
Cartilage Lesions of the Patella: Management After … Cartilage...Cartilage Lesions of the Patella:...
5
310 COPYRIGHT © SLACK INCORPORATED Section Editor: Darren L. Johnson, MD n sports medicine update Cartilage Lesions of the Patella: Management After Acute Patellar Dislocation Adam V. Metzler, MD; Christian Lattermann, MD; Darren L. Johnson, MD P atellar dislocations are common knee injuries, and in patients younger than 16 years, the annual incidence is 43/100,000. 1 Risk factors for patellar dislocation include patella alta, family history, previous dislocation, troch- lear dysplasia, and high Q- angle. 2 Fithian et al 3 reported a 17% redislocation rate after a first-time patellar dislocation and a 50% rate after a second dislocation. The main concern with each dislocation is the re- petitive trauma to the articular cartilage of the patellofemo- ral joint potentially leading to early osteoarthritis. In the setting of an acute patellar dislocation, most au- thors would suggest nonsur- gical treatment for first-time dislocations. Exceptions to this include osteochondral fracture, substantial disruption of the medial patellar stabiliz- ers, a laterally subluxed patella with normal alignment of the contralateral patella, a second dislocation, or a patient who is not improving with appropri- ate rehabilitation. 4 When com- paring medial patellofemoral ligament (MPFL) reconstruc- tion with repair, a recent sys- tematic review showed that there was a statistically sig- nificantly higher failure rate among those who underwent MPFL repair (26.9%) than those who underwent recon- struction (6.6%) or medial retinacular repair/plication (16.5%). 5 Common sequelae of acute patellar dislocations are chon- dral and osteochondral inju- ries to the patella or the lateral femoral condyle. The reported rate of chondral injury after patellar dislocation has been reported to be as high as 95%. 6,7 Nomura et al 7 reported that, after acute patellar dislo- cations in 39 patients, 17% of patellar lesions had chondral or osteochondral fracturing, 23% had cracks (fissures), and 54% had lesions with both frac- turing and cracks (fissures). 7 These chondral lesions may cause swelling, pain, mechani- cal symptoms, and functional impairment. The complexity of the patellofemoral joint and high shear forces, in addition to the avascularity of articu- lar cartilage, makes treatment challenging. 8,9 This article discusses the challenges faced when attempting to treat acute chondral/osteochondral inju- ries after acute patellar dislo- cations. CASE REPORT A 16-year-old starting high school football player sustained a valgus load to his left knee from another player’s helmet. He had no previous history of patellar instability or knee injury. He presented with a diffusely swollen knee and significant lateral patellar apprehension. Radiographs showed a well-centered pa- The authors are from Commonwealth Orthopaedic Centers (AVM), Edge- wood; and the Department of Orthopaedic Surgery (CL, DLJ), University of Kentucky School of Medicine, Lexington, Kentucky. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Darren L. Johnson, MD, De- partment of Orthopaedic Surgery, University of Kentucky School of Medi- cine, 740 S Limestone St, K-415 Kentucky Clinic, Lexington, KY 40536-0284 ([email protected]). doi: 10.3928/01477447-20150504-05 Abstract: Articular cartilage injuries to the patella are fre- quent after patellar dislocation. The management of these acute cartilage injuries in the acute setting can be challenging. It is well documented that acute fixation is the optimal choice for treatment of osteochondral injuries. This article discuss- es the challenges and potential treatment options for acute chondral/osteochondral injuries to the patella after acute pa- tellar dislocation. [Orthopedics. 2015; 38(5):310-314.]
Transcript of Cartilage Lesions of the Patella: Management After … Cartilage...Cartilage Lesions of the Patella:...
310 Copyright © SLACK inCorporAted
Section Editor: Darren L. Johnson, MD
n sports medicine update
Cartilage Lesions of the Patella: Management After Acute Patellar DislocationAdam V. Metzler, MD; Christian Lattermann, MD; Darren L. Johnson, MD
Patellar dislocations are common knee injuries,
and in patients younger than 16 years, the annual incidence is 43/100,000.1 Risk factors for patellar dislocation include patella alta, family history, previous dislocation, troch-lear dysplasia, and high Q-angle.2 Fithian et al3 reported a 17% redislocation rate after a first-time patellar dislocation
and a 50% rate after a second dislocation. The main concern with each dislocation is the re-petitive trauma to the articular cartilage of the patellofemo-ral joint potentially leading to early osteoarthritis.
In the setting of an acute patellar dislocation, most au-thors would suggest nonsur-gical treatment for first-time dislocations. Exceptions to
this include osteochondral fracture, substantial disruption of the medial patellar stabiliz-ers, a laterally subluxed patella with normal alignment of the contralateral patella, a second dislocation, or a patient who is not improving with appropri-ate rehabilitation.4 When com-paring medial patellofemoral ligament (MPFL) reconstruc-tion with repair, a recent sys-tematic review showed that there was a statistically sig-nificantly higher failure rate among those who underwent MPFL repair (26.9%) than those who underwent recon-struction (6.6%) or medial retinacular repair/plication (16.5%).5
Common sequelae of acute patellar dislocations are chon-dral and osteochondral inju-ries to the patella or the lateral femoral condyle. The reported rate of chondral injury after patellar dislocation has been reported to be as high as 95%.6,7 Nomura et al7 reported that, after acute patellar dislo-cations in 39 patients, 17% of
patellar lesions had chondral or osteochondral fracturing, 23% had cracks (fissures), and 54% had lesions with both frac-turing and cracks (fissures).7 These chondral lesions may cause swelling, pain, mechani-cal symptoms, and functional impairment. The complexity of the patellofemoral joint and high shear forces, in addition to the avascularity of articu-lar cartilage, makes treatment challenging.8,9 This article discusses the challenges faced when attempting to treat acute chondral/osteochondral inju-ries after acute patellar dislo-cations.
Case RepoRtA 16-year-old starting
high school football player sustained a valgus load to his left knee from another player’s helmet. He had no previous history of patellar instability or knee injury. He presented with a diffusely swollen knee and significant lateral patellar apprehension. Radiographs showed a well-centered pa-
The authors are from Commonwealth Orthopaedic Centers (AVM), Edge-wood; and the Department of Orthopaedic Surgery (CL, DLJ), University of Kentucky School of Medicine, Lexington, Kentucky.
The authors have no relevant financial relationships to disclose.Correspondence should be addressed to: Darren L. Johnson, MD, De-
partment of Orthopaedic Surgery, University of Kentucky School of Medi-cine, 740 S Limestone St, K-415 Kentucky Clinic, Lexington, KY 40536-0284 ([email protected]).
doi: 10.3928/01477447-20150504-05
Abstract: Articular cartilage injuries to the patella are fre-quent after patellar dislocation. The management of these acute cartilage injuries in the acute setting can be challenging. It is well documented that acute fixation is the optimal choice for treatment of osteochondral injuries. This article discuss-es the challenges and potential treatment options for acute chondral/osteochondral injuries to the patella after acute pa-tellar dislocation. [Orthopedics. 2015; 38(5):310-314.]

MAY 2015 | Volume 38 • Number 5 311
n sports medicine update
tella in the trochlea (Figure 1). Lateral radiographs showed a Caton ratio of 1.05 (Figure 2). Emergent magnetic reso-nance imaging (MRI) showed a significant chondral injury to the medial patellar facet con-sistent with an acute patellar dislocation and multiple loose chondral fragments (Figure 3). It appeared that the MPFL was torn in multiple locations. The tibial tubercle-trochlear groove distance was 16 mm. The patient was scheduled for emergent MPFL reconstruc-tion and possible chondral fix-ation. Arthroscopic evaluation showed multiple macerated and ground-up loose bodies, with the largest piece being approximately 2×1.5 cm, in addition to multiple smaller fragments (Figure 4). The full extent of the cartilage injury was not fully appreciated un-til the patella was everted via a medial parapatellar arthroto-my (Figure 5). There was no bone on the backside of any of the cartilaginous pieces, and the larger pieces were macer-ated.
Preoperatively, an exten-sive conversation was had with the family regarding treatment plans. The goal was to acutely repair the chondral injury (if able) and perform an MPFL reconstruction. The fam-ily was made aware that the chondral fragments may not be repairable and were given options for this scenario. In the setting of the inability to repair the chondral fragments, the following options were discussed: (1) microfracture with allograft cartilage aug-mentation (BioCartilage; Ar-
threx, Naples, Florida) and MPFL reconstruction as a single-stage procedure; (2) osteochondral autograft plus MPFL reconstruction as a single-stage procedure; (3) autologous chondrocyte im-plantation (ACI) with MPFL reconstruction in 2 stages; and (4) minced juvenile cartilage implantation (DeNovo NT; Zimmer, Warsaw, Indiana) in addition to MPFL reconstruc-tion in 2 stages. The literature was discussed with the family in detail, and in this case the family elected for a single-stage procedure. The athlete was entering into his senior year of football.
Once it was determined that the chondral injury was unable to be fixed with screw/pin fixation due to the extent of the chondral injury, the family was notified, and they wished to proceed with microfracture with supplemental BioCarti-lage in a single-stage proce-dure. A medial parapatellar ar-throtomy was performed; the patella was everted (Figure 5) and extensive chondral fis-sure was noted with significant instability of the surrounding fissured cartilage. The un-stable cartilage was debrided back to a stable base, creating vertical walls, and the basic principles of a microfracture were followed (Figures 6-7). To augment the microfracture, a novel composite graft con-sisting of platelet-rich plasma and micronized allogenous cartilage fragments (BioCarti-lage) was used (Figures 8-9). The MPFL reconstruction was performed using a gracilis ten-don allograft, and the patient
was placed in a continuous passive motion machine post-operatively.
Therapy included weight bearing as tolerated in a hinged brace locked at 0°, with range of motion from 0° to 45° for the first 4 weeks. After 4 weeks, the brace was unlocked for ambulation, and range of motion was progressed as tol-erated. The patient returned to full competitive sports at 7 months postoperatively in a patella J brace. He had no pain with running, cutting, or foot-ball drills. Range of motion was 0° to 135°, and the patella was stable with no crepitance or apprehension on examina-tion.
DisCussionThe management of acute
focal chondral/osteochondral
injuries after patellar disloca-tions can be challenging. Giv-en its prevalence, these inju-ries should be suspected in all patellar dislocations, especial-ly if the patient presents with a knee effusion. Radiographs, including a sunrise view or a Merchant view, should be ob-tained; however, chondral in-juries may be missed, and an MRI should be considered if the patient has any signs of an intra-articular effusion or me-chanical symptoms.10,11
In the setting of a repair-able chondral/osteochondral fragment, anatomic repair is advised using the most ap-propriate fixation principles, including the options of both absorbable and nonabsorb-able implants that provide compression of the fragment.
Figure 1: Sunrise radiograph of the patella.
Figure 2: Lateral radiograph of the knee.
Figure 3: Axial magnetic resonance image showing a large chondral in-jury to the patella (orange arrow) and large loose body (red arrow).
Figure 4: Loose bodies removed from the knee.
312 Copyright © SLACK inCorporAted
n sports medicine update
Nonabsorbable screws may re-quire removal and potentially takedown of the MPFL recon-struction to gain access to the hardware. Therefore, appro-priate planning for removal is imperative before placement of nonabsorbable implants in the patellofemoral joint. Small defects (<1 cm2) may be asymptomatic and may be appropriate for loose body removal and limited chondro-plasty.12,13 Microfracture may also be performed; however, the literature reports less fa-vorable outcomes for larger lesions in the weight-bearing aspect of the patella.12,13
Off-the-shelf augmenta-tions such as BioCartilage may be a novel option to sup-plement a microfracture in dif-ficult environments such as the patella; however, no clinical data exist on this technology to date.14-19
Osteochondral autograft offers another intraoperative option that can be used in the acute setting; however, this de-pends on the size and location of the defect. With any osteo-chondral autograft, donor-site morbidity remains a concern. An osteochondral autograft transplantation to the patella is technically challenging given the contour of the pa-tella and the depth that can be drilled.20-22
For larger lesions (2-10 cm2), ACI has the most sup-portive literature for chronic patellar cartilage defects.23-28 Gillogly et al27 reported an 83% good-to-excellent result after ACI with anteromedial-ization of the tibial tubercle
for isolated patellar cartilage defects with 5- to 11-year follow-up. However, the study had an overall reoperation rate of 40%.27 Gomoll et al28 per-formed a multicenter study looking at 110 patients with a minimum of 4 years’ follow-up who underwent ACI to the patella; they reported an 86% good-to-excellent result.
In addition to ACI, matrix-assisted autologous chondro-cyte implantation (MACI) has also shown promise in the lit-erature.29 However, although the results show good or very good results in 70% to 86% of patients treated with MACI or ACI to the patella, the results are still not as promising as the 90% good-to-excellent results seen with ACI to the femoral condyles.30-33 At the time of publication, ACI remains an off-label use in the patella, and prospective patients must be informed of this during the consent process.
Particulated juvenile car-tilage implantation (DeNovo NT) can also be an option with the possibility of a single-stage procedure.34-38 Thomp-kins et al36 performed a case series of 15 knee surgeries for grade 4 lesions of the patella treated with DeNovo NT. At an average follow-up of 28 months, mean fill was 89% and the International Cartilage Repair Society cartilage repair assessment score on MRI was nearly normal for all patients. Clinical outcomes scores for International Knee Documen-tation Committee and Knee Injury and Osteoarthritis Out-come Score scales were com-parable with those published
for ACI.36 One limitation is in the acute setting in which a pa-tient is taken to the operating room for possible fixation of a chondral/osteochondral frag-ment; DeNovo NT is often not available acutely. In ad-dition, if the MRI under- or overestimates the size of the defect compared with the in-traoperative findings, then too little or too much implant may be ordered. The lack of long-term literature on DeNovo NT makes insurance approval a major obstacle. Currently in the authors’ practice, if De-Novo NT is used, it is done in a staged procedure so the chondral injury can be appro-priately sized intraoperatively and the appropriate amount of DeNovo NT graft is ordered.
ConClusionOsteochondral injuries to
the patella are relatively com-mon after lateral patellar dis-locations. However, most of these defects are small and can simply be debrided. Manage-ment of acute, large cartilage injuries in the setting of an acute patellar dislocation can present many challenges to the surgeon. Accurate and quick diagnosis of patellar chondral injuries is imperative because the ideal situation is to directly fix all chondral injuries that are unstable. In some cases, the chondral injures are not fixable, and other cartilage restoration techniques must be performed. The case presented in this article shows the com-plex decision making needed for such cases and the impor-tance of shared decision mak-ing with the patient and fam-
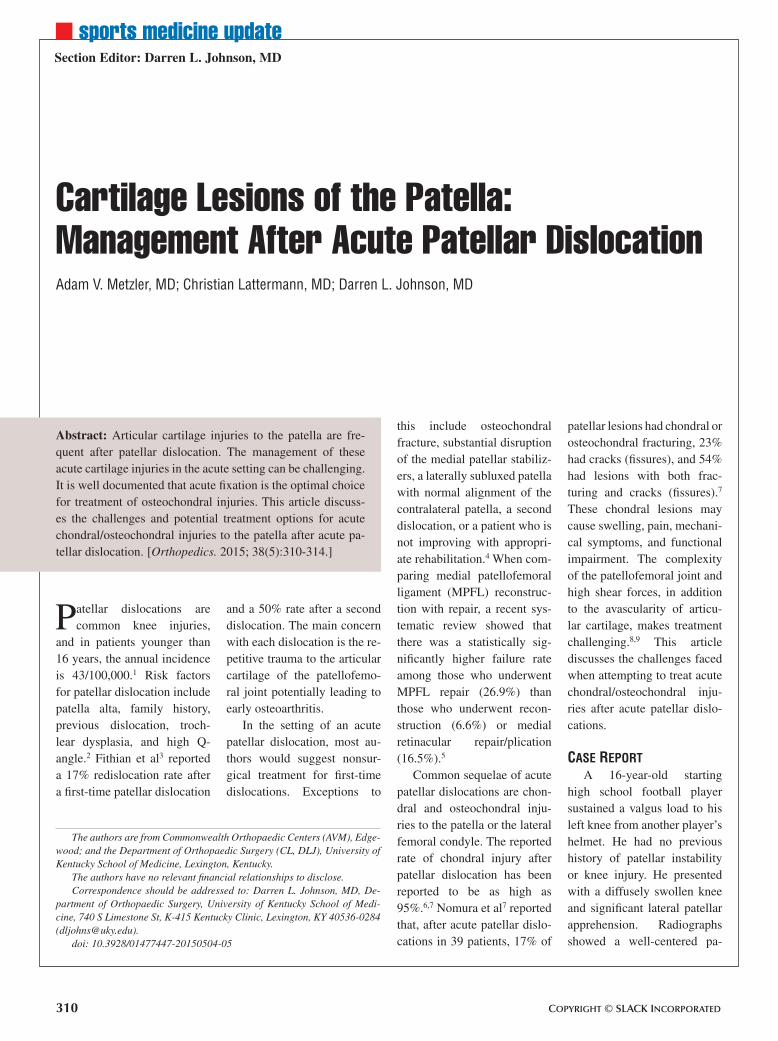
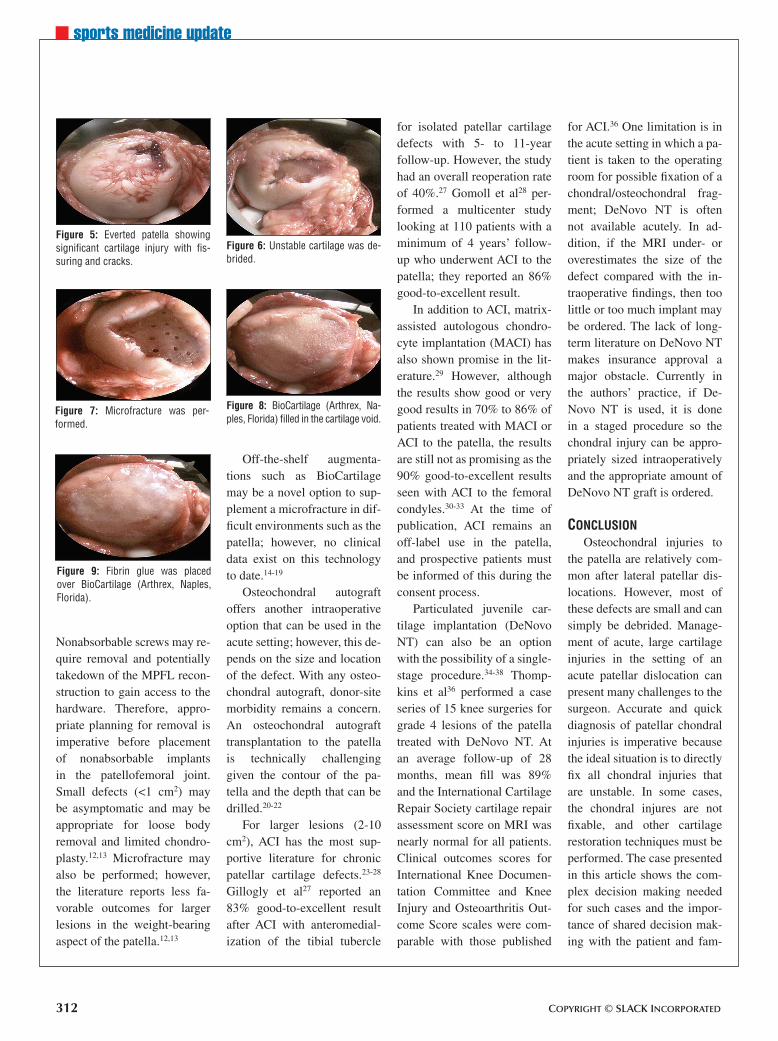
Figure 8: BioCartilage (Arthrex, Na-ples, Florida) filled in the cartilage void.
Figure 7: Microfracture was per-formed.
Figure 5: Everted patella showing significant cartilage injury with fis-suring and cracks.
Figure 6: Unstable cartilage was de-brided.
Figure 9: Fibrin glue was placed over BioCartilage (Arthrex, Naples, Florida).

MAY 2015 | Volume 38 • Number 5 313
n sports medicine update
ily. The surgeon should make every option available and should be comfortable with different cartilage restoration techniques.
Clinical data are available to support ACI or DeNovo NT for chronic patellar car-tilage injuries; however, this cannot be done in an acute setting. There is a paucity of higher-level data for the acute management of chondral in-juries associated with patel-lar dislocations. The literature currently supports nonsurgi-cal management of first-time patellar dislocations, except in the setting of chondral in-juries.4 Microfracture may be a viable option in the acute setting for smaller lesions but may have limited success with larger defects. The addition of graft substitutes to the micro-fracture, such as platelet-rich plasma or BioCartilage, may improve outcomes, as early basic science research shows. However, this still needs to be proven in clinical studies.
RefeRenCes 1. Nietosvaara Y, Aslto K, Kallio
PE. Acute patellar dislocation in children: incidence and as-sociate osteochondral frac-tures. J Pediatr Orthop. 1994; 14(4):513-515.
2. Balcarek P, Walde TA, Frosch S, Schüttrumpf JP, Wachowski MM, Stürmer KM. MRI but not arthroscopy accurately diag-nosis femoral MPFL injury in first-time patellar dislocations. Knee Surg Sports Traumatol Arthrosc. 2012; 20(8):1575-1580.
3. Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med. 2004; 32(5):1114-1121.
4. Stefancin JJ, Parker RD. First-time traumatic patellar dislo-
cations: a systematic review. Clin Orthop Relat Res. 2007; 455:91-101.
5. Matic GT, Magnussen RA, Kolovich GP, Flanigan DC. Return to activity after medial patellofemoral ligament repair or reconstruction. Arthroscopy. 2014; 30(8):1018-1025.
6. Stanitski CL, Paletta GA Jr. Articular cartilage injury with acute patellar dislocations in adolescents: arthroscopic and radiologic correlation. Am J Sports Med. 1998; 26(1):52-55.
7. Nomura E, Inoue M, Kurimura M. Chondral and osteochondral injuries associated with acute patella dislocation. Arthrosco-py. 2003; 19(7):717-721.
8. Hawkins RJ, Bell RH, Anisette G. Acute patellar dislocations: the natural history. Am J Sports Med. 1986; 14(2):117-120.
9. Cash JD, Hughston JC. Treat-ment of acute patellar disloca-tion. Am J Sports Med. 1988; 16(3):244-249.
10. Farr J, Covell DJ, Lattermann C. Cartilage lesions in patello-femoral dislocations: incidents/locations/when to treat. Sports Med Arthrosc. 2012; 20(3):181-186.
11. Lee BJ, Christino MA, Daniels AH, Hulstyn MJ, Eberson CP. Adolescent patellar osteochon-dral fracture following patellar dislocation. Knee Surg Sports Traumatol Arthrosc. 2013; 21(8):1856-1861.
12. Fu FH, Zurakowski D, Browne JE, et al. Autologous chondro-cyte implantation versus de-bridement for treatment of full thickness chondral defects of the knee: an observational co-hort study with 3- year follow-up. Am J Sports Med. 2005; 33(11):1658-1666.
13. Kruez PC, Steinwachs MR, Erggelet C, et al. Results after microfracture of full-thickness chondral defects in different compartments of the knee. Os-teoarthritis Cartilage. 2006; 14(11):1119-1125.
14. Abrams GD, Mall NA, For-tier LA, Roller BL, Cole BJ. BioCartilage: background and operative technique. Oper Tech Sports Med. 2013; 21(2):116-124.
15. Shin JJ, Mellano C, Cvetanov-ich GL, Frank RM, Cole BJ. Treatment of glenoid chondral defect using micronized allo-geneic cartilage matrix implan-tation. Arthrosc Tech. 2014; 3(4):e519-e522.
16. Cole W. BioCartilage use in the 1st MPJ. Podiatry Manage-ment. 2013; 32(5):135-138.
17. Clanton TO, Johnson NS, Ma-theny LM. Use of cartilage extracellular matrix and bone marrow aspirate concentrate in treatment of osteochondral le-sions of the talus. Techniques in Foot & Ankle Surgery. 2014; 13(4):212-220.
18. Desai S. Surgical treatment of a tibial osteochondral defect with debridement, marrow stimulation, and micronized al-lograft cartilage matrix—an all-arthroscopic technique: a case report. J Foot Ankle Surg. 2014; S1067-S2516.
19. Malinin T, Temple HT, Car-penter EM. Induction of regen-eration of articular cartilage de-fects by freeze dried particulate cartilage allografts. Poster pre-sented at: 8th World Congress of the International Cartilage Repair Society (ICRS); May 23-26, 2009; Miami, FL.
20. Hangody L, Kish G, Karpati Z, Eberhardt R. Osteochon-dral plugs: autogenous osteo-chondral mosaicplasty for the treatment of focal chondral osteochondral articular de-fects. Oper Tech Orthop. 1997; 7:312-322.
21. Bentley G, Biant LC, Car-rington RW, et al. A prospec-tive, randomised comparison of autologous chondrocyte im-plantation versus mosaicplasty for osteochondral defects in the knee. J Bone Joint Surg Br. 2003; 85(2):223-230.
22. Bobic V. Arthroscopic os-teochondral autograft trans-plantation in anterior cruciate ligament reconstruction: a pre-liminary clinical study. Knee Surg Sports Traumatol Ar-throsc. 1996; 3(4):262-264.
23. Knutsen G, Engebretsen L, Ludvigsen TC, et al. Autolo-gous chondrocyte implantation compared with microfracture in the knee: a randomized trial. J Bone Joint Surg Am. 2004; 86:455-464.
24. Peterson L, Minas T, Brittberg M, Lindahl A. Treatment of os-teochondritis dissecans of the knee with autologous chondro-cyte transplantation: results at two to ten years. J Bone Joint Surg Am. 2003; 85(suppl 2):17-24.
25. Minas T, Bryant T. The role of autologous chondrocyte im-plantation in the patellofemoral joint. Clin Orthop Relat Res. 2005; 436:30-39.
26. Farr J. Autologous chondrocyte implantation improves patello-femoral cartilage treatment out-comes. Clin Orthop Relat Res. 2007; 463:187-194.
27. Gillogly SD, Arnold RM. Au-tologous chondrocyte implan-tation and anteromedialization for isolated patellar articular cartilage lesions: 5- to 11-year follow-up. Am J Sports Med. 2014; 42(4): 912-920.
28. Gomoll AH, Gillogly SD, Cole BJ, et al. Autologous chondro-cyte implantation in the patella: a multicenter experience. Am J Sports Med. 2014; 42(5):1074-1081.
29. Filardo G, Kon E, Andriolo L, Di Martino A, Zaffagnini S, Marcacci M. Treatment of “patellofemoral” cartilage le-sions with matrix-assisted autologous chondrocyte trans-plantation: a comparison of pa-tellar and trochlear lesions. Am J Sports Med. 2013; 42(3):626-633.
30. Minas T, Bryant T. The role of autologous chondrocyte im-plantation in the patellofemoral joint. Clin Orthop Relat Res. 2005; 436:30-39.
31. Moseley JB Jr, Anderson AF, Browne JE, et al. Long term durability of autologous chon-drocyte implantation: a multi-center, observational study in US patients. Am J Sports Med. 2010; 38(2):238-246.
32. Niemeyer P, Steinwachs M, Erggelet C, et al. Autologous chondrocyte implantation for the treatment of retropatellar cartilage defects: clinical re-sults referred to defect locali-sation. Arch Orthop Trauma Surg. 2008; 128(11):1223-1231.
33. Peterson L, Vasiliadis HS, Britt-berg M, Lindahl A. Autologous chondrocyte implantation: a

314 Copyright © SLACK inCorporAted
n sports medicine update
long-term follow-up. Am J Sports Med. 2010; 38(6):1117-1124.
34. Farr J, Cole BJ, Sherman S, Karas V. Particulated articu-lar cartilage: CAIS and De-Novo NT. J Knee Surg. 2012; 25(1):23-29.
35. Bonner KF, Daner W, Yao JQ.
2-year postoperative evaluation of a patient with a symptomatic full-thickness patellar cartilage defect repaired with particu-lated juvenile cartilage tissue. J Knee Surg. 2010; 23(2):109-114.
36. Tompkins M, Hamann JC, Di-duch DR, et al. Preliminary results of a novel single-stage
cartilage restoration technique: particulated juvenile articular cartilage allograft for chondral defects of the patella. Arthros-copy. 2013; 29(10):1661-1670.
37. Coetzee JC, Giza E, Schon LC, et al. Treatment of osteo-chondral lesions of the talus with particulated juvenile car-tilage. Foot Ankle Int. 2013;
34(9):1205-1211.
38. Farr J, Tabet SK, Margerrison E, Cole BJ. Clinical, radiographic, and histological outcomes after cartilage repair with particulat-ed juvenile articular cartilage: a 2-year prospective study. Am J Sports Med. 2014; 42(6):1417-1425.


















