Case series of pseudocyst of pancreas
29
CASE SERIES OF PSEUDOCYST OF PANCREAS STANLEY MEDICAL COLLEGE & HOSPITAL,CHENNAI
-
Upload
kaushik-kumar-eswaran -
Category
Health & Medicine
-
view
27 -
download
0
Transcript of Case series of pseudocyst of pancreas
CASE SERIES OF PSEUDOCYST OF PANCREAS
STANLEY MEDICAL COLLEGE & HOSPITAL,CHENNAI


Authors
Prof.Dr.D.Nagarajan Dr.G.Venkatesh Dr.S.Jim Jebakumar Dr.K.Gautham
Dr.E.Kaushik Kumar, (MS Final Year PG)
குறள் 414:
கற்றி�லனா�யினுங்கேகட்கஅஃதொ��ருவற்கு
ஒற்கத்��ன்ஊற்றி�ந்துணை�.
. உரை�: நூல்கணை க்கற்றிவல்ணைலயி�யினும், கற்றிறி�ந்�வர்க $டம்
கேகட்டறி�யி கேவண்டும், அதுஒருவனுக்குவ�ழ்க்ணைகயில் � ர்ச்சி� வந்� கே+�துஊன்றுகேக�ல் கே+�ல்துணை�யி�கும்..

Chronic Collection of amylase-rich fluid enclosed in a non-epitheliazed wall of fibrous(collagen) or granulation tissue.
Follow after Acute Pancreatitis(5-15%)
Chronic Pancreatitis(20-38%)
Trauma
4- 8 weeks from the onset of AP
Single or multiple or multilobulated

Duct leak Intrapancreatic or extend beyond into other cavities
or compartments Regress spontaneously 50% Chronic pseudocysts may persist
Thick-walled or large (over 6 cm in diameter)
Lasted for a long time (over 12 weeks)
Arisen in the context of chronic pancreatitis

Symptoms
Pain
SatietyLoss of Weight
Fullness

Complications
Abscess /systemic sepsisIntracystic
hemorrhage/pseudoaneurysms
SMV/PV thrombosis
Peritonitis/intraperitoneal bleeding

-US,C
T
- Identificati
on of pseudocyst
and differentiat
es from abscess
EUS- Guided
FNA
Differentiates between
chronic pseudocyst and cystic neoplasms
ERCP/MRCP
ductal communicatio
n,ductal anomalies,
chronic pancreatitis,plan treatment

Amylase- Level usually high in pseudocysts, but occasionally in tumours
Cytology- Inflammatory cells in pseudocyst CA 19-9,CEA and MUCIN – negative

Intervention
INDICATIONS
Symptoms
If complications develop
Distinction has to be made between a pseudocyst and a tumour
Symptomatic, failure with conservative treatment, persistence over 4 weeks or longer

EndoscopicSurgical
Distance of pseudocyst to the gastrointestinal wall <1 cm
Size>5 cm, gut compression, single cyst, mature cyst, no disconnected segment of pancreatic duct
Complications
Drainage internallyStomachDuodenum Jejunum
Recurrence <5%

Newer techniques
Forward-viewing echoendoscope
PFC puncture devices
Combination devices
Devices for maintenance of cystenterostomy
Multiple transluminal gateway technique (MTGT)

Case 1
36 year female presented with complaints of yellowish discolouration of eyes, high coloured urine,pale stools for 1 month associated with upper abdominal discomfort and intense itching. No vomiting/ugi bleed. H/o treatment for Acute Pancreatitis 6 months before. No addictive habits. No other contributory history. O/e Icteric,non-tender epigastric mass of size 8 x 6 cm extending to right hypochondrium, smooth surface,firm in consistency,no movement with respiration. No free fluid and other systems were normal.
Transabdominal USG revealed a pseudocyst from head of pancreas compressing the CBD causing dilation of CBD and IHBR. CECT - 7.3 x 6.7 x 5.1 cm pseudocyst from head of pancreas compressing the CBD(1.2cm). TBR-6.3mg%. SAP- 517 IU/L. Coagulation profile-Normal.
UGI Scopy- Normal

Patient was taken up for surgery and a Roux loop
Cystojejunostomy was done which relieved the
biliary compression. Post operatively the total
bilirubin was 3.2 on POD 4 and subsequently
returned to normal level. Cyst fluid amylase
was 1210 IU and cytology negative for malignant
cells. Cyst wall HPE – Inflammatory tissue. Patient
was relieved of symptoms and no post operative
complications. Review
USG after 2 months, no radiologically detectable
pseudocyst.
Case 2 A 32-year-old male was admitted with complaints of upper abdominal pain and jaundice of 3 months duration. A history of a
passage of clay-colored stools and high-colored urine was present. The patient gave a history of acute abdominal pain following a binge of alcohol 6 months ago which was managed conservatively. On examination he was icteric and pruritic marks were present all over the body. Abdominal examination revealed an epigastric mass of size 7*6 cm, which was firm in consistency, had the upper border not made out, and which did not move with respiration. The liver was enlarged and palpable 3 cm below the right costal margin. A liver function test showed elevated serum bilirubin of 16 mg/dL (normal < 1 mg/dL), the direct component being 14 mg/dL (< 0.8 mg/dL), and serum alkaline phosphatase was 206 IU/L (normal value 20–140 IU/L). CA 19-9 was within normal limits (less than 10 IU/Ml.Recently diagnosed DM started on Insulin
USG abdomen - 8*7cm hypoechoic lesion arising from the head of the pancreas with dilatation of the intrahepatic and extrahepatic biliary tree. The common bile duct (CBD) measured 1.1 cm in diameter. Cholelithiasis was also seen.
MRCP and CECT-confirmed the USG findings of a pseudocyst arising from the head of the pancreas compressing the distal CBD, causing dilatation of biliary radicles
CECT showed additional features of chronic calcific pancreatitis involving the body and tail of the pancreas.
UGIendoscopy - normal gastric and duodenal mucosa with extraneous compression of the antropyloric region of the stomach and duodenum.
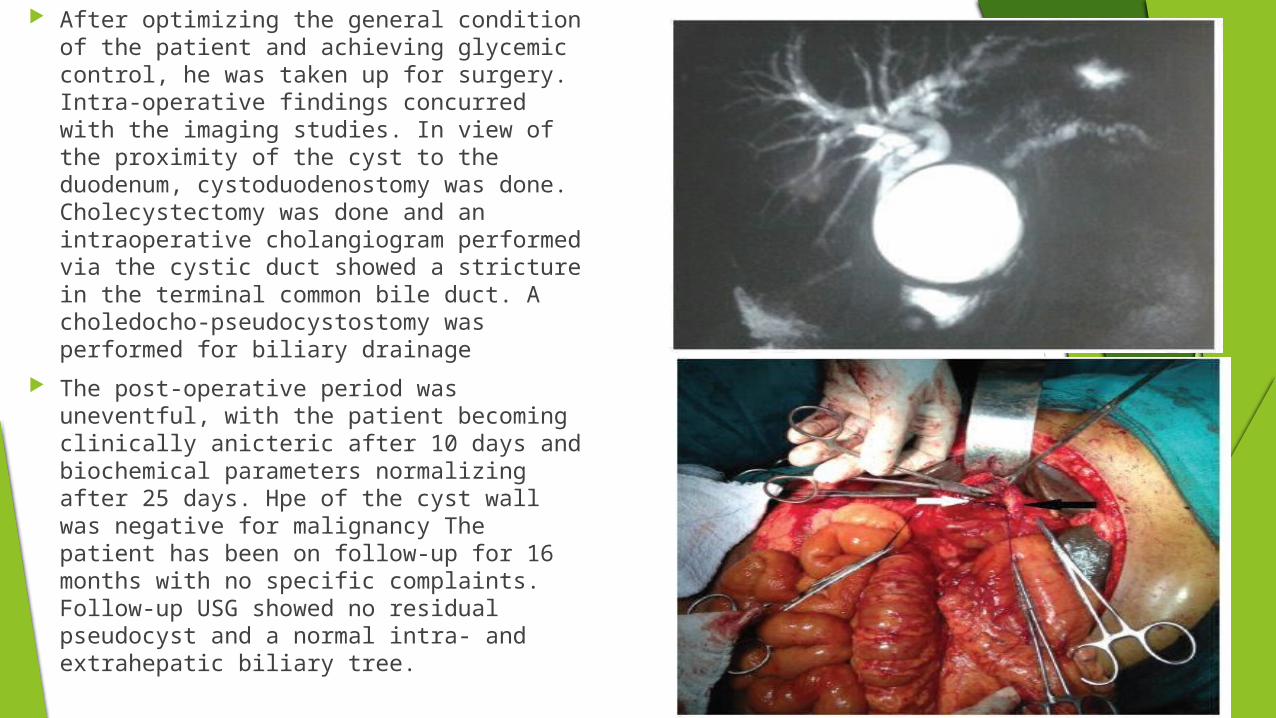
After optimizing the general condition of the patient and achieving glycemic control, he was taken up for surgery. Intra-operative findings concurred with the imaging studies. In view of the proximity of the cyst to the duodenum, cystoduodenostomy was done. Cholecystectomy was done and an intraoperative cholangiogram performed via the cystic duct showed a stricture in the terminal common bile duct. A choledocho-pseudocystostomy was performed for biliary drainage
The post-operative period was uneventful, with the patient becoming clinically anicteric after 10 days and biochemical parameters normalizing after 25 days. Hpe of the cyst wall was negative for malignancy The patient has been on follow-up for 16 months with no specific complaints. Follow-up USG showed no residual pseudocyst and a normal intra- and extrahepatic biliary tree.

Case 3 48 year male chronic alcoholic presented with complaints of fullness in upper abdomen for 4
months. No h/o fever/ vomiting/jaundice/bowel/bladder disturbances. H/o anorexia and weight loss +. H/o three episodes of acute pancreatitis conservatively managed since 4 years. Stopped alcohol after the second episode. No h/o exocrine pancreatic insufficiency. Recently diagnosed DM on OHAs. On examination, thin built and ill nourished,anicteric,flat abdomen, firm to hard non tender, oval mass of size 6 x 5 cm in epigastrium,not moving with respiration with restricted mobility. Other systems normal.
Blood parameters and amylase,lipase and LFT normal range.Ca 19-9 – 12 IU Transabdominal USG – 4.3 x 5 cm cystic lesion in body of pancreas with altered echoes. MRCP- ? Chronic Pseudocyst of pancreas. ? IPMN of pancreatic body. No e/o calcifications in
parenchyma or ductal system. Usg guided FNAC- No e/o tumour cells in the material studied. UGI Scopy- pan gastritis

Surgery- Roux loop Cysto-Jejunostomy
Follow up- HPE- Chronic Inflammatory cells.
Cyst Fluid- Amylase- 774 IU
6 months after surgery – no radiologically detectable cyst.

Case 4
54year male non alcoholic presented with complaints of pain in upper left quadrant of abdomen radiating to back for 6 months. No h/of fever /vomiting/ jaundice/bowel/bladder disturbances. No H/o anorexia and weight loss . H/o one episode of acute pancreatitis conservatively managed before 7 months. No addictive habits. On examination,anicteric,no pallor, upper abdomen fullness +. Tenderness + epigastrium and left hypochondrium. Ill defined mass occupying the above quadrants,no organomegaly/freefluid.Other systems normal.
Blood parameters and amylase,lipase and LFT normal range. Transabdominal USG – 8.6 x 6.4 cm cystic lesion in tail of pancreas abutting the spleen.
Another cyst of size 3.2 x 2.2 cm in body of pancreas. ? Pseudocyst ? Cystic neoplasm MRCP- Pseudocyst of pancreas in body and tail abutting spleen. To r/o Cystic
neoplasm. Usg guided FNAC- No e/o tumour cells in the material studied. UGI Scopy- ulcer + pre pyloric region. HPE- Chronic non-specific inflammation

Surgery – Roux loop cystojejunostomy Follow up- HPE- non specific Inflammatory cells. Cyst Fluid- Amylase- 1564 IU 3 months after surgery – symptomatic relief,
radiologically cyst not seen in tail of pancreas. 2 x 2cm seen in body of pancreas.

Case 5 32 year male chronic alcoholic presented with complaints of acute onset
epigastric pain for 2 days. H/o fever & vomiting +.No h/o jaundice/bowel/bladder disturbances. H/o anorexia +. Last binge of alcohol 1 day before admission.On examination, moderately built and nourished,anicteric,tachypnoeic,tachycardic,flat abdomen,upper abdomen movement reduced with respiration,epigatric tenderness and guarding +.BS sluggish. . Other systems normal.
CXR – No e/o hollow viscus perforation. Amylase – 2150 IU, Lipase – 983 IU .LFT normal range. Transabdominal USG – bulky edematous pancreas with surrounding fat
stranding and fluid collection. CECT Abdomen- F/s/o Acute Pancreatitis with Acute fluid collection and
minimal left pleural effusion. UGI Scopy- erosive antral gastritis

Patient managed as acute moderate pancreatitis conservatively.
After 1 month patient reported with complaints of abdominal discomfort and difficulty in breathing on exertion. No h/o fever or vomiting. On examination, epigastric fullness +. 10 x 6 cm smooth surfaced,firm non-tender mass occupying epigastrium,right and left hypochondrium. Left base breath sounds were absent.

Trans abdominal ultrasound – Pseudocyst of pancreas occupying body and tail with left pleural effusion and ascites
Cect abdomen - Pseudocyst of pancreas occupying body and tail with left pleural effusion and ascites. Wall thickness 4mm.
Conservatively managed. 6 weeks after- cyst size reduced to 4 x 3 cm.

Case 6 26 year male presented with Abdominal pain for 2 weeks-Acute
onset,Epigastrium to start with later became diffuse,Continuous,pricking pain,radiating to back,relieved by leaning forward and with medications.H/o non-bilious vomiting immediately after food intake + for the past one week.H/o constipation + x 3 days. H/o yellowish discolouration of sclera with passage of high coloured urine and clay coloured stools x 4 days +. No h/o fever /pruritus/abdominal distension/recent loss of weight/loss of appetite.H/o intermittent epigastric pain x 3 months. No comorbidities. Chronic Alcoholism x 3 yrs >360ml/day-last drink 8 days back
Not Anaemic,Deeply Icteric,No clubbing,No Generalised Lymphadenopathy,No Pedal Edema
Examination of Abdomen- Abdomen flat, Tenderness + Epigastrium,Right Hypochondrium,No guarding/rigidity,No obliteration of liver dullness,No mass/organomegaly,No free fluid,Murphys sign –ve.

Ultrasound Abdomen: Normal study UGI SCOPY: Pangastritis/Erosive Antral
Gastritis,Bulbar healed duodenal lesions.Submucosal lesion at D2 entry with luminal obstruction ?Pseudocyst causing duodenal obstruction.
SVS: Extrinsic compression at the level of D2,scope not passed beyond
CECT ABDOMEN: Possibility of stricture at the junction of 3rd and 4th part duodenum causing luminal obstruction
MRCP: ?Intramural Pseudocyst in the submucosal layer of Duodenum at the junction of D2,D3
Patient was managed conservatively and clinically improved.
Follow up serial radiological investigations showed gradual regression and disappearance after 12 weeks

Conclusion Due to progress in sensitivity and more widespread availability of diagnostic
imaging techniques, the incidence of pancreatic pseudocysts seems to be increasing steadily. .
In the above series the different presentations of pseudocyst of pancreas and the different techniques of management was elaborated
The majority of these cysts are asymptomatic, and the decision whether or not to operate is not always straightforward
The apparent question is how to proceed after the detection of an asymptomatic pancreatic cyst choosing one of the following options: no further investigations, additional imaging ± fine needle aspiration (FNA), surveillance, or surgical/endoscopic treatment.
Intervention is contemplated if the patient has Symptoms,if complications develop or a distinction has to be made between a pseudocyst and a tumour
References
Sabiston textbook of surgery,19th edition
Schwartz’s Principles of surgery,9th edition
Novel Technique in the Management of Obstructive Jaundice Caused by Pancreatic Pseudocyst , Archives of ClinicalExperimental Surgery,Gautham Krishnamurthy, Venkatesh Gottumukala, A Rajendran, P Darwin
www.giejournal.org ,GASTROINTESTINAL ENDOSCOPY Volume 77, No. 6 : 2013
World J Gastroenterol 2009 January 7; 15(1): 38-47 [email protected] World Journal of Gastroenterology ISSN 1007-9327
Pancreatic pseudocysts (Part I)Article by John Baillie, MB, ChB, FRCP,Durham, North Carolina








![Differential Diagnosis of Pancreatic Cyst Tumors · The pancreas has signs of pancreatitis [25]. Pseudocyst contains of fluid that often transparent or brown, leaking, low viscosity,](https://static.fdocuments.net/doc/165x107/5f0753117e708231d41c6c0f/differential-diagnosis-of-pancreatic-cyst-tumors-the-pancreas-has-signs-of-pancreatitis.jpg)