Case Studies in Enhanced Recovery and Improved...
12
Release date: December 31, 2015 Last review: November 11, 2015 Expiration date: December 31, 2016 Estimated time to complete activity: 1.25 hours Target Audience is activity is intended for colorectal surgeons, gen- eral surgeons, and other gastrointestinal surgeons. Learning Objectives Upon completion of this activity, learners will have improved their ability to: 1 Evaluate the efficacy and safety of current strat- egies to reduce perioperative complications in procedures involving gastrointestinal (GI) tract surgeries 2 Manage patients who are candidates for procedures involving GI/genitourinary tract surgeries with evidence-based perioperative strategies to prevent postoperative ileus 3 Articulate features of perioperative enhanced recovery after surgery protocols that might improve patient outcomes System Requirements for Digital Edition If you are viewing this activity online please ensure the computer you plan to use meets the following requirements: • Operating System: Windows or Macintosh • Media Viewing Requirements: Flash Player or Adobe Reader • Supported Browsers: Microsoft Internet Explorer, Firefox, Google Chrome, Safari, and Opera • A good Internet connection Accreditation Statement is activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continu- ing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and MedEdicus LLC. e Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians. Credit Designation e Postgraduate Institute for Medicine designates this enduring material for a maximum of 1.25 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. Disclosure of Conflicts of Interest Postgraduate Institute for Medicine (PIM) requires instructors, planners, managers, and other individu- als who are in a position to control the content of this activity to disclose any real or apparent conflict of interest (COI) they may have as related to the content of this activity. All identified COI are thoroughly vetted and resolved according to PIM policy. PIM is committed to providing its learners with high- quality CME activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of a com- mercial interest. e faculty reported the following financial relation- ships or relationships to products or devices they or their spouse/life partner have with commercial inter- ests related to the content of this CME activity: Floriano Marchetti, MD, has no real or apparent con- flicts of interest to report. Laurence R. Sands, MD, MBA, has had a financial agreement or affiliation during the past year with the following commercial interest in the form of Con- sulting Fees (e.g., advisory boards): France Foundation and Fees for Non-CME/CE Services Received Directly from a Commercial Interest or their Agents (e.g., speakers’ bureaus): Pacira Pharmaceuticals, Inc. e planners and managers reported the following financial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity: e following PIM planners and managers, Trace Hutchison, PharmD, Samantha Mattiucci, PharmD, CHCP, Judi Smelker-Mitchek, RN, BSN, and Jan Schultz, RN, MSN, CHCP, hereby state that they or their spouse/life partner do not have any financial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months. Peer Reviewer: Robert MacLaren, PharmD, has no real or apparent conflicts of interest to report. e following medical writer, Robert M. Geist IV, MD, and MedEdicus planners and managers, Diane McArdle, PhD, and Cynthia Tornallyay, RD, MBA, CCMEP, have no real or apparent conflicts of inter- est to report. Method of Participation and Request for Credit ere are no fees for participating in and receiv- ing CME credit for this activity. During the period December 31, 2015, through December 31, 2016, par- ticipants must read the learning objectives and faculty disclosures and study the educational activity. To receive CME credit, participants should read the preamble and the monograph, and complete the post- test and activity evaluation online at http://cmezone. com/activities/sr1543/2406/. Upon successfully com- pleting the post-test with a score of 75% or better and the activity evaluation, a certificate will be made avail- able immediately. Or you can mail or fax the completed post-test and evaluation to Postgraduate Institute for Medicine, 304 Inverness Way South, Suite 100, Engle- wood, CO 80112; Fax: (303) 858-8848. Media Print and Internet Disclosure of Unlabeled Use is educational activity might contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. e planners of this activity do not recommend the use of any agent out- side of the labeled indications. e opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discus- sion of approved indications, contraindications, and warnings. Disclaimer Participants have an implied responsibility to use the newly acquired information to enhance patient out- comes and their own professional development. e information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagno- sis or treatment discussed or suggested in this activ- ity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindi- cations and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities. Case Studies in Enhanced Recovery and Improved Patient Outcomes: Preventing Postoperative Ileus in Colorectal Surgeries Faculty Laurence R. Sands, MD, MBA Professor and Chief, Division of Colon and Rectal Surgery Miller School of Medicine University of Miami Miami, Florida Floriano Marchetti, MD Associate Professor of Clinical Surgery, Division of Colon and Rectal Surgery Director, Colon and Rectal Surgery Residency Program DeWitt Daughtry Family Department of Surgery Miller School of Medicine University of Miami Miami, Florida The content of this activity was developed by the faculty indicated herein under the supervision of Postgraduate Institute for Medicine and assistance from MedEdicus LLC. Applied Clinical Education (ACE) is responsible for graphic design and distribution of the activity via General Surgery News and CMEZone.com. All information included in this activity is believed to be true and accurate at the date of publication. ACE makes no warranty, expressed or implied, with respect to the material contained herein. This activity is jointly provided by Postgraduate Institute for Medicine (www.pimed.com) and MedEdicus LLC. This activity is supported by an independent educational grant from Merck & Co., Inc. Distributed via General Surgery News and CMEZone.com This CME activity is copyrighted to MedEdicus LLC © 2015. All rights reserved
Transcript of Case Studies in Enhanced Recovery and Improved...

Release date: December 31, 2015 Last review: November 11, 2015Expiration date: December 31, 2016 Estimated time to complete activity: 1.25 hours
Target AudienceTh is activity is intended for colorectal surgeons, gen-eral surgeons, and other gastrointestinal surgeons.
Learning ObjectivesUpon completion of this activity, learners will have improved their ability to:1 Evaluate the effi cacy and safety of current strat-
egies to reduce perioperative complications in procedures involving gastrointestinal (GI) tract surgeries
2 Manage patients who are candidates for procedures involving GI/genitourinary tract surgeries withevidence-based perioperative strategies to prevent postoperative ileus
3 Articulate features of perioperative enhanced recovery after surgery protocols that might improve patient outcomes
System Requirements for Digital EditionIf you are viewing this activity online please ensure the computer you plan to use meets the following requirements:• Operating System: Windows or Macintosh• Media Viewing Requirements: Flash Player or
Adobe Reader• Supported Browsers: Microsoft Internet
Explorer, Firefox, Google Chrome, Safari, and Opera
• A good Internet connection
Accreditation StatementTh is activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continu-ing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and MedEdicus LLC. Th e Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians.
Credit DesignationTh e Postgraduate Institute for Medicine designates this enduring material for a maximum of 1.25 AMA PRA Category 1 Credits™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Disclosure of Confl icts of InterestPostgraduate Institute for Medicine (PIM) requires instructors, planners, managers, and other individu-als who are in a position to control the content of this
activity to disclose any real or apparent confl ict of interest (COI) they may have as related to the content of this activity. All identifi ed COI are thoroughly vetted and resolved according to PIM policy. PIM is committed to providing its learners with high-quality CME activities and related materials that promote improvements or quality in healthcare and not a specifi c proprietary business interest of a com-mercial interest.Th e faculty reported the following fi nancial relation-ships or relationships to products or devices they or their spouse/life partner have with commercial inter-ests related to the content of this CME activity:Floriano Marchetti, MD, has no real or apparent con-fl icts of interest to report.Laurence R. Sands, MD, MBA, has had a fi nancial agreement or affi liation during the past year with the following commercial interest in the form of Con-sulting Fees (e.g., advisory boards): France Foundation and Fees for Non-CME/CE Services Received Directly from a Commercial Interest or their Agents (e.g., speakers’ bureaus): Pacira Pharmaceuticals, Inc.Th e planners and managers reported the following fi nancial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity:Th e following PIM planners and managers, Trace Hutchison, PharmD, Samantha Mattiucci, PharmD, CHCP, Judi Smelker-Mitchek, RN, BSN, and Jan Schultz, RN, MSN, CHCP, hereby state that they or their spouse/life partner do not have any fi nancial relationships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.Peer Reviewer: Robert MacLaren, PharmD, has no real or apparent confl icts of interest to report.Th e following medical writer, Robert M. Geist IV, MD, and MedEdicus planners and managers, Diane McArdle, PhD, and Cynthia Tornallyay, RD, MBA, CCMEP, have no real or apparent confl icts of inter-est to report.
Method of Participation and Request for CreditTh ere are no fees for participating in and receiv-ing CME credit for this activity. During the period December 31, 2015, through December 31, 2016, par-ticipants must read the learning objectives and faculty disclosures and study the educational activity.To receive CME credit, participants should read the
preamble and the monograph, and complete the post-test and activity evaluation online at http://cmezone.com/activities/sr1543/2406/. Upon successfully com-pleting the post-test with a score of 75% or better and the activity evaluation, a certifi cate will be made avail-able immediately. Or you can mail or fax the completed post-test and evaluation to Postgraduate Institute for Medicine, 304 Inverness Way South, Suite 100, Engle-wood, CO 80112; Fax: (303) 858-8848.
MediaPrint and Internet
Disclosure of Unlabeled UseTh is educational activity might contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. Th e planners of this activity do not recommend the use of any agent out-side of the labeled indications.Th e opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the offi cial prescribing information for each product for discus-sion of approved indications, contraindications, and warnings.
DisclaimerParticipants have an implied responsibility to use the newly acquired information to enhance patient out-comes and their own professional development. Th e information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagno-sis or treatment discussed or suggested in this activ-ity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindi-cations and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
Case Studies in Enhanced Recovery and Improved Patient Outcomes: Preventing Postoperative Ileus in Colorectal Surgeries
Faculty
Laurence R. Sands, MD, MBAProfessor and Chief, Division of Colon and Rectal SurgeryMiller School of MedicineUniversity of MiamiMiami, Florida
Floriano Marchetti, MDAssociate Professor of Clinical Surgery, Division of Colon and Rectal SurgeryDirector, Colon and Rectal Surgery Residency ProgramDeWitt Daughtry Family Department of SurgeryMiller School of MedicineUniversity of MiamiMiami, Florida
The content of this activity was developed by the faculty indicated herein under the supervision of Postgraduate Institute for Medicine and assistance from MedEdicus LLC. Applied Clinical Education (ACE) is responsible for graphic design and distribution of the activity via General Surgery News and CMEZone.com.
All information included in this activity is believed to be true and accurate at the date of publication. ACE makes no warranty, expressed or implied, with respect to the material contained herein.
This activity is jointly provided by Postgraduate Institute for Medicine (www.pimed.com) and MedEdicus LLC.
This activity is supported by an independent educational grant from Merck & Co., Inc.
Distributed via General Surgery News and CMEZone.com
This CME activity is copyrighted to MedEdicus LLC © 2015. All rights reserved

Visit http://cmezone.com/activities/sr1543/2406/ for online testing and instant CME certificate
2
IntroductionColorectal procedures account for only 12.7% of general surgical
cases, but they represent nearly 25% of all operative complications.1,2 To help minimize patient morbidity, Kehlet et al devised a compre-hensive approach to improve postoperative organ function, accel-erate rehabilitation, and reduce costs.3 Although the use of these “fast-track” protocols for patients undergoing both laparoscopic and colorectal surgery has been shown to improve several key out-comes,4 many centers around the country that perform these pro-cedures have been slow to adopt them. A survey of 407 general and colorectal surgeons found that only 30% practiced in hospitals with a specific care pathway designed to accelerate gastrointestinal (GI) recovery.5 Other studies examining the outcomes of laparoscopic colorectal procedures on an enhanced recovery pathway program found that compliance with the pathway resulted in reduced use of opioids, shorter hospitalization, and fewer complications.6 Patient education regarding the nature of the procedure and the postopera-tive pathway being used are essential to improving outcomes.
Complications of Colorectal Surgery
Dr Sands: Colorectal surgeons face many unique challenges when performing a primary colon resection with anastomosis. The most devastating complication associated with this procedure is the possibility of anastomotic leakage. The incidence of this complica-tion is approximately 3.8% based on a recent retrospective analysis of cases performed at hospitals affiliated with the American College of Surgeons National Surgical Quality Improvement Program.7 In addition, colorectal surgeons must address the possibility of wound infection, which is one of the more common complications, occur-ring in approximately 6% to 26% of patients who undergo colorec-tal procedures.8 The risk for deep venous thrombosis (DVT) is also higher in colorectal cases than in other general surgeries. Postop-erative ileus is yet another problem that is commonly encountered, although the return of GI function seems to occur more rapidly with laparoscopic procedures, most likely due to the less-invasive techniques used and less bowel manipulation. All of these chal-lenges can contribute to increased utilization of nursing resources, increased hospital length of stay (LOS), and higher costs.
Dr Marchetti: The time for bowel recovery can depend on the anatomic localization of the procedure. It may take 24 hours for GI
function to return after surgeries that involve only the small bowel, whereas it may take 120 hours after procedures that involve the colon.9 Anything that contributes to a longer hospitalization can increase the patient’s morbidity and his or her financial costs. Other factors that can contribute to the development of ileus (Table 1)10 are the duration of the procedure, open surgical technique, and sur-gery involving the lower GI tract.
Enhanced Recovery After Surgery Protocols
The Enhanced Recovery After Surgery (ERAS) protocol was developed to expedite recovery of patients, minimize surgical com-plications, and decrease utilization of hospital resources, thereby lowering health care costs for patients. Following a standardized pathway may improve outcomes, such as the levels of postoperative pain, rate of GI recovery, and hospital LOS, all of which may lead to greater patient safety. The 3 main components of the ERAS pro-gram are preoperative patient care and counseling, intraoperative management, and postoperative care (Figure 1).11
PreoperativeSeveral preoperative elements of ERAS protocols can enhance
postoperative outcomes. Preoperative counseling of patients, including defining the operative procedure and postoperative course as well as setting proper expectations, is a key element of overall good patient care and a vital component of an effective ERAS protocol.
In addition, the use of preoperative prophylactic antibiotics is well established. The practice of antibiotic prophylaxis before colorectal surgery was assessed in a recent Cochrane review. The assessment sup-ported the use of oral or intravenous (IV) antibiotics or a combination of both before elective colorectal surgery, with the potential to reduce postoperative wound infections by up to 75%.12 It is not known whether oral antibiotics would carry this degree of benefit when the colon has not been emptied via mechanical bowel preparation.12
With respect to the merits of preoperative oral mechanical bowel preparation (OMBP) for colorectal surgery, there is still some degree of controversy. OMBP is widely practiced in the United States, with recent assessments showing more than 80% utilization among surgeons.13-15 Some studies have shown that OMBP prior to colorectal surgery does not provide statistically significant benefits,12 leading the Canadian
Table 1. Clinical Outcomes With Laparoscopic and Open Colectomy10
Laparoscopic Colectomy, % Open Colectomy, % All, %
Any complication 26.0 31.8 29.8
Ileus 15.4 17.6 16.9
Pulmonary 6.5 9.0 8.2
Intraoperative 3.8 4.4 4.2
Infections 2.9 3.7 3.4
Cardiovascular 1.9 2.7 2.4
Wound 1.4 2.1 1.9
Systemic 1.1 1.5 1.4
Urinary 1.0 1.3 1.2

Why wait? Access this program and post-test @ CMEZone.com
3
Society of Colon and Rectal Surgeons to endorse the omission of bowel preparation for elective open left- or right-sided resections.16
A recent meta-analysis of evidence pertaining to the relative safety and efficacy of OMBP utilization could not exclude modest beneficial or harmful effects.17 In other words, the evidence regard-ing the use of OMBP was fairly equivocal. However, bowel prepa-ration remains a part of most ERAS protocols.13 One recent study did find that the combination of oral antibiotics with mechanical bowel preparation reduced surgical site infection, ileus, and anasto-motic leakage.18 However, no studies have specifically examined the efficacy of bowel preparation as part of an ERAS pathway.
With respect to DVT prophylaxis, most surgeons use compres-sion boots intraoperatively and postoperatively, heparin preoper-atively, and enoxaparin postoperatively. The incidence of DVT in patients who undergo colorectal procedures without prophylaxis is approximately 30%, which is much higher than that seen with other general surgical procedures.19
Lastly, the use of preoperative carbohydrate loading has been associated with a significantly shorter hospital LOS and a trend toward a more rapid return of bowel function relative to fasting or preoperative oral water (1.5 days to first flatus vs 3 days in fasting/water groups; P = .13).20,21
IntraoperativeThe nature of the procedures being performed can influence
postoperative outcomes. Laparoscopic procedures are associated with less pain, reduced narcotic use, quicker return of bowel func-tion, and decreased hospital LOS. Recent estimates of the use of the laparoscopic technique for colon resection now show rates exceed-ing 40%, increasing from 37.5% in 2008 to 44.1% in 2011.22 Sur-gical incisions clearly are smaller in laparoscopic procedures, many of which accomplish specimen extraction via a stoma site, obviat-ing the need for surgical incision other than port sites. Patient sat-isfaction is greater with the improved cosmesis from laparoscopic
surgery as well. Regardless of whether the surgery is done open or laparoscopically, ERAS pathways can, and should, be employed.
Intraoperative fluid management is another key component of optimizing patient outcomes. The amount of fluid administered to patients in the operating room (OR) should be limited in view of the fluid shifts that may occur after abdominal surgery. More recent data have shown an association between a fluid-restrictive regimen and improved outcomes in colorectal surgery. Excess fluids given intraoperatively have been associated with a higher risk for anasto-motic leakage and greater incidence of postoperative wound infec-tions as well as increased cardiopulmonary morbidity. Bleier et al found that using a restrictive fluid approach can reduce LOS.23 Abraham-Nordling et al found that patients in a restricted IV fluid cohort had fewer major and minor complications (P = .027).24 The proper balance of fluids administered intraoperatively poses a real challenge that requires collaboration and effective commu-nication between the surgeon and the anesthesiologist. The use of transesophageal Doppler to monitor stroke volume can guide fluid administration,25 but it might not be practical at many institutions.26
PostoperativeDietary advancement is a key aspect of ERAS protocols. It starts
with removal of the nasogastric (NG) tube at the conclusion of the operative procedure and continues with the initiation of a liquid diet once patients are fully awake from anesthesia. The diet can be advanced by postoperative day (POD) 2. Studies have shown that this may accelerate the return of GI function after elective colorec-tal resections, even in patients undergoing open procedures.27,28 Routine placement of NG tubes has not been shown to improve GI recovery time; furthermore, the tube may cause greater patient anxiety and discomfort and may increase the likelihood of respira-tory problems.29 The avoidance of NG tube placement has been a strong predictor of a shorter hospital LOS in patients undergoing operative treatment for colorectal cancer (CRC).30
Figure 1. ERAS Components11
Preoperative
• Preadmission counseling• Carbohydrate loading• Fluid loading• Antibiotic prophylaxis• Thromboprophylaxis• Avoid prolonged fasting• Avoid or limit bowel preparation• Avoid premedication
Intraoperative
• Use short-acting anesthetics• Use midthoracic epidural anesthesia and analgesia• Maintain normothermia• Avoid surgical drains• Avoid salt and water overload
Postoperative
• Use midthoracic epidural anesthesia and analgesia• Prophylaxis for nausea and vomiting• Early catheter removal• Early oral nutrition• Nonopioid oral analgesia/ nonsteroidal anti-
inflammatory drugs • Early mobilization• Stimulation of gut motility• Audit compliance and outcomes• Avoid nasogastric tubes• Avoid salt and water overload

Visit http://cmezone.com/activities/sr1543/2406/ for online testing and instant CME certificate
4
Because postoperative ileus has significant adverse effects on multiple patient outcomes, including postoperative pain, increased nausea and vomiting, prolonged time to regular diet, prolonged time to mobilization, increased health care costs, and prolonged hospitalization,31 there is clearly a need to use other methods to combat this problem. Additional interventions such as the use of gum chewing and the perioperative use of alvimopan in appropri-ate clinical situations have been studied individually, and both have been shown to help reduce postoperative ileus.9
Perioperative Pain ManagementPain management is a critical component to address in maxi-
mizing surgical outcomes, both intraoperatively and postopera-tively. The influence of opioids on bowel function has been studied at length, and higher doses of opioid analgesics have been asso-ciated with a greater incidence of postoperative ileus.32 Although opioids remain a part of patient analgesia, systemic and regional alternatives can help to provide satisfactory pain control while min-imizing GI impairment.
Nonsteroidal anti-inflammatory drugs (NSAIDs), including ibuprofen and ketorolac, have been used; however, these medica-tions have been associated with a risk for anastomotic leaks after colorectal surgery.33 As a result, perioperative pain management with NSAIDs should be evaluated meticulously on a case-by-case basis.34 Intravenous acetaminophen also has been studied as part of an ERAS protocol following laparoscopic colectomy. In a case-matched study, the addition of a transverse abdominis plane block and IV acetaminophen to an existing ERAS protocol significantly reduced hospital LOS from 3.7 to 2.6 days (P < .01).35
Although the use of epidural analgesia in laparoscopic colorec-tal surgery has been shown to be more efficacious than conven-tional analgesia, the benefit with respect to other outcomes and cost-effectiveness is not as certain.36,37 One retrospective analy-sis found that the use of epidural analgesia was linked with a lon-ger hospital LOS of .60 days (P = .003), greater financial costs of $3,732.71 (P = .02), and a higher rate of urinary tract infections (P = .05).36
Surgeons also have used local wound infiltrations with bupiva-caine. A recent analysis of 6 prospective, phase 4, sequential, cohort studies found that liposomal bupivacaine-based multimodal anal-gesia (incorporating NSAID and acetaminophen administration) reduced postsurgical opioid use and opioid-related problems, such as impaired GI motility, and may lead to better outcomes, including reduced hospital LOS, compared with conventional opioid-based regimens in patients undergoing laparoscopic colectomy.38 Simi-lar findings have been demonstrated in studies looking at patients undergoing open colectomy.39
ERAS Protocol Example: Dr Sands and Dr Marchetti
Preoperative: We should risk stratify our patients and be cer-tain that they are properly counseled prior to surgery to ensure that they understand what will happen and what is expected of them after surgery. We also need to ensure that the lesions that we intend to remove are appropriately marked with a tattoo in advance of the surgical procedure to help reduce intraoperative
time. Reviewing the surgical plan with nursing and OR staff before the procedure is essential. The patients are given a mechan-ical bowel preparation. Antibiotics and DVT prophylaxis should be administered before the procedure, with placement of an epi-dural for pain control if one is to be used. Alvimopan should be given to the patients in the holding area preoperatively if they meet proper criteria.
Intraoperative: We try to perform many of our cases lapa-roscopically. Careful fluid management and blood sugar control can help optimize outcomes. NG tubes should be removed in the OR at the end of the case, and we do not use routine drain tube placement.
Postoperative: On POD 0, patients start a liquid diet. Typically, this is continued on POD 1, and if the patient is tolerating the liq-uid diet well, then the IV is locked with heparin. Urinary output is monitored closely, and we remove the Foley catheter, if possible, on POD 1. The patient is encouraged to chew gum on POD 1. Anti-biotics are stopped after 24 hours; we usually just give 1 dose pre-operatively, but antibiotics are allowed up to 24 hours by Surgical Care Improvement Project (SCIP) guidelines. For pain manage-ment, patients receive IV acetaminophen, ibuprofen, or ketorolac. Narcotics are ordered for breakthrough pain and given as needed. The patient is moved to a chair on POD 1 as well and is encour-aged to ambulate, if possible.
On POD 2, the patient’s diet is advanced, and we make the transition to oral pain medications. The patient should be ambu-lating by POD 2.
On POD 3, the epidural catheter is removed if placed intraoper-atively. Usually patients are sent home with adequate pain control if they are tolerating a diet and voiding. These are the key elements of our typical ERAS protocol.
Some patients are not ideal candidates for an ERAS pathway; however, we try to implement as many elements as possible. If a patient is unable to adhere to the protocol, we modify it to meet his or her needs. Patients who come into the emergency room with an acute abdomen or perforated viscus or showing signs of systemic sepsis with multiple comorbidities typically are not candidates for an ERAS protocol. However, it may be possible to implement some aspects of the protocol to assist with the patient’s overall recov-ery. The ideal patient for an ERAS protocol would be one who is motivated, has a low American Society of Anesthesiologists (ASA) Physical Status (PS) classification, and is undergoing elective sur-gery. Patients who require emergent surgery, have a high ASA PS classification, or who are severely malnourished are not going to conform to conventional methodologies and would be poor candi-dates for fast tracking.
There has been concern regarding the implementation of ERAS colorectal protocols due to the possibility of early readmission after discharge. However, several studies have shown that the readmis-sion rate is not higher among patients who were on fast-track protocols.40-42
The SCIP measures should be followed, with careful attention to the role of DVT prophylaxis as well as prevention of infections and adverse cardiac events.43 There is great incentive to adhere to these performance measures, given the supportive alignment between the Joint Commission and the Centers for Medicare & Medicaid Services.43

Why wait? Access this program and post-test @ CMEZone.com
5
CASE 1
A 48-year-old white male presents for assessment of rectal bleeding for the past 4 months and a change in bowel habits. He has a 6-month history of altered stool caliber, which is associated with cramping abdominal pain, rectal bleeding, a 4.54-kg weight loss over the past 3 months, and decreased appetite. His med-ical history is remarkable for hypertension, which is treated with a β-blocker, and mild benign prostatic hypertrophy, with no prior abdominal surgery. He has a family history of CRC. In particular, his father had CRC at age 65 and underwent a segmental colec-tomy with postoperative chemotherapy. His father has been dis-ease free for more than 5 years after completing chemotherapy. The patient works as a banker, is an occasional social drinker, and denies any other history of smoking or illicit drug use.
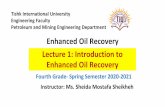
After examination, the patient is advised to undergo a colonos-copy and a computed tomography (CT) scan to explore the eti-ology of his change in bowel habits, rectal bleeding, weight loss, and abdominal pain. His CT scan shows masses in each side of the colon. His carcinoembryonic antigen (CEA) level is 0.5 ng/mL (normal), and his exercise stress test is negative. His colonoscopy reveals several sessile and pedunculated polyps as well as 2 distinct colonic masses: 1 in the ascending colon and 1 in the sigmoid colon (Figure 2).
There are no rectal polyps. His biopsies show tubular adeno-matous polyps and 2 invasive adenocarcinomas of the colon: 1 on the right side and 1 on the left side. The patient is scheduled to undergo a laparoscopic total abdominal colectomy with an ileo-rectal anastomosis.
The patient is fed a liquid diet the day before surgery and undergoes a full mechanical bowel preparation. He receives oral antibiotics, including 1 g of neomycin and 1 g of metronida-zole, both at 7 pm and again at 11 pm the night before surgery. He is administered nothing orally after midnight before sur-gery. He receives preoperative counseling regarding the ERAS protocol. On the day of surgery, he receives DVT prophylaxis with 5,000 U of subcutaneous heparin. Antibiotic prophylaxis is administered with 1 g of IV ertapenem 30 minutes before sur-gery. He is taken to the OR, where he undergoes general anes-thesia and is placed in a low-lying lithotomy position, with both arms tucked at his side. A Foley catheter and orogastric tube are placed for the time of surgery.
The patient’s procedure is performed laparoscopically and takes a total of 290 minutes. His urinary output is 150 mL, and he has 50 mL of blood loss. The orogastric tube is removed at the con-clusion of the procedure. He is taken to the recovery room and is started on a clear liquid diet once he is awake, alert, and able to eat according to anesthesia recovery room guidelines. He is provided pain control with a morphine patient-controlled analgesia pump and is moved to a regular floor.
On POD 1, the patient mobilizes out of bed to the chair in his room. His urinary output is low, and he receives an IV fluid bolus and increase in his baseline IV rate. On POD 2, he is ambulating.
On POD 3, the patient complains of severe abdominal pain and is slightly tachycardic, without fever. On physical examination, his abdo-men is tender and distended. This is felt to be consistent with a prob-able ileus, and the patient is restricted from oral consumption. He is given increased IV fluids for continued low urinary output. He has
Figure 2. Colonoscopy Findings: Polyps and Colonic Masses
Images Courtesy of Laurence R. Sands, MD, MBA

Visit http://cmezone.com/activities/sr1543/2406/ for online testing and instant CME certificate
6
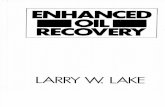
a nonroutine laboratory assessment with a complete blood count to look for signs of bleeding or infection as well as an electrolyte panel. His abdominal x-ray shows dilated loops of the small bowel consistent with a postoperative ileus (Figure 3), and an NG tube is put in place.
Upon insertion of the NG tube, 850 cc of bilious material is aspirated from the patient’s stomach, and he is maintained on low continuous suction, with a plan to maintain the NG tube until his bowel function returns. The tube remains in place for 7 days, and he is started on total parenteral nutrition (TPN).
The patient’s bowel function eventually returns, and on POD 10, the NG tube is removed. On POD 11, a clear liquid diet is resumed. On POD 12, he starts a low-fat, low-residue diet, which is toler-ated. On POD 13, he is discharged home. His pathology report reveals stage 3 disease (T3N1), with 2 adenocarcinomas and tubu-lar adenomas, and he is referred to medical oncology for postoper-ative chemotherapy.
Case DiscussionDr Marchetti: Dr Sands, what factors may have contributed to
the prolonged LOS in this patient’s case?Dr Sands: Laparoscopic total abdominal colectomies lasting
longer than 270 minutes may be associated with more postopera-tive complications, longer time before resumption of a normal diet, and longer hospitalizations relative to shorter surgeries.44 Postop-erative ileus has significant adverse effects on multiple outcomes, including increased health care costs and prolonged hospitalization.
Dr Marchetti: What strategies might have made a difference in LOS for this patient?
Dr Sands: He did not have opioid-sparing analgesia. Although opioids are used frequently, they decrease GI motility, inhibit-ing small and large bowel propulsion. Opioids may lead to other GI effects as well. Optimal practice would involve minimization of the use of opioids after surgery, looking at other options such as nonsteroidal medications, epidurals, IV lidocaine, liposomal-based bupivacaine for local injection, or gabapentin. Many of the investigations of opioid-sparing strategies have been conducted in patients after open colorectal surgeries, and the benefit for laparo-scopic colorectal procedures is not quite as clear. Intravenous ketor-olac has been used to reduce patient discomfort in cases of open and laparoscopic surgery.45
Dr Marchetti: What is the effect of postoperative ileus in terms of cost and resource utilization?
Dr Sands: Postoperative ileus is a real entity with real com-plications, including increased morbidity and prolonged hospital LOS. It would be ideal to minimize narcotic use for pain control as much as possible. Sometimes it is not possible to avoid narcotic use completely, and alvimopan may be helpful in preventing post-operative ileus by allowing narcotic use without affecting bowel motility. Alvimopan is a peripherally acting μ-opioid receptor antag-onist (PAMORA) agent that allows patients to experience the nar-cotic effect while not affecting the return of GI function.46 Studies have evaluated methylnaltrexone, another PAMORA agent, for
Figure 3. Flat Plate of Abdomen: POD 3
Image Courtesy of Laurence R. Sands, MD, MBA

Why wait? Access this program and post-test @ CMEZone.com
7
the treatment of postoperative ileus; however, these studies failed to demonstrate efficacy for postoperative ileus.47,48 Alvimopan has been studied extensively, showing a reduction in hospital LOS by about 1.1 days.49 It has been a component of several ERAS protocols, and
we try to use it when appropriate within a comprehensive pathway that can improve outcomes. For patients undergoing total abdomi-nal colectomy or longer procedures, strong consideration should be given to measures that can reduce postoperative ileus.
CASE 2
A 58-year-old woman presents for assessment of rectal bleeding. Her medical history is remarkable for hypertension, and she
has a surgical history of a total abdominal hysterectomy–bilateral salpingo-oophorectomy 20 years ago, 2 cesarean deliveries, and an appendectomy as a child. Her family history is negative for CRC. She undergoes a colonoscopy, which reveals midsigmoid colon can-cer. The lesion is marked with India ink, and a biopsy reveals adeno-carcinoma. A CT scan of the chest, abdomen, and pelvis is negative for metastatic disease. Her CEA level is 3.1 ng/mL, and her other laboratory results are normal.
The operative plan is for the patient to undergo a laparoscopic sigmoid colectomy. She receives a mechanical bowel preparation before the procedure as well as preoperative IV antibiotics, DVT prophylaxis, and alvimopan.
The patient has an open Hasson port placed above her umbili-cus. She is noted to have numerous dense adhesions, and additional ports are placed cautiously. She undergoes laparoscopic adhesioly-sis. Several serosal tears are noted, and 2 segments of the bowel are injured, with exposed mucosa and enteric spillage.
The surgery is converted to an open procedure. Extensive enteroly-sis is performed, with 2 small bowel resections in addition to the colec-tomy. An NG tube is placed, and the total operative time is 4.5 hours.
Fast-track protocols used at the hospital are unable to be ini-tiated and maintained. Postoperatively, the patient is taken to the intensive care unit, where she remains for 3 days. Intrave-nous antibiotics are continued due to the intraoperative spillage of her enteric contents. TPN is initiated on POD 3. She experi-ences a prolonged postoperative ileus. The NG tube remains in
place for 10 days until she experiences passage of flatus and stool on POD 12. Intravenous fluids are maintained. A clear liquid diet is started on POD 13. Her diet is advanced over the next few days, and she is discharged home on POD 16.
Case DiscussionDr Sands: Dr Marchetti, what are the key problems in this case?Dr Marchetti: The procedure should have been converted to an
open surgery sooner, before the bowel injury. Although laparoscopy is associated with reduced LOS, quicker bowel recovery, less post-operative pain, fewer problems with wound infection, and improved cosmesis,10,50 proceeding with laparoscopic enterolysis with multi-ple bowel injuries delayed postoperative recovery and increased this patient’s operative morbidity. ERAS protocols can be done with both open and laparoscopic procedures. However, in this case, fast-track protocols could not be followed due to the surgical complications.
Dr Sands: What are your thoughts on the role of IV fluid administration in this patient’s case?
Dr Marchetti: You certainly want to obtain a balance of fluid in a situation in which excess IV fluid can contribute to several com-plications. You can see increases in interstitial volume and total body water. Ambulation can be more difficult, and patients may experience greater cardiopulmonary morbidity. Studies have com-pared standard and restrictive fluid administration protocols, and a meta-analysis has suggested some benefit to the practice of fluid restriction, with less morbidity after colorectal resection.51 How-ever, fluid management remains very challenging and requires coor-dination between the surgeon and the anesthesiologist.
CASE 3
A 60-year-old white male presents for assessment of rectal bleed-ing. His medical history is remarkable for hypertension, with
no surgical history. His family history is negative for CRC. A colo-noscopy reveals right colon cancer, and the lesion is marked with India ink. A biopsy of the area indicates adenocarcinoma, and the patient’s CEA level is 3.3 μg/dL. His other laboratory values are normal. A CT scan of the chest, abdomen, and pelvis is negative for metastatic disease.
The operative plan is for the patient to undergo a robotic-assisted right colectomy with intracorporeal anastomosis. He receives preoperative counseling. Before his procedure, he receives a mechanical bowel preparation, DVT prophylaxis, alvimopan, and IV antibiotics. Robotic ports are placed along the patient’s mid-line, and he undergoes a robotic right colectomy with intracorpo-real anastomosis, which is stapled in a side-to-side fashion with the common enterotomy handsewn with the robot. The duration of the procedure is 75 minutes, and he receives a bupivacaine liposome–injectable suspension for local anesthetic treatment of his wounds.
The patient is started on a clear liquid diet in the recovery room.
He receives IV acetaminophen and ketorolac for pain control, with IV hydromorphone for postoperative breakthrough pain. The Foley catheter is removed on POD 1. He continues alvimopan postop-eratively and also starts chewing gum. A regular diet is offered to the patient on POD 2. He passes flatus and moves his bowels on POD 2 and is discharged home on POD 3.
Case DiscussionDr Sands: Dr Marchetti, can you explain the rationale for hav-
ing the patient chew gum as part of his postoperative protocol?Dr Marchetti: Gum chewing can be an effective means of pre-
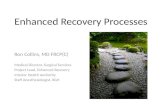
venting postoperative ileus. It has been examined in several stud-ies, and beneficial effects, such as decreased time to first passage of flatus, decreased time to first stool, and decreased hospital LOS, have been seen (Figure 4).52 Other components of ERAS protocols also address bowel recovery so it may be difficult to distinguish how much benefit comes from chewing gum in this context.
Dr Sands: What are your thoughts about the patient’s postop-erative dietary pathway?

Visit http://cmezone.com/activities/sr1543/2406/ for online testing and instant CME certificate
8
Figure 4. Randomized Controlled Studies Examining the Association Between Outcomes and Gum Chewing52
Pooled estimates: reduction in time to passage of flatus by 14 hours (95% confidence interval [CI], 20 to 8 hours; P = .001).
Reduction in time to bowel movement by 23 hours (95% CI: -32 to -15 hours; P < .001).
Reduction in hospitalization time: 1.1 days (95% CI: -1.9 to -0.2 days; P = .016).
Reprinted with permission.
-5
-80
-50
-2.5
-40
-25
0
0
0
2.5
40
25
5
80
50
Time to flatus
Asao 2002
Hirayama 2006
Kouba 2007
Matros 2006
McCormick 2006
Quah 2006
Schuster 2006
Watson 2008
Zhang 2008
I-V Subtotal (I-squared = 57.5%, P = .016)
D+L Subtotal
Time to passing stool
Asao 2002
Hirayama 2006
Kouba 2007
Matros 2006
McCormick 2006
Quah 2006
Schuster 2006
I-V Subtotal (I-squared = 51.1%, P = .056)
D+L Subtotal
Length of postoperative hospital stay
Asao 2002
Kouba 2007
Matros 2006
McCormick 2006
Quah 2006
Schuster 2006
Watson 2008
I-V Subtotal (I-squared = 78.0%, P = .000)
D+L Subtotal
Trial
10
10
51
22
62
19
17
27
9
10
10
51
22
62
19
17
10
51
22
62
19
17
27
Withgum
9
14
51
21
40
19
17
26
9
9
14
51
21
40
19
17
9
51
21
40
19
17
26
Withoutgum
-26.40 (-42.35, -10.45)
-34.70 (-47.99, -21.41)
-12.00 (-17.59, -6.41)
-6.00 (-21.20, 9.20)
-4.80 (-16.80, 7.20)
-7.20 (-22.46, 8.06)
-14.80 (-26.29, -3.31)
-20.00 (-44.78, 4.78)
-7.78 (-14.49, -1.07)
-12.33 (-15.69, -8.97)
-13.75 (-19.62, -7.87)
-64.80 (-102.98, -26.62)
-51.50 (-89.37, -13.63)
-16.80 (-23.39, -10.21)
-7.00 (-26.86, 12.86)
-14.40 (-26.09, -2.71)
-16.80 (-39.69, 6.09)
-26.20 (-37.89, -14.51)
-18.72 (-23.51, -13.92)
-20.72 (-29.29, -12.14)
-1.00 (-5.40, 3.40)
-0.40 (-0.81, 0.01)
-0.58 (-2.02, 0.86)
-0.80 (-1.52, -0.08)
-1.70 (-5.17, 1.77)
-2.50 (-3.19, -1.81)
-0.71 (-1.56, 0.14)
-0.89 (-1.18, -0.60)
-1.05 (-1.83, -0.27)
WMD (95% CI)
4.43
6.39
36.12
4.88
7.83
4.84
8.55
1.84
25.10
100.00
1.58
1.60
52.98
5.83
16.82
4.39
16.81
100.00
0.43
49.96
3.99
15.88
0.69
17.61
11.43
100.00
%Weight
(I-V)

Why wait? Access this program and post-test @ CMEZone.com
9
Dr Marchetti: Early postoperative feeding can aid in quicker bowel recovery. A meta-analysis of 13 clinical trials in which oral/enteral nutrition was initiated within 24 hours of intestinal sur-gery found several interesting points. Mortality was reduced with early postoperative feeding, and the data were suggestive of reduced wound infections, a lower incidence of pneumonia, and a shorter LOS with early feeding. There was no evidence of increased risk for anastomotic dehiscence, and ultimately, no benefit to restricting postoperative oral/enteral nutrition.53
Dr Sands: Finally, what are your thoughts about the inclusion of alvimopan in this patient’s pathway?
Dr Marchetti: The use of alvimopan allows for a quicker return of bowel function and decreased LOS (Figure 5).49 A retrospec-tive, matched-cohort study of patients undergoing bowel resec-tion examined the potential influence of accelerated GI recovery on a variety of postoperative outcomes. The incidence of GI com-plications was lower in the group treated with alvimopan (29.8% vs 35.7%; P < .0001).49 Cardiovascular, infectious, pulmonary, and thromboembolic complications were significantly lower in the group treated with alvimopan (Figure 5).49 The alvimopan-treated group had lower mortality (0.4% vs 1.0%; P = .0007) and a lower mean intensive care unit LOS (0.3 vs 0.6 days; P < .0001).49
Due to concerns regarding the potential risk for myocardial infarction that was seen in a long-term study (12 months), patients may receive alvimopan only for short-term use (<15 doses) in the hospital through a Risk Evaluation and Mitigation Strategy (REMS) program. In-service education is absolutely necessary for
everyone involved in the prescription, dispensation, and administra-tion of alvimopan. The responsibility for following these protocols ultimately lies with the surgeon at our institution. It is important for surgeons to have a close working relationship with pharmacists to enhance the efficiency and accuracy of the medical management of patients who have undergone surgical procedures.54
Cost is always a consideration as well. One analysis of patients undergoing laparotomy for bowel resection with primary anasto-mosis found a mean estimated hospital cost reduction of $879 to $977 for those who received alvimopan compared with those who received placebo.55 Another study showed that the mean cost sav-ings associated with alvimopan use was $531 for patients undergo-ing laparoscopic bowel resection and $997 for patients undergoing open bowel resection.56
Take-Home Points
• Early postoperative feeding and avoidance of routine NG tube placement may enhance outcomes for patients undergoing bowel resection
• Patients who undergo bowel resection are at an elevated risk for venous thromboembolism relative to other surgical patients
• Careful management of intraoperative fluids can greatly enhance patient outcomes
• Chewing gum, use of alvimopan, and avoidance or minimiza-tion of opioid analgesia can facilitate GI recovery for patients undergoing bowel resection with primary anastomosis
Figure 5. Clinical Complication Rates With and Without Alvimopan Use49
N = 3,525 patients in the alvimopan and control cohorts
* P ≤ .003† P = .0532
Gastrointestinal Morbidity*
Cardiovascular Morbidity*
Infections* 30-day Readmission† Pulmonary Morbidity* Thromboembolic* 0
1
2
3
4
5
6
7
Length of Stay*
Days

Visit http://cmezone.com/activities/sr1543/2406/ for online testing and instant CME certificate
10
References
1. Debarros M, Steele SR. Perioperative protocols in colorectal surgery. Clin Colon Rec-tal Surg. 2013;26(3):139-145.
2. Valentine RJ, Jones A, Biester TW, et al. General surgery workloads and practice pat-terns in the United States, 2007 to 2009: a 10-year update from the American Board of Surgery. Ann Surg. 2011;254(3):520-525.
3. Kehlet H. Multimodal approach to control postoperative pathophysiology and reha-bilitation. Br J Anaesth. 1997;78(5):606-617.
4. Kelley SR, Wolff BG, Lovely DK, Larson DV. Fast-track pathway for minimally invasive colorectal surgery with and without alvimopan (Entereg)TM: which is more cost-effective? Am Surg. 2013;79(6):630-633.
5. Delaney CP, Senagore AJ, Gerkin TM, et al. Association of surgical care practices with length of stay and use of clinical protocols after elective bowel resection: results of a national survey. Am J Surg. 2010;199(3):299-304.
6. Larson DW, Lovely JK, Cima RR, et al. Outcomes after implementation of a multimodal standard care pathway for laparoscopic colorectal surgery. Br J Surg. 2014;101(8):1023-1030.
7. Midura EF, Hanseman D, Davis BR, et al. Risk factors and consequences of anasto-motic leak after colectomy: a national analysis. Dis Colon Rectum. 2015;58(3):333-338.
8. Nakamura T, Mitomi H, Ihara A, et al. Risk factors for wound infection after surgery for colorectal cancer. World J Surg. 2008;32(6):1138-1141.
9. Lubawski J, Saclarides T. Postoperative ileus: strategies for reduction. Ther Clin Risk Manag. 2008;4(5):913-917.
10. Delaney CP, Chang E, Senagore AJ, et al. Clinical outcomes and resource utilization associated with laparoscopic and open colectomy using a large national database. Ann Surg. 2008;247(5):819-824.
11. ERAS protocol. ERAS Society Web site. http:/www.erassociety.org/index.php/eras-care-system/eras-protocol. Accessed November 20, 2015.
12. Nelson RL, Gladman E, Barbateskovic M. Antimicrobial prophylaxis for colorectal surgery. Cochrane Database Syst Rev. 2014;5:CD001181.
13. Agency for Healthcare Research and Quality. Oral mechanical bowel preparation for colorectal surgery. AHRQ Pub. No. 14-EHC018-1-EF. April 2014. http://effective-healthcare.ahrq.gov/ehc/products/458/1901/colorectal-surgery-preparation-execu-tive-140428.pdf. Accessed September 18, 2015.
14. Zmora O, Wexner SD, Hajjar L, et al. Trends in preparation for colorectal surgery: survey of the members of the American Society of Colon and Rectal Surgeons. Am Surg. 2003;69(2):150-154.
15. Englesbe MJ, Brooks L, Kubus J, et al. A statewide assessment of surgical site infec-tion following colectomy: the role of oral antibiotics. Ann Surg. 2010;252(3):514-519.
16. Eskicioglu C, Forbes SS, Fenech DS, et al; for the Best Practice in General Surgery Committee. Preoperative bowel preparation for patients undergoing elective colorec-tal surgery: a clinical practice guideline endorsed by the Canadian Society of Colon and Rectal Surgeons. Can J Surg. 2010;53(6):385-395.
17. Dahabreh IJ, Steele DW, Shah N, et al. Oral mechanical bowel preparation for colorectal surgery: systematic review and meta-analysis. Dis Colon Rectum. 2015;58(7):698-707.
18. Kiran RP, Murray AC, Chiuzan C, et al. Combined preoperative mechanical bowel preparation with oral antibiotics significantly reduces surgical site infection, anasto-motic leak, and ileus after colorectal surgery. Ann Surg. 2015;262(3):416-425.
19. Alizadeh K, Hyman N. Venous thromboembolism prophylaxis in colorectal surgery. Surg Technol Int. 2005;14:165-170.
20. ERAS Compliance Group. The impact of enhanced recovery protocol compliance on elective colorectal cancer resection: results from an international registry. Ann Surg. 2015;261(6):1153-1159.
21. Noblett SE, Watson DS, Huong H, et al. Pre-operative oral carbohydrate loading in colorectal surgery: a randomized controlled trial. Colorectal Dis. 2006;8:563-569.
22. Simorov A, Shaligram A, Shostrom V, et al. Laparoscopic colon resection trends in utilization and rate of conversion to open procedure: a national database review of academic medical centers. Ann Surg. 2012;256(3):462-468.
23. Bleier JIS, Aarons CB. Perioperative fluid restriction. Clin Colon Rectal Surg. 2013;26(3):197-202.
24. Abraham-Nordling M, Hjern F, Pollack J, et al. Randomized clinical trial of fluid restriction in colorectal surgery. Br J Surg. 2012;99(2):186-191.
25. Noblett SE, Snowden CP, Shenton BK, et al. Randomized clinical trial assessing the effect of Doppler-optimized fluid management on outcome after elective colorectal resection. Br J Surg. 2006;93(9):1069-1076.
26. Eng OS, Melstrom LG, Carpizo DR. The relationship of perioperative fluid admin-istration to outcomes in colorectal and pancreatic surgery: a review of the literature. J Surg Oncol. 2015;111(4):472-477.
27. Fujii T, Morita H, Sutoh T, et al. Benefit of oral feeding as early as one day after elec-tive surgery for colorectal cancer: oral feeding on first versus second postoperative day. Int Surg. 2014;99(3):211-215.
28. Sindell S, Causey MW, Bradley T, et al. Expediting return of bowel function after colorectal surgery. Am J Surg. 2012;203(5):644-648.
29. Rao W, Zhang X, Zhang J, et al. The role of nasogastric tube in decompres-sion after elective colon and rectum surgery: a meta-analysis. Int J Colorectal Dis. 2011;26(4):423-429.
30. Bakker N, Cakir H, Doodeman HJ, et al. Eight years of experience with Enhanced Recovery After Surgery in patients with colon cancer: impact of measures to improve adherence. Surgery. 2015;157(6):1130-1136.
31. Berger NG, Ridolfi TJ, Ludwig KA. Delayed gastrointestinal recovery after abdomi-nal operation – role of alvimopan. Clin Exp Gastroenterol. 2015;8:231-235.
32. Gan TJ, Robinson SB, Oderda GM, et al. Impact of postsurgical opioid use and ileus on economic outcomes in gastrointestinal surgeries. Curr Med Res Opin. 2015;31(4):677-686.
33. Subendran J, Siddiqui N, Victor JC, et al. NSAID use and anastomotic leaks fol-lowing elective colorectal surgery: a matched case-control study. J Gastrointest Surg. 2014;18(8):1391-1397.
34. Blouin M, Rhainds M. Use of nonsteroidal anti-inflammatory drugs in colorec-tal surgery: do the risks cast a shadow on the benefits? Ann Pharmacother. 2014;48(12):1662-1664.
35. Keller DS, Stulberg JJ, Lawrence JK, et al. Process control to measure process improvement in colorectal surgery: modifications to an established enhanced recovery pathway. Dis Colon Rectum. 2014;57(2):194-200.
36. Halabi WJ, Kang CY, Nguyen VQ, et al. Epidural analgesia in laparoscopic colorectal surgery: a nationwide analysis of use and outcomes. JAMA Surg. 2014;149(2):130-136.
37. Kaminski JP, Pai A, Ailabouni L, et al. Role of epidural and patient-controlled anal-gesia in site-specific laparoscopic colorectal surgery. JSLS. 2014;18(4).
38. Candiotti KA, Sands LR, Lee E, et al. Liposome bupivacaine for postsurgical anal-gesia in adult patients undergoing laparoscopic colectomy: results from prospective phase IV sequential cohort studies assessing health economic outcomes. Curr Ther Res Clin Exp. 2013;76:1-6.
39. Cohen SM. Extended pain relief trial utilizing infiltration of Exparel (®), a long-act-ing multivesicular liposome formulation of bupivacaine: a phase IV health economic trial in adult patients undergoing open colectomy. J Pain Res. 2012;5:567-572.
40. Greco M, Capretti G, Beretta L, et al. Enhanced recovery program in colorec-tal surgery: a meta-analysis of randomized controlled trials. World J Surg. 2014;38(6):1531-1541.
41. Paton F, Chambers D, Wilson P, et al. Effectiveness and implementation of enhanced recovery after surgery programmes: a rapid evidence synthesis. BMJ Open. 2014;4(7):e005015.
42. Geltzeiler CB, Rotramel A, Wilson C, et al. Prospective study of colorectal enhanced recovery after surgery in a community hospital. JAMA Surg. 2014;149(9):955-961.
43. Core measure sets. The Joint Commission Web site. http:/www.jointcommission.org/core_measure_sets.aspx. Accessed September 18, 2015.
44. Scheer A, Martel G, Moloo H, et al. Laparoscopic colon surgery: does operative time matter? Dis Colon Rectum. 2009;52(10):1746-1752.
45. Chen JY, Ko TL, Wen YR, et al. Opioid-sparing effects of ketorolac and its correla-tion with the recovery of postoperative bowel function in colorectal surgery patients: a prospective randomized double-blinded study. Clin J Pain. 2009;25(6):485-489.

Why wait? Access this program and post-test @ CMEZone.com
11
46. Nguyen DL, Maithel S, Nguyen ET, et al. Does alvimopan enhance return of bowel function in laparoscopic gastrointestinal surgery? A meta-analysis. Ann Gastroenterol. 2015;28(4):475-480.
47. Rodriguez RW. Off-label uses of alvimopan and methylnaltrexone. Am J Health Syst Pharm. 2014;71(17):1450-1455.
48. Yu CS, Chun HK, Stambler N, et al. Safety and efficacy of methylnaltrexone in shortening the duration of postoperative ileus following segmental colectomy: results of two randomized, placebo-controlled phase 3 trials. Dis Colon Rectum. 2011;54(5):570-578.
49. Delaney CP, Craver C, Gibbons MM, et al. Evaluation of clinical outcomes with alvimopan in clinical practice: a national matched-cohort study in patients undergo-ing bowel resection. Ann Surg. 2012;255(4):731-738.
50. Kaiser AM. Evolution and future of laparoscopic colorectal surgery. World J Gastroenterol. 2014;20(41):15119-15124.
51. Rabhari NN, Zimmermann JB, Schmidt T, et al. Meta-analysis of standard, restrictive and supplemental fluid administration in colorectal surgery. Br J Surg. 2009;96(4):331-341.
52. Noble EJ, Harris R, Hosie KB, et al. Gum chewing reduces postoperative ileus? A systematic review and meta-analysis. Int J Surg. 2009;7(2):100-105.
53. Lewis SJ, Andersen HK, Thomas S. Early enteral nutrition within 24 h of intestinal surgery versus later commencement of feeding: a systematic review and meta- analysis. J Gastrointest Surg. 2009;13(3):569-575.
54. Lovely JK, Larson DW, Quast JM. A clinical practice agreement between pharma-cists and surgeons streamlines medication management. Jt Comm J Qual Patient Saf. 2014;40(7):296-302.
55. Bell TJ, Poston SA, Kraft MD, et al. Economic analysis of alvimopan in North American phase III efficacy trials. Am J Health Syst Pharm. 2009;66(15):1362-1368.
56. Absher RK, Gerkin TM, Banares LW. Alvimopan use in laparoscopic and open bowel resections: clinical results in a large community hospital system. Ann Pharmacother. 2010;44(11):1701-1708.
Post-Test1. All of the following techniques may facilitate recovery of GI
function after colorectal surgery except:a. Chewing gumb. Administration of alvimopanc. NG tube placementd. Avoidance of opioid analgesia
2. Which of the following patients would not be a candidate for placement on an ERAS pathway after colorectal surgery?a. Patients with an ASA classification of IV or higherb. Patients older than 65 yearsc. Patients with adenocarcinomad. Patients who have not had previous abdominal surgery
3. Patients who undergo colorectal procedures without DVT prophylaxis have a _____% chance of developing a venous thromboembolic event.a. 10b. 20c. 30d. 60
4. Measures that may reduce reliance on opioid analgesia after colorectal procedures include all of the following except:a. Local wound infiltration with bupivacaine liposomeb. Use of IV acetaminophenc. Use of epidural analgesiad. Placing the patient on nothing-by-mouth status following the
procedure
5. A 72-year-old patient has just undergone a successful colonic resection for colon cancer. He has had an NG tube placed. His respiratory and GI outcomes may be improved by:a. Keeping the NG tube in place for 48 hoursb. Keeping the NG tube in place for 72 hoursc. Removing the NG tube as soon as possibled. Prompt initiation of TPN and keeping the NG tube in place for
48 hours
6. Early postoperative feeding after colorectal procedures is associated with which of the following outcomes?a. Increased risk for anastomosis dehiscenceb. Increased risk for wound infectionsc. Increased risk for pneumoniad. None of the above
7. Which of the following statements regarding the use of mechanical bowel preparation before colorectal proce-dures is false?a. It is a practice employed by most colorectal surgeons in the
United Statesb. Its use prior to left- and right-sided resections has not been
endorsed by the Canadian Society of Colon and Rectal Surgeons
c. It has been demonstrated conclusively to have only adverse effects on postoperative outcomes
d. It has not been studied independently as part of an ERAS pathway
8. Which of the following IV fluid management strategies may improve outcomes for patients undergoing colorectal procedures?a. Aggressive IV fluid administration both intraoperatively and
postoperativelyb. Complete withholding of fluid during the operative procedurec. Careful administration of fluids, with monitoring of cardiac
output through Doppler technologyd. Administration of IV fluid in conjunction with routine NG tube
placement
9. Which of the following statements regarding the use of alvimopan in cases involving bowel resection with primary anastomosis is false?a. It can be administered after patients are discharged from the
hospitalb. It should only be administered for fewer than 15 doses in totalc. It may reduce hospitalization duration and costd. It requires a REMS plan
10. As part of an ERAS protocol, patients may begin enteral feeding on POD:a. 0b. 2c. 3d. 4

12 89 GI
SR1543
Evaluation Form Activity ID: 11278-EJ-42
Case Studies in Enhanced Recovery and Improved Patient Outcomes: Preventing Postoperative Ileus in Colorectal SurgeriesPlease complete the following evaluation questions to receive your certificate.
1. What degree best describes you?❑ MD/DO ❑ PA/PA-C ❑ NP❑ RN ❑ PharmD/RPh ❑ PhD❑ Other, please specify:
2. What is your area of specialization?❑ Surgery, surgical oncology ❑ Gastroenterology❑ Oncology, medical❑ Other, please specify:
3. Which of the following best describes your primary practice setting?❑ Solo practice ❑ Group practice❑ Government ❑ University/teaching system❑ Community hospital ❑ HMO/managed care❑ Nonprofit/community ❑ I do not actively practice❑ Other, please specify:
4. How long have you been in practice?❑ More than 20 years ❑ 11-20 years❑ 6-10 years ❑ 1-5 years❑ Less than 1 year ❑ I do not directly provide care
5. Approximately how many patients do you see each week?❑ Less than 50 ❑ 50-99 ❑ 100-149❑ 150-199 ❑ 200+❑ I do not directly provide care
6. How many patients undergoing radical cystectomy do you currently see each week?❑ Less than 5 ❑ 5-15 ❑ 16-25❑ 26-35 ❑ 36-45 ❑ 46-55❑ 56 or more ❑ I do not directly provide care
7. Please select the extent to which you agree/disagree that the activity supported the achievement of each learning objective
StronglyAgree
Agree Neutral Disagree Strongly Disagree
Evaluate the efficacy and safety of current strategies to reduce perioperative complications in procedures involving gastrointestinal (GI) tract surgeries
5 4 3 2 1
Manage patients who are candidates for procedures involving GI/genitourinary tract surgeries with evidence-based perioperative strategies to prevent postoperative ileus
5 4 3 2 1
Articulate features of perioperative enhanced recovery after surgery protocols that might improve patient outcomes
5 4 3 2 1
8. Please select the extent to which you agree/disagree that the activity achieved the following:
StronglyAgree
Agree Neutral Disagree Strongly Disagree
The faculty were effective in presenting the material 5 4 3 2 1The content was evidence based 5 4 3 2 1The educational material provided useful informa-tion for my practice 5 4 3 2 1
The activity enhanced my current knowledge base 5 4 3 2 1The activity provided appropriate and effective opportunities for active learning (eg, case studies, discussion, Q&A, etc)
5 4 3 2 1
The opportunities provided to assess my own learn-ing were appropriate (eg, questions before, during, or after the activity)
5 4 3 2 1
9. Based upon your participation in this activity, do you intend to change your practice behavior? (Choose only one of the following options)❑ I do plan to implement changes in my practice based on the
information presented❑ My current practice has been reinforced by the information
presented❑ I need more information before I will change my practice
10. Thinking about how your participation in this activity will influence your patient care, how many of your patients are likely to benefit? Please use a number (eg 250): __________
11. If you plan to change your practice behavior, what type of changes do you plan to implement? (Check all that apply)❑ Apply latest guidelines❑ Choice of treatment/management approach❑ Change in pharmaceutical therapy❑ Change in current practice for referral❑ Change in nonpharmaceutical therapy❑ Change in differential diagnosis❑ Change in diagnostic testing ❑ Other, please specify: ____________________________________
12. How confident are you that you will be able to make your intended changes?❑ Very confident ❑ Somewhat confident ❑ Unsure ❑ Not very confident
13. Which of the following do you anticipate will be the primary barrier to implementing these changes?❑ Formulary restrictions ❑ Insurance/financial issues❑ Time constraints ❑ Lack of multidisciplinary support❑ System constraints ❑ Treatment-related adverse events❑ Patient adherence/compliance❑ Other, please specify: _____________________________________
14. Was the content of this activity fair, balanced, objective, and free of bias?❑ Yes ❑ No, please explain: ______________________________
15. Please list any clinical issues/problems within your scope of practice you would like to see addressed in future educa-tional activities: ____________________________________________
Request for Credit (*required fields)Name*
Degree*
Organization
Specialty*
Address*
City, State, ZIP*
Telephone Fax
IMPORTANT: Your certificate will be EMAILED to your listed email address* below. (Please print legibly)
Post-Test Answers
1 2 3 4 5 6 7 8 9 10
*Valid email address required for receipt of your certificate.You will receive your certificate from [email protected].
For Physicians Only❑ I participated in the entire activity and claim 1.25 credits.❑ I participated in only part of the activity and claim _____ credits.