophils, and 1+ polychromasia. The anion gap, venous blood-gas measurements, and results of renal-function tests were normal, as were blood levels of sodium, potassium, chloride, car-bon dioxide, magnesium, glucose, amylase, lipase, and fibrinogen; additional laboratory test results are shown in Table 1. Testing for urinary human chorionic gonadotropin was negative. A serum toxicology screen was negative, and a urine toxicology screen was positive for opiates and negative for all other analytes. Urinalysis re-vealed slightly cloudy, amber-colored urine with a specific gravity of 1.019, a pH of 6.0, 2+ bili-rubin, 2+ urobilinogen, and 1+ occult blood by dipstick; there were 0 to 2 white cells and 0 to 2 red cells per high-power field. An electrocar-diogram showed sinus tachycardia.
Dr. Davarpanah: Doppler ultrasonography of the abdomen revealed persistent evidence of wall edema and intraluminal sludge in the gallblad-der. Murphy’s sign was absent, although this finding was not reliable because of the prior
Cases in Primary Care NEJM.org

16
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017270
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
VariableReference Range, Other Hospital
On Presentation, Other Hospital
Reference Range, This Hospital†
On Presentation, This Hospital
Hematocrit (%) 36–48 19.6 36.0–46.0 23.4
Hemoglobin (g/dl) 12.0–15.8 6.4 12.0–16.0 7.9
White-cell count (per mm3) 4.8–11.2 10.1 4.5–13.0 11.1
Differential count (%)
Neutrophils 45–85 72 40–62 77
Band forms 0–8 5
Lymphocytes 15–45 10 27–40 9
Monocytes 0–12 6 4–11 10
Eosinophils 0–7 1 0–8 1
Myelocytes 0 4 0 2
Metamyelocytes 0 2 0 1
Platelet count (per mm3) 150,000–400,000 140,000 150,000–400,000 175,000
Red-cell count (per mm3) 3,600,000–5,400,000 1,720,000 4,000,000–5,200,000 2,210,000
Nucleated red-cell count (per 100 white cells) 0 0 0 1
Mean corpuscular volume (fl) 82–98 113.8 80.0–100.0 105.9
Mean corpuscular hemoglobin (pg/red cell) 27.0–35.0 37.4 26.0–34.0 35.7
Mean corpuscular hemoglobin concentration (g/dl) 32.0–37.0 32.9 31.0–37.0 33.8
Red-cell distribution width (%) 9.0–17.9 22.1 11.5–14.5 24.4
Direct antiglobulin test Negative Negative
Prothrombin time (sec) 11.0–14.0 24.5
Prothrombin-time international normalized ratio 0.9–1.1 2.6 0.9–1.1 2.1
Activated partial-thromboplastin time (sec) 22.0–35.0 43.4
d-Dimer (ng/ml) <500 591
Calcium (mg/dl) 8.7–10.5 7.2 8.5–10.5 7.2
Phosphorus (mg/dl) 2.6–4.5 1.8
Total protein (g/dl) 6.4–8.6 5.5 6.0–8.3 5.3
Albumin (g/dl) 3.4–4.8 2.1 3.3–5.0 2.2
Globulin (g/dl) 1.9–4.1 3.1
Alanine aminotransferase (U/liter) 0–45 20 7–33 24
Aspartate aminotransferase (U/liter) 0–40 152 9–32 152
Alkaline phosphatase (U/liter) 40–150 22 15–350 14
Total bilirubin (mg/dl) 0.2–1.2 19.7 0–1.0 26.3
Direct bilirubin (mg/dl) 0–0.4 21.9
γ-Glutamyltransferase (U/liter) 5–36 116
Lactate dehydrogenase (U/liter) 110–210 344
Lactic acid (mmol/liter) 0.5–2.2 3.9 0.5–2.2 1.7
Ammonia (μmol/liter) 12–48 49
* To convert the values for calcium to millimoles per liter, multiply by 0.250. To convert the values for phosphorus to millimoles per liter, multiply by 0.3229. To convert the values for bilirubin to micromoles per liter, multiply by 17.1. To convert the values for lactic acid to milli-grams per deciliter, divide by 0.1110. To convert the values for ammonia to micrograms per deciliter, divide by 0.5872.
† Reference values are affected by many variables, including the patient population and the laboratory methods used. The ranges used at Massachusetts General Hospital are for adults who are not pregnant and do not have medical conditions that could affect the results. They may therefore not be appropriate for all patients.
Table 1. Laboratory Data.*
Cases in Primary Care NEJM.org

17
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017 271
Case Records of the Massachusetts Gener al Hospital
administration of analgesic agents. Pulsed-wave Doppler ultrasonography revealed normal arte-rial flow in the main hepatic artery (Fig. 1D). There was also normal hepatopetal flow in the
portal veins (Fig. 1E) and hepatofugal flow in the hepatic veins (Fig. 1F).
Dr. Boscia: The administration of N-acetylcys-teine was continued, and the chin laceration was
Figure 1. Abdominal Ultrasound Images.
Grayscale ultrasound images show mildly echogenic parenchyma of the liver (Panel A) and distention of the gall-bladder, with layering sludge, wall edema, and a small amount of pericholecystic fluid (Panel B). A color Doppler ultrasound image shows that the common bile duct is normal in diameter (Panel C). Pulsed-wave Doppler ultra-sound images show normal flow of the hepatic artery (Panel D), portal veins (Panel E), and hepatic veins (Panel F).
A B
DC
FE
Cases in Primary Care NEJM.org

18
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017272
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
sutured. Additional laboratory tests were per-formed, and a diagnosis was made.
Differ en ti a l Di agnosis
Dr. Kristian R. Olson: This previously healthy 18- year-old woman presented 11 weeks after the birth of her first child with evidence of worsen-ing liver failure after a nonspecific 7-day illness. To develop a differential diagnosis, it is impor-tant to determine whether the patient’s liver dysfunction is consistent with a diagnosis of acute liver failure.
Acute Liver Failure
Acute liver failure in adults is characterized by a sudden loss of hepatic function without evidence of preexisting liver disease. Criteria for the diag-nosis include the presence of coagulopathy (inter-national normalized ratio [INR], >1.5), hepatic encephalopathy, and an illness of less than 24 weeks’ duration.1 This patient has evidence of liver injury and an INR well above 1.5. She does not have features of encephalopathy, such as al-tered consciousness, compromised intellectual functioning, tremors, or asterixis, and thus she may meet only the criteria for acute liver injury. However, in the pediatric population (which can be considered to include patients who are up to
21 years of age), up to 50% of patients who pre-sent with acute liver failure do not present with encephalopathy.2 Modified criteria for the diag-nosis of acute liver failure in children include evidence of acute liver injury and severe coagu-lopathy (INR, >2.0) in the absence of encepha-lopathy. Given this patient’s age, I would argue that she meets the criteria for acute liver failure.
A specific diagnosis is important in deter-mining prognosis, guiding treatment, and coun-seling the patient’s relatives. Using data derived from several large, multicenter series involving the Pediatric Acute Liver Failure Study Group and the Acute Liver Failure Study Group, we can construct lists of recognized causes of acute liver failure in children older than 10 years of age and in adults.1,3 Because this patient is at the threshold of adulthood, we need to consider the causes in each population (Fig. 2).
This patient has nonspecific symptoms and findings on physical examination, and so it might seem futile to arrive at a specific diagnosis. However, the presence or absence of relatively elevated values on routine laboratory tests can help immensely. She has an aspartate amino-transferase level that is nearly 5 times the upper limit of the normal range, whereas the alanine aminotransferase level is not elevated at all. The direct bilirubin level is more than 26 times the
Figure 2. Causes of Acute Liver Failure in Children and Adults.
Data are adapted from Lee et al.1 and Squires and Alonso.3 The numbers shown are percentages. Among children older than 10 years of age, Wilson’s disease accounted for 90% of metabolic disease.
Metabolic disease, 9
Wilson'sdisease, 2
Autoimmunedisease, 5
Ischemia, 4
Drug-inducedliver injury, 11
Hepatitis A or Bvirus infection, 10
Other cause, 7
Autoimmunedisease, 10
Viral hepatitis, 5
Shock or ischemia, 3
Drug-inducedliver injury, 7
Veno-occlusive disease, 2
Other cause, 2
Multiple causes, 1 Indeterminatecause, 14
3%
Indeterminatecause, 32
Acetaminophenexposure, 29
Children >10 Yr of Age
Acetaminophenexposure, 47
Adults
Cases in Primary Care NEJM.org

19
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017 273
Case Records of the Massachusetts Gener al Hospital
upper limit of the normal range, with the major-ity being conjugated bilirubin (22 mg per deciliter [374.5 μmol per liter]). Cholestasis, which repre-sents a decrease in bile flow caused by either impaired secretion of hepatocytes or obstruc-tion, is heralded by prominent elevations in the bilirubin level and in the alkaline phosphatase or γ-glutamyltransferase level. Despite the direct hyperbilirubinemia in this patient, the alkaline phosphatase level is below the normal range. However, with a γ-glutamyltransferase level of more than 3 times the upper limit of the normal range, evidence of a cholestatic pattern remains.
Acetaminophen Exposure
Although a serum acetaminophen level was un-detectable in this patient on presentation, it is important to maintain suspicion for either inad-vertent chronic ingestion or an acute one-time ingestion several days before presentation. The Rumack–Matthew nomogram, which is used to assess for potential hepatotoxicity after an acet-aminophen exposure, is developed to assess only for acute, single ingestions. The prevalence of postpartum depression is approximately 10%,4 and young age and unplanned pregnancy have been identified as risk factors. Although this patient could have ingested acetaminophen 48 to 72 hours before presentation and had an unde-tectable level on presentation, there is no history of a psychiatric illness, which might suggest the possibility of an intentional overdose. In addi-tion, the mechanism of acetaminophen hepato-toxicity is centrilobular necrosis, which is caused by the accumulation of N-acetyl-p-benzoquinone imine. The hallmark of liver injury is markedly elevated aminotransferase levels, which are usu-ally in the thousands and frequently 400 times the upper limit of the normal range. This bio-chemical feature is not consistent with this pa-tient’s laboratory test results. However, she re-ceived treatment with N-acetylcysteine, which results in increased survival even among pa-tients with acute liver failure that is unrelated to acetaminophen exposure.5
Drug-Induced Liver Injury
Idiosyncratic hepatic reactions to medications other than acetaminophen and to complemen-tary or alternative therapies are referred to as drug-induced liver injury. In adults, 11% of cases
of acute liver failure are caused by drug-induced liver injury. This patient did not report use of over-the-counter medication; however, it is im-portant to confirm that she includes dietary and nutritional supplements as over-the-counter med-ications. She began taking azithromycin and promethazine–dextromethorphan 3 days before the current presentation. Antimicrobial therapy is the most frequent cause of drug-induced liver injury, and in particular, the incidence of azith-romycin-associated hepatic injury is increasing. Drug-induced liver injury affects women in 72% of cases and results in hepatocellular injury in 61% of cases.6 A cholestatic pattern can arise but typically does so 1 to 3 weeks after the patient has started a new medication. In addition, eosino-philia and fever are typical features of drug-induced liver injury that are not present in this patient. Furthermore, the time between the ini-tiation of azithromycin therapy and the develop-ment of acute liver failure in this patient was only a few days, which makes the diagnosis of drug-induced liver injury unlikely.
Pregnancy
During pregnancy, dilutional hypoalbuminemia and elevation of the placental-derived alkaline phosphatase level can lead providers to falsely assume that the patient has liver disease. How-ever, the elevations of the aspartate aminotrans-ferase level, INR, and γ-glutamyltransferase level in this patient are uniformly abnormal. Eclamp-sia affects 2 to 8% of pregnant women and can occur up to 6 weeks post partum, but this pa-tient’s symptoms developed later. Furthermore, in pregnant women, the aminotransferase levels are typically 10 to 20 times the upper limit of the normal range and the bilirubin level is typically less than 5 mg per deciliter (85.5 μmol per liter); also, the alkaline phosphatase level in this pa-tient is higher than would be expected during pregnancy.
The HELLP syndrome (hemolysis, elevated liv-er enzyme levels, and a low platelet count) occurs in less than 1% of pregnant women, and only one third of cases occur after delivery.7 In this case, examination of a peripheral-blood smear did not reveal typical features of hemolysis, al-though the presence of indirect hyperbilirubine-mia may suggest a hemolytic process. However, the patient’s platelet count was normal, and thus
Cases in Primary Care NEJM.org

20
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017274
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
the diagnosis of the HELLP syndrome is un-likely.
Ischemic Hepatopathy
Although the patient had hypotension when the EMS team arrived, the hemodynamic insult in ischemic hepatopathy is normally present well before evidence of liver injury. In addition, the typical biochemical profile of ischemic hepatopa-thy includes a dramatic rise in aminotransferase and lactate dehydrogenase levels and normal or only mildly abnormal hepatic synthetic function. The Budd–Chiari syndrome, or hepatic venous outflow obstruction, is another consideration because the pooled prevalence during pregnancy and the puerperium is approximately 6.8%.8 However, acute liver failure develops in less than 5% of patients with the Budd–Chiari syndrome. In addition, although the aminotransferase levels may be only moderately elevated (as in this patient), the bilirubin level is seldom higher than 7 mg per deciliter (119.7 μmol per liter), whereas the bilirubin level in this patient is higher than 20 mg per deciliter (342.0 μmol per liter). This patient also had a normal vascular Doppler ultrasound evaluation, which rules out the diagnosis of the Budd–Chiari syndrome.
Viral Infection
Viral hepatitis is the cause of acute liver failure in 10% of cases in developed countries. It is inter-esting to note that this patient’s grandmother had “unspecified liver disease” and that the pa-tient is of Southeast Asian descent. In the United States, the rate of chronic hepatitis B virus infec-tion is 6% among pregnant women of Asian descent versus only 0.6% among pregnant white women. An exacerbation of hepatopathy can oc-cur as the result of the relative immunosuppres-sion associated with pregnancy. However, if this patient received prenatal care, she would have been screened for hepatitis B virus. In addition, she had no fever and few risk factors for acute hepatitis B virus infection, and viral hepatitis typically results in aminotransferase levels that are more than 25 times the upper limit of the normal range.
Autoimmune Hepatitis
Autoimmune hepatitis is a chronic, progressive disorder, but it can also cause acute liver failure.9
Patients with autoimmune hepatitis typically present with nonspecific symptoms, including fatigue, lethargy, malaise, anorexia, nausea, ab-dominal pain, and itching.10 Symptoms may first become evident during pregnancy, and postpar-tum exacerbations do occur. However, some fea-tures of autoimmune hepatitis are absent in this patient, including coexisting autoimmune condi-tions, associated small-joint arthralgias, and the typical pattern of markedly elevated aminotrans-ferase levels. In addition, she does not have ele-vated globulin levels (which typically correlate with IgG levels, even in the setting of acute liver failure).11 Given that the patient is female and her ratio of alkaline phosphatase (IU per liter) to aspartate aminotransferase (IU per liter) is lower than 1.5, her globulin level is not elevated, and there is no evidence of illicit-drug or excessive alcohol use, we can calculate that she has a score on the scoring system of the International Autoimmune Hepatitis Group of 7 (on a scale ranging from –20 to 31, with a score of 10 to 15 indicating probable autoimmune hepatitis and a score higher than 15 indicating definite auto-immune hepatitis).9 Although the information we are given at this point is inadequate to allow us to completely calculate the score and defini-tively rule out the possibility of autoimmune hepatitis, it makes this diagnosis unlikely.
Wilson’s Disease
Wilson’s disease, also known as hepatolenticular degeneration, is an autosomal recessive disease characterized by impaired copper metabolism due to a defective ATPase. The mean age at onset ranges from 12 to 23 years, and this patient’s age falls within that range. Patients with Wilson’s disease may present with chronic liver disease, acute liver failure, hemolysis, and psychiatric or neurologic manifestations. The Leipzig criteria for Wilson’s disease might be helpful in deter-mining the diagnosis in this patient, but we are not given the results of biochemical tests for copper or genetic testing.12
Fortunately, rapid diagnostic criteria for Wil-son’s disease can be used in patients who pre-sent with acute liver failure. A screen that shows a ratio of alkaline phosphatase (IU per liter) to total bilirubin (mg per deciliter) of lower than 4.0 and then subsequently shows a ratio of aspar-tate aminotransferase (IU per liter) to alanine
Cases in Primary Care NEJM.org

21
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017 275
Case Records of the Massachusetts Gener al Hospital
aminotransferase (IU per liter) of higher than 2.2 has been described as 100% sensitive and specific for the diagnosis of Wilson’s disease.13 According to these criteria, this patient has a presumptive diagnosis of Wilson’s disease. Fur-thermore, patients with acute liver failure who have Wilson’s disease have a median alkaline phosphatase level of 20.5 U per liter, as com-pared with a median level of 146.5 U per liter among patients with acute liver failure who do not have Wilson’s disease. This patient’s alkaline phosphatase level was 22.0 U per liter.
In Wilson’s disease, acute liver failure devel-ops in the setting of subclinical chronic liver disease. If liver transplantation is not performed, acute liver failure due to Wilson’s disease is fatal. I believe that serum copper and 24-hour urinary copper levels were most likely obtained to con-firm the diagnosis of Wilson’s disease in this patient and that, if she survived, she underwent liver transplantation.
Dr. Virginia M. Pierce (Pathology): Dr. Schaefer, what was your impression when you evaluated this patient?
Dr. Esperance A. Schaefer: The hepatology service was consulted after the patient’s arrival at the emergency department. The pattern of liver injury — including minimal elevation of aminotrans-ferase levels, marked hyperbilirubinemia, and a low-to-normal alkaline phosphatase level — did not fit neatly into a hepatocellular or cholestatic pattern. These biochemical findings, combined with the parenchymal changes observed on ultra-sonography, suggested preexisting chronic liver disease with superimposed acute liver injury.
Given that this patient was taking azithromy-cin, we considered the diagnosis of drug-induced liver injury.13,14 However, several clinical features in this case strongly suggested an alternative diagnosis. The patient’s age, sex, possible hemo-lytic anemia, and low alkaline phosphatase level raised strong clinical suspicion for Wilson’s disease. We used the rapid diagnostic criteria for Wilson’s disease,13 and the ratio of alkaline phosphatase to total bilirubin was 0.5 and the ratio of aspartate aminotransferase to alanine aminotransferase was 6.3; these findings sug-gest that a diagnosis of Wilson’s disease could be made with 100% sensitivity and specificity. It has been previously noted that viral infection or drug toxicity may serve as a trigger for fulmi-
nant Wilson’s disease.15 In this patient, there-fore, either the antecedent illness or treatment with azithromycin may have played a role.
The revised Wilson’s disease prognostic index is highly accurate in predicting death due to fulminant Wilson’s disease in both children and adults.16,17 A score higher than 11 portends death if the patient does not undergo transplantation, and in this patient, the score was 14. Given the patient’s vanishingly low likelihood of survival, we recommended admission to the intensive care unit (ICU) and immediate evaluation for orthotopic liver transplantation.
After the patient was admitted to the ICU, the 24-hour urinary copper level was obtained. She underwent a slit-lamp examination, and there was no evidence of Kayser–Fleischer rings. Because she had intact renal function, chelation therapy with penicillamine was initiated to promote uri-nary copper excretion as a bridging measure while she awaited transplantation.
During hospital days 2 through 4, additional testing was performed. The patient’s serum copper level was normal (0.96 μg per milliliter [15.1 μmol per liter]; reference range, 0.75 to 1.45 [11.8 to 22.8 μmol per liter]), her cerulo-plasmin level was low (8 mg per milliliter; refer-ence range, 20 to 60), and her 24-hour urinary copper level was markedly elevated (1419 μg per specimen; reference range, 15 to 60). Her coagu-lopathy worsened, and confusion and hyperam-monemia developed. Shortly after the patient was placed on the liver transplantation list, a donor was identified, and the patient underwent ortho-topic liver transplantation that day.
Clinic a l Di agnosis
Fulminant hepatic failure due to Wilson’s disease.
Dr . K r is ti a n R . Ol son’s Di agnosis
Wilson’s disease (hepatolenticular degeneration).
Pathol o gic a l Discussion
Dr. Joseph Misdraji: On examination of the ex-planted liver, the cut surface was mottled and had a subtle nodular appearance, with scattered regenerative nodules that varied in color from
Cases in Primary Care NEJM.org

22
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017276
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
Figure 3. Explanted Liver.
A photograph of the cut surface of the liver shows a mottled appearance, with several regenerative nodules that vary in color from tannish-brown to yellow (Panel A). Hematoxylin and eosin staining shows that the parenchyma has a nodular appearance and widespread inflammation (Panel B). At higher magnification, the hepatocytes have relatively abundant eosinophilic cytoplasm and cytoplasmic vacuolization at the periphery of the cell (Panel C). Several central veins have endophlebitis, with mononuclear infiltrates in the endothelium of the veins (Panel D). A trichrome stain for collagen highlights a portal tract with pale, bluish-gray septa that are indicative of collapse and fibrosis (Panel E). A rhodanine stain for copper shows copper deposition (reddish granules) in hepatocytes in a nodule (Panel F).
A B
DC
FE
Cases in Primary Care NEJM.org

23
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017 277
Case Records of the Massachusetts Gener al Hospital
tannish-brown to yellow (Fig. 3A). On micro-scopic examination, the parenchyma was nodu-lar and had moderate inflammation, and some nodules were steatotic (Fig. 3B). At higher mag-nification, the hepatocytes had abundant eosin-ophilic cytoplasm, and many of them showed vacuolization of the cytoplasm (Fig. 3C). Portal tracts showed mononuclear inflammation and occasional plasma cells. Several hepatic veins showed endophlebitis, with mononuclear cells infiltrating the endothelium (Fig. 3D); this par-ticular feature has been described only rarely in Wilson’s disease.18 A trichrome stain highlighted septa, which did not have the dense, blue stain-ing typical of established cirrhosis but rather had pale, bluish-gray staining, which is suggestive of fibrosis and collapse (Fig. 3E). A rhodanine stain for copper was performed, and copper was iden-tified in hepatocytes in a few nodules (Fig. 3F). The pathological diagnosis of Wilson’s disease is generally based on the presence of compatible histomorphologic features and results of stain-ing for copper, including a rhodanine stain. How-ever, staining for copper in tissue is unreliable, since the presence of copper in the cytoplasm of hepatocytes might not be detected on a rhodanine stain.19 Therefore, in patients with suspected Wil-son’s disease, copper quantification performed on either a dedicated core-biopsy specimen or a paraffin-embedded tissue sample is considered to be the best available diagnostic test.20 A value of 30 μg per gram of dry weight is normal, and a diagnosis of Wilson’s disease is highly likely when the value exceeds 250 μg per gram. In this case, copper quantification was performed on a formalin-fixed, paraffin-embedded tissue sample from the explanted liver, and a value of 978 μg per gram was obtained, confirming the diagno-sis of Wilson’s disease.
M a nagemen t a nd Foll ow-up
Dr. Nahel Elias: Identifying the cause of acute liver failure in this patient was critical in determining her place on the liver transplantation list.21 In this country, the highest priority (United Net-work for Organ Sharing status 1A) is reserved for patients with liver failure who have a life expectancy of less than 7 days if they do not
undergo transplantation.22 Wilson’s disease is the only cause of acute liver failure that allows a patient with preexisting liver disease to be listed as status 1A. Therefore, making this diagnosis is essential, as was shown in this case.
This patient received a good-quality liver do-nated from a deceased 23-year-old man who had been declared brain dead because of penetrating head trauma and hemorrhagic shock. We per-formed liver transplantation with the use of the “piggyback” technique, in which the surgeon performs hepatectomy with preservation of the inferior vena cava and then performs anastomo-sis to attach the donor’s suprahepatic inferior vena cava to the recipient’s inferior vena cava at the level of the hepatic veins. The graft cold ischemic time was 5 hours, and the graft warm ischemic time was 27 minutes. Total blood loss was 800 ml. The patient was extubated on day 1 after transplantation and transferred to the in-patient transplant unit the following day. She received maintenance therapy with a triple im-munosuppression regimen (tacrolimus, mycophe-nolate mofetil, and prednisone) and was dis-charged home on day 9 after transplantation.
Since the transplantation, the patient has done well, with the exception of three episodes of allograft dysfunction; the first was relatively minor and occurred during an upper respiratory tract infection, and the second and third were due to acute rejection during the administration of subtherapeutic tacrolimus levels 11 and 15 months after transplantation. The two episodes of rejection resolved after treatment with intra-venous methylprednisolone and an increase in immunosuppression maintenance therapy. The outcomes associated with liver transplantation for acute liver failure induced by Wilson’s dis-ease are excellent, if transplantation is per-formed prior to neurologic deterioration.23-25
A nat omic a l Di agnosis
Fulminant hepatic failure due to Wilson’s disease.This case was presented at the Internal Medicine Case Con-
ference.No potential conflict of interest relevant to this article was
reported.Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
Cases in Primary Care NEJM.org

24
BacktoTableofContents
n engl j med 376;3 nejm.org January 19, 2017278
Case Records of the Massachusetts Gener al Hospital
Lantern SLideS Updated: CompLete powerpoint SLide SetS from the CLiniCopathoLogiCaL ConferenCeS
Any reader of the Journal who uses the Case Records of the Massachusetts General Hospital as a teaching exercise or reference material is now eligible to receive a complete set of PowerPoint slides, including digital images, with identifying legends, shown at the live Clinicopathological Conference (CPC) that is the basis of the Case Record. This slide set contains all of the images from the CPC, not only those published in the Journal. Radiographic, neurologic, and cardiac studies, gross specimens, and photomicrographs, as well as unpublished text slides, tables, and diagrams, are included. Every year 40 sets are produced, averaging 50-60 slides per set. Each set is supplied on a compact disc and is mailed to coincide with the publication of the Case Record.
The cost of an annual subscription is $600, or individual sets may be purchased for $50 each. Application forms for the current subscription year, which began in January, may be obtained from the Lantern Slides Service, Department of Pathology, Massachusetts General Hospital, Boston, MA 02114 (telephone 617-726-2974) or e-mail [email protected].
References1. Lee WM, Squires RH Jr, Nyberg SL, Doo E, Hoofnagle JH. Acute liver failure: summary of a workshop. Hepatology 2008; 47: 1401-15.2. Squires RH Jr. Acute liver failure in children. Semin Liver Dis 2008; 28: 153-66.3. Squires RH, Alonso EM. Acute liver failure in children. In: Suchy FJ, Sokol RJ, Balistreri WF, eds. Liver disease in chil-dren. 4th ed. New York: Cambridge Uni-versity Press, 2012: 32-50.4. Banti S, Mauri M, Oppo A, et al. From the third month of pregnancy to 1 year postpartum: prevalence, incidence, recur-rence, and new onset of depression — results from the Perinatal Depression–Research & Screening Unit Study. Compr Psychiatry 2011; 52: 343-51.5. Hu J, Zhang Q, Ren X, Sun Z, Quan Q. Efficacy and safety of acetylcysteine in “non-acetaminophen” acute liver failure: a meta-analysis of prospective clinical tri-als. Clin Res Hepatol Gastroenterol 2015; 39: 594-9.6. Chalasani N, Bonkovsky HL, Fontana R, et al. Features and outcomes of 899 patients with drug-induced liver injury: the DILIN Prospective Study. Gastroen-terology 2015; 148(7): 1340-52.e7.7. Bacak SJ, Thornburg LL. Liver failure in pregnancy. Crit Care Clin 2016; 32: 61-72.8. Ren W, Li X, Jia J, Xia Y, Hu F, Xu Z. Prevalence of Budd-Chiari syndrome dur-ing pregnancy or puerperium: a systematic review and meta-analysis. Gastroenterol Res Pract 2015; 2015: 839875.
9. Czaja AJ. Diagnosis and management of autoimmune hepatitis. Clin Liver Dis 2015; 19: 57-79.10. Krawitt EL. Autoimmune hepatitis. N Engl J Med 2006; 354: 54-66.11. Tanaka S, Okamoto Y, Yamazaki M, Mitani N, Nakqjima Y, Fukui H. Signifi-cance of hyperglobulinemia in severe chronic liver diseases — with special ref-erence to the correlation between serum globulin/IgG level and ICG clearance. Hepatogastroenterology 2007; 54: 2301-5.12. Ferenci P, Caca K, Loudianos G, et al. Diagnosis and phenotypic classification of Wilson disease. Liver Int 2003; 23: 139-42.13. Korman JD, Volenberg I, Balko J, et al. Screening for Wilson disease in acute liver failure: a comparison of currently avail-able diagnostic tests. Hepatology 2008; 48: 1167-74.14. Hadem J, Tacke F, Bruns T, et al. Eti-ologies and outcomes of acute liver failure in Germany. Clin Gastroenterol Hepatol 2012; 10(6): 664-9.e2.15. Roberts EA, Schilsky ML. Diagnosis and treatment of Wilson disease: an up-date. Hepatology 2008; 47: 2089-111.16. Dhawan A, Taylor RM, Cheeseman P, De Silva P, Katsiyiannakis L, Mieli-Vergani G. Wilson’s disease in children: 37-year ex-perience and revised King’s score for liver transplantation. Liver Transpl 2005; 11: 441-8.17. Petrasek J, Jirsa M, Sperl J, et al. Re-vised King’s College score for liver trans-
plantation in adult patients with Wilson’s disease. Liver Transpl 2007; 13: 55-61.18. Stromeyer FW, Ishak KG. Histology of the liver in Wilson’s disease: a study of 34 cases. Am J Clin Pathol 1980; 73: 12-24.19. Johncilla M, Mitchell KA. Pathology of the liver in copper overload. Semin Liver Dis 2011; 31: 239-44.20. Ludwig J, Moyer TP, Rakela J. The liver biopsy diagnosis of Wilson’s disease: methods in pathology. Am J Clin Pathol 1994; 102: 443-6.21. Reddy KR, Ellerbe C, Schilsky M, et al. Determinants of outcome among patients with acute liver failure listed for liver transplantation in the United States. Liver Transpl 2016; 22: 505-15.22. Organ Procurement and Transplanta-tion Network. Policy 9: allocation of livers and liver–intestines. Washington, DC: De-partment of Health and Human Services, 2016 (https:/ / optn .transplant .hrsa .gov/ governance/ policies/ ).23. Eghtesad B, Nezakatgoo N, Geraci LC, et al. Liver transplantation for Wilson’s disease: a single-center experience. Liver Transpl Surg 1999; 5: 467-74.24. Guillaud O, Dumortier J, Sobesky R, et al. Long term results of liver transplan-tation for Wilson’s disease: experience in France. J Hepatol 2014; 60: 579-89.25. Medici V, Mirante VG, Fassati LR, et al. Liver transplantation for Wilson’s disease: the burden of neurological and psychiatric disorders. Liver Transpl 2005; 11: 1056-63.Copyright © 2017 Massachusetts Medical Society.
Cases in Primary Care NEJM.org

25
BacktoTableofContents
Cases in Primary Care NEJM.org
CLINICAL PROBLEM-SOLVINGAppearing in the first issue of each month, this Journal feature presents particulars about real patients in stages to experts, who respond to the information, sharing their clinical reasoning with the reader.

26
BacktoTableofContents
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 376;5 nejm.org February 2, 2017476
Clinical Problem-Solving
A 41-year-old man with a weight of 159 kg and a body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) of 49.1 presented for con-sideration of bariatric surgery. He had been morbidly obese since childhood; he had tried several commercial weight-loss programs in addition to dieting on his own but had had little long-term success.
Bariatric surgical procedures are a well-established approach to the treatment of morbid obesity, offering sustainable weight loss and a reduction in the risk of conditions related to obesity. Candidacy is stratified according to BMI. Adults with a BMI of 40 or higher are potential candidates for the procedure. Patients with a BMI of 35.0 to 39.9 are generally considered to be eligible if they have at least one serious coexisting condition, such as obstructive sleep apnea, type 2 diabetes, or hypertension.
The patient had a history of hyperlipidemia and had undergone cholecystectomy. His medications included rosuvastatin and ezetimibe. He had no known drug allergies. He lived with his wife and three children and worked in information technology. He was a current smoker, with a 30-year history of one to three packs per day. He had a remote history of excessive alcohol use and had been abstinent for the past 15 years. He reported no illicit drug use. He had no known family history of gastrointestinal disorders. After consultation, he decided to undergo Roux-en-Y gastric bypass.
Roux-en-Y gastric bypass is one of the most common bariatric surgical treatments for obesity. The procedure involves the creation of a small upper gastric pouch (with a capacity of approximately 30 ml), stapling of the stomach, and division of the small intestine at the proximal jejunum, with anastomosis of the distal portion (the ali-mentary, or Roux, limb) to the gastric pouch. The proximal end of the divided jeju-num (the biliopancreatic limb) is anastomosed farther down the jejunum (Fig. 1). Pancreatic and biliary secretions come into contact with food below this anasto-mosis, in the “common channel” of the small intestine. Although the initial the-ory was that Roux-en-Y gastric bypass led to weight loss through mechanical re-striction of the upper gastric pouch and a reduction in the surface area for nutrient absorption, it is now known that the surgery also causes neurohormonal changes that may influence metabolism and weight.
From Departments of Medicine (A.R.S., C.C.T., A.L.M., J.L.) and Surgery (A.T.), Brigham and Women’s Hospital, Harvard Medical School, Boston. Address reprint requests to Dr. Miller at the Department of Medicine, Brigham and Women’s Hos-pital, 75 Francis St., Boston, MA 02115, or at almiller@ partners . org.
N Engl J Med 2017;376:476-82.DOI: 10.1056/NEJMcps1602495Copyright © 2017 Massachusetts Medical Society.
Caren G. Solomon, M.D., M.P.H., Editor
Making the ConnectionAllison R. Schulman, M.D., Ali Tavakkoli, M.D., Christopher C. Thompson, M.D.,
Amy L. Miller, M.D., Ph.D., and Joseph Loscalzo, M.D., Ph.D.
In this Journal feature, information about a real patient is presented in stages (boldface type) to an expert clinician, who responds to the information, sharing his or her reasoning with the reader (regular type).
The authors’ commentary follows.
Cases in Primary Care NEJM.org
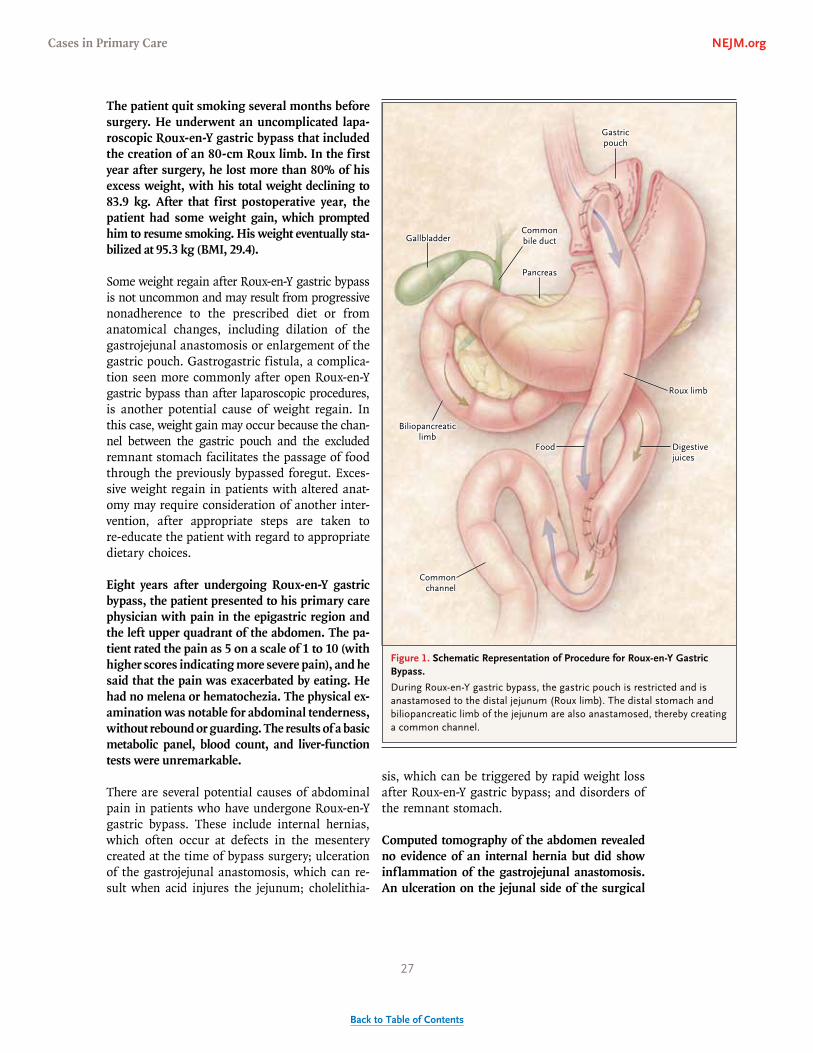
27
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017 477
Clinical Problem-Solving
The patient quit smoking several months before surgery. He underwent an uncomplicated lapa-roscopic Roux-en-Y gastric bypass that included the creation of an 80-cm Roux limb. In the first year after surgery, he lost more than 80% of his excess weight, with his total weight declining to 83.9 kg. After that first postoperative year, the patient had some weight gain, which prompted him to resume smoking. His weight eventually sta-bilized at 95.3 kg (BMI, 29.4).
Some weight regain after Roux-en-Y gastric bypass is not uncommon and may result from progressive nonadherence to the prescribed diet or from anatomical changes, including dilation of the gastrojejunal anastomosis or enlargement of the gastric pouch. Gastrogastric fistula, a complica-tion seen more commonly after open Roux-en-Y gastric bypass than after laparoscopic procedures, is another potential cause of weight regain. In this case, weight gain may occur because the chan-nel between the gastric pouch and the excluded remnant stomach facilitates the passage of food through the previously bypassed foregut. Exces-sive weight regain in patients with altered anat-omy may require consideration of another inter-vention, after appropriate steps are taken to re-educate the patient with regard to appropriate dietary choices.
Eight years after undergoing Roux-en-Y gastric bypass, the patient presented to his primary care physician with pain in the epigastric region and the left upper quadrant of the abdomen. The pa-tient rated the pain as 5 on a scale of 1 to 10 (with higher scores indicating more severe pain), and he said that the pain was exacerbated by eating. He had no melena or hematochezia. The physical ex-amination was notable for abdominal tenderness, without rebound or guarding. The results of a basic metabolic panel, blood count, and liver-function tests were unremarkable.
There are several potential causes of abdominal pain in patients who have undergone Roux-en-Y gastric bypass. These include internal hernias, which often occur at defects in the mesentery created at the time of bypass surgery; ulceration of the gastrojejunal anastomosis, which can re-sult when acid injures the jejunum; cholelithia-
sis, which can be triggered by rapid weight loss after Roux-en-Y gastric bypass; and disorders of the remnant stomach.
Computed tomography of the abdomen revealed no evidence of an internal hernia but did show inflammation of the gastrojejunal anastomosis. An ulceration on the jejunal side of the surgical
Figure 1. Schematic Representation of Procedure for Roux-en-Y Gastric Bypass.
During Roux-en-Y gastric bypass, the gastric pouch is restricted and is anastamosed to the distal jejunum (Roux limb). The distal stomach and biliopancreatic limb of the jejunum are also anastamosed, thereby creating a common channel.
Gastricpouch
Commonbile duct
Pancreas
Gallbladder
Roux limb
Digestivejuices
Food
Biliopancreaticlimb
Commonchannel
Cases in Primary Care NEJM.org

28
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017478
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
anastomosis was identified on esophagogastro-duodenoscopy (Fig. 2). Suture material was re-moved from the site to prevent further irritation of the mucosa.
High-dose proton-pump inhibitors are the main-stay of therapy and should be initiated, and the patient’s nutrition status should also be re-viewed to make sure that it will allow for ade-quate tissue healing. Discontinuation of smoking, avoidance of nonsteroidal antiinflammatory drugs (NSAIDs), and the removal of endoscopic sutures or staples at or near the site of marginal ulcer-ation are associated with an increased likelihood of successful healing. With appropriate treatment, these ulcers heal in the majority of patients.
The patient was treated with 40 mg of omeprazole twice daily, but despite excellent adherence to the regimen, his abdominal pain did not abate. Su-cralfate, 1 g per 10 ml administered four times per day, was added as adjunctive therapy, but serial repeat endoscopies conducted at 2-month inter-vals revealed that the ulcer was persistent. Within 6 months after the diagnosis of marginal ulcer-ation, the patient suddenly began to have foul-smelling, watery diarrhea six to seven times a day, without nocturnal diarrhea. These episodes were most voluminous after meals and often had visi-ble particulate matter that was consistent with what he had recently eaten. There were no spe-
cific dietary triggers. Episodes were associated with mild urgency but no tenesmus or fecal in-continence. The stool was pale, without melena or hematochezia, often floated, and left a residue after flushing. The patient also noted an increase in flatus and daily feculent eructation.
The symptoms are suggestive of a malabsorptive process, which is typically manifested in pale, greasy, voluminous, foul-smelling stools that float and are difficult to flush, in addition to weight loss despite adequate food intake. In this spe-cific case a secondary osmotic diarrhea is likely, with the poorly absorbed solutes causing water retention in the bowel. Osmotic diarrhea resolves with fasting and thus does not typically occur overnight. Disorders that may cause malabsorp-tion after Roux-en-Y gastric bypass include bac-terial overgrowth in the small intestine and en-teroenteric fistula; the latter limits the surface area for intestinal absorption and is also known to cause feculent eructation.
Although enteroenteric fistulas are rare and are most commonly associated with inflamma-tory bowel disease, ulceration causes a predispo-sition to their formation. Other causes of malab-sorption in the general population (which can also be present after bariatric surgery) include new lactose intolerance, chronic pancreatitis, celiac disease, bile-salt deficiency, and chronic infections.
The patient did not initially pursue further evalu-ation, but after 4 months of persistent symptoms, including progressive generalized weakness, my-algias, and muscle cramps, he presented to the emergency department for evaluation. His weight had decreased from 95.3 kg to 72.6 kg.
This patient has chronic diarrhea, as defined by persistently loose stools for more than 4 weeks, occurring at an average of more than three times per day. His associated symptoms suggest clini-cally significant electrolyte abnormalities, which should be addressed expeditiously.
Biopsy of the colonic mucosa should be pur-sued. Normal-appearing mucosa will be observed in many processes that cause chronic diarrhea, which makes histologic examination an essential component of the evaluation. Although this ex-amination could be accomplished by means of
Figure 2. Endoscopic View of the Jejunal Aspect of the Gastrojejunal Anastomosis, Showing Ulceration.
A marginal ulceration can be seen (arrows).
Cases in Primary Care NEJM.org

29
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017 479
Clinical Problem-Solving
flexible sigmoidoscopy, the fecal eructation is sug-gestive of an enteroenteric fistula, which makes colonoscopy a better choice, since it allows visu-alization of the entire colon. In general, upper endoscopic evaluation should be considered in patients with chronic diarrhea if the lower endo-scopic evaluation is unrevealing. This recommen-dation is particularly appropriate in this case given the possibility of an enteroenteric fistula; if the fistula involves the upper gastrointestinal tract, it may be more easily visualized through upper endoscopy. Breath testing for small intestinal bac-terial overgrowth should also be considered.
The patient’s temperature was 37.0°C, pulse 97 beats per minute, blood pressure 113/69 mm Hg, respi-ratory rate 16 breaths per minute, and oxygen saturation 99% while he was breathing ambient air. He appeared to be chronically ill and cachectic but was not in acute distress. The oropharynx was clear, with dry mucous membranes and feculent breath. His thyroid was not palpable. The cardiac and pulmonary examinations were normal. His abdomen was nondistended, with minimal ten-derness to deep palpation in the epigastrum and left upper quadrant. Excessive loose, sagging skin was noted around his midabdomen. The skin turgor in his legs was diminished. The results of neurologic and rectal examinations were unremark-able, and a stool test for guaiac was negative.
The potassium level was 2.2 mmol per liter, magnesium 1.6 mg per deciliter (0.7 mmol per li-ter; reference range, 1.7 to 2.6 mg per deciliter [0.7 to 1.1 mmol per liter]), and phosphorus 1.5 mg per deciliter (0.5 mmol per liter; reference range, 2.4 to 4.3 mg per deciliter [0.8 to 1.4 mmol per li-ter]). Sodium and chloride levels were normal. The blood urea nitrogen level was 5 mg per decili-ter (1.8 mmol per liter) and creatinine 0.85 mg per deciliter (75 μmol per liter). The hematocrit was 35.4%. The white-cell count and platelet count were normal. The thyrotropin level was 2.96 mIU per liter. The level of albumin was 1.5 g per decili-ter, and prealbumin 9.3 mg per deciliter (reference range, 20 to 40). The erythrocyte sedimentation rate was 16 mm per hour (reference range, 0 to 13), and the C-reactive protein level 13.4 mg per liter (reference range, 0 to 5). The prothrombin time was elevated at 15.9 seconds (reference range, 12.0 to 14.4). Liver-function tests were normal.
Tests for antibodies to tissue transglutaminase IgA and the human immunodeficiency virus were negative; the total IgA level was normal. Stool studies were negative for bacterial infection and for ova and parasites. The fecal fat level was elevat-ed, and fecal leukocytes were rare.
Whereas excessive loose, sagging skin can be seen after substantial weight loss, the diminished skin turgor and dry mucous membranes in the patient indicate interstitial volume depletion. The severe hypokalemia and hypomagnesemia are conse-quences of his profound diarrhea. The low levels of albumin and prealbumin suggest that he is se-verely malnourished. His anemia may reflect poor iron absorption or could be due to gastrointesti-nal blood loss that was not detected on a single guaiac test. The prolongation of prothrombin time is probably due to the depletion of vitamin K–dependent coagulation factors, and the elevat-ed level of C-reactive protein, although nonspe-cific, suggests inflammation. Although tissue levels of antibodies to transglutaminase IgA have high sensitivity and specificity for celiac disease in the presence of normal total IgA levels, nor-mal findings do not definitively rule out celiac disease. However, celiac disease would not ac-count for the feculent eructation in this patient. Fecal fat excretion can be increased in diarrheal illnesses even in the absence of fat malabsorp-tion. The standard for the diagnosis of increased fecal fat excretion in patients with malabsorption is quantitative measurement with a biochemical assay. Normal excretion is less than 6 g per day, assuming that the patient is consuming 70 to 120 g per day of dietary fat. Collection periods of 3 days or longer increase the sensitivity of detection.
The patient was admitted to the hospital for hydra-tion and electrolyte supplementation, diagnostic testing, and monitoring. After hydration and elec-trolyte repletion, a colonoscopy revealed a small area of erythema near the hepatic flexure; no other abnormalities were noted. Biopsy specimens of the colon and terminal ileum were normal. Upper endoscopy revealed normal esophageal mucosa, with marginal ulceration and severe inflamma-tion at the gastrojejunal anastomosis; when pres-sure was exerted on one of the areas of inflamma-
Cases in Primary Care NEJM.org

30
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017480
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
tion, the endoscope passed through a fistulous tract, terminating in the transverse colon.
The endoscopy revealed an enteroenteric fistula. Symptoms vary depending on the location of the fistula and the extent of the bowel that is by-passed. Enteroenteric fistulas in which only a short segment of the bowel is circumvented may be asymptomatic. Conversely, fistulas that bypass a larger segment of the bowel typically cause di-arrhea but may also be associated with weight loss or abdominal pain. Gastrocolic fistula is a well-recognized but rare complication of peptic ulcer disease, stomach and colon cancer, Crohn’s disease, and surgical procedures. The combina-tion of feculent eructation and vomiting, diar-rhea, and malnutrition is the classic symptom complex.
An upper gastrointestinal series showed contrast material traversing the gastric pouch into a fistu-lous tract that terminated in the transverse colon. The contrast material did not pass into the small bowel or the proximal large bowel (Fig. 3).
These findings confirm the diagnosis of a gas-trocolic fistula and also help to delineate the
anatomy of the gastrointestinal tract. Although surgical repair is indicated, the patient’s poor nutritional status makes him a poor candidate for such a procedure.
Total parenteral nutrition was provided for 8 weeks before the endoscopic removal of the gastrocolic fistula and the revision of the gastrojejunal anas-tomosis and gastric pouch. After surgery, the pa-tient began to have normal formed bowel move-ments and transitioned back to oral nutrition. Complete resolution of the fistulous connection was confirmed on a repeat upper gastrointestinal series. At follow-up 5 months after surgery, the patient had returned to a weight of 95.3 kg.
Commen ta r y
This patient initially presented with abdominal pain, for which the differential diagnosis was broad given his history of gastric bypass surgery. The marginal ulceration identified at that time failed to heal and was eventually complicated by a profound malabsorptive diarrhea, with resul-tant dehydration. Although dumping syndrome and bacterial overgrowth in the small intestine are common causes of diarrhea after gastric by-
Figure 3. Upper Gastrointestinal Series.
Contrast material can be seen traveling down the esophagus and through the gastric pouch and fistulous tract to the transverse colon, from which it traverses the descending colon. No contrast material is seen within the small bowel or the proximal large bowel, findings that are diagnostic of a gastrocolic fistula.
Esophagus
Gastric pouchFistula
Transversecolon
Fistula
Descendingcolon
Cases in Primary Care NEJM.org

31
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017 481
Clinical Problem-Solving
pass, other causes, including enteroenteric fis-tula, must be considered in this patient popula-tion, especially when fecal eructation is present. These patients should therefore undergo anatomi-cal evaluation before their symptoms are attrib-uted to the more common causes. In this case, a full diagnostic workup ultimately led to the diag-nosis of gastrocolic fistula.
The increasing prevalence of severe obesity and associated conditions has resulted in a sub-stantial increase in the number of bariatric pro-cedures performed.1-5 Roux-en-Y gastric bypass is one of the most commonly performed weight-loss surgeries. Outcomes of bariatric procedures have improved substantially in the past decade, but complications can occur; vigilance and thorough assessment of patients presenting with symptoms is required.
The cause of marginal ulceration is usually multifactorial.6-8 Poor perfusion of local tissue is believed to contribute to the occurrence of ul-cers, which can also be caused by excessive acid exposure in the gastric pouch; analysis of a consecutive series of patients suggests that for-eign materials (e.g., sutures or staples), a history of smoking, and the use of NSAIDs are associ-ated with an increased incidence of marginal ulceration.9 The potential role of Helicobacter py-lori infection as a predisposing factor remains controversial.
Retrospective data support the view that the majority of patients with marginal ulcerations have a response to medical therapy with high doses of proton-pump inhibitors and sucralfate8; the ad-dition of sucralfate has been recommended in patients who are already taking a proton-pump inhibitor at the time of diagnosis.10 In addition, smoking cessation and indefinite discontinua-tion of NSAIDs are recommended. The removal of foreign material and testing for H. pylori (as well as treatment, if test results are positive) should also be considered.11 The use of endoscopic sutur-
ing to oversew the ulceration has been proposed in the treatment of recalcitrant marginal ulcer-ation, but more information regarding efficacy and durability is needed.12
Fistulous complications have also been re-ported after Roux-en-Y gastric bypass and are often associated with a chronic leak from the surgical anastomosis or with a marginal ulcer that does not heal. Gastrogastric fistulas — which occur when a channel develops between the gastric pouch and the excluded stomach remnant and allows ingested food to enter the bypassed foregut — are most commonly associ-ated with Roux-en-Y gastric bypass procedures that are performed with an open approach, al-though fistulas may also occur after laparoscopic procedures. Gastrocolic fistulas are a rare com-plication of the formation of a gastrojejunosto-my and are typically initiated by ulceration at the site of the anastomosis. This type of fistula for-mation has been reported as late as 20 years after the surgical Roux-en-Y gastric bypass has been performed.13 Depending on the size and location of the fistula, consideration of endoscopic clo-sure (including endoscopic suturing or over-the-scope clips) or surgical closure should be consid-ered. In rare instances, other types of fistulas have been reported after gastric bypass surgery, including gastrobronchial, gastropericardial, and jejunocolic fistulas.14
The current case underscores the importance of considering late complications of bariatric sur-gery as causes of new symptoms in patients who have had this surgery. Although gastrocolic fis-tula is an uncommon complication of Roux-en-Y gastric bypass, the combination of malabsorptive diarrhea, fecal eructation, and previous marginal ulceration provided important clues that pointed to this complication.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References1. Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery: a systematic re-view and meta-analysis. JAMA 2004; 292: 1724-37.2. Arterburn DE, Olsen MK, Smith VA, et al. Association between bariatric surgery and long-term survival. JAMA 2015; 313: 62-70.
3. Colquitt J, Clegg A, Loveman E, Royle P, Sidhu MK. Surgery for morbid obesity. Cochrane Database Syst Rev 2005; 4: CD003641.4. Perry CD, Hutter MM, Smith DB, Ne-whouse JP, McNeil BJ. Survival and chang-es in comorbidities after bariatric sur-gery. Ann Surg 2008; 247: 21-7.
5. Buchwald H, Oien DM. Metabolic/bariatric surgery worldwide 2011. Obes Surg 2013; 23: 427-36.6. Azagury DE, Abu Dayyeh BK, Green-walt IT, Thompson CC. Marginal ulceration after Roux-en-Y gastric bypass surgery: characteristics, risk factors, treatment, and outcomes. Endoscopy 2011; 43: 950-4.
Cases in Primary Care NEJM.org

32
BacktoTableofContents
n engl j med 376;5 nejm.org February 2, 2017482
Clinical Problem-Solving
7. Dallal RM, Bailey LA. Ulcer disease after gastric bypass surgery. Surg Obes Relat Dis 2006; 2: 455-9.8. Rasmussen JJ, Fuller W, Ali MR. Mar-ginal ulceration after laparoscopic gastric bypass: an analysis of predisposing fac-tors in 260 patients. Surg Endosc 2007; 21: 1090-4.9. Coblijn UK, Lagarde SM, de Castro SM, Kuiken SD, van Wagensveld BA. Symptom-atic marginal ulcer disease after Roux-en-Y gastric bypass: incidence, risk factors and management. Obes Surg 2015; 25: 805-11.
10. Carr WR, Mahawar KK, Balupuri S, Small PK. An evidence-based algorithm for the management of marginal ulcers following Roux-en-Y gastric bypass. Obes Surg 2014; 24: 1520-7.11. Steinemann DC, Bueter M, Schiesser M, Amygdalos I, Clavien PA, Nocito A. Management of anastomotic ulcers after Roux-en-Y gastric bypass: results of an international survey. Obes Surg 2014; 24: 741-6.12. Jirapinyo P, Watson RR, Thompson CC. Use of a novel endoscopic suturing
device to treat recalcitrant marginal ul-ceration (with video). Gastrointest Endosc 2012; 76: 435-9.13. Fronza JS, Martin JA, Nagle AP. Jeju-nocolic fistula after Roux-en-Y gastric bypass. Surg Obes Relat Dis 2012; 8(5): e60-2.14. Sakran N, Assalia A, Keidar A, Goit-ein D. Gastrobronchial fistula as a com-plication of bariatric surgery: a series of 6 cases. Obes Facts 2012; 5: 538-45.Copyright © 2017 Massachusetts Medical Society.
clinical problem-solving series
The Journal welcomes submissions of manuscripts for the Clinical Problem-Solving series. This regular feature considers the step-by-step process of clinical decision
making. For more information, please see authors.NEJM.org.
Cases in Primary Care NEJM.org

33
BacktoTableofContents
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 376;18 nejm.org May 4, 2017 1783
Clinical Problem-Solving
An 82-year-old man presented to the emergency department with a 6-month history of worsening back and left hip pain. He had been well until 6 months earlier, when acute fever and cough developed. Pneumonia was diagnosed, and a 10-day course of levofloxacin was prescribed. His respiratory symptoms resolved. At about the same time that the respiratory symptoms resolved, low back pain began to develop. The patient did not recall any antecedent trauma, fall, or heavy lifting. Over the course of the ensuing months, his back pain continued to worsen, and left hip pain developed; he presented to the emergency department after walking became painful. The pain did not radiate down his legs, but it occasionally woke him from sleep and was worse after activity. He reported no relief from bending forward. He reported no morning stiffness, fever, chills, or night sweats. He noted that he had lost 9 kg (20 lb) of weight over the course of the preceding few months. He had no bowel or bladder inconti-nence.
This patient has chronic (duration of >12 weeks) back pain. Demographic and clinical features, including age, the presence of constitutional symptoms, pain awak-ening him from sleep, and persistence and worsening of the pain, indicate the need for imaging. This history arouses concern for an underlying systemic illness, such as metastatic cancer, a systemic infection, or an autoimmune process. Polymyalgia rheumatica can cause hip pain and systemic symptoms such as weight loss, but it is associated with morning stiffness, particularly in the shoulders and hips.
The patient’s medical history included the sick sinus syndrome for which a pace-maker had been placed years earlier, diastolic heart failure, pulmonary fibrosis, hyper-lipidemia, hypertension, gout, herpes zoster with postherpetic neuralgia, and basal-cell carcinoma for which the patient underwent Mohs micrographic surgery. His medications included allopurinol, aspirin, metoprolol, simvastatin, gabapentin, and recently, oxycodone and acetaminophen for the low back pain. He had no known drug allergies. He was retired but had worked previously as a university professor. He lived with his wife and had grown children. He had smoked cigars for many years but had quit 28 years before the current presentation. He reported drinking one glass of alcohol per night until 6 months before this presentation, when his current illness began. He reported no history of illicit-drug use. He had traveled internationally in the distant past, including trips to Asia and South America, and had traveled throughout the United States. His family history was notable for congestive heart failure in his mother, coronary heart disease in his father, and non-Hodgkin’s lym-phoma in his brother.
From the Department of Medicine, Brigham and Women’s Hospital and Har-vard Medical School, Boston. Address reprint requests to Dr. Levy at Brigham and Women’s Hospital, Harvard Insti-tutes of Medicine Building, 77 Ave. Louis Pasteur (HIM855), Boston, MA 02115, or at blevy@ partners . org.
N Engl J Med 2017;376:1783-8.DOI: 10.1056/NEJMcps1607608Copyright © 2017 Massachusetts Medical Society.
Caren G. Solomon, M.D., M.P.H., Editor
Back to the HistoryMary W. Montgomery, M.D., Sigal Yawetz, M.D., Bruce D. Levy, M.D.,
and Joseph Loscalzo, M.D., Ph.D.
In this Journal feature, information about a real patient is presented in stages (boldface type) to an expert clinician, who responds to the information, sharing his or her reasoning with the reader (regular type).
The authors’ commentary follows.
Cases in Primary Care NEJM.org

34
BacktoTableofContents
n engl j med 376;18 nejm.org May 4, 20171784
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
The most important risk factor for metastatic cancer to the spine is a personal history of cancer. The patient has a history of basal-cell carcinoma, but this type of cancer rarely causes distant metas-tases and is unlikely to be related to his current presentation. He has a remote smoking history, which puts him at risk for lung cancer. His age is a risk factor for prostate cancer, which can metastasize to the vertebrae. He has had no re-cent device implantation, surgery, or trauma that could have introduced infection. His previous travel to Asia and South America could put him at risk for tuberculous spondylitis.
On physical examination, he appeared to be in no acute distress. His temperature was 37.1°C (98.7°F), the blood pressure 110/60 mm Hg, the pulse 60 beats per minute, the respiratory rate 16 breaths per minute, and the oxygen saturation 98% while he was breathing ambient air. The oropharynx was clear, without thrush or oral ulcerations. The lungs were clear to auscultation. A cardiovascular examination revealed a regular rate and rhythm without murmurs, rubs, or gallops. A pacemaker generator was palpated over the left pectoralis muscle, and no erythema, fluctuance, or tender-ness was noted. The abdomen was soft and non-tender, with normal bowel sounds and without hepatosplenomegaly. There was no palpable cervical, axillary, or inguinal lymphadenopathy. A neurologic examination revealed that the patient was oriented to person, place, and time. Cranial nerves II to XII were normal. He had no muscle wasting in his legs, and the muscle strength in his legs was 5/5 both proximally and distally. The patellar reflexes were slightly diminished in both knees. A sensory examination showed that sensa-tions to light touch and vibration were intact. No saddle anesthesia was present, and the rectal tone was normal. He had no point tenderness over any portion of his spine or his sacroiliac joints. The straight-leg raising maneuver revealed no radicu-lar symptoms in either leg. A bilateral hip exami-nation, including f lexion, internal rotation, and external rotation, was normal. No Janeway lesions or Osler nodes were present.
The patient has no neurologic deficits to suggest spinal cord compression or the cauda equina syn-drome. The negative results of the straight-leg raising test make lumbosacral radiculopathy un-likely. The absence of focal spinal tenderness
does not rule out vertebral osteomyelitis since only one quarter of patients with vertebral osteo-myelitis present with this finding. Focal tender-ness on examination can also be absent in early metastatic spinal disease. Spondyloarthropathy is unlikely, given his age, the normal hip examina-tion, and his history of worsening pain with activity (rather than with rest).
The white-cell count was 8000 per cubic milli-meter, with 87% neutrophils, 8% lymphocytes, 2% monocytes, and 0% eosinophils. The hemato-crit level was 39.1%, and the platelet count was 231,000 per cubic millimeter. A comprehensive metabolic panel and coagulation studies were normal. The erythrocyte sedimentation rate was 64 mm per hour, and the C-reactive protein level was 47.9 mg per liter (normal range, 1 to 3).
The elevations in erythrocyte sedimentation rate and C-reactive protein are of concern and sug-gest an inflammatory, infectious, or neoplastic cause of the back pain. These tests have high sensitivity in vertebral osteomyelitis and spinal metastatic disease but are nonspecific. The nor-mal white-cell count does not rule out vertebral osteomyelitis, since more than one third of pa-tients with this condition present without leuko-cytosis. When systemic disease is suspected, as in this case, the preferred imaging method is mag-netic resonance imaging (MRI), unless a contra-indication exists. Pacemakers are a relative con-traindication to MRI, although some devices are MRI-compatible.
Because the patient had a pacemaker, MRI was not performed. Computed tomography (CT) of the lumbar spine with contrast enhancement revealed end-plate irregularity and destruction of the L4 and L5 vertebrae, with a surrounding left paraver-tebral and ventral epidural soft-tissue collection extending into the right foramen. There was no evidence of nerve-root compression (Fig. 1).
The imaging findings arouse suspicion for verte-bral osteomyelitis. Involvement of two contigu-ous vertebrae is more consistent with osteomyeli-tis than with cancer. Vertebral osteomyelitis is primarily the result of hematogenous seeding, direct infection after spinal surgery, or extension from an infected adjacent tissue. The most com-monly isolated organism is Staphylococcus aureus,
Cases in Primary Care NEJM.org

35
BacktoTableofContents
n engl j med 376;18 nejm.org May 4, 2017 1785
Clinical Problem-Solving
followed by gram-negative bacilli and streptococ-cus. Coagulase-negative staphylococci and Propi-onibacterium acnes are often causes of osteomyeli-tis after spinal surgery with fixation devices. This patient has had no recent spinal surgery; however, the history of pacemaker placement could be relevant. Persistent bacteremia from pacemaker lead infections with nonvirulent organ-isms, such as coagulase-negative staphylococci, can lead to vertebral osteomyelitis that manifests subacutely.
Given the CT findings, more thorough travel and dietary histories were obtained to assess the pa-tient’s epidemiologic risk for atypical causes of vertebral osteomyelitis. The patient’s travel history included trips to Thailand, Malaysia, Venezuela, Belize, Nicaragua, Australia, and New Zealand, as well as locations throughout the United States. He resided in Boston during the summer and spent the winters in Arizona, which is where he was residing when the back pain first developed 6 months earlier. He had never worked or lived on a farm and did not consume unpasteurized dairy products.
His extensive travel history broadens the differ-ential diagnosis to include infection with Myco-bacterium tuberculosis and infection with brucella species, both of which may manifest subacutely. This patient reports no exposure to livestock or to unpasteurized dairy products, which makes the diagnosis of brucellosis unlikely. Other possi-bilities include infection with endemic fungi, such as Cryptococcus neoformans, Histoplasma capsu-latum, Blastomyces dermatitidis, or Coccidioides im-mitis. Rare cases of vertebral osteomyelitis have also been reported with Burkholderia pseudomallei, the causative agent of melioidosis, which is en-demic to parts of Australia and Southeast Asia.
Overall, the patient appears well, without any neurologic deficits, so there is no immediate need for surgical intervention or empirical antibiotics. A definitive diagnosis determined by laboratory evaluation, including blood cultures, followed by aspiration biopsy if the blood cultures are nega-tive, should be pursued before therapy is initiated.
Testing for human immunodeficiency virus (HIV) antibody was negative. The prostate-specific anti-gen level was 0.7 ng per milliliter (reference range, 0 to 4). The blood level of angiotensin-converting
enzyme was normal. Three sets of blood cultures were negative. Chest radiography showed multi-ple calcified mediastinal and hilar lymph nodes. CT of the chest confirmed this finding and also showed parenchymal scarring in the right upper lobe and a trace pleural effusion on the right side (Fig. 2).
The patient has extensive calcified mediastinal lymph nodes, a finding that is suggestive of previ-ous granulomatous disease. Disease processes that can lead to calcification include tuberculosis, histoplasmosis, coccidioidomycosis, and sarcoid-
Figure 1. CT Scans of the Lumbar Spine.
CT scans of the lumbar spine with contrast enhance-ment show end-plate irregularity and destruction of the L4 and L5 vertebrae (Panel A, arrow), with a sur-rounding left paravertebral and ventral epidural soft-tissue collection (Panel B, arrow.)
A
B
Cases in Primary Care NEJM.org

36
BacktoTableofContents
n engl j med 376;18 nejm.org May 4, 20171786
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
osis. Sarcoidosis and histoplasmosis are rare causes of vertebral osteomyelitis; therefore, tuber-culosis and coccidioidomycosis are the more likely diagnoses.
A purified protein derivative skin test was nega-tive. A test for urinary Histoplasma capsulatum anti-gen was negative. Antibiotics were not initiated, and the patient underwent CT-guided L4–L5 disc aspiration and core-needle biopsy. Fluid could not be aspirated on the initial attempt; 2 to 3 cc of sterile saline were injected and reaspirated. This sample and two core bone-biopsy specimens were sent for culture and histopathological examina-tion. The results of initial staining for bacteria, fungi, and acid-fast bacilli were negative. The core bone-biopsy specimens were sent to the state lab-oratory to test for M. tuberculosis by means of a polymerase-chain-reaction assay; the results were negative.
One of the leading possible diagnoses before the biopsy was performed was tuberculous spondy-litis. The negative results of the purified protein derivative skin test, acid-fast bacilli stains, and polymerase-chain-reaction assay for tuberculosis make tuberculosis an unlikely diagnosis.
Another diagnostic possibility is coccidioido-mycosis, given that the back pain developed while the patient was in Arizona, soon after pneumo-nia was diagnosed. Primary coccidioidomycosis is often misclassified as community-acquired pneumonia since it also manifests as fever, cough, and an infiltrate on chest imaging. Coc-cidioides species can disseminate hematogenous-
ly outside the lungs and seed the spine soon after the initial exposure.
Pathological analysis of the vertebral disk-biopsy specimens revealed chronic granulomatous in-flammation with giant cells, plasma cells, and necrotic bone, as well as round, thick-walled, nonbudding fungal forms that were 15 to 25 μm in diameter, as best seen on fungal stain (Fig. 3). A fungal culture grew mold, which was identified as C. immitis. Serologic testing for coccidioidal antibodies was positive. The complement-fixing antibody titer was 1:64. The patient was offered initial treatment with amphotericin, but he de-clined this intravenous therapy and was instead started on oral itraconazole. Because he had side effects with itraconazole, he was switched to high-dose fluconazole. Six months later, he had progression of his coexisting conditions and chose to discontinue the antifungal therapy; he died after transitioning to hospice care.
Commen ta r y
Coccidioidomycosis, which is caused by the fungi C. immitis and C. posadasii, is endemic to the south-western United States. Infections occur after the inhalation of spores. The majority of infections are acquired in southern Arizona (as was prob-ably the case with this patient), central Califor-nia, New Mexico, and Texas.1
Up to two thirds of persons with coccidioido-mycosis have an asymptomatic or mild illness and do not present for medical care. Of persons who seek care, the majority present with a self-limited subacute pulmonary process or flulike illness, often referred to as valley fever. Many patients have evidence of infiltrates on chest imaging, which makes it difficult to differentiate valley fever from community-acquired pneumo-nia. In endemic regions, coccidioidomycosis ac-counts for up to one quarter of the cases of community-acquired pneumonia.2 This patient had a history of pneumonia that antedated the development of back pain; in retrospect, his respi-ratory symptoms were probably caused by coccidi-oidomycosis.
Most respiratory infections resolve without treatment, and extrapulmonary dissemination from the hematogenous spread of coccidioido-mycosis develops in less than 0.5% of immuno-competent patients. The most common sites of
Figure 2. CT Scan of the Chest.
A CT scan of the chest shows multiple calcified medi-astinal and hilar lymph nodes.
Cases in Primary Care NEJM.org
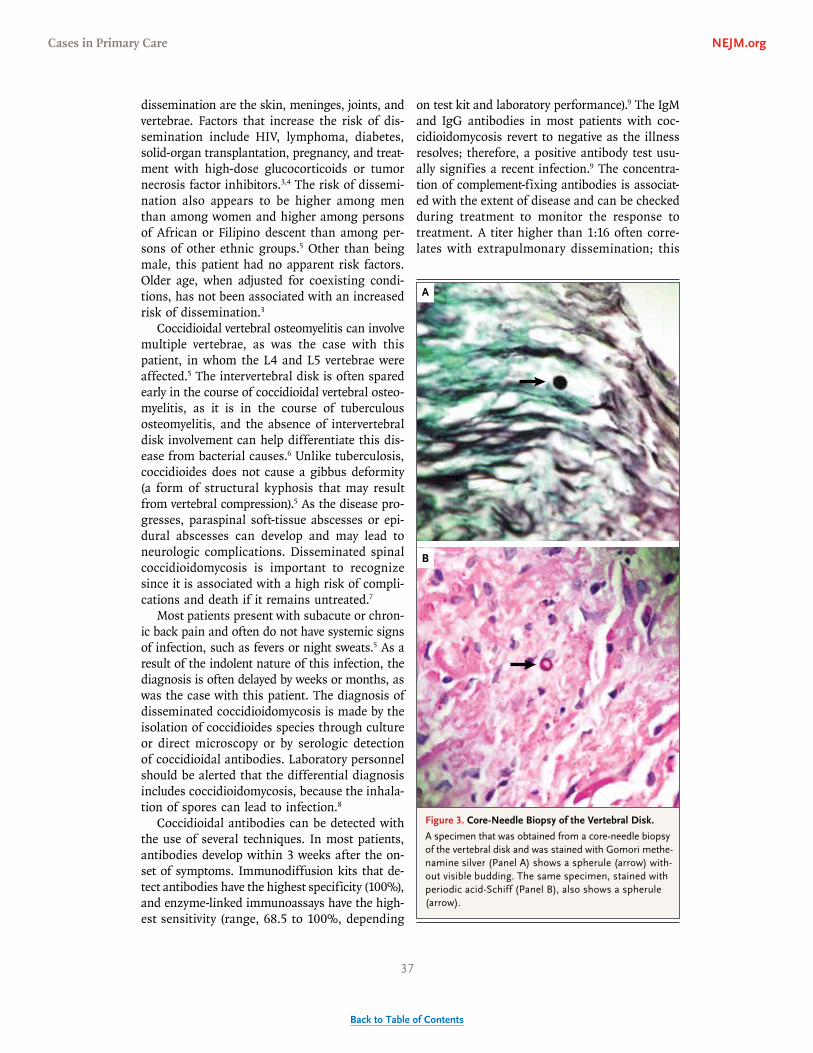
37
BacktoTableofContents
n engl j med 376;18 nejm.org May 4, 2017 1787
Clinical Problem-Solving
dissemination are the skin, meninges, joints, and vertebrae. Factors that increase the risk of dis-semination include HIV, lymphoma, diabetes, solid-organ transplantation, pregnancy, and treat-ment with high-dose glucocorticoids or tumor necrosis factor inhibitors.3,4 The risk of dissemi-nation also appears to be higher among men than among women and higher among persons of African or Filipino descent than among per-sons of other ethnic groups.5 Other than being male, this patient had no apparent risk factors. Older age, when adjusted for coexisting condi-tions, has not been associated with an increased risk of dissemination.3
Coccidioidal vertebral osteomyelitis can involve multiple vertebrae, as was the case with this patient, in whom the L4 and L5 vertebrae were affected.5 The intervertebral disk is often spared early in the course of coccidioidal vertebral osteo-myelitis, as it is in the course of tuberculous osteomyelitis, and the absence of intervertebral disk involvement can help differentiate this dis-ease from bacterial causes.6 Unlike tuberculosis, coccidioides does not cause a gibbus deformity (a form of structural kyphosis that may result from vertebral compression).5 As the disease pro-gresses, paraspinal soft-tissue abscesses or epi-dural abscesses can develop and may lead to neurologic complications. Disseminated spinal coccidioidomycosis is important to recognize since it is associated with a high risk of compli-cations and death if it remains untreated.7
Most patients present with subacute or chron-ic back pain and often do not have systemic signs of infection, such as fevers or night sweats.5 As a result of the indolent nature of this infection, the diagnosis is often delayed by weeks or months, as was the case with this patient. The diagnosis of disseminated coccidioidomycosis is made by the isolation of coccidioides species through culture or direct microscopy or by serologic detection of coccidioidal antibodies. Laboratory personnel should be alerted that the differential diagnosis includes coccidioidomycosis, because the inhala-tion of spores can lead to infection.8
Coccidioidal antibodies can be detected with the use of several techniques. In most patients, antibodies develop within 3 weeks after the on-set of symptoms. Immunodiffusion kits that de-tect antibodies have the highest specificity (100%), and enzyme-linked immunoassays have the high-est sensitivity (range, 68.5 to 100%, depending
on test kit and laboratory performance).9 The IgM and IgG antibodies in most patients with coc-cidioidomycosis revert to negative as the illness resolves; therefore, a positive antibody test usu-ally signifies a recent infection.9 The concentra-tion of complement-fixing antibodies is associat-ed with the extent of disease and can be checked during treatment to monitor the response to treatment. A titer higher than 1:16 often corre-lates with extrapulmonary dissemination; this
Figure 3. Core-Needle Biopsy of the Vertebral Disk.
A specimen that was obtained from a core-needle biopsy of the vertebral disk and was stained with Gomori methe-namine silver (Panel A) shows a spherule (arrow) with-out visible budding. The same specimen, stained with periodic acid-Schiff (Panel B), also shows a spherule (arrow).
B
A
Cases in Primary Care NEJM.org

38
BacktoTableofContents
n engl j med 376;18 nejm.org May 4, 20171788
Clinical Problem-Solving
patient had a titer of 1:64.10 A urine coccidioides antigen enzyme immunoassay was found to have a sensitivity of 71% in patients with profound immunosuppression, although more data are needed to assess its performance in immuno-competent patients.11
On the basis of limited data from case series, treatment of severe coccidioidal osteomyelitis, defined as extensive vertebral involvement, spine instability, or risk of spinal cord impingement, often consists of initial administration of am-photericin B, followed by administration of itra-conazole, fluconazole, posaconazole, or voricon-azole. Liposomal amphotericin B can be used as an alternative to amphotericin B in patients who are at risk for drug-induced renal toxic effects. Moderate-to-severe disease is often treated with an oral azole alone.9 A randomized, controlled trial that compared fluconazole with itraconazole for nonmeningeal coccidioidomycosis showed no significant difference in response rates between the two treatments; however, a subgroup analy-sis suggested that patients who have skeletal infections are more likely to have a response to therapy with itraconazole than to therapy with
fluconazole.12 Adjunctive surgical débridement or stabilization is often indicated in these cases and is crucial if there is cord impingement or spine instability.13 The combination of medical and surgical treatment has been associated with better outcomes, including symptom relief and control of the disease, than medical therapy alone.5 Most cases of coccidioidal vertebral osteomyeli-tis require more than 1 year of antifungal treat-ment, and some require indefinite treatment.9
This case highlights an uncommon cause of vertebral osteomyelitis that manifested as chron-ic low back pain in an elderly man. It is important to consider the possible presence of C. immitis in the differential diagnosis of vertebral osteomy-elitis, even in areas in which coccidioidomycosis is not endemic, since patients may have previously lived in, or even briefly visited, endemic areas.
Presented at the Clinical Pathological Conference Series, De-partment of Medicine, Brigham and Women’s Hospital, and Harvard Medical School — both in Boston.
No potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
We thank Dr. Danny Milner for assistance with the patho-logical analysis and images.
References1. Galgiani JN, Ampel NM, Blair JE, et al. Coccidioidomycosis. Clin Infect Dis 2005; 41: 1217-23.2. Valdivia L, Nix D, Wright M, et al. Coccidioidomycosis as a common cause of community-acquired pneumonia. Emerg Infect Dis 2006; 12: 958-62.3. Brown J, Benedict K, Park BJ, Thomp-son GR III. Coccidioidomycosis: epidemi-ology. Clin Epidemiol 2013; 5: 185-97.4. Stevens DA. Coccidioidomycosis. N Engl J Med 1995; 332: 1077-82.5. Martirosyan NL, Skoch JM, Zaninovich O, Zoccali C, Galgiani JN, Baaj AA. A para-digm for the evaluation and management of spinal coccidioidomycosis. Surg Neurol Int 2015; 6: 107.6. Mirochnik BD, Lev S, Weingarten EP. Case 209: Disseminated coccidioidal spon-dylodiskitis. Radiology 2014; 272: 914-8.
7. Crum NF, Lederman ER, Stafford CM, Parrish JS, Wallace MR. Coccidioidomy-cosis: a descriptive survey of a reemerging disease: clinical characteristics and cur-rent controversies. Medicine (Baltimore) 2004; 83: 149-75.8. Stevens DA, Clemons KV, Levine HB, et al. Expert opinion: what to do when there is Coccidioides exposure in a labo-ratory. Clin Infect Dis 2009; 49: 919-23.9. Galgiani JN, Ampel NM, Blair JE, et al. 2016 Infectious Diseases Society of America (IDSA) clinical practice guide-line for the treatment of coccidioidomy-cosis. Clin Infect Dis 2016; 63(6): e112-e146.10. Nguyen C, Barker BM, Hoover S, et al. Recent advances in our understanding of the environmental, epidemiological, im-munological, and clinical dimensions of
coccidioidomycosis. Clin Microbiol Rev 2013; 26: 505-25.11. Durkin M, Connolly P, Kuberski T, et al. Diagnosis of coccidioidomycosis with use of the Coccidioides antigen enzyme im-munoassay. Clin Infect Dis 2008; 47(8): e69-e73.12. Galgiani JN, Catanzaro A, Cloud GA, et al. Comparison of oral f luconazole and itraconazole for progressive, nonmenin-geal coccidioidomycosis: a randomized, double-blind trial. Ann Intern Med 2000; 133: 676-86.13. Kakarla UK, Kalani MY, Sharma GK, Sonntag VK, Theodore N. Surgical man-agement of coccidioidomycosis of the spine: clinical article. J Neurosurg Spine 2011; 15: 441-6.Copyright © 2017 Massachusetts Medical Society.
clinical problem-solving series
The Journal welcomes submissions of manuscripts for the Clinical Problem-Solving series. This regular feature considers the step-by-step process of clinical decision
making. For more information, please see authors.NEJM.org.
Cases in Primary Care NEJM.org

39
BacktoTableofContents
Cases in Primary Care NEJM.org
CLINICAL PRACTICEThis Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the authors’ clinical recommendations.

40
BacktoTableofContents
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 376;2 nejm.org January 12, 2017 149
Clinical Practice
A 79-year-old woman visits your office for routine health maintenance. She has nor-mal daily bowel movements without rectal bleeding. Her medical history is notable for osteoarthritis but no other medical conditions. She takes nonsteroidal anti-inflammatory medication and multivitamins. Her maternal uncle received a diagno-sis of colorectal cancer at 65 years of age, but she has never undergone screening for colorectal cancer. Would you advise this patient to undergo screening for colorectal cancer, and if so, which screening strategy would you recommend?
The Clinic a l Problem
Colorectal cancer is the third most commonly diagnosed can-cer and cause of death from cancer in the United States1; however, it can be detected in asymptomatic patients at a curable stage, and several ran-
domized, controlled trials have shown lower mortality among patients who undergo screening than among those who do not. Screening can also detect precancerous polyps that can be removed during colonoscopy, thereby reducing the incidence of cancer. This review focuses on screening patients at average risk for the develop-ment of colorectal cancer.
S tr ategies a nd E v idence
Screening Options
Multiple strategies are available to screen patients who are at average risk for the development of colorectal cancer, including fecal occult blood testing (with the use of guaiac-based or immunochemical tests) alone or in combination with stool DNA examination, endoscopy (flexible sigmoidoscopy or colonoscopy), radiologic examination (computed tomographic [CT] colonography), and testing for blood-based molecular markers, such as circulating methylated septin 9 gene (SEPT9) DNA. Each strategy has differing characteristics with respect to accuracy, invasive-ness, interval, costs, and quality of evidence supporting its use. The advantages and disadvantages associated with each screening strategy are summarized in Table 1. Colorectal cancer screening involves not only the one-time use of a screen-ing test, but also repeated testing over a person’s lifetime (programmatic screening). In addition, if colonoscopy is not performed as the primary screening test, all other screening strategies require colonoscopy as follow-up to a positive test.
An audio version of this article is available at NEJM.org
From the Division of Gastroenterology, Department of Medicine, University of Washington School of Medicine, and the Department of Health Services, Univer-sity of Washington School of Public Health — both in Seattle. Address reprint requests to Dr. Inadomi at the Division of Gastroenterology, Department of Medi-cine, University of Washington School of Medicine, 1959 N.E. Pacific St., Seattle, WA 98195, or at jinadomi@ uw . edu.
N Engl J Med 2017;376:149-56.DOI: 10.1056/NEJMcp1512286Copyright © 2017 Massachusetts Medical Society.
Caren G. Solomon, M.D., M.P.H., Editor
Screening for Colorectal NeoplasiaJohn M. Inadomi, M.D.
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist.
The article ends with the author’s clinical recommendations.
Cases in Primary Care NEJM.org

41
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017150
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
150
Fecal Screening TestsFecal screening can be divided into two broad categories: those that detect blood from ulcerated colonic mucosa resulting from cancer or large polyps and those that detect molecular markers that are shed from cancerous epithelial cells. Fecal occult blood tests include guaiac-based tests and immunochemical tests that use anti-bodies to detect human blood. The fecal immu-nochemical test (FIT) has the advantage of not requiring dietary restrictions; such restrictions are necessary with guaiac-based tests because they may be falsely positive in the presence of blood from red meat or food that reacts with the guaiac (e.g., raw horseradish, turnips, or broccoli). FIT should be performed at home on successive bowel movements; digital rectal examination in the clinic does not provide an adequate stool sample for testing. One-time FIT has been re-ported to have a sensitivity of 79% (95% confi-dence interval [CI], 69 to 86) and a specificity of 94% (95% CI, 92 to 95) for detection of cancer, and two or three samples do not significantly increase the accuracy over a single sample.2 However, many types of immunochemical tests are available, and their test characteristics vary widely.
High-quality evidence supports a strategy of fecal occult blood testing every year or every 2 years to screen for colorectal cancer, with colo-noscopy used as follow-up to a positive test. Several randomized, controlled trials have shown up to 32% lower mortality from colorectal can-cer with this strategy than with no screening, with up to 30 years of follow-up (Table S1 in the Supplementary Appendix, available with the full text of this article at NEJM.org).3-7 Although these
studies used guaiac-based testing, almost all cur-rent population-based screening programs use immunochemical tests because their accuracy is greater and dietary restrictions are not required.
Molecular markers including abnormal DNA from cancerous cells can be detected in stool. FIT combined with a stool DNA test (FIT-DNA) has been approved by the Food and Drug Ad-ministration (FDA) for colorectal cancer screen-ing. One study showed that one-time FIT-DNA had a higher sensitivity for detection of colorec-tal cancer than one-time FIT alone (92.3% vs. 73.8%), but specificity was lower (86.6% vs. 94.9%).11 The screening interval differs between FIT (annual) and FIT-DNA (interval unknown, although the U.S. Preventive Services Task Force recommends 1 or 3 years), which makes a com-parison of the effectiveness of programmatic screening difficult. Data from studies evaluating the colorectal cancer mortality benefit of screen-ing FIT-DNA are lacking.
Endoscopic ScreeningFlexible Sigmoidoscopy
Randomized trials have shown that screening with flexible sigmoidoscopy, followed by colonos-copy if precancerous polyps are detected, reduces colorectal cancer mortality. Although not all tri-als have shown a significant benefit with respect to reducing mortality (mortality benefit),15,16 the intention-to-treat analyses in several large, ran-domized, controlled trials have confirmed the effectiveness of one-time and periodic (every 3 to 5 years) sigmoidoscopy, with a 26 to 31% lower mortality from colorectal cancer among patients who underwent flexible sigmoidoscopy screening than among those who underwent no screening
Key Clinical Points
Colorectal Cancer Screening
• Patients at average risk for the development of colorectal cancer should begin screening at 50 years of age. Screening between 76 and 85 years of age should be tailored, and screening should stop after 85 years of age.
• There is no “best” strategy for colorectal cancer screening; therefore, the most effective strategy is the one that a patient can adhere to consistently.
• Screening strategies for colorectal cancer among patients at average risk include annual fecal occult blood testing (with the use of highly sensitive guaiac-based or immunochemical tests) or colonoscopy every 10 years. If these strategies are declined, other screening options may include flexible sigmoidoscopy, computed tomographic colonography, or blood or stool DNA testing.
• Although the harms of specific tests vary greatly, the overall risks of complications from screening are related mainly to colonoscopies (performed up front or as follow-up to other positive screening tests) and polypectomies; these risks are low and similar among all strategies.
Cases in Primary Care NEJM.org

42
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017 151
Clinical Pr actice
Tabl
e 1.
Com
pari
son
of K
ey F
eatu
res
of S
cree
ning
Str
ateg
ies.
*
Stra
tegy
and
Eff
ect
on C
ance
r M
orta
lity†
Qua
lity
of E
vide
nce
Inte
rval
Cos
t-Ef
fect
iven
ess‡
Con
veni
ence
and
Req
uire
men
tsD
etec
tion
of P
reca
ncer
ous
Neo
plas
ia
Gua
iac
FOB
T an
d FI
T:
32%
low
er m
orta
lity
Mul
tiple
RC
Ts h
ave
show
n a
mor
tali-
ty b
enef
it (r
educ
tion
in m
orta
lity)
fo
r gu
aiac
FO
BT2-
7 ; al
thou
gh F
IT
is m
ore
accu
rate
than
gua
iac
FOB
T, R
CTs
eva
luat
ing
FIT
are
lack
ing
Ann
ual
May
be
mor
e ef
fect
ive
and
less
exp
ensi
ve th
an n
o sc
reen
ing;
tota
l cos
ts
low
er th
an n
o sc
reen
-in
g, b
ecau
se o
f the
hig
h ex
pens
e of
late
-sta
ge
canc
er tr
eatm
ent w
ith
biol
ogic
age
nts
Perf
orm
ed a
t hom
eD
oes
not r
elia
bly
dete
ct
prec
ance
rous
neo
plas
ia
Flex
ible
sig
moi
dosc
opy:
27
% lo
wer
mor
talit
yR
CTs
hav
e sh
own
a m
orta
lity
bene
fit8,
9Ev
ery
5 yr
Cos
t-effe
ctiv
e as
com
pare
d w
ith n
o sc
reen
ing
and
othe
r st
rate
gies
Lim
ited
bow
el p
repa
ratio
n as
co
mpa
red
with
col
onos
copy
Can
det
ect p
reca
ncer
ous
neop
lasi
a
Flex
ible
sig
moi
dosc
opy
plus
FI
T: 3
8% lo
wer
mor
talit
yA
sin
gle
RC
T sh
owed
that
flex
ible
si
gmoi
dosc
opy
plus
FIT
red
uces
ca
ncer
mor
talit
y m
ore
than
sig
-m
oido
scop
y al
one10
Ann
ual (
FIT)
and
ev
ery
10 y
r (s
ig-
moi
dosc
opy)
Cos
t-effe
ctiv
e as
com
pare
d w
ith n
o sc
reen
ing
and
othe
r st
rate
gies
Stra
tegy
that
com
bine
s en
do-
scop
ic a
nd s
tool
test
ing
Can
det
ect p
reca
ncer
ous
neop
lasi
a
FIT-
DN
A: u
nkno
wn
effe
ct
on m
orta
lity
Dat
a fr
om s
tudi
es s
how
ing
a m
orta
l-ity
ben
efit
are
lack
ing;
stu
dies
w
ere
limite
d to
the
dete
ctio
n of
ca
ncer
and
pre
canc
erou
s po
lyps
by
FIT
-DN
A a
s co
mpa
red
with
co
lono
scop
y11
Ever
y 1
or 3
yr
Less
effe
ctiv
e an
d m
ore
cost
ly th
an F
OB
T, F
IT,
or c
olon
osco
py
Perf
orm
ed a
t hom
eD
oes
not r
elia
bly
dete
ct
prec
ance
rous
neo
plas
ia
Col
onos
copy
: 68%
low
er
mor
talit
yA
pro
spec
tive
coho
rt s
tudy
sho
wed
a
mor
talit
y be
nefit
12Ev
ery
10 y
rC
ost-e
ffect
ive
as c
ompa
red
with
no
scre
enin
g an
d ot
her
stra
tegi
es
Req
uire
s fu
ll bo
wel
pre
para
tion;
us
ually
req
uire
s se
datio
n an
d an
esc
ort
Can
det
ect p
reca
ncer
ous
neop
lasi
a
CT
colo
nogr
aphy
: unk
now
n ef
fect
on
mor
talit
yD
ata
from
stu
dies
sho
win
g a
mor
tal-
ity b
enef
it ar
e la
ckin
g; s
tudi
es
wer
e lim
ited
to th
e de
tect
ion
of
canc
er b
y C
T co
lono
grap
hy a
s co
mpa
red
with
col
onos
copy
13
Ever
y 5
yrLe
ss e
ffect
ive
and
mor
e co
stly
than
FO
BT,
FIT
, or
col
onos
copy
No
seda
tion
requ
ired
but
re-
quir
es b
owel
pre
para
tion
Can
det
ect p
reca
ncer
ous
neop
lasi
a
Cir
cula
ting
met
hyla
ted
SE
PT9
DN
A: u
nkno
wn
ef
fect
on
mor
talit
y
Dat
a fr
om s
tudi
es s
how
ing
a m
orta
l-ity
ben
efit
are
lack
ing;
stu
dies
w
ere
limite
d to
the
dete
ctio
n of
ca
ncer
by
circ
ulat
ing
met
hyla
ted
SEPT
9 D
NA
as
com
pare
d w
ith
colo
nosc
opy14
Unk
now
nU
nkno
wn
A b
lood
test
may
be
asso
ciat
ed
with
gre
ater
adh
eren
ce th
an
that
with
oth
er s
cree
ning
te
sts
Doe
s no
t rel
iabl
y de
tect
pr
ecan
cero
us n
eopl
asia
* C
T de
note
s co
mpu
ted
tom
ogra
phy,
FIT
feca
l im
mun
oche
mic
al te
st, F
IT-D
NA
feca
l im
mun
oche
mic
al te
st c
ombi
ned
with
sto
ol D
NA
test
, FO
BT
feca
l occ
ult b
lood
test
, and
RC
T ra
ndom
ized
, co
ntro
lled
tria
l.†
The
effe
ct o
n m
orta
lity
repr
esen
ts a
com
pari
son
of t
he s
trat
egy
with
eith
er n
o sc
reen
ing
or o
ther
str
ateg
ies.
‡ C
ost-
effe
ctiv
enes
s w
as d
eter
min
ed a
s th
e co
st p
er q
ualit
y-ad
just
ed li
fe-y
ear
gain
ed.
Cases in Primary Care NEJM.org

43
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017152
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
(Table S1 in the Supplementary Appendix).8-10,13,17 However, the benefit of sigmoidoscopy is limited to cancer in the distal colon (rectum, sigmoid, and descending colon), for which the reduction in mortality was reported to be 46%.17
ColonoscopyCase-control and prospective cohort studies have estimated cancer mortality to be 68 to 88% lower among persons who undergo screening colonoscopy than among those who do not (Table S1 in the Supplementary Appendix).12,17-19 A meta-analysis of observational studies showed that despite a 68% lower mortality overall, no significant mortality benefit from colonoscopy was seen with respect to cancer in the proximal colon.17 This discrepancy may be explained by the quality of colonoscopy (i.e., incomplete colo-noscopy, poorer bowel preparation, or more dif-ficult polyp removal in the proximal colon) or differences in the biologic characteristics of prox-imal and distal colorectal cancer. The mechanism underlying the majority of colorectal cancers is chromosomal instability with early mutations in APC followed by KRAS and late mutations in P53.20 Sessile serrated polyps are more commonly associated with early KRAS or BRAF mutations that may lead to chromosomal or microsatellite instability than are adenomatous polyps.21 Ses-sile serrated polyps are often flat or minimally raised, making them more difficult than other polyps to detect by colonoscopy, and are more common in the proximal colon, which may con-tribute to the higher risk of proximal cancer than distal cancer after colonoscopy.22
Radiographic TestsPublished data from studies evaluating the effect of CT colonography on colorectal cancer inci-dence and mortality are lacking. The reported sensitivity and specificity of CT colonography to detect adenomas 1 cm in diameter or larger have ranged from 66.7 to 93.5% and from 86.0 to 97.9%, respectively.13 Because sessile serrated polyps are flat, CT colonography is inferior to colonoscopy for detection of these polyps.22 A polyp 6 mm in diameter or larger typically prompts a referral for optical colonoscopy, al-though the most useful size cutoff is controver-sial. Disadvantages of CT colonography include exposure to radiation and associated concerns regarding radiation-induced cancers and the po-tential need for additional testing and care for
lesions outside the colon that were discovered incidentally.
Blood-Based TestsThe FDA has approved a blood-based colorectal cancer screening test that detects circulating methylated SEPT9 DNA. Data from studies evalu-ating the colorectal cancer mortality benefit of blood-based screening are lacking. In a prospec-tive study conducted in a screening population, in which colonoscopy was used as the reference standard, the presence of circulating methylated SEPT9 DNA was shown to have a sensitivity of 48.2% (95% CI, 32.4 to 63.6), a specificity of 91.5% (95% CI, 89.7 to 93.1), a positive predic-tive value of 5.2% (95% CI, 3.5 to 7.5), and a negative predictive value of 99.5% (95% CI, 99.2 to 99.6) for detection of colorectal cancer.14
When to Start and Stop Screening
The U.S. Preventive Services Task Force used com-parative effectiveness modeling to examine dif-ferent ages at which to initiate screening. Start-ing screening at 45 years of age instead of 50 years could increase life-years and reduce cancer mortality but could also increase the potential harms due to the increased burden of colonos-copy; for this reason, the recommendations are to begin screening at 50 years of age in patients at average risk for colorectal cancer.23 Although the risk of colorectal cancer increases with age, the competing risk of death from other diseases and the risk of serious complications from colo-noscopy also increase with age.24,25 Several na-tional organizations recommend that screening for patients between 76 and 85 years of age should be tailored on the basis of the presence of coexisting illnesses and that screening should be stopped after patients reach 85 years of age.23,26 A microsimulation model suggested that the intensity of prior screening and the individual risk of colorectal cancer should also be consid-ered in determining the age at which to stop screening. Patients without a notable coexisting illness who are at average or higher risk for colorectal cancer and have had no prior screen-ing would be expected to benefit from screening into their 80s.27
Adherence
The percentage of U.S. residents with up-to-date screening for colorectal cancer has not increased
Cases in Primary Care NEJM.org

44
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017 153
Clinical Pr actice
appreciably since 2010 and remains at approxi-mately 60%.28 Currently, the percentage of U.S. adults undergoing colonoscopy screening greatly exceeds the percentage screened by fecal occult blood testing, and less than 1% undergo flexible sigmoidoscopy.29 Barriers to screening include costs, lack of knowledge of colorectal cancer and screening, underappreciation of the effect or se-verity of colorectal cancer, fatalism, and a per-ceived lack of importance or fear of screening tests.30 Costs remain a barrier despite the man-date in the Affordable Care Act that health plans cover colorectal cancer screening with no patient cost-sharing, because Medicare and other insur-ers impose a cost-sharing requirement when a colonoscopy is performed to evaluate a positive screening test or when a screening colonoscopy becomes a therapeutic procedure with the inclu-sion of polypectomy.31
Various interventions used in randomized, controlled trials have been shown to increase pa-tient participation in screening; such interventions include sending patients invitations from their primary care provider, sending reminder letters and making telephone calls, and mailing fecal occult blood test kits to patients’ homes. The most successful programs use patient navigators to reduce logistic barriers, address cultural issues, and encourage participants to undergo screen-ing; the use of patient navigators is especially important in underserved populations.32,33
The National Colorectal Cancer Roundtable has established a goal of 80% adherence to colorec-tal cancer screening by the year 2018. Kaiser Permanente has implemented a comprehensive strategy focused on FIT screening, with colonos-copy performed as follow-up to a positive test, and has reached and maintained the goal of 80% adherence through four rounds of screening.34 Adherence to screening tests varies among strat-egies, and preference of strategy varies by race and ethnic group; white participants more com-monly prefer colonoscopy, and nonwhite partici-pants tend to prefer fecal testing.30,35 To achieve the highest level of adherence to colorectal can-cer screening, it may be best to provide partici-pants a choice, because the “best” strategy is the one that they will adhere to consistently.
Quality of Screening
Maximizing the benefit of colorectal cancer screening requires a programmatic approach to
implementing screening strategies. The quality of a screening program should be measured by its ability to identify patients who are due for screen-ing, provide access to screening, assess adherence to the screening test and to follow-up colonos-copy if a noncolonoscopy screening test is posi-tive, document test outcomes and disseminate accurate follow-up recommendations, identify patients with a negative test to follow them for repeat screening at the appropriate intervals, and provide timely surgery for cancers. The rate of adenoma detection (the percentage of patients in whom precancerous polyps are detected during screening colonoscopy) differs substantially among endoscopists and may be used as a measure of the ability of screening to prevent colorectal cancer.36 A retrospective study showed that for every 1% increase in the rate of adenoma detec-tion, there is a 3% decrease in the rate of cancer developing after colonoscopy.37
Harms and Cost-Effectiveness
The harms of noncolonoscopy screening tests are low; however, all strategies require colonoscopy as follow-up to a positive test. As a result, the programmatic harms of screening are propor-tional to the number of colonoscopies and in particular polypectomies that are performed over the lifetime of the screened population. The tech-nical report from the Cancer Intervention and Surveillance Modeling Network (CISNET) Colorec-tal Cancer Working Group estimated the number of complications (perforations, gastrointestinal bleeding, nausea and vomiting, ileus, dehydration, abdominal pain, myocardial infarction, angina, arrhythmias, congestive heart failure, respira-tory arrest, syncope, hypotension, or shock) in a population of 1000 persons screened between 50 and 75 years of age to be 14 to 15 with colonos-copy at 10-year intervals, 9 to 12 with flexible sigmoidoscopy at 5-year intervals, 9 to 10 with FIT-DNA at 3-year intervals, and 10 to 11 with annual FIT.38
Cost-effectiveness models more than a decade ago suggested that programmatic screening with fecal occult blood testing, flexible sigmoidoscopy, or colonoscopy reduced colorectal cancer mor-tality at a cost society was willing to pay.39 Find-ings from a more recent analysis suggest that given the high expense of late-stage cancer treat-ment with biologic agents, FIT screening may be cost-saving, with reductions in both cancer mor-
Cases in Primary Care NEJM.org

45
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017154
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
tality and overall costs — even if one includes program support costs to increase screening uptake.40 Moreover, screening with colonosco-py or FIT is more effective in reducing cancer mortality and less expensive than screening with FIT-DNA41 or CT colonography.42 From an eco-nomic perspective, FIT-DNA or CT colonography should not be recommended unless screening with FIT, sigmoidoscopy, or colonoscopy has been declined.
Patients at Elevated Risk for Colorectal Cancer
Earlier and more frequent screening is recom-mended for patients at higher risk (Table S2 in the Supplementary Appendix). Patients with a first-degree relative in whom colorectal cancer developed before 60 years of age should undergo colonoscopy at 40 years of age or an age 10 years younger than the relative’s age when cancer de-veloped, whichever is earlier.52
A r e a s of Uncerta in t y
Data from completed randomized, controlled trials of screening colonoscopy are lacking, al-though several studies are under way. The Colo-noscopy versus Fecal Immunochemical Test in Reducing Mortality from Colorectal Cancer (CONFIRM) trial (ClinicalTrials.gov number, NCT01239082) is a randomized comparison of one-time colonoscopy with annual FIT plus colo-noscopy as follow-up to a positive test, to exam-ine colorectal cancer incidence and mortality over 10 years.44 A similar trial comparing colo-noscopy with FIT is being conducted in Spain (COLONPREV).45 Two additional European stud-ies are comparing screening colonoscopy with no screening (the Nordic-European Initiative on Colorectal Cancer [NordICC])4647 or with FIT or no screening (Screening of Swedish Colons [SCREESCO], NCT02078804) with respect to mor-tality from colorectal cancer.
Strategy
U.S. Preventive Services Task Force
(2016)23*
National Comprehensive Cancer Network
(2015)43
Multi-Society Task Force (2008)50†
American College of Gastroenterology
(2009)51
Sensitive guaiac FOBT‡ Annually Recommended (annually)
Recommended (annually)
Recommended (annually)
FIT‡ Annually Recommended (annually)
Recommended (annually)
Recommended (annually)
Stool DNA test Annually or every 3 yr§
Not recommended Recommended (interval unknown)
Recommended (every 3 yr)
Flexible sigmoidoscopy Every 5 yr Recommended¶ (every 5 yr)
Recommended (every 5 yr)
Recommended (every 5 yr)
Flexible sigmoidoscopy plus FIT
Every 10 yr, with annual FIT or sensitive FOBT
Not recommended Not recommended Not recommended
Colonoscopy Every 10 yr Recommended (every 10 yr)
Recommended (every 10 yr)
Preferred‖ (every 10 yr)
CT colonography Every 5 yr Not recommended Recommended (every 5 yr)
Recommended (every 5 yr)
Circulating methylated SEPT9 DNA
Not specified Unavailable for guideline
Unavailable for guideline
Unavailable for guideline
* No recommended strategy was provided.† The Multi-Society Task Force included the American Gastroenterological Association, the American Society for Gastrointestinal Endoscopy,
the American College of Gastroenterology, the American Cancer Society, and the American College of Radiology.‡ Sensitivity for detection of colorectal cancer is higher than 70%.§ The screening interval is for multitarget FIT-DNA.¶ Stool-based testing may be added at year 3.‖ Colonoscopy was identified as the preferred strategy.
Table 2. U.S. Guideline Recommendations for Screening and Screening Intervals to Reduce Mortality from Colorectal Cancer in Patients at Average Risk.
Cases in Primary Care NEJM.org

46
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017 155
Clinical Pr actice
Additional factors that might influence colorec-tal screening strategies include race, lifestyle fac-tors, or aspirin use. For example, among black men and women, the rates of death from colorec-tal cancer are 28.4 and 18.9 per 100,000 popula-tion, respectively; among white men and women, the corresponding rates are 18.7 and 13.2 per 100,000 population.48 Obesity, tobacco smoking, low physical activity, high intake of alcohol, high intake of red or processed meat, and low intake of fruits and vegetables are associated with in-creased risk of colorectal cancer, and regular use of aspirin has been associated with reduced risk. However, none of these factors are currently used to differentiate screening strategy, age of screening initiation, or surveillance intervals.49
Guidelines
Several national organizations have published guidelines on strategies to reduce colorectal cancer mortality, including the National Com-prehensive Cancer Network,43 the U.S. Multi-Society Task Force,50 and the American College of Gas-troenterology.51 Whereas these organizations rec-ommend certain screening strategies over others (Table 2), the 2016 U.S. Preventive Services Task Force recommendations do not support any spe-cific testing strategy or strategies over others, but rather highlight the importance of screening pa-tients at average risk for colorectal cancer between
50 and 75 years of age, with tailored screening for those between 76 and 85 years of age.23
Conclusions a nd R ecommendations
Although the patient described in the vignette is 79 years of age, she has not previously under-gone screening for colorectal cancer. Because of her limited coexisting illnesses, she is expected to derive an overall benefit from a first screening for colorectal cancer, and thus I would recom-mend screening for this patient. I would explore her reasons for not previously pursuing screen-ing and review with her the benefits and harms of different strategies. Because it is not feasible to summarize the entire menu of options dur-ing the span of a routine health maintenance visit, I would initially focus the discussion on colonoscopy or on annual FIT, followed by colonoscopy if the test was positive, and engage the patient in shared decision making. If she declined colonoscopy and FIT, I would discuss additional screening options, with the under-standing that insurance coverage, cost-sharing, and other barriers may affect the feasibility of some options.
Dr. Inadomi reports receiving consulting fees from ChemImage. No other potential conflict of interest relevant to this article was reported.
Disclosure forms provided by the author are available with the full text of this article at NEJM.org.
References1. United States Cancer Statistics. 1999-2013 Incidence and mortality data. Atlan-ta: Centers for Disease Control and Pre-vention, 2015 (https:/ / nccd .cdc .gov/ uscs/ ).2. Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal immuno-chemical tests for colorectal cancer: sys-tematic review and meta-analysis. Ann Intern Med 2014; 160: 171.3. Faivre J, Dancourt V, Lejeune C, et al. Reduction in colorectal cancer mortality by fecal occult blood screening in a French controlled study. Gastroenterology 2004; 126: 1674-80.4. Shaukat A, Mongin SJ, Geisser MS, et al. Long-term mortality after screening for colorectal cancer. N Engl J Med 2013; 369: 1106-14.5. Scholefield JH, Moss SM, Mangham CM, Whynes DK, Hardcastle JD. Notting-ham trial of faecal occult blood testing for colorectal cancer: a 20-year follow-up. Gut 2012; 61: 1036-40.6. Kronborg O, Jørgensen OD, Fenger C,
Rasmussen M. Randomized study of bien-nial screening with a faecal occult blood test: results after nine screening rounds. Scand J Gastroenterol 2004; 39: 846-51.7. Lindholm E, Brevinge H, Haglind E. Survival benefit in a randomized clinical trial of faecal occult blood screening for colorectal cancer. Br J Surg 2008; 95: 1029-36.8. Atkin WS, Edwards R, Kralj-Hans I, et al. Once-only flexible sigmoidoscopy screening in prevention of colorectal can-cer: a multicentre randomised controlled trial. Lancet 2010; 375: 1624-33.9. Schoen RE, Pinsky PF, Weissfeld JL, et al. Colorectal-cancer incidence and mor-tality with screening flexible sigmoidos-copy. N Engl J Med 2012; 366: 2345-57.10. Holme Ø, Løberg M, Kalager M, et al. Effect of flexible sigmoidoscopy screen-ing on colorectal cancer incidence and mor-tality: a randomized clinical trial. JAMA 2014; 312: 606-15.11. Imperiale TF, Ransohoff DF, Itzkowitz
SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med 2014; 370: 1287-97.12. Nishihara R, Wu K, Lochhead P, et al. Long-term colorectal-cancer incidence and mortality after lower endoscopy. N Engl J Med 2013; 369: 1095-105.13. Lin JS, Piper MA, Perdue LA, et al. Screening for colorectal cancer: an updated systematic review for the U.S. Preventive Services Task Force. Portland, OR: Kaiser Permanente Research Affiliates Evidence-based Practice Center, October 2015. (AHRQ publication no. 14-05203-EF-1) (https:/ / www .uspreventiveservicestaskforce .org/ Home/ GetFile/ 1/ 685/ coloncandraftes 135/ pdf).14. Church TR, Wandell M, Lofton-Day C, et al. Prospective evaluation of methylated SEPT9 in plasma for detection of asymp-tomatic colorectal cancer. Gut 2014; 63: 317-25.15. Hoff G, Grotmol T, Skovlund E, Bretthauer M. Risk of colorectal cancer
Cases in Primary Care NEJM.org

47
BacktoTableofContents
n engl j med 376;2 nejm.org January 12, 2017156
Clinical Pr actice
seven years after flexible sigmoidoscopy screening: randomised controlled trial. BMJ 2009; 338: b1846.16. Segnan N, Armaroli P, Bonelli L, et al. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian Randomized Controlled Trial — SCORE. J Natl Cancer Inst 2011; 103: 1310-22.17. Brenner H, Stock C, Hoffmeister M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal can-cer incidence and mortality: systematic review and meta-analysis of randomised controlled trials and observational stud-ies. BMJ 2014; 348: g2467.18. Kahi CJ, Imperiale TF, Juliar BE, Rex DK. Effect of screening colonoscopy on colorectal cancer incidence and mortality. Clin Gastroenterol Hepatol 2009; 7: 770-5.19. Manser CN, Bachmann LM, Brunner J, Hunold F, Bauerfeind P, Marbet UA. Colonoscopy screening markedly reduces the occurrence of colon carcinomas and carcinoma-related death: a closed cohort study. Gastrointest Endosc 2012; 76: 110-7.20. Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell 1990; 61: 759-67.21. O’Brien MJ, Zhao Q, Yang S. Colorec-tal serrated pathway cancers and precur-sors. Histopathology 2015; 66: 49-65.22. IJspeert JE, Tutein Nolthenius CJ, Kui-pers EJ, et al. CT-colonography vs. colo-noscopy for detection of high-risk sessile serrated polyps. Am J Gastroenterol 2016; 111: 516-22.23. U.S. Preventive Services Task Force, Bibbins-Domingo K, Grossman DC, et al. Screening for colorectal cancer: US Pre-ventive Services Task Force recommenda-tion statement. JAMA 2016; 315: 2564-75.24. Rutter CM, Johnson E, Miglioretti DL, Mandelson MT, Inadomi J, Buist DS. Ad-verse events after screening and follow-up colonoscopy. Cancer Causes Control 2012; 23: 289-96.25. Day LW, Kwon A, Inadomi JM, Walter LC, Somsouk M. Adverse events in older patients undergoing colonoscopy: a sys-tematic review and meta-analysis. Gastro-intest Endosc 2011; 74: 885-96.26. Qaseem A, Denberg TD, Hopkins RH Jr, et al. Screening for colorectal cancer: a guidance statement from the American College of Physicians. Ann Intern Med 2012; 156: 378-86.27. van Hees F, Saini SD, Lansdorp-Voge-laar I, et al. Personalizing colonoscopy screening for elderly individuals based on screening history, cancer risk, and comorbidity status could increase cost effectiveness. Gastroenterology 2015; 149: 1425-37.
28. Sabatino SA, White MC, Thompson TD, Klabunde CN. Cancer screening test use — United States, 2013. MMWR Morb Mortal Wkly Rep 2015; 64: 464-8.29. Vital signs: colorectal cancer screen-ing test use — United States, 2012. MMWR Morb Mortal Wkly Rep 2013; 62: 881-8.30. Brenner AT, Ko LK, Janz N, Gupta S, Inadomi J. Race/ethnicity and primary language: health beliefs about colorectal cancer screening in a diverse, low-income population. J Health Care Poor Under-served 2015; 26: 824-38.31. Doubeni CA, Corley DA, Zauber AG. Colorectal cancer health disparities and the role of US law and health policy. Gas-troenterology 2016; 150: 1052-5.32. Myers RE, Bittner-Fagan H, Daskala-kis C, et al. A randomized controlled trial of a tailored navigation and a standard intervention in colorectal cancer screen-ing. Cancer Epidemiol Biomarkers Prev 2013; 22: 109-17.33. Ritvo PG, Myers RE, Paszat LF, et al. Personal navigation increases colorectal cancer screening uptake. Cancer Epide-miol Biomarkers Prev 2015; 24: 506-11.34. Jensen CD, Corley DA, Quinn VP, et al. Fecal immunochemical test program per-formance over 4 rounds of annual screen-ing: a retrospective cohort study. Ann In-tern Med 2016; 164: 456-63.35. Inadomi JM, Vijan S, Janz NK, et al. Adherence to colorectal cancer screening: a randomized clinical trial of competing strategies. Arch Intern Med 2012; 172: 575-82.36. Barclay RL, Vicari JJ, Doughty AS, Johanson JF, Greenlaw RL. Colonoscopic withdrawal times and adenoma detection during screening colonoscopy. N Engl J Med 2006; 355: 2533-41.37. Corley DA, Jensen CD, Marks AR, et al. Adenoma detection rate and risk of colorectal cancer and death. N Engl J Med 2014; 370: 1298-306.38. Zauber A, Knudsen A, Rutter CM, Lansdorp-Vogelaar I, Kuntz KM. Evaluat-ing the benefits and harms of colorectal cancer screening strategies: a collabora-tive modeling approach. Rockville, MD: Agency for Healthcare Research and Quality, October 2015. (AHRQ publica-tion no. 14-05203-EF-2) (https:/ / www .uspreventiveservicestaskforce .org/ Home/ GetFile/ 1/ 16540/ cisnet-draft-modeling -report/ pdf).39. Pignone M, Saha S, Hoerger T, Man-delblatt J. Cost-effectiveness analyses of colorectal cancer screening: a systematic review for the U.S. Preventive Services Task Force. Ann Intern Med 2002; 137: 96-104.40. Lansdorp-Vogelaar I, Knudsen AB,
Brenner H. Cost-effectiveness of colorec-tal cancer screening. Epidemiol Rev 2011; 33: 88-100.41. Ladabaum U, Mannalithara A. Com-parative effectiveness and cost effective-ness of a multitarget stool DNA test to screen for colorectal neoplasia. Gastroen-terology 2016; 151(3): 427-439.e6.42. Vijan S, Hwang I, Inadomi J, et al. The cost-effectiveness of CT colonography in screening for colorectal neoplasia. Am J Gastroenterol 2007; 102: 380-90.43. Provenzale D, Jasperson K, Ahnen DJ, et al. Colorectal Cancer Screening, version 1.2015. J Natl Compr Canc Netw 2015; 13: 959-68.44. Robertson DJ, Kaminski MF, Brett-hauer M. Effectiveness, training and qual-ity assurance of colonoscopy screening for colorectal cancer. Gut 2015; 64: 982-90.45. Castells A, Quintero E. Program-matic screening for colorectal cancer: the COLONPREV study. Dig Dis Sci 2015; 60: 672-80.46. Kaminski MF, Bretthauer M, Zauber AG, et al. The NordICC Study: rationale and design of a randomized trial on colo-noscopy screening for colorectal cancer. Endoscopy 2012; 44: 695-702.47. Bretthauer M, Kaminski MF, Løberg M, et al. Population-based colonoscopy screening for colorectal cancer: a random-ized clinical trial. JAMA Intern Med 2016; 176: 894-902.48. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin 2015; 65: 5-29.49. Cancer facts & figures 2016. Atlanta: American Cancer Society, 2016 (http://www .cancer .org/ acs/ groups/ content/ @research/ documents/ document/ acspc-047079 .pdf).50. Levin B, Lieberman DA, McFarland B, et al. Screening and surveillance for the early detection of colorectal cancer and adenomatous polyps, 2008: a joint guide-line from the American Cancer Society, the US Multi-Society Task Force on Colo-rectal Cancer, and the American College of Radiology. Gastroenterology 2008; 134: 1570-95.51. Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, Inadomi JM. American College of Gastroenterology guidelines for colorectal cancer screening 2009 [corrected]. Am J Gastroenterol 2009; 104: 739-50.52. Schoen RE, Razzak A, Yu KJ, et al. In-cidence and mortality of colorectal cancer in individuals with a family history of colorectal cancer. Gastroenterology 2015; 149(6): 1438-1445.e1.Copyright © 2017 Massachusetts Medical Society.
Cases in Primary Care NEJM.org
48
BacktoTableofContents
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
n engl j med 375;19 nejm.org November 10, 20161868
Clinical Practice
A 73-year-old woman with a history of dyspnea on exertion presents for a follow-up visit after hospitalization for acute worsening of dyspnea and orthopnea. On admission to the hospital, the patient had atrial fibrillation with a ventricular rate of 120 beats per minute, and chest radiography revealed pulmonary venous hypertension. Despite anticoagulation, rate control with a beta-blocker, and administration of loop diuret-ics during the hospitalization, she continues to have fatigue and exertional dyspnea. On physical examination, the body-mass index (BMI; the weight in kilograms divided by the square of the height in meters) is 39, pulse 76 beats per minute, and blood pres-sure 160/70 mm Hg. There is jugular venous distention and lower-extremity edema but no third heart sound, murmurs, or rales. The serum creatinine level is 1.4 mg per deciliter (124 μmol per liter), estimated glomerular filtration rate (GFR) 37 ml per min-ute per 1.73 m2 of body-surface area, and N-terminal pro–brain natriuretic peptide (NT-proBNP) level 300 pg per milliliter (age-specific and sex-specific normal range, 10 to 218 pg per milliliter). Echocardiography reveals an ejection fraction of 70%, a normal left ventricular cavity dimension and wall thickness, and left atrial enlarge-ment. Doppler echocardiography shows elevated left atrial pressure (E/e′ ratio, 22) and an estimated pulmonary-artery systolic pressure of 52 mm Hg. How should this patient’s condition be managed?
The Clinic a l Problem
Epidemiologic studies indicate that up to 50% of patients with heart failure have a preserved ejection fraction, and this proportion has in-creased over time.1 In observational studies, rates of hospitalization and death
among patients who have heart failure with a preserved ejection fraction approach those among patients who have heart failure with a reduced ejection fraction,1 but in clinical-trial populations, outcomes are better in patients who have heart failure with a preserved ejection fraction.2 Death from noncardiovascular causes is more common in patients who have heart failure with a preserved ejection fraction than in those with a reduced ejection fraction.3,4
Ventricular diastolic dysfunction (impaired relaxation and increased diastolic stiff-ness) that is present at rest or induced by stress (from exercise, tachycardia, or hyper-tension) is a central perturbation in heart failure with a preserved ejection frac-tion.1,5-9 Although the ejection fraction is normal at rest, the ejection fraction does not increase appropriately with stress,1 and other measures of systolic function are abnor-mal.10 Endothelial dysfunction, arterial stiffening, and increased ventricular systolic
An audio version of this article
is available at NEJM.org
From the Department of Cardiovascular Diseases, Mayo Clinic, Rochester, MN. Address reprint requests to Dr. Redfield at Guggenheim 9, Mayo Clinic, 200 First St. SW, Rochester, MN 55905, or at redfield . margaret@ mayo . edu.
N Engl J Med 2016;375:1868-77.DOI: 10.1056/NEJMcp1511175Copyright © 2016 Massachusetts Medical Society.
Caren G. Solomon, M.D., M.P.H., Editor
Heart Failure with Preserved Ejection Fraction
Margaret M. Redfield, M.D.
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist.
The article ends with the author’s clinical recommendations.
Cases in Primary Care NEJM.org

49
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 2016 1869
Clinical Pr actice
1869
stiffness are also common and may result in heightened sensitivity to changes in load; this sen-sitivity manifests as rapid-onset pulmonary edema with increases in load and excessive hypotension with decreases in load.1 Exercise performance is impaired owing to impaired chronotropic, vaso-dilatory, and ventricular diastolic and systolic re-serve functions and impaired oxygen uptake and utilization in the peripheral muscles.5,11,12
The fundamental pathophysiological pertur-bation leading to heart failure with a preserved ejection fraction remains incompletely defined, but traditionally it has been attributed to hypertensive left ventricular remodeling1 (Fig. 1). Systemic mi-crovascular endothelial inflammation related to coexisting conditions has been proposed as an additional mechanism leading to myocardial in-flammation and fibrosis, increases in oxidative stress, and alterations in cardiomyocyte signal-ing pathways. These alterations promote cardio-myocyte remodeling and dysfunction (Fig. 1)13,14 as well as microvascular dysfunction and rarefac-tion in cardiac15,16 and skeletal11,12 muscle (Fig. 1).
S tr ategies a nd E v idence
Diagnosis and Evaluation
Since signs and symptoms of heart failure are non-specific, clinicians should maintain a high index of suspicion for heart failure in patients with risk factors, but they also should consider alternative or contributing diagnoses (Fig. 2). The clinical his-tory should include ascertainment of reduced symptoms in response to diuretic therapy and
previous hospitalizations for or complicated by heart failure. In some patients, heart failure mani-fests as “unexplained” exertional dyspnea. In such patients, differentiating heart failure from noncar-diac dyspnea or deconditioning can be challeng-ing. In patients with suspected heart failure, com-prehensive Doppler echocardiography should be performed.
Echocardiographic Findings and Natriuretic Peptide Levels
In observational studies and clinical trials, the value used to define a “preserved” ejection frac-tion has ranged from 40 to 55%, but current guide-lines recommend a partition value of 50%.17,18 An ejection fraction of 40 to 49% is a gray area.17 Patients who previously had an ejection fraction of less than 40% but in whom the ejection frac-tion increased with therapy for heart failure are considered to have “recovered” heart failure with a reduced ejection fraction. In these patients, medications for heart failure that have a proven benefit in patients with a reduced ejection frac-tion should be continued.
If the ejection fraction is preserved, evidence of altered cardiac structure and function should be sought to provide further objective evidence of heart failure (Fig. 2). The size of the left ven-tricular cavity is usually normal. Evidence of left ventricular hypertrophy (Fig. 2) is common but absent in many patients.8,19 Doppler echocardio-graphic evidence of diastolic dysfunction (slowed ventricular relaxation and increased diastolic stiff-ness or elevated left atrial pressure) is common
Key Clinical Points
Heart Failure with Preserved Ejection Fraction
• In patients who have signs and symptoms of heart failure but a preserved ejection fraction, objective evidence of abnormal cardiac structure and function should be confirmed by means of echocardiography, electrocardiography, chest radiography, and measurement of natriuretic peptide levels.
• Natriuretic peptide levels may be normal in patients who have heart failure with a preserved ejection fraction, particularly in obese patients or those with symptoms only on exertion.
• Right heart catheterization may be required in patients in whom there is indeterminate noninvasive testing or evidence of pulmonary hypertension.
• Medications that improve outcomes in patients who have heart failure with a reduced ejection fraction have not been shown to be of benefit in those who have heart failure with a preserved ejection fraction.
• Treatment of heart failure with a preserved ejection fraction should include diuretics for volume overload, treatment for cardiovascular and noncardiovascular coexisting conditions, aerobic exercise training to increase exercise tolerance, education regarding self-care, and disease management programs for patients with refractory symptoms or frequent hospitalizations for heart failure.
Cases in Primary Care NEJM.org

50
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 20161870
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
(Fig. 2).8,9,20 However, diastolic dysfunction also may be present in patients who do not have heart failure21 and absent in patients who have received aggressive treatment for heart failure or those with predominantly exertional symptoms.6,7 The left atrium is usually enlarged. Pulmonary-artery systolic pressure, estimated by means of Doppler echocardiography, is often elevated (>35 mm Hg).22 Right ventricular systolic dysfunction is present in 20 to 30% of patients, often in association with atrial fibrillation.23 Atrial remodeling can lead to annular dilatation and functional mitral and tri-cuspid regurgitation, but primary valvular disease should be ruled out.
Atrial fibrillation is very common and may precede, present concurrently with, or occur sub-sequent to the onset of heart failure with a pre-served ejection fraction.24 Radiographic evidence of heart failure (Fig. 2) is common in patients who present with acute heart failure, but radio-graphic evidence of heart failure is not necessar-ily present in patients who are in stable condi-tion. Ventricular wall stress and thus circulating levels of natriuretic peptides are lower in patients who have heart failure with a preserved ejection fraction than in patients who have heart failure with a reduced ejection fraction.25 Levels of na-triuretic peptides may be normal in up to 30%
Figure 1. Traditional and Emerging Pathophysiological Models of Heart Failure with Preserved Ejection Fraction.
Most patients who have heart failure with a preserved ejection fraction have a history of hypertension. In the traditional pathophysiolog-ical model, pressure overload leads to concentric left ventricular hypertrophic and fibrotic remodeling and diastolic dysfunction. Ulti-mately, the left ventricular diastolic dysfunction leads to left atrial hypertension and remodeling, pulmonary venous hypertension, and right ventricular and atrial remodeling and dysfunction. Atrial fibrillation is common because of the chronic left atrial hypertension and subsequent structural and electrical remodeling. In the emerging model, proinflammatory cardiovascular and noncardiovascular coex-isting conditions (e.g., hypertension, obesity, diabetes, the metabolic syndrome, lung disease, smoking, and iron deficiency) lead to sys-temic microvascular endothelial inflammation, global cardiac and skeletal-muscle inflammation, and subsequent fibrosis. These condi-tions also lead to increases in oxidative stress that limit nitric oxide–cyclic guanosine monophosphate (NO–cyclic GMP)–protein kinase G signaling, promoting global cardiomyocyte hypertrophy and intrinsic myofiber stiffness. Finally, coronary microvascular inflammation results in microvascular dysfunction and rarefaction with reduced microvascular density and coronary flow reserve. Similar changes oc-cur in the skeletal-muscle vasculature with reduced oxygen delivery and utilization.
A Traditional Model B Emerging Model
Increases in oxidative stressDecreases in NO–cyclic GMP
signaling
Microvascular dysfunctionand rarefaction
Muscle inflammation
Myofiber stiffnessCardiomyocyte hypertrophy
Fibrosis
RemodelingDiastolic dysfunctionSystolic dysfunction
Concentric hypertrophyFibrosisDiastolic dysfunction
Systemic hypertensionVascular dysfunction
Left Ventricle
Left Atrium
RemodelingDiastolic dysfunctionSystolic dysfunction
RemodelingDiastolic dysfunctionSystolic dysfunction
Right Ventricle
Right Atrium
Proinflammatory coexisting conditions
Systemic microvascular endothelial inflammation
Global cardiac remodeling and dysfunctionImpaired coronary flow reserveImpaired oxygen delivery, uptake, and utilization
in skeletal muscle
Left atrial hypertension
Right atrial hypertension
Pulmonary hypertensionAtrial fibrillation
Cases in Primary Care NEJM.org
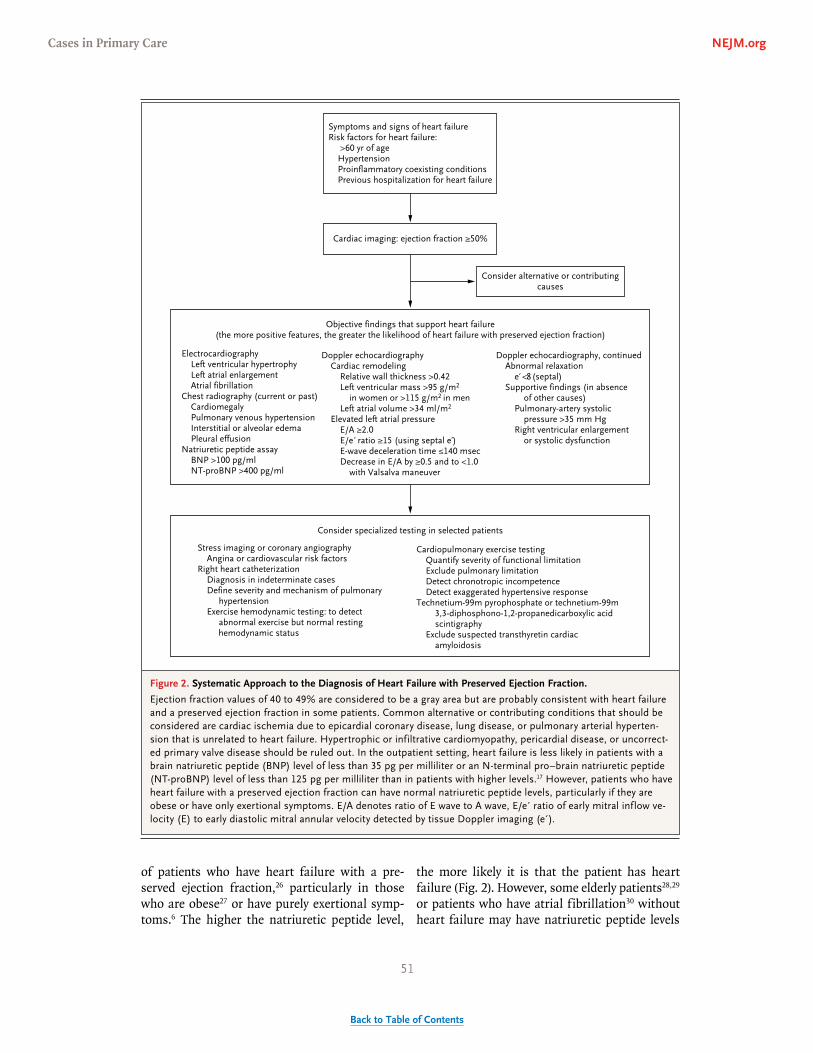
51
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 2016 1871
Clinical Pr actice
of patients who have heart failure with a pre-served ejection fraction,26 particularly in those who are obese27 or have purely exertional symp-toms.6 The higher the natriuretic peptide level,
the more likely it is that the patient has heart failure (Fig. 2). However, some elderly patients28,29 or patients who have atrial fibrillation30 without heart failure may have natriuretic peptide levels
Figure 2. Systematic Approach to the Diagnosis of Heart Failure with Preserved Ejection Fraction.
Ejection fraction values of 40 to 49% are considered to be a gray area but are probably consistent with heart failure and a preserved ejection fraction in some patients. Common alternative or contributing conditions that should be considered are cardiac ischemia due to epicardial coronary disease, lung disease, or pulmonary arterial hyperten-sion that is unrelated to heart failure. Hypertrophic or infiltrative cardiomyopathy, pericardial disease, or uncorrect-ed primary valve disease should be ruled out. In the outpatient setting, heart failure is less likely in patients with a brain natriuretic peptide (BNP) level of less than 35 pg per milliliter or an N-terminal pro–brain natriuretic peptide (NT-proBNP) level of less than 125 pg per milliliter than in patients with higher levels.17 However, patients who have heart failure with a preserved ejection fraction can have normal natriuretic peptide levels, particularly if they are obese or have only exertional symptoms. E/A denotes ratio of E wave to A wave, E/e′ ratio of early mitral inflow ve-locity (E) to early diastolic mitral annular velocity detected by tissue Doppler imaging (e′).
Objective findings that support heart failure(the more positive features, the greater the likelihood of heart failure with preserved ejection fraction)
Symptoms and signs of heart failureRisk factors for heart failure:
>60 yr of ageHypertensionProinflammatory coexisting conditionsPrevious hospitalization for heart failure
Consider alternative or contributingcauses
Cardiac imaging: ejection fraction ≥50%
ElectrocardiographyLeft ventricular hypertrophyLeft atrial enlargementAtrial fibrillation
Chest radiography (current or past)CardiomegalyPulmonary venous hypertensionInterstitial or alveolar edemaPleural effusion
Natriuretic peptide assayBNP >100 pg/mlNT-proBNP >400 pg/ml
Doppler echocardiographyCardiac remodeling
Relative wall thickness >0.42Left ventricular mass >95 g/m2
in women or >115 g/m2 in menLeft atrial volume >34 ml/m2
Elevated left atrial pressureE/A ≥2.0E/e ratio ≥15 (using septal e′)E-wave deceleration time ≤140 msecDecrease in E/A by ≥0.5 and to <1.0
with Valsalva maneuver
Doppler echocardiography, continuedAbnormal relaxation
e′ <8 (septal)Supportive findings (in absence
of other causes)Pulmonary-artery systolic
pressure >35 mm HgRight ventricular enlargement
or systolic dysfunction
Consider specialized testing in selected patients
Stress imaging or coronary angiographyAngina or cardiovascular risk factors
Right heart catheterizationDiagnosis in indeterminate casesDefine severity and mechanism of pulmonary
hypertensionExercise hemodynamic testing: to detect
abnormal exercise but normal resting hemodynamic status
Cardiopulmonary exercise testingQuantify severity of functional limitationExclude pulmonary limitationDetect chronotropic incompetenceDetect exaggerated hypertensive response
Technetium-99m pyrophosphate or technetium-99m3,3-diphosphono-1,2-propanedicarboxylic acidscintigraphy
Exclude suspected transthyretin cardiacamyloidosis
Cases in Primary Care NEJM.org

52
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 20161872
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
that are similar to those of patients with heart failure.
Specialized Testing in Selected Patients
Specific cardiac conditions that can cause heart failure when a preserved ejection fraction is pres-ent (e.g., pericardial disease and hypertrophic or infiltrative cardiomyopathies) must be considered in the differential diagnosis in patients who have heart failure with a preserved ejection fraction (Fig. 2). Epicardial coronary atherosclerosis can account for symptoms of heart failure with exer-tional dyspnea or angina, but angina is also com-mon in patients who do not have coronary dis-ease.31 In most patients with coronary disease, the coronary disease is of insufficient severity to ac-count for the severity of heart failure, but it is a risk factor for future coronary events and death.31
Stress testing, coronary angiography, or both should be performed if the patient has symptoms of or risk factors for coronary artery disease and is a candidate for anti-ischemic medications or revascularization. Standard exercise stress testing provides information about functional limitation and about the possibility of chronotropic incom-petence or exaggerated hypertensive response to exercise. Cardiopulmonary exercise testing can be useful to rule out noncardiac limitations to exercise such as poor effort, deconditioning, and pulmonary disease. Pulmonary-artery catheteriza-tion with or without exercise may be needed to establish the diagnosis in patients in whom the findings of noninvasive studies are indeterminate or to document the severity and mechanism of pulmonary hypertension when pulmonary-artery systolic pressure estimated with Doppler echocar-diography is significantly elevated (>50 mm Hg).
Pulmonary hypertension in heart failure is due to pulmonary venous hypertension and sometimes modest increases (2 to 4 Wood units) in pulmo-nary vascular resistance22; higher values should spur evaluation of other causes contributing to pulmonary hypertension. Large “V waves” (twice the mean pulmonary arterial wedge pressure value and >25 mm Hg) in the pulmonary arterial wedge pressure wave forms at rest or with stress (in the absence of marked mitral regurgitation) indicate reduced left atrial compliance, a hemo-dynamic hallmark of this condition.32,33
Cardiac magnetic resonance imaging may be useful if infiltrative cardiomyopathy (amyloidosis) or inflammatory cardiomyopathy (sarcoidosis) is
suspected. Scintigraphy with specific radioactive tracers can also assist in the recognition of transthyretin cardiac amyloidosis34 and should be considered in older patients with increased ventricular-wall thickness (≥12 mm) on echocar-diography.35
Renal artery stenosis should be considered in patients with risk factors for this condition (e.g., renal dysfunction or peripheral vascular disease) and a history of recurrent acute episodes of heart failure with a preserved ejection fraction.36 In pa-tients who have a normal or only mildly elevated creatinine level, the requirement for a high dose of a diuretic should prompt further evaluation of renal function (e.g., measurement of the cystatin C level).
Treatment
Since no therapy has been shown to improve out-comes in patients who have heart failure with a preserved ejection fraction, current therapy (Fig. 3) includes the relief of volume overload (when pres-ent), treatment of coexisting conditions, addition-al strategies that may increase exercise tolerance or reduce symptoms, and strategies to manage chronic disease and prevent hospitalizations.
Trials of Therapies to Improve OutcomesIndividually or in a meta-analysis, three random-ized trials of angiotensin antagonists (angiotensin-converting–enzyme [ACE] inhibitors or angio-tensin-receptor antagonists) involving patients who had heart failure with a preserved ejection fraction did not show significant effects of these agents on composite end points of all-cause or cardiovascular mortality and hospitalizations for heart failure.37 The mineralocorticoid-receptor an-tagonist spironolactone did not reduce rates of the primary composite outcome of death from cardio-vascular causes, aborted cardiac arrest, or hospi-talization for heart failure in these patients.38 Spironolactone reduced the rate of hospitalization for heart failure but not the rate of death from any cause or hospitalization for any cause, and it increased the rate of renal dysfunction and hyper-kalemia. Analyses that were limited to patients who were enrolled in centers in the Americas (which had higher event rates) showed beneficial effects of spironolactone on the composite pri-mary end point, but these post hoc analyses must be interpreted with caution.39The effect of beta-blockers in patients with heart failure and a pre-
Cases in Primary Care NEJM.org

53
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 2016 1873
Clinical Pr actice
served ejection fraction has not been evaluated in an adequately powered study, and the limited available data are conflicting.40-43
Thus, the use of angiotensin antagonists and
beta-blockers in the treatment of patients who have heart failure with a preserved ejection frac-tion should be limited to patients who have al-ternative indications for their use. The use of
Figure 3. Treatment Algorithm for Heart Failure with Preserved Ejection Fraction.
ACE denotes angiotensin-converting–enzyme inhibitor, and ARB angiotensin-receptor blocker.
Volume overload
Diuretics
HypertensionLung diseaseSleep apnea
Kidney diseaseObesityAtrial fibrillationCoronary diseaseElevated cardio-
vascular risk
DiureticsACE or ARB
(if patient has chronic kidneydisease)
Other agentsaccording toside effects andeffectiveness
Recenthospitalization
Consider disease managementprogram for heart failure
Consider pulmonary-arterypressure–guidedmanagement
Therapy accordingto guidelines
ACE or ARB(for hypertension)
Behavioralstrategies
PharmacotherapySurgery
Rate control Anticoagulation
according torisk scores
StatinsMedical therapyConsider revas-
cularization
Statins accordingto guidelines
Evaluate and manage underlying cardiovascular diseases and coexisting conditions
Education regarding heart failure and self-careAerobic exercise training
Consider rhythm controlfor persistent symptoms
Referral to clinical trials of agents and devices for heartfailure with preserved ejection fraction
Persistent symptoms
Yes No
Cases in Primary Care NEJM.org

54
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 20161874
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
spironolactone in patients who have heart failure with a preserved ejection fraction remains con-troversial.
Treatment of Volume OverloadDiuretics, which should be used for relief of symp-toms in patients with volume overload, should be adjusted according to the patient’s body weight, symptoms, and electrolyte status. Intermittent use of a thiazide-like diuretic such as metolazone, administered before the dose of a loop diuretic, may be helpful in outpatients with volume over-load that is refractory to higher doses of loop diuretics. However, the use of this agent calls for careful monitoring because of the risk of hypo-kalemia, hyponatremia, and worsening renal function. Persistent diuretic resistance may result from impaired diuretic absorption, necessitating intravenous administration of loop diuretics.
Although the evidence base is limited,17,18 so-dium restriction (to 2 g per day) may be helpful in patients who are prone to volume overload. At a minimum, high-sodium diets (>6 g per day) and rapid fluctuations in sodium intake should be avoided.17,18
Treatment of Coexisting ConditionsData to guide treatment of coexisting conditions and risk factors specifically in patients with heart failure and a preserved ejection fraction are very limited. Hypertension can exacerbate heart failure and predispose patients to other adverse out-comes.18 The Eighth Joint National Committee guidelines do not include a specific blood-pressure target for persons with heart failure. However, they recommend target blood pres-sures of less than 150/90 mm Hg in persons who are 60 years of age or older in the general population44 and of less than 140/90 mm Hg in persons with kidney disease (estimated GFR, <60 ml per minute per 1.73 m2 of body-surface area or >30 mg of albumin per gram of creatinine, regardless of diabetic status) and for persons with diabetes, regardless of age. A recent trial showed that lower rates of cardiovascular events and death were associated with blood-pressure targets lower than those recommended by current guidelines, but the trial did not enroll patients with heart failure.45
Most patients with heart failure and hyper-tension will require a diuretic. All patients with
hypertension and concomitant kidney disease should receive an angiotensin antagonist, re-gardless of their race or diabetic status44 (Fig. 3). In patients who do not have concomitant kidney disease, a thiazide-like diuretic, angiotensin an-tagonist, or calcium-channel blocker for non-blacks and a thiazide-like diuretic or calcium-channel blocker for blacks are appropriate for initial management.44 Aggressive use of vasodi-lators may lead to unacceptable side effects in patients with heart failure with a preserved ejec-tion fraction. The choice of additional agents to achieve blood-pressure control should be guided by the presence of coexisting conditions, the pa-tient’s ability to receive the agent without adverse effects, and the effect of the agent on blood pressure.
Patients should be treated with statins accord-ing to the usual criteria. Observational studies, including a propensity-score–matched analysis,46 have shown lower mortality among patients with heart failure with a preserved ejection fraction who have received statins than among those who have not received statins, but it remains unclear whether this association is causal.
Patients with coronary artery disease should receive medical therapies according to current guidelines.47 Limited (and potentially confound-ed) observational data in patients who have heart failure with a preserved ejection fraction and coronary disease have suggested better out-comes among those who have undergone com-plete revascularization than among those who have not.31 Revascularization can be considered for symptom relief in patients who are otherwise eligible for this procedure and who have clini-cally significant angina or in whom clinically significant ischemia is evident and thought to contribute to dyspnea as an angina equivalent.18
Atrial fibrillation should be managed accord-ing to current guidelines, which recommend rate control and anticoagulation initially, and a trial of rhythm control should be considered if symptoms persist despite adequate rate con-trol.17,18,48 Patients may be most likely to benefit from rhythm control if the symptoms of heart failure started or worsened after the onset of atrial fibrillation.
Obesity may contribute to exercise intoler-ance. In a small randomized trial, intentional weight loss significantly increased exercise toler-
Cases in Primary Care NEJM.org

55
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 2016 1875
Clinical Pr actice
ance but did not increase a heart failure–spe-cific quality-of-life score in obese patients who had heart failure with a preserved ejection frac-tion.49 To increase exercise tolerance, weight loss in obese patients (BMI, ≥35) with heart failure should be considered.17
Lung disease and disordered breathing dur-ing sleep are common comorbid conditions in patients with heart failure, provoke symptoms (dyspnea and fatigue) that are similar to those of heart failure, and may exacerbate hypertension and heart failure. Thus, aggressive treatment of concomitant lung disease and sleep apnea ac-cording to current guidelines is reasonable.
Other Therapies to Reduce Symptoms or Increase Exercise ToleranceNitrates are often prescribed for patients who have heart failure and a preserved ejection frac-tion. However, a randomized, placebo-controlled trial of isosorbide mononitrate did not show in-creases in submaximal exercise capacity or qual-ity-of-life scores in these patients.50
In small studies, exercise training has consis-tently been shown to produce clinically meaning-ful increases in exercise capacity and a reduction in symptoms.49,51 Cardiac rehabilitation programs are reimbursed by U.S. government payers for patients who have heart failure with a reduced ejection fraction but not for those with a preserved ejection fraction. Clinicians should recommend a daily target of 30 minutes of aerobic exercise tailored to the abilities and resources particular to each patient and should monitor compliance and address barriers to exercise training in on-going follow-up.17,18
Disease ManagementAll patients with heart failure should receive edu-cation regarding self-care. Self-care includes moni-toring of weight and symptoms, adjustment of doses of diuretics, compliance with dietary re-strictions, use of medications, exercise, and regu-lar follow-up.
In patients with refractory symptoms or fre-quent hospitalizations for heart failure, referral to a disease management program should be con-sidered. In patients who do not have a response to aggressive management, a palliative care pro-gram for symptom management and assistance in end-of-life planning should be considered.18
The effect of remote-monitoring strategies is unclear. However, a randomized trial of pulmo-nary-artery pressure–guided management in pa-tients with heart failure showed that this strat-egy reduced hospitalizations for heart failure in patients with a reduced or a preserved ejection fraction.52
A r e a s of Uncerta in t y
Owing to positive findings in a phase 2 study,53 a large outcomes trial of a neprilysin–angioten-sin-receptor inhibitor (sacubitril–valsartan) in patients with heart failure and a preserved ejec-tion fraction is ongoing (ClinicalTrials.gov num-ber, NCT01920711). Information from ongoing phase 2, randomized trials of a variety of other drugs and medical devices in patients with heart failure and a preserved ejection fraction is needed.54
The incidence of ventricular arrhythmias and the role of implantable defibrillators are unknown. The most appropriate strategies for the treatment of hypertension, obesity, diabetes, atrial fibrilla-tion, iron deficiency, anemia, and coronary dis-ease in patients with heart failure and a pre-served ejection fraction have not been defined.
Guidelines
Recently updated guidelines for the management of heart failure with a preserved ejection fraction are available.17,18 The recommendations in this ar-ticle are largely consistent with those guidelines.
Conclusions a nd R ecommendations
The patient in the vignette has heart failure with a preserved ejection fraction, exacerbated by, but probably predating, the onset of atrial fibrilla-tion. The dose of diuretics should be increased to reduce the patient’s clinical congestion. Given her hypertension and renal dysfunction, an angioten-sin antagonist should be added and other agents used as needed to achieve a blood pressure of less than 140/90 mm Hg. She should receive education regarding self-care for heart failure. Anticoagula-tion should be continued. If symptoms persist, a trial of rhythm control should be considered.
The patient’s atherosclerotic risk and the
Cases in Primary Care NEJM.org

56
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 20161876
T h e n e w e ngl a nd j o u r na l o f m e dic i n e
presence of coronary disease should be assessed to guide the use of statins and other treatments for coronary disease. Evaluation for sleep apnea may also be reasonable, given her obesity, fa-tigue, hypertension, and atrial fibrillation. Once her condition is stable, exercise and weight-loss programs should be commenced. Persistent symp-toms or recurrent hospitalizations should prompt referral to a disease management program for patients with heart failure. She should be in-
formed about clinical trials of therapeutic strate-gies for heart failure with a preserved ejection fraction.
Dr. Redfield reports serving as a member of a scientific com-mittee for Novartis (unpaid) and receiving consulting fees from Merck, Eli Lilly, and Actelion, fees for serving on a data and safety monitoring board for Covaria, and grant support from St. Jude Medical and Medtronic. No other potential conflict of in-terest relevant to this article was reported.
Disclosure forms provided by the authors are available with the full text of this article at NEJM.org.
References1. Gladden JD, Linke WA, Redfield MM. Heart failure with preserved ejection frac-tion. Pflugers Arch 2014; 466: 1037-53.2. Campbell RT, Jhund PS, Castagno D, Hawkins NM, Petrie MC, McMurray JJ. What have we learned about patients with heart failure and preserved ejection frac-tion from DIG-PEF, CHARM-preserved, and I-PRESERVE? J Am Coll Cardiol 2012; 60: 2349-56.3. Chan MM, Lam CS. How do patients with heart failure with preserved ejection fraction die? Eur J Heart Fail 2013; 15: 604-13.4. Lee DS, Gona P, Albano I, et al. A sys-tematic assessment of causes of death af-ter heart failure onset in the community: impact of age at death, time period, and left ventricular systolic dysfunction. Circ Heart Fail 2011; 4: 36-43.5. Borlaug BA. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction. Circ J 2014; 78: 20-32.6. Borlaug BA, Nishimura RA, Sorajja P, Lam CS, Redfield MM. Exercise hemody-namics enhance diagnosis of early heart failure with preserved ejection fraction. Circ Heart Fail 2010; 3: 588-95.7. Franssen C, Paulus WJ. Normal rest-ing pulmonary artery wedge pressure: a diagnostic trap for heart failure with pre-served ejection fraction. Eur J Heart Fail 2015; 17: 132-4.8. Lam CS, Roger VL, Rodeheffer RJ, et al. Cardiac structure and ventricular-vas-cular function in persons with heart fail-ure and preserved ejection fraction from Olmsted County, Minnesota. Circulation 2007; 115: 1982-90.9. Zile MR, Baicu CF, Gaasch WH. Dia-stolic heart failure — abnormalities in active relaxation and passive stiffness of the left ventricle. N Engl J Med 2004; 350: 1953-9.10. Borlaug BA, Lam CS, Roger VL, Rode-heffer RJ, Redfield MM. Contractility and ventricular systolic stiffening in hyper-tensive heart disease: insights into the pathogenesis of heart failure with pre-served ejection fraction. J Am Coll Cardiol 2009; 54: 410-8.11. Dhakal BP, Malhotra R, Murphy RM,
et al. Mechanisms of exercise intolerance in heart failure with preserved ejection fraction: the role of abnormal peripheral oxygen extraction. Circ Heart Fail 2015; 8: 286-94.12. Haykowsky MJ, Tomczak CR, Scott JM, Paterson DI, Kitzman DW. Determi-nants of exercise intolerance in patients with heart failure and reduced or pre-served ejection fraction. J Appl Physiol 2015; 119: 739-44.13. Paulus WJ, Tschöpe C. A novel para-digm for heart failure with preserved ejec-tion fraction: comorbidities drive myocar-dial dysfunction and remodeling through coronary microvascular endothelial in-flammation. J Am Coll Cardiol 2013; 62: 263-71.14. Shah SJ, Kitzman DW, Borlaug BA, et al. Phenotype-specific treatment of heart failure with preserved ejection fraction: a multiorgan roadmap. Circulation 2016; 134: 73-90.15. Mohammed SF, Hussain S, Mirzoyev SA, Edwards WD, Maleszewski JJ, Red-field MM. Coronary microvascular rar-efaction and myocardial fibrosis in heart failure with preserved ejection fraction. Circulation 2015; 131: 550-9.16. Mohammed SF, Majure DT, Redfield MM. Zooming in on the microvasculature in heart failure with preserved ejection fraction. Circ Heart Fail 2016; 9(7): e003272.17. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2016; 37: 2129-200.18. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the man-agement of heart failure: a report of the American College of Cardiology Founda-tion/American Heart Association Task Force on Practice Guidelines. Circulation 2013; 128(16): e240-327.19. Zile MR, Gottdiener JS, Hetzel SJ, et al. Prevalence and significance of altera-tions in cardiac structure and function in patients with heart failure and a pre-served ejection fraction. Circulation 2011; 124: 2491-501.20. Borlaug BA, Jaber WA, Ommen SR,
Lam CS, Redfield MM, Nishimura RA. Diastolic relaxation and compliance re-serve during dynamic exercise in heart failure with preserved ejection fraction. Heart 2011; 97: 964-9.21. Redfield MM, Jacobsen SJ, Burnett JC Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ven-tricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA 2003; 289: 194-202.22. Thenappan T, Prins KW, Cogswell R, Shah SJ. Pulmonary hypertension second-ary to heart failure with preserved ejec-tion fraction. Can J Cardiol 2015; 31: 430-9.23. Chatterjee NA, Steiner J, Lewis GD. It is time to look at heart failure with pre-served ejection fraction from the right side. Circulation 2014; 130: 2272-7.24. Zakeri R, Chamberlain AM, Roger VL, Redfield MM. Temporal relationship and prognostic significance of atrial fibrilla-tion in heart failure patients with pre-served ejection fraction: a community-based study. Circulation 2013; 128: 1085-93.25. Iwanaga Y, Nishi I, Furuichi S, et al. B-type natriuretic peptide strongly re-flects diastolic wall stress in patients with chronic heart failure: comparison be-tween systolic and diastolic heart failure. J Am Coll Cardiol 2006; 47: 742-8.26. Anjan VY, Loftus TM, Burke MA, et al. Prevalence, clinical phenotype, and out-comes associated with normal B-type na-triuretic peptide levels in heart failure with preserved ejection fraction. Am J Cardiol 2012; 110: 870-6.27. Bishu K, Deswal A, Chen HH, et al. Biomarkers in acutely decompensated heart failure with preserved or reduced ejection fraction. Am Heart J 2012; 164(5): 763-770.e3.28. Costello-Boerrigter LC, Boerrigter G, Redfield MM, et al. Amino-terminal pro-B-type natriuretic peptide and B-type na-triuretic peptide in the general commu-nity: determinants and detection of left ventricular dysfunction. J Am Coll Cardiol 2006; 47: 345-53.29. Redfield MM, Rodeheffer RJ, Jacob-sen SJ, Mahoney DW, Bailey KR, Burnett
Cases in Primary Care NEJM.org

57
BacktoTableofContents
n engl j med 375;19 nejm.org November 10, 2016 1877
Clinical Pr actice
JC Jr. Plasma brain natriuretic peptide concentration: impact of age and gender. J Am Coll Cardiol 2002; 40: 976-82.30. Richards M, Di Somma S, Mueller C, et al. Atrial fibrillation impairs the diag-nostic performance of cardiac natriuretic peptides in dyspneic patients: results from the BACH Study (Biomarkers in ACute Heart Failure). JACC Heart Fail 2013; 1: 192-9.31. Hwang SJ, Melenovsky V, Borlaug BA. Implications of coronary artery disease in heart failure with preserved ejection frac-tion. J Am Coll Cardiol 2014; 63: 2817-27.32. Pichard AD, Diaz R, Marchant E, Casanegra P. Large V waves in the pulmo-nary capillary wedge pressure tracing without mitral regurgitation: the influ-ence of the pressure/volume relationship on the V wave size. Clin Cardiol 1983; 6: 534-41.33. Rossi A, Gheorghiade M, Triposkiadis F, Solomon SD, Pieske B, Butler J. Left atrium in heart failure with preserved ejec-tion fraction: structure, function, and sig-nificance. Circ Heart Fail 2014; 7: 1042-9.34. Gillmore JD, Maurer MS, Falk RH, et al. Nonbiopsy diagnosis of cardiac trans-thyretin amyloidosis. Circulation 2016; 133: 2404-12.35. González-López E, Gallego-Delgado M, Guzzo-Merello G, et al. Wild-type transthyretin amyloidosis as a cause of heart failure with preserved ejection frac-tion. Eur Heart J 2015; 36: 2585-94.36. Anderson JL, Halperin JL, Albert NM, et al. Management of patients with pe-ripheral artery disease (compilation of 2005 and 2011 ACCF/AHA guideline rec-ommendations): a report of the American College of Cardiology Foundation/Ameri-can Heart Association Task Force on Prac-tice Guidelines. Circulation 2013; 127: 1425-43.37. Shah RV, Desai AS, Givertz MM. The effect of renin-angiotensin system inhibi-tors on mortality and heart failure hospi-talization in patients with heart failure and preserved ejection fraction: a system-
atic review and meta-analysis. J Card Fail 2010; 16: 260-7.38. Pfeffer MA, Pitt B, McKinlay SM. Spi-ronolactone for heart failure with pre-served ejection fraction. N Engl J Med 2014; 371: 181-2.39. Pfeffer MA, Claggett B, Assmann SF, et al. Regional variation in patients and outcomes in the Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist (TOPCAT) trial. Circulation 2015; 131: 34-42.40. Conraads VM, Metra M, Kamp O, et al. Effects of the long-term administra-tion of nebivolol on the clinical symp-toms, exercise capacity, and left ventricu-lar function of patients with diastolic dysfunction: results of the ELANDD study. Eur J Heart Fail 2012; 14: 219-25.41. Liu F, Chen Y, Feng X, Teng Z, Yuan Y, Bin J. Effects of beta-blockers on heart failure with preserved ejection fraction: a meta-analysis. PLoS One 2014; 9(3): e90555.42. van Veldhuisen DJ, Cohen-Solal A, Böhm M, et al. Beta-blockade with nebivo-lol in elderly heart failure patients with impaired and preserved left ventricular ejection fraction: data from SENIORS (Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure). J Am Coll Cardiol 2009; 53: 2150-8.43. Yamamoto K, Origasa H, Hori M. Ef-fects of carvedilol on heart failure with preserved ejection fraction: the Japanese Diastolic Heart Failure Study (J-DHF). Eur J Heart Fail 2013; 15: 110-8.44. James PA, Oparil S, Carter BL, et al. 2014 Evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311: 507-20.45. Wright JT Jr, Williamson JD, Whelton PK, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med 2015; 373: 2103-16.
46. Alehagen U, Benson L, Edner M, Dahlström U, Lund LH. Association be-tween use of statins and mortality in pa-tients with heart failure and ejection fraction of ≥50. Circ Heart Fail 2015; 8: 862-70.47. Ohman EM. Chronic stable angina. N Engl J Med 2016; 374: 1167-76.48. January CT, Wann LS, Alpert JS, et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibril-lation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014; 130(23): e199-267.49. Kitzman DW, Brubaker P, Morgan T, et al. Effect of caloric restriction or aero-bic exercise training on peak oxygen con-sumption and quality of life in obese old-er patients with heart failure with preserved ejection fraction: a randomized clinical trial. JAMA 2016; 315: 36-46.50. Redfield MM, Anstrom KJ, Levine JA, et al. Isosorbide mononitrate in heart fail-ure with preserved ejection fraction. N Engl J Med 2015; 373: 2314-24.51. Pandey A, Parashar A, Kumbhani DJ, et al. Exercise training in patients with heart failure and preserved ejection frac-tion: meta-analysis of randomized con-trol trials. Circ Heart Fail 2015; 8: 33-40.52. Adamson PB, Abraham WT, Bourge RC, et al. Wireless pulmonary artery pres-sure monitoring guides management to reduce decompensation in heart failure with preserved ejection fraction. Circ Heart Fail 2014; 7: 935-44.53. Solomon SD, Zile M, Pieske B, et al. The angiotensin receptor neprilysin in-hibitor LCZ696 in heart failure with pre-served ejection fraction: a phase 2 double-blind randomised controlled trial. Lancet 2012; 380: 1387-95.54. Nanayakkara S, Kaye DM. Manage-ment of heart failure with preserved ejec-tion fraction: a review. Clin Ther 2015; 37: 2186-98.Copyright © 2016 Massachusetts Medical Society.
Cases in Primary Care NEJM.org

58
BacktoTableofContents
Cases in Primary Care NEJM.org
INTERACTIVE MEDICAL CASESEach interactive case presents an evolving patient history and a series of questions and exercises designed to test diagnostic and therapeutic skills. Immediate feedback is given on answers and treatment choices, along with the opportunity to compare final scores with peers. Video, animation, and interactive content allows one to learn more about mechanisms, diagnostic tests, and treatments.

59
BacktoTableofContents
UNDER PRESSURE
PlaytheInteractiveMedicalCasenow. An internet connection is required.The following text summarizes information provided in the Interactive Medical Case.
E.M. DeFilippis, M.D., A. Vaidya, M.D., S. Ramani, M.D., B.S., C. French, M.D., and J.M. Kirshenbaum, M.D.
C a se Pr esen tation
A 61-year-old man presented to the emergency department with cough and shortness of breath. Earlier that morning, he had had sudden onset of severe shortness of breath and tightness in his chest. The chest tightness had resolved, but he continued to feel short of breath. He reported no fevers but did have a productive cough.
The patient also reported increasing shortness of breath when he was lying flat and waking from sleep, with the sudden need to sit upright in order to breathe. To breathe comfortably, he had to sleep on two or three pillows.
The patient also described a 2-month history of worsening fatigue, along with swelling of the legs and an unintentional weight loss of 6.5 kg. He used to walk about 5 km per day without difficulty, but now had chest tightness and shortness of breath when climbing a few stairs or walking a few steps.
Cases in Primary Care NEJM.org

60
BacktoTableofContents
DISSECTING A CASE OF ABDOMINAL PAIN
PlaytheInteractiveMedicalCasenow. An internet connection is required.The following text summarizes information provided in the Interactive Medical Case.
J.Casey, M.D., A. Vaidya, M.D., N. Frank, M.D., J.A. Beckman, M.D., and A. Miller, M.D., Ph.D
C a se Pr esen tation
A 43-year-old man with no notable medical history presented to the emergency department within 1 hour after the abrupt onset of abdominal pain. The patient stated that he had been dressing for work when severe, “crampy” abdominal pain occurred in the left upper quadrant. On a scale of 0 to 10, with 0 indicating no pain and 10 the worst imaginable pain, the patient rated the pain at 10. After the onset of pain, the patient had nausea, several episodes of nonbilious, nonbloody emesis, and flatus.
Cases in Primary Care NEJM.org


















