Carrie de Moor, MD Associate Medical Director/ED Trauma Director JPS Health Network 4/21/2012.
45
EMERGENCY AIRWAY MANAGEMENT UPDATE Carrie de Moor, MD Associate Medical Director/ED Trauma Director JPS Health Network 4/21/2012
-
Upload
elijah-nelson -
Category
Documents
-
view
216 -
download
0
Transcript of Carrie de Moor, MD Associate Medical Director/ED Trauma Director JPS Health Network 4/21/2012.

EMERGENCY AIRWAY MANAGEMENT UPDATE
Carrie de Moor, MDAssociate Medical Director/ED Trauma Director
JPS Health Network4/21/2012

Objectives
Recognize potential difficult airways Review Techniques for Advanced Airway
Management Understand options for sedation in RSI
during a national shortage of Etomidate Become familiar with new advanced
airway management tools

The Decision to Intubate
Poor oxygenation or ventilation Inability to protect the aiway (Decreased
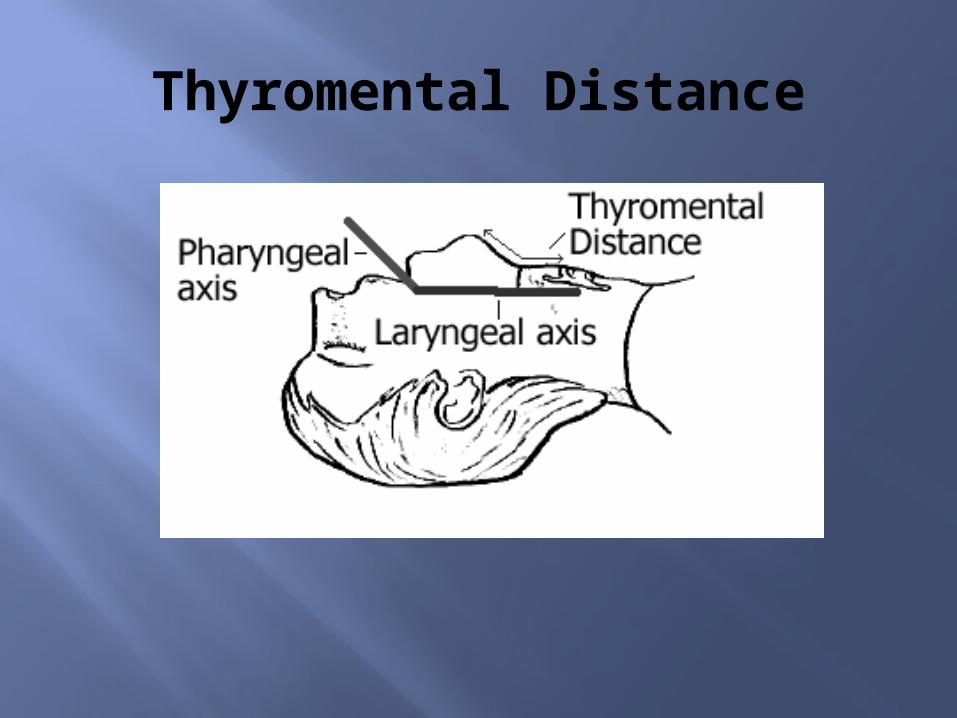
LOC/GCS, secretions, swelling, severe facial trauma)
Potential for rapid deterioration Patient/Staff safety ( The acutely agitated
patient)

The Ideal Intubation Setup
Positioning Assistance at bedside (nursing/RT) Time to prepare and plan Fasting patient Ability to abort the procedure Anesthesia/surgical back up available

The Ideal Patient for Intubation
Intact, clear airway Wide open mouth Pre-Oxygenated Intact respiratory drive Normal dentition Normal and Easily identifiable anatomy Good Neck Mobility

Identifying the Difficult Airway
This ideally should occur before you attempt!
Review Past Medical History Physical Exam
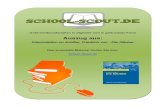
Mallampati Classification Thyromental Distance Obvious deformities/Trauma Signs of obstruction Neck Mobility

Important Past Medical Conditions to Know!
Previous Difficult Intubations Previous Surgical Airway Congenital Conditions- Pierre Robin
Syndrome Arthritis- Rheumatoid, Ankylosing
Spondylitis Prior C-spine/Neck Surgeries Head and Neck tumors

Mallampati Classification

If you see this…. Be Concerned
Thyromental Distance
Somethings are obvious…

More Physical Exam Cues
Limited Neck Mobility Facial Instability Burns Obesity or very small. Short Muscular neck Receding Jaw Signs of Anaphylaxis Stridor/FBAO Scars from Previous Surgeries
More Questions to Ask Yourself
Is there blood in the airway? Is the patient actively vomiting? Are there teeth missing? Is there clinical suspicion for Epiglottitis,
RPA, or Ludwig’s Angina? Is the patient immobilized?

Clues this might not go so well…


Now you know….

Preparing for the Difficult Airway
Consider Alternatives for Airway Support CPAP/BiPAP Call Backup/Intubation in controlled OR setting
Prepare for need to change equipment Different blades Different tube sizes Bougie LMA/Combitube Advanced Airway Equipment- Glidescope,
Fiberoptics etc Prepare for Surgical Airway

Techniques to Remember
Sellick’s Maneuver/Cricoid Pressure ( +/-) BURP maneuver Good Positioning- Sniff position Always have a bougie in your pocket Cricothyrotomy
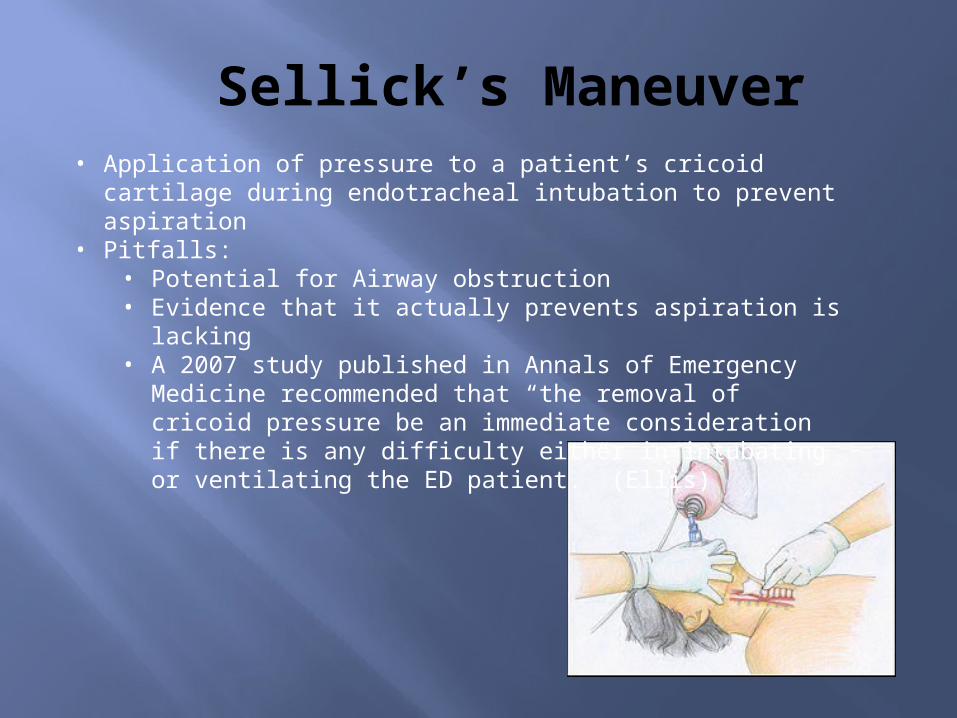
Sellick’s Maneuver• Application of pressure to a patient’s cricoid cartilage during
endotracheal intubation to prevent aspiration• Pitfalls:
• Potential for Airway obstruction • Evidence that it actually prevents aspiration is lacking• A 2007 study published in Annals of Emergency Medicine
recommended that “the removal of cricoid pressure be an immediate consideration if there is any difficulty either in intubating or ventilating the ED patient.” (Ellis)

BURP
BURP : “backward-upward-rightward pressure” of the larynx Displaces the thyroid cartilage dorsally so that
the larynx is pressed against cervical vertebrae’s body
Ideally two centimeters in cephalic direction, until resistance is felt
Next it should be displaced 0.5 cm -2.0 cm rightward
When used with Sellick’s may actually worsen view

Ideal Positioning
Sniffing Position First Described in 1936 by Bannister and
MacBeth- to align oral, pharyngeal, laryngeal axes to provide optimal exposure of the glottis
Pitfalls: Inadequate for the morbidly obese patient, not an option with suspected cervical spine injury


Positioning for the Obese Patient
Ear-to-sternal notch positioning improves the mechanics of ventilation, both with spontaneous breathing, and with mask ventilation.
In the obese patient: shoulders are elevated, the head and neck are extended, and the external auditory meatus is in line with the sternal notch
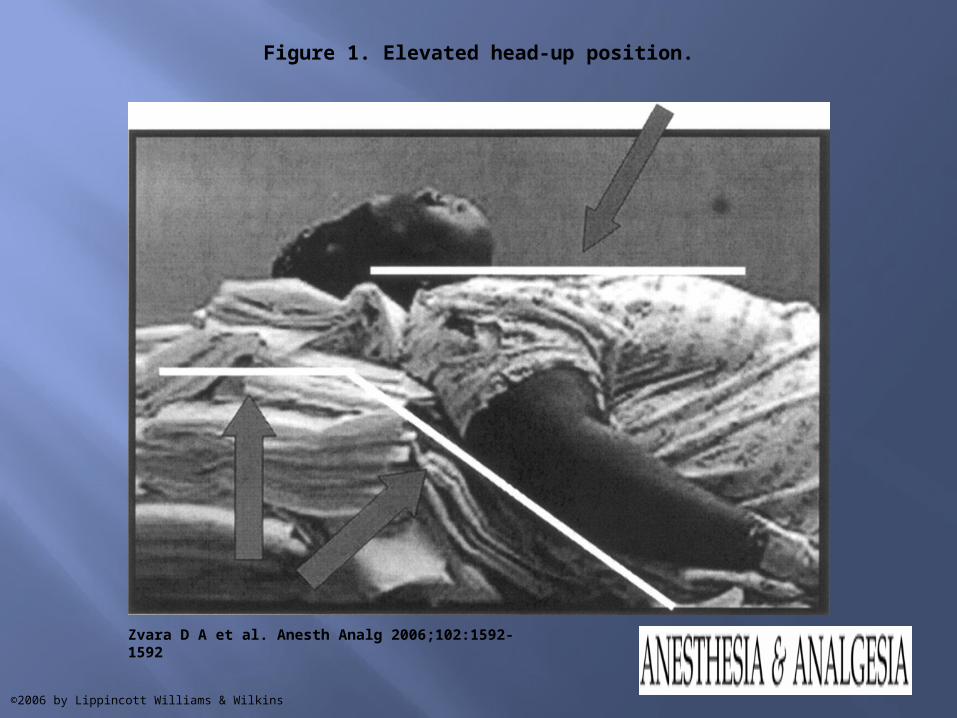
Figure 1. Elevated head-up position.
Zvara D A et al. Anesth Analg 2006;102:1592-1592
©2006 by Lippincott Williams & Wilkins

Figure 2. Whelan-Calicott position.
Zvara D A et al. Anesth Analg 2006;102:1592-1592
©2006 by Lippincott Williams & Wilkins

Position for Trauma Patients
Atlanto-occipital extension is necessary to bring the vocal cords within line-of-sight of the mouth, manual axial in-line stabilization reduces this movement by 60%.

Bougie

How to Bougie
Bougie for Intubation

Review of Cricothyrotomy
Video

RSI DRUGS“Hey Doc.. We’re out of
Etomidate”

RSI Options
There are a number of options for RSI- choose wisely
Succinylcholine vs. Rocuronium/Vecuronium
Consider potential for awake intubation/sedated but not paralyzed intubation
Know your drugs and your doses
Propofol
Dosage: 2-3 mg/kg IV Push Onset of action: < 1 minute Duration 3-10minutes Benefits: Rapid onset, brief duration,
amnestic Caution: Causes cardiovascular
depression and hypotension
Ketamine
Dosage: 1-2mg/kg slow IVP Onset: 30 seconds to 1 minute Duration: 5-10 minutes Benefits: Potent Bronchodilator, leaves
protective airway reflexes intact, maintains cardiovascular stability
Caution: Old Dogma regarding elevated ICP with use, increases sympathetic tone, emergence delirium common

Ketamine in Trauma?
Often underutilized due to old dogma regarding ICP
Ketamine is a non-competitive NMDA receptor antagonist and has neuroprotective effects
Studies claiming ketamine should be avoided in head injury are based on 3 studies from the 1970’s, recent studies have shown no convincing evidence that these claims are valid
Acute agitation and emergence reactions may be of concern for conscious sedation. However, in the RSI population where continued sedation with benzodiazepines is possible, this is of less concern.

Benzodiazepines/Opiates
Dosage needs vary from patient to patient
Onset of action can be unpredictable Poor choice for true Rapid Sequence
Intubation

Advanced Airway Devices

Glidescope
Glidescope
Cost: $11,000 for the Cobalt Benefits: Easy to use, easy to observe
student/resident procedures, minimal need to manipulate the neck
Features- Pediatric and Adult Sizes, unique 60 degree blade, disposable and reusable options
3 options: Cobalt, Ranger, GVL Pitfalls: Expensive, limited visibility with
significant secretions or blood

King Vision
King Vision Video Laryngoscope
Cost: $700-800 Benefits: Easily portable, affordable, no
need for special stylette Pitfalls: Lower resolution than glidescope,
less useful in teaching scenarios due to size of screen
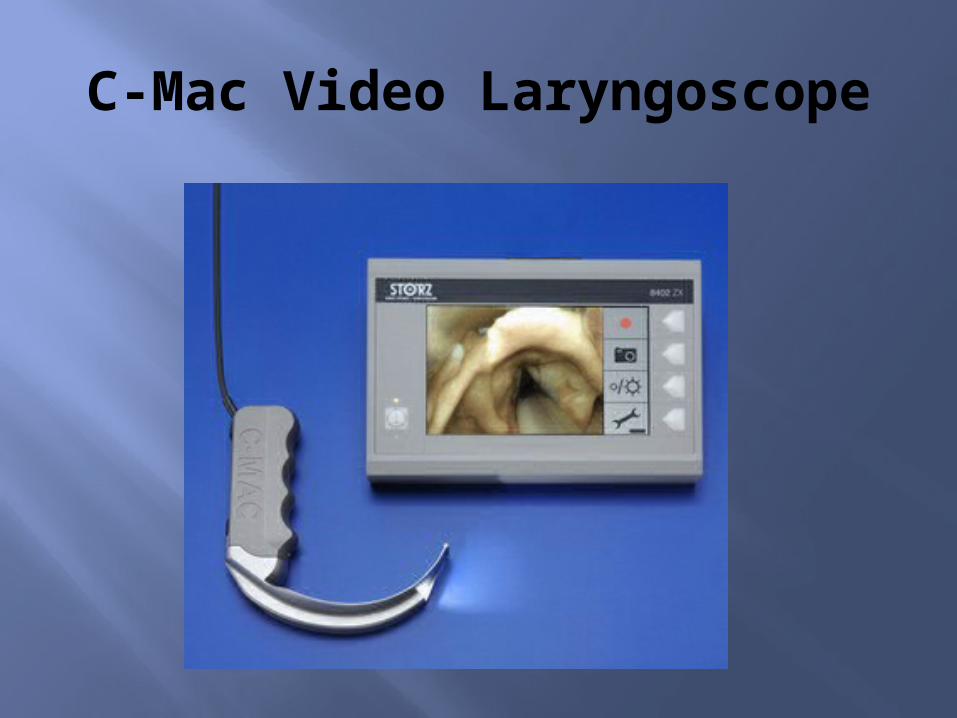
C-Mac Video Laryngoscope

C-Mac
Cost: $60,000 Benefits: Maintains the same curvature
are the basic MAC blade, may be used for conventional direct laryngoscopy or with video assistance, benefits for teaching scenarios
Pitfalls: Price, mobility
QUESTIONS?

References Abrams K.J., Grande C.M. "Airway Management of the trauma patient with
cervical spine injury", Current Opinion in Anesthesiology 1994;7:184-190
The BURP Maneuver . Images in Anesthesiology .Vol. 31. No. 1 January-March 2008 pp 63-6
Cattano, D. Cavallone, L. Airway Management and Airway Positioning: A Clinical Perspective. Anesthesiology News. 2010:35-40.
Ellis DY, Harris T, Zideman D. Cricoid pressure in emergency department rapid sequence tracheal intubations: A risk-benefit analysis. Annals of Emergency Medicine. 2007;50:653-665
EmCrit. “Use of the Bougie for Intubation” http://youtu.be/E7Lo1JD2Brk
Hastings R.H., Marks J.D. "Airway Management for Trauma Patients with Potential Cervical Injuries", Anesth Analg 1991;73:471-82.
Zvara D A et al. Positioning for Intubation in Morbidly Obese Patients Anesth Analg 2006;102:1592-1592