Case Report: Dental science “Case Report of a compound ...ijhbr.com/pdf/325-330.pdf · Case...
6
International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330 325 www.ijhbr.com Case Report: Dental science “Case Report of a compound composite odontome with an impacted maxillary canine” 1 Dr. Deepa Das , 2 Dr. Gopal Sharma, 3 Dr. Jaya Mukherjee , 4 Dr. Bhagyashri Purandare 1 Associate Professor, Dept of Oral medicine and Radiology, YMT Dental College and Hospital 2 Head of Department, Oral Medicine and Radiology, YMT Dental College and Hospital 3 Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental College and Hospital 4 Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental College and Hospital Institute: YMT Dental College and Hospital, kharghar, Navi Mumbai, Maharashtra, India Corresponding author: Dr Jaya Mukherjee , Email id :[email protected] ABSTRACT: Odontomas are the most common type of odontogenic tumours and are generally asymptomatic. Frequently they interfere with the eruption of the teeth. This is the case report of a compound composite odontoma in a 15 years old girl, which resulted in failure of eruption of the permanent maxillary left canine while the contra lateral tooth had erupted. A calcified mass was seen in the radiograph and was provisionally diagnosed as a compound composite odontoma following which the odontoma was enucleated along with disimpaction of the left maxillary canine. Keywords: odontomas, calcified, disimpaction, enucleation INTRODUCTION Odontomas are the most common of odontogenic tumors of the jaws. They are mixed tumors, consisting of both epithelial and mesenchymal cells, that present a complete dental tissue differentiation (enamel, dentin, cementum, and pulp). 1,2 These tumours are basically formed of enamel and dentin but they can also have variable amounts of cementum and pulp tissue. It was in 1867 that Paul Broca first used the term “Odontoma.” Broca defined the term as “tumors formed by the overgrowth of transitory or complete dental tissues”. 3 Odontomas are further sub- classified based upon their gross and radiographic features into compound (small tooth like structures) or complex (a conglomeration of dentin, enamel and cementum) 4 . In 1974, Shafer, Hine and Levy described odontomes as tumors of odontogenic origin but their current views support that an odontome is now widely accepted by most authorities as a hamartoma. 5 CASE PRESENTATION A 15 years old female patient reported to the Department of Oral Medicine and Radiology, YMT Dental College and Hospital, Kharghar with a chief complaint of unerupted upper left front tooth, while the contra lateral tooth had already erupted. Medical and family histories were non- contributory. No history of trauma to the face or mouth was reported. Clinical examination revealed no facial asymmetry extra orally on inspection. On palpation, there was no swelling or tenderness present. Intraorally, unerupted 23 without any swelling or inflammation of the overlying mucosa was noticed (Fig. 1&2).On palpation intra orally, slight tenderness was reported by the patient in the upper left vestibule above the missing tooth (23).
Transcript of Case Report: Dental science “Case Report of a compound ...ijhbr.com/pdf/325-330.pdf · Case...

International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
325
www.ijhbr.com
Case Report: Dental science
“Case Report of a compound composite odontome with an impacted maxillary canine” 1Dr. Deepa Das , 2Dr. Gopal Sharma, 3Dr. Jaya Mukherjee , 4Dr. Bhagyashri Purandare
1Associate Professor, Dept of Oral medicine and Radiology, YMT Dental College and Hospital 2 Head of Department, Oral Medicine and Radiology, YMT Dental College and Hospital 3Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental College and Hospital 4Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental College and Hospital
Institute: YMT Dental College and Hospital, kharghar, Navi Mumbai, Maharashtra, India
Corresponding author: Dr Jaya Mukherjee , Email id :[email protected]
ABSTRACT:
Odontomas are the most common type of odontogenic tumours and are generally asymptomatic. Frequently they interfere
with the eruption of the teeth. This is the case report of a compound composite odontoma in a 15 years old girl, which
resulted in failure of eruption of the permanent maxillary left canine while the contra lateral tooth had erupted. A calcified
mass was seen in the radiograph and was provisionally diagnosed as a compound composite odontoma following which the
odontoma was enucleated along with disimpaction of the left maxillary canine.
Keywords: odontomas, calcified, disimpaction, enucleation
INTRODUCTION
Odontomas are the most common of odontogenic
tumors of the jaws. They are mixed tumors,
consisting of both epithelial and mesenchymal
cells, that present a complete dental tissue
differentiation (enamel, dentin, cementum, and
pulp).1,2
These tumours are basically formed of
enamel and dentin but they can also have variable
amounts of cementum and pulp tissue. It was in
1867 that Paul Broca first used the term
“Odontoma.” Broca defined the term as “tumors
formed by the overgrowth of transitory or complete
dental tissues”. 3Odontomas are further sub-
classified based upon their gross and radiographic
features into compound (small tooth like structures)
or complex (a conglomeration of dentin, enamel
and cementum)4.In 1974, Shafer, Hine and Levy
described odontomes as tumors of odontogenic
origin but their current views support that an
odontome is now widely accepted by most
authorities as a hamartoma.5
CASE PRESENTATION
A 15 years old female patient reported to the
Department of Oral Medicine and Radiology, YMT
Dental College and Hospital, Kharghar with a chief
complaint of unerupted upper left front tooth, while
the contra lateral tooth had already erupted.
Medical and family histories were non-
contributory. No history of trauma to the face or
mouth was reported. Clinical examination revealed
no facial asymmetry extra orally on inspection. On
palpation, there was no swelling or tenderness
present. Intraorally, unerupted 23 without any
swelling or inflammation of the overlying mucosa
was noticed (Fig. 1&2).On palpation intra orally,
slight tenderness was reported by the patient in the
upper left vestibule above the missing tooth (23).

International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
326
www.ijhbr.com
Figure 1 Figure2
INVESTIGATIONS
The intraoral periapical (Fig. 3), Occlusal (Fig 4 )
and panoramic radiographs (Fig. 5) revealed the
presence of a radiopaque mass in 23 region
obstructing its eruption. Clark’s radiographic
technique revealed the presence of two radiopaque
masses ,one in the palatal region (impacted upper
left maxillary canine ) of the upper left central and
lateral incisors and the other (calcified mass)
buccal to it.
Figure 3 Figure 4 The radiograph showed the presence of impacted maxillary left canine and a radiopaque mass consisting of
tooth like structures.
Figure 5 : On the basis of clinical and radiographic findings, it was provisionally diagnosed as a compound
composite odontoma.

International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
327
www.ijhbr.com
TREATMENT
Under local anaesthesia, surgical removal was
done. A mucoperiosteal flap on the palatal surface
(Fig 6) from the right permanent central incisor to
left permanent second molar was raised. The layer
of bone overlying the palatal surface from 11 to 23
was removed and the crown of the canine was
exposed. (Fig 7).
Figure 6 Figure 7
The bone was further removed to expose the root of
the impacted canine and it was removed. (Fig 8). A
window was then created in the bone from the
labial aspect between 22 and 24 to gain access to
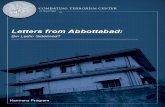
the calcified mass. (Fig 9) This mass was excised
completely and submitted for histopathological
evaluation.(Fig 10)
Figure 8 Figure 9
OUTCOME AND FOLLOW-UP :The histopathological report confirmed the specimen to be compound
composite odontoma . The patient was kept under observation and followed up for 6 months. The healing was
uneventful.
International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
328
www.ijhbr.com
Figure 10
Figure 11
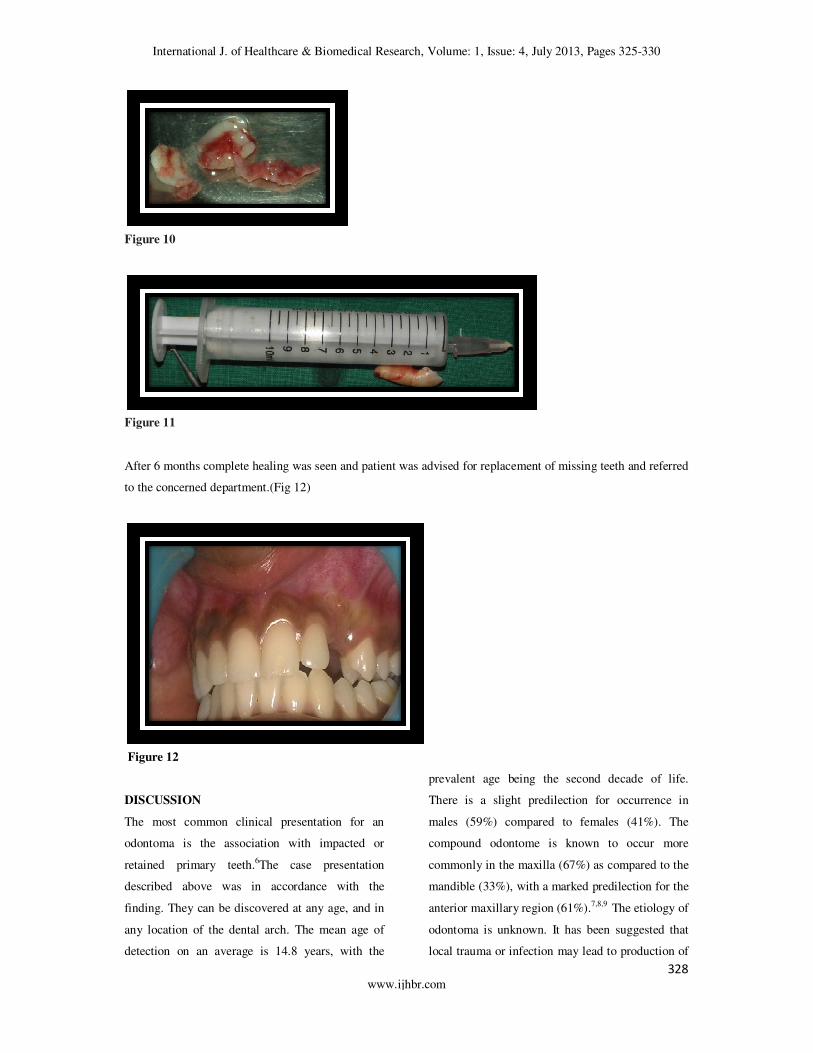
After 6 months complete healing was seen and patient was advised for replacement of missing teeth and referred
to the concerned department.(Fig 12)
Figure 12
DISCUSSION
The most common clinical presentation for an
odontoma is the association with impacted or
retained primary teeth.6The case presentation
described above was in accordance with the
finding. They can be discovered at any age, and in
any location of the dental arch. The mean age of
detection on an average is 14.8 years, with the
prevalent age being the second decade of life.
There is a slight predilection for occurrence in
males (59%) compared to females (41%). The
compound odontome is known to occur more
commonly in the maxilla (67%) as compared to the
mandible (33%), with a marked predilection for the
anterior maxillary region (61%).7,8,9
The etiology of
odontoma is unknown. It has been suggested that
local trauma or infection may lead to production of

International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
329
www.ijhbr.com
such lesion. It may also be caused due to a mutant
gene or interference or by traumatic interference.
10,11
In 1946, Thoma and Goldman gave a classification
which is as follows.
• Geminated composite odontomes: Two or
more, more or less well-developed teeth
fused together.
• Compound composite odontomes: Made
up of more or less rudimentary teeth.
• Complex composite odontomes: Calcified
structure bearing no great resemblance to
the normal anatomical arrangement of
dental tissues.
• Dilated odontomes: The crown or root part
of tooth shows marked enlargement.
• Cystic odontomes: An odontome that is
normally encapsulated by fibrous
connective tissue in a cyst or in the wall of
a cyst.
According to World Health Organization (WHO)
classification, odontomes can be divided into three
groups.
• Complex odontome: When the calcified
dental tissues are simply arranged in an
irregular mass bearing no morphologic
similarity to rudimentary teeth.
• Compound odontome: Composed of all
odontogenic tissues in an orderly pattern,
which result in many teeth-like structures,
but without morphologic resemblance to
normal teeth.
• Ameloblastic fibro-odontome: Consists of
varying amounts of calcified dental tissue
and dental papilla-like tissue, the later
component resembling an ameloblastic
fibroma. The ameloblastic fibro-odontome
is considered as an immature precursor of
complex odontoma.
A new type known as hybrid odontome is also
reported by some authors.12
The radiographic
findings of odontomas depend on their stage of
development and degree of mineralization. The
first stage is characterized by radiolucency due to
lack of calcification. Partial calcification is
observed in the intermediate stage, while in the
third stage the lesion usually appears as radiopaque
masses surrounded by radiolucent areas
corresponding to the connective tissue
histologically.13,14
Histopathologically, odontomas
are normal appearing enamel or enamel matrix,
dentin, pulp tissue and cementum, which may
exhibit a normal relation to one another.15
Compound odontomas are formed by tooth-like
structures which resemble pulp tissue in the central
portion surrounded by a dentin shell and partially
covered by enamel. Complex odontomas are
conglomerates without orientation of dentin,
enamel; enamel matrix, cementum and areas of
pulp tissue. Odontomas are treated by conservative
surgical removal and there is little probability of
recurrence. 16
Timely detection and surgical
enucleation of odontoma followed by curettage is
recommended to prevent complications such as
tooth loss, cystic changes, bone expansion and
delayed eruption of permanent teeth.17
Surgical
excision of odontoma and its surrounding soft
tissue is recommended as the treatment of choice
because of the possibility of its cystic degeneration.
The lack of recurrence indicates that conservative
excision is adequate18
REFERENCES
1. Philipsen HP, Reichart PA, Praetorius F. Mixed odontogenic tumours and odontomas. Considerations
on interrelationship. Review of the literature and presentation of 134 new cases of odontomas. Oral
Oncol. 1997;33:86–99.

International J. of Healthcare & Biomedical Research, Volume: 1, Issue: 4, July 2013, Pages 325-330
330
www.ijhbr.com
2. Amado Cuesta S, Gargallo Albiol J, Berini Aytés L, Gay Escoda C. Review of 61 cases of
odontoma.Presentation of an erupted complex odontoma. Med Oral. 2003;8:366–73.
3. Batra P, Duggal R, Kharbanda OP, Parkash H. Orthodontic treatment of impacted anterior teeth due to
odontomas: A report of two cases. J Clin Pediatr Dent. 2004;28:289–94.
4. Bordini J, Jr, Contar CM, Sarot JR, Fernandes A, Machado MA. Multiple compound odontomas in the
jaw: case report and analysis of the literature. J Oral Maxillofac Surg. 2008;66(12):2617–2620. doi:
10.1016/j.joms.2007.08.027
5. Shafer GW, Hine MK, Levy BM. A textbook of oral pathology (3rd ed). Philadelphia: WB Saunders
1974;276
6. Yassin OM . Delayed eruption of maxillary primary cuspid associated with compound odontoma . J
Clin Pediatr Dent 1999 ; 23 : 147 – 9
7. Owens BM, Sachuman NJ, Mineer H, Turner JE, Oliver FM. Dental odontomas: A retrospective study
of 104 cases. Clin Pediat Dent. 1997;21:261–4.
8. Shafer, Hine, Levy . Shafer's Textbook of Oral Pathology. In: Rajendran R, Sivapathasundharam B,
editors. Cysts and tumors of odontogenic origin. 5th ed. New Delhi: Elsevier; 2006. pp. 404–7.
9. Syed MR, Meghana SM, Ahmedmujib BR. Bilateral complex odontomas in mandible. J Oral
Maxillofac Pathol. 2006;10:89–91.
10. Levy SH. Cysts and Tumours of the Jaws. In a Textbook of Oral Pathology. 4 th ed. United States: W.
B .Saunders Company; 2003.
11. Owens HM, Schuman NJ. Dental odontomas: A retrospective study of 104 cases. Int J Clin Pediatr
Dent 1997;21:261-4.
12. Natl J Maxillofac Surg. 2010 Jul-Dec; 1(2): 157–160. Vibha Singh, Satish Dhasmana,1 Shabad
Mohammad, and Nimisha Singh
13. Tomizawa M, Otsuka Y, Noda T. Clinical observations of odontomas in Japanese children: 39 cases
including one recurrent case. Int J Paediatr Dent. 2005;15:37–43.
14. Kodali RM, Venkat Suresh B, Ramanjaneya Raju P, Vora SK. An unusual complex odontoma. J
Maxillofac Oral Surg. 2010;9:314–317.
15. . Lopez-Areal L, Silvestre Donat F, Gil Lozano J. Compound odontomas erupting in the mouth: 4-year
follow-up of a clinical case. J Oral Pathol Med 1992;21:285
16. Areal-Lopez L, Silvestre DF, Gil LJ. Compound odontoma erupting in the mouth: Four years follow-up
of a clinical case. J Oral Path 1992;21:285-88
17. John J B, John R R, Punithavathy I, Elango ICompound Odontoma Associated with Maxillary Primary
Tooth –A Case Report. Journal of Indian academy of dental specialists 2010;1:49-51
18. Kaugars GE, Miller ME, Abbey LM . Odontomas . Oral Surg Oral Med OralPathol 1989 ; 67 : 172 – 6
.
Date of submission: 30 May 2013
Date of provisional acceptance: 11 June 2013
Date of Final acceptance: 28 June 2013
Date of Publication: 03 July 2013
Source of support: Nil; Conflict of Interest: Nil