Case Sinusitis
33
CASE DISCUSSION SINUSITIS Supervisor dr. H. Oscar Djauhari, Sp. THT-KL Presentants Marcella Aprilia Lonatrista 2010.061.150 Arga Aditya 200873 0006 Otolaryngology, Head and Neck Department Medical Faculty of Unika Atma Jaya Medical Faculty of Muhammadiyah Jakarta University R. Syamsudin, S.H. Regional General Hospital, Sukabumi 1
-
Upload
darari-genadita -
Category
Documents
-
view
66 -
download
0
description
word
Transcript of Case Sinusitis
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 1/33
CASE DISCUSSION
SINUSITIS
Supervisordr. H. Oscar Djauhari, Sp. THT-KL
Presentants
Marcella Aprilia Lonatrista 2010.061.150
Arga Aditya 2008730006
Otolaryngology, Head and Neck Department
Medical Faculty of Unika Atma Jaya
Medical Faculty of Muhammadiyah Jakarta University
R. Syamsudin, S.H. Regional General Hospital, Sukabumi
1
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 2/33
26th November 2012 – 29th December 2012
CASE DISCUSSION
A. PATIENT’S IDENTITY
Name : Ms. I
Gender : Female
Age : 28 years old
Occupation : employer
Address : Sukabumi
B. HISTORY
• Chief Complaint
recurrent common cold since 4 months before admission
• History of Present Illness
A 28-year old woman came to ENT department at Syamsyudin
hospital with a chief complaint of recurrent cold at the morning since 4 month
before admission. The nose discharge had yellowish geen colour and smelled
odour since 1 month before admission. She also complained had nasal speech.
Fever and cough were denied. She had taken over the counter medication but
she hadn’t feel any improvement. No complainded on eyes.
• Additional Complaints :
headache, located at the base of the nose
• History of Past Illness
o History of right nose trauma with three times nose bleeding since 11 years
ago
o History of hypertension was denied
• History of Family Illness
History of family illness was denied
• Habits
o Recurrent cold
o Does not smoke
2
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 3/33
o Does not drink any alcohol substance.
o Does not use any routine medication.
o Does not use any narcotics.
C. PHYSICAL EXAMINATION
General condition : Appear calm
Body weight : 45 kg
Height : 156 cm
Blood pressure : 110/90 mmHg
Pulse : 80 beat per minute
Respiratory rate : 22 times per minutes
Temperature : 36
o
C
ENT Examination
• Ear
Right ear
- Auricle : normal
-
External auditory canal:
hyperemic (-), edema (-), mass (-), laceration (-) secretion (-) , cerumen (-)
- Tymphanic membrane:
Intact, hyperemic (-), retraction (-), light reflex (+)
Left ear
- Auricle : normal
- External auditory canal:
hyperemic (-), edema (-), mass (-), laceration (-) secretion (-) , cerumen (+)
- Tymphanic membrane:
Intact, bulging (-), light reflex (+)
3
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 4/33
Tuning fork test
• Rinne test : air conduction is being louder or louder than bone conduction
on both ear
• Weber test : no lateralization
• Schwabach test : same with examiner on both ear
•Nose
Right nose
- Mucous membrane:
hyperemic (+), edema (+), secretion (+), mass (-), laceration (-), crust (-)
- Inferior conchae : eutrophy
- Septum : no deviation
- Air passage : decreased
Left nose
- Mucous membrane:
hyperemic (+), edema (-), secretion (+), mass (-), laceration (-), crust (-)
- Inferior conchae : eutrophy
- Septum : no deviation
- Air passage : normal
4
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 5/33
• Oropharynx
- Posterior pharynx : hyperemic (-)
- Palatine tonsils : T1 / T1, hyperemic (-), detritus (-)
- Uvula : symmetrical
- Dental : no abnormatlities
• Maxillofacial : symmetrical
• Neck : no lymphadenopathy
D. WORKING DIAGNOSIS
Sinusitis
E. DIFFERENTIAL DIAGNOSIS
Allergic sinusitis
F. WORK-UP
Laboratory:
1. Routine blood count
2. Liver function test
5

7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 6/33
3. Blood glucose test
4. Renal function test
5. Bleeding time- clotting time
Chest X-ray PA position
Paranasal Sinus X-ray Water’s position
ECG
G. TREATMENT
Antral Wash Out dextra
Ceftriaxone 2 x 1 gram vial
Ketorolac 3 x 1 ampul (@30 mg/ml)
Tranexamic acid 3 x 2 ampul (@ 250 mg/ml)
6
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 7/33
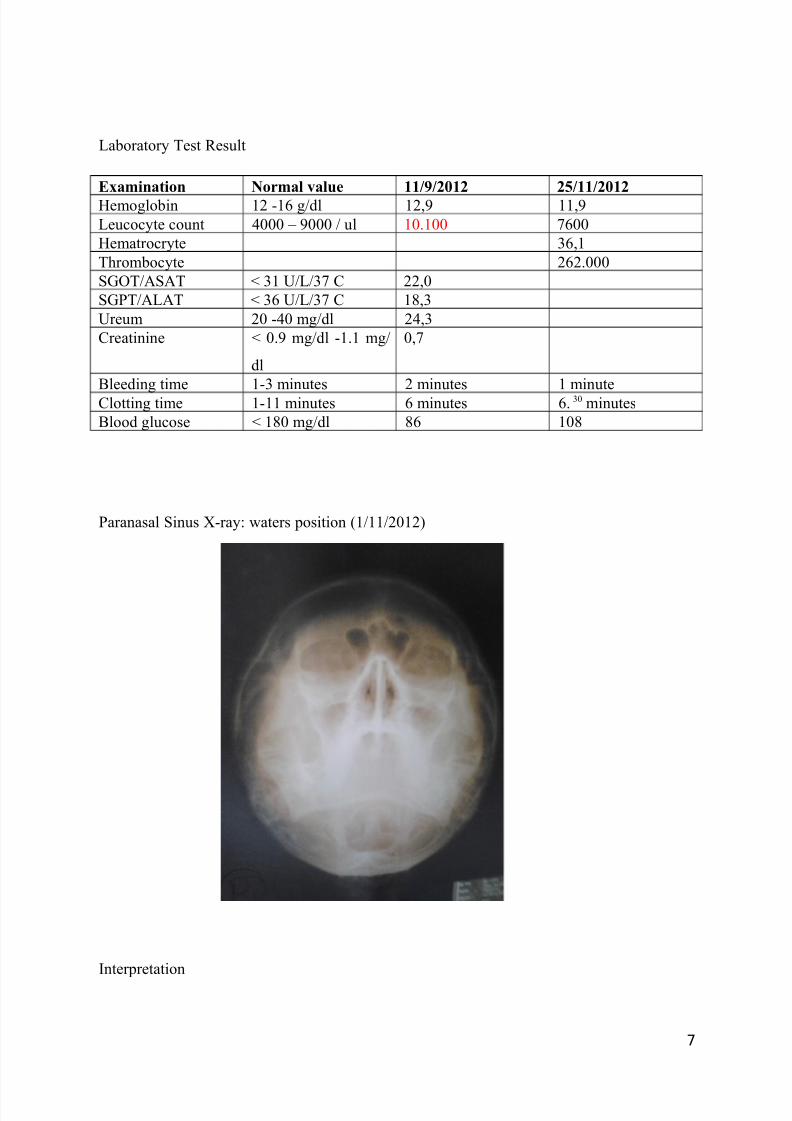
Laboratory Test Result
Examination Normal value 11/9/2012 25/11/2012
Hemoglobin 12 -16 g/dl 12,9 11,9
Leucocyte count 4000 – 9000 / ul 10.100 7600
Hematrocryte 36,1
Thrombocyte 262.000
SGOT/ASAT < 31 U/L/37 C 22,0
SGPT/ALAT < 36 U/L/37 C 18,3
Ureum 20 -40 mg/dl 24,3
Creatinine < 0.9 mg/dl -1.1 mg/
dl
0,7
Bleeding time 1-3 minutes 2 minutes 1 minute
Clotting time 1-11 minutes 6 minutes 6. 30 minutes
Blood glucose < 180 mg/dl 86 108
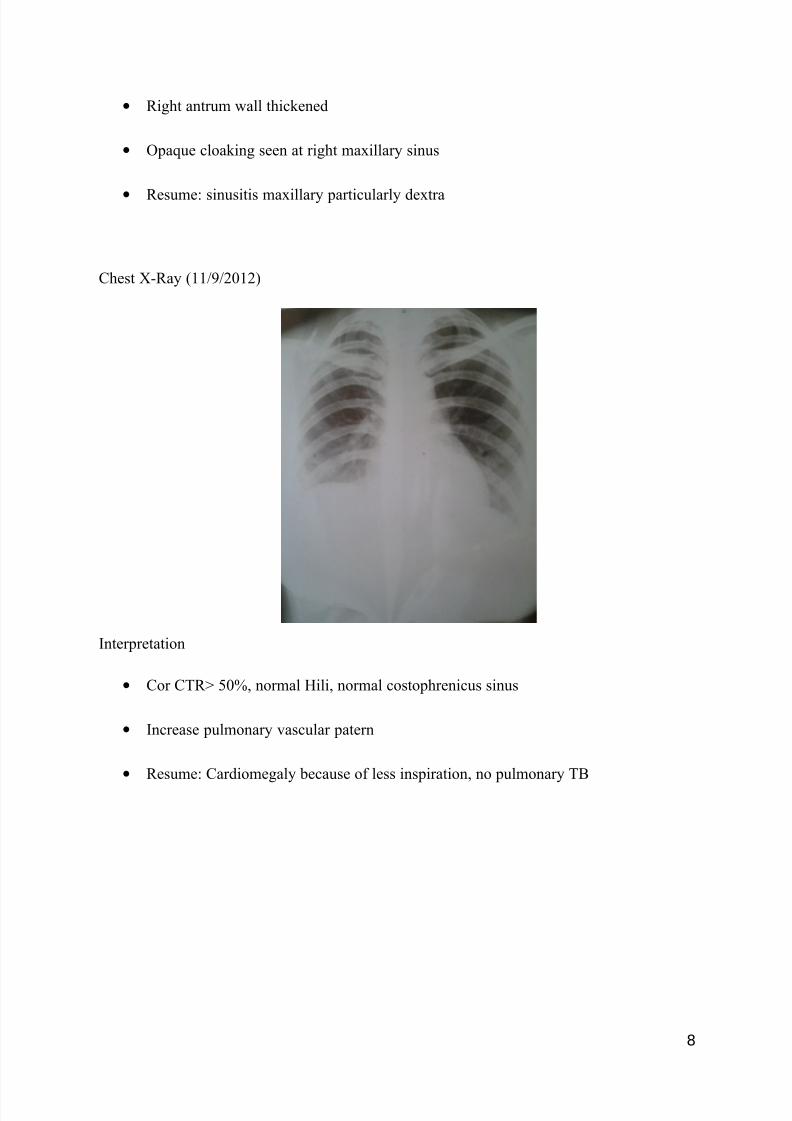
Paranasal Sinus X-ray: waters position (1/11/2012)
Interpretation
7
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 8/33
• Right antrum wall thickened
• Opaque cloaking seen at right maxillary sinus
• Resume: sinusitis maxillary particularly dextra
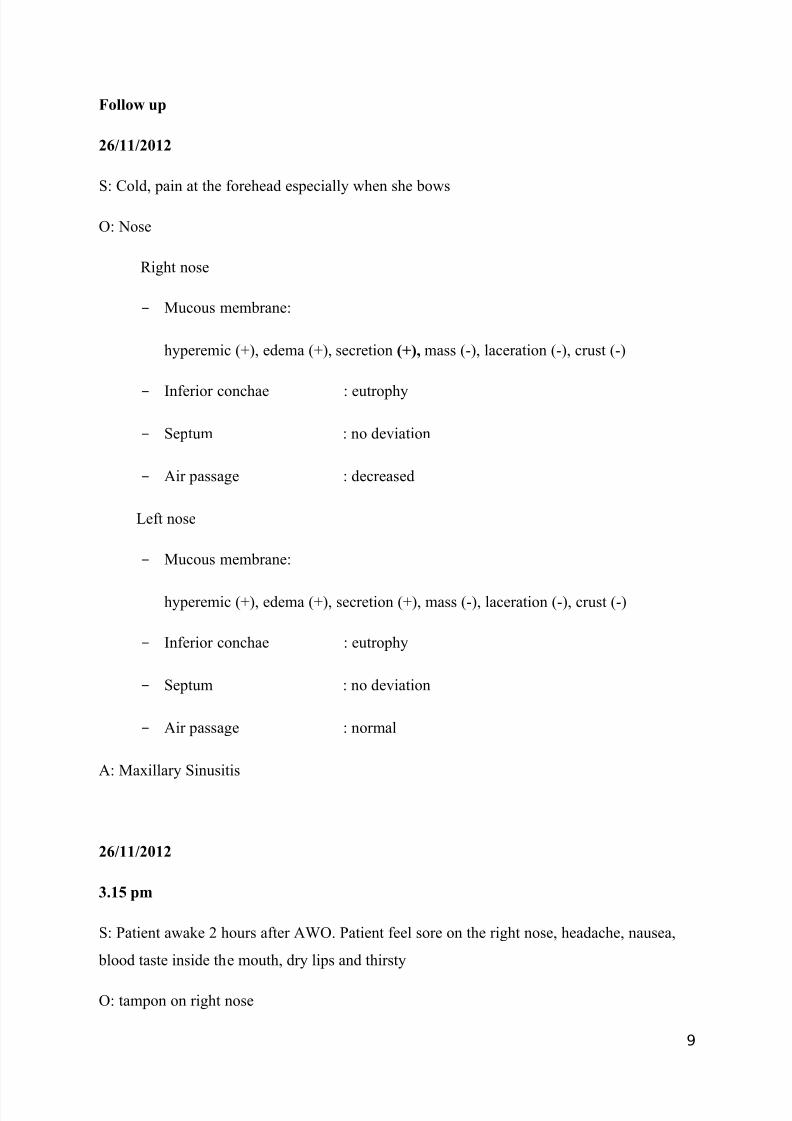
Chest X-Ray (11/9/2012)
Interpretation
• Cor CTR> 50%, normal Hili, normal costophrenicus sinus
• Increase pulmonary vascular patern
• Resume: Cardiomegaly because of less inspiration, no pulmonary TB
8
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 9/33
Follow up
26/11/2012
S: Cold, pain at the forehead especially when she bows
O: Nose
Right nose
- Mucous membrane:
hyperemic (+), edema (+), secretion (+), mass (-), laceration (-), crust (-)
- Inferior conchae : eutrophy
- Septum : no deviation
- Air passage : decreased
Left nose
- Mucous membrane:
hyperemic (+), edema (+), secretion (+), mass (-), laceration (-), crust (-)
- Inferior conchae : eutrophy
- Septum : no deviation
- Air passage : normal
A: Maxillary Sinusitis
26/11/2012
3.15 pm
S: Patient awake 2 hours after AWO. Patient feel sore on the right nose, headache, nausea,
blood taste inside the mouth, dry lips and thirsty
O: tampon on right nose
9
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 10/33
A: post-op sinusitis maxillaris dextra (AWO)
27/11/2012
08.00 am
S: Patient getting better, but still feel sore on the right nose, headache, blood taste inside the
mouth. Patient eat (liquid diet) and drink normally.
O: there’s still tampon plug on right nose
A: post-op sinusitis maxillaris dextra (AWO)
10
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 11/33
Chronic Rhinosinusitis
Chronic sinusitis is one of the more prevalent chronic illnesses in the United States,
affecting persons of all age groups. It is an inflammatory process that involves the paranasal
sinuses and persists for 12 weeks or longer. The literature has supported that chronic sinusitis
is almost always accompanied by concurrent nasal airway inflammation and is often preceded
by rhinitis symptoms; thus, the term chronic rhinosinusitis (CRS) has evolved to more
accurately describe this condition.
Most cases of chronic sinusitis are continuations of unresolved acute sinusitis;
however, chronic sinusitis usually manifests differently from acute sinusitis. Symptoms of
chronic sinusitis include nasal stuffiness, postnasal drip, facial fullness, and malaise.
Chronic sinusitis may be noninfectious and related to allergy, cystic fibrosis,
gastroesophageal reflux, or exposure to environmental pollutants. Allergic rhinitis,
nonallergic rhinitis, anatomic obstruction in the ostiomeatal complex, and immunologic
disorders are known risk factors for chronic sinusitis.
Medical therapy is directed toward controlling predisposing factors, treating
concomitant infections, reducing edema of sinus tissues, and facilitating the drainage of sinussecretions. The goal in surgical treatment is to reestablish sinus ventilation and to correct
mucosal opposition in order to restore the mucociliary clearance system. Surgery strives to
restore the functional integrity of the inflamed mucosal lining.
Anatomy
Knowledge of the anatomy of paranasal sinuses is essential for understanding the
pathophysiology and management of chronic sinusitis. The 4 pairs of paranasal sinuses are
11
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 12/33
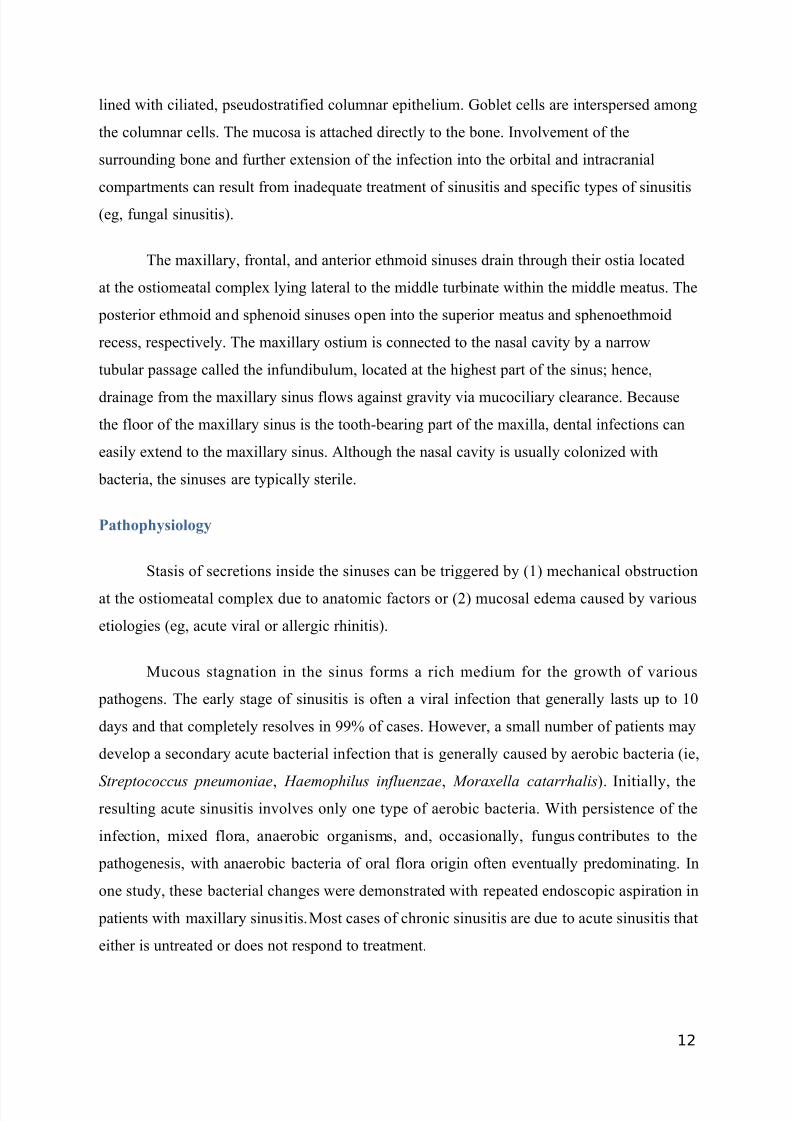
lined with ciliated, pseudostratified columnar epithelium. Goblet cells are interspersed among
the columnar cells. The mucosa is attached directly to the bone. Involvement of the
surrounding bone and further extension of the infection into the orbital and intracranial
compartments can result from inadequate treatment of sinusitis and specific types of sinusitis
(eg, fungal sinusitis).
The maxillary, frontal, and anterior ethmoid sinuses drain through their ostia located
at the ostiomeatal complex lying lateral to the middle turbinate within the middle meatus. The
posterior ethmoid and sphenoid sinuses open into the superior meatus and sphenoethmoid
recess, respectively. The maxillary ostium is connected to the nasal cavity by a narrow
tubular passage called the infundibulum, located at the highest part of the sinus; hence,
drainage from the maxillary sinus flows against gravity via mucociliary clearance. Because
the floor of the maxillary sinus is the tooth-bearing part of the maxilla, dental infections can
easily extend to the maxillary sinus. Although the nasal cavity is usually colonized with
bacteria, the sinuses are typically sterile.
Pathophysiology
Stasis of secretions inside the sinuses can be triggered by (1) mechanical obstruction
at the ostiomeatal complex due to anatomic factors or (2) mucosal edema caused by various
etiologies (eg, acute viral or allergic rhinitis).
Mucous stagnation in the sinus forms a rich medium for the growth of various
pathogens. The early stage of sinusitis is often a viral infection that generally lasts up to 10
days and that completely resolves in 99% of cases. However, a small number of patients may
develop a secondary acute bacterial infection that is generally caused by aerobic bacteria (ie,
Streptococcus pneumoniae, Haemophilus influenzae, Moraxella catarrhalis). Initially, theresulting acute sinusitis involves only one type of aerobic bacteria. With persistence of the
infection, mixed flora, anaerobic organisms, and, occasionally, fungus contributes to the
pathogenesis, with anaerobic bacteria of oral flora origin often eventually predominating. In
one study, these bacterial changes were demonstrated with repeated endoscopic aspiration in
patients with maxillary sinusitis. Most cases of chronic sinusitis are due to acute sinusitis that
either is untreated or does not respond to treatment.
12
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 13/33
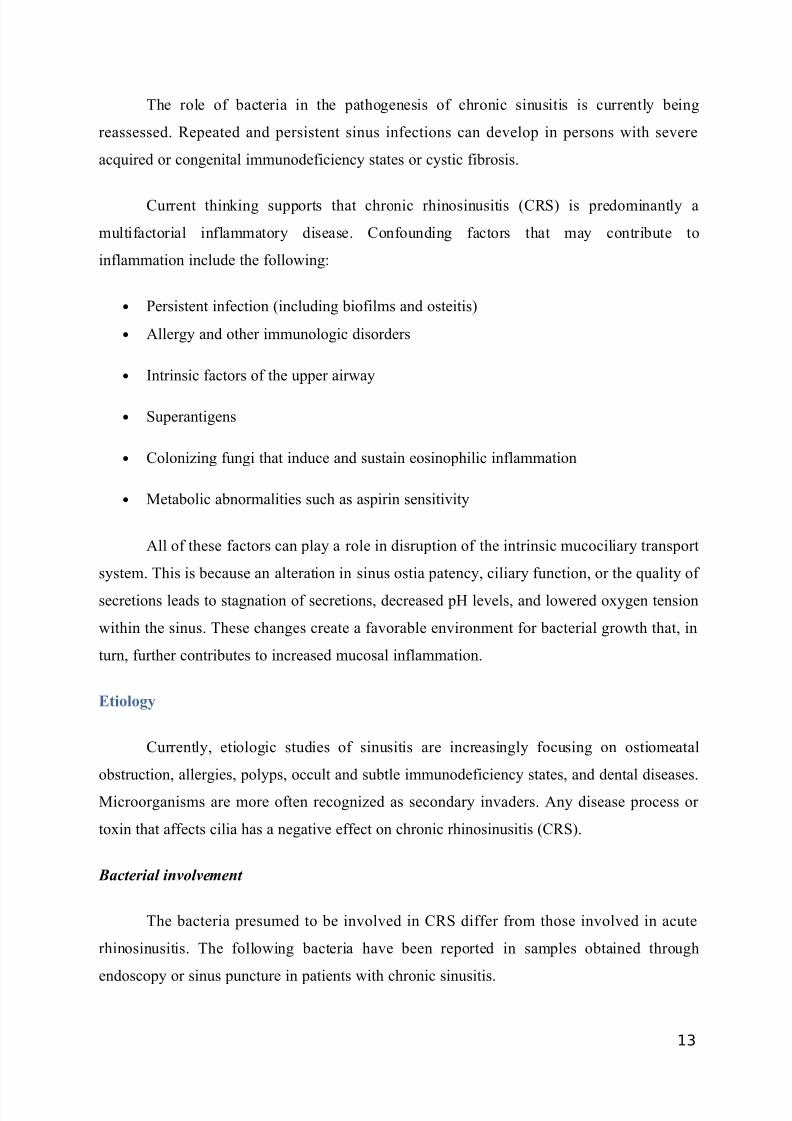
The role of bacteria in the pathogenesis of chronic sinusitis is currently being
reassessed. Repeated and persistent sinus infections can develop in persons with severe
acquired or congenital immunodeficiency states or cystic fibrosis.
Current thinking supports that chronic rhinosinusitis (CRS) is predominantly a
multifactorial inflammatory disease. Confounding factors that may contribute to
inflammation include the following:
• Persistent infection (including biofilms and osteitis)
• Allergy and other immunologic disorders
• Intrinsic factors of the upper airway
• Superantigens
• Colonizing fungi that induce and sustain eosinophilic inflammation
• Metabolic abnormalities such as aspirin sensitivity
All of these factors can play a role in disruption of the intrinsic mucociliary transport
system. This is because an alteration in sinus ostia patency, ciliary function, or the quality of
secretions leads to stagnation of secretions, decreased pH levels, and lowered oxygen tension
within the sinus. These changes create a favorable environment for bacterial growth that, in
turn, further contributes to increased mucosal inflammation.
Etiology
Currently, etiologic studies of sinusitis are increasingly focusing on ostiomeatal
obstruction, allergies, polyps, occult and subtle immunodeficiency states, and dental diseases.
Microorganisms are more often recognized as secondary invaders. Any disease process or
toxin that affects cilia has a negative effect on chronic rhinosinusitis (CRS).
Bacterial involvement
The bacteria presumed to be involved in CRS differ from those involved in acute
rhinosinusitis. The following bacteria have been reported in samples obtained through
endoscopy or sinus puncture in patients with chronic sinusitis.
13
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 14/33
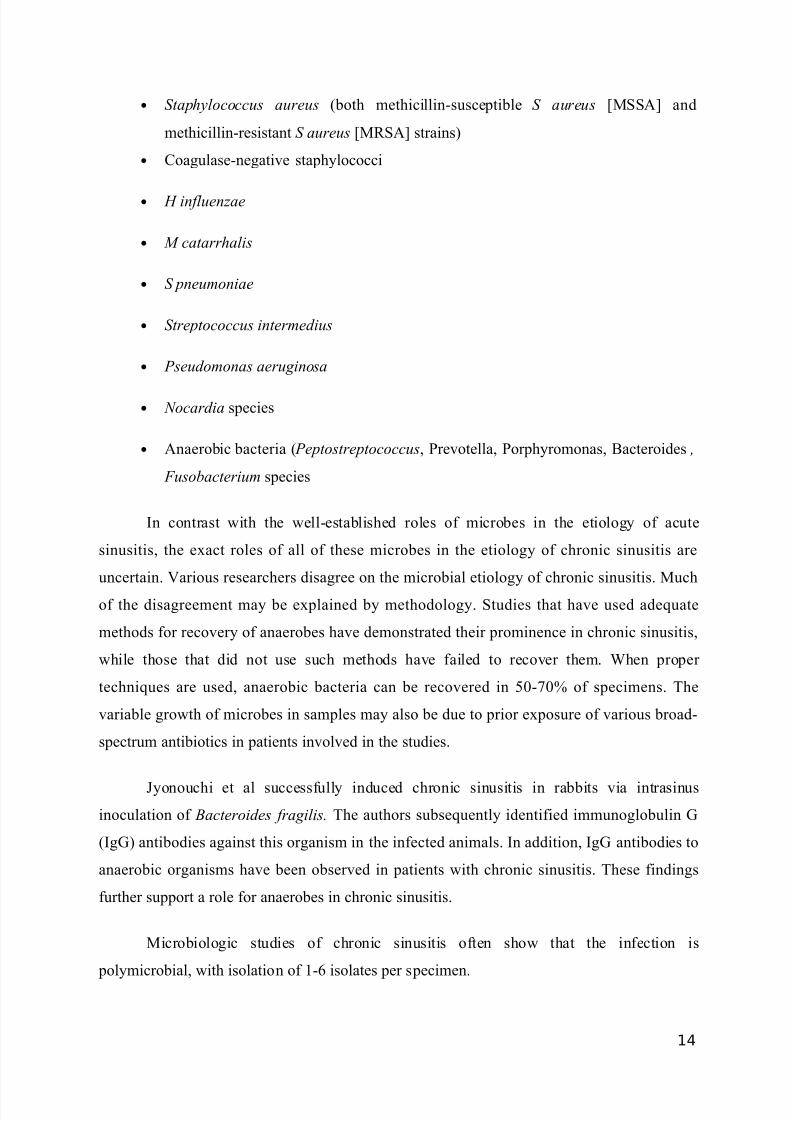
• Staphylococcus aureus (both methicillin-susceptible S aureus [MSSA] and
methicillin-resistant S aureus [MRSA] strains)
• Coagulase-negative staphylococci
• H influenzae
• M catarrhalis
• S pneumoniae
• Streptococcus intermedius
• Pseudomonas aeruginosa
• Nocardia species
• Anaerobic bacteria ( Peptostreptococcus, Prevotella, Porphyromonas, Bacteroides ,
Fusobacterium species
In contrast with the well-established roles of microbes in the etiology of acute
sinusitis, the exact roles of all of these microbes in the etiology of chronic sinusitis are
uncertain. Various researchers disagree on the microbial etiology of chronic sinusitis. Much
of the disagreement may be explained by methodology. Studies that have used adequate
methods for recovery of anaerobes have demonstrated their prominence in chronic sinusitis,
while those that did not use such methods have failed to recover them. When proper
techniques are used, anaerobic bacteria can be recovered in 50-70% of specimens. The
variable growth of microbes in samples may also be due to prior exposure of various broad-
spectrum antibiotics in patients involved in the studies.
Jyonouchi et al successfully induced chronic sinusitis in rabbits via intrasinus
inoculation of Bacteroides fragilis. The authors subsequently identified immunoglobulin G
(IgG) antibodies against this organism in the infected animals. In addition, IgG antibodies to
anaerobic organisms have been observed in patients with chronic sinusitis. These findings
further support a role for anaerobes in chronic sinusitis.
Microbiologic studies of chronic sinusitis often show that the infection is
polymicrobial, with isolation of 1-6 isolates per specimen.
14
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 15/33
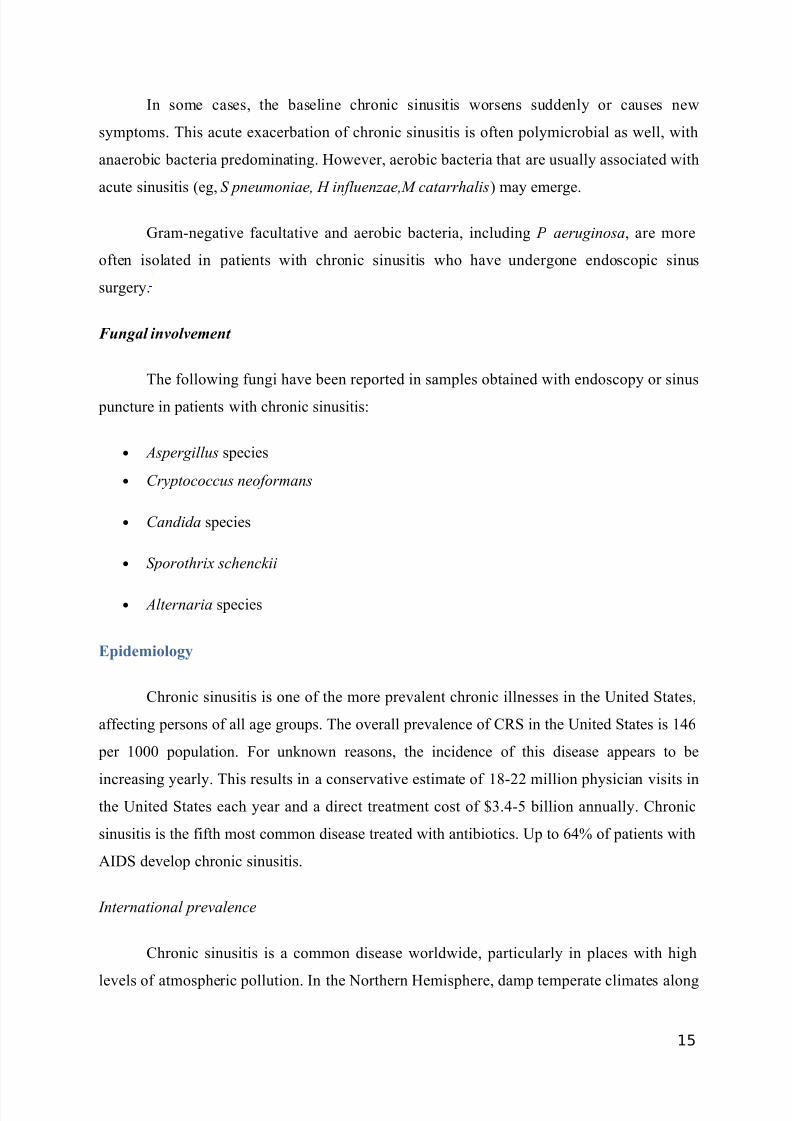
In some cases, the baseline chronic sinusitis worsens suddenly or causes new
symptoms. This acute exacerbation of chronic sinusitis is often polymicrobial as well, with
anaerobic bacteria predominating. However, aerobic bacteria that are usually associated with
acute sinusitis (eg, S pneumoniae, H influenzae,M catarrhalis) may emerge.
Gram-negative facultative and aerobic bacteria, including P aeruginosa, are more
often isolated in patients with chronic sinusitis who have undergone endoscopic sinus
surgery.
Fungal involvement
The following fungi have been reported in samples obtained with endoscopy or sinus
puncture in patients with chronic sinusitis:
• Aspergillus species
• Cryptococcus neoformans
• Candida species
• Sporothrix schenckii
• Alternaria species
Epidemiology
Chronic sinusitis is one of the more prevalent chronic illnesses in the United States,
affecting persons of all age groups. The overall prevalence of CRS in the United States is 146
per 1000 population. For unknown reasons, the incidence of this disease appears to be
increasing yearly. This results in a conservative estimate of 18-22 million physician visits inthe United States each year and a direct treatment cost of $3.4-5 billion annually. Chronic
sinusitis is the fifth most common disease treated with antibiotics. Up to 64% of patients with
AIDS develop chronic sinusitis.
International prevalence
Chronic sinusitis is a common disease worldwide, particularly in places with high
levels of atmospheric pollution. In the Northern Hemisphere, damp temperate climates along
15
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 16/33
with higher concentrations of pollens are associated with a higher prevalence of chronic
sinusitis.
Rhinosinusitis in children
Rhinosinusitis is more common in the pediatric population because this term includes
both acute and chronic infection and both viral and bacterial disease. This is likely secondary
to an increased frequency of exposure to upper respiratory tract infections in the pediatric
population.
Risk factors
The following conditions and risk factors predispose patients to the development of
chronic sinusitis:
• Anatomic abnormalities of the ostiomeatal complex (eg, septal deviation, concha
bullosa, deviation of uncinate process, Haller cells)
• Allergic rhinitis
• Nasal polyps
• Nonallergic rhinitis (eg, vasomotor rhinitis, rhinitis medicamentosa, cocaine abuse)
• Nasotracheal intubation
• Nasogastric intubation
• Hormonal (eg, puberty, pregnancy, oral contraception)
• Tumoral obstruction
• Immunologic disorders (eg, common variable immunodeficiency, immunoglobulin A
[IgA] deficiency, IgG subclass deficiency, AIDS)
• Cystic fibrosis
• Primary ciliary dyskinesia, Kartagener syndrome
• Wegener granulomatosis
• Repeated upper respiratory tract infections
16
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 17/33
• Smoking
• Environmental pollution
• Periodontitis/significant dental disease
History
Patient history is extremely important in chronic rhinosinusitis (CRS) because of the
broad overlap between sinus symptoms and other disease processes, as well as poor
correlation between symptoms and endoscopic and radiographic findings.
Chronic sinusitis manifests more subtly than acute sinusitis. Unless an appropriate
history is taken, the diagnosis may be missed. The typical symptoms of acute sinusitis—fever
and facial pain—are usually absent in chronic sinusitis. Fever, when present, may be low
grade.
Patients with chronic sinusitis may present with the following symptoms:
• Nasal stuffiness
•
Nasal discharge (of any character from thin to thick and from clear to purulent)
• Postnasal drip
• Facial fullness, discomfort, and headache
• Chronic unproductive cough
• Hyposmia
• Sore throat
• Fetid breath
• Malaise
• Easy fatigability
• Anorexia
• Exacerbation of asthma
17
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 18/33
• Dental pain
• Visual disturbances
• Sneezing
• Stuffy ears
• Unpleasant taste
• Fever of unknown origin
In pediatric settings, halitosis is reported more commonly by parents of younger
children. Nasal obstruction with mouth breathing and associated sore throat may be present.In some individuals with chronic sinusitis, parents may note occasional and painless morning
eye swelling. Older children may complain of loss of taste due to associated nasal obstruction
and anosmia. Nocturnal symptoms may include snoring and coughing due to associated
postnasal drip.
The patient history should focus on the following key factors, beginning with
consideration of major and minor diagnostic criteria:
• The presence of major symptoms (including purulent anterior nasal drainage,
purulent-discolored posterior nasal drainage, nasal obstruction or blockage, facial
congestion or fullness, facial pain or pressure, and hyposmia or anosmia)
• The presence of minor symptoms (including headache, ear pain or fullness, halitosis,
dental pain, cough, fever, fatigue)
• Duration of symptoms
• Exacerbating and relieving factors
• History of previous nasal or paranasal sinus surgery
• Current medications
• Previous treatments and their duration
• Other confounding health problems (including asthma, allergy, and
immunocompromising disorders)
18
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 19/33
• Active or passive tobacco smoke
Physical Examination
Physical examination in patients with chronic sinusitis may reveal various findings. It
should include a complete head and neck examination (lymphadenopathy) to confirm the
diagnosis and to rule out more serious disorders.
Sinus palpation is performed to evaluate tenderness or swelling. Pain or tenderness on
palpation over frontal or maxillary sinuses may be noted. Transillumination of maxillary or
frontal sinuses may be useful; it lacks sensitivity but may have value in experienced hands.
An oral cavity and oropharynx examination is used to evaluate the integrity of the
palate and the condition of dentition and to look for evidence of postnasal drip.
Oropharyngeal erythema and purulent secretions may be noted. Dental caries may be present.
Anterior rhinoscopy, with the use of a nasal speculum, is used to evaluate the
condition of the nasal mucosa and to look for purulent drainage or evidence of polyps or
other nasal masses. Other contributing factors to CRS that can be evaluated are nasal septal
deviation and turbinate hypertrophy. The nasal examination should be carried out both beforeand after the use of a topical decongestant.
The nasal examination can be supplemented with the use of nasal endoscopy (if
available). Endoscopic (rhinoscopic) examination findings include the following:
• Nasal mucosal erythema, edema
• Purulent secretions
• Nasal obstruction due to deviated nasal septum or hypertrophied turbinates
• Nasal polyps
Ear examination for the presence of middle ear fluid that may be the sign of a mass in
the nasopharynx is indicated.
Ocular examination for spread of disease to the orbit and function of ocular
musculature is indicated. Ophthalmic manifestations include the following:
19
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 20/33
• Conjunctival congestion
• Lacrimation
• Proptosis, extraocular muscle palsies, and visual disturbances (when complicated by
orbital extension)
Laryngeal examination is used to look for other confounding upper airway pathology
including laryngeal-pharyngeal reflux (LPR). Lung examination is performed to determine if
coexisting lower airway disease is present.
Cranial nerve examination is performed to look for underlying sinus malignancy or
neurological disorder.
Manifestations of fungal sinusitis
Fungal sinusitis can manifest in different ways. Unlike acute invasive fungal sinusitis,
which is observed in patients who are immunosuppressed or who have diabetes, chronic
fungal sinusitis is usually observed in immunocompetent patients. Mycetomas or fungus balls
may be asymptomatic or may manifest as chronic sinusitis. Allergic fungal sinusitis usually
manifests as nasal polyps and allergic sinusitis. Fungal elements in the sinuses are the inciting
allergens.
Diagnostic Criteria
In 1996, the American Academy of Otolaryngology-Head & Neck Surgery convened
a multidisciplinary Rhinosinusitis Task Force (RTF). This group defined adult rhinosinusitis
diagnostic criteria. These 1996 diagnostic criteria required 2 or more major factors or 1 major
factor and 2 minor factors for the diagnosis of rhinosinusitis.
Major factors included facial pain or pressure, nasal obstruction or blockage, nasal
discharge or purulence or discolored postnasal discharge, hyposmia or anosmia, purulence in
nasal cavity, and fever (for acute rhinosinusitis only).
Minor factors were defined as headache, fever (for CRS), halitosis, fatigue, dental
pain, cough, and ear pain, pressure, or fullness. Of note, facial pain requires another major
factor associated with it for diagnosis (facial pain plus 2 minor factors is not deemed
sufficient for diagnosis of rhinosinusitis).
20
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 21/33
In 2003, the RTF’s definition was amended to require confirmatory radiographic or
nasal endoscopic or physical examination findings in addition to suggestive history.The 2003
diagnostic criteria for CRS require the above criteria for longer than 12 weeks or more than
12 weeks of physical findings. In addition, one of the following signs of inflammation must
be present:
• Discolored nasal drainage from the nasal passages, nasal polyps, or polypoid swelling
as identified on physical examination with anterior rhinoscopy after decongestion or
nasal endoscopy
• Edema or erythema of the middle meatus or ethmoid bulla on nasal endoscopy
• Generalized or localized erythema, edema, or granulation tissue (If the middle meatus
or ethmoid bulla is not involved, radiologic imaging is required to confirm a
diagnosis.)
Imaging modalities confirming the diagnosis include the following:
• Computed tomography (CT) scanning demonstrating isolated or diffuse mucosal
thickening, bone changes, or air-fluid levels
OR
• Plain sinus radiography revealing air-fluid levels or greater than 5 mm of
opacification of one or more sinuses
• Magnetic resonance imaging (MRI) not recommended for routine diagnosis because
of its excessive sensitivity and lack of specificity
In general, plain radiography has low sensitivity and specificity. CT scanning isconsidered the imaging standard for evaluation of chronic sinusitis.
The latest executive summary on adult sinusitis has altered the definition for CRS to
read 12 weeks or longer of 2 or more of the following symptoms:
• Anterior or posterior mucopurulent drainage
• Nasal obstruction
• Facial-pain-pressure-fullness
21
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 22/33
• Decreased sense of smell
In addition, inflammation must be documented by demonstrating one of the
following:
• Purulent mucus or edema in the middle meatus or ethmoid region
• Polyps in the nasal cavity or middle meatus
• Imaging showing inflammation of the paranasal sinuses
This is in contrast to recurrent acute sinusitis, which is present when 4 or more
episodes per year of acute bacterial rhinosinusitis without signs and symptoms of
rhinosinusitis between episodes.
Imaging Studies
Plain radiography may show mucosal thickenings or sinus opacities. Air fluid levels
are uncommon in chronic sinusitis. Ethmoid sinuses and the ostiomeatal complex are not
visualized well on plain sinus radiography.
Contrast-enhanced CT scanning is the current radiologic criterion standard for the
evaluation of sinus diseases, although performing CT scanning in all patients with chronic
sinus disease may be prohibitively expensive or medically unnecessary. CT scans are usually
indicated after failure of maximal medical therapy, before surgical planning for evaluation of
suspected complications, and when a neoplasm is a possibility. CT scan combined with
endoscopic examination helps the surgeon to make operative decisions.
Coronal CT scan of the sinus correlates best with the surgical approach, permitting
visualization of the anatomy of the nasal cavity, ostiomeatal complex, sinus cavities, and
surrounding structures such as the orbit, cribriform plate, and optic canal. Anatomic
obstructions at the ostiomeatal complex and dental pathologies are visualized well. Specific
entities in the sinus cavity, such as aspergilloma, are also visualized well.
Most centers now offer limited sinus CT scans that consist of 5-12 coronal cuts. These
limited or screening CT scans cost about the same as a plain radiography but provide more
information.
22
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 23/33
Magnetic resonance imaging (MRI) is generally reserved only for complex cases.
Soft-tissue contrast is better with MRI. Neoplasms, orbital and intracranial complications,
and fungal sinusitis can be better evaluated with MRI.
Biopsy
Biopsy samples from the maxillary sinus mucosa of patients with chronic sinusitis
show basement membrane thickening, atypical gland formation, goblet cell hyperplasia,
mononuclear cell infiltration, and subepithelial edema. The mononuclear cell infiltrate often
predominantly demonstrates neutrophils in acute disease and eosinophils in chronic disease.
Rarely, squamous cell metaplasia may be seen.
Brush biopsy or turbinate biopsy
Evaluation of cilia function with a brush biopsy or turbinate biopsy can be considered
in cases of presumed cilia dysfunction.
Endoscopic biopsy
Specimens obtained from sinus openings via endoscopy correlate well with those
obtained with endoscopic surgery or sinus puncture. These should be processed for
cultivation of aerobic and anaerobic bacteria, as well as fungi. Specimens evaluated for
anaerobic bacteria should be sent in proper transport media. Liquid specimens are preferred
to swab specimens.
Cultures
Calcium-alginate tipped applicators are a readily available device that can be used to
obtain a culture. Studies of chronic sinusitis have demonstrated no correlation between nasal
flora and culture from the sinuses. Nasal swab cultures have no diagnostic value.
Occasionally, an abundance of eosinophils in the nasal smear suggests an allergic etiology. In
severe cases, blood cultures, including fungal blood cultures, may be helpful.
Endoscopically directed middle meatal culture
Recent literature has supported the use of endoscopically directed culture of themiddle meatus (the primary drainage system of the anterior ethmoid, maxillary, and frontal
23
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 24/33
sinuses) with the use of either a suction trap or a swab. Endoscopically directed middle
meatal cultures had a sensitivity of 80.9% and a specificity of 90.5% in a recent meta-
analysis.
Maxillary sinus tap
Traditionally, maxillary sinus tap via inferior meatal puncture was performed for
sinus culture. Many otolaryngologists have moved away from maxillary sinus tap because of
the discomfort of the procedure and the understanding that a culture of an organism from the
middle meatus may be more accurate to determine the bacteria involved in the disease
process.
Symptomatic Treatment
Symptoms may be relieved with topical decongestants, topical steroids, antibiotics,
nasal saline, topical cromolyn, or mucolytics.
Steam inhalation and nasal saline irrigation may help by moistening dry secretions,
reducing mucosal edema, and reducing mucous viscosity.
Initial oral steroid therapy followed by topical steroid therapy was found to be more
effective than topical steroid therapy alone in decreasing polyp size and improving olfaction
in patients with chronic rhinosinusitis (CRS) with at least moderate nasal polyposis.
Catalano et al evaluated balloon dilation for the treatment of chronic frontal sinusitis
in 20 patients with advanced sinus disease in whom medical therapy had failed and therefore
required operative intervention. Preoperative and postoperative CT scans were compared.
There were no significant complications from balloon dilation, and there was significantimprovement in patients with certain subsets of CRS.
Antimicrobial Therapy
An adequate antibiotic trial in CRS usually consists of a minimum of 3-4 weeks of
treatment, preferably culture directed. Oral antibiotic regimens are generally used to treat
chronic sinusitis, since this condition is primarily treated in an outpatient setting. For resistant
cases, there may be a role for intravenous antibiotic therapy.
24
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 25/33
Initial choice of the appropriate antimicrobial(s) is usually empiric. Sinus cultures are
not generally obtained for community-acquired infections unless empiric therapy fails to
elicit a response. The agent(s) chosen should be effective against the most likely bacterial
etiologies, including both aerobic and anaerobic pathogens. The likelihood of involvement by
beta-lactamase–producing organisms should be considered. If methicillin-resistant
Staphylococcus aureus (MRSA) is a possible pathogen, coverage for this should be included.
History of drug allergies (if any) and cost of therapy should be taken into account as well. In
addition, if the patient has received antibiotics during the preceding 3 months, a different
class of antibiotics should be used.
Therapeutic regimens include the combination of a penicillin (eg, amoxicillin) plus a
beta-lactamase inhibitor (eg, clavulanic acid), clindamycin, a combination of metronidazole
plus a macrolide or a second- or third-generation cephalosporin, and the newer quinolones
(eg, moxifloxacin). All of these agents (or similar ones) are available in oral and parenteral
forms. Other effective antimicrobials are available only in parenteral form (eg, cefoxitin,
cefotetan). If aerobic gram-negative organisms (eg, Pseudomonas aeruginosa) are involved,
parenteral therapy with an aminoglycoside, a fourth-generation cephalosporin (cefepime or
ceftazidime), or oral or parenteral treatment with a fluoroquinolone (only in postpubertal
patients) is added. Parenteral therapy with a carbapenem (ie, imipenem, meropenem) is more
expensive but provides coverage for most potential pathogens, both anaerobes and aerobes.
Clindamycin as initial therapy provides coverage for MRSA and is effective against
anaerobes. Alternatives include trimethoprim-sulfamethoxazole or linezolid, which are added
to other regimens that cover anaerobes. Parenteral antimicrobials effective against MRSA
include vancomycin, linezolid, and daptomycin.
Ferguson et al performed a prospective observational study of 125 adults with classic
symptoms of chronic rhinosinusitis who underwent nasal endoscopy and sinus CT. Severe
symptoms occurred more often in younger patients with normal CT scans of the sinus than in
those with positive CT findings. Improvement in response to antibiotics was similar for
patients with positive CT findings and those with normal CT scans. The authors concluded
that most symptoms considered to be typical for chronic rhinosinusitis proved to be
nonspecific, and they suggest that objective evidence of mucopurulence assessed by
endoscopy or CT should be obtained if a prolonged course of antibiotics is being considered.
25
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 26/33
Surgical Care
Presurgical
A preoperative antibiotic course may be administered in the weeks prior to surgery if
an active infection is present. A preoperative steroid course may be administered if
significant edema or polyps are observed on examination.
In the preoperative holding area, nasal decongestion is begun with the patient
receiving sprays of oxymetazoline. Following the commencement of general endotracheal
anesthesia, the eyes are protected with eye ointment and thin strips of tape. The nasal
passages are decongested with appropriate vasoconstrictors such as topical cocaine if not
medically contraindicated.
If septoplasty is to be performed, the septum should be infiltrated with 1% lidocaine
with 1:100,000 epinephrine in the submucochondrial plane. Then, the patient is draped and
prepared for surgery. A 4-mm 0- or 30-degree endoscope may be used, depending on the
surgeon's preference. If septoplasty is to be performed, it may be done either before or after
sinus surgery. Place the septoplasty incision in the unobstructed nasal passage to allow better
visualization of the more obstructed side.
Management of Chronic Maxillary Sinusitis
Three main surgical options are available: (1) endoscopic uncinectomy with or
without maxillary antrostomy, (2) the Caldwell-Luc procedure, and (3) inferior antrostomy
(nasoantral window).
Today, endoscopic maxillary antrostomy and uncinectomy are the standard for
treatment for refractory chronic maxillary sinusitis. The Caldwell-Luc and inferior
antrostomy approaches are reserved for rare circumstances, such as a case of severe allergic
fungal sinusitis in which standard antrostomy alone does not allow complete extirpation of
fungal concretions or complete drainage.
Additionally, further FESS with mucosal-sparing techniques may be performed if
additional disease is present within the ethmoid, sphenoid, and frontal sinuses.
26
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 27/33
Endoscopic Maxillary Antrostomy
Under endoscopic guidance, the middle turbinate may gently be moved medially, with
care to avoid fracturing the turbinate–skull base junction. At this point, the uncinate process
should be within view, and it is injected with 1% lidocaine with 1:100,000 epinephrine. Local
injections can be made using a 10-mL control syringe with a Luer lock 27-gauge needle
attached.
First, the root of the uncinate process is injected. Next, the inferior portion of the
uncinate process is injected. The root of the middle turbinate is infiltrated as well. Finally, an
injection is placed at the inferior junction of the basal lamella with the lateral nasal wall. This
serves to vasoconstrict the sphenopalatine artery. Approximately 1-2 mL of local anesthetic isused at each injection site, with the bevel down (toward mucosa). An appreciable blanch of
the mucosa should be observed with each injection.
If using an image-guided system, it can be calibrated at this time (thereby giving time
for vasoconstriction from the injections to take effect). Alternatively, the system may be
calibrated prior to beginning the case. When using an image-guided system, checking the
position of the guidance tracking in a few different known points and confirming the
accuracy in 3 dimensions is important. Typically, for isolated chronic maxillary sinus disease,
image-guided surgery is not necessary.
After decongestion, uncinectomy is the next step. Uncinectomy can be performed in
numerous ways. The following is the authors' preference. Under endoscopic guidance, a
maxillary ostium seeker is insinuated just behind the uncinate process and used carefully to
displace the free edge of the uncinate outwardly and anteriorly. To prevent lamina papyracea
injury, care is taken to very gently manipulate only the uncinate process and not to penetratedeeply.
Next, 90-degree upbiting forceps are used to grasp the free edge of the uncinate
process. In a controlled push-and-pull fashion, staying parallel to the lacrimal duct, the
uncinate process is then removed. Care is taken to engage the uncinate process parallel to the
lateral nasal wall to prevent injury to the lamina papyracea. Any remaining uncinate process
may be removed using a combination of microdebrider powered instrumentation and
pediatric forceps. All portions of the uncinate should be taken down completely to permit
27
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 28/33
visualization of the natural maxillary sinus ostium, roughly parallel to the inferior portion of
the middle turbinate.
Once the natural ostium is identified, an ostium seeker can be placed through the
ostium and then carefully pushed posteriorly to widen the ostium. Using a through-cutting
forceps, the ostium is enlarged, thereby completing a maxillary antrostomy. The maxillary
sinus should be inspected with a 30- or 70-degree scope to ensure that no further disease is
present within the sinus and that the natural ostium was included in the antrostomy.
If either a microlith or a polyp is present, it may be removed using curved giraffe
forceps or a curved suction. Further endoscopic work can be performed if disease is present
in other sinuses.
If lateralization of the middle turbinate is a concern and to allow easier postoperative
examination of the maxillary antrostomy in the office, the controlled synechiae technique, as
described by Bolger et al, may be used. Briefly, this involves abrading the opposing areas of
mucosa from the medial middle turbinate and septum. With healing, the two roughened areas
appose, thus medializing the turbinate for improved postoperative visualization of the
maxillary sinus antrostomy.
The middle meatus may be packed with various products if either postoperative
bleeding or lateralization of the middle turbinate is a concern. Many packing materials have
been described, ranging from rolled Gelfilm to Merocel packing. The authors' preference is
for a latex-free, glove-covered, trimmed Merocel in the middle meatus. This should be
removed at the first postoperative visit (3-5 d).
Balloon catheters in endoscopic sinus surgery
Balloon catheter technology has been used to dilate the maxillary sinus natural ostia
without bone or soft-tissue removal. Early reports show sustained patient symptom
improvement and sinus ostia patency. Further study and long-term outcomes with this
technology will determine its role in endoscopic sinus surgery.
28
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 29/33
Caldwell-Luc Procedure
For patient comfort, this procedure typically is performed under general anesthesia.
However, if medical comorbidities preclude general anesthesia, the procedure may be
performed with local anesthetic and sedation. It may be performed in conjunction with
nasoantral window (inferior antrostomy) to facilitate postoperative surveillance.
Lidocaine, 1% with 1:100,000 epinephrine, is injected in the incision site, and time is
allowed for vasoconstriction. Make a 3-cm incision centered over the canine tooth and first
premolar while leaving about 0.5-1 cm of gingiva intact above the dentition to facilitate
closure.
Using electrocautery, dissection is carried down through the soft tissue and
periosteum to bone. Next, a periosteal elevator is used to widely elevate periosteum from the
anterior wall of the maxilla. Care is taken to identify and avoid injury to the infraorbital
nerve, which is vertical and inferior to the midpupillary line. In the canine fossa, with mallet
and osteotome, the maxillary sinus is entered through its anterior thin bone. Thereafter,
rongeurs are used to enlarge the opening. Any pus from the maxillary cavity may be sent for
culture. The disease within the sinus can be addressed appropriately. Next, the sinus is
irrigated. The incision is then closed using 3-0 or 4-0 absorbable suture.
Inferior Antrostomy
Vasoconstriction is begun with topical oxymetazoline on pledgets. Next, 1% lidocaine
with 1:100,000 epinephrine is injected under endoscopic guidance along the lateral nasal wall
underneath the inferior turbinate. A 3-mL syringe with a 27-gauge needle facilitates the
injection. Because the nasolacrimal duct lies approximately 1 cm anterior to the natural
maxillary ostium, the injection and surgical antrostomy site is about one to two thirds of the
distance back along the inferior turbinate.
Next, the maxillary sinus is punctured in this region using a curved suction or trocar.
This antrostomy should then be enlarged with through-cutting forceps. The maxillary sinus
disease should then be extirpated as appropriate.
Functional Endoscopic Sinus Surgery
29
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 30/33
Surgical care is used as an adjunct to medical treatment in some cases. Surgical care is
usually reserved for cases that are refractory to medical treatment and for patients with
anatomic obstruction. Recent studies suggest that preoperative CT findings prior to sinus
surgery may be poor predictors of surgical outcomes.
The goal in surgical treatment is to reestablish sinus ventilation and to correct
mucosal opposition in order to restore the mucociliary clearance system. Surgery strives to
restore the functional integrity of the inflamed mucosal lining.
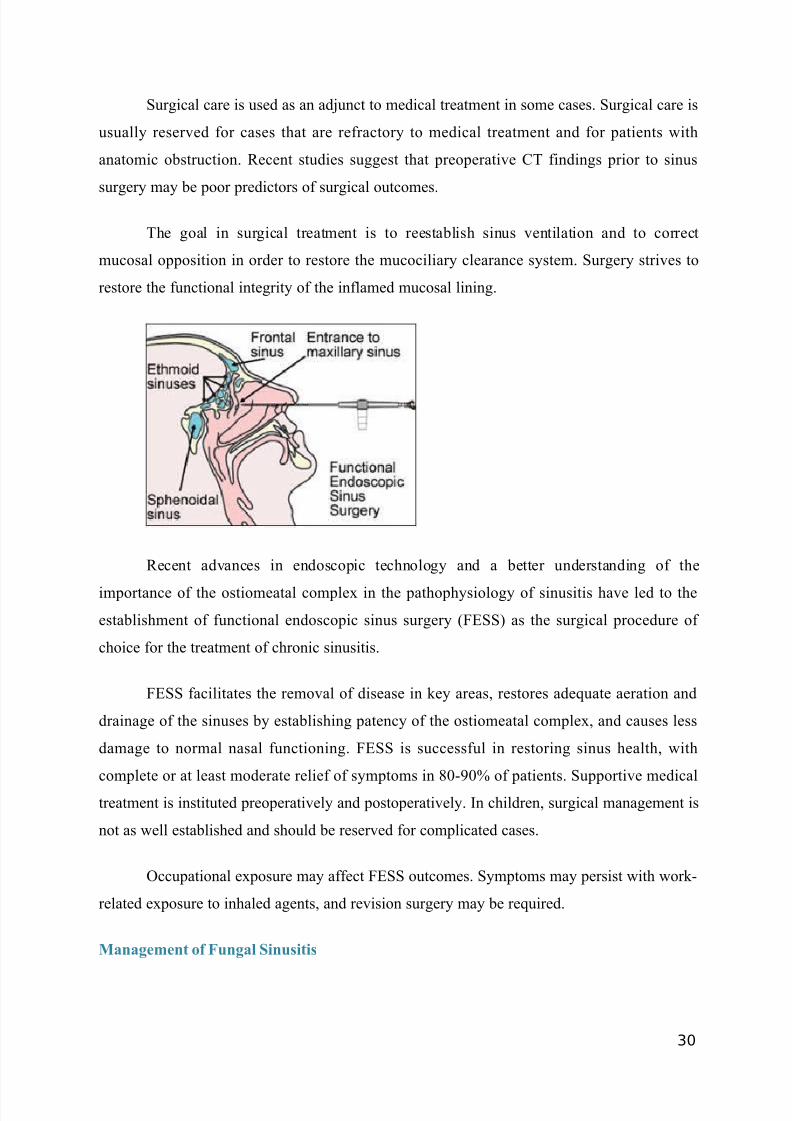
Recent advances in endoscopic technology and a better understanding of the
importance of the ostiomeatal complex in the pathophysiology of sinusitis have led to the
establishment of functional endoscopic sinus surgery (FESS) as the surgical procedure of
choice for the treatment of chronic sinusitis.
FESS facilitates the removal of disease in key areas, restores adequate aeration and
drainage of the sinuses by establishing patency of the ostiomeatal complex, and causes less
damage to normal nasal functioning. FESS is successful in restoring sinus health, with
complete or at least moderate relief of symptoms in 80-90% of patients. Supportive medical
treatment is instituted preoperatively and postoperatively. In children, surgical management is
not as well established and should be reserved for complicated cases.
Occupational exposure may affect FESS outcomes. Symptoms may persist with work-
related exposure to inhaled agents, and revision surgery may be required.
Management of Fungal Sinusitis
30
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 31/33
The preferred treatment for chronic fungal sinusitis is surgical debridement.
Mycetomas or fungus balls are best treated by means of surgical removal. Allergic fungal
sinusitis, which usually manifests as nasal polyps and allergic sinusitis, is treated by means of
systemic steroids and surgical removal of polyps and mucinous secretions.
Prognosis
Because of its persistent nature, chronic sinusitis can become a significant cause of
morbidity. If left untreated, it can reduce the quality of life and the productivity of the
affected person.
Chronic sinusitis is associated with exacerbation of asthma and serious complications
such as brain abscess and meningitis, which can produce significant morbidity and mortality.
Early and aggressive medical treatment for chronic sinusitis typically results in
satisfactory outcomes. Functional endoscopic sinus surgery (FESS) restores sinus health with
complete or moderate relief of symptoms in 80-90% of patients with recurrent or medically
unresponsive chronic sinusitis.
Chronic sinusitis is rarely life threatening, although serious complications can occur
because of the proximity to the orbit and cranial cavity. Approximately 75% of all orbital
infections are directly related to sinusitis. Intracranial complications remain comparatively
rare, with 3.7-10% of intracranial infections related to sinusitis.
Complications
The most common complication of chronic sinusitis is superimposed acute sinusitis.
In children, the presence of pus in the nasopharynx may cause adenoiditis, and a high percentage of such patients develop secondary serous or purulent otitis media. Dacryocystitis
and laryngitis may also occur as complications of chronic sinusitis in children.
Orbital complications include preseptal cellulitis, subperiosteal abscess, orbital cellulitis,
orbital abscess, and cavernous sinus thrombosis. Intracranial complications include
meningitis, epidural abscess, subdural abscess, and brain abscess.
31
7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 32/33
Some studies have suggested a higher incidence of complications associated with
fungal sinusitis. Untreated chronic sinusitis can lead to life-threatening complications, as in
patients with cystic fibrosis. Other complications include osteomyelitis and mucocele
formation.
Reference
32

7/16/2019 Case Sinusitis
http://slidepdf.com/reader/full/case-sinusitis-5633879b26523 33/33
Adams L George, Boies L, et al. Boies Buku Ajar Penyakit THT edisi 6 . Penerbit buku
kedokteran EGC. Jakarta 1997
Brook, Itzhakm, et al. Chronic Sinusitis. Updated: Feb 15, 2012. Medscape.
http://emedicine.medscape.com/article/232791-overview
Patel, Ankit, et al. Surgical Treatment of Chronic Maxillary Sinusitis Surgical Overview .
Updated: Mar 29, 2011. Medscape. http://emedicine.medscape.com/article/861886-
overview#aw2aab6b4
Soepardi, Efiaty Arsyad dan Nurbaiti Iskandar (ed.). 2003. Buku Ajar Telinga Tenggorok
Kepala Leher . Jakarta : Fakultas Kedokteran Universitas Indonesia.
Singh, Ameet, et al. Paranasal Sinus Anatomy. Updated: Jun 28, 2011. Medscape.
http://emedicine.medscape.com/article/1899145-overview#showall