Case Study-Acute Pyelonephritis
14
INTRODUCTION A. Current trends about the disease condition Acute pyelonephritis can occur at any age. In neonates it is 1.5 times more common in boys and tends to be associated with abnormalities of the renal tract. Uncircumcised boys tend to have a higher incidence than circumcised boys. Beyond that age girls have a 10-fold higher incidence. In adult life it reflects the incidence of urinary tract infection (UTI) in that it is much more common in young women. Over 65 the incidence in men rises to match that of women. Glomerulonephritis (GN) comprises 25-30% of all cases of end-stage renal disease (ESRD).About one fourth of patients present with acute nephritis syndrome. Most cases that progress do so relatively quickly, and end-stage renal failure may occur within weeks or months of acute nephritic syndrome onset. Geographic and seasonal variations in the prevalence of post streptococcal glomerulonephritis (PSGN) are more marked for pharyngeally associated GN than for cutaneously associated disease. PGN has no predilection for any racial or ethnic group. A higher incidence (related to poor hygiene) may be observed in some socioeconomic group. Acute GN predominantly affects males (2:1 male- to-female ratio). PGN can occur at any age but usually develops in children. Outbreaks of PSGN are common in children aged 6-10 years. Acute glomerulonephritis refers to a specific set of renal diseases in which an immunologic mechanism triggers inflammation and proliferation of glomerular tissue that can result in damage to the basement membrane, mesangium, or capillary endothelium. Hippocrates originally described the manifestation of back pain and hematuria, which lead to oliguria or anuria. With the development of the microscope, Langhans was later able to describe these pathophysiologic glomerular changes. Most original research focuses on the post streptococcal patient. Acute glomerulonephritis is defined as the sudden onset of hematuria, proteinuria, and red blood cell casts. This clinical picture is often accompanied by hypertension, edema, and impaired renal function. Acute glomerulonephritis can be due to a primary renal or systemic disease. Glomerulonephritis represents 10-15% of glomerular diseases. Variable
-
Upload
mary-france-gonzaga -
Category
Documents
-
view
177 -
download
33
Transcript of Case Study-Acute Pyelonephritis
INTRODUCTION
A. Current trends about the disease condition
Acute pyelonephritis can occur at any age. In neonates it is 1.5 times more common in boys and tends to be associated with abnormalities of the renal tract. Uncircumcised boys tend to have a higher incidence than circumcised boys. Beyond that age girls have a 10-fold higher incidence. In adult life it reflects the incidence of urinary tract infection (UTI) in that it is much more common in young women. Over 65 the incidence in men rises to match that of women. Glomerulonephritis (GN) comprises 25-30% of all cases of end-stage renal disease (ESRD).About one fourth of patients present with acute nephritis syndrome. Most cases that progress do so relatively quickly, and end-stage renal failure may occur within weeks or months of acute nephritic syndrome onset. Geographic and seasonal variations in the prevalence of post streptococcal glomerulonephritis (PSGN) are more marked for pharyngeally associated GN than for cutaneously associated disease. PGN has no predilection for any racial or ethnic group. A higher incidence (related to poor hygiene) may be observed in some socioeconomic group. Acute GN predominantly affects males (2:1 male-to-female ratio). PGN can occur at any age but usually develops in children. Outbreaks of PSGN are common in children aged 6-10 years.
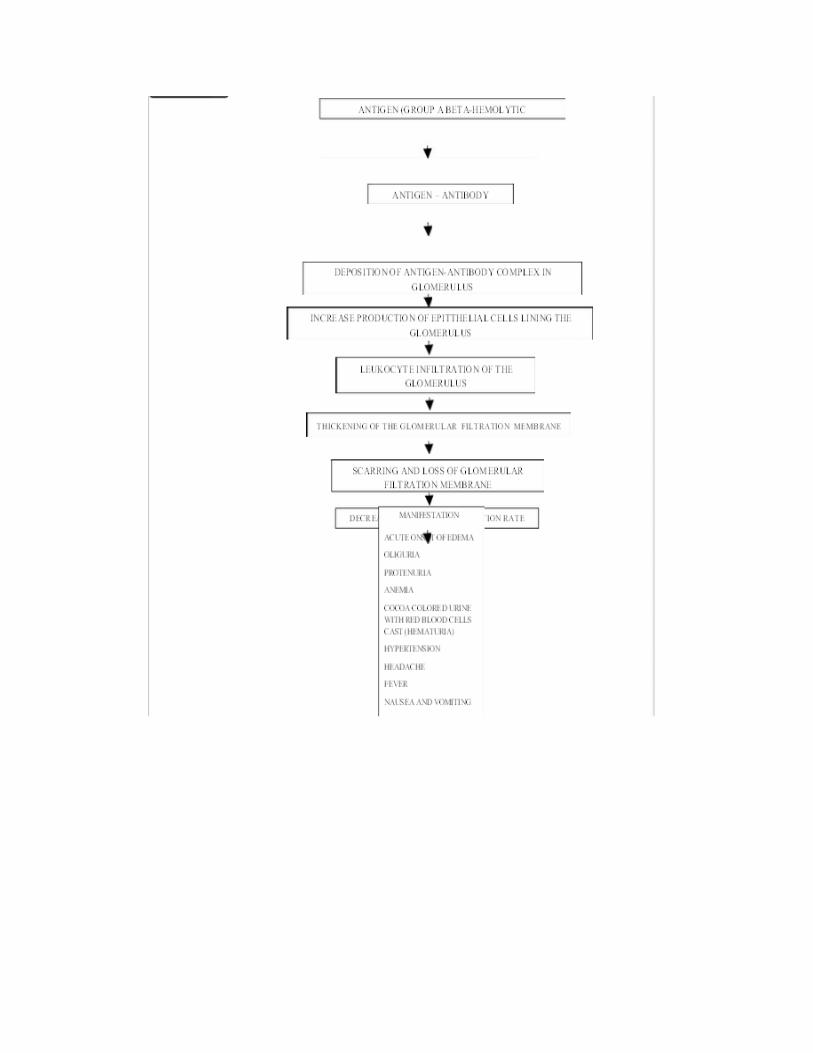
Acute glomerulonephritis refers to a specific set of renal diseases in which an immunologic mechanism triggers inflammation and proliferation of glomerular tissue that can result in damage to the basement membrane, mesangium, or capillary endothelium. Hippocrates originally described the manifestation of back pain and hematuria, which lead to oliguria or anuria. With the development of the microscope, Langhans was later able to describe these pathophysiologic glomerular changes. Most original research focuses on the post streptococcal patient. Acute glomerulonephritis is defined as the sudden onset of hematuria, proteinuria, and red blood cell casts. This clinical picture is often accompanied by hypertension, edema, and impaired renal function. Acute glomerulonephritis can be due to a primary renal or systemic disease. Glomerulonephritis represents 10-15% of glomerular diseases. Variable incidence has been reported due in part to the subclinical nature of the disease in more than one half the affected populations. Despite sporadic outbreaks, incidence of post streptococcal glomerulonephritis has fallen over the last few decades. Factors responsible for this decline may include better health care delivery and improved socioeconomic conditions. With some exceptions, a reduction in the incidence of post streptococcal glomerulonephritis has occurred inmost western countries. It remains much more common in regions such as Africa, the Caribbean, India, Pakistan, Malaysia, Papua New Guinea, and South America. Immunoglobulin A (IgA) nephropathy glomerulonephritis (ie, Berger disease) is the most common cause of glomerulonephritis worldwide. Most epidemic cases follow a course ending in complete patient recovery (as many as 100%). Sporadic cases of acute nephritis often progress to a chronic form. This progression occurs in as many as 30% of adult patients and 10% of pediatric patients .Glomerulonephritis is the most common cause of chronic renal failure (25%). The mortality rate of acute glomerulonephritis in the most commonly affected age group, pediatric patients; has been reported at 0-7% .A male-to-female ratio of 2:1 has been reported. Most cases occur in

patients aged 5-15 years and only 10% occur in patients older than 40 years. Acute nephritis may occur at any age, including infancy.
NURSING PROCESS
A. ASSESSMENT
1. PERSONAL DATA
A. Demographic Data
Name: Girl X Age: 15 y/o Sex: femaleReligious Affiliation: Catholic Role position of the family: Third daughterAddress: Libon, Albay Date of Birth: February 21, 1996Nationality: Filipino Health care Financing: FatherUsual source of medical care: Doctor
B. Environmental Status:Their house structures are made of concrete and wooden materials which was build
within a compound with their relatives. They have 2 bed rooms and their appliances are arranged properly in their divider as verbalized by the mother. They have water pump which their particular source of water for bathing, cleaning cooking etc. but not a source of water to drink because the family usually bought mineral water for their source.
C. Personal Habits:
She went to school every morning from 7:30 am to 4:30 am and play with her peers every
afternoon. She usually eats variety of vegetables like “sayote, papaya, carrots, kalabasa” as
verbalized by her mother, which are good for her heath but she loves to eat junk foods every
after meal. She usually plays a long period of time outside with her friends
D. Social:
She is the third daughter of Mr. and Mrs. Z and a high school student.
E. Psychological:
She loves to hang outside with her friend so when her mother cannot permit her to go
outside she usually cries and make herself busy inside the house by playing in the room alone.
2 .FAMILY HISTORY OF PAST ILLNESS
Her mother was the history of hypertension while her father has no illness.
3. HISTORY OF PAST ILLNESSS
According to the mother the patient has asthma which started when she was 3months
old. Since then every time the patient experiences the symptoms of asthma they take
salbutamol with the use of nebulizer to alleviate symptoms and improves airway function. The
patient’s asthma is usually triggered due to the weather changes, it usually occurs during
summer season or hot weather as the mother stated. When the patient has fever, cough and
colds the mother used OTC drugs like paracetamol for the patient condition. The patient had not
experience other childhood illnesses. Girl X has completed her childhood immunizations. The
patient has no allergies to drugs, animals, or insects, and was never hospitalized due to serious
illness.
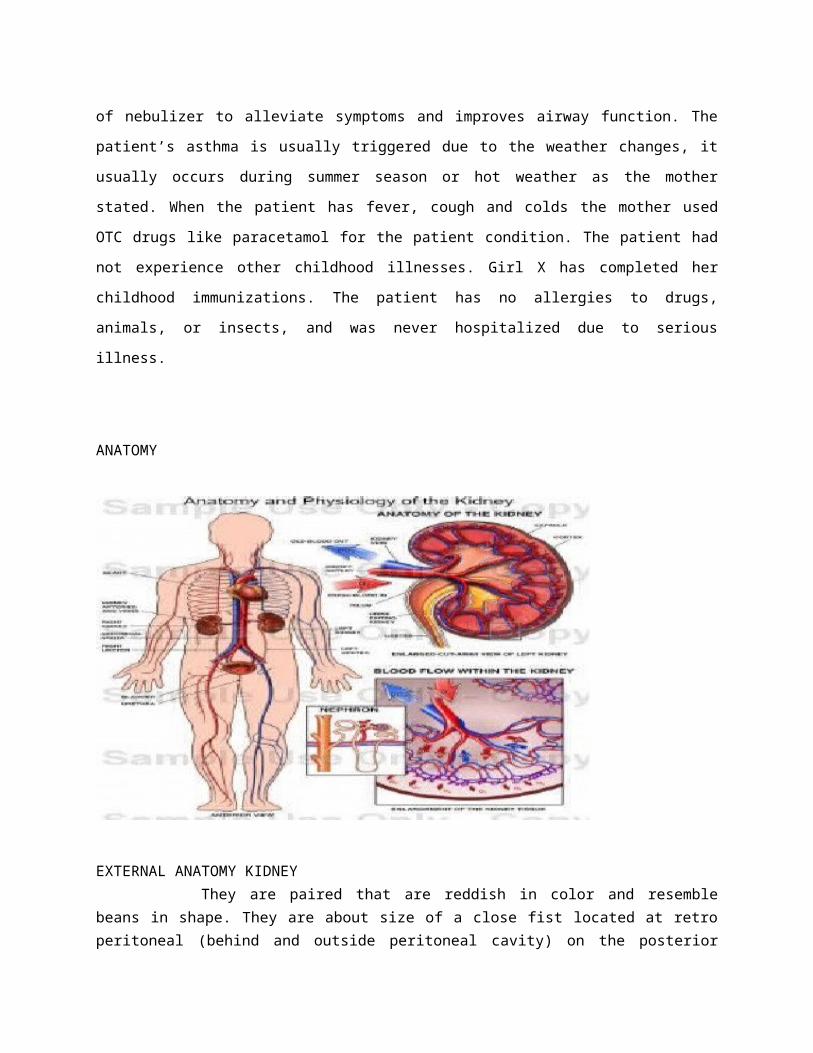
ANATOMY
EXTERNAL ANATOMY KIDNEY
They are paired that are reddish in color and resemble beans in shape. They
are about size of a close fist located at retro peritoneal (behind and outside peritoneal cavity) on
the posterior wall of the abdomen from 12 thoracic vertebrae to the third lumbar vertebrae in
adult
The average adult kidney weighs approximately 133-170g. (4.5 oz)and is 10-12
cm long 6 cm wide and 2.5 cm thick the right kidney is slight lower than the left due to the
location of the liver
Kidney are well protected by the ribs and by the muscles of the abdomen and back
3 LAYERS OF TISSUE SURROUNDING EACH KIDNEY1. RENAL CAPSULE- innermost layer, it is a smooth transparent fibrous connective tissue
membrane that connects with the outermost covering of the ureter at the hilum. It serves as a barrier against infection and trauma to the kidney
2. ADIPOSE CAPSULE- second layer it is a mass of fatty tissue that protects the kidney from blows. It firmly holds the kidney in the abdominal activity
3. RENAL CAPSULE- outer most layer which consist of a thin of a layer of fibrous connective tissue that also anchors the kidney to their surrounding structures and to the abdominal wall
INTERNALANATOMY OF KIDNEY The renal parenchyma is divided into two parts the cortex and the medulla
MEDULLA
Medulla is approximately 5 cm wide which is the inner portion of the kidney. It contains
the loop of Henle, the Vasa Recta and the collecting ducts of the juxtamedullary nephrons the
collecting duct from both the juxtamedullary and the cortical nephrons connect to renal pyramids
which are triangular and are situated with base facins the concave surface of the kidney and the
point (papilla)facins the hilum/pelvis. Each kidney contains approximately 8-18 pyramids. The
pyramids drain into 4 to 13 minor calices which drain into 2 major calices that open directly into
the renal pelvis. The renal pelvis is the beginning of the collecting system and is composed of
structures that are designed to collect and transport urine. Once the urine leaves the renal
pelvis, the composition of urine does not change.
CORTEX
- It is approximately 2 cm wide, is located farthest from the center of the kidney and around the
outer most edges. It contains the nephrons.
NEPHRONS
-these are the functional units of kidney. It is microscopic renal tubule which functions
as a filter. Each kidney has 1 million nephrons, which usually allows for adequate renal function
even if the opposite kidney is damaged or becomes nonfunctional. The structures are located
within the renal parenchymas that are responsible for initial formation of urine.
2 KINDS OF NEPHRONS
a. Cortical nephrons – this makes up 80 to 85% of total number of nephrons in the kidney which
are located in the innermost part of the cortex.
b. Juxtamendullary – nephrons which make up the remaining 15 to 20% are located deeper in
the cortex. There are distinguished by long loops of Henle, which are surrounded by long
capillary loops called Vasa Recta that dip into Medulla of the Kidney.
Nephrons are made up of two basic components; a filtering element component of an enclosed
capillary network and the attach tubule. The glumerulus is a unique network of capillaries
suspended between the afferent and efferent blood vessels, which are enclosed in an epithelial
structure called Bowman’s capsule. The glumerular membrane is composed of three filtering
layers: (a) Capillary endothelium, (b) basement membrane, and (c) epithelium. This membrane
normally allows filtration of fluid and small molecules yet limits passage of larger molecules,
such as blood cells and albumin.
The tubular component of the nephrons begins in the Bowman’s capsule. The filtrate
created in the Bowman’s capsule travel first into the proximal tubule, then into loops of Henle,
distal tubule, and either the cortical or medullary collecting ducts. The structural arrangement of
the tubule allows the distal tubule to lie in close proximity to where the afferent and efferent
arteriole respectively enter and leave the glumerulus. The distal tubular cells located in this
area, known as the Macula Densa which functions with the adjacent afferent arteriole and
create what is known as juxtaglumerulus apparatus. This is the site of the renin production.
Renin is a hormone directly involved in the control of arterial blood pressure; it is essential for
proper functioning of the glumerulus.
The tubular component consists of the Bowman’s capsule, the proximal tubule, the
descending and ascending limbs of the loop of Henle, and the cortical and medullary collecting
ducts. This portion of the nephrons is responsible in making adjustments in the filtrate based on
the body’s needs. Changes are continually made as the filtrate travels through the tubules until
it enters the collecting system and is expended from the body.
BLOOD SUPPLY TO THE KIDNEY
The hilum of pelvis is the concave portion of the kidney through which are renal artery
enters and ureters and renal vein exit. The kidney received 20% to 25% of the total cardiac
output, which means that all of the body’s blood circulates through the kidneys approximately
12times per hour. The renal artery (arising from the abdominal aorta) divided into smaller and
smaller vessels, eventually forming the afferent arterioles. Each afferent arterioles branches to
form a glomerulus, which is the capillary bed responsible for glumerular filtration
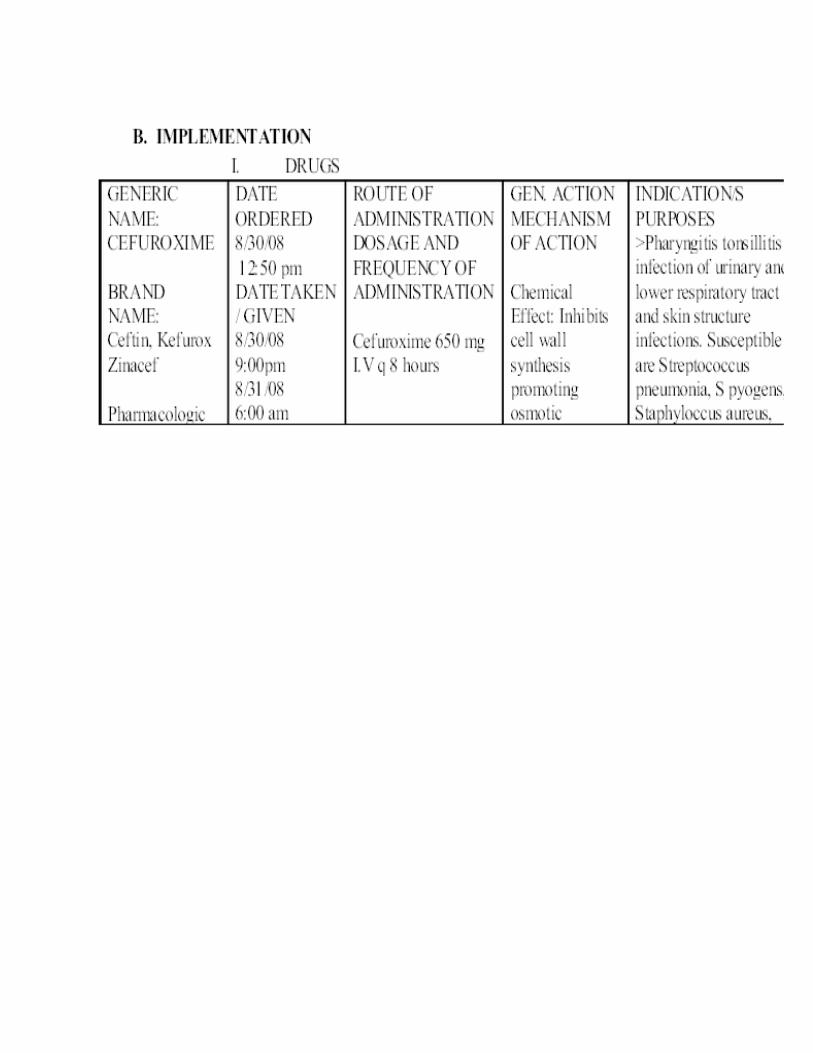
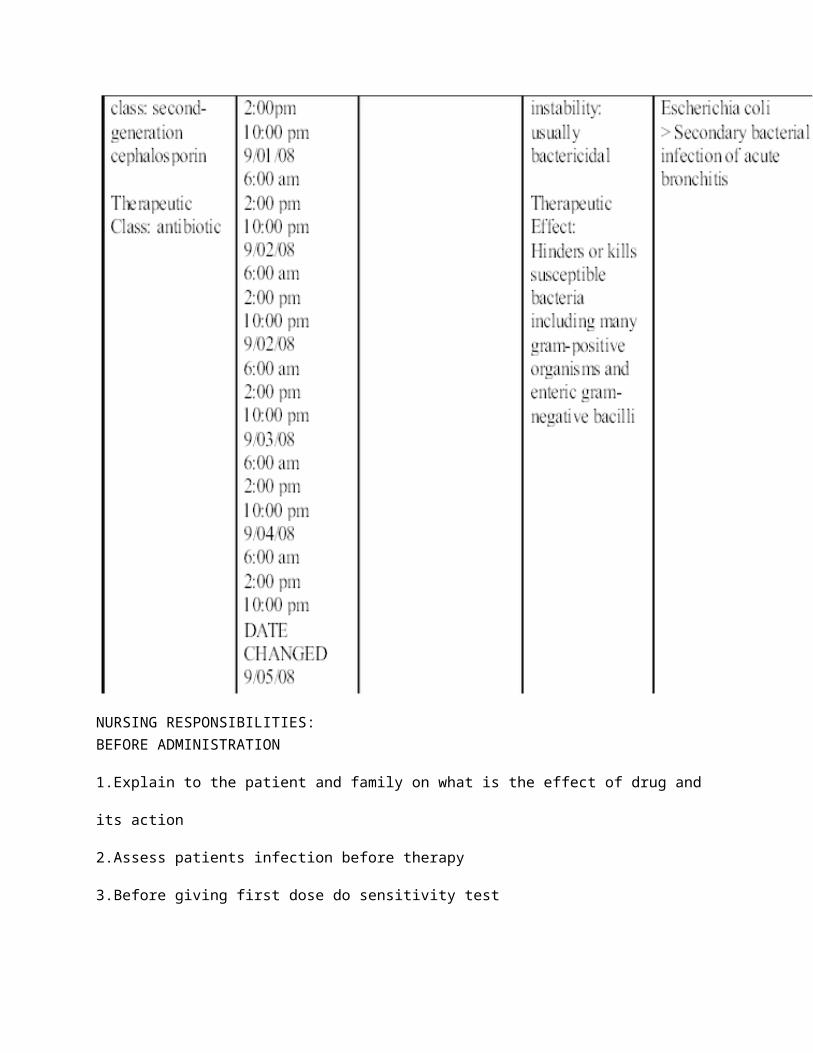
NURSING RESPONSIBILITIES:
BEFORE ADMINISTRATION
1.Explain to the patient and family on what is the effect of drug and its action
2.Assess patients infection before therapy
3.Before giving first dose do sensitivity test
4.Before giving the first dose , ask patient about previous reaction to cephalosporins or
penicillin
AFTER ADMINISTRATION
1 .Be alert for adverse reaction and drug interaction
2.If adverse GI reaction occur, monitor patients hydration
3.Tell patient/ significant others to report adverse effect seen and experience
4.Assess patients infection after the therapy
NURSING RESPONSIBILITIES
BEFORE ADMINISTRATION:
1. Explain to the patient and family on what is the effect of drug and its action
2.Assess patient temperature before the therapy
AFTER ADMINISTRATION:
1. Assess patient temperature after the therapy
2.Be alert for adverse reaction and drug interaction
3.Tell patient/ significant others to report adverse effect seen and experience
DISCHARGE SUMMARY
M: Take home medication instructed to the patient mother as follows:E: Advised the mother to let his child continue his usual daily activities as toleratedT: ØH: The following are advised to the patient’s mother:
Increase the patients fluid intake to prevent dehydration Watch her child carefully for symptoms of asthma to prevent further
complications Don’t let her child to stay outside on hot environment for long period of time.
O: Scheduled for OPD check up D: Advised the mother to give her child nutritious food like fruits and vegetables to sustain the needed nutrients of the body. Advised the mother not to let her child to eat junk foods
III CONCLUSIONIV RECOMMENDATION
Patient education is directed toward maintaining kidney function and preventing complications. Fluid and diet restrictions must be reviewed with the patient, such as avoiding dietary protein when renal insufficiency and nitrogen retention (elevated BUN) develop, and sodium when the patient has hypertension, edema and heart failure. The importance of follow-up evaluations of blood pressure, urinalysis for protein and serum BUN and creatinine levels to determine if the disease has progressed is stressed to the patient. A referral for home care may be indicated, a visit from a home care nurse provides an opportunity for careful assessment of the patient’s progress and detection of early signs and symptoms of renal insufficiency. Void every 2-3 hours during the day and completely empty the bladder. This prevents over distention of the bladder and compromised blood supply to the bladder wall. With regards to hygiene, shower rather than bathe in tub because bacteria in the bath water may enter the urethra. After each bowel movement, clean urethral meatus. Indicate that strenuous exercise should be avoided because exercise can induce proteinuria, hematuria, and cylindruria (renal cylinders or casts in the urine). Some recommend other nutritional approaches such as consuming cranberry juice, blueberry juice, and fermented milk products containing probiotic bacteria, have been shown to inhibit adherence of bacteria to the epithelial cells of the urinary tract