Case for Change & Model of Care...4/6/18 Redraft – 11/7/18 0.4 Rachel Noble & Alex Vincent of Case...
102
Case for Change & Model of Care Respiratory services V0.14
Transcript of Case for Change & Model of Care...4/6/18 Redraft – 11/7/18 0.4 Rachel Noble & Alex Vincent of Case...

Case for Change & Model of Care
Respiratory services V0.14

Title Case for Change & Model of Care for Greater Manchester Respiratory Services
Theme Lead Diane Whittingham
Project Lead Darren Banks, Provider Transformation Lead (Director of Strategy, Manchester University NHS Foundation Trust)
Author Dr Jennifer Hoyle, Clinical Lead (Consultant Respiratory Physician, Pennine Acute NHS Foundation Trust)
Alex Vincent
Version 0.14
Target Audience Theme 3 Clinical Reference Group HR & Workforce Reference Group Theme 3 Board
Date Created 24/01/2018
Date of Issue
Document Status Draft
Description This document presents the clinical case for change and outline model of care for respiratory services within Greater Manchester.
File name & path
Document History:
Date Version Author Notes
24/01/18 0.1 Ruth Clark First draft
03/03/18 0.2 Ruth Clark Additional work on first draft
21/03/18 0.3 Ruth Clark Amendments and additions
4/6/18 – 11/7/18 0.4 Rachel Noble & Alex Vincent Redraft of Case for Change
13/7/18 0.5 Rachel Noble Population of Case for Change in combined document
13/7/18 - 16/7/18 0.6 Alex Vincent Development of combined document with Clinical Lead
17/7/18 - 18/7/18 0.7 Alex Vincent Changes made after discussion with Clinical Lead
20/7/18 0.8 Alex Vincent Draft prepared for circulation CRG
4/9/18 – 7/9/18 0.9 Alex Vincent Development based on feedback
17/9/18 0.10 Alex Vincent Final amendments for circulation to DOF
02/10/18 0.11 Alex Vincent Amendments following DOF
09/10/18 0.12 Rachel Noble Amendments following ECAP
11/10/18 0.13 Jenny Hoyle Clinical review and amendments following ECAP
12/10/18 0.14 Rachel Noble Review and final ECAP amendments
Approved by:

Greater Manchester Health and Social Care Partnership
4
Distribution
Ver. Group Date Purpose
0.8 Clinical Reference Group 20/7/18 For meeting 25/7/18
0.10 Design Overview Forum 17/9/18 For meeting 20/9/18
0.11 Provider Transformation Lead,
Clinical Lead and Theme 3 Board 02/10/18 FERG, WRG & ECAP
0.14 Theme 3 Exec 12/10/18 For meeting 17/10/18
T A B L E O F CO N T E N T S
Table of Contents 4
1. Executive Summary 7
1.1. Case for change 7
1.2. Outline Model of Care 8
2. Context 10
2.1. Scope and purpose 10
2.2. Background – work completed to date in GM 11
2.3. Recent developments 12
3. Key drivers for change 16
3.1. Demographic Changes 16
3.2. Health Outcomes 17
3.3. Activity and Spend on Delivery 20
3.4. Referral to Treatment Times (RTT) 28

Greater Manchester Health and Social Care Partnership
5
3.5. Patient Safety & Experience 29
3.6. Current outcomes in GM 30
3.7. Current Respiratory sites & provision within GM 31
3.8. Headlines: Fixed points 33
3.9. SWOT Analysis 34
4. Design Approach 36
4.1. Engagement and Co-design Process 36
4.2. Patient Principles and Feedback 36
5. Challenges 38
5.1. Key Risks 38
5.2. Seven Day Working 41
6. Recommendations 43
6.1. Theme 3 – Acute & Specialised Care 43
6.2. Summary of Financial and Operational Efficiency Benefits 44
7. Preferred Model of Care 45
7.1. Model of Care 45
7.2. Governance & Clinical Leadership 47
7.3. Service Description and Care Pathway 47
7.4. COPD Model of Care 48
7.5. GM Framework for Influenza 56
7.6. Pneumonia 57
7.7. Standard Respiratory Offer 60
7.8. Service Access Requirements 62
7.9. Follow up and aftercare 63

Greater Manchester Health and Social Care Partnership
6
7.10. Audit, Research and Education 64
8. Financial Considerations 65
8.1. Financial principles for Theme 3 65
8.2. Logic modelling for financial impact of new model of care 66
9.1. Enablers 69
9.2. Critical Success Factors 70
10. Appendices 72
10.1. Appendix A - Supporting Data 72
10.2. Appendix B - Table 6: Population of CCGs at mid-point 2016 78
10.3. Appendix C - Right Care, Commissioning for Value; Pathway on a page 79
10.4. Appendix D – Clinical COPD Audit Participants 82
10.5. Appendix E – Attendance Sheet at COPD Workshop 83
10.6. Appendix F - Patient Questionnaire 84
10.7. Appendix G - Clinical Co-dependencies 93
10.8. Appendix H - Service Standards 96
10.9. Appendix I – Free Vaccination for Influenza 99
10.10. Appendix J - Abbreviations Table 100

Greater Manchester Health and Social Care Partnership
7
1.EX E C U T I V E S U M M A R Y
This document is designed to inform the decision-making process on the transformation of Greater
Manchester (GM) Respiratory Services, focussing on Theme 3, Standardising Acute and Specialist
Care. Respiratory medicine covers the diagnosis and treatment of a wide variety of diseases of the
airway and lungs, their linings and blood vessels and the muscles and nerves required for breathing.
A list of respiratory medicine services is described in Appendix A.
1.1. Case for change
Greater Manchester has some of the highest rates of respiratory disease in the country, and
mortality rates for preventable respiratory disease are high. The conurbation has a high prevalence
of lung cancer, Chronic Obstructive Pulmonary Disease (COPD), asthma and unacceptable variation in
length of stay across a number of respiratory disease areas. Demand for respiratory services is high
and in 2016/17, there were over 50,000 hospital spells for respiratory disease and over 70,000
Finished Consultant Episodes (FCEs). When weighted by age and gender, premature mortality from
respiratory disease is significantly higher than the national rate in seven of the twelve Greater
Manchester CCGs, and similar for the remaining five.
From a public health perspective, Greater Manchester has higher-than average smoking rates, and
insufficient smoking cessation services to meet demand (though a strategy is being put in place to
address this1). 18.4% of the adult population smokes compared to a national average of 15.5%2, and
this contributes to above-average prevalence of smoking-related disease. Greater Manchester’s
industrial history has also contributed to an increased incidence of industrial lung disease.
1 http://www.gmhsc.org.uk/wp-content/uploads/2018/04/Tobacco-Free-Greater-Manchester-Strategy.pdf 2 http://www.gmhsc.org.uk/wp-content/uploads/2018/04/Tobacco-Free-Greater-Manchester-Strategy.pdf

Greater Manchester Health and Social Care Partnership
8
There are significant opportunities across GM to improve patient experience and potentially, to
reduce secondary care costs through reducing variation, a reduction in length of stay (LOS) and
avoiding admission through the provision of responsive, accessible, high-quality community, primary
and intermediate care. The model includes the appropriate use of evidence-based risk-stratification
tools to be standardised across GM in order to avoid admission in the acute footprint where possible.
1.2. Outline Model of Care
Focussing on three aspects of respiratory care, the outline model of care makes recommendations
for further development:
i. Chronic Obstructive Pulmonary Disease (COPD); creation of a single model of care delivered to
an agreed set of standards across all GM
ii. Influenza; development of a single policy framework and commissioning for influenza, across
all themes in GM
iii. Pneumonia; development of a deeper understanding of the pneumonia challenge, through
detailed diagnosis review, prior to developing a single model of care for GM
Creating a single COPD pathway, accessible to all, which incorporates both in-reach and outreach
support by specialist respiratory nurses alongside early specialist clinical review, will improve not
only the quality of care received by patients, but also their length of stay in hospital and the support
they receive on discharge. Virtual Multidisciplinary Team (MDT) clinics, training of community staff
and inclusion of pulmonary rehabilitation, smoking cessation, education, vaccination and
psychosocial support will enable those diagnosed with COPD to remain healthier longer. For hospital
admissions, standardising the respiratory pathway, making it shorter and more responsive, with a
focus on Non-Invasive Ventilation (NIV) national standards and domiciliary services (including home-
NIV) will have similar benefits.
The huge variation currently seen in the treatment of those with influenza will be reduced by a single
GM-wide policy framework incorporating:
Health promotion
Vaccination criteria

Greater Manchester Health and Social Care Partnership
9
Diagnosis criteria and process
Treatment standards
Prescribing information
Pneumonia requires further examination. Initial investigation suggests that although, the diagnostic
process is well understood, not everyone diagnosed with pneumonia has undergone this process,
with diagnosis made based on history and current symptoms. By understanding this assumption
more fully, a coherent, comprehensive model can be developed for this cohort.
With a flexible specialist workforce which will support the patient and MDT across themes, the
document describes a model of care that wraps around the patient and their families.
Delivery of this model requires a development in how the clinical and nursing teams work, along with
the widening of their skill set. An increased number of specialist respiratory nurses will be required,
along with a possible increase in access to radiology services. Services based on single sites will need
to increase their outreach, allowing patients to be treated at home, creating improved outcomes and
better mental health and wellbeing, along with a reduction in time spent in hospital.
Financial sustainability is created through the reduction of inpatient care and admissions, by using
the appropriate person to deliver care, based on a multi-skilled respiratory specialist nursing team
and earlier clinical intervention when people present at the Emergency Department (ED).

Greater Manchester Health and Social Care Partnership
10
2.CO N T E X T
This case for change builds on the recommendations made in the scoping assessment and is for
Acute and Specialist Respiratory services in GM only.
2.1. Scope and purpose
Respiratory and Cardiology services were made a priority area for transformation under Theme 3,
noting that the frail elderly must be an underpinning theme. The Project Initiation Document (PID)
for Respiratory and Cardiology Services was completed and signed off in October 2016 by the Theme
3 Delivery Board.
The PID recommended that:
A whole-system scoping exercise would be required to fully understand current issues and
variations across the whole cardiology and respiratory pathway
The programme would focus on the standardisation of acute respiratory and cardiology
services through the development of a single GM single operating model and GM wide
clinical and patient standards as well as ensuring flow and fit across the entire system
There should be an improved interface between primary and secondary care
Likely areas of pathway development for respiratory medicine, would include severe
respiratory failure, chronic respiratory conditions, and respiratory infection
Following on from the recommendations made in the PID, a scoping assessment was produced in
order to better understand the current issues and variations across the entire Respiratory and
Cardiology pathway. The scoping assessment was signed off by the Clinical Reference Group (CRG) in
September 2017 with the following recommendations agreed:

Greater Manchester Health and Social Care Partnership
11
Respiratory and Cardiology should be split into two separate work streams, each with its own
case for change and model of care
The Respiratory and Cardiology work streams, although separate, would still need to link in
closely with Themes 1 and 2 to ensure a fully integrated, seamless service providing a high-
quality service for all. Respiratory-related projects in Themes 1 and 2 are key to supporting
this case for change and therefore key stakeholders from all three themes must work
together in an integrated way
2.2. Background – work completed to date in GM
Whist there has been a significant amount of work relating to respiratory care across GM, this has
taken place in individual localities and has added to the variation we see across CCGs. Focus has been
on Theme 2 primary and community support, along with admission avoidance for people with
respiratory disease. Virtual clinics, outreach respiratory nurse specialists, and even advanced nurse
practitioners working alongside the ambulance service to identify possible opportunities to avoid
escalation to hospital and deliver increased provision of domiciliary care have all been incorporated
into locality plans.
The focus of this project however is Theme 3, acute and specialist care, and whilst some of the
models described above will support the management of acute exacerbations in the community,
patients will still escalate to secondary care. By engaging with the localities and using the best of
these developments to describe a Theme 2 and 3 interface - and wherever possible incorporating
these aspects into the new model - a pathway for the most acute patients can be created that utilises
existing best practice, whilst creating a future proof model.
It is worth noting that the extra clinical resource from Theme 3, planned into Theme 2’s model,
would create additional workload pressures in the short to medium term, although it is expected that
- with additional knowledge and skills within the community - a proportionately reduced number of
patients would need to escalate or attend the acute services. It is recognised that it traditionally

Greater Manchester Health and Social Care Partnership
12
takes up to five years for the knowledge and skill transfer to take place and for the impact of change
to be felt, during which time there would be a continued additional pressure on secondary care
provision.
2.3. Recent developments and disease burden
There have been a significant number of developments in respiratory care in recent years, with a
particular focus on community and primary care services, supported self-management and the
introduction of evidence-based, best-practice pathways. In summary:
The British Thoracic Society has published the Quality Standards for Pulmonary Rehabilitation3
NHS RightCare has published a COPD pathway which is based on best-practice and NICE
guidance
The successful lung cancer screening project run in partnership between Wythenshawe
Hospital and Macmillan has been commissioned by MHCC to provide an additional screening
round for the North Manchester population
MRI and Wythenshawe Hospitals partnered on a Royal College of Physicians Future Hospitals
programme to improve community COPD care
Development of Greater Manchester Medicines Management Group (GMMMG) guidance on
COPD pharmacological treatments
Development of GMMG guidance on tobacco control and the introduction of the CURE
programme at MFT
Working with the housing sector to promote health in the local population
A working group with urgent care (111, NWAS, Go2Doc) to pilot an admission avoidance
scheme using care records that can be shared across the urgent care system
Local planning group with British Lung Foundation to increase awareness of respiratory disease
in the local population and promote peer support
Patient experience group (led by patients)
3https://www.brit-thoracic.org.uk/document-library/clinical-information/pulmonary-rehabilitation/bts-guideline-for-pulmonary-rehabilitation/

Greater Manchester Health and Social Care Partnership
13
The delivery of influenza and pneumonia vaccinations to high risk patients in secondary care
Nationally, lung disease and other respiratory conditions constitute large part of UK hospital
admissions. Lung disease, for example, is responsible for over 700,000 hospital admissions and more
than 6.1 million hospital bed days in the UK each year4. Lung cancer, COPD and pneumonia are
within the top six most common causes of death in the UK.
In recent years, it has also been recognised that, whilst there has been some noticeable
improvements in COPD-related care, unacceptable national variation still exists in regards to the
treatment of this condition. One important aspect to highlight in regards to this variation is the
differing proportions of admitted COPD patients who have access to specialist respiratory services
such specialist treatment, interaction with specialist staff and administration of NIV5.
Linking hospital-based care with community based care (i.e. clear evidence of follow-up care being
provided between different services) has also been recognised as an area of importance in regards to
various respiratory conditions. Services such as pulmonary rehabilitation programmes for example
have been associated with improved outcomes in regards to both reduced hospital admission rates
and reduced rates of mortality6 for patients with conditions such as COPD.
Idiopathic pulmonary fibrosis (IPF) is a type of lung disease that causes progressive scarring and
inflammation of the lungs. Despite it being a relatively uncommon disease when compared to
conditions such as COPD, it has a noticeable impact on those that it afflicts in regards to mortality.
Statistics on IPF suggest that the median survival rate from IPF is 3 years from diagnosis and only 20%
of IPF patients are reported to survive to 5 years post diagnosis7. Recent advancements in the
treatment of IPF in the UK include4:
4 The Battle For Breath Report, 2016, British Lung Foundation 5 COPD Who Cares Organisational Audit, November 2014, Royal College of Physicians, British Thoracic Society 6 Pulmonary Rehabilitation: Beyond Better Breathing, 2017, Royal College of Physicians, British Thoracic Society 7 The British Thoracic Society Interstitial Lung Disease Registry Programme Annual Report, 2015/16, British Thoracic Society

Greater Manchester Health and Social Care Partnership
14
Clear NICE guidelines for the diagnosis and management of adults with IPF
Quality standards of care for IPF patients published by NICE
New IPF treatments have become available, including the drugs pirfenidone and nintedanib
In a similar fashion to other respiratory conditions, developments relating to IPF have emphasised
the importance of both specialist clinician input and cross boundary care between hospital and
community services.
2.3.1. Virtual Clinics – COPD A consultant-led virtual clinic (VC) model was established in GM in 2016/17 to support GPs in the
management of patients with COPD. Patients were identified through targeted searches and their
primary care record reviewed in a joint primary/secondary care education session. These sessions
aim to educate and up-skill primary care staff, promote non-pharmacological interventions such as
pulmonary rehabilitation and smoking cessation, and promote safe prescribing practices as per the
GMMMG guidelines. In the early stages of the programme, 522 patients were identified and
discussed as a result of the VCs and of those reviewed, 50-75% had treatment stepped down, leading
to a cost-saving of £306 patient/year. Table one summarises the feedback data:
Table 01: Feedback from 5 out of 14 GP practiced after virtual clinics

Greater Manchester Health and Social Care Partnership
15

Greater Manchester Health and Social Care Partnership
16
3.KE Y D R I V E R S F O R C H A N G E
3.1. Demographic Changes
GM has an ageing population; the 75+ age group is expected to increase by approximately 37%
between 2016 and 2030, and the 60-74 age group has a projected increase of 21% between 2016
and 2030.
The risk and impact of respiratory disease increases with age, with many patients having multiple co-
morbidities, therefore it is expected that there will be a significant increase in activity for respiratory
services if we do nothing. Wigan Borough CCG has the highest predicted increase in >75 population
at 19.57% with Tameside and Glossop, Bolton and Bury CCG’s being next highest at 13.95%, 13.62%
and 13.60% respectively.
The highest rates for growth in GM across all age ranges are expected to be in South Manchester
(4.86%), North Manchester (4.44%) and Trafford (3.63%) in the next five years1
Whilst there is a significant amount of work to improve the health of the population and reduce the
incidence of respiratory disorders, the number of patients presenting continues to grow and, as the
risk and complexity of certain respiratory related diseases increases as they get older, it can be
assumed that there will be an increase in respiratory related activity in GM in years to come.
Figure 01: Estimated demographic changes 2016 – 2021

Greater Manchester Health and Social Care Partnership
17
Age group
% increase 2016-
25 % increase 2016-30
0-14 4.70 2.85
15-29 -3.04 0.59
30-44 8.40 6.87
45-59 -3.19 -4.30
60-74 11.33 21.13
75+ 26.34 36.83
Source: Office for National Statistics, mid-2016 population projections by local authority.
3.2. Health Outcomes
Greater Manchester (GM) has some of the most deprived areas and the poorest respiratory health in
the UK, and amongst the highest prevalence rates for lung diseases. 18.8% of adults in GM are
smokers, and Manchester, Salford and Rochdale local authorities had amongst the highest rate of

Greater Manchester Health and Social Care Partnership
18
premature deaths from lung disease in England between 2013-2015 with Manchester the worst
performing area in the country with a rate of 68.3 premature deaths per 100,000 population.
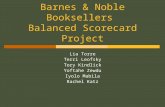
Figure 02: Bottom 12 ranking local authorities for Lung Disease
Additionally a key driver for change in relation to public health is the prevalence of respiratory
related diseases within the population (figure 03):
11 out of 12 GM CCGs have a reported prevalence of COPD that is above the national average
of 1.85%
Only 2 out of the 12 CCGs have a prevalence that is above that of their comparator CCGs.
There is a variation of 1.35% in reported COPD prevalence between GM CCGs
9 out of 12 GM CCGs have a prevalence of Asthma that is above the national average of 5.91%.
Half of these s also have a prevalence that is above that of their comparator CCGs
There is a variation of 1.52% in Asthma prevalence between GM CCGs

Greater Manchester Health and Social Care Partnership
19
Figure 03: Respiratory Disease Prevalence in GM CCGs 2015/16
Source: NHS Right Care (2017). ‘Where to look’ packs. [Online] Available at: https://www.england.nhs.uk/rightcare/products/ccg-data-packs/. Last accessed: 26th February 2018
Figure 04: Premature mortality in GM from Respiratory Disease

Greater Manchester Health and Social Care Partnership
20
Source: NHS Right Care (2017). ‘Where to look’ packs. [Online] Available at: https://www.england.nhs.uk/rightcare/products/ccg-data-packs/. Last accessed: 26th February 2018 Rate of premature mortality has been directly age and sex standardised to England population
Only two of the GM CCGs have a mortality rate for under 75 year olds of less than the national
average. These CCGs are also not where the lowest prevalence occurs, once again demonstrating the
variation in service delivery and its impact on outcomes.
Future respiratory related care will, therefore, need to have clear links between acute, primary and
community services. Integration of patient pathways across respiratory care can help ensure earlier
diagnosis of conditions such as COPD, promote self-management, help reduce admissions to
secondary care and ensure that appropriate referrals are being made across all respiratory services in
GM.
3.3. Activity and Spend on Delivery
There were just over 52000 respiratory spells in GM in 2016/17 with over 50% of those attributable
to two main disease groupings 1) chronic lower respiratory diseases which includes: asthma; COPD;
emphysema; and simple and mucopurulent bronchitis, and 2) influenza and pneumonia
Median LOS for both disease groupings are:

Greater Manchester Health and Social Care Partnership
21
4.8 days for chronic lower respiratory diseases;
9.7 days for influenza and pneumonia.
Of the hospitals that treat the highest volume of cases (classed as those which saw over 1000 cases
in 2016/17), the ranges are as follows:
Chronic lower respiratory: shortest – 3.7 (Salford) and longest is 5.9 (MRI)
Influenza and pneumonia: shortest – 6.4 (Fairfield) and longest is 12.6 (MRI)
National data from the COPD Audit Programme suggests an average length of stay for COPD patients
of 4 days, indicating that work is needed in GM to target a reduction in LOS from the existing 4.8days.
Data for average LOS for pneumonia is less readily available but one study suggests a median LOS of
9 days compared to the GM 9.7days.
RightCare identifies Respiratory services as an area of opportunity for eight CCGs (Bolton; Heywood,
Middleton and Rochdale; Manchester; Oldham; Salford; Stockport; Tameside and Glossop; Trafford).
Data on potential lives saved as a result of a reduction in mortality from COPD, emphysema and
bronchitis in the under 75s is not available for all CCGs, but estimates are provided for five. This data
indicates that 125 lives could be saved if these CCGs performed at the level of the five best
performing CCGs in the country. Given the high volume of respiratory cases in GM, it is reasonable to
assume that the potential for lives saved exceeds this estimate
Data for the potential reduction in bed days is provided for seven CCGs and it is estimated that
performing to the same standard as the five best performing CCGs would save around 50,275 bed
days per annum

Greater Manchester Health and Social Care Partnership
22
Estimated potential savings for non-elective care are provided for seven CCG areas and are
significant: performing at the same standard as the five best-performing CCGs in the country could
equate to savings of £12.1m.
Estimated potential saving on elective respiratory care are provided for seven CCG areas and amount
to £3.2m.
3.3.1. Elective Care Figure 05: Activity by hospital site for elective patients 2016/17
The majority of elective respiratory care takes place at Wythenshawe. Housing the North West Lung
Centre it would be anticipated that elective activity would be highest on this site.
The greatest activity occurs in “Other diseases of the upper respiratory tract”, including tonsil
infections, allergic rhinitis, sinusitis and other larynx and pharynx disorders, followed by “chronic
lower respiratory disease” which includes COPD.
Although Wythenshawe cater to the vast majority of elective admissions, the numbers still remain
small.

Greater Manchester Health and Social Care Partnership
23
In addition to the above information, the following figures derived from NHS RightCare also provide
an insight into the variation across GM CCGs in terms of elective spending8.
Figure 06: Total elective spend per 1000 population (weighted for age & sex) 15/16
The spend data leaves us able to draw a number of conclusions:
There is variation in elective spend between the 12 GM CCGs when compared with the
national average
9 of the CCGs have an elective spend that is above the national average. Most notable is South
Manchester, which spent £2620 above the national average in 2015/16
3 of the CCGs have an elective spend that is below the national average. Most notable is Bury,
which spent £773 below the national average in 2015/16
8 NHS Right Care (2017) ‘where to look’ CCG Data packs. [Online] Available at: https://www.england.nhs.uk/rightcare/products/ccg-data-
packs/where-to-look-packs/ Last accessed 12th February 2018

Greater Manchester Health and Social Care Partnership
24
There is also a clear variation in elective spend between the CCGs themselves. There was a
difference in spend of £3,393 between the lowest and highest spending CCGs, Bury and
South Manchester, respectively
3.3.2. Non-Elective Care Figure 07: Activity by hospital site for non-elective patients 2016/17
With a much higher activity in non-elective care, it is clear that those sites with an ED have the
majority of their activity in “Influenza and Pneumonia” and “chronic lower respiratory disease”
condition groups. Activity is also more evenly spread across the sites.
Figure 08: influenza and Pneumonia non-elective admissions

Greater Manchester Health and Social Care Partnership
25
Source: RightCare Greater Manchester Respiratory Insight, May 2018
The highest levels of non-elective admissions for influenza (flu) and pneumonia occur between
November and March each year, with the older age bands contributing the most to admissions. The
growth in admissions can be seen clearly with the number of admissions increasing by nearly 500
(23%) between January 2015/16 and 2016/17.
Empirically every Trust and CCG manages influenza patients differently, so variation amongst this
group of patients is large, and opportunities for standardisation numerous.
Figure 09: Percentage of people over 65 years vaccinated at 31st March 2017

Greater Manchester Health and Social Care Partnership
26
Flu, whilst not totally avoidable, can have the incidence significantly reduced by vaccinating the
population. The variation in vaccines given to the age 65+ population, most vulnerable to flu, is
significant across GM, with only two CCGs performing better than the highest 5 similar peers.
Empirically, not all patients diagnosed with pneumonia have undergone a formal process for
diagnosis and have confirmed physiological changes expected to be seen in those with the disease.
Anecdotally this is particularly true for those who have died, with an existing respiratory disease and
expectorations. Although the evidence is limited at this time, an audit to understand the extent of
these reported concerns should be undertaken.
Figure 10: Total non-elective spend per 1000 population (weighted for age & sex) 15/16

Greater Manchester Health and Social Care Partnership
27
Source: NHS Right Care (2017) ‘where to look’ CCG Data packs.
Again the RightCare data demonstrates:
Only 1 out of the 12 GM CCGs spent below the national average. This CCG was Bury, and spent
£2,889 below the national average
The other 11 CCGs spent varying amounts above the national average, most notably South
Manchester, which spent £19,903 above the national average in 2015/16
There is also a clear variation in non-elective spend between the CCGs themselves. There was a
difference in spend of £22,793 between the lowest and highest spending CCGs, Bury and
South Manchester, respectively
It is interesting to note that GM currently spends £9.6m more on non-elective admissions for
Influenza and Pneumonia than the best 5 CCGs.
Figure 11: Non-elective spend on admissions for Influenza and Pneumonia

Greater Manchester Health and Social Care Partnership
28
By using the RightCare data with values of spend and bed days per 1000 population (adjusted for age
and sex), these do not take into account the complexity of a particular patient’s diagnosis or
treatment. This could be the reason why South Manchester, which houses the specialist services
located in the NWLC, has such a high rate of spend and bed days compared to the other GM CCGs for
both elective and non-elective care.
3.4. Referral to Treatment Times (RTT)
The average wait for new referrals into GM respiratory service remains under 60 days and has done
so for the last 2 years, however consultant to consultant referrals for the most complex cases and
domiciliary NIV assessment into Wythenshawe have a mean referral time of 396 days and a median

Greater Manchester Health and Social Care Partnership
29
of 168 days9. This wait has been increasing over the last year, suggesting that the demand for these
services outweighs the capacity.
This assumption is supported by anecdotal evidence and empirical verification, including the delivery
of a separate service for Wigan CCG patients, delivered by WWL, again highlighting variation of
service and standards.
3.5. Patient Safety & Experience
From the data above it is clear to see that the variation in care across GM is significant, inherently
suggesting that not all GM patients are receiving the best possible care.
Best practice tariffs are attached to COPD care and GM patients are only receiving these in 38% of
cases10. It should be noted that not all providers submitted data for this audit.
Figure 12: Achievement of Best Practice Tariffs 2017
Source: RightCare Greater Manchester Respiratory Insight, May 2018
9 Dr Foster outpatient waiting times; accessed on the 17/07/18. 10 Data from the National Asthma and COPD Audit; via https://nacap.org.uk/nacap/welcome.nsf/reportsSCbpt.html
Last accessed 16/07/18
CCG Name Trust
Respiratory Review
within 24 hrs (%)
Discharge Bundle
(%) BPT Passed (%) BPT >= 60%
NHS Manchester CCG University Hospital of South Manchester NHS Foundation Trust 83 91 78 1
NHS Salford CCG Salford Royal NHS Foundation Trust 77 77 66 1
NHS Manchester CCG Central Manchester University Hospitals NHS Foundation Trust 69 91 66 1
NHS Stockport CCG Stockport NHS Foundation Trust 44 71 34 0
NHS Wigan Borough CCG Wrightington, Wigan and Leigh NHS Foundation Trust 51 26 20 0
NHS Heywood, Middleton and Rochdale CCG Pennine Acute Hospitals NHS Trust 33 29 11 0
NHS Bolton CCG Bolton NHS Foundation Trust 56 15 10 0
NHS Tameside and Glossop CCG Tameside Hospital NHS Foundation Trust 28 13 5 0
Overall Attainment 37.50%

Greater Manchester Health and Social Care Partnership
30
3.6. Current outcomes in GM
In November 2014, the National COPD Audit Programme released their national organisation audit
report11. Contained within this report is site level data on the organisation and resources of COPD
care in acute NHS units (Appendix D). As part of this data, each unit was scored against key criteria
relating to COPD care. Components that made up a unit’s total score included:
Whether a senior review on admission as received
Whether the patient had access to specialist care
Whether a patient had access to NIV
Managing respiratory failure and oxygen therapy
Integrating care across a primary and secondary sectors
Extra items such as: having a system of early warning detection, smoking cessation services
within the unit and the availability of on-site palliative care
The highest possible score for these combined criteria is 51, the highest achieved 48 (Royal Devon & Exeter Hospital) and lowest 12 (Sandwell General Hospital). The Median Score was 33.
From analysing the scores for each of these sites, the following observations can be made about
COPD-related acute care in GM:
The median overall score of the eleven GM trusts was 34, just above the median score of 33
for all participating sites in England and Wales
Three GM sites (Trafford General, Tameside general and Stepping Hill) fell into the lowest 25%
of organisations in terms of total score
11 Royal College of Physicians & British Thoracic Society (2014) National COPD Audit: COPD: Who cares? National Chronic Obstructive Pulmonary Disease (COPD) Audit Programme; Resources and organisation of care in acute NHS units in England and Wales 2014 via: https://www.rcplondon.ac.uk/projects/outputs/copd-who-cares-organisational-audit-2014 Last accessed 17/07/18

Greater Manchester Health and Social Care Partnership
31
Three GM sites (North Manchester General Hospital, Salford Royal and Royal Bolton) fell into
the highest 25% of organisations in terms of total score
Only one site (Salford Royal) received the maximum possible score for the ‘senior review on
admission’ category
Eight out of the eleven GM sites received the maximum possible score for the ‘NIV’ category;
Four out of the eleven GM sites received the maximum possible score for the ‘managing
respiratory failure and oxygen therapy’ category
Only one site (North Manchester General Hospital) received the maximum possible score for
‘integrating care across primary and secondary sectors’
No GM sites received the maximum possible score for the ‘extra items’ category, although it
should be noted that no sites in the audit actually achieved the maximum score for this
category
It is notable that three sites (Wythenshawe, Royal Albert Edward Infirmary and Tameside General
Hospital) could have potentially increased their overall score (by 2, 4 and 1 respectively) if they had
not missed submitting certain data to the audit.
In summary, it is encouraging to see that most sites in GM achieved maximum scores in at least one
of the categories, and over half of GM sites were above the median value of all participating
organisations in regards for their total score. The high scores corresponding to the use of NIV should
also be noted. However, the fact that a considerable proportion of the sites’ fall into either the top
25% or the bottom 25% in regards to their overall score shows variation in practice across GM in
regards to COPD. The lack of maximum scoring in regards to the integration between primary and
secondary sectors is also something that should be noted.
3.7. Current Respiratory sites & provision within GM
All GM trusts provide some respiratory care with high rates of emergency Finished Consultant
Episodes (FCEs) across the conurbation in all disease groupings. 10 of the 13 hospitals providing

Greater Manchester Health and Social Care Partnership
32
respiratory services have a high rate of emergency presentations, classed as those with more than
4000 FCEs in 2016/17.
Table 02: GM Hospitals with over 4000 emergency respiratory FCEs in 2016/17*
Hospital Emergency FCEs in 2016/17
Wythenshawe Hospital 9628
Salford Royal 8711
Royal Bolton Hospital 7421
Stepping Hill Hospital 7158
Manchester Royal Infirmary 7124
Tameside General Hospital 6685
Fairfield General Hospital 6677
Royal Oldham Hospital 6135
Royal Albert Edward Infirmary 5405
North Manchester General Hospital 4417 *Categories of less than 5 FCEs supressed to ensure patient confidentiality
Interestingly this does not correlate with the population size in the respective areas during this time
(Appendix B), with a range between 3.5% of the population admitted in Salford, to 1.7% in Wigan,
again suggesting variation in the care received by these patients.
There is considerable research and development in the field of COPD management and a clear
imperative to standardise pathways to reduce length of stay and overall costs, and it is on that basis
that this case largely focuses on the opportunities related to COPD.
Total emergency FCEs for respiratory across GM amount to 71,472 in 2016/17 and 74% of these
cases were classified as chronic lower respiratory disease (which includes COPD, emphysema,
bronchitis and asthma) and influenza and pneumonia with the following percentage split:
28% chronic lower respiratory diseases;
47% influenza and pneumonia.
The high volume of cases of both COPD and influenza and pneumonia suggest that these conditions
should be the primary focus of the case for change. The nature of influenza means that demand for
services are influenced by factors such as uptake of the vaccination, public health messaging, and

Greater Manchester Health and Social Care Partnership
33
indeed, the strain of the virus. It is critical that there is a standard pathway for influenza in GM which
focuses on best practice management, but this appears to be an area where transformation efforts
are not best targeted, as the caseload is subject to factors that are largely difficult to control. The
transformation programme may wish to consider a review of pandemic readiness and to link with
public health to ensure active promotion of the vaccination and hand hygiene prior to the flu season.
More data is required on the incidence of pneumonia. There are organisational based audits carried
out regularly, but further understanding is needed of how and when diagnosis of pneumonia are
made and its links to frailty, aspiration, hospital acquired pneumonia and production of sputum.
Although all providers are able to support COPD patients, only one is commissioned to deliver
provision of domiciliary Non-invasive ventilation (NIV), a key treatment for many of our most poorly
COPD patients. The RAEI does deliver a non-GM commissioned provision due to delays in the
referral process. Consequently this does not have the same backup team as the commissioned
service. All sites have separate arrangements for sleep (CPAP) ventilation services; in additionSalford
has a neurology service and ventilation service as part of neurological causes of ventilatory failure..
3.8. Headlines: Fixed points
The points below outline recent developments in GM which provide further context for the project:
Manchester University NHS Foundation Trust was created on 1 October 2017 following the merger of
Central Manchester Foundation Trust (CMFT) and University Hospital of South Manchester (UHSM).
It is anticipated that Manchester Foundation Trust (MFT) will acquire North Manchester General
Hospital some 12 to 18 months later. The agreement with Greater Manchester Health and Social
Care Partnership (GMH&SCP) is that in areas such as respiratory, where there is a Theme 3 project,
the Trust will align its merger plans with the wider Theme 3 programme.

Greater Manchester Health and Social Care Partnership
34
North, Central and South Manchester CCGs have merged and integrated with the health team of
Manchester City Council to form Manchester Health and Care Commissioning
With the creation of four Healthier Together (HT) sectors Salford, Stockport, Oldham and MRI will
become “high acuity” hospitals providing 24/7 A&E services with full surgical support and
undertaking high risk emergency and elective general surgery for their sector
The North West Lung Centre based at Wythenshawe, provides a tertiary referral service for people
across the North West and whist this service forms part of the overall redesign, it will be included in a
way cognisant of this.
3.9. SWOT Analysis
Strengths Weaknesses
Very high level of specialist respiratory
expertise in GM
Wythenshawe is host to the North West Lung
Centre
Significant variation in clinical practice
pathways, quality of care and patient
experience across GM for patients with
acute respiratory conditions
Variation in length of stay
Despite good practice, disease prevalence
remains high
Lack of smoking cessation services in GM has
meant smoking rates remain high
Variation in workforce availability across the
sites
Opportunities Threats
GM wide Pulmonary Rehabilitation
Self-Management and Care Plans
Access to Secondary Care by Primary Care
when required
Individual localities already commenced
redesign work
Capacity of the service as respiratory disease
diagnosis continue to grow

Greater Manchester Health and Social Care Partnership
35
Development of GM-wide integrated and
standardised pathways
System wide approach for areas of specialist
care such as: lung cancer, severe respiratory
failure, chronic respiratory conditions and
respiratory infections
Rollout of virtual clinic educational model for
COPD
Development of community care services to
support admission avoidance
To implement best-practice learning e.g. Royal
College of Physicians Future Hospitals
partnership project between MRI and
Wythenshawe Hospitals
Reduction in variation

Greater Manchester Health and Social Care Partnership
36
4.DE S I G N AP P R O A C H
4.1. Engagement and Co-design Process
Engagement activity continues to be a priority of this project. Whilst time has been very limited for
the initial phase of the project, engagement has already commenced with a COPD workshop on the
11th July 2018 (attendance sheet in Appendix E) Further engagement events and formal DOFs are
planned for September to ensure availability and the required 8 weeks’ notice is given for clinicians.
The scoping and design phases of the project were led through meetings with the Provider
Transformation Leads (John Wareing - Director of Strategy at Manchester University NHS Foundation
Trust), and the TU project lead. The Clinical Lead (Dr Jennifer Hoyle, Consultant Respiratory
Physician, Pennine Acute NHS Foundation Trust) joined the project on the 1st July 2018.
As documents are to be shared with the Design Oversight Forum (DOF) feedback following the initial
agreement of concept from the Clinical Reference Group, and will be formally reviewed at the DOF
meeting on the 5th September 2018.
4.2. Patient Principles and Feedback
One of the key drivers for the transformation of Respiratory Services is to improve the quality and
consistency of services for patients in GM. It has been crucial therefore to involve patients as much
as possible given the timeframe available and to use their experiences and opinions to help inform
the design of the model of care.
Several approaches have been taken to involve patients, their relatives and potential service users in
the project:
Patient focus groups at GM based COPD and other respiratory disease patient groups;
Questionnaire to patients in target cohorts;
Identification of patients interested in further involvement, to invite to any further DOF
opportunities.

Greater Manchester Health and Social Care Partnership
37
Feedback from the focus groups gave a unified voice to the need for localised services, describing
how difficult it is to access services further afield as disease progresses. This was further described in
the strong message that respiratory disease is something people live with, that community access to
services is essential and that people are keen to have control over their care.
A patient questionnaire was circulated across all localities between 24th July – 24th August 2018 and
52 responses were received (Appendix F). From those responses several salient points which will be
considered and incorporated into the model of care where possible, are outlined below:
43% of those who responded came from the Salford and Wigan areas
48% consider themselves to have a disability, and 79% consider themselves to have a long
term conditions
80% of those who responded are currently using respiratory services within GM
Respondents attend 13 different hospitals with 44% attending Leigh infirmary
Staff helpfulness, friendliness and professionalism was the best thing about the service for
almost half the respondents
39% said nothing could be improved about the service they received;
Neither initial waiting times after referral or waiting times between diagnosis and treatment
were an issue for 80% of those accessing the service
Of those who smoke, only half have received advice and support to stop, however only 9% of
respondents believe there is not enough support for those who wish to stop, suggesting
some disparity between perception and reality
Over a quarter of respondents have not been offered influenza vaccinations and one person
was unsure, suggesting the target group for this prevention programme are not being
reached
A specialist team, care close to home and involvement in the decision making process account
for half the answers when asked what would be important for a hospital stay
Pulmonary rehabilitation had not been offered to 65% of those who responded, however this
may not have been appropriate for all patients e.g. those with sleep apnoea, but only half
those who commenced pulmonary rehabilitation completed The most important thing to
people in terms of future respiratory services is that it remains the same and that they are
kept informed and involved in any changes. Ease of access and shorter waiting times are also
mentioned, although previous questions suggest waiting times are not a significant issue for
this cohort.

Greater Manchester Health and Social Care Partnership
38
5.CH A L L E N G E S
5.1. Key Risks
5.1.1. Increasing Demand As the population increases, particularly in the 75+ age group, we will continue to see an increase in
the diagnosis and treatment of respiratory disorders. Without a change in how we manage these,
particularly in relation to delivery of increased and enhanced community care, smoking cessation,
the respiratory service will be overwhelmed.
By increasing the use of technology to deliver education, support and monitoring, improved
medicines management and compliance, and a shift in treatment of COPD and other exacerbations
into the community, we can start to relieve some of the pressure on secondary care, reduce the
variation we see across GM and improve outcomes.
5.1.2. Workforce Although the workforce is supporting the present service, there have been a number of challenges
recruiting to both respiratory consultant and advanced nurse specialist roles. With increasing
demand due to the aging population, the demand for these roles will increase.
Through new ways of working, particularly the use of technology, it would be possible to increase
opportunities for flexible working within these roles, as many aspects of the developing models of
care in Theme 2 which require secondary care input, could be delivered from any setting.
It would be possible for GM, with the support of local universities to train its own respiratory
specialists and advanced practitioners, particularly if a way to tie these to the GM workforce could be
identified. This could include both contractual arrangements and job enhancements e.g. rotation
through areas of clinical interest or specialist centres.

Greater Manchester Health and Social Care Partnership
39
Whilst there is a large body of respiratory clinical expertise in GM the majority of this is based on one
site at Wythenshawe. To deliver an equitable service across all the GM population, there will need to
be a sharing of skills, and a move towards a hub and spoke, rather than solely centralised model for
respiratory services.
5.1.3. Mental health and long-term conditions As respiratory conditions are long-term, with stable periods and exacerbations, many patients
experience deterioration over time. This means the access to services is an important aspect of care.
Limited mobility, social isolation, frailty and poor prognosis all mean that the development of mental
health issues in this patient group is two to three times more likely than in people without long-term
conditions12.
Delivering support and care in local social settings, encouraging pulmonary rehabilitation as a group,
rather than as an isolated undertaking and avoiding unplanned admissions where possible with the
use of enhanced domiciliary and community support, can all reduce the incidence and impact of
mental health issues on these patients13.
5.1.4. Accessibility An inability to effectively manage their disease, coupled with an inability to access services increases
the isolation and contributes to the anxiety and depression most typical among this group6.
Additionally the increased age and frailty that often accompanies these diagnoses often make the
person less able to travel across the region for treatment and appointments.
Solutions to this could be twofold:
1. Keep services accessible, in locations older people who may have reduced mobility can access
12
Naylor C, Parsonage M, McDaid D, Knapp M, Fossey M, Galea A (2012). Long-term conditions and mental health: the cost of co-
morbidities. London: The King’s Fund and Centre for Mental Health. Via: www.kingsfund.org.uk/publications/long-term-conditions-and-mental-health Last accessed: 16/07/18 13 Naylor C, Das P, Ross S, Honeyman M, Thompson J, Gilburt H. (2016) Bringing Together Physical and Mental Health; A new frontier for
integrated care, The Kings Fund Via: https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/Bringing-together-Kings-Fund-March-2016_1.pdf Last accessed: 16/07/18

Greater Manchester Health and Social Care Partnership
40
2. Where appropriate deliver services in the home and community to ease access
The majority of respiratory contacts in acute and specialist care are non-elective. For these services
patients are able to access care across most sites in GM, particularly those with an Emergency
Department (ED) or Urgent Care Centre (UCC).
Figure 13: Acute sites across GM and population who have accessed non-elective respiratory care
It is clear from the map that urgent and emergency services are available in the locality for those
needing this level of care, however the increased incidence in central and western GM also indicates
a need to ensure services are continued to be provided in these areas.
5.1.5. Multiple concurrent redesigns Although this project forms the basis of the Theme 3 redesign for GM, it has become evident that
there are a number of pieces of work on-going to deliver improved respiratory services. Some
will relate directly, having a positive impact (e.g. virtual MDT clinics), whilst others may
create pathways either synergic or disparate to the model.
Keeping the various stakeholders involved will be challenging and ensuring the transparency and
engagement required for organisations such as Health Innovation Manchester, the Respiratory

Greater Manchester Health and Social Care Partnership
41
Strategic Clinical Network, the North West Care Alliance, the Advancing Quality Alliance (AQuA), to
name but a few will be a significant challenge during this project.
5.2. Seven Day Working
Not all sites are currently able to deliver the ‘7 Day Clinical Standards’6 in full and the model
recommends that GM works towards the provision of seven-day access to specialist respiratory
clinicians. Challenges arise concerning the following standards:
Standard Two - All emergency admissions must be seen and have a thorough clinical
assessment by a suitable consultant as soon as possible but at the latest within 14 hours
from the time of admission to hospital.
Standard Three - All emergency inpatients must be assessed for complex or on-going needs
within 14 hours by a multi-professional team, overseen by a competent decision-maker,
unless deemed unnecessary by the responsible consultant. An integrated management plan
with estimated discharge date and physiological and functional criteria for discharge must be
in place along with completed medicines reconciliation within 24 hours. (further supporting
information suggests that this should be a specialty team)
Standard Five - Hospital inpatients must have scheduled seven-day access to diagnostic
services, typically ultrasound, computerised tomography (CT), magnetic resonance imaging
(MRI), echocardiography, endoscopy, and microbiology. Consultant-directed diagnostic tests
and completed reporting will be available seven days a week:
Within 1 hour for critical patients
Within 12 hours for urgent patients
Within 24 hours for non-urgent patients
Standard Six - Hospital inpatients must have timely 24-hour access, seven days a week, to key
consultant-directed interventions that meet the relevant specialty guidelines, either on-site
or through formally agreed networked arrangements with clear written protocols. These
interventions would include:
Critical care
Interventional radiology

Greater Manchester Health and Social Care Partnership
42
Interventional endoscopy
Standard Eight - All patients with high dependency needs should be seen and reviewed by a
consultant twice daily (including all acutely ill patients directly transferred and others who
deteriorate). Once a clear pathway of care has been established, patients should be reviewed
by a consultant at least once every 24hours, seven days a week, unless it has been
determined that this would not affect the patient’s care pathway.
Arrangements are already in place for sector working to facilitate the delivery of these standards at
some of the sites that do not currently have them in place. The challenge moving forward will be to
deliver all these standards at all the appropriate sites. Further clinical engagement will be required to
determine how GM can deliver access to a seven day specialist respiratory advice, and the
establishment of a GM on-call rota will form part of those discussions.
The model of care will be required to meet all relevant standards set out in Appendix H and in
addition meet standards such as Acute Non-Invasive Ventilation National standards at the sites
where this is delivered.

Greater Manchester Health and Social Care Partnership
43
6.R E C O M M E N D A T I O N S
6.1. Theme 3 – Acute & Specialised Care
It is critical that, in the short term, transformation in respiratory services focuses on the need to maintain responsive, emergency care across hospital sites for patients with respiratory disease. Patients will continue to present at their local hospital when experiencing acute symptoms of respiratory disease, and therefore local secondary services must remain accessible.
Whilst accessibility is a key aspect of any new respiratory care model, there are a number of
opportunities to reduce variation and escalation, including:
Opportunity to standardise the respiratory pathway, and to ensure appropriate emergency
triage, particularly where patients are experiencing breathlessness;
It is recommended that GM adopts a single model for COPD care;
An accessible Pulmonary rehabilitation service is commissioned for the population to a basic
standard to include delivery during acute admissions;
The development of community services to include suitably skilled outreach enabling patients
to access appropriate care and support when they do not require a hospital admission, this
may include specialist nurses or Allied Health Professionals (AHPs) with enhanced skills;
Creation of a single policy for care of people with influenza and commission centrally;
To gain a clearer understanding of those who present and those who die with a pneumonia
diagnosis and an agreed GM-wide policy for diagnosis;
Implementation of learning from programmes such as the Future Hospitals project to build
teams to deliver the new model;
To plug the education gap in primary and secondary care by providing opportunities for
patient review, potentially utilising the virtual clinic model described later in this document;
There is a need to explore the benefits of provision of psychosocial support for patients with
chronic respiratory disease and ensure the provision of peer support groups and social
prescribing;

Greater Manchester Health and Social Care Partnership
44
Any impact from Theme 1 public health awareness is felt in the long or very long term, services will
require further review.
6.2. Summary of Financial and Operational Efficiency Benefits
By implementing the above recommendations GM would:
Improve further the number of bed days used for all patients as they will receive the best
practice pathway;
Admissions for COPD would not increase despite the increasing aging population as the impact
of increased secondary care support to community services and GPs enables people to be
better managed in their own homes;
A reduction people waiting in hospital for domiciliary NIV;
A reduction in readmission rates due to improved treatment, outcomes and post discharge
support;
An increase in patient satisfaction due to improved pathway and reduced bed days;
Improved short and long term outcomes, enabling people to return to their families, lives and
work faster, with more support and better informed about their condition than previously.
In turn for influenza model there will also be an:
A reduction in those contracting influenza;
Improvement in the bed days and severity of the influenza for those who require admission;
Reduction in the number who go on to develop pneumonia;
A reduction in the amount of level 2 & 3 critical care required
An improvement in the number of days people are unable to participate in their normal lives,
including childcare, work, etc.
It is recommended that further patient engagement take place during the modelling phase of this
redesign due to the constraints placed by limited time on the breadth and depth of engagement.
.

Greater Manchester Health and Social Care Partnership
45
7.1. Model of Care
Based on equitable, improved access to acute and specialist assessment, diagnosis and treatment
services the recommended GM model of care is designed to improve patient experience and
outcomes, by reducing variation and improving access to essential diagnostics and treatment. To
deliver this a robust clinical network should be formed across all sites where respiratory services are
delivered, to continue to support and enhance the health benefits delivered by a robust public
health, primary and community care model.
7.1.1. Service aims In developing the recommended model of care, the service aims to:
reduce the unwarranted variation currently experienced by patients, their relatives and carers
in Greater Manchester by delivering consistent high-quality care regardless of where patients
access and receive their care in GM;
maximise a patient’s functional capability and quality of life by establishing a service that
offers timely and safe access to appropriate care throughout the whole pathway, including
seamless integration with aspects that are outside of the hospital setting;
implement standardisation in GM of processes identified as offering substantial gains in
productivity and efficiency to drive improvements in the service.
The future service will be delivered through a specialist Respiratory multi-disciplinary team that
works in close collaboration with teams throughout the pathway. This will include forming
relationships with local health and social care providers to help optimise any care provided locally for
the patient. This will include liaison with consultants, GPs, community nurses, social workers, primary
care clinicians, voluntary organisations, patient representatives and health trainers.
7.P R E F E R R E D MO D E L O F CA R E

Greater Manchester Health and Social Care Partnership
46
The service will achieve all the markers of high quality care set out in the NICE quality standard for
patient experience in adult NHS services.
The service will ensure that patients:
are appropriately diagnosed and treated for their condition;
are treated in a safe, clean and confidential environment;
feel well-informed about their diagnosis and the services that they are receiving;
will be treated as a member of the team to make decisions in partnership with the team;
are informed and involved in the decision about the care they receive.
7.1.2. Service objectives The objectives of the future service and model of care will be to achieve the following:
Implementation of all agreed GM Quality Standards;
Ensure equity of access and choice of treatment modalities for the whole GM population
Ensure consistency and uniformity of care, delivering improved patient outcomes and
experience of care for all patients.
Ensure consistent and timely decision making and management planning for all patients.
Ensure most effective use of Greater Manchester NHS and Social Care funding and optimise
the use of existing resources and infrastructure
A networked service that builds on existing established examples of best practice across GM
Optimised care for patients and access to clinical expertise in all cases, including patients with
co-morbidities
A sustainable future-proofed service – ensuring that future model remains viable over the
long-term, and able to withstand any changes such as population growth
or incidence rates.
Secure excellent clinical leadership, team working and real job satisfaction and maximise
opportunities for education, research and innovation to deliver excellent services
Consistent adoption of evidence-based innovation including use of technology
Carry out effective monitoring of patients to ensure that clinical treatment is safe and
effective;

Greater Manchester Health and Social Care Partnership
47
Ensure compliance with Care Quality Commission regulations and a commitment to continual
service improvement;
Provide care with a patient and family centred focus to maximise the patient experience;
Provide high quality information for patients, families and carers in appropriate and accessible
formats and media.
This will ensure that the proposed optimal service configuration can deliver the highest international
standards in clinical outcomes, patient experience, training, research and education for patients,
carers and the next generation of clinicians.
7.2. Governance & Clinical Leadership
The model will require a combined governance to operate effectively. As the model relies on the
delivery of enhanced Theme 1 and 2 care, the relationship between all three themes will need to
remain cohesive and the clinical leadership consistent.
Governance may be managed through existing networks as long as this cohesive, consistent clinical
leadership remains.
7.3. Service Description and Care Pathway
The model of care will focus on three main areas:
1. The development of a COPD model of care, with GM-wide outcomes
2. The identification of a single GM-wide policy framework for Influenza
3. Initial audit of diagnosis of pneumonia and identification of single diagnosis criteria for all GM
patients.

Greater Manchester Health and Social Care Partnership
48
7.4. COPD Model of Care
Patients accessing the COPD care pathway will, in the new model, be either patients with respiratory
problems who are being diagnosed with COPD, or those whose COPD is unable to be managed with
clinical support in their normal place of residence or community setting. This group may include:
People with uncontrolled exacerbations of their COPD
People with significant deterioration in condition who require specialist support
People admitted for other clinical co-morbidities significantly hindering their ability to manage
their COPD whilst acutely unwell
The model will be based on and fully support an improved, enhanced primary and community care
service by delivering specialist nurse outreach to more complex COPD patients unable to be managed
by the GP and community teams, through training of community respiratory nurses and GPs and
through MDT clinics, risk stratification and advice support. This will ensure that only those patients
who require an appropriate admission, acute Non-invasive Ventilation (NIV) and domiciliary NIV
access the Theme 3 service.
Escalation may take place from a number of sources:
GP
Community nurses/ physiotherapists or other AHP
Walk-in-centre
Patient (self-referral or 999 call)
If a GP or community team member initiates the escalation, a call will be made to the secondary care
COPD team who may offer, dependant on the information received, to commence management of
the patient on an enhanced community pathway, supporting the Theme 2 model, to avoid admission.
This pathway will include the advice and support for the GP by the hospital based respiratory
consultant led team and outreach by Specialist Respiratory (Nurse or other appropriately trained
professional) Practitioners (SR(N)P) into the person’s home; either with or additionally to the

Greater Manchester Health and Social Care Partnership
49
community team. The person may be further escalated into an acute inpatient bed at any time by
the respiratory Consultant, GP or SR(N)P.
Should the patient not be suitable for this type of care, either on risk stratification due to severity of
the COPD, home circumstances, or if they have self-presented at the Emergency Department, then
they will be streamed directly into a respiratory pathway. This pathway will also include
resuscitation at various levels, if required, but will begin with access to a senior respiratory clinician.
For those accessing an Emergency Department directly, review by a senior respiratory clinician
(nursing or medical) will take place as soon as possible and patients not requiring admission will be
signposted to the appropriate service. This may include the community services, GP, or enhanced
community services.
Care will be delivered, at all stages, by a respiratory multi-disciplinary team (MDT) with the patient
moving onto a specialist respiratory ward as soon as possible. This ward will be managed with
infections such as chest infections and influenza taken into account, as this is likely to increase the
risk of further deterioration through spread. Prescribing for exacerbation will be managed with the
support of a respiratory pharmacist as per the developing NICE guidance16 and further treatment as
per guidance7.
The person’s baseline will be identified at admission, with the aim to create a plan to discharge and
support the person at home as soon as practicable and where appropriate; looking to return the
person as close to their usual health as possible whilst supported outside the acute environment.
Risk stratification tools will be utilised throughout the pathway to ensure that length of stay is
minimised and that patients at risk of readmission are provided with appropriate support. Pulmonary
rehabilitation, patient education, tobacco control, appropriate oxygen-prescribing and social
prescribing (including review of mental health wellbeing) will be commenced during an acute
16 NICE (2018) Chronic obstructive pulmonary disease (acute exacerbation): antimicrobial prescribing: draft guidance, Via: https://www.nice.org.uk/guidance/indevelopment/gid-ng10115/documents Last accessed: 17/07/18

Greater Manchester Health and Social Care Partnership
50
admission and continue along agreed pathways in primary care. Further clinical consultation is
required within GM to agree which risk stratification tools are used, however it is envisaged that
there will be a consistent and agreed approach. Examples of such tools include the DECAF17 score
(Dyspnea, Eosinopenia, Consolidation on chest x-ray, Acidemia, Atrial Fibrillation) for COPD, which
contributes to informing the development of personalised plan for acute stays.
NIV assessment and acute NIV currently takes place in 10 localities within GM. Further consultation is
required to ensure delivery meets national standards, particularly to address how to achieve
appropriate and timely review by respiratory clinicians, appropriate staff ratios and access to specific
ventilation support areas in the hospitals. Domiciliary NIV will be delivered within each locality that
provides acute NIV in a timely way and to agreed standards, with training and support from the NW
Lung Centre. The services should be limited by the patient’s disease severity, rather than service
availability. It is recommended that a dedicated NIV task group is established to review NIV provision
and develop appropriate pathways for acute and home NIV provision.
All acute sites will offer a consistent tobacco control/smoking cessation service which is linked with
primary care. The CURE programme currently piloted by MFT is an evidence-based, inpatient
treatment for tobacco addiction aimed to increase the chance of long-term smoking cessation by
60%. The pilot is based on the Ottawa Model for Smoking Cessation18 and if successful, this model
will be made available at other GM hospitals. .
Patients admitted with other conditions that render them unable to manage their COPD, will be
monitored by the SRNP and care escalated to a respiratory consultant only if required. A process will
need to be created to alert the MDT to the admission of a person who is unable to manage their
COPD due to other co-morbidities.
17 https://www.mdcalc.com/decaf-score-acute-exacerbation-copd#next-steps 18 https://ottawamodel.ottawaheart.ca/

Greater Manchester Health and Social Care Partnership
51
The MDT, through virtual clinics, outreach services or remote monitoring as appropriate, will support
discharge; this will be delivered as part of the wider MDT including community services, smoking
cessation, pulmonary rehabilitation, GP involvement and social care.
Those within the patient group experiencing psychosocial issues relating to their COPD will be able to
access the appropriate support in their area and this will be commissioned along with physical health
care and social prescribing.
All patients discharged from this service will receive smoking cessation support, influenza and
pneumococci vaccinations as appropriate described in section 7.7 Standard Respiratory Offer.
Figure 14: COPD Model of Care

Greater Manchester Health and Social Care Partnership
52
7.4.1. Workforce Although the numbers of patients with COPD are expected to increase due to the aging population
and lifestyles, the increased community management should see maintenance of numbers attending
acute sites. The development of outreach support for both patients and healthcare practitioners will
require an initial increase in specialist nurses, however, in time, the increased knowledge and skill of
the community teams will enable this number to maintain, despite the increase in people with COPD
and the long term nature of the disease.
Considering this, a different model of workforce will need to be developed, that is able to work
across settings in both acute and community environments.

Greater Manchester Health and Social Care Partnership
53
Table 03: Description of Workforce for COPD Pathway
Role Additional Skills requires
Respiratory
Consultant / Senior
Respiratory Clinician
Virtual clinics
Advice and guidance
Emergency department respiratory care cover
Specialist Respiratory
(Nurse) Practitioner
Spirometry
Basic chest physiotherapy skills
Expertise in inhaler usage
Relevant appropriate pharmaceutical knowledge
Advice & guidance
Training for community teams
Home visits (lone working, decision making, etc.)
Knowledge of other services and how to access them
Remote monitoring
Emergency department respiratory care cover
Ability to immunise
Oxygen prescription
Pulmonary
Rehabilitation
Support
Working in an acute setting
Pulmonary Rehabilitation links to community
Smoking Cessation training
Allied Health Occupational Therapy
Physiotherapy
Pharmacist-immunisation, smoking cessation, inhaler advice
Radiology
Voluntary groups
Professional patients

Greater Manchester Health and Social Care Partnership
54
Where skills or roles are not available, GM will need to identify how and when this training is
accessed or provided. The respiratory network group would identify this with support from the
Respiratory Strategic Clinical Network (SCN).
7.4.2. Access to service The Theme 3 COPD Service will only be accessed if all other avenues have been considered and
judged inappropriate. If a patient attends directly at the Emergency Department they will be seen by
a specialist respiratory clinician who will then make a decision as to whether admission is appropriate
or the patient should be treated elsewhere. If admission is not considered appropriate the patient
will be referred to the community COPD service; if the patient is admitted they will go straight to a
specialist respiratory service.
Figure 15: Flow Chart of Access to COPD Secondary Care

Greater Manchester Health and Social Care Partnership
55
7.4.3. Transition to Implementation
It is anticipated that this would need to be delivered in stages, with some aspects being more
straightforward than others.
Where good practice already exists in some CCGs, for example virtual clinics, we would see this rolled
out across the whole of GM as commissioning arrangements were being agreed. It is recognised that
some aspects of the implementation (e.g. virtual clinics) may only need to be made available for a
finite period depending on the needs of each practice, and in the long term, frequency will be
reviewed and reduced as necessary.

Greater Manchester Health and Social Care Partnership
56
Where training would be required to develop roles, this would also be identified and commissioned
at the onset.
An outline plan for implementation will be created once the model has been agreed by an engaged
DOF and CRG.
7.5. GM Framework for Influenza
A single GM-wide framework will be created to describe how GM will manage those with suspected
or diagnosed influenza, education and communication regarding influenza, along with an influenza
immunisation plan for the vulnerable and their carers - both paid and unpaid - and a pneumococcal
immunisation plan for the most vulnerable.
Centrally commissioned, influenza management will commence much earlier in the year, with
vaccinations as soon as available, ideally over August and September. These will be offered free of
charge to the following groups:
People 65 years of age or over
Those who are pregnant
People with certain medical conditions (Appendix I)
Those living in a long-stay residential care home, nursing care or other long-stay or group living
care facility
Those who receive a carer's allowance, or you are the main carer for an elderly or disabled
person whose welfare may be at risk if you fall ill
Healthcare workers
*Medical and nursing students
*Social care workers who have regular contact with the vulnerable groups
Children – Age 0 – 9 or as evidence describes

Greater Manchester Health and Social Care Partnership
57
As the availability of pneumococcal vaccination is often significantly reduced in comparison to the
influenza vaccine, it will only be offered to the most vulnerable. This will include:
People 65 years of age or over
People with certain medical conditions
Those living in a group living or other long-stay care facility
A GM-wide protocol to include swabbing, point of care testing for influenza, the use of CRP testing,
and use of antivirals based on best practice and NICE guidance19 is currently being developed by the
Strategic Clinical Network in conjunction with Public Health England.
Reducing the severity of the influenza reduces the likelihood of development of pneumonia and
reduces the severity of the disease, improving outcomes, patient experience and saving the NHS a
significant amount financially.
Each Trust should have a plan to cohort patients with influenza based on intelligence and in line with
the GM/Public Health plan. Work is currently underway with regards to the Flu pathway and advice
about locality wide plans should be made for the cohorting and management of people presenting
with suspected influenza and other respiratory tract infections as per guidance. .
Any patients admitted with influenza will receive smoking cessation support and pneumococci
vaccination as appropriate as described in section 7.7 Standard Respiratory Offer.
7.6. Pneumonia
* New groups to receive Influenza Vaccine
19NICE (2008) Oseltamivir, amantadine (review) and zanamivir for the prophylaxis of influenza Via:
https://www.nice.org.uk/guidance/ta158 Last accessed: 17/07/18

Greater Manchester Health and Social Care Partnership
58
The treatment and management of pneumonia is a clearly defined pathway indicated in NICE
guidance20 as is the diagnosis.
The model of care is focussed on two groups of patients:
those patients with Hospital Acquired Pneumonia (HAP)
those diagnosed with pneumonia on admission to hospital
Some patients diagnosed with Pneumonia in the community may receive their treatment, including
intravenous (IV) antibiotics through the enhanced services provided by Theme 2.
It is recognised that there are a number of pneumonia codes which complicate the pneumonia
picture and in turn skews pneumonia mortality. Anecdotal evidence comparing local pneumonia
audits to RightCare data suggests that there may be a difference between those cases which fulfil the
NICE definitions of pneumonia and those reported as death due to pneumonia. It is likely that there
is a subgroup of frailty and end of life care within the pneumonia cohort that merits further
investigation going forward.
7.6.1. Hospital Acquired Pneumonia As with most other respiratory conditions, Hospital-Acquired Pneumonia (HAP) diagnosis and
treatment will be required at each acute site. Unlike others types of pneumonia, HAP can be
prevented in some instances by appropriate cohorting of vulnerable patients and ensuring they are
not exposed to patients with chest infections, including influenza. This may prove difficult during
times of high demand, including winter months, but effort should be taken to limit or reduce
exposure.
Diagnosis is traditionally required through culture of lower respiratory tract secretions and White
Blood Cell Count alongside chest X-ray, pulse oximetry and pyrexia, however other diagnostic
investigations may be considered including Computerised Tomography (CT) of the Chest. NICE21 and
20
NICE (2016) Pneumonia Via: https://pathways.nice.org.uk/pathways/pneumonia Last accessed 17/07/18
21 NICE (2018) Management of Hospital Acquired Pneumonia Via: https://pathways.nice.org.uk/pathways/pneumonia#content=view-
node%3Anodes-management-of-hospital-acquired-pneumonia Last accessed 06/09/18

Greater Manchester Health and Social Care Partnership
59
accepted best practice22 guidance describe the antibiotic therapy required for those patients and
although these patients are at a higher risk of contracting infections from antibiotic resistant
organisms23, this particularly rises when the patient is ventilated, further increasing their risk of
pneumonia.
This guidance is widely accepted and implemented across GM and practice - in most instances - meet
the required standard for this cohort. Further work, however, needs to be done to reduce the
incidence of HAP, other Hospital Acquired Infections (HAI), particularly influenza, and increased
exacerbation of existing respiratory disease. A model of care describing the standard offer for all
patients admitted to a hospital with any form of respiratory disease, infectious or chronic is based on
the initial COPD pathway of assessment, risk stratification, application of national standards and
appropriate intervention including tobacco control, vaccination and education. Further clinical
engagement is required to agree these pathways.
7.6.2. Diagnosis of Pneumonia on Admission Diagnosis of pneumonia will necessitate a Chest X-ray and, where possible, culture of lower
respiratory tract secretions and White Blood Cell Count as described in NICE Guidance18. Further
clinical consensus is required as to the diagnosis at end of life where chest infection is common,
however, frailty may be an overwhelming feature. Antibiotic therapy as described by the Greater
Manchester Medicines Management Group (GMMMG), will be prescribed unless contraindicated.
It is envisaged that risk stratification tools will be employed, with clinical consensus, to help
determine those who can be safely cared for in the community with or without extra support. Those
who require an appropriate inpatient admission will be reviewed by the respiratory team and be
cared for on a respiratory ward where appropriate according to stratification.
22 BMJ Best Practice, Hospital Acquired Pneumonia Via: https://bestpractice.bmj.com/topics/en-gb/720 Last accessed 06/09/18 23 Rotstein C, Evans G, Born A, Grossman R, Light B, Magder S, McTaggart B, Weiss K, Zhanel G G (2008) Clinical practice guidelines for
hospital-acquired pneumonia and ventilator-associated pneumonia in adults. Canadian Journal of Infectious Diseases and Medical Microbiology. 19(1); pg 19-53 Via https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2610276/ Last Accessed 06/09/2018

Greater Manchester Health and Social Care Partnership
60
Those people who are recognised to be at the end of life should be managed through an Individual
Care Plan with involvement of the family and/or carers. It is envisaged that further engagement is
required to define the most appropriate pathway. Delivery of this care should take into account both
patient and carer wishes as well as service delivery requirements, for should involve support from
relevant services such as palliative care and oxygen provision.
Any patients admitted with pneumonia, if appropriate, will receive smoking cessation support,
influenza and pneumococci vaccination as described in section 7.7 Standard Respiratory Offer.
7.7. Standard Respiratory Offer
Each patient admitted to hospital with a respiratory disease will be offered a number of interventions
whilst they are inpatients. These will be aimed at improving health and wellbeing, reducing the risk
of infection and increasing self-management of the disease.
The offer will include where appropriate:
i. Influenza vaccination
ii. Pneumonia vaccination
iii. Smoking Cessation support in line with Greater Manchester Medicines Management
Guidelines (GMMMG)
iv. Pulmonary rehabilitation including exercise, nutritional advice, inhaler technique, patient
education as appropriate
v. Psychosocial support
vi. Family/ carer Involvement
It is anticipated that this will capture those people who have not either had the offer of vaccination
or have refused vaccination due to not enough information or understanding about the vaccines,
thus reducing both the number people with influenza and severity of disease as less people contract
and spread both influenza and pneumonia.

Greater Manchester Health and Social Care Partnership
61
Smoking Cessation as described in section 7.4 is one of the few interventions that can improve
COPD24&25, reduce the risk of Lower Respiratory tract Infections (LRTI)26, and reduce the impact of
diseases such as pneumonia and influenza27. As such it is imperative to offer wherever possible. The
patient survey demonstrates that only half of those patients who smoke were offered smoking
cessation support, demonstrating a need to improve access to the offer.
The benefits of pulmonary rehabilitation are again well evidenced and the advantage of commencing
this programme as an inpatient long understood. By creating this package of care, used to the
appropriate extent for all respiratory inpatients, it is anticipated that the number of bed days,
severity, impact and risk of further deterioration will reduce. Aspects of pulmonary rehabilitation
will be agreed within GM by a clinical and commissioner panel and will include evidence based face
to face, virtual, and visual material as appropriate (Section 7.9). Standards for inclusion will be
agreed through the SCN and will be based on British Thoracic Society Guidelines28. It is recognised
that uptake of pulmonary rehabilitation is historically poor and may need to be delivered in a more
attractive way. Long term health benefits and educational packages should involve self-help tools,
social isolation strategies, carers and the voluntary sector.
As these interventions all require skills existing within the workforce at all levels, there would only be
a requirement for further spread of skills rather than extra staffing or resources.
Whilst vaccinations will occur in the hospital this is a cohort of patients identified and budgeted for
vaccination in the community, so this will only require a shift in resource.
24 Tønnesen P (2013) Smoking cessation and COPD. European Respiratory Review Via:
http://err.ersjournals.com/content/22/127/37 Last accessed 06/09/18 25
Willemse B, Postma D S, Timens W, ten Hacken N (2004) The impact of smoking cessation on respiratory symptoms, lung
function, airway hyperresponsiveness and inflammation. European Respiratory Journal 2004 23: 464-476 Via: http://erj.ersjournals.com/content/23/3/464.long Last accessed 06/09/18 26 Saldias F & Diaz O (2010) Cigarette Smoking and Lower Respiratory Tract Infection. Via:
https://www.intechopen.com/books/bronchitis/cigarette-smoking-and-lower-respiratory-tract-infection Last accessed 06/09/18 27 Wong CM, Yang L, Chan KP, Chan WM, Song L, Lai HK, Thach TQ, Ho LM, Chan KH, Lam TH, Peiris JS. (2013) Cigarette smoking as a risk
factor for influenza-associated mortality: evidence from an elderly cohort. Influenza and Other Respiratory Viruses, 2013 Jul;7(4):531-9 Via: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5855151/ Last Accessed 06/09/18 28 https://www.brit-thoracic.org.uk/document-library/clinical-information/pulmonary-rehabilitation/bts-guideline-for-pulmonary-rehabilitation/

Greater Manchester Health and Social Care Partnership
62
Psychological support for the person living with long term disease or coming to terms with a terminal
disease will be offered. Alongside this any social or other wellbeing needs will be considered and
referrals, assessments and introductions will take place as expeditiously as possible.
Family and carer involvement in aspects of the persons diagnosis, prognosis and health education
will be considered individually for each patient.
The delivery of the Standard Respiratory Offer for all respiratory inpatients should therefore be cost
neutral, save for some training regarding smoking cessation and pulmonary rehabilitation
conversations. The benefits will deliver a reduction in readmissions and hospital bed days, improved
health and self-management.
7.8. Service Access Requirements
To access the COPD pathway each patient will receive a diagnosis of COPD from a , using quality
assured Spirometry, and ensuring other causes of airflow obstruction are ruled out as described in
the NICE guidance29
The COPD service described will be delivered to the appropriate service standards and
specifications. Changing thresholds for escalation and sharing knowledge and expertise can achieve
reductions in admissions, readmissions and bed days for those we do admit.
Future pathway improvements based on developments in clinical expertise, pharmacology or
technology can be more efficiently implemented due to the increased communication and support
across Theme 2 and 3.
29 NICE (2018) Chronic obstructive pulmonary disease in over16s: diagnosis and management, Via:
https://www.nice.org.uk/guidance/gid-ng10026/documents/short-version-of-draft-guideline Last accessed 17/07/18

Greater Manchester Health and Social Care Partnership
63
Specialist and emergency care will be more easily available to these vulnerable patients and if they
do enter hospital it will be with a reduced risk of hospital acquired respiratory tract infections or
pneumonia.
Travel and access is an important consideration for patients and carers and accessibility needs to be
considered in relation to the travel implication for patients, as many are unable to travel or walk
longer distances.
Influenza cohorts for vaccination will be identified by their GP, or employer, or in the case of carers
the Department of Work and Pensions. A GM-wide campaign will be created to not only identify
those people but also encourage them to take up the opportunity.
7.9. Follow up and aftercare
Support of the person at home following discharge will look to return the person to as close to their
baseline as is practicable whilst supported outside the acute environment by community teams. This
care will be enhanced where required by Specialist Respiratory Nurses, based in the hospital, but
providing both in-reach and outreach services will provide initial support, and be available as an
ongoing source of expertise to the community teams.
Wherever possible the use of technology will be incorporated into the pathway. This will take on a
number of forms:
Video conferencing – used for both MDT and advice, more use will be made of video calls to
engage with GPs and other clinicians, both in the community and across provider sites;
Telephone/ tablet applications – Apps may be used to remind clinicians of investigations,
referral methods or other pathway criteria both during implementation. They may also be
used by patients to monitor or manage their condition on discharge, to commence and
participate in cardiac rehabilitation, or to receive requests or instructions from the clinicians;

Greater Manchester Health and Social Care Partnership
64
Monitoring – pulse and oxygen saturation can be l monitored remotely. Wherever possible
these and any other appropriate observations will be delivered remotely allowing the patient
as little disruption as possible to their day-to-day life, improving outcomes and wellbeing by
creating reassurance without anxiety. Results will be monitored by specialist nursing staff,
escalating to consultants only when required.
As other forms of technology are developed they will be reviewed by the network group and
incorporated into the pathway as appropriate.
Patient Reported Outcome Measure (PROMS) will be used to understand the efficacy and impact of the model of
care, Pulmonary Rehabilitation and Theme 2/3 interface.
7.10.Audit, Research and Education
By creating a single model and set of standards for care there will be increased continuity of clinical
audit. The Board will be able to deliver the oversight and identify areas of focus for both junior
doctor and senior clinical audit. There will be increased GM-wide understanding of area outcomes
and where these differ from expected, audits will focus on these, alongside the standard audits.
Share care across Theme 2 and 3 creates significant opportunities for education amongst medical,
nursing and allied healthcare professionals. The network will work with the deaneries of various
universities to create training opportunities for hospital physicians, GPs, junior doctors, nurses,
radiologists and other allied health professionals.

Greater Manchester Health and Social Care Partnership
65
8.F I N A N C I A L CO N S I D E R A T I O N S
There are a number of financial considerations immediately evident from the model described above
the detail will only become evident once the full impact is understood and a full cost benefit analysis
will be completed at that time.
8.1. Financial principles for Theme 3
The development of the Future Model of Care will be underpinned by the following set of principles,
agreed by the Theme 3 Finance and Estates Reference Group (FERG) in September 2017.
8.1.1. Financial impact:
Demonstrable positive recurrent revenue impact across the GM Health & Social care system
when compared to actual current delivery;
Stranded costs should be minimised, and a clear distinction should be drawn between
cashable and non-cashable benefits;
Financial savings should not be achieved at the expense of achieving appropriate clinical
outcomes;
To access Transformation Fund funding, be able to demonstrate a positive return on
investment within four years.
8.1.2. Estates impact:
Seek to make best use of ALL existing estate in order to minimise costs;
The use of empty/under-utilised estate where costs are fixed/have already been committed
should be a priority;
Stranded capacity and associated costs should be minimised;
Capital will not be granted to build new hospital estate unless either:
Existing estate is appropriately utilised; or
Building new estate is demonstrably better value for money than repurposing existing empty
estate.

Greater Manchester Health and Social Care Partnership
66
8.1.3. Workforce impact:
Additional workforce costs (e.g. redundancy and re-training costs) should be kept to a
minimum;
Expenditure on non-substantive posts should be reduced in so far as appropriate;
Agency costs should only be incurred after due consideration has been given as to whether
new/vacant substantive posts should be covered by agency staff or whether it may be
appropriate to delay implementation and recruit to the post substantively.
8.2. Logic modelling for financial impact of new model of care
Key:
* Timescale column: Timescales in this column are from the point of decision to implement, not from submission of this paper. ǂ Financial impact columns:
↑ = cost increases for providers/commissioners (as indicated) ↓ = cost decreases for providers/commissioners (as indicated) ↔ = no significant cost increase/decrease for providers/commissioners (as indicated)
± Direct Impacts column:
↑ = quantity increases ↓ = quantity decreases ↔ = no significant impact on quantity
Intervention… Drives… Direct impacts…
± Timescale *
Confidence
Financial impact on
providers ǂ Financial impact on
commissioners ǂ
COPD
Accessible COPD model of networked service supporting Theme 2
Better clinical outcomes for patients and shorter lengths of stay
Quality targets ↑
Greater achievement of
Best Practice Tariff improves
income
↓ Fewer
readmissions from variable practice
↓
Capacity usage ↓
Less use of inpatient beds
(but ? Cashable) ↓
Fewer admissions for planned
investigations ↓
Workforce demand ↑
Demand on existing
workforce will increase in the
short to medium term
↑
Reduced number of outpatient attendances
↓

Greater Manchester Health and Social Care Partnership
67
Staff working across sectors
Equipment & workforce
Short term↑
Long term ↓
Improved access and use of diagnostic
equipment
↑ Reduced number of investigations
carried out ↓
Reduced patient transfers as expertise on site
Patient delays in discharge ↓
Reduced delays and bed usage
↓ Reduced number
of spells ↓
Influenza
Standardised key processes for Influenza management
Improved immunization reduces incidence
NHS Activity ↓ Reduced activity and admission
↓
Purchasing vaccine ↑
Increased initial outlay on
vaccine will reduce
admissions
↑
Time spent in hospital ↓
Faster diagnosis
Less use of inpatient beds
(but ? Cashable)
Reduced variation in
delivery
↓
Reduction in the number of patients treated in level 2 &
3 care
↓
Use of level 2&3 HDU & ICU ↓
Reduction in hospital acquired infections
Time spent in hospital↓
Reduced LoS for vulnerable
patients
(but ?cashable)
↓
Pneumonia
Standardisation of treatment of HAP
Standardised treatment as described in NICE
Variation in treatment↓
Possible increased
demand for diagnostic activity
↑
Standard Respiratory Offer
Influenza & Pneumonia vaccinations, smoking cessation & pulmonary rehabilitation
All respiratory patients to receive appropriate offer
Readmissions↓
Bed Days↓
Admissions↓
Short Term
Long Term
Reduction in readmissions
Reduction in admissions
↓ Reduced number
of spells ↓
The combined impact of the full implementation of the model will see:
A reduction in admissions A reduction in bed days across all sites A reduction in unnecessary testing Some increase in cost of vaccinations

Greater Manchester Health and Social Care Partnership
68
Reduction in costs associated with high dependency care Reduction in admissions due to outreach service A reduction in outpatient costs due to use of healthcare technology in remote monitoring

Greater Manchester Health and Social Care Partnership
69
9. KEY ENABLERS & CRITICAL SUCCESS FACTORS
9.1. Enablers
To deliver this model, based on improved patient experience, improved outcomes and reduced long-
term costs, there are a number of enabling factors that are key to deliver:
9.1.1. Further Engagement with Clinicians and Patients Although the project team has initiated clinical and patient engagement, the limited amount of time
has given limited opportunity for full and widespread engagement and involvement in the
development of this model. It is therefore proposed that the project team continue to engage
clinical colleagues and patients following agreement of the model of care.
With full engagement the further modelling, workforce and delivery phases of the project will be
more effectively and efficiently delivered.
9.1.2. Commissioning across GM As COPD and influenza services will be providing care delivered to a single set of principles/ policy for
patients across all CCGs, the service will require commissioning in a different way. By creating single
commissioning criteria across all of GM, based on basic standards and outcomes, those issues that
may have arisen, due to individual locality commissioning will not be possible.
9.1.3. Supporting Theme 2 whist still sustaining Theme 3. Much of the work that has been developed to date across GM has focussed on out of hospital care of
COPD patients. This has generally included an element of secondary care, either support or delivery,
in the community. Theme 3 acknowledges the need for cross-theme working and supports the aims
of the other pieces of work, but acknowledges the finite workforce currently delivering care in the
acute and specialist setting.
Plans will be made to support the community and primary care developments, whilst maintaining the
services within the hospital, and this will include the up-skilling and multi-skilling of the specialist
nurse, physiotherapy and pharmacy workforce, to allow them to undertake roles currently requiring
two or three different professionals.

Greater Manchester Health and Social Care Partnership
70
9.1.4. Workforce Current difficulties in recruiting respiratory physicians and specialist nurses will significantly hinder
the delivery of the preferred model. This difficulty is, in part, due to the lack of appropriately trained
workforce available and, as part of the GM respiratory development, it is required that GM will
identify and work with local further education establishments to create opportunities for training in
these particularly affected roles.
Sharing existing skills and services across GM without the need to increase workforce, will create a
sustainable, future-proof respiratory GM network of care.
Further consideration of the voluntary sector and their role needs to be explored in particular to
social isolation.
9.1.5. Use of Technology The delivery of an improved COPD service can only be sustained through the increased use of
technology including remote monitoring, developments in NIV and virtual clinics and educational
tools. As part of the governance for the model the respiratory network will be required to assess and
recommend new technologies and equipment that will support continued delivery within GM.
9.2. Critical Success Factors
The critical success factors of the model are primarily focused on the people affected by the model.
Figure 16: Critical success factors for respiratory redesign

Greater Manchester Health and Social Care Partnership
71
The most critical factors include the engagement of those affected by the redesign. Confidence in
the model and implementation support can be created by ensuring that patients, clinicians, nurses,
and other AHPs, the organisations (including the healthcare Trusts, GPs, social care and NWAS), and
professional groups, are involved in the process of formal agreement of the model, modelling and
delivery planning.
The Project and Clinical Lead therefore recommended that a more comprehensive design and
engagement period be entered into to ensure smooth transition into the next phase of the redesign.
ENGAGEMENT
Actively involving those affected by the change in co-design, including
patients
TRUST
Developing trust between all groups
involved by honest and open discourse
OPENNESS
Transparency in both design and decision making will create
further Trust
PATIENT FOCUSSED
Developing pathways with patients and for patients listening to their priorities and
needs
IMPROVED OUTCOMES
Creating a service that delivers improved
clinical, patient experience,
perfornance and financial outcomes

Greater Manchester Health and Social Care Partnership
72
10.AP P E N D I C E S
10.1.Appendix A - Supporting Data
Respiratory medicine involves the diagnosis and treatment of conditions affecting the respiratory
system. Conditions that are diagnosed and treated under respiratory services include:
Chronic Obstructive Pulmonary Disease (COPD)
Asthma
Obstructive Lung Disease
Pneumonia
Upper and Lower Respiratory Tract Infections (RTI) including Tuberculosis
Influenza
Bronchitis
Bronchiectasis
Interstitial Lung Disease (ILD) including Idiopathic Pulmonary Fibrosis
Cystic Fibrosis
Acute Respiratory Distress Syndrome
Respiratory Failure
Pleural Effusion
Lung cancer
Sleep disorders
Occupational Lung Disease
10.1.1.Admissions The figure below illustrates how inpatient admissions (elective and non-elective) for respiratory are
split between different sites in GM. Note that inpatient respiratory admissions were also recorded at:
Manchester Royal Eye Hospital, St Mary’s Hospital, Leigh Infirmary and Manchester Skin Care North
Hub – but as their volume was much lower than the other sites (20 episodes or less) they have not
been included in the figure below.

Greater Manchester Health and Social Care Partnership
73
Figure 16: Respiratory adult inpatient admissions 16/17
© Health and Social Care Information Centre – HES Data 2016/17
From the above figure it is evident that there is a clear variation in Respiratory related activity
across all of the GM sites. Wythenshawe Hospital is clearly accountable for the majority of
activity. You can also break these figures down further into elective and non-elective
admissions:
For elective admissions, there is an even more pronounced variation in Respiratory related
activity. Wythenshawe once again clearly accounts for the majority of activity; with almost
2,000 more episodes than the next highest site, Royal Bolton Hospital (see Appendix A Figure
16).
For non-elective (emergency) admissions, variation in Respiratory activity still exists, although
it is less pronounced than when compared to elective admissions. Wythenshawe still
accounts for the highest amount of activity (see Appendix A Figure 17).

Greater Manchester Health and Social Care Partnership
74
An analysis of day case episodes also shows a similar level of variation across GM sites. Once again,
Wythenshawe clearly accounts for the highest amount of day case activity, with over 1,200 more
episodes than the next highest site, North Manchester General Hospital.
Respiratory activity can also be grouped by CCG for GM. This is shown in the figure below:
Figure 17: Respiratory adult inpatient episodes 16/17
© Health and Social Care Information Centre – HES Data 2016/17
From the above figure it should be noted that:
Even though those residing in South Manchester CCG account for 4,941 inpatient episodes of
the respiratory activity across GM its corresponding hospital site, Wythenshawe, accounts
for over 12,591 inpatient episodes. This means that, potentially, over 7,500 inpatient
episodes at Wythenshawe Hospital come from outside the nearest CCG.
Conversely, even though those residing in Trafford CCG account for 5,998 episodes of
respiratory activity across GM its corresponding hospital site, Trafford General only accounts
for 1,167 inpatient episodes. This means that, potentially, over 4,800 residents of Trafford
CCG do not use Trafford General for inpatient respiratory admissions.

Greater Manchester Health and Social Care Partnership
75
This could imply that in certain cases, residents of a particular CCG may not be opting to use their
nearest hospital to access inpatient respiratory services and may instead be using inpatient services
elsewhere in GM.
10.1.2.Length of Stay
The figure below shows the average length of stay for elective respiratory inpatient admissions
across the different hospital sites in GM:
Figure 19: Average LoS for elective inpatient 16/17
© Health and Social Care Information Centre – HES Data 2016/17 *Note that Leigh Infirmary, St Mary’s, Rochdale Infirmary and Manchester Skin Care also recorded 1 admission each, but have not been included on the figure due to their low admission numbers being potentially skewed by outliers.
From the above figure a clear variation in terms of length of stay can be observed, with the longest
average length of stay at Tameside General, at a value of 10.4 days. There is a variation in average
length of stay of 8.8 days between the sites in the above figure.

Greater Manchester Health and Social Care Partnership
76
Figure 20: Average inpatient length of stay for non-elective 16/17
© Health and Social Care Information Centre – HES Data 2016/17 Note that St Mary’s and Manchester Royal Eye Hospital had a much lower number of admissions compared to the rest of the sites (6 and 10 admissions respectively) and have not been included as their average lengths of stay are potentially more subject to being strongly skewed by outliers.
From the above figure, variation in average length of stay in a non-elective setting can also be
observed. There is variation in average length of stay of 7.0 days between the GM sites in the above
figure.
It is worth noting however, for both elective and non-elective average length of stay, that the above
two graphs do not take into account factors such as the distribution of age and sex, or the case
complexity, of individual patients visiting these sites or the community based services currently
available.
10.1.3.LOS – COPD National data suggests that hospitals should target an average LOS of 4 days for COPD, and work is
clearly needed to bring GM in line with that ambition. The National COPD Audit Programme’s 2017

Greater Manchester Health and Social Care Partnership
77
report30 notes that, for patients discharged alive after a spell in hospital for COPD, mortality is higher
within 30 days of admission, and higher still at 90 days.
Figure 21: Summary detail from COPD audit
30 file:///C:/Users/rnoble/Downloads/COPD%20-%20Who%20cares%20when%20it%20matters%20most.%20Results%20and%20data%20analysis%20(1).pdf

Greater Manchester Health and Social Care Partnership
78
10.2.Appendix B - Table 6: Population of CCGs at mid-point 201631
CCG Population Size (mid 2016)
NHS Manchester CCG 541,263
NHS Wigan Borough CCG 323,060
NHS Stockport CCG 290,557
NHS Bolton CCG 283,115
NHS Tameside and Glossop CCG 256,424
NHS Salford CCG 248,726
NHS Trafford CCG 234,673
NHS Oldham CCG 232,724
NHS Heywood, Middleton and Rochdale CCG
216,165
NHS Bury CCG 188,669
31 Office for National Statistics, Clinical Commissioning Group, Mid Year Population Estimate 2016 via: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/clinicalcommissioninggroupmidyearpopulationestimates Last accessed: 18/07/18

Greater Manchester Health and Social Care Partnership
79
10.3.Appendix C - Right Care, Commissioning for Value; Pathway on a page

Greater Manchester Health and Social Care Partnership
80

Greater Manchester Health and Social Care Partnership
81

Greater Manchester Health and Social Care Partnership
82
10.4.Appendix D – Clinical COPD Audit Participants
Eleven GM sites participated in this audit:
Fairfield General Hospital (Pennine Acute Trust);
Manchester Royal Infirmary (MFT);
North Manchester General Hospital (Pennine Acute Trust);
Royal Albert Edward Infirmary (WWLFT);
Royal Bolton Hospital (Bolton Foundation trust);
Royal Oldham Hospital (Pennine Acute Trust);
Salford Royal (SRFT);
Stepping Hill Hospital (Stockport Foundation Trust);
Tameside General Hospital (Tameside Hospital Foundation Trust);
Trafford General Hospital (MFT);
Wythenshawe Hospital (UHSM).

Greater Manchester Health and Social Care Partnership
83
10.5.Appendix E – Attendance Sheet at COPD Workshop
Lead: Dr Jennifer Hoyle
Facilitated: Alex Vincent

Greater Manchester Health and Social Care Partnership
84
10.6.Appendix F - Patient Questionnaire

Greater Manchester Health and Social Care Partnership
85

Greater Manchester Health and Social Care Partnership
86

Greater Manchester Health and Social Care Partnership
87

Greater Manchester Health and Social Care Partnership
88

Greater Manchester Health and Social Care Partnership
89

Greater Manchester Health and Social Care Partnership
90

Greater Manchester Health and Social Care Partnership
91

Greater Manchester Health and Social Care Partnership
92

Greater Manchester Health and Social Care Partnership
93
10.7.Appendix G - Clinical Co-dependencies
10.7.1.Services Required by Respiratory Services: Respiratory services have numerous clinical co-dependencies, specifically:
Serv
ice
sh
ou
ld b
e c
o-l
oca
ted
(bas
ed
in s
ame
sit
e a
nd
can
be
acce
sse
d w
ith
in 1
hr
Serv
ice
sh
ou
ld c
om
e t
o p
atie
nt
(pat
ien
t tr
ansf
er
no
t
app
rop
riat
e),
2-2
4hrs
. Co
uld
be
pro
vid
ed
by
visi
tin
g/in
-re
ach
fro
m a
no
the
r si
te (
ph
ysic
ally
, or
via
tele
com
m li
nks
) if
no
t b
ase
d
at t
he
sam
e s
ite
Ide
ally
on
sam
e s
ite
bu
t co
uld
alte
rnat
ive
ly b
e n
etw
ork
ed
via
rob
ust
em
erg
en
cy a
nd
ele
ctiv
e
refe
rral
an
d t
ran
sfe
r p
roto
cols
Do
es
no
t n
ee
d t
o b
e o
n s
ame
site
- m
anag
ed
via
ap
pro
pri
ate
refe
rral
pro
cess
No
t re
qu
ire
d
C O P D
Sen
ior
Re
spir
ato
ry P
hys
icia
ns
Cri
tica
l Car
e L
eve
ls 2
&3
Spe
cial
ist
Re
spir
ato
ry N
urs
e
Eme
rge
ncy
De
par
tme
nt
Hae
mat
olo
gy
Spir
om
etr
y
Co
ho
rte
d b
ed
s
NIV
Rad
iolo
gy
Rad
iolo
gy
NIV
Acu
te g
en
era
l in
tern
al m
ed
icin
e
Ph
ysio
the
rap
y
Mic
rob
iolo
gy
Spe
cial
ist
Ph
arm
acis
t
Pal
liat
ive
Car
e
Smo
kin
g C
ess
atio
n
Pu
lmo
nar
y R
eh
abil
itat
ion
Car
dio
resp
irat
ory
se
rvic
es
Spe
cial
ist
Nu
rse
Ou
tre
ach
Occ
up
atio
nal
Th
era
py
Soci
al C
are
Do
mic
ilia
ry N
IV
Pro
gram
me
d In
vest
igat
ion
Un
it
Car
dio
logy
Rh
eu
mat
olo
gy
Spe
ech
an
d L
angu
age
Th
era
py
Ou
tpat
ien
t D
ep
artm
en
t
ENT
All
erg
y Se
rvic
es
Imm
un
olo
gy
Infl
ue
nza
imm
un
isat
ion
Pn
eu
mo
cco
cial
imm
un
isat
ion
Oxy
gen
Se
rvic
e
The
atre
s
On
colo
gy
I N F L U E N Z A
Sen
ior
Re
spir
ato
ry P
hys
icia
ns
Cri
tica
l Car
e L
eve
ls 2
&3
Acu
te g
en
era
l in
tern
al m
ed
icin
e
Spe
cial
ist
Re
spir
ato
ry N
urs
e
Hae
mat
olo
gy
Mic
rob
iolo
gy (
swab
bin
g)
Co
ho
rte
d b
ed
s
Inte
nsi
vist
s
Rad
iolo
gy
Ph
ysio
the
rap
y
Spe
cial
ist
Ph
arm
acis
t
Smo
kin
g C
ess
atio
n
Pu
lmo
nar
y R
eh
abil
itat
ion
Car
dio
resp
irat
ory
se
rvic
es
Soci
al C
are
Occ
up
atio
nal
Th
era
py
Pn
eu
mo
cco
cial
imm
un
isat
ion
Infl
ue
nza
imm
un
isat
ion
Imm
un
olo
gy
Spir
om
etr
y
NIV
Rh
eu
mat
olo
gy
Pro
gram
me
d In
vest
igat
ion
Un
it
Spe
ech
an
d L
angu
age
Th
era
py
Ou
tpat
ien
t D
ep
artm
en
t
All
erg
y Se
rvic
es
Oxy
gen
Th
era
py
The
atre
s
On
colo
gy
P N E U M O N I A
Sen
ior
Re
spir
ato
ry P
hys
icia
ns
Cri
tica
l Car
e L
eve
l 2&
3
Acu
te g
en
era
l in
tern
al m
ed
icin
e
Spe
cial
ist
Re
spir
ato
ry N
urs
e
Hae
mat
olo
gy
Mic
rob
iolo
gy
Rad
iolo
gy
Inte
nsi
vist
s
Ph
ysio
the
rap
y
Spe
cial
ist
Ph
arm
acis
t
Smo
kin
g C
ess
atio
n
Pu
lmo
nar
y R
eh
abil
itat
ion
Car
dio
resp
irat
ory
se
rvic
es
Ocu
pat
ion
al T
he
rap
y
Soci
al C
are
Infl
ue
nza
imm
un
isat
ion
Pn
eu
mo
cocc
ial i
mm
un
isat
ion
Spe
ech
an
d L
angu
age
Th
era
py
Pn
eu
mo
cco
cial
imm
un
isat
ion
Infl
ue
nza
imm
un
isat
ion
Spir
om
etr
y
NIV
Co
ho
rte
d b
ed
s
Rh
eu
mat
olo
gy
Pro
gram
me
d In
vest
igat
ion
Un
it
Imm
un
olo
gy
Ou
tpat
ien
t D
ep
artm
en
t
All
erg
y se
rvic
es
Oxy
gen
se
rvic
e
The
atre
s
On
colo
gy

Greater Manchester Health and Social Care Partnership
94
All Reparatory services require access to a number of diagnostic specialities:
Laboratory medicine – all sites providing acute, secondary or tertiary care for respiratory
patients will require access to a full suite of laboratory medicine tests. These will need to be
responsive, accurate and both point-of-care and centralised (locally or regionally) testing
should be incorporated into care.
Radiology – plain imaging, ultrasound, CT and MRI are all used for diagnosis and access along
with radiologist reporting is essential. How this is organised will depend on the model of
care.
Other specialities including cardiology and geriatric medicine may be required as the number of
people with both cardiac and respiratory disorders increases and incidence of the disease increases
beyond 75yrs.
10.7.2.Supporting other dependent services/specialties Respiratory medicine is required at all acute sites, although this may be an on-call respiratory
consultant rather than a clinician on site 24/7. Sites without an A&E may only require access to a
respiratory consultant for advice and guidance and this could be managed through virtual or
telephone contact.
Sites with cardiology services will also need access to respiratory clinicians due to the often synergies
between cardiac and respiratory disease; the level of access would depend on the acuity of the site.
Outpatient sites would require access to advice and virtual MDT, inpatient to respiratory physicians
able to see the patient on site.
Community & primary care will benefit from access to a respiratory specialist due to the expectancy
of increased referral thresholds for COPD and increased community management, which will enable
the delivery of care to the required standards. All models considered will only succeed if the
threshold of community manageable conditions increases.

Greater Manchester Health and Social Care Partnership
95
Secondary care respiratory consultants would support this by participating in virtual MDTs or clinics
alongside the GP and community clinicians, to enable appropriate advice and guidance is available as
required to optimise the health of the individual patients and therefore reduce the need for hospital
admissions.

Greater Manchester Health and Social Care Partnership
96
10.8.Appendix H - Service Standards
There are a number of sources available for respiratory standards and guidance, which requires
consideration and, where appropriate, incorporation into the model of care.
10.8.1.Royal College of Physicians (RCP) The RCP have one guideline useful in this project, “Non-invasive ventilation in chronic obstructive
pulmonary disease”32, however this again focuses on acute NIV, so does not inform the domiciliary
NIV standard.
10.8.2.British Lung Foundation (BLF) Whilst the BLF don not produce guidance for professionals, their information and guidance to the
patients and families of those affected by respiratory disease is clear and should be considered,
particularly when developing a more detailed GM standard for pulmonary rehabilitation. Effort will
be taken to combine the recommendations of BLF into any model produced.
10.8.3.British Thoracic Society (BTS) Standards of Care Committee The BTS have release a number of standards of care pertinent to this project33:
•Guideline for oxygen use in healthcare and emergency settings;
•Guidelines for Home Oxygen Use in Adults;
•Non-invasive ventilation in acute respiratory failure;
•Guidelines for the Management of Community Acquired Pneumonia in Adults;
•Guideline on Pulmonary Rehabilitation in Adults.
Alongside these there are also a number of quality standards that have been considered whilst
creating the outline model34. They include:
32 Royal College of Physicians Non-invasive ventilation in chronic obstructive pulmonary disease. Via:
https://www.rcplondon.ac.uk/guidelines-policy/non-invasive-ventilation-chronic-obstructive-pulmonary-disease Last accessed 19/7/18 33 British Thoracic Society Guidelines. Via: https://www.brit-thoracic.org.uk/standards-of-care/guidelines/ Last accessed 19/07/18 34 Britich Thoracic Society Quality Standards. Via: https://www.brit-thoracic.org.uk/standards-of-care/quality-standards/ Last accessed
19/7/18

Greater Manchester Health and Social Care Partnership
97
BTS Hope Oxygen Quality Standards;
BTS NIV Quality Standards;
BTS Pulmonary Rehabilitation Quality Standards.
These give clear direction as to the standards expected from the relevant aspects of the model, and
will be incorporated in at all stages of development. However the focus on acute NIV means this
standard is not relevant for domiciliary NIV.
10.8.4.Seven Day Services In 2015 NHS England (NHSE) published ‘Seven Day Services Clinical Standards’ in relation to hospital-
based care. An update of this document was published in September 201735 and contains
recommendations in relation to cardiology-based services. The state that inpatients must have
timely 24-hour access, seven days a week, to key consultant-directed interventions that meet the
relevant specialty guidelines, either on-site or through formally agreed networked arrangements
with clear written protocols. With regards to respiratory, this includes critical care, interventional
radiology and endoscopy. Whilst all sites currently adhere to this standard, it is important that we
consider the implications through the lens of Healthier Together and any future model to realign
inpatient beds or interventions.
10.8.5.National Institute of Health and Care Excellence (NICE) Guidance exists for the following respiratory conditions pertinent to this project36:
Chronic obstructive pulmonary disease
Pneumonia
Respiratory conditions: general and other
Respiratory infections
35 Seven Day Services Clinical Standards, 2017, NHS England 36 NICE Guidance for respiratory conditions. Via: https://www.nice.org.uk/guidance/conditions-and-diseases/respiratory-conditions
Last accessed 19/7/18

Greater Manchester Health and Social Care Partnership
98
Sleep apnoea and snoring
Management of Hospital Acquired Pneumonia
From this guidance particular attention has been paid to ensure the outline meets a minimum
standard of the guidance set out for COPD, Pneumonia and where appropriate Respiratory
conditions: general and other, and Respiratory Infections. Sleep apnoea and snoring remains of
interest due to the use of NIV as a treatment for this condition.
10.8.6.Getting It Right First Time
The GIRFT programme is a national programme commissioned by the Department of Health to
identify areas of unwarranted clinical variation and divergence from best practice. GIRFT has
appointed a clinical lead for their respiratory workstream, and whilst they have published reports
relating to other work streams, a Respiratory report has not been released37.
37 GIRFT Respiratory care via: http://gettingitrightfirsttime.co.uk/medical-specialties/respiratory/ Last accessed 19/7/18

Greater Manchester Health and Social Care Partnership
99
10.9.Appendix I – Free Vaccination for Influenza
NHS Choices38 list those who should have free vaccines.
“The injected flu vaccine is offered free of charge on the NHS to anyone with a serious long-term
health condition, including:
chronic (long-term) respiratory diseases, such as asthma (which requires an inhaled or tablet
steroid treatment, or has led to hospital admission in the past), chronic obstructive
pulmonary disease (COPD), emphysema or bronchitis
chronic heart disease, such as heart failure
chronic kidney disease
chronic liver disease, such as hepatitis
chronic neurological conditions, such as Parkinson's disease, motor neurone
disease or multiple sclerosis (MS)
diabetes
problems with your spleen – for example, sickle cell disease or if you have had your spleen
removed
a weakened immune system as the result of conditions such as HIV and AIDS, or
medication such as steroid tablets or chemotherapy
being seriously overweight (BMI of 40 or above)
This list of conditions isn't definitive. It's always an issue of clinical judgement.”
38 NHS Choices, Who should have the flu jab? Via: https://www.nhs.uk/conditions/vaccinations/who-should-have-flu-vaccine/ Last Accessed 17/07/18

Greater Manchester Health and Social Care Partnership
100
10.10.Appendix J - Abbreviations Table
Abbreviation Description
BLF British Lung Foundation
CCG Clinical Commissioning Group
CMFT Central Manchester Foundation Trust
COPD Chronic Obstructive Pulmonary Disease
GIRFT Getting it Right First Time
GMHSCP Greater Manchester Health and Social Care Partnership
GM Greater Manchester
HAP Hospital Acquired Pneumonia
HES Hospital Episode Statistics
ILD Interstitial Lung Disease
IPF Idiopathic Pulmonary Fibrosis
LoS Length of Stay
MRI Manchester Royal Infirmary
NICE National Institute for Health and Care Excellence
NIV Non-invasive Ventilation
NWLC North West Lung Centre
PAHT Pennine Acute Hospitals NHS Trust
RCP Royal College of Physicians
RTI Respiratory Tract Infection
SRN Specialist Respiratory Nurse
SRFT Salford Royal Foundation Trust
UHSM University Hospital of South Manchester
WWL (FT) Wrightington Wigan and Leigh Foundation Trust

Greater Manchester Health and Social Care Partnership
101
10.11 Feedback log
Governance group Feedback Response / Action
CRG1 Focus for Pneumonia should be on Hospital Acquired
Focus narrowed until DOF when discussion required widening of model to include all hospital admissions with pneumonia
CRG2 All patients require a set of interventions including smoking cessation and vaccinations
A single respiratory offer created within the model
CRG3 Influenza standards should be managed through Theme 1
This has been incorporated into the model of care
CRG4 Clear NIV standards should be agreed
Further work needed to agree standards
CRG5
CRG outcome Endorse the case for change to go to the Theme 3 Executive
Governance group Feedback Response / Action
FERG1 No fundamental changes in delivery
FERG2
FERG3
FERG outcome
Governance group Feedback Response / Action
WRG1 Lack of detailed information about GM requirements for workforce
Added some information to case for change and noted for inclusion in models of care
WRG2
WRG3
WRG outcome
Governance group Feedback Response / Action
ECAP1 Pneumonia proposals need further clarity
Updated to reflect the need for compliance with NICE guidance in the

Greater Manchester Health and Social Care Partnership
102
diagnosis and management of pneumonia, which is the first step towards ensuring that pneumonia is only cited as the cause of death where there is a primary diagnosis. This is the starting point in addressing the panel’s feedback that clinical coding and data accuracy are critical to informing a true picture of disease incidence.
ECAP2 Point of care testing for Influenza is imperative
The model has been updated to clarify the need for point of care testing and the isolation of patients with suspected influenza. The document will continue to reflect the capacity challenges associated with providing adequate isolation in times of high demand.
ECAP3 NIV standards and domiciliary care require further development
NIV standards are now referenced in the document, though further GM-wide engagement is needed to determine the final NIV model for GM.
ECAP4 Chest infection management of the COPD patient needs to be considered
Updated to reflect this.
ECAP5 Smoking cessation standards need to be agreed
This work is ongoing in GM and the document has been updated to reflect this. Reference has also been made to the GM CURE programme, which is based on the Ottawa Model for Smoking Cessation.
ECAP6
Fundamentally the proposed model of care is sound and would benefit from focusing on the COPD element of the pathway in the next stage of development
No changes required to the document.
ECAP7
Risk stratification Emergency
Departments and Acute Medical Units
and access to specialist respiratory
clinicians are important inclusions in
further iterations of the model of care
GM Trusts already use a range of risk stratification tools, and further clinical engagement is required to assess the available evidence and determine the most appropriate tools for adoption GM-wide.
ECAP8
Implementing this model of care will require very strong and credible medical leadership and buy in from senior NHS managers if such a profound transformation is to succeed.
No changes required to the document.

Greater Manchester Health and Social Care Partnership
103
ECAP outcome
Governance group Feedback Response / Action
T3E1 Needs further engagement Patient focus groups, questionnaire and DOF completed and outcomes included in the model
T3E2 Single commissioner approach to influenza needs clarification
Model amended to describe single set of standards across GM not single commissioner
T3E3 NIV hub & spoke model needs clarity
NIV to be managed through standards set by clinical experts at the hub and delivered a spoke sites. Not all sites require NIV, but one per sector.
T3E4 Consolidation and rationalisation is unclear
Consolidation of services limited to NIV
T3E5 Lack of clarity on the pathway There is no single pathway, each condition will require its own model
T3E6 The balance of advocating substantial shift of activity to out of hospital needs to be clear
Commissioning Lead and Theme 2 GMHSCP engaged, work continuing through SCN
Theme 3 Executive outcome
Governance group Feedback Response / Action
Theme 3 Board outcome