
Case Report # 733 Submitted by:James E. Dimaala, M.D. Faculty reviewer:Sandra Oldham, M.D, The...
14
Case Report # 733 Submitted by: James E. Dimaala, M.D. Faculty reviewer: Sandra Oldham, M.D, The University of Texas Medical School-Houston Date accepted: 12 January, 2011 Radiological Category: Principal Modality (1): Principal Modality (2): Thoracic Chest Radiography Computed Tomography
-
Upload
eleanore-carroll -
Category
Documents
-
view
214 -
download
0
Transcript of Case Report # 733 Submitted by:James E. Dimaala, M.D. Faculty reviewer:Sandra Oldham, M.D, The...

Case Report # 733
Submitted by: James E. Dimaala, M.D.
Faculty reviewer: Sandra Oldham, M.D, The University of Texas Medical School-Houston
Date accepted: 12 January, 2011
Radiological Category: Principal Modality (1):
Principal Modality (2):
Thoracic
Chest Radiography
Computed Tomography

Case History
HPI: 74yo white female presented to an outside hospital with sudden onset bradycardia, dizziness, chest pain and SOB after a several week history of dry cough. She was transferred to MHH at the request of the family after developing altered mental status. Review of systems was negative for sick contacts or prior history of similar symptoms.
PMH: HTN, HLD, multiple TIAs, Afib for 1.5yrs.
Meds: Plavix, Coumadin, Amiodarone, Nifedipine, Nexium, Gabapentin, Toprol
FH: Positive for CVAs and CAD.

Case History
SH: Previously held jobs include work in a rug factory and as a hospital aid. She has lived near both coal refineries and sugar factories, as well as in Pasadena. Currently works at Wal-Mart.
PE: Pertinent exam findings include bilateral diffuse lower lobe crackles and mild end expiratory wheezes. Heart rate regular without murmurs, gallops, or rubs. Extremities revealed no clubbing, cyanosis, or edema.

PA and Lateral Chest Radiographs

CT Chest without contrast, mediastinal window, coronal and axial sections

CT Chest without contrast, mediastinal window, axial section of lung bases and upper abdomen

• Iodinated Oil Embolism
• Amyloidosis
• Silicosis/Progressive Massive Fibrosis
• Amiodarone Toxicity
• Hemochromatosis
Which one of the following is your choice for the appropriate diagnosis? After your selection, go to next page.
Test Your Diagnosis

PA and Lateral Chest radiographs shows bilateral effusions.
Noncontrast CT scan shows focal areas of high attenuating alveolar consolidation containing air bronchograms in the bilateral lower lobes with associated pleural effusions. Diffuse high attenuation is also noted in the liver parenchyma.
Findings:
Differentials:
Findings and Differentials
• Iodinated Oil Embolism
• Amyloidosis
• Silicosis/Progressive Massive Fibrosis
• Amiodarone Toxicity

The differential for high attenuation consolidative opacities in the includes amyloidosis, iodinated oil embolism, occupational exposure such as silicosis/progressive massive fibrosis, and amiodarone toxicity.
Primary amyloidosis results from abnormal production and excessive deposition of amyloid light chain protein secreted by B lymphocytes and plasma cell, with pulmonary involvement occuring in up to 50% of patients1. Three pulmonary manifestations exist: tracheobronchial, nodular and diffuse parenchymal. Tracheobronchial amyloidosis manifests as focal or diffuse wall thickening. The nodular form shows solitary or multiple nodules of well-defined round or lobular margins, with approximately 50% calcified1. The diffuse parenchymal form shows interlobular septal thickening, well-defined 1-2 mm nodules, reticular opacities, and subpleural confluent consolidation1. Amyloidosis would not account for high liver attenuation on CT as seen in this patient.
Discussion
Nodular form of amyloidosis
Marchiori E, Souza A, Franquet T, Muller N. Diffuse High-Attenutation Pulmonary Abnormalities: A Pattern-Oriented Diagnostic Approach on High-Resolution CT. AJR 2005; 184:273-282

Iodinated oil embolism is seen in patients after transcatheter oil chemoembolization or lymphangiography1. Chest CT demonstrates patchy ground glass opacities with high density areas of consolidation and atelectasis1. Although, high density areas may be seen in the liver in the setting of chemoembolization, it is usually focal and would not account for the diffuse high hepatic attenuation in this patient.
Discussion
Iodinated oil embolism
Marchiori E, Souza A, Franquet T, Muller N. Diffuse High-Attenutation Pulmonary Abnormalities: A Pattern-Oriented Diagnostic Approach on High-Resolution CT. AJR 2005; 184:273-282
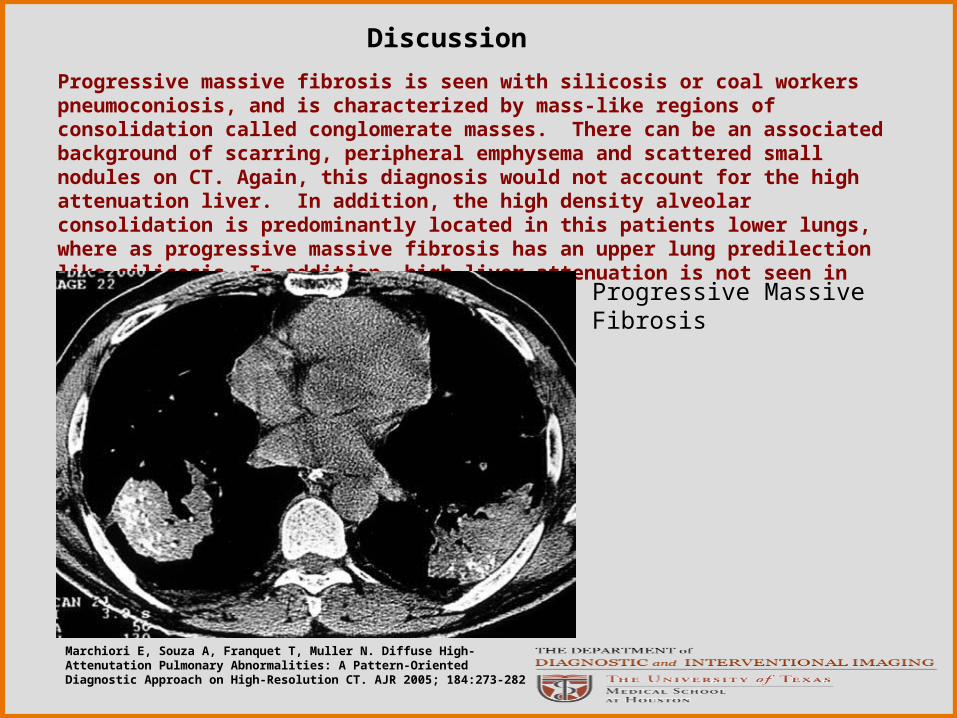
Progressive massive fibrosis is seen with silicosis or coal workers pneumoconiosis, and is characterized by mass-like regions of consolidation called conglomerate masses. There can be an associated background of scarring, peripheral emphysema and scattered small nodules on CT. Again, this diagnosis would not account for the high attenuation liver. In addition, the high density alveolar consolidation is predominantly located in this patients lower lungs, where as progressive massive fibrosis has an upper lung predilection like silicosis. In addition, high liver attenuation is not seen in progressive massive fibrosis.
Discussion
Progressive Massive Fibrosis
Marchiori E, Souza A, Franquet T, Muller N. Diffuse High-Attenutation Pulmonary Abnormalities: A Pattern-Oriented Diagnostic Approach on High-Resolution CT. AJR 2005; 184:273-282

-Amiodarone is a widely used anti-arrhythmic used to treat atrial fibrillation. The compound is acidophilic, contains three iodine moieties and is 37% iodine by weight2. The medication usually accumulates in the lung and liver, being trapped by macrophages where it interacts with phospholipids forming a drug-lipid complex; this allows for biodegradable resistance and accumulation of large amounts within these tissues2. Pulmonary toxicity occurs in 2-18% of patients3.
-The most common presentation of amiodarone toxicity is subacute pneumonia after months of beginning treatment. Symptoms include shortness of breath, non-productive cough, malaise, and fever. Pulmonary function tests demonstrate a restrictive pattern.
-No correlation exists between the development of drug toxicity and duration of therapy or total cumulative dose, however the risk is increased if the daily maintenance dose is greater than 400 mg and if the patient is elderly4. CT findings include nonspecific septal thickening and interstitial fibrosis; high-attenuation pleuroparenchymal opacities and increased liver attenuation are more characteristic of amiodarone exposure2.
-Treatment consists of withdrawal and corticosteroid treatment.
Discussion

Amiodarone Induced Pulmonary Toxicity
Diagnosis

1. Marchiori E, Souza A, Franquet T, Muller N. Diffuse High-Attenutation Pulmonary Abnormalities: A Pattern-Oriented Diagnostic Approach on High-Resolution CT. AJR 2005; 184:273-2822. Kuhlman J, Teigen C, Ren H, Hurban R, Hutchins G, Fishman E. Amiodarone Pulmonary Toxicity: Ct Findings in Symptomatic Patients. Radiology 1990; 177:121-1253. Chai J, Patz E. CT of the Lung: Patterns of Calcification and Other High Attenuation Abnormalities. AJR 1994; 162:1063-10664. Rossi SE, Erasmus JJ, McAdams P, Sporn T, Goodman P. Pulmonary Drug Toxicity: Radiologic and Pathologic Manifestations. Radiographics 2000; 20:1245-1259
Images from Marchiori et al. are used with the permission of the copyright owner, American Roentgen Ray Society.
References





![Case Report # [] Submitted by:Kandra Vogt, MSIV Faculty reviewer:Sandra A. A. Oldham, M.D. Date accepted:31 August 2007 Radiological Category:Principal.](https://static.fdocuments.net/doc/165x107/56649d875503460f94a6c286/case-report-submitted-bykandra-vogt-msiv-faculty-reviewersandra-a.jpg)












