
Carla Research Assignment FINAL
50
Running head: SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED Cognitive Restructuring and Exposure in the Group Treatment of Generalised Social Anxiety Disorder: A Comparison of the Outcome of two Programmes CA Nortje 16954653 Research Assignment for partial fulfilment of the requirements of the degree Honours BA (Psychology) at Stellenbosch University Supervisor: Mr HR Steel, Department of Psychology Stellenbosch University 12 October 2015
-
Upload
carla-nortje -
Category
Documents
-
view
320 -
download
0
Transcript of Carla Research Assignment FINAL

Running head: SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED
Cognitive Restructuring and Exposure in the Group Treatment of
Generalised Social Anxiety Disorder: A Comparison of the Outcome of two
Programmes
CA Nortje
16954653
Research Assignment for partial fulfilment of the requirements of the degree Honours BA
(Psychology) at Stellenbosch University
Supervisor: Mr HR Steel, Department of Psychology
Stellenbosch University
12 October 2015
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 1
Abstract
The aim of this study was to compare the efficacy of two active, group treatment
programmes, cognitive restructuring plus exposure (CBGT) versus exposure alone (EA), in
the treatment of generalised social anxiety disorder (GSAD) within a time-limited period (12
weekly sessions; 2-2.5 hours each). A basic quantitative, cross-sectional research design with
repeated measures was used. Participants (n = 44; 21-68 years old; diagnosed with GSAD
according to the DSM-IV-TR) were allocated to three treatment conditions namely, CBGT (n
= 15), EA (n = 15) and a control group (CTRL; n = 14). MANOVA results showed that,
compared to CTRL, both active treatment programmes showed significant treatment effects
on GSAD symptomatology (p < .01). The two programmes did not differ significantly from
one another with regards to the four dependent variables (i.e., depression; target phobia
avoidance; general social phobia symptomatology; and thought functionality). However,
CBGT was more effective in improving the cognitive variable. Future studies are required to
determine possible changes in the two treatment effects over time, and additionally, to
identify whether changes in the cognitive variable predicts changes in the other GSAD
variables.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 2
According to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.,
DSM-5; American Psychiatric Association [APA], 2013) social anxiety disorder (SAD), also
known as social phobia, is characterised by an irrational fear of potential humiliation and
embarrassment when performing in front of people (e.g., giving a speech), being in social
situations (e.g., interacting with others) and/or being observed (e.g., while eating). When the
fear is experienced in all or almost all situations it is classified as social anxiety disorder,
generalised type. SAD is a debilitating disorder that often has significant, detrimental effects
on the sufferer's social and occupational functioning and general health (APA, 2013).
SAD is one of the most common psychiatric disorders with an estimated prevalence
of between 4% and 6%, and a lifetime risk from 7% to 13% (Lochner et al., 2007). Williams
et al. (2007) suggest that mental disorders, including SAD, are one of the major contributors
to disease burden in South Africa. There is a variety of available treatments for people who
suffer from SAD, broadly categorised in somatic treatment (medication) and psychological
treatment (psychotherapy). Cognitive behaviour therapy (CBT) is a popular approach to the
psychotherapeutic treatment of SAD (Leichsenring et al., 2013), and it may be presented in
an individual or a group format. CBT within a group format will be the focus of the present
study.
CBT is a form of psychotherapy that developed from 1) the philosophical school of
behaviourism (Watson, 1930, cited in Schultz & Schultz, 1992), 2) behaviour therapy,
emphasising the centrality of overt, functional behaviour which originated simultaneously in
South Africa (cf Wolpe & Lazarus, 1966), England (cf Eysenck, 1960, cited in Hergenhahn,
1992) and the United States of America (cf Skinner, 1953, cited in Spiegler & Guevremont,
2003), and 3) cognitive therapy (Beck, 1976; Beck, Rush, Shaw, & Emery, 1979). Today, the
cognitive model (which underlies CBT) advocates that dysfunctional and irrational thinking
(affecting mood and behaviour) is common to most psychological disturbances (Beck &
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 3
Beck, 2011; Clark & Beck, 2010). Although, according to the model, cognitive changes are
essential for improving emotional disturbances (including anxiety and depression), cognitive
restructuring is not the only available CBT technique to accomplish this (Beck & Beck,
2011). Behaviour focused techniques (e.g., repetitive and prolonged exposure to feared
objects and situations) are also regarded as powerful treatment methods for emotional
disorders by having an effect on cognitive changes (Marks, 1987; Mörtberg, 2014). Cognitive
change is viewed as one potential mechanism by which exposure affects positive outcomes in
anxiety disorder treatment; others are, for example, habituation, toughening-up, reciprocal
inhibition, counter-conditioning and emotional processing (Marcus, 1977).
Exposure based treatment was once described as the “gold standard” (Mersch, 1995,
p. 260) for the treatment of anxiety disorders. Although cognitive restructuring (e.g., by
correcting irrational thoughts), exposure (e.g., being made to repetitively present a speech in
front of people, in vivo or in fantasy) and an integrated combination of these two therapeutic
approaches, have proven to be effective treatments for SAD (Hope, Heimberg, & Bruch,
1995), it is not clear which is the best treatment strategy within a specific, limited time-frame
(e.g., in 10 to 15 treatment sessions). In dismantling studies, the relative strength of
components of an integrated cognitive restructuring plus exposure approach were
investigated (e.g., Hope et al., 1995). A different question, however, is the following: within a
limited time period, which of two CBT group treatment programmes (cognitive restructuring
plus exposure versus exposure alone) is the most efficient? Investigating this research
question will have theoretical relevance, for example, by providing answers to the question:
is it essential to involve cognitive restructuring in the treatment of SAD, or is exposure alone
sufficient? The social relevance of this study is related to which is the best treatment for SAD
and for providing the best relief for its debilitating effects. This description of the theoretical
and social relevance of the planned study forms the core of its rationale.

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 4
Literature Review
Classification and Diagnostic Features of Social Anxiety Disorder
SAD is defined as “the fear of being embarrassed or humiliated in front of others”
(Sadock, Sadock, & Ruiz, 2015, p. 293). The social fear occurs upon exposure to feared
social stimuli (social situations), creating a tendency to avoid or escape from the situation.
When escape or avoidance is not possible the individual becomes very anxious. When phobic
stimuli include all or most social situations, the disorder is classified as a generalised subtype
of SAD (referred to in this study as GSAD; APA, 2013).
The DSM-5 (APA, 2013) defines six presenting diagnostic features as criteria that
should be met to diagnose SAD. They include the following: fear in social situations, anxiety
when these situations cannot be avoided, insight that these fears are excessive, attempts to
avoid them, significant detrimental effects on the individual's functioning and duration of the
symptoms for at least six months.
To better conceptualise the clinical features of SAD and select an appropriate
therapeutic approach, psychologists have developed theoretical frameworks that are based on
selected criterion-related symptoms. One such framework is the Cognitive Model of Social
Phobia (CMSP; Clark & Beck, 2010), which focuses on cognitive variables (e.g.,
dysfunctional thinking patterns [Heimberg, Nyman, & O'Brien, 1987] as well as a fear of
negative evaluation [Watson & Friend, 1969]). The model will be discussed later in further
detail.
The Course, Prevalence and Effects of Social Anxiety Disorder
The onset of SAD may follow a traumatic or embarrassing experience (e.g., being
criticised, trembling and blushing during a speech), or it may develop slowly without the
individual being aware of it and persist over many years (APA, 2013; Sadock et al., 2015).

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 5
Social phobia has an early onset (40% of social phobias appear before the age of 10 and 90%
before the age of 20 years), has a chronic progression (with a 12-month prevalence of 7% and
a lifetime prevalence of 12%) and is one of the most prevalent mental disorders in the world
(Leichsenring et al., 2013) According to Williams et al. (2007), mental disorders, including
SAD, are one of the major contributors to disease burden in South Africa, which often result
in harsh psychosocial impairments. Sadock et al. (2015) state that the psychosocial
impairments include effects on a person’s functioning (e.g., academic success, social
development, job performance) as well as on the individual's informal, leisure activities (e.g.,
family gatherings, holidays and parties).
A Theoretical Model of Social Anxiety Disorder
My research will be based on Clark and Beck’s (2010) Cognitive Model of Anxiety
(CMA) and anxiety disorders, including social anxiety disorder (SAD), called the Cognitive
Model of Social Phobia (CMSP; Clark & Beck, 2010). This model originated from an earlier
cognitive theory of anxiety disorders (Beck, Emery, & Greenberg, 1985). The latter model
was at a later stage specifically adapted for SAD (Rapee & Heimberg, 1997) and more
recently revised as a cognitive model for SAD (Clark & Beck, 2010). The CMA provides an
account for why morbid (dysfunctional) anxiety develops in certain individuals and persists
in the absence of danger in these situations.
The central theme of the CMSP (Clark & Beck, 2010; Rapee & Heimberg, 1997;
Wells et al., 1995) is related to the role of cognitive variables, namely the effects of
dysfunctional thoughts (Heimberg et al., 1987) and the fear of negative evaluation by others
(Watson & Friend, 1969). The individual with SAD is concerned with the approval of other
people but is insecure about the impression they have made or will make (Wells et al., 1995).
This insecurity activates dysfunctional core beliefs (i.e., schemas; e.g., “I am vulnerable”, or

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 6
“People are unusually critical of others”), which, in turn, leads to dysfunctional intermediate
beliefs (including attitudes; e.g., “It’s terrible!”, rules; e.g., “I must make a good impression”,
“I should not show anxiety”, and conclusions/assumptions; e.g., “If I show anxiety, then I
will be looked upon as a failure!”).
These beliefs then give rise to negative automatic thoughts (NAT’s; e.g., “Oh no!
They can see I’m anxious”), replacing more positive thinking patterns. These cognitive
changes, in turn, lead to an increased state of self-awareness (self-processing of the self as a
social object from an onlookers perspective) and social phobic responses (i.e.,
symptomatology, including subjective feelings [feeling anxious], physiological reactions
[somatic symptoms; e.g., heart palpitations and blushing], behavioural characteristics
[including avoidance and escape; so-called safety behaviours], as well as cognitive symptoms
[e.g., reduction in concentration on the task and the social demand at hand]). These
symptoms, in turn, have a debilitating effect on the social phobic’s performance, and as such
form an important link in a vicious cycle. The model also distinguishes between three phases
of SAD: the anticipatory phase, the situational exposure phase, and the post-event processing
phase (Clark & Beck, 2010).
The first phase is characterised by potentially conscious, automatic thoughts about
pending social situations (i.e., expectations about a future experience, e.g., “Oh no! I will
have to make a speech at my brother’s wedding.”). The individual may experience as much
anxiety during this phase as they may during exposure to the actual situation.
The second phase involves both beliefs and automatic (potentially conscious)
thoughts during exposure to the feared social situation. The sequence of this maladaptive
cognitive process firstly involves the stimulation of maladaptive social schemas (e.g., core
beliefs about disapproval from others and personal weaknesses) that arise during social
exposure. This is followed by intermediate beliefs and automatic thoughts (ATs), which then
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 7
lead to an increased anxiety level and attempts to conceal the symptoms (by applying safety
behaviours) that, in turn, increase anxiety symptoms. Beliefs are less accessible consciously
than ATs.
The final phase involves post-event recollection and review by the individual of his or
her performance during the social situation. The biased, negative recollection of the event
plays a vital role in the maintenance of social anxiety as the individual is unable to escape the
anxiety process even after the social event has taken place (Beck, 1976; Beck et al., 1985;
Beck et al., 1979; Clark & Beck, 2010).
Cognitive Behaviour Group Treatment of Social Anxiety Disorder
Cognitive behaviour therapy (CBT) is a form of psychotherapy developed by Aaron
T. Beck (Beck et al., 1979, 1985; Clark & Beck, 2010). Beck developed CBT as a time-
restricted, structured approach that uses a cognitive (i.e., information-processing) model to
understand and treat disorders such as SAD. The therapist’s role is to assist SAD sufferers in
overcoming their fears by changing their thinking (e.g., “I am vulnerable”, “Everyone is
going to laugh at me”) and behaviour (e.g., automatic, safety responses such as avoidance).
Although medication can be effective, SAD can also be treated using
psychotherapeutic approaches such as CBT (Andersson & Carlbring, 2009). CBT has the
strongest experimental support among the psychotherapeutic approaches (e.g., compared to
psychodynamic treatment and interpersonal therapy; Acarturk, Cuijpers, van Straten, & de
Graaf, 2009; Andersson & Carlbring, 2009). CBT is an umbrella term that refers to several
treatment techniques (used in combination to treat psychopathological conditions such as
SAD), which include imagery rescripting, exposure, psychoeducation, cognitive
restructuring, social skills training and relaxation methods (Holmes, Arntz, & Smucker, 2007;
Hope, Burns, Hayes, Herbert, & Warner, 2010; Jørstad-Stein & Heimberg, 2009; Turner,
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 8
1994). The range of the current study is restricted to comparing the effects of two specific
treatment programmes, namely Cognitive Behaviour Group Therapy (CBGT; characterised
by cognitive restructuring plus exposure) and Exposure Alone (EA; characterised by only
exposure, without cognitive restructuring exercises) and the integration of the two techniques,
as described in a treatment manual by Heimberg (1991).
The goal of CBT is to change dysfunctional schemata (i.e., core cognitive structures)
that result in increased symptomatology (Hope et al., 2010). This is done through a major
component of CBGT known as cognitive restructuring. Cognitive restructuring, a verbal
questioning and disputation technique that targets ATs that occur when the client thinks about
or is exposed to the feared stimulus (and affect their underlying dysfunctional beliefs). It
involves four steps: 1) the identification of the problematic ATs, 2) the identification of the
irrational thought processes (cognitive errors) in the ATs, 3) rational discussion and
questioning of ATs through an explorative dialogue technique, and 4) development of
constructive alternative thoughts to replace these ATs. In CBGT, cognitive restructuring is
integrated with exposure therapy (Hope et al., 2010). Cognitive restructuring is used to
identify and confront thoughts that occur before, during and after exposure to the feared
stimulus.
Exposure therapy is used to treat negative emotional responses such as fear and
anxiety by exposing clients to the feared event or stimulus (Hofmann & Otto, 2008; Marcus,
1977). In order to avoid worsening the symptoms and for exposure to be therapeutic, the
therapist must decide on the duration and mode of exposure. It may be presented to the client
in a stepwise progression (gradually), as well as repetitively and over a prolonged period of
time. Exposure may also be presented to the client on an imaginary level (in fantasy) or in a
real life (in vivo) situation. Imaginary (in fantasy) scenarios involve the client imagining and
'experiencing' a frightening situation. In vivo exposure refers to confronting feared situations
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 9
in real life whereby the client is exposed to actual frightening situations (e.g., a person
suffering from SAD giving a speech to a group of strangers; Hofmann & Otto, 2008).
The Efficacy of Cognitive Behaviour Group Treatment on Social Anxiety Disorder
CBGT for SAD has been shown to be efficacious within research components and
effective within numerous clinical settings (McEvoy, Nathan, Rapee, & Campbell, 2012).
Below is a discussion of research that has been done on the various components of CBGT
and the efficaciousness of each.
For decades there have been viewpoints that cognitive restructuring is the best
treatment for changes in cognitive variables such as fear of negative evaluation and thought
dysfunctionality (Butler, 1989; Emmelkamp, 1982). It is an opinion still expressed in more
recent times (Beck & Beck, 2011; Clark & Beck, 2010).
Studies focused on cognitive restructuring without exposure attempted to determine if
cognitive restructuring alone is effective for SAD. According to cognitive theory of anxiety
disorders (e.g., Beck et al., 1985; Clark & Beck, 2010), cognitive change is essential for the
improvement of SAD, and there is a viewpoint from influential researchers in the field of
SAD (e.g., Beidel, Turner, & Dancu, 1985; Butler, 1985; Clark & Beck, 2010; Hammen,
Jacobs, Mayol, & Cochran, 1980; Heimberg, Dodge, Hope, Kennedy, & Zollo, 1990) that
change of dysfunctional cognitions is necessary for the successful treatment of SAD.
Several studies that focused on the efficacy of exposure alone have found that
exposure therapy has resulted in significantly greater improvement rates when being
compared to placebo groups (Blomhoff et al., 2001; Heimberg et al., 1990a) or control groups
(Mersh, 1995). In three studies (Alström, Nordlund, Persson, Harding, & Ljungqvist, 1984;
Hope et al., 1995; Wlazlo, Schroeder-Hartwig, Hand, Kaiser, & Munchau, 1990), published
more than two decades ago, EA was expressed as having the best outcome results.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 10
Heimberg's treatment (1991) was only used in one of them namely, Hope et al. (1995).
Alström et al. (1984) compared EA with traditional relaxation therapy and found that
exposure therapy was superior in the treatment of SAD. An outcomes study done by Hope et
al. (1995) showed that EA was significantly superior to cognitive restructuring plus exposure
in a CBGT programme (see also an earlier study by Biran, Augusto, & Wilson, 1981). Lastly,
Wlazlo et al. (1990) found that EA had a significantly greater improvement than social skills
training in two groups of patients suffering from SAD.
Previous studies (e.g., Hindo & Gonzalez-Prendes, 2011; Mattick & Peters, 1988) that
compared the components of CBT, namely cognitive restructuring and exposure, as well as
theoretical arguments (Clark & Beck, 2010; Rodebaugh, Holaway, & Heimberg, 2004) argue
that the combination of the components would result in the best outcome. The expectation
that cognitive restructuring will improve the effects of exposure is emphasised in SAD
literature. Therefore, many theorists argue for the combined treatment. This argument is
based on a variety of opinions and research findings, some of which are given below.
Various meta-analytical studies (Norton & Price, 2007; Taylor, 1996; Wersebe,
Sijbrandij, & Cuijpers, 2013) demonstrate the facilitating effect that cognitive restructuring
has on exposure. Specific arguments are offered about potential ways in which cognitive
restructuring and exposure mutually facilitate one another (Hope et al., 1995) and there are
findings in SAD research outcome studies that cognitive restructuring sometimes facilitates
exposure (Butler, Cullington, Munby, Amies, & Gelder, 1984; Emmelkamp, Mersh, Vissia,
& Van der Helm, 1985; Shikatani, Anthony, Kuo, & Cassin, 2014). Mattick, Peters, and
Clarke (1989) showed a worsening of symptoms (a deterioration of initial therapeutic gains)
when EA was used but not when cognitive restructuring in combination with exposure was
used, and it was found that the improvement on cognitive measures seems bigger after
treatments where cognitive restructuring was included compared to EA based treatments
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 11
(Butler et al., 1984; Emmelkamp et al., 1985; Jerremalm, Jansson, & Öst, 1986; Kanter &
Goldfried, 1979). Finally, it seems as though cognitive restructuring treatments (that were
effective) also included exposure treatments (Jerremalm et al., 1986; Kanter & Goldfried,
1979; Shikatani et al., 2014).
Method
Archival data of a treatment outcomes study done in 2000 by Dr C Nortje and Dr T
Posthumus was used in this study. The original study compared two treatment procedures for
SAD with the CTRL group. The treated groups were namely 1) EA and 2) CBGT. The
participants that were diagnosed with GSAD were randomly allocated to groups as follows:
15 to the CBGT group, 15 to the EA group and 14 to the CTRL group.
Aims
The main aim of the study was to investigate and compare the effectiveness of CBGT
(i.e., cognitive restructuring plus exposure) and exposure alone (EA; also presented in group
format) in the treatment of generalised social anxiety disorder (GSAD). The specific aims of
this study were to investigate 1) the effectiveness of CBGT in the treatment of GSAD, 2) the
effectiveness of EA in the treatment of GSAD, 3) the difference between the two treatment
programs with regards to their effectiveness in treating GSAD.
Hypotheses
In the present study the data for certain selected dependent variables from the original
study were analysed to test the following hypotheses:
1. The two treatment condition groups (CBGT, EA) and the control group (CTRL) will
not differ significantly from one another with regards to the following variables at the
pre-treatment phase: target phobia as measured by the Fear Questionnaire-Target
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 12
Phobia (FQ-TP; Marks & Mathews, 1979), social phobia as measured by the Social
Phobia and Anxiety Inventory (SPAI; Turner, Beidel, Dancu, & Stanley, 1989), a
cognitive variable measured by the Thought-listing Technique (TLT; Heimberg et al.,
1987) and depression as measured by the Beck Depression Inventory II (BDI-II;
Beck, Steer, & Brown, 1996).
2. The treatment condition CBGT and CTRL will differ significantly at post-treatment
with regards to the above-mentioned dependent variables, with CBGT demonstrating
larger improvements of GSAD symptomatology compared to CTRL.
3. The treatment condition EA and CTRL will differ significantly at post-treatment with
regards to the above-mentioned dependent variables, with EA demonstrating larger
improvements of GSAD symptomatology compared to CTRL.
4. The treatment conditions, CBGT and EA, will differ significantly from one another at
post-treatment with regards to the above-mentioned dependent variables, with CBGT
demonstrating larger improvements of GSAD symptomatology compared to EA.
Research Design
A basic quantitative, cross-sectional research design with repeated measures was used
in the original study. Two groups each received different treatments, namely exposure plus
cognitive restructuring, or exposure alone.
Sampling Strategy and Participants
In the sampling of participants, the original researchers distributed about 300
pamphlets to general medical practitioners in the Stellenbosch area recruiting potential
participants who suffer from GSAD. Advertisements were also placed in local newspapers
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 13
and magazines. The original researchers' own clients and other clinical psychologists' clients
in the Western Cape were approached and invited to participate in the study.
The target population was determined to be middle-to-upper class individuals who
met the DSM-IV-TR (APA, 2000) diagnostic criteria for GSAD. Interviews were conducted
by two independent clinical psychologists (i.e., not involved in the treatment). The
participants were evaluated on a 5-axial diagnosis of SAD. Those who presented with GSAD
as their most serious problem were selected. Exclusion criteria were individuals younger than
18 years, individuals who suffered from another severe mental disorder, and individuals who
were recently (less than 3 weeks) prescribed medication for SAD.
The final sample consisted of 44 participants who met the DSM-IV-TR (APA, 2000)
criteria for GSAD. There were 30 females and 14 males, aged between 21 and 68 years old.
Participants were randomly assigned to one of the three treatment groups, namely 15 to
CBGT, 15 to EA and 14 to CTRL.
Procedure and Evaluation
The weekly group treatment sessions took place over 12 weeks and were two to two
and a half hours each. The dependent variables were measured at pre- and post-treatment
stage as well as at a 3-month follow-up (the latter data will not be analysed for the purpose of
the present study). The evaluation of the participants was done individually by one of the two
psychologists that were responsible for the initial selection process. A variety of different
scenes (scenarios), self-report questionnaires, a thought-listing technique and Likert-type
scales were used during the evaluation.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 14
Measurements
A social target fear scene was created for each participant. Various measurements
were used in participant selection and for the measurement of idiosyncratic social fears, SAD
symptomatology, a SAD cognitive variable and depression. These measures are discussed
below.
Structured interview for selection of participants. The Anxiety Disorders Interview
Schedule Revised (ADIS-R; DiNardo & Barlow, 1988) was used as a structured interview for
participant selection. It was initially developed to assist the DSM-III-R diagnosis of SAD
(APA, 1980). The criteria, however, did not change in the DSM-IV-TR (APA, 2000) nor in
the DSM-5 (APA, 2013) diagnosis of SAD. It therefore remains relevant for and comparable
with more recent research. As stated previously, the participants were interviewed by two
independent psychologists. In the diagnosis of SAD, the ADIS-R had a strong inter-rater
reliability kappa-coefficient of = .77 (n = 80; Brown, DiNardo, Lehman, & Campbell,
2001).
Construction of idiosyncratic fear scenes. A unique and specific social target fear
scene was created for each participant (e.g., to make a speech, to meet someone of the
opposite sex.). The scene was assessed to be very relevant and anxiety provoking for the
individual. It was constructed as a written piece in two versions. A longer version, which
included an audio-recorded description of the scene, was developed for and used as part of a
thought-listening technique (Heimberg, Bruch, Hope, & Dombeck, 1990b; Heimberg et al.,
1987), and a shorter version has been developed and used as part of the FQ-TP (Marks &
Mathews, 1979).
Dependent variables and measuring scales.
Measurement of target phobia. The Fear Questionnaire-Target Phobia (FQ-TP), a
subscale of the Fear Questionnaire (FQ; Marks & Mathews, 1979), measured the level of
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 15
target phobia avoidance on a 0-to-8 point Likert type scale. The FQ-TP consisted of five
items referring to the idiosyncratic social fear identified in the ADIS-R interview. The
participants would rate their level of avoidance of their target phobia from 0 (e.g., “I will not
avoid it”) to 8 (e.g., “I will always avoid it”). The FQ was found to have good discriminatory
power and internal consistency (Cronbach alpha = .74; Cox, Swinson, & Shaw, 1991).
Measurement of generalised social anxiety disorder symptomatology. The Social
Phobia and Anxiety Inventory (SPAI; Turner et al., 1989) was used in the measurement of
GSAD symptomatology. It is a 45-item measure and comprises of two subscales namely, the
social phobia subscale (32 items) and the agoraphobia subscale (13 items). The former
measures somatic, behavioural and cognitive manifestations of SAD, and the latter measures
symptoms of agoraphobia. Turner et al. (1989) subtracted the score of the agoraphobia
subscale from the social phobia subscale to obtain a final total score as a measure of SAD
symptomatology. The reason for this was to accommodate and take into account the overlap
between agoraphobia and social phobia symptomatology. The study used a 7-point Likert
type scale ranging from 0 (never) to 7 (always) where the SPAI total score is calculated as the
difference between the subscales. The scale showed both high internal consistency (alpha =
.96) and test-retest reliability (r = .86) from a sample of 182 participants (Turner et al., 1989).
Measurement of a cognitive variable related to social anxiety disorder. The
Thought-listing Technique based on a State of Mind ratio (TLT-SOM; Heimberg et al.,
1990b; Heimberg et al., 1987) was used to determine and calculate the thought functionality
of ATs. The TLT-SOM was administered by using the typed, longer version of the
idiosyncratic target fear developed during the ADIS-R interview, whereby participants
reported in writing their spontaneous thoughts they recalled thinking while listening to an
audio-taped description of their idiosyncratic feared situation. Thereafter, two registered
clinical psychologists classified the self-reported thoughts into positive, neutral or negative

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 16
categories. These numbers were inserted onto a formula, called a State of Mind ratio (i.e., the
number of positive thoughts, divided by the number of positive thoughts plus negative
thoughts). It is important to emphasise that high TLT-SOM measures reflect thought
functionality and not thought dysfunctionality. On the other hand, low TLT-SOM scores may
be interpreted as reflecting thought dysfunctionality. In the study of Heinrichs and Hoffman
(2005) this measurement showed good convergent, divergent and construct validity, as well
as treatment sensitivity.
Measurement of depression. The Beck Depression Inventory-II (BDI-II; Beck et al.,
1996), a popular 21-item instrument, measured the depression symptoms intensity levels of
the 44 participants. The reason for adding this measure is related to the significant
comorbidity of social anxiety and depression (APA, 2000; APA, 2013). In Dozois, Dobson
and Ahnberg's (1998) study, the BDI-II demonstrated convergent validity, treatment
sensitivity and high internal consistency (Cronbach alpha = .91; see also Beck, Steer, &
Carbin, 1988).
Treatment
The two treatment condition programmes used in this study are the CBGT and the EA
programme. They are explained and discussed below.
Cognitive behaviour group therapy (CBGT) programme. The combined cognitive
restructuring plus exposure treatment that was used was based on a treatment manual of a
structured treatment programme developed by Heimberg (1991). According to Heimberg
(1989, 1991) the programme consisted of the following components: (a) Explanation of
treatment and the (SAD) cognitive model; (b) skills training of the patients through structured
exercises (i.e., identification, analysis and contention of maladaptive cognitions); (c)
simulated exposure exercises during group treatment; (d) teach patients to control
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 17
problematic cognitions through utilising cognitive restructuring methods before, during and
after exposure; (e) in vivo exposure homework assignments of already confronted exposure
exercises during treatment; and (f) the learning of the cognitive restructuring routine for use
before and after exposure assignments.
Exposure alone (EA) programme. The exposure alone condition is also described in the
treatment manual of Heimberg (1991). It is the same as the above mentioned treatment
programme except that it leaves out cognitive restructuring exercises. The rationale for the
treatment was based on the learning model of classical conditioning.
Data Analysis
The data were analysed by conducting between-groups and repeated-measures
multivariate analyses of variance (MANOVA’s) to determine the significance of differences
between- and within-groups. This was followed by post hoc analyses when the omnibus
multivariate test statistics were significant. Pairwise comparisons using the Bonferroni
correction for multiple comparisons were executed.
Ethical Considerations and Approval
This study used archival data. Therefore, the current study posed no risk to
participants and application for institutional permission was not necessary. The original study
in 2000 obtained ethical clearance before the research was conducted (Appendix A). At that
stage, the Department of Psychology made use of their own committee (the departmental
committee for ethical clearance) for ethical clearance of research proposals of master’s theses
and doctoral dissertations. The application for ethical clearance was submitted to the
Department of Psychology Research and Ethics Committee (DESC) and was approved before
data analysis commenced.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 18
Results
Descriptive Statistics
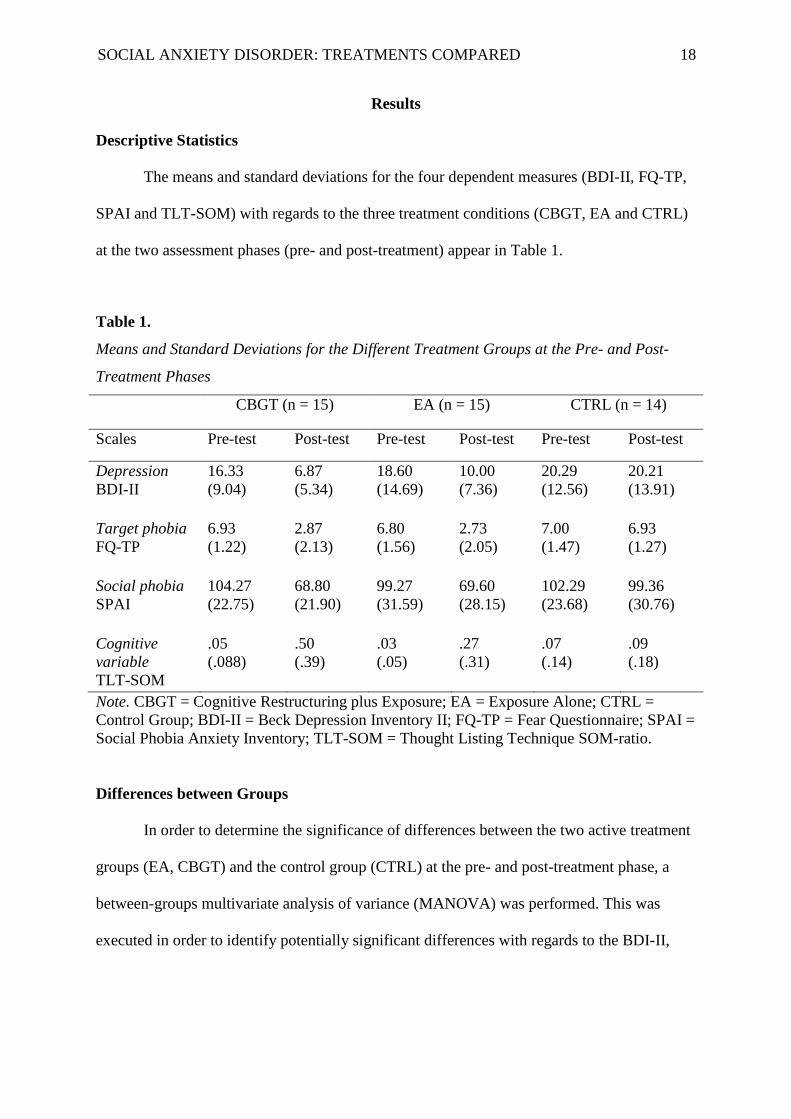
The means and standard deviations for the four dependent measures (BDI-II, FQ-TP,
SPAI and TLT-SOM) with regards to the three treatment conditions (CBGT, EA and CTRL)
at the two assessment phases (pre- and post-treatment) appear in Table 1.
Table 1.
Means and Standard Deviations for the Different Treatment Groups at the Pre- and Post-
Treatment Phases
CBGT (n = 15) EA (n = 15) CTRL (n = 14)
Scales Pre-test Post-test Pre-test Post-test Pre-test Post-test
Depression
BDI-II
16.33
(9.04)
6.87
(5.34)
18.60
(14.69)
10.00
(7.36)
20.29
(12.56)
20.21
(13.91)
Target phobia
FQ-TP
6.93
(1.22)
2.87
(2.13)
6.80
(1.56)
2.73
(2.05)
7.00
(1.47)
6.93
(1.27)
Social phobia
SPAI
104.27
(22.75)
68.80
(21.90)
99.27
(31.59)
69.60
(28.15)
102.29
(23.68)
99.36
(30.76)
Cognitive
variable
TLT-SOM
.05
(.088)
.50
(.39)
.03
(.05)
.27
(.31)
.07
(.14)
.09
(.18)
Note. CBGT = Cognitive Restructuring plus Exposure; EA = Exposure Alone; CTRL =
Control Group; BDI-II = Beck Depression Inventory II; FQ-TP = Fear Questionnaire; SPAI =
Social Phobia Anxiety Inventory; TLT-SOM = Thought Listing Technique SOM-ratio.
Differences between Groups
In order to determine the significance of differences between the two active treatment
groups (EA, CBGT) and the control group (CTRL) at the pre- and post-treatment phase, a
between-groups multivariate analysis of variance (MANOVA) was performed. This was
executed in order to identify potentially significant differences with regards to the BDI-II,
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 19
FQ-TP, SPAI and TLT-SOM dependent variable measures between the three aforementioned
groups.
Pre-treatment differences between groups. The first hypothesis predicted that the
three treatment condition groups (CBGT, EA and CTRL) will not differ significantly from
one another on all four of the dependent variables (BDI-II, FQ-TP, SPAI and TLT-SOM) in
the pre-treatment phase. The omnibus statistic Wilks’ lambda (i.e., U statistic) is frequently
used for testing overall significance between groups with numerous dependent variables
(Hair, Black, Babin & Anderson, 2010). In the pre-treatment phase, the MANOVA indicated
that there were no significant differences between groups for the collective dependent
variables, with U = .92, F(8, 76) = .38, p = .926, partial 2 = .039. Therefore, the first
hypothesis was supported, suggesting that there were no significant differences between the
CBGT, EA and CTRL groups with regards to the dependent variables at the pre-treatment
phase.
Post-treatment differences between groups. A MANOVA was also executed at the
post-treatment phase. Wilks’ lambda was significant, with U = .39, F(8, 76) = 5.77, p = .000,
partial 2 = .38, indicating significant differences between the three treatment condition
groups (CBGT, EA and CTRL) with regards to the dependent variables. Between-groups
univariate ANOVA’s indicated significant differences between groups on all four dependent
variables (see Table 2).
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 20
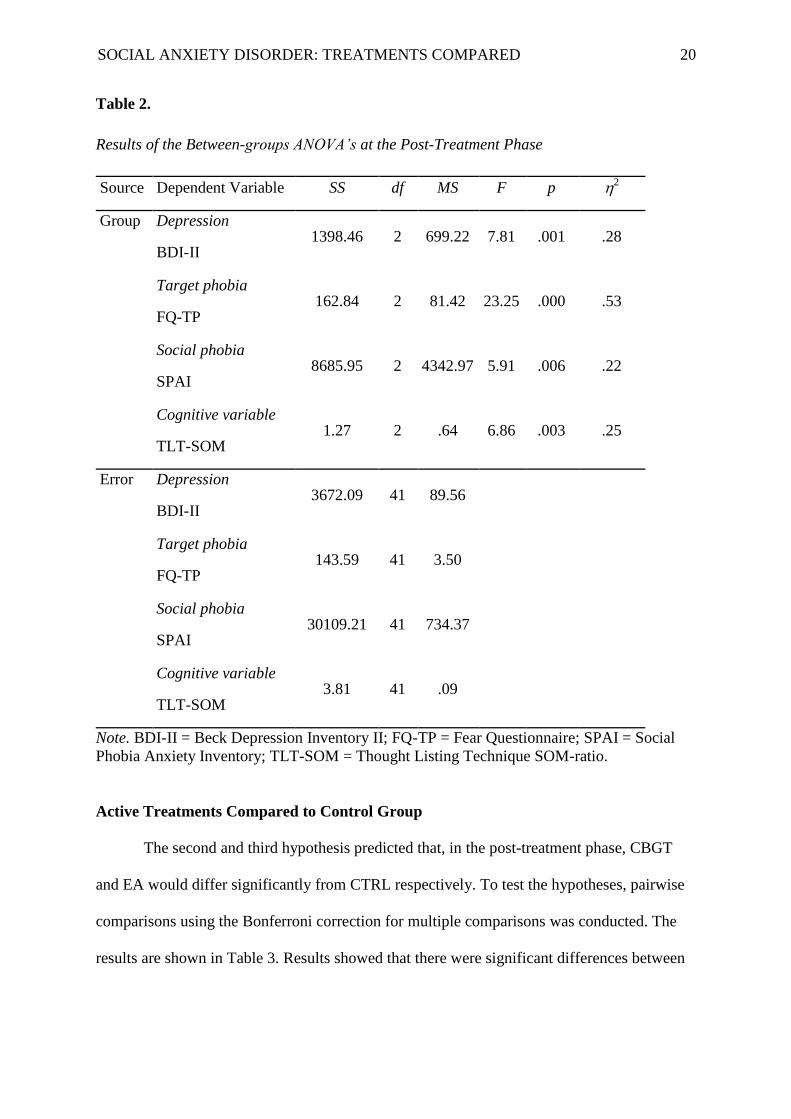
Table 2.
Results of the Between-groups ANOVA’s at the Post-Treatment Phase
Source Dependent Variable SS df MS F p 2
Group Depression
BDI-II 1398.46 2 699.22 7.81 .001 .28
Target phobia
FQ-TP 162.84 2 81.42 23.25 .000 .53
Social phobia
SPAI 8685.95 2 4342.97 5.91 .006 .22
Cognitive variable
TLT-SOM 1.27 2 .64 6.86 .003 .25
Error Depression
BDI-II 3672.09 41 89.56
Target phobia
FQ-TP 143.59 41 3.50
Social phobia
SPAI 30109.21 41 734.37
Cognitive variable
TLT-SOM 3.81 41 .09
Note. BDI-II = Beck Depression Inventory II; FQ-TP = Fear Questionnaire; SPAI = Social
Phobia Anxiety Inventory; TLT-SOM = Thought Listing Technique SOM-ratio.
Active Treatments Compared to Control Group
The second and third hypothesis predicted that, in the post-treatment phase, CBGT
and EA would differ significantly from CTRL respectively. To test the hypotheses, pairwise
comparisons using the Bonferroni correction for multiple comparisons was conducted. The
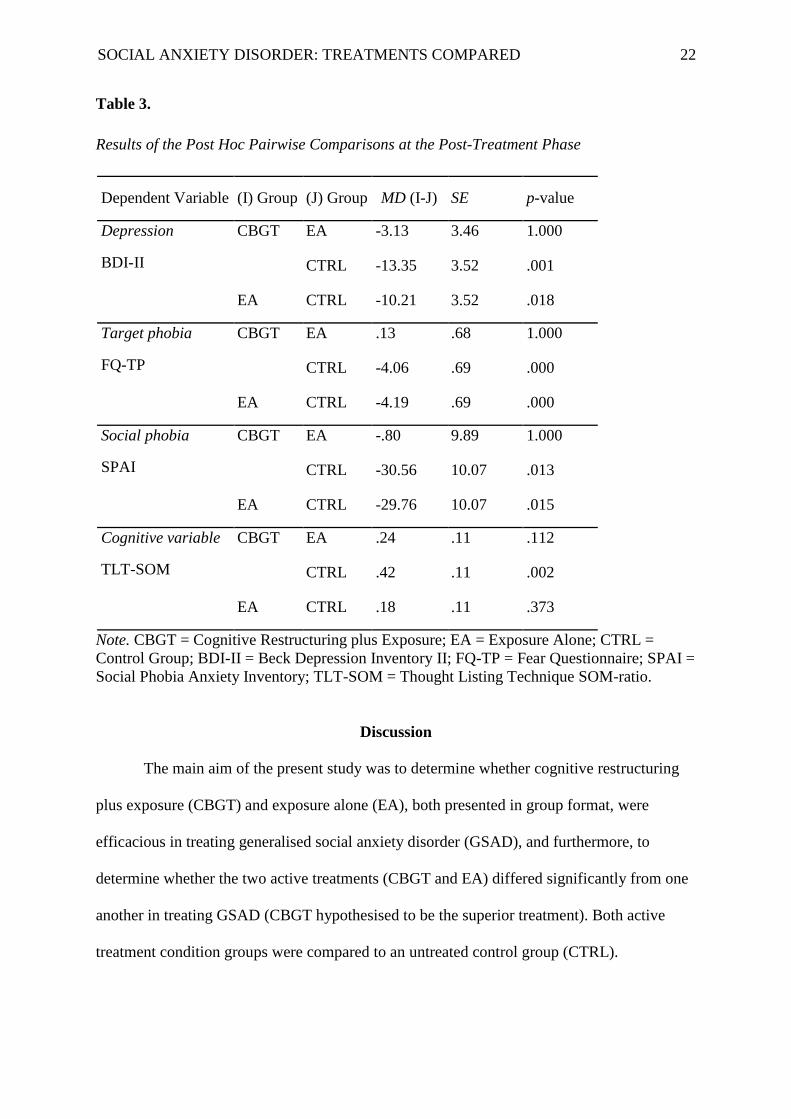
results are shown in Table 3. Results showed that there were significant differences between
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 21
CBGT and CTRL, as well as between EA and CTRL. Therefore, the second and third
hypothesis were supported. These results are discussed in more detail below.
Cognitive restructuring plus exposure (CBGT) compared to control. The mean
scores on the BDI-II, FQ-TP and SPAI for CBGT were significantly lower than for CTRL (p
< .05). The mean score on the TLT-SOM was significantly higher for CBGT than for CTRL
(p = .002).
Exposure alone (EA) compared to control. As for CBGT, the mean scores on the
BDI-II, FQ-TP and SPAI for EA were also significantly lower than for CTRL (p < .05).
There was, however, no significant difference between EA and CTRL on the TLT-SOM (p =
.373).
Active Treatments Compared
The fourth and final hypothesis was that the treatment conditions, CBGT and EA, will
differ significantly from one another at post-treatment on the BDI-II, FQ-TP, SPAI and TLT-
SOM. However, analyses of the data showed that there were no significant differences
between CBGT and EA on the dependent variables (p > .05). Therefore, the last hypothesis is
not supported. These results are shown in Table 3 and interpreted below.
Cognitive restructuring plus exposure (CBGT) compared to exposure alone
(EA). The mean scores on the BDI-II, FQ-TP and SPAI for CBGT were not significantly
different from those of EA (p = 1.000 on all three dependent variables). The mean score for
thought functionality (cognitive variable; TLT-SOM) was also not significant (p = .112) but
was, however, almost significant on the 10% level. This result will be discussed in the
following section as it may have implications for further research.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 22
Table 3.
Results of the Post Hoc Pairwise Comparisons at the Post-Treatment Phase
Dependent Variable (I) Group (J) Group MD (I-J) SE p-value
Depression
BDI-II
CBGT EA -3.13 3.46 1.000
CTRL -13.35 3.52 .001
EA CTRL -10.21 3.52 .018
Target phobia
FQ-TP
CBGT EA .13 .68 1.000
CTRL -4.06 .69 .000
EA CTRL -4.19 .69 .000
Social phobia
SPAI
CBGT EA -.80 9.89 1.000
CTRL -30.56 10.07 .013
EA CTRL -29.76 10.07 .015
Cognitive variable
TLT-SOM
CBGT EA .24 .11 .112
CTRL .42 .11 .002
EA CTRL .18 .11 .373
Note. CBGT = Cognitive Restructuring plus Exposure; EA = Exposure Alone; CTRL =
Control Group; BDI-II = Beck Depression Inventory II; FQ-TP = Fear Questionnaire; SPAI =
Social Phobia Anxiety Inventory; TLT-SOM = Thought Listing Technique SOM-ratio.
Discussion
The main aim of the present study was to determine whether cognitive restructuring
plus exposure (CBGT) and exposure alone (EA), both presented in group format, were
efficacious in treating generalised social anxiety disorder (GSAD), and furthermore, to
determine whether the two active treatments (CBGT and EA) differed significantly from one
another in treating GSAD (CBGT hypothesised to be the superior treatment). Both active
treatment condition groups were compared to an untreated control group (CTRL).
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 23
It was hypothesised that CBGT and EA will both demonstrate significantly larger
improvement effects on GSAD symptomatology compared to the untreated control group.
The second hypothesis (i.e., that CBGT and CTRL will differ significantly at post-treatment
on all four variables) was supported for four out of four of the main effects; depression;
target phobia avoidance; general social phobia symptomatology; and thought functionality
all demonstrated statistical significance. Results thus indicate that the combined treatment
programme was efficacious for significantly improving all GSAD symptomatology.
Findings for the third hypothesis (i.e., that EA and CTRL will differ significantly at
post-treatment on all four variables) were not as compelling as those seen for CBGT. With
regards to EA, only three out of the four main effects (depression, target phobia avoidance,
and general social phobia symptomatology) showed significant differences, whereas effects
on thought functionality were non-significant.
Results suggest that exposure alone (i.e., without the cognitive restructuring
component) was insufficient in ensuing cognitive change (i.e., improving thought
functionality). The statistical non-significance of EA's effects on the cognitive variable is
supported by the results reported in other studies (Hope et al., 1995; Mattick et al., 1989).
Contrastingly, with regards to the combined treatment programme (CBGT), the statistical
significant effect on thought functionality suggests that the combination of exposure and
cognitive restructuring was not only effective but necessary in targeting and improving the
cognitive component of SAD symptomatology (i.e., bringing about cognitive change).
Subsequently, it was lastly hypothesised that CBGT would demonstrate significantly
larger improvements to GSAD when compared to EA. However, the results of this study
showed that there were no significant statistical differences between the two active treatments
regarding their effects on all four dependent variables. This finding is congruent with the

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 24
results of Scholing and Emmelkamp (1993) who found that the integrated treatment
programme (i.e., CBGT) and EA were equally effective in treating GSAD.
Results from the present study suggest that regardless of EA having a non-significant
effect on the cognitive variable, it is still an effective therapeutic treatment for GSAD (i.e.,
changes in thought functionality did not correspond with changes in other dimensions in
GSAD pathology and overall treatment effects). Despite theoretical assumptions that
cognitive change is central to successful treatment of GSAD (e.g., Beidel et al., 1985; Butler,
1985; Clark & Beck, 2010), the findings of this study suggest that, compared to EA, adding
the cognitive restructuring component (CBGT) demonstrated no improvement for GSAD.
This, in turn, raises questions about Beck's cognitive theory of anxiety disorders which
maintain that cognitive interventions and cognitive change are essential for successful
treatment of GSAD (Clark & Beck, 2010).
As mentioned previously, when compared to the CTRL condition, CBGT showed
significant effects on more dependent variables than EA (i.e., also for the cognitive variable
thought functionality). Compared to CTRL, the cognitive variable (i.e., thought functionality)
showed significant improvements with regards to the CBGT condition, whereas the EA
condition did not. Supportive findings include those reported by Heimberg et al. (1990)
where significant increases in the number of positive thoughts from pre- to post-treatment
were discovered. Hope et al. (1995) found that the EA condition failed to demonstrate
significant improvements in thought functionality, supporting this study’s finding.
Furthermore, the inclination of CBGT to be regarded as the superior treatment for
improving thought functionality is supported by a treatment related recommendation made by
Rodebaugh et al. (2004). They argued that GSAD clients’ distorted expectations and
cognitions are limited to very specific (idiosyncratic) feared social situations, rather than
general (common) social situations. Therefore, Rodebaugh et al. (2004) proposed that clients,
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 25
through exposure to the feared social situation, experience a genuine feared response.
Cognitive restructuring may now assist the client in making situation specific cognitive
changes. Based on this view, both exposure and cognitive restructuring may be considered as
crucial strategies for treating the cognitive component of GSAD.
Limitations and Recommendations
I have identified two primary limitations to this study. Firstly, in terms of
methodological issues, the sample size was fairly small. Each treatment condition had a
maximum of 15 participants per treatment group. Therefore, the non-significant differences
between the CBGT and EA groups may be accredited to poor statistical power. This, in turn,
may have concealed potentially significant treatment differences. The differential efficacy of
the two active treatments (EA and CBGT) may be explored by future studies using bigger
samples.
Another factor which may have obscured potentially significant treatment differences
is the single post-treatment measurement of the variables. That is, even though the effects of
two active treatments did not differ significantly directly after treatment, they may differ
significantly over a longer follow-up time (i.e., the one may have increasingly larger long-
term effects). A question that may be asked is: as more time elapses after treatment, would
follow-up tests reveal a significant difference between the two active treatments and their
effects on the cognitive variable? I would, secondly, therefore recommend that future
research compare the effects of the two treatments (CBGT and EA) over different follow-up
periods.
As indicated by the post-treatment MANOVA, the best candidate for potentially
mediating such increasing improvements over time is the variable thought functionality (the
cognitive variable measured by the TLT-SOM). Therefore, a final recommendation for future

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 26
research would be to identify whether changes in the cognitive variable (i.e., thought
functionality indicated by the TLT-SOM) predicts changes in the GSAD symptomatology
(e.g., depression, target phobia and social phobia), as well as increasing effects during the
follow-up period. Future research should also concentrate on clinically significant effects,
rather than comparing only statistically significant changes.
Conclusion
The main aim of the study was to investigate and compare the efficacy of CBGT and
EA in the treatment of generalised social anxiety disorder (GSAD). A MANOVA was
executed to compare differences between treatment conditions. This was followed by post
hoc analyses, namely pairwise comparisons using the Bonferroni correction for multiple
comparisons. The results of the present study indicate that both active treatments (CBGT and
EA) were effective in reducing overall social phobic symptomatology (i.e., both had
significant effects on improving GSAD symptomatology). The two treatments did not differ
significantly from one another on any of the dependent variables (depression, target phobia,
social phobia, and the cognitive variable), therefore, suggesting that EA and CBGT are
equally efficacious in treating GSAD within a limited treatment time period.
However, unlike EA, CBGT had a significant effect on the cognitive variable when
compared to the CTRL group. Therefore, the present study’s results demonstrate a favourable
tendency for the combined treatment programme being the better treatment, which
corresponds with an outcome study by Heimberg et al. (1990a). It suggests that CBGT may
be the superior treatment in improving thought functionality (initiating positive cognitive
changes), theorised as necessary in reducing GSAD symptomatology (Heimberg et al.
1990b).

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 27
References
Acarturk, C., Cuijpers, P., van Straten, A., & de Graaf, R. (2009). Psychological
treatment of social anxiety disorder: A meta-analysis. Psychological Medicine, 39,
241–254. doi:10.1017/S0033291708003590
Alström, J. E., Nordlund, C. L., Persson, G., Harding M., & Ljungqvist, C. (1984).
Effects of four treatment methods on social phobic patients not suitable for
insight-oriented psychotherapy. Acta Psychiatrica Scandanavia, 70(1), 97-110.
American Psychiatric Association. (1980). Diagnostic and statistical manual of mental
disorders (3rd ed.).Washington, DC: Author.
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental
disorders (4th ed., text rev.). Washington, DC: Author.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental
disorders (5th ed.). Washington, DC: Author.
Andersson, G., & Carlbring, P. (2009). Commentary on Berger, Hohl, and Caspar's
(2009) Internet-based treatment for social phobia: a randomized controlled
trial. Journal of Clinical Psychology, 65, 1036-1038. doi:10.1002/jclp.20617
Beck, A. (1976). Cognitive therapy and the emotional disorders. New York, N.Y:
International Universities Press.
Beck, A. T., Emery, G., & Greenberg, R. L. (1985). Anxiety disorders and phobias: A
cognitive perspective. New York, NY: Basic Books.
Beck, A. T., Rush, A., Shaw, B., & Emery, G. (1979). Cognitive therapy of depression.
New York, N.Y: Guilford Press.
Beck, A., Steer, R., & Carbin, M. (1988). Psychometric properties of the Beck Depression
Inventory: Twenty-five years of evaluation. Clinical Psychology Review, 8, 77-
100. doi:10.1016/0272-7358(88)90050-5
Beck, A.T., Steer, R.A., & Brown, G.K. (1996). Manual for Beck Depression Inventory-
II. San Antonio, TX: Psychological Corporation.
Beck, J., & Beck, J. (2011). Cognitive behavior therapy. New York, N.Y: Guilford Press.
Beidel, D. C., Turner, S. M., & Dancu, C. V. (1985). Physiological, cognitive, and
behavioral aspects of social anxiety. Behaviour Research and Therapy, 23, 109–
117.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 28
Biran, M., Augusto, F., & Wilson, G. (1981). In vivo exposure vs cognitive restructuring
in the treatment of scriptophobia. Behaviour Research and Therapy, 19, 525-532.
doi:10.1016/0005-7967(81)90079-6
Blomhoff, S., Haug, T. T., Hellström, K., Holme, I., Humble, M., Madsbu, H. P., &
Wold, J. E. (2001). Randomised controlled general practice trial of sertraline,
exposure therapy and combined treatment in generalised social phobia. The
British Journal of Psychiatry, 179, 23–30. doi:10.1192/bjp.179.1.23
Brown, T. A., DiNardo, P. A., Lehman, C. L., & Campbell, L. A. (2001). Reliability of
DSM-IV anxiety and mood disorders: Implications for the classification of
emotional disorders. Journal of Abnormal Psychology, 110, 49–58.
doi:10.1037//0021-843X.110.1.49
Butler, G. (1985). Exposure as a treatment for social phobia: Some instructive difficulties.
Behaviour Research and Therapy, 23, 651-657.
Butler, G. (1989). Issues in the applications of cognitive and behavioral strategies to the
treatment of social phobia. Clinical Psychology Review, 9(1), 91-106.
Butler, G., Cullington, A., Munby, M., Amies, P., & Gelder, M. (1984). Exposure and
anxiety management in the treatment of social phobia. Journal of Consulting and
Clinical Psychology, 52, 642-650. doi:10.1037/0022-006x.52.4.642
Clark, D., & Beck, A. (2010). Cognitive therapy of anxiety disorders. New York, N.Y:
Guilford Press.
Cox, B. J., Swinson, R. P., & Shaw, B. F. (1991). Value of the Fear Questionnaire in
differentiating agoraphobia and social phobia. British Journal of Psychology, 159,
842–845. doi: 10.1192/bjp.159.6.842
DiNardo, P. A., & Barlow, D. H. (1988). Anxiety Disorders Interview Schedule - Revised
(ADIS-R). New York, N.Y: Graywind Publications: Albany.
Dozois, D. J. A., Dobson, K. S., & Ahnberg, J. L. (1998). A psychometric evaluation of
the Beck Depression Inventory–II. Psychological Assessment, 10, 83–89.
doi:10.10372F2F1040-3590.10.2.83
Emmelkamp, P. M. G. (1982). Phobic and obsessive-compulsive disorders: Theory,
research and practice. New York: Plenum Press.
Emmelkamp, P., Mersch, P., Vissia, E., & van der Helm, M. (1985). Social phobia: A
comparative evaluation of cognitive and behavioral interventions. Behaviour
Research and Therapy, 23, 365-369. doi:10.1016/0005-7967(85)90015-4
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 29
Hair, J. F., Black, W. C., Babin, B. J., & Anderson, R. E. (2010). Multivariate data
analysis (7th ed.). New Jersey: Pearson Education.
Hammen, C., Jacobs, M., Mayol, A., & Cochran, S. (1980). Dysfunctional cognitions and
the effectiveness of skills and cognitive behavioral assertion training. Journal of
Consulting and Clinical Psychology, 48, 685-695. doi:10.1037//0022-
006x.48.6.685
Heimberg, R. G. (1989). Cognitive and behavioral treatments for social phobia: A critical
analysis. Clinical Psychology Review, 9, 107-128. doi:10.1016/0272-
7358(89)90050-0
Heimberg, R. G. (1991). Cognitive behavioral treatment for social phobias in a group
setting: A treatment manual (Second Edition). New York, N.Y: University at
Albany, State University of New York.
Heimberg, R. G., Dodge, C. S., Hope, D. A., Kennedy, C. R., & Zollo, L. J. (1990a).
Cognitive behavioural group treatment for social phobia: Comparison with a
credible placebo control. Cognitive Therapy and Research, 14, 1–23.
doi:10.1007/BF01173521
Heimberg, R. G., Nyman, D., & O’Brien, G. T. (1987). Assessing variations of the
Thought-Listing Technique: Effects of instructions, stimulus intensity, stimulus
modality, and scoring procedures. Cognitive Therapy and Research, 11, 12–24.
doi:10.10072FBF01183129
Heimberg, R., Bruch, M., Hope, D., & Dombeck, M. (1990b). Evaluating the states of
mind model: Comparison to an alternative model and effects of method of
cognitive assessment. Cognitive Therapy and Research, 14, 543-557.
doi:10.1007/bf01173363
Heimberg, R.G. (1991). Cognitive behavioral treatment for social phobias in a group
setting: A treatment manual (2nd Ed.).New York, N.Y: University at Albany,
State University of New York.
Heinrichs, N., & Hoffman, S. G. (2005). Cognitive assessment of social anxiety: A
comparison of self-report and thought listing methods. Cognitive Behavior
Therapy, 34, 3–25. doi:10.1080/16506070410030106
Hergenhahn, B. R. (1992). An introduction to the history of psychology (2nd Ed.).
Belmont, CA: Wadsworth.

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 30
Hindo, C., & Gonzalez-Prendes, A. (2011). One-session exposure treatment for social
anxiety with specific fear of public speaking. Research on Social Work
Practice, 21, 528-538. doi:10.1177/1049731510393984
Hofmann S. G., & Otto, M. W. (2008). Cognitive-behavior therapy of social anxiety
disorder: Evidence-based and disorder specific treatment techniques. New York,
NY: Routledge.
Holmes, E. A., Arntz, A., & Smucker, M. R. (2007). Imagery rescripting in cognitive
behaviour therapy: Images, treatment techniques and outcomes. Journal of
Behavior Therapy & Experimental Psychiatry, 38, 297-305.
doi:10.1016/j.jbtep.2007.10.007
Hope, D. A., Burns, J. A., Hayes, S. A., Herbert, J. D., & Warner, M. D. (2010).
Automatic thoughts and cognitive restructuring in cognitive behavioral group
therapy for social anxiety disorder. Cognitive Therapy and Research, 34, 1-12.
doi:10.1007/s10608-007-9147-9
Hope, D. A., Heimberg, R. G., & Bruch, M. A. (1995). Dismantling cognitive-
behavioural group therapy for social phobia. Behavior Research and Therapy, 33,
637–650. doi:10.1016/0005-7967(95)00013-N
Jerremalm, A., Jansson, L., & Öst, L. (1986). Cognitive and physiological reactivity and
the effects of different behavioral methods in the treatment of social phobia.
Behaviour Research and Therapy, 24, 171-180. doi:10.1016/0005-
7967(86)90088-4
Jørstad-Stein, E. C., & Heimberg, R. G. (2009). Social phobia: An update on treatment.
Psychiatric Clinics of North America, 32, 641-663.
Kanter, N., & Goldfried, M. (1979). Relative effectiveness of rational restructuring and
self-control desensitization in the reduction of interpersonal anxiety. Behavior
Therapy, 10, 472-490. doi:10.1016/s0005-7894(79)80051-9
Leichsenring, F., Salzer, S., Beutel, M. E., Herpertz, S., HiDer, W., Hoyer, J., & ...
Leibing, E. (2013). Psychodynamic therapy and cognitive-behavioral therapy in
social anxiety disorder: A multicenter randomized controlled trial. American
Journal of Psychiatry, 170, 759-767. doi:10.1176/appi.ajp.2013.12081125
Lochner, C., Hemmings, S., Seedat, S., Kinnear, C., Schoeman, R., Annerbrink, K., &
Stein, D. J. (2007). Genetics and personality traits in patients with social anxiety
disorder: A case-control study in South Africa. European
Neuropsychopharmacology, 17, 321-327. doi:10.1016/j.euroneuro.2006.06.010
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 31
Marcus, H. (1977). Self-schemata and processing information about the self. Journal of
Personality and Social Psychology, 35(2), 63-78.
Marks, I. M. (1987). Fears, phobias, and rituals. New York, NY: Oxford University
Press.
Marks, I. M., & Mathews, A. M. (1979). Brief standard self-rating for phobic patients.
Behaviour Research and Therapy, 24, 83-85.
Mattick, R. P., & Peters, L. (1988). Treatment of severe social phobia: Efforts of guided
exposure with and without cognitive restructuring. Journal of Consulting and
Clinical Psychology, 56, 251–260.
Mattick, R. P., Peters, L., & Clarke, J. C. (1989). Exposure and cognitive restructuring for
social phobia: A controlled study. Behavior Therapy, 20, 3– 23.
doi:10.1016/S0005-7894(89)80115-7
McEvoy, P., Nathan, P., Rapee, R., & Campbell, B. (2012). Cognitive behavioural group
therapy for social phobia: Evidence of transportability to community clinics.
Behaviour Research and Therapy, 50, 258-265. doi:10.1016/j.brat.2012.01.009
Mersch, P. P. A. (1995). The treatment of social phobia: The differential effectiveness of
exposure in vivo and an integration of exposure in vivo, rational emotive therapy
and social skills training. Behavior Research and Therapy, 33, 259–269.
doi:10.1016/0005-7967(94)00038-L
Mörtberg, E. (2014). Working alliance in individual and group cognitive therapy for
social anxiety disorder. Psychiatry Research, 220, 716-718.
doi:10.1016/j.psychres.2014.07.004
Norton, P., & Price, E. (2007). A meta-analytic review of adult cognitive-behavioral
treatment outcome across the anxiety disorders. The Journal of Nervous and
Mental Disease, 195, 521-531. doi:10.1097/01.nmd.0000253843.70149.9a
Rapee, R. M., & Heimberg, R. G. (1997). A cognitive–behavioural model of anxiety in
social phobia. Behavior Research and Therapy, 35, 741–756. doi:10.1016/S0005-
7967(97)00022-3
Rodebaugh, T., Holaway, R., & Heimberg, R. (2004). The treatment of social anxiety
disorder. Clinical Psychology Review, 24(7), 883-908.
http://dx.doi.org/10.1016/j.cpr.2004.07.007
Sadock, B., Sadock, V., & Ruiz, P. (2015). Kaplan and Sadock's synopsis of psychiatry.
Philadelphia, P.A: Wolter Kluwer.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 32
Scholing, A., & Emmelkamp, P. (1993). Exposure with and without cognitive therapy for
generalized social phobia: Effects of individual and group treatment. Behaviour
Research and Therapy, 31(7), 667-681. doi:10.1016/0005-7967(93)90120-j
Schultz, D. P. & Schultz, S. E. (1992). A history of modern psychology (5th Ed.). New
York, N.Y: Harcourt Brace.
Shikatani, B., Antony, M. M., Kuo, J. R., & Cassin, S. E. (2014). The impact of cognitive
restructuring and mindfulness strategies on postevent processing and affect in
social anxiety disorder. Journal of Anxiety Disorders, 28, 570-579.
doi:10.1016/j.janxdis.2014.05.012
Spiegler, M.D., & Guevremont, D.C. (2003). Contemporary behavior therapy (4th Ed.).
Belmont, CA: Thomson / Wadsworth.
Taylor, S. (1996). Meta-analysis of cognitive–behavioural treatments for social phobia.
Journal of Behavior Therapy and Experimental Psychiatry, 27, 1–9.
doi:10.10162F0005-791628952900058-5
Turner, S. (1994). A multicomponent behavioral treatment for social phobia: Social
effectiveness therapy. Behaviour Research and Therapy, 32, 381-390.
doi:10.1016/0005-7967(94)90001-9
Turner, S., Beidel, D., Dancu, C., & Stanley, M. (1989). An empirically derived inventory
to measure social fears and anxiety: The social phobia and anxiety inventory.
Psychological Assessment, 1, 35-40. doi:10.1037//1040-3590.1.1.35
Watson, D., & Friend, R. (1969). Measurement of social-evaluative anxiety. Journal of
Consulting and Clinical Psychology, 33, 448–457. doi:10.10372Fh0027806
Wells, A., Clark, D. M., Salkovskis, P., Ludgate, J., Hackmann, A., & Gelder, M. (1995).
Social phobia: The role of in-situation safety behaviors in maintaining anxiety and
negative beliefs. Behavior Therapy, 26, 153–161. doi:10.1016/S0005-
7894(05)80088-7
Wersebe, H., Sijbrandij, M., & Cuijpers, P. (2013). Psychological group-treatments of
social anxiety disorder: A meta-analysis. Plos ONE, 8, 1-4.
doi:10.1371/journal.pone.0079034
Williams, D., Herman, A., Stein, D., Heeringa, S., Jackson, P., Moomal, H., & Kessler, R.
(2007). Twelve-month mental disorders in South Africa: Prevalence, service use
and demographic correlates in the population-based South African Stress and
Health Study. Psychological Medicine, 38(2), 211-220.
doi:10.1017/s0033291707001420

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 33
Wlazlo, Z., Schroeder-Hartwig, K., Hand, I., Kaiser, G., & Munchau, N. (1990).
Exposure in vivo vs. social skills training for social phobia: Long-term outcome
and differential effects. Behaviour Research and Therapy, 28, 181-193.
Wolpe, J., & Lazarus, A. A. (1966). Behavior therapy techniques. Oxford, UK: Pergamon
Press.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 34
Appendices
Please find the following Appendices attached to this research proposal:
A. Ethical Clearance Form
B. Measuring Instruments
C. Plagiarism declaration
D. Turn-it-in report
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 35
Appendix A
Ethical Clearance Form
(See next page)

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 36
Appendix B
Measuring Instruments:
1. General questionnaire
2. Fear Questionnaire
3. Thought Listing Technique
4. Social Phobia Anxiety Index
5. Becks Depression Inventory
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 37
1. General Questionnaire
Please fill in this questionnaire and post it to:
The Social Research Project (TEL.: 021-8084994)
Unit of Clinical Psychology (FAKS.: 021- )
University of Stellenbosch
Private Bag X1
MATIELAND
7602
Please omit those questions that you are uncertain of. These can be discussed during our first
interview. The questionnaire must reach us before the interview date.
NAME (e.g. Mrs. T.D. Cloete): ...............................
FIRST NAME (e.g. Trudie): ...................................
____________________________________________________________
FOR ADMINISTRATIVE PURPOSES ONLY:
Dates: First interview:............Interviewer:.............
Pretest:.............................................
Posttest:............................................
Follow up:...........................................
Group:............
Referred by:.................................Tel:...........
____________________________________________________________
ADDRESSES: Home:............................................
............................................
Postal:..........................................
Other (e.g. university residence):...............
TEL. (code and number please):
Home:..................................................
Work:..................................................
Other: (e.g. spouse, parents, during holidays; specify
please)................................. .......................................................
DATE OF BIRTH:.................. AGE:.........SEX:..........
MARITAL HISTORY (e.g. married, single, cohabiting, divorced, widowed; specify dates where
applicable):
....................................................................................................................................................................
................
............................................................
CHILDREN:
Still If not,
Age Sex Standard/ Occupation at home? When left?
... ... ................... ........ ..........
... ... ................... ........ ..........
... ... ................... ........ ..........
... ... ................... ........ ..........
... ... ................... ........ ..........
EDUCATIONAL AND OCCUPATIONAL HISTORY:
Date Specifications (e.g. highest standard, qualifications, previous and present occupation[s])
........ .............................................
........ .............................................
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 38
........ .............................................
........ .............................................
........ .............................................
Spouse
........ .............................................
........ .............................................
........ .............................................
........ .............................................
RELIGIOUS DENOMINATION:.....................................
NAME OF GENERAL PRACTITIONER:...................TEL: .......
MEDICAL HISTORY:
Present:
Specify any physical illness and/or mental (emotional/ psychological) problems that you are currently
experiencing, when it started, and any times or periods of remission (when it didn't bother you or
when you were temporarily well):
....................................................................................................................................................................
........................................................................................................................................
Specify all prescribed medicines you are currently taking, the dose, the doctor who prescribed it and
the period you are taking it:
............................................................
............................................................
............................................................
............................................................
............................................................
Specify any other form of treatment (e.g., psychotherapy) that you are receiving or received in the
past month:
....................................................................................................................................................................
................
Past:
Specify major physical and mental (emotional/ psychological) problems of the past, when it started,
how long it lasted, the medicine you took, how long you took it, and/or any other form of treatment
(e.g., psychotherapy) you received:
....................................................................................................................................................................
................
............................................................
............................................................
Past or present:
Have you experienced problems with medications such as side effects, withdrawel problems?
Yes ........ No..........
Specify: ...................................................
.......................................................
TOBACCO, CAFFEINE AND ALCOHOL USE:
Specify average intake per day:
Smoking: ..............................................
Coffee: ...............................................
Tea: ..................................................
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 39
Specify your approximate current average alcohol intake (type of drink and amount) during the week
and on weekends: .......................................................
............................................................
............................................................
EXERCISE, HOBBIES, RECREATION:
Specify your current activities and any changes in past year (e.g., went to Gym for two months but
stopped in November):
....................................................................................................................................................................
............................................................................
FAMILY HISTORY OF PSYCHOLOGICAL DISORDERS:
Has anybody in your family (mother, father, siblings, aunts, uncles, grandparents) ever been treated or
hospitalized for anxiety, depression, alcohol or drug abuse, or other such problems, or had any such
problems but did not seek treatment?
Yes ........ No..........
Relationship
....................................................................................................................................................................
................
Dates
....................................................................................................................................................................
................
Description of problem
....................................................................................................................................................................
................
Treatment
....................................................................................................................................................................
................

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 40
2. Fear Questionnaire – FQ-TP
Marks & Mathews
Name:........................Group:.......Date:.............
Choose a number from the scale below to show how much you would avoid each of the situations
listed below because of fear or other upleasant feelings. Then write the number you chose in the box
opposite each situation.
0 1 2 3 4 5 6 7 8
------------------------------------------------------------
Would Slightly Definitely Markedly Always
not avoid avoid avoid avoid
avoid it it it it
it
1. Main phobia you want treated (describe in
your own words)...................................
..................................................
.........................................................
2. Eating or drinking with other people.....................
3. Being watched or stared at...............................
4. Talking to people in authority...........................
5. Being criticised........................................
6. Speaking or acting to an audience.......................
How would you rate the present state of your phobic symptoms on the scale below?
0 1 2 3 4 5 6 7 8
------------------------------------------------------------
No Slightly Definitely Markedly Very
phobias disturbing/ disturbing/ disturbing/ severely
present not really disabling disabling disturbing/
disabling disabling
Please circle one number between 0 and 8
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 41
3. Thought Listing Technique – TLT-SOM
Name:........................ Group:............ Date:..................
In the boxes below, please write down as many thoughts as you can recall having while you were
involved (in your imagination) in the interaction or speaking situation just completed. Examples of
thoughts a person may have include:
"I'm not making a good impression"
"They probably won't like me"
"I know I'm going to panic"
"I'm all alone"
"There is no reason for me to be upset like this"
"I think they like me"
"I feel like . . ."
Remember, these are only examples. Please write whatever you were thinking. Please be completely
honest and remember that your responses will remain confidential. Don't spend too much time on any
one thought and don't worry about spelling or grammar. Write only one thought in each box. Please
try to remember as many thoughts as possible.
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\
\------------------------------------------------------------------------/
/------------------------------------------------------------------------\

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 42
4. Social Phobia Anxiety Index - SPAI
Developed by S. M. Turner. C. V. Dancu. and D. C. Beidel
Below is a list of behaviors that may or may not be relevant for you. Based on your personal
experience, please indicate how frequently you experience these feelings and thoughts in social
situations. A social situation is defined as a gathering of two or more people. For example: A
meeting; a lecture; a party; bar or restaurant; conversing with one other person or group of people,
etc. FEELING ANXIOUS IS A MEASURE OF HOW TENSE. NERVOUS OR
UNCOMFORTABLE YOU ARE DURING SOCIAL ENCOUNTERS. Please use the scale listed
below and circle the number which best reflects how frequently you experience these responses.
Never
Very
Infrequent Infrequent Sometimes Frequent
Very
Frequent Always
1 2 3 4 5 6 7 !
1. I feel anxious when entering social situations where there is a small group.............................
2. I feel anxious when entering social situations where there is a large group.......................................
3. I feel anxious when I am in a social situation and I become the center of
a t t e n t i o n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4. I feel anxious when I am in a social situation and I am expected to engage in s o me a c t i v i t y
5. I feel anxious when making a speech in front of an audience.............................................
6. I fed anxious when speaking in a small informal meeting..........................................
7. I fed so anxious about attending social gatherings that I avoid these
s i t u a t i o n s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8. I fed so anxious in social situations that I leave the social gathering.....................................
9. I fed anxious when in a small lathering with:
s t r a n g e r s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
a u t h o r i t y f i gu r e s . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
o p p o s i t e s e x . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
people in genera l . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11. I feel anxious when in a bar or restaurant with:
strangers ................................................................................................................ ............................... authority figures ............................................................... opposite sex ........................................................................................................................................... people in general ...............................................................................................................................
12. I feel anxious and I do not know what to do when in a new situation with: strangers ................................................................................................................................................ authority figures ...................................................................................................... ............................ opposite sex .............................................................................................................. ............................ people in general ..................................................................................................... ............................
13. I fed anxious and I do not know what to do when in a situation involving
confrontation with: strangers ..................................................................................................................... authority figures ........................................................................................................ opposite sex ...............................................................................................................
people in general .................................................................................................
14. I feel anxious and I do not know what to do when in an embarrassing
situation with:
strangers ...............................................................................................................
authority figures ............................................................................................... opposite sex ...........................................................................................................
people in general ..................................................................................................
15. I feel anxious when discussing intimate feelings with:
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 43
strangers .................................................................................................................
authority figures ....................................................................................................
opposite sex ...........................................................................................................
people in general ..................................................................................................
16. I feel anxious when stating an optional to:
strangers .................................................................................................................
authority figures ................................................................................................ opposite sex ............................................................................................................
people in general .................................................................................................. 17. I feel anxious when calking about business with:
strangers .................................................................................................................. authority figures .................................................................................................... opposite sex .......................................................................................................................... people in general .................................................................................................
18. I feel anxious when approaching and/or initiating a conversation with: strangers ................................................................................................................... authority figures ..................................................................................................... opposite sex ........................................................................................................................ .. people in general ................................................................................................. ..
19. I feel anxious when having to interact for longer than a few minutes with:
strangers ................................................................................................................ .. authority figures. opposite sex .......................................................................................................................... . people in general .................................................................................................. .
20. I fed anxious when drinking (any type of beverage) and/or eating in front
of: strangers .................................................................................................................. ... authority figures .........................................................................................................
opposite sex ...................................................................................................... people in general .....................................................................................................
21. I feel anxious when writing or typing in front of: strangers .....................................................................................................................
authority figures ................................................................................................
opposite sex ....................................................................................................... people in general .................................................................................................. ...
22. I fed anxious when speaking in front of: strangers .................................................................................................................. .
authority figures ........................................................................................ ..... opposite sex ......................................................................................................... people in general ....................................................................................................
23. I feel anxious when being criticized or rejected by: strangers ......................................................................... ........................................ authority figures ............................................................ ....................................... opposite sex ............................................................................ ...................................... people in general ........................................................ ......................................
24. I attempt to avoid social situations where there are: strangers ................................................................................................................ authority figures ............................................................ ....................................... opposite sex ............................................................................. ...................................... people in general .......................................................... ......................................
25. I leave social situations where there are: strangers ........................................................................... ...................................... authority figures ............................................................ ...................................... opposite sex ............................................................................. ...................................... people in general ......................................................... ......................................
26. Before entering a social situation I think about all the things that can go wrong. The types of
thoughts I experience are:
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 44
Will I be dressed properly? ................................................................................. I will probably make a mistake and look foolish ............................................ What will 1 do if no one speaks to me? ............................................................
If there is a lag in the conversation what can [ talk about? ........................ People will notice how anxious I am .................................................................
27. I feel anxious before entering a social situation ..................................... — 28. My voice leaves me or changes when I am talking in a social situation ------
29. I am not likely to speak to people until they speak to me .........................
.
30. I experience troublesome thoughts when I am in a social setting. For
example:
I wish I could leave and avoid the whole situation .....................................
If I mess up again I will really lose my confidence...................................
. What kind of impression am I making? ..................................................... Whatever I say it will probably sound stupid ...............................................
31. I experience the following prior to entering a social situation: sweating................................................................................................................. frequent urge to urinate...................................................................................... heart palpitations __ ..........................................................................................
32. I experience the following in a social situation:
sweating ...........................................................................................................
blushing ...........................................................................................................
shaking ............................................................................................................
frequent urge to urinate ..................................................................................
heart palpitations ............................................................................................
33. I feel anxious when I am home alone .............................................................
34. I feel anxious when I am in a strange place.....................................................
35. I fed anxious when I am on any form of public transportation (i.e., bus,
train, airplane).." ..............................................................................................
36. I fed anxious when crossing streets .................................................................
37. I fed anxious when I am in crowded public places (i.e., stores, church,
movies, restaurants, etc.) .................................................................................
38. Being in large open spaces makes me feel anxious ............................ ".;.- ----
39. I fed anxious when I am in enclosed places (elevators, tunnels, etc.) ..........
40. Being in high places makes me feel anxious (i.e., tall buildings) ...................
41. I fed anxious when waiting in a long line .....................................................
42. There are times when I feel like I have to hold on to things because I am
afraid I will fall ...............................................................................................
43. When I leave home and go to various public places, I go with a family
member or friend ..............................................................................................
44. ( fed anxious* when riding in a car .................................................................
45. There are certain places I do not go to because I may feel trapped .........

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 45
5. Beck’s Depression Inventory - BDI
Instructions: This questionnaire consists of 21 groups of statements. Please read each group of
statements carefully, and then pick out the one statement in each group that best describes the way
you have been feeling during the past two weeks, including today. Circle the number beside the
statement you have picked. If several statements in the group seem to apply equally well, circle the
highest number for that group. Be sure that you do not choose more than one statement for any group,
including Item 16 (Changes in sleeping pattern) or Item 18 (Changes in appetite).
1. Sadness
0 I do not feel sad.
1 I feel sad much of the time.
2 I am sad all the time.
3 I am so sad or unhappy that I can't stand it.
2. Pessimism
0 I am not discouraged about my future.
1 I feel more discouraged about my future than I used to be.
2 I do not expect things to work out for me.
3 I feel my future is hopeless and will only get worse.
3. Past failure
0 I do not feel like a failure.
1 I have failed more than I should have.
2 As I look back, I see a lot of failures.
3 I feel I am a total failure as a person.
4. Loss of pleasure
0 I get as much pleasure as I ever did from the things I enjoy.
1 I don't enjoy things as much as I used to.
2 I get very little pleasure from the things I used to enjoy.
3 I can't get any pleasure from the things I used to enjoy.
5. Guilty feelings
0 I don't feel particularly guilty.
1 I feel guilty over many things I have done or should have done.
2 I feel quite guilty most of the time.
3 I feel guilty all of the time.
6. Punishment feelings
0 I don't feel I am being punished.
1 I feel I may be punished.
2 I expect to be punished.
3 I feel I am being punished.
7. Self-dislike
0 I feel the same about myself as ever.
1 I have lost confidence in myself.
2 I am disappointed in myself.
3 I dislike myself.
8. Self-criticalness

SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 46
0 I don't criticize or blame myself more than usual.
1 I am more critical of myself than I used to be.
2 I criticize myself for all of my faults.
3 I blame myself for everything bad that happens.
9. Suicidal thoughts or whishes
0 I don't have any thoughts of killing myself.
1 I have thoughts of killing myself, but I would not carry them out.
2 I would like to kill myself.
3 I would kill myself if I had the chance.
10. Crying
0 I don't cry anymore than I used to.
1 I cry more than I used to.
2 I cry over every little thing.
3 I feel like crying, but I can't.
11. Agitation
0 I am no more restless or wound up than usual.
1 I feel more restless or wound up than usual.
2 I am so restless or agitated that it's hard to stay still.
3 I am so restless or agitated that I have to keep moving or doing something.
12. Loss of interest
0 I have not lost interest in other people or activities.
1 I am less interested in other people or things than before.
2 I have lost most of my interest in other people or things.
3 It's hard to get interested in anything.
13. Indecisiveness
0 I make decisions about as well as ever.
1 I find it more difficult to make decisions than usual.
2 I have much greater difficulty in making decisions than I used to.
3 I have trouble making any decisions.
14. Worthlessness
0 I do not feel I am worthless.
1 I don't consider myself as worthwhile and useful as I used to.
2 I feel more worthless as compared to other people.
3 I feel utterly worthless.
15. Loss of energy
0 I have as much energy as ever.
1 I have less energy than I used to have.
2 I don't have enough energy to do very much.
3 I don't have enough energy to do anything.
16. Changes in sleeping pattern
0...I have not experienced any change in my sleeping pattern.
1a I sleep somewhat more than usual.
1b I sleep somewhat less than usual.
2a I sleep a lot more than usual.
2b I sleep a lot less than usual.
3a I sleep most of the day.
3b I wake up 1-2 hours early and can't get back to sleep.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 47
3b I wake up 1-2 hours early and can't get back to sleep.
17. Irritability
0 I am no more irritable than usual.
1 I am more irritable than usual.
2 I am much more irritable than usual.
3 I am irritable all the time.
18. Changes in appetite
0..I have not experienced any change in my appetite.
1a My appetite is somewhat less than usual.
1b My appetite is somewhat greater than usual.
2a My appetite is much less than before.
2b My appetite is much greater than usual.
3a I have no appetite at all.
3b I crave food all the time.
19. Concentration difficulty
0 I can concentrate as well as ever.
1 I can't concentrate as well as usual.
2 It's hard to keep my mind on anything for very long.
3 I find I can't concentrate on anything.
20. Tiredness or fatigue
0 I am no more tired or fatigued than usual.
1 I get more tired or fatigued more easily than usual.
2 I am too tired or fatigued to do a lot of the things I used to do.
3 I am too tired or fatigued to do most of the things I used to do.
21. Loss of interest in sex
0 I have not noticed any recent change in my interest in sex.
1 I am less interested in sex than I used to be.
2 I am much less interested in sex now.
3 I have lost interest in sex completely.
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 48
Appendix C
Plagiarism Declaration
1 Plagiarism is the use of ideas, material and other intellectual property of another’s work
and to present is as my own.
2 I agree that plagiarism is a punishable offence because it constitutes theft.
3 I also understand that direct translations are plagiarism.
4 Accordingly all quotations and contributions from any source whatsoever (including
the internet) have been cited fully. I understand that the reproduction of text without
quotation marks (even when the source is cited) is plagiarism.
5 I declare that the work contained in this assignment is my original work and that I have
not previously (in its entirety or in part) submitted it for grading in this
module/assignment or another module/assignment.
Student number
Signature
Initials and surname
Date
SOCIAL ANXIETY DISORDER: TREATMENTS COMPARED 49
Appendix D
Turn-it-in report
(See next page)
















