
Case Report Esophageal Perforation with Unilateral...
3
Case Report Esophageal Perforation with Unilateral Fluidothorax Caused by Nasogastric Tube Lukas P. Mileder, 1 Martin Müller, 1 Friedrich Reiterer, 1 Alexander Pilhatsch, 2 Barbara Gürtl-Lackner, 3,4 Berndt Urlesberger, 1 and Wolfgang Raith 1 1 Division of Neonatology, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria 2 Division of Pediatric Radiology, Department of Radiology, Medical University of Graz, Graz, Austria 3 Institute of Pathology, Medical University of Graz, Graz, Austria 4 Department of Pathology, Sk˚ ane Regional and University Laboratories, Lund, Sweden Correspondence should be addressed to Lukas P. Mileder; [email protected] Received 29 July 2016; Accepted 24 August 2016 Academic Editor: Ian J. Griffin Copyright © 2016 Lukas P. Mileder et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Preterm infants are highly susceptible to injuries following necessary and oſten life-saving medical interventions. Esophageal perforation is a rare, yet serious complication that can be caused by aerodigestive tract suction, endotracheal intubation, or nasogastric tube placement. We present the case of a neonate born at 23 weeks plus three days of gestation with chest radiography showing malposition of the nasogastric feeding tube and massive right-sided effusion of Iopamidol in the pleural cavity due to esophageal perforation. In addition, the article summarizes common signs and symptoms associated with esophageal perforation in infants and discusses diagnostic approaches. 1. Introduction Esophageal perforation (EP) is a rare, yet serious complica- tion [1], with an incidence of 1 : 124 among preterm infants weighing less than 1500 g at birth [2]. Mortality is as high as 20% in these vulnerable patients [3]. 2. Case Presentation A female twin neonate born at 23 weeks plus three days of gestation with a birth weight of 538 g was intubated aſter birth due to respiratory distress and received surfactant repeatedly. Because of signs of evolving bronchopulmonary dysplasia and pulmonary hypertension, she was treated with hydrocortisone and nitric oxide. Transcranial sonography revealed grade II intraventricular hemorrhage. On day 8 of life, feeding problems with bilious gastric residuals, constipation, abdominal distension, and lactic acidosis developed, which were initially managed conserva- tively. Spontaneous ileum perforation necessitated laparo- scopic surgery, including local bowel resection and creation of an ileostomy, on day 12. One day aſter surgery, clinical signs suggested development of an intestinal volvulus. Aſter injec- tion of Iopamidol for evaluation of intestinal obstruction, chest radiography showed massive right-sided effusion in the pleural cavity and malposition of the nasogastric feeding tube (Figure 1). Pleural drainage resulted in prompt stabilization of vital parameters aſter extraction of 10 mL of serous liquid. Nitric oxide therapy was gradually reduced and could be abandoned on day 13. Due to numerous morbidities including intraventricu- lar hemorrhage and arterial hypotension despite inotropic support, the neonate died on day 20. Autopsy showed regular esophageal development with minimal inflammatory reac- tion below the muscular layer and found lung immaturity to be the cause of death. 3. Discussion Iatrogenic EP can be caused by vigorous pharyngoesophageal suction, traumatic endotracheal intubation, and insertion of Hindawi Publishing Corporation Case Reports in Pediatrics Volume 2016, Article ID 4103734, 2 pages http://dx.doi.org/10.1155/2016/4103734
Transcript of Case Report Esophageal Perforation with Unilateral...

Case ReportEsophageal Perforation with UnilateralFluidothorax Caused by Nasogastric Tube
Lukas P. Mileder,1 Martin Müller,1 Friedrich Reiterer,1 Alexander Pilhatsch,2
Barbara Gürtl-Lackner,3,4 Berndt Urlesberger,1 and Wolfgang Raith1
1Division of Neonatology, Department of Pediatrics and Adolescent Medicine, Medical University of Graz, Graz, Austria2Division of Pediatric Radiology, Department of Radiology, Medical University of Graz, Graz, Austria3Institute of Pathology, Medical University of Graz, Graz, Austria4Department of Pathology, Skane Regional and University Laboratories, Lund, Sweden
Correspondence should be addressed to Lukas P. Mileder; [email protected]
Received 29 July 2016; Accepted 24 August 2016
Academic Editor: Ian J. Griffin
Copyright © 2016 Lukas P. Mileder et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Preterm infants are highly susceptible to injuries following necessary and often life-saving medical interventions. Esophagealperforation is a rare, yet serious complication that can be caused by aerodigestive tract suction, endotracheal intubation, ornasogastric tube placement. We present the case of a neonate born at 23 weeks plus three days of gestation with chest radiographyshowing malposition of the nasogastric feeding tube and massive right-sided effusion of Iopamidol in the pleural cavity due toesophageal perforation. In addition, the article summarizes common signs and symptoms associated with esophageal perforationin infants and discusses diagnostic approaches.
1. Introduction
Esophageal perforation (EP) is a rare, yet serious complica-tion [1], with an incidence of 1 : 124 among preterm infantsweighing less than 1500 g at birth [2]. Mortality is as high as20% in these vulnerable patients [3].
2. Case Presentation
A female twin neonate born at 23 weeks plus three days ofgestation with a birth weight of 538 g was intubated afterbirth due to respiratory distress and received surfactantrepeatedly. Because of signs of evolving bronchopulmonarydysplasia and pulmonary hypertension, she was treated withhydrocortisone and nitric oxide. Transcranial sonographyrevealed grade II intraventricular hemorrhage.
On day 8 of life, feeding problems with bilious gastricresiduals, constipation, abdominal distension, and lacticacidosis developed, which were initially managed conserva-tively. Spontaneous ileum perforation necessitated laparo-scopic surgery, including local bowel resection and creation
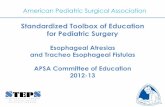
of an ileostomy, on day 12. One day after surgery, clinical signssuggested development of an intestinal volvulus. After injec-tion of Iopamidol for evaluation of intestinal obstruction,chest radiography showedmassive right-sided effusion in thepleural cavity andmalposition of the nasogastric feeding tube(Figure 1). Pleural drainage resulted in prompt stabilizationof vital parameters after extraction of 10mL of serous liquid.Nitric oxide therapy was gradually reduced and could beabandoned on day 13.
Due to numerous morbidities including intraventricu-lar hemorrhage and arterial hypotension despite inotropicsupport, the neonate died on day 20. Autopsy showed regularesophageal development with minimal inflammatory reac-tion below the muscular layer and found lung immaturity tobe the cause of death.
3. Discussion
Iatrogenic EP can be caused by vigorous pharyngoesophagealsuction, traumatic endotracheal intubation, and insertion of
Hindawi Publishing CorporationCase Reports in PediatricsVolume 2016, Article ID 4103734, 2 pageshttp://dx.doi.org/10.1155/2016/4103734

2 Case Reports in Pediatrics
Figure 1: Chest radiograph after contrast agent application showingmassive effusion in the pleural cavity and abnormal right-sidedposition of the nasogastric tube.
naso-/orogastric feeding tubes [4]. Clinical signs and symp-toms of EP include inability to pass a gastric tube, feeding dif-ficulties, bloody oral secretions, fever, cyanosis, and subcuta-neous emphysema [4, 5]. In our case, EP did not present withsudden respiratory deterioration, which is the most commonsymptom [1]. Apparently, there is a wide spectrum of theclinical presentation of EP especially in extremely preterminfants, including malposition of the nasogastric feedingtube.
Diagnosis of EP is based on clinical findings, chestradiography, and endoscopy [3]. Radiographic evidence ofEP includes pneumothorax, pneumomediastinum, or subcu-taneous air [4], with proximal EP usually causing left-sidedabnormalities and distal perforations commonly appearingon the right side [6]. Flexible endoscopy has been shownto allow for diagnosis and precise location of EP at thebedside while avoiding contrast use and radiation exposure[7] and should therefore be considered as diagnostic measureespecially in preterm infants with clinical signs of EP.
Competing Interests
The authors declare that there is no conflict of interestregarding the publication of this paper.
Authors’ Contributions
Friedrich Reiterer, Wolfgang Raith, Martin Muller, BerndtUrlesberger, and Alexander Pilhatsch were involved in clin-ical management of the patient. Barbara Gurtl-Lackner per-formed postmortem autopsy. Lukas P. Mileder andWolfgangRaith acquired patient consent. Lukas P. Mileder and MartinMuller drafted the manuscript. All authors critically revisedit for important intellectual content and approved the finalversion before submission.
References
[1] P. S. Shah,M. S. Dunn, andV. S. Shah, “Oesophageal perforationin preterm neonates: not an innocent bystander,” Journal ofPaediatrics and Child Health, vol. 39, no. 9, pp. 697–699, 2003.
[2] L. Filippi, M. Pezzati, and C. Poggi, “Use of polyvinyl feed-ing tubes and iatrogenic pharyngo-oesophageal perforation invery-low-birthweight infants,” Acta Paediatrica, vol. 94, no. 12,pp. 1825–1828, 2005.
[3] E. Sapin, L. Gumpert, A. Bonnard et al., “Iatrogenic pharyngoe-sophageal perforation in premature infants,” European Journalof Pediatric Surgery, vol. 10, no. 2, pp. 83–87, 2000.
[4] N. Sudhakaran and C. P. Kirby, “Pitfalls of gastric intubation inpremature infants,” Journal of Paediatrics and Child Health, vol.37, no. 2, pp. 195–197, 2001.
[5] S. A. Engum, J. L. Grosfeld, K. W. West, F. J. Rescorla, L. R.Scherer, and W. G. Vaughan, “Improved survival in childrenwith esophageal perforation,” Archives of Surgery, vol. 131, no.6, pp. 604–611, 1996.
[6] E. Panieri, A. J. W. Millar, H. Rode, R. A. Brown, and S.Cywes, “Iatrogenic esophageal perforation in children: patternsof injury, presentation, management, and outcome,” Journal ofPediatric Surgery, vol. 31, no. 7, pp. 890–895, 1996.
[7] W.-J. Soong, “Endoscopic diagnosis and management of iatro-genic cervical esophageal perforation in extremely prematureinfants,” Journal of the Chinese Medical Association, vol. 70, no.4, pp. 171–175, 2007.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com
![Mediastinal abscess complicating esophageal dilatation: a ...frequently isolated from cases of acute mediastinitis secondary to esophageal perforation [6], and that was clearly demonstrated](https://static.fdocuments.net/doc/165x107/60a2b0eeeed65f4a956146e0/mediastinal-abscess-complicating-esophageal-dilatation-a-frequently-isolated.jpg)
















