Case Report Imaging Manifestations of a Subependymal Giant...
6
Case Report Imaging Manifestations of a Subependymal Giant Cell Astrocytoma in Tuberous Sclerosis Joseph R. Stein and Daniel A. Reidman e Regional Medical Center, 3000 St. Matthews Road, Orangeburg, SC 29118, USA Correspondence should be addressed to Joseph R. Stein; [email protected] Received 22 September 2015; Revised 31 December 2015; Accepted 3 January 2016 Academic Editor: Amit Agrawal Copyright © 2016 J. R. Stein and D. A. Reidman. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Tuberous sclerosis is a rare genetic disorder resulting in benign tumor growth in various organs including the brain, heart, skin, eyes, kidney, and lung as well as systemic manifestations including seizures, cognitive impairment, and dermatologic abnormalities. is report shows the radiological findings and differentiation between a subependymal nodule and subependymal giant cell astrocytoma in a patient with tuberous sclerosis presenting with new onset seizures. 1. Introduction Tuberous sclerosis complex (TSC) is an autosomal dominant genetic disorder resulting from mutations in the TSC1 gene or the TSC2 gene [1]. e disease is characterized by benign hamartoma development in several organs, including the brain, heart, skin, eyes, kidney, lung, and liver. e disease has an estimated prevalence between 1/6800 and 1/15000 [2– 4]. Clinical manifestations of TSC seem to have an age-related expression pattern, as some manifestations are typically iden- tifiable at birth while others develop later at different ages. Some patients may have a milder form of the disease and can remain undiagnosed while others can be debilitated by the disease from birth. Since the diagnosis of TS cannot be made based on a single clinical manifestation, careful attention to physical exam findings and radiologic abnormalities is vital for correct diagnosis. In this presentation, clinical and radio- logical findings of subependymal giant cell astrocytoma and cortical tubers leading to new onset seizures will be discussed. 2. Case Summary A 26-year-old female with history of hypertension and dialysis-dependent ESRD with a GFR of 5 was admitted aſter having a seizure at work. Significant family history includes a father with tuberous sclerosis and brother with tuberous sclerosis and seizures. e patient stated she was at work the night before admission when she “felt hot” and started “shaking.” She described 1-2-second duration and serial, generalized myoclonic twitching lasting roughly 5 minutes prior to reported loss of consciousness. During EMS stabilization and transfer another generalized tonic-clonic convulsion occurred accompanied by postictal lethargy and confusion. e patient denied any prior history of seizures, cognitive impairment, or frequent headaches. On examination vital signs revealed the patient to be tachycardic (164 beats per minute) and hypertensive (249 mmHg/153 mmHg). Neurological examination was nor- mal. Several facial and body hyperpigmented fibrous plaques and a posterior lumbar Shagreen patch were noted. 3. Imaging Findings A nonenhanced head computed tomography was performed to exclude ischemia or hemorrhage. is revealed a rounded, heterogeneous, soſt tissue mass with central calcifications opposing the ependymal surface in the ventral body of the right lateral ventricle measuring approximately 12 mm × 18 m. No accompanying hydrocephalus or local neoplastic extension was evident. Subsequent contrast enhanced brain MRI demonstrated a 23 mm × 23 mm × 18 mm round, well-circumscribed mass in the right lateral ventricle and roof of the third ventricle. e mass was heterogeneous with several internal signal Hindawi Publishing Corporation Case Reports in Radiology Volume 2016, Article ID 3750450, 5 pages http://dx.doi.org/10.1155/2016/3750450
Transcript of Case Report Imaging Manifestations of a Subependymal Giant...

Case ReportImaging Manifestations of a Subependymal Giant CellAstrocytoma in Tuberous Sclerosis
Joseph R. Stein and Daniel A. Reidman
The Regional Medical Center, 3000 St. Matthews Road, Orangeburg, SC 29118, USA
Correspondence should be addressed to Joseph R. Stein; [email protected]
Received 22 September 2015; Revised 31 December 2015; Accepted 3 January 2016
Academic Editor: Amit Agrawal
Copyright © 2016 J. R. Stein and D. A. Reidman.This is an open access article distributed under theCreativeCommonsAttributionLicense, which permits unrestricted use, distribution, and reproduction in anymedium, provided the originalwork is properly cited.
Tuberous sclerosis is a rare genetic disorder resulting in benign tumor growth in various organs including the brain, heart, skin,eyes, kidney, and lung as well as systemicmanifestations including seizures, cognitive impairment, and dermatologic abnormalities.This report shows the radiological findings and differentiation between a subependymal nodule and subependymal giant cellastrocytoma in a patient with tuberous sclerosis presenting with new onset seizures.
1. Introduction
Tuberous sclerosis complex (TSC) is an autosomal dominantgenetic disorder resulting from mutations in the TSC1 geneor the TSC2 gene [1]. The disease is characterized by benignhamartoma development in several organs, including thebrain, heart, skin, eyes, kidney, lung, and liver. The diseasehas an estimated prevalence between 1/6800 and 1/15000 [2–4]. Clinicalmanifestations of TSC seem to have an age-relatedexpression pattern, as somemanifestations are typically iden-tifiable at birth while others develop later at different ages.Some patients may have a milder form of the disease and canremain undiagnosed while others can be debilitated by thedisease from birth. Since the diagnosis of TS cannot be madebased on a single clinical manifestation, careful attention tophysical exam findings and radiologic abnormalities is vitalfor correct diagnosis. In this presentation, clinical and radio-logical findings of subependymal giant cell astrocytoma andcortical tubers leading to newonset seizureswill be discussed.
2. Case Summary
A 26-year-old female with history of hypertension anddialysis-dependent ESRD with a GFR of 5 was admittedafter having a seizure at work. Significant family historyincludes a father with tuberous sclerosis and brother withtuberous sclerosis and seizures. The patient stated she was
at work the night before admission when she “felt hot”and started “shaking.” She described 1-2-second durationand serial, generalized myoclonic twitching lasting roughly 5minutes prior to reported loss of consciousness. During EMSstabilization and transfer another generalized tonic-clonicconvulsion occurred accompanied by postictal lethargy andconfusion. The patient denied any prior history of seizures,cognitive impairment, or frequent headaches.
On examination vital signs revealed the patient tobe tachycardic (164 beats per minute) and hypertensive(249mmHg/153mmHg). Neurological examination was nor-mal. Several facial and body hyperpigmented fibrous plaquesand a posterior lumbar Shagreen patch were noted.
3. Imaging Findings
A nonenhanced head computed tomography was performedto exclude ischemia or hemorrhage.This revealed a rounded,heterogeneous, soft tissue mass with central calcificationsopposing the ependymal surface in the ventral body of theright lateral ventricle measuring approximately 12mm ×18m. No accompanying hydrocephalus or local neoplasticextension was evident.
Subsequent contrast enhanced brain MRI demonstrateda 23mm × 23mm × 18mm round, well-circumscribed massin the right lateral ventricle and roof of the third ventricle.The mass was heterogeneous with several internal signal
Hindawi Publishing CorporationCase Reports in RadiologyVolume 2016, Article ID 3750450, 5 pageshttp://dx.doi.org/10.1155/2016/3750450

2 Case Reports in Radiology
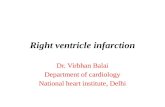
(a) (b)
Figure 1: Axial noncontrast CT demonstrating a 12 × 18mm partially calcified, enhancing soft tissue mass in the anterior body of the rightlateral ventricle (a). Axial CT with contrast showing SEGA enhancement but no enhancement of tubers (b).
voids. There was mild mass effect (4mm septum pellucidumleftward shift), with adjacent white matter mild edema andgliosis. Scattered cortical based T2 and FLAIR hyperin-tensities were seen throughout both cerebral hemispheres,suggestive of cortical tubers.
Prior renal ultrasound and abdominal CT were obtainedwhich demonstrated chronic cystic renal atrophy/chronicmedical renal disease (Figures 4 and 5).
4. Discussion
The majority of TSC patients present with neurologicsymptoms, with approximately 90% of affected individualsexperiencing seizures and roughly half experiencing cog-nitive impairment, autism, or other behavioral disorders[5]. Epilepsy is seen in 70% to 90% of patients, mostcommonly presenting in the first year of life [6]. Autismspectrum disorder, intellectual disability, and other neurode-velopmental and psychiatric disorders associated with TSCalso lead to a significant disability. Renal manifestations arethe second most common finding associated with TS, withangiomyolipomas (AMLs) occurring in 80% and renal cysticdisease in 50% of the patients [7]. Pulmonary involvement,specifically lymphangioleiomyomatosis (LAM), is the thirdmost common cause of TSC associated morbidity, occurringin approximately 35% of reproductive age female TS patients[8, 9]. Cardiac rhabdomyoma can be found in 50%–65% ofpatients with TS [10]. Other features of TS include retinalnodular hamartomas, dental pits, gingival fibromas, rectalpolyps, and bone cysts.
The main structural brain lesions include cortical tubers,subependymal nodules (SENs), and subependymal giantcell astrocytomas (SEGAs) [1, 5]. Cortical tubers developprenatally and are seen in 90% of patients (Figure 1) [11].Cortical tubers are a collection of giant cells, dysmorphic
neurons, and gliosis that destroy the normal six-layer corticalstructure [11]. There is a positive correlation between thenumber of cortical tubers and cognitive impairment andseizure control difficulty [12]. Magnetic resonance is themodality of choice for detecting cortical tubers. Increasedsignal intensity on T2-weighted images and decreased signalintensity on T1-weighted ones are demonstrated in almost allpatients with the exception being infants and neonates whereT1-weighted images show enhancement due to the similarrelaxation time of T1 and the unmyelinated brain [13]. Only10% of cortical tubers will be enhanced after administrationof contrast material [13]. The patient in this case showed thetypical findings of T2 and FLAIR hyperintensities in multipleareas suggesting cortical tubers, the likely etiology of herseizures (Figures 2 and 3).
Subependymal nodules are collections of abnormal,swollen glial cells and giant cells which cannot be differ-entiated as normal neural tissue. They have a tendencyto calcify and can progress into subependymal giant cellastrocytomas, which are histologically indistinguishable fromSENs but distinguishable based on their larger size, highergrowth rate, and potential for mass effect compared to therelatively static course of SENs [14, 15]. The radiographicappearance of SENs on unenhanced CT will show smallcalcified foci along the wall of the lateral and third ventricle[13] (Figure 1). MR imaging will demonstrate hyperintensityon T1-weighted imaging and isointense or hyperintense T2signal [13]. This variability is likely due to the extent ofcalcifications. SEGAs are slow growing tumors and mostcommonlymanifest in the first two decades of life. Occurringin 1.7–26% of patients with TS, they consist of proliferativeastrocytes and giant cells [11]. The most common locationof SEGAs is the foramen of Monroe, leading to obstructivehydrocephalus and manifesting with signs and symptoms ofincreased intracranial pressure, but most are asymptomatic.

Case Reports in Radiology 3
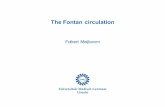
(a) (b)
Figure 2: T2 weighted coronal (a) and axial (b) MRI showing 23 × 23 × 18m lobulated mass in the right lateral ventricle and roof of the thirdventricle which is isointense to grey matter and has small signal voids in keeping with calcifications.
(a) (b)
Figure 3: T2 FLAIR axial MRI showing subcortical areas of mixed signal mass in the right occipital cortex (a) and left frontal cortex (b),suggestive of cortical tubers.
Intermediate cells have been identified in SENs and SEGAssuggesting that SENs can transform into SEGAs [16]. Serialimaging can monitor growth of subependymal nodules andpotential for transformation into SEGAs [16]. Compared toSENs, SEGAs demonstrate more intense enhancement onCT and are larger tumors (>1 cm) [17] (Figure 1). Suspicionfor transformation should be considered if lesions measure5mm or greater in diameter, are incompletely calcified, anddemonstrate enhancement [18]. There is also a reportedincreased frequency of malignant transformation in massesapproximating the foramen of Monroe [18]. SEGAs show
heterogenous enhancement on MR imaging, demonstrat-ing T1 isointense and hypointense signal and T2/FLAIRisointense and hyperintense signal [19] (Figures 2 and 3).The imaging findings of this patient are suggestive of asubependymal giant cell astrocytoma versus a subependymalnodule based on its incomplete calcification, enhancementwith gadolinium, and size (>1 cm). Surgical resection remainsthe recommended treatment for symptomatic SEGAs [20].Surgery also remains the standard treatment for SEGAsdemonstrating serial growth on neuroimaging, but expertsindicate that some patients may benefit more from medical

4 Case Reports in Radiology
Figure 4: Renal US long R kidney demonstrating atrophy and cysts.
Figure 5: CT abdomen chronic cystic renal atrophy/chronic medical renal disease.
treatment depending on the size of the lesion [20]. Ourpatient’s SEGA warranted neurosurgical consult given theabove noted findings.
Generally speaking, tumors greater than 3 cm carry sig-nificant risk for complications and should be medically man-aged. Surgical intervention of SEGA > 3 cm carries a 67% riskof surgery-related complications and surgery on tumors >4 cm was associated with a 73% risk of complications [21, 22].Bilateral SEGAs, regardless their size, were associated with67% risk of complications after surgery. No complicationswere observed in patients undergoing surgery for SEGAs <2 cm. The 23mm SEGA in our patient would likely benefitfrom surgical intervention and accordingly a neurosurgicalconsult was recommended. In the event in which surgicalintervention is declined, serial monitoring of tumor growthin this patient would be based on clinical judgment. It isrecommended that SEGAs are monitored serially with MRIevery 1–3 years in patients younger than 25 as these tumorsusually grow in children and adolescents but do not have atendency to grow in adulthood [21, 22].
5. Conclusion
This case of a new onset seizure illustrated CNS manifesta-tions of tuberous sclerosis. The patient presented with a newonset seizure and was found to have multiple cortical tubersand subependymal giant cell astrocytoma on brain imaging.The cortical tubers were the likely etiology of her seizureand the patient was placed on Keppra but more concerningwas the astrocytoma mass in the body of the right lateralventricle. The proximity to the right foramen of Monroe,its incomplete calcification, enhancement on MRI, and largesize (>1 cm)make SEGA the likely diagnosis. A neurosurgeryconsult was recommended off-site, but surgery was not per-formed because of the patient’s comorbidities and symptomsattributed to cortical tubers rather than symptomatic SEGA.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.

Case Reports in Radiology 5
References
[1] P. Curatolo, R. Bombardieri, and S. Jozwiak, “Tuberous sclero-sis,”The Lancet, vol. 372, no. 9639, pp. 657–668, 2008.
[2] J. R. Sampson, S. J. Scahill, J. B. P. Stephenson, L. Mann, and J.M. Connor, “Genetic aspects of tuberous sclerosis in the west ofScotland,” Journal of Medical Genetics, vol. 26, no. 1, pp. 28–31,1989.
[3] F. J. K. O’Callaghan, A. W. Shiell, J. P. Osborne, and C. N.Martyn, “Prevalence of tuberous sclerosis estimated by capture-recapture analysis,”The Lancet, vol. 351, no. 9114, p. 1490, 1998.
[4] J. R. W. Yates, “Tuberous sclerosis,” European Journal of HumanGenetics, vol. 14, no. 10, pp. 1065–1073, 2006.
[5] P. Curatolo and B. L. Maria, “Tuberous sclerosis,” in Handbookof Clinical Neurology, vol. 111, chapter 38, pp. 323–331, Elsevier,2013.
[6] C. J. Chu-Shore, P.Major, S. Camposano,D.Muzykewicz, and E.A. Thiele, “The natural history of epilepsy in tuberous sclerosiscomplex,” Epilepsia, vol. 51, no. 7, pp. 1236–1241, 2010.
[7] P. Prather and P. J. de Vries, “Behavioral and cognitive aspectsof tuberous sclerosis complex,” Journal of Child Neurology, vol.19, no. 9, pp. 666–674, 2004.
[8] D. N. Franz, J. J. Bissler, and F. X. McCormack, “Tuberoussclerosis complex: neurological, renal and pulmonary manifes-tations,” Neuropediatrics, vol. 41, no. 5, pp. 199–208, 2010.
[9] C. J. Cudzilo, R. D. Szczesniak, A. S. Brody et al., “Lymphangi-oleiomyomatosis screening in women with tuberous sclerosis,”Chest, vol. 144, no. 2, pp. 578–585, 2013.
[10] E. G. Muhler, V. Turniski-Harder, W. Engelhardt, and G. vonBernuth, “Cardiac involvement in tuberous sclerosis,” BritishHeart Journal, vol. 72, no. 6, pp. 584–590, 1994.
[11] P. Van Tassel, J. K. Cure, and K. R. Holden, “Cystlike whitematter lesions in tuberous sclerosis,” American Journal ofNeuroradiology, vol. 18, no. 7, pp. 1367–1373, 1997.
[12] R. S. Kandt, “Tuberous sclerosis complex andneurofibromatosistype 1: the twomost common neurocutaneous diseases,”Neuro-logic Clinics, vol. 21, no. 4, pp. 983–1004, 2003.
[13] J. C. Evans and J. Curtis, “The radiological appearances of tuber-ous sclerosis,” British Journal of Radiology, vol. 73, no. 865, pp.91–98, 2000.
[14] V. Moran and F. O’Keeffe, “Giant cell astrocytoma in tuberoussclerosis: computed tomographic findings,” Clinical Radiology,vol. 37, no. 6, pp. 543–545, 1986.
[15] S. K. McMurdo Jr., S. G. Moore, M. Brant-Zawadzki et al., “MRimaging of intracranial tuberous sclerosis,” American Journal ofRoentgenology, vol. 148, pp. 791–796, 1987.
[16] K. Morimoto and H. Mogami, “Sequential CT study of sube-pendymal giant-cell astrocytoma associated with tuberous scle-rosis. Case report,” Journal of Neurosurgery, vol. 65, no. 6, pp.874–877, 1986.
[17] A. Nezu, K. Uetake, Y. Nomura, and M. Segawa, “Roles of asubependymal nodule of tuberous sclerosis on pathophysiologyof epilepsy,” Japanese Journal of Psychiatry and Neurology, vol.45, no. 2, pp. 372–377, 1991.
[18] H.-D. Rott, B. Lemcke, M. Zenker, W. Huk, J. Horst, and K.Mayer, “Cyst-like cerebral lesions in tuberous sclerosis,” Ameri-can Journal ofMedical Genetics, vol. 111, no. 4, pp. 435–439, 2002.
[19] Y. Baron and A. J. Barkovich, “MR imaging of tuberous sclero-sis in neonates and young infants,” American Journal of Neuro-radiology, vol. 20, no. 5, pp. 907–916, 1999.
[20] M. Berhouma, “Management of subependymal giant celltumors in tuberous sclerosis complex: the neurosurgeon’s per-spective,” World Journal of Pediatrics, vol. 6, no. 2, pp. 103–110,2010.
[21] K. Kotulska, J. Borkowska, M. Roszkowski et al., “Surgicaltreatment of subependymal giant cell astrocytoma in tuberoussclerosis complex patients,” Pediatric Neurology, vol. 50, no. 4,pp. 307–312, 2014.
[22] J. Roth, E. S. Roach, U. Bartels et al., “Subependymal giant cellastrocytoma: diagnosis, screening, and treatment. Recommen-dations from the International Tuberous sclerosis ComplexConsensus Conference 2012,” Pediatric Neurology, vol. 49, no.6, pp. 439–444, 2013.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com