albumin microspheres for study of the reticuloendothelial system

JK SCIENCE
96 www.jkscience.org Vol. 17 No.2, April - June 2015
From the Deptt of G. Surgery, Govt. Medical College, Srinagar, Kashmir J&K IndiaCorrespondence to : Dr M.R. Attri, Assistant Professor, Department of G Surgery, Govt Medical College Srinagar, Kashmir J&K India.
Laparoscopic SpleenectomyM.R. Attri, Shahnawaz Ahangar, Rajni Bhardwaj, Muhammad Idrees Bashir
CASE REPORT
AbstractSpleen is the largest reticuloendothelial organ in the body consisting of an encapsulated mass of vascularand lymphoid tissue and responsible for defensive actions and hence the name defense organ for it. Likeany other organ in the body it is also afflicted by a number of disorders among which are splenic cysts.Herein we report a case of large primary splenic cyst that was treated successfully by laparoscopicSpleenectomy
Key WordsSpleen, Laparoscopic Spleenectomy
IntroductionSpleen is the largest reticuloendothelial organ in the
body consisting of an encapsulated mass of vascular andlymphoid tissue and responsible for defensive actions andhence the name defense organ for it. Like any other organin the body it is also afflicted by a number of disordersamong which are splenic cysts (1). Herein we report acase of large primary splenic cyst that was treatedsuccessfully by laparoscopic Spleenectomy.Case Report
A 45 years male with no previously significant medicaland/or surgical history presented with chief complaintsof pain left upper quadrant of abdomen for the last 3years. It was deep dull aching in type and used to turn toa dragging type of sensation on prolonged standing. Therewas no history of trauma, fever, constipation, hematuriaor dysuria. The patient was evaluated clinically and thedata analyzed. His general physical examination wasunremarkable, per abdomen examination revealed asmooth shaped mass in left hypochondrium, moving withrespiration with inability to pass fingers between it andthe costal margin.
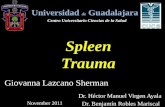
His blood counts, kidney function tests, serumelectrolytes, peripheral blood films were within normallimits.Chest radiograph depicted slight tenting of lefthemidiaphragm, abdomen radiograph was normal.ECGrevealed sinus rhythm.Ultrasound abdomen: - revealed alarge splenic cyst 15.3X12 cms with a volume of 438ml,
homogenous , filled with fluid and absence of anyclacifications or septations (Fig 1). CECT abdomenrevealed a large splenic cyst occupying most of the organ,water density and absent clacifications or septations (Fig2).Hydatid serology: - was negative.From all of the abovedata diagnosis of primary splenic cyst was made and thepatient offered laparoscopic Spleenectomy after he andhis attendants were fully explained about the nature oflaparoscopic surgery and a possibility of conversion toopen in case it could not be completed laparoscopicallyand written consent was taken from the patient beforesurgery . The patient was initially positioned supine forintravenous access, the induction of general anesthesia,endotracheal intubation, bladder catheterization, andnasogastric tube placement. The patient was thenpositioned in a modified lateral decubitus position.Approximately 30 degrees of rotation of the chest andabdomen was used. Pneumoperitoneum was establishedby closed technique using veress needle periumblicallyand insufflating to an intra-abdominal pressure of 15mmHg. The first trocar (10 mm) for the introduction ofendocamera was placed periumblically through ahorizontal skin incision. After inspection of abdominalcavity additional trocars were placed under direct vision;a 10 mm and two 5mm ports inserted in epigastrium, leftand right upper quadrants respectively. Spleen was foundto be enlarged and harbouring a very large cyst (Fig 3).

JK SCIENCE
Vol. 17 No.2, April - June 2015 www.jkscience.org 97
The splenic flexure of the colon was mobilized andretracted down and to the right and dividing the tissuesbetween the colon and spleen. The posterior dissectionof the spleen was continued by dividing the splenophrenicand splenorenal ligaments. Entry into the lesser sac wasmade by dividing the greater omentum between thestomach and spleen. Then the short gastric vessels weredivided sequentially. Then the splenic hilum was carefullydissected and the splenic artery and vein identified, doublyclipped and divided (Fig 4-6). Complete hemostasis wasensured and a tube drain kept in splenic fossa. Thespecimen was retrieved in an endobag through a 5cminguinal crease incision. The patient had an uneventfulpostoperative recovery. Nasogastric tube and Foley'scatheter were removed after 24 hours, drain on 2ndpostoperative day and the patient was discharged on 3rdpostoperative day. The patient has been asymptomaticsince then.DiscussionSplenic cysts are rare lesions. The most common etiologyfor splenic cysts worldwide is parasitic infestation,particularly echinococcal. Symptomatic parasitic cystsare best treated with splenectomy, though selected casesmay be amenable to percutaneous aspiration, instillationof protoscolicidal agent, and reaspiration. Nonparasiticcysts most commonly result from trauma and are calledpseudocysts; however, dermoid, epidermoid, and epithelialcysts have been reported as well (1). TraditionallySpleenectomy has been the treatment of choice forparasitic and symptomatic non-parasitic cysts. Spleniccysts have been classified by Martin etal. Type I cystsare true (Primary) cysts with a cellular lining of parasiticor non-parasitic origin. Type II cysts are false (secondary)cysts without a cellular lining, the most commonly foundfollowing blunt trauma to the spleen (2). The prevelanceof splenic cysts has increased recently secondary toincreased detection with CT scans and non-operativemanagement of certain types of splenic trauma. Blunttrauma to the abdomen is the commonest cause ofsecondary cyst formation, responsible for 75% of
Fig 1 &2. USG & CECT Abdomen Showing a Large Splenic Cyst
secondary splenic cysts (3). Splenic cysts may remainasymptomatic in 30 - 60% of patients (4). Indications foroperative intervention include cysts with a diameter >5cmand those which are symptomatic. Cysts with a diameterof >5cms are more likely to rupture resulting in lifethreatening hemorrhage (5).Traditionally Spleenectomyhas been the treatment of choice for splenic cysts (6). Itcan be done both open as well laparoscopically.Laparoscopic Spleenectomy is preferred over open asthe latter offers all advantages of minimal accesssurgery (7).Conclusion
Laparoscopic Spleenectomy is a safe and effectiveprocedure and offers all advantages of minimal accesssurgery.
References
1. Charles Brunicardi F. Schwartz's principles of surgery. 2005;8th edition Pages 1297-1315.
2. Martin JW. Congenital splenic cysts. Am J Surg 1958;96:302-08
3. Wu H, Kortbeek J. Management of splenic pseudocystsfollowing trauma: A retrospective case series. Am J Surg2006;5:631-14
4. Labruzzo C, Haritopoulos KN, Tayar AR, Hakim NS.Posttraumatic cysts of spleen: A case report and review ofliterature. Intl Surg 2002; 82:152-56
5. Geraghty M, Khan IZ, Conion KC. Large primary spleniccyst: A laparoscopic technique. J Min Access Surg 2009;5:14-16
6. Simmons TC. Traumatic Pseudocyst of the spleen. J NatlMed Assoc 1990; 82:727-29
7. Glasgow RE, Yee LF, Muhilvill SJ. LaparoscopicSpleenectomy. The emerging standard. Surg Endosc 1997;11:108
Fig 4-6. Intraoprative Pictuers of Laproscopic Spleenectomy