
Career transitions of inactive nurses: A registration database analysis (1993–2006)
9
Career transitions of inactive nurses: A registration database analysis (1993–2006) Mohamad Alameddine a, *, Andrea Baumann b , Kanecy Onate c , Raisa Deber c a Faculty of Health Sciences, Department of Health Management and Policy, American University of Beirut, Van Dyck - Room 140B, PO Box 11-0236, Riad El-Solh, Beirut 1107 2020, Lebanon b Faculty of Health Sciences International Health, Michael G. DegGroote Centre for Learning, McMaster University, Canada c Health Policy Management and Evaluation Department, Faculty of Medicine, University of Toronto, Health Sciences Building, 155 College Street, Suite 425. Toronto, ON M5T 3M6, Canada International Journal of Nursing Studies 48 (2011) 184–192 ARTICLE INFO Article history: Received 25 February 2010 Received in revised form 13 May 2010 Accepted 16 June 2010 Keywords: Canada Career transitions Nurses Policy Reintegration ABSTRACT Background: One important strategy to address nursing shortages is to tap into the pool of licensed nurses who are not currently working in nursing and induce them to return to the nursing labour market. However, there is a paucity of research examining their likelihood of return to the active labour market. Objective: Analyze the career transitions of nurses registered with the College of Nurses Ontario but not working in the province’s nursing labour market to determine the proportion of these nurses rejoining the active nursing workforce and examine the variation by inactive sub-category and age group. Design: Quantitative analysis of a linked longitudinal database for all those registered with the College of Nurses of Ontario for the years 1993–2006. Methods: Registration records of all 215,687 nurses registered at any time in those years were merged by their unique registration number. Each nurse was placed for each year into an employment category. Two groups of nurses were defined: active (registered, working in nursing in Ontario) and inactive (registered, not working in nursing in Ontario). Inactive nurses were then sub-categorized into five mutually exclusive sub-categories: ‘not working and seeking nursing employment’, ‘working in non-nursing and seeking nursing employment’, ‘not working and not seeking nursing employment’, ‘working in non-nursing and not seeking nursing employment’ and ‘working outside Ontario’. One- year career movements of nurses were tracked by generating 13 year-to-year transition matrixes. Results: In the short-term, inactive nurses seeking a nursing job had the highest average rate of return to the active workforce (27.3–30.8%), though they might become high risk of leaving the profession if they do not find employment in a timely manner. Inactive nurses not seeking nursing employment are a heterogeneous group, and include nurses on leave who are likely to subsequently rejoin the active workforce should appropriate opportunities arise. The proportion of nurses rejoining the active workforce decreased with age. Conclusion: Because ‘inactive’ nurses are a heterogeneous group, their optimal reintegra- tion to the nursing workforce requires governments, professional associations and employers to work collaboratively to design targeted and timely recruitment strategies to avoid the permanent loss of skilled nursing resources. ß 2010 Elsevier Ltd. All rights reserved. * Corresponding author. Tel.: +961 1 350000x4693; fax: +961 1 744470. E-mail address: [email protected] (M. Alameddine). Contents lists available at ScienceDirect International Journal of Nursing Studies journal homepage: www.elsevier.com/ijns 0020-7489/$ – see front matter ß 2010 Elsevier Ltd. All rights reserved. doi:10.1016/j.ijnurstu.2010.06.009
-
Upload
mohamad-alameddine -
Category
Documents
-
view
214 -
download
0
Transcript of Career transitions of inactive nurses: A registration database analysis (1993–2006)

International Journal of Nursing Studies 48 (2011) 184–192
Career transitions of inactive nurses: A registration database analysis(1993–2006)
Mohamad Alameddine a,*, Andrea Baumann b, Kanecy Onate c, Raisa Deber c
a Faculty of Health Sciences, Department of Health Management and Policy, American University of Beirut, Van Dyck - Room 140B, PO Box 11-0236, Riad El-Solh,
Beirut 1107 2020, Lebanonb Faculty of Health Sciences International Health, Michael G. DegGroote Centre for Learning, McMaster University, Canadac Health Policy Management and Evaluation Department, Faculty of Medicine, University of Toronto, Health Sciences Building, 155 College Street, Suite 425. Toronto,
ON M5T 3M6, Canada
A R T I C L E I N F O
Article history:
Received 25 February 2010
Received in revised form 13 May 2010
Accepted 16 June 2010
Keywords:
Canada
Career transitions
Nurses
Policy
Reintegration
A B S T R A C T
Background: One important strategy to address nursing shortages is to tap into the pool of
licensed nurses who are not currently working in nursing and induce them to return to the
nursing labour market. However, there is a paucity of research examining their likelihood
of return to the active labour market.
Objective: Analyze the career transitions of nurses registered with the College of Nurses
Ontario but not working in the province’s nursing labour market to determine the
proportion of these nurses rejoining the active nursing workforce and examine the
variation by inactive sub-category and age group.
Design: Quantitative analysis of a linked longitudinal database for all those registered
with the College of Nurses of Ontario for the years 1993–2006.
Methods: Registration records of all 215,687 nurses registered at any time in those years
were merged by their unique registration number. Each nurse was placed for each year
into an employment category. Two groups of nurses were defined: active (registered,
working in nursing in Ontario) and inactive (registered, not working in nursing in Ontario).
Inactive nurses were then sub-categorized into five mutually exclusive sub-categories:
‘not working and seeking nursing employment’, ‘working in non-nursing and seeking
nursing employment’, ‘not working and not seeking nursing employment’, ‘working in
non-nursing and not seeking nursing employment’ and ‘working outside Ontario’. One-
year career movements of nurses were tracked by generating 13 year-to-year transition
matrixes.
Results: In the short-term, inactive nurses seeking a nursing job had the highest average
rate of return to the active workforce (27.3–30.8%), though they might become high risk of
leaving the profession if they do not find employment in a timely manner. Inactive nurses not
seeking nursing employment are a heterogeneous group, and include nurses on leave who
are likely to subsequently rejoin the active workforce should appropriate opportunities arise.
The proportion of nurses rejoining the active workforce decreased with age.
Conclusion: Because ‘inactive’ nurses are a heterogeneous group, their optimal reintegra-
tion to the nursing workforce requires governments, professional associations and
employers to work collaboratively to design targeted and timely recruitment strategies to
avoid the permanent loss of skilled nursing resources.
� 2010 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
* Corresponding author. Tel.: +961 1 350000x4693; fax: +961 1 744470.
E-mail address: [email protected] (M. Alameddine).
0020-7489/$ – see front matter � 2010 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ijnurstu.2010.06.009

M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192 185
What is already known about the topic
� M
ost countries around the globe are suffering from achronic shortage of nurses; expected to intensify in thefuture. � A more efficient utilization of the pool of nurses ispossible; many educated and experienced nurses areeither unemployed or not working as nurses.
� In active nurses outside the nursing labour market are astrategic pool potentially providing a relatively quickrelief to nursing shortages.
What this paper adds
� N
urses not currently working in nursing and seeking anursing job might get discouraged and leave nursing ifthey do not find an appropriate job in a timely manner. � N ot seeking nursing employment is a heterogeneouscategory, and may include those on leave who maysubsequently rejoin the active workforce should appro-priate work opportunities arise.
� T he proportion of nurses returning to the activeworkforce decreases with age irrespective of the eligiblesub-category.
1. Introduction
Over the last few decades, many jurisdictions havefound that attempts to contain health care costs have hadthe unintended consequence of destabilizing nursinglabour markets and pushing many practicing nursesoutside the nursing labour market. A variety of reasonshave contributed to destabilizing nursing markets includ-ing hospital downsizing, reengineering, mergers andclosures, cost containment, increased patient acuity andadvances in technology (Aiken et al., 2001; Baranek et al.,2004; Baumann et al., 1998). In many jurisdictions,restructuring negatively impacted the nursing workforceand resulted in serious challenges including: inadequatestaffing and heavy workloads; lack of job stability with theboom-bust cycles of nursing workforce shortages andsurplus; a shift of care outside hospitals and a poor qualityof practice environment (Duffield et al., 2007; McCloskeyand Diers, 2005; Pollock et al., 1999). The trends aredisconcerting as they have been empirically related topoorer health outcomes (including increased mortality),sub-optimal quality of patient care and an exodus of nursesfrom the active workforce (Aiken et al., 2003; O’Brien-Pallas et al., 2004; Unruh, 2003).
Health care delivery requires highly skilled humanresources, and nurses are a key component. Widespreadconcerns have been expressed that the worldwideshortages of nurses are expected to become more severe,particularly given increased service demands, and theaging of the workforce (International Centre for HumanResources in Nursing, 2007). One important strategy toaddress nursing shortage is to tap into the pool ofeducated, trained and licensed yet inactive nurses. Despiteof the strategic importance of this pool of nurses, there is apaucity of research examining the career transitions of
inactive nurses and the likelihood of their return to theactive labour market.
To determine the proportion of inactive nurses rejoin-ing the active nursing workforce and examine variation byinactive sub-category and age group, this study analyzedthe career transitions of inactive nurses using the linkedlongitudinal database for all nurses registered with theCollege of Nurses of Ontario, Canada, for the years 1993–2006.
2. Background
2.1. The nursing labour market
Labour economics provides a framework with which toanalyze the supply and demand for workers in a particularoccupation. It notes that the number of workers can beseen as a stock; over time, people enter and exit thatmarket. The current stock of Full Time Equivalences (FTEs)of nurses in a particular labour market (e.g., province,country) can be replenished through various meansincluding: the supply of new nursing graduates, therecruitment of foreign trained nurses, increase of workhours for nurses (e.g., shift from working part-time to full-time employment) and the return of inactive nursesoutside the labour market to the workforce. Factorscontributing to decreasing the number of nursing FTEsin a particular labour market include: death, disability,emigration, layoffs, retirement and decrease in the numberof work hours (Benjamin et al., 2002).
A labour economics framework points to a number ofpotential policy options to enhance the supply of nursesinto the health labour market. Note that they are notmutually exclusive; most jurisdictions use combinations ofthem. One clear strategy is to train more nurses. Thesestrategies are obviously essential in the long-term (if for noother reason than to balance losses from retirement anddeath), but cannot deal with shortages on the short run.They must also deal with such issues as difficulty attractingqualified students into nursing programs (Crow et al.,2008; Steinbrook, 2002), difficulties with securing thenecessary human and financial resources to expandtraining capacity for nurses (Allan and Aldebron, 2008;Berlin and Sechrist, 2002; Eastaugh, 2004) and the time lagnecessary to train new nurses (Buchan, 2002). Anotherstrategy to addressing nursing shortages is throughemigration/immigration, including the recruitment offoreign trained nurses into the local labour market. Notethat, if the total number is unchanged, these strategies willoften address shortages in one area by creating them inothers, unless some jurisdictions are seen to have too manynurses. Accordingly, the ethics of such a strategy have beenoften criticized since most of these nurses will be recruitedfrom under-resourced developing countries (Blythe andBaumann, 2009; Hooper, 2008; Labonte et al., 2006). Inaddition, certification requirements often hinder thetimely assimilation of foreign trained nurses into thelabor market (Blythe et al., 2009; Kawi and Xu, 2009).
The strategy of encouraging educated and experiencednurses who are currently outside the nursing labourmarket to return enhances and complements health

M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192186
human resources planning and offers the possibility of aquick relief to a shortage situation. A well thought inactivenurses’ recruitment approach could bring a relatively quickinflux of nurses into the workforce, especially if thesenurses have maintained their registration with thecertifying/regulatory body in their country. Investigatingthe career transitions of inactive nurses and the propensityof their return to the active labour market is important toguide recruitment efforts for this strategically importantcohort of nurses.
2.2. Inactive nurses—an overview
We define inactive nurses as those educated as nursesand licensed to practice nursing by the professionalnursing body, who are not currently working in nursingin the jurisdiction where they are licensed. In this study,we focused on those likely to be available for the workforcein the short term; the definition thus excludes thosereaching retirement age (65 years) but includes nursesretiring early from the profession while maintainingregular registration with their licensing body. Inactivenurses account for a sizable proportion of the nursingworkforce in both developing and developed countries. Forexample, the initial findings from the US 2008 NationalSample Survey of Registered Nurses (NSSRN) reports thatinactive nurses constituted 15.2% (466,564) of individualslicensed to practice nursing in the US in 2008 (HumanResources and Service Administration, 2010). Note thatthis definition is jurisdiction-specific, some of these nursesmay indeed be working in another jurisdiction (migrantnurses). Nurse migration presents a different set of policyproblems which are not the focus of this paper, but can behighly significant for some countries.
Inactive nurses who have remained in the samejurisdiction not only represent important opportunitiesto address labour shortages in the short-term, but also arelikely to posses much needed knowledge, skills andexperience for patient care; they may also contribute tothe mentoring of the next generation of nurses (Dussaultet al., 2007). The international literature has pointed to amyriad of reasons for nurses to leave the nursing labourmarket, including better pay outside the health sector,household and family responsibilities, poor workingconditions, heavy work demands and professional burnout(Langan et al., 2007; Myers and Bushnell, 2007; Williamset al., 2006). In the US, issues related to the attractivenessof the workplace were found to be the most commonreason for nurse inactivity in 2004, with 91% of inactivenurses under age 30 selecting it as the main reason for non-participation in the nursing workforce (Black et al., 2008).Clearly, some of these can be addressed by policy changes,while others cannot. Some of these factors are also likely tovary by work setting, while others relate to characteristicsof the individual nurse.
One tool developed for examining the relative attrac-tiveness of a particular work setting for nurses is theconcept of ‘stickiness’—defined as the transition probabil-ity of a nurse who is working in a given setting in year ‘t’remaining in that setting in year ‘t + 1’ (Alameddine et al.,2006). Note that setting can be defined narrowly (e.g., a
particular job or workplace), more broadly (e.g., aparticular sub-sector), or broadly (e.g., remaining innursing). Literature reports that stickiness varies bynursing sub-sector; for example, in Ontario, nurses weremore likely to remain in the hospital sub-sector than in thehome care setting (Alameddine et al., 2006).
Variations across sub-sectors are important clues forexamining the implications of policy changes. For example,in Ontario, as technology has allowed care to shift fromhospital to home and community, hospitals have reducedtheir nurse labour force (Baranek et al., 2004). This shift ofcare outside hospitals occurred without proper transitionplanning, and may have contributed to pushing nursesoutside the nursing labor market. Although policy makershad expected those nurses displaced from hospitals to takenursing jobs in other sectors/sub-sectors of employment,many instead left nursing. Between 1993 and 2006,between one- and two-thirds of nurses transitioning outof the hospital sector became inactive, temporarily orpermanently dropping out of the nursing labour market inthe province between 1993 and 2006 (Alameddine et al.,2009). One purpose of this paper is to examine the extentto which various categories of inactive nurses subsequent-ly returned to the labour force.
3. The study
3.1. Aim
Analyze the career transitions of nurses registered withthe College of Nurses Ontario but not working in theprovince’s nursing labour market to determine theproportion of these nurses rejoining the active nursingworkforce and examine the variation by inactive sub-category, sector/sub-sector of employment and age group.
3.2. Ethical considerations
The study was approved by the appropriate researchethics and governance committees at the University ofToronto. Privacy protection was ensured by anonymizingthe data so that no personal identifiers could be observedfor any of the nurses over the period of the analysis. Alldata analysis was carried out in a secured facility usingpassword-protected computers.
3.3. Design
Registration with the CNO is a prerequisite to workingas a nurse in Ontario. A unique registration number isprovided to each nurse upon registration; afterwards,nurses are required to submit an annual membershiprenewal to CNO in order to be eligible to work. With carefulattention to privacy issues, we created a longitudinaldataset containing linked individual registration data forall nurses registered with the College of Nurses of Ontario,Canada at any time in the years 1993–2006. In order toobserve the career transitions of CNO registered nurses, wehave carried out quantitative analysis of the linkedlongitudinal registration database and generated year-

Table 1
Distribution of nurses in Ontario by employment category (1993–2006).
Employment
category/ year
Total active Total inactive
Number % Number %
1993 109,654 82.1 23,946 17.9
1994 108,028 80.1 26,761 19.9
1995 106,232 81.1 26,334 19.9
1996 105,728 80.5 25,584 19.5
1997 104,039 81.0 24,353 19.0
1998 102,544 80.8 24,432 19.2
1999 102,186 80.4 24,961 19.6
2000 107,553 84.5 19,524 15.4
2001 107,939 84.0 20,571 16.0
2002 107,015 83.2 21,569 16.8
2003 109,392 83.7 21,350 16.3
2004 105,730 83.6 20,778 16.4
2005 109,713 84.1 20,808 15.9
2006 108,186 82.9 22,335 17.1
M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192 187
to-year transition matrixes by sector and sub-sector ofemployment, nurse type and age group.
3.4. Sample
In order to practice in the Province of Ontario, a nursemust be registered with the regulatory body, the College ofNurses of Ontario (CNO). Completion of an annual surveyand payment of dues is necessary to maintain registration.Databases are kept on all nurses registered in Ontario byCNO. The data includes basic demographic information(age, sex), type of nurse (RN, RPN), level of education(Diploma, B.Sc.), employment category, employmentstatus (FT, PT, casual) and employment sector/sub-sector(College of Nurses of Ontario, 2010).
3.5. Data collection
The Nursing Health Services Research Unit (NHSRU)site at the University of Toronto provided the researchteam with an anonymized sub-set of the key variables forall nurses registered with CNO for each of the years of theanalysis. This sub-set contained information about thespecified set of variables (e.g., age, sex, education,employment category, and sector/sub-sector of employ-ment), as well as an encoded registration number toallow data linkage. Provided data was thoroughlychecked for consistency to ensure consistent definitions;for example, because the coding form was modified fromyear to year, we were careful to ensure that sub-sectorswould still be comparable. The coding was validated bydiscussions with the data custodians at the NHSRU and atthe CNO.
3.6. Employment categories
The employment information and place of employmentsections indicated on the CNO annual registration renewalforms were used to classify nurses into two aggregateemployment categories: active and inactive. Note thatnurses in the longitudinal database who are retired or nolonger registered have been dropped from the analysis inthis paper, because they would not be available for nursingjobs in the province. (We accordingly excluded any nurseswho had migrated elsewhere and dropped their registra-tion, but not those who maintained their Ontarioregistration.)
Each nurse was assigned a value for employmentcategory for each year. Active nurses are those registeredwho indicated on their registration form that they work innursing in Ontario in that year. Inactive nurses weredefined as those registered in Ontario, but not working asnurses in the province in that year. Depending on theirwork status and whether they were seeking a job as nursesin Ontario, inactive nurses were divided into five mutuallyexclusive sub-categories: (1) ‘Not Working–Seek’: notworking and seeking nursing employment; (2) ‘Not
Working–Not Seek’: not working and not seeking nursingemployment; (3) ‘Working Non-Nursing–Seek’: working innon-nursing and seeking nursing employment; (4) ‘Work-
ing Non-Nursing–Not Seek’: working in non-nursing and not
seeking nursing employment and (5) ‘Workout’: workingoutside Ontario.
To simplify analysis, nurses were also pooled into one ofthree major employment categories: active nurses, seekingemployment (‘Not Working–Seek’ and ‘Working Non-Nursing–Seek’) and inactive nurses (‘Not Working–NotSeek’, ‘Working Non-Nursing–Not Seek’ and ‘Workout’).
3.7. Data analysis
Each nurse was assigned a unique number. This uniqueidentifier was used to merge the yearly registration recordsof 215,687 nurses registered with CNO. In order to observethe career transition of nurses, we computed ‘‘Stickiness’’—defined as the transition probability of a nurse working in aparticular sector/sub-sector of employment in year ‘‘t’’ wasstill working in that sector/sub-sector in year ‘‘t + l’’.Stickiness was used in this study to measure nurses’transfer across the active/inactive employment statuses orbetween the various inactive sub-categories (Alameddineet al., 2006). Year-to-year transition matrixes weregenerated to investigate what the nurses that wereinactive in year ‘‘t’’ were doing in year ‘‘t + 1’’. SAS-PC(SAS Institute Inc., Cary, NC, USA) was utilized to generate aseries of cross-tabulations for each sub-sector of nursingemployment over the ‘1993–2006’ period. Acknowledgingyear-to-year fluctuation, aggregate proportions werecalculated for ease of analysis and clarity of display.
4. Results
4.1. Distribution of inactive nurses
As Table 1 shows, the total number of active nursesshrank somewhat during the years of fiscal restraint in the1990s, as did the number of nurses registered with theCNO. However, in each year, over 80% of nurses registeredwere working as nurses in Ontario (actives). That still left arelatively large group of inactive nurses, who couldpotentially return to the labour force, the size of whichfluctuated somewhat with changes in the labour market(e.g., in 2000, the higher number of nurses in the activeworkforce, resulting in part from deliberate efforts by
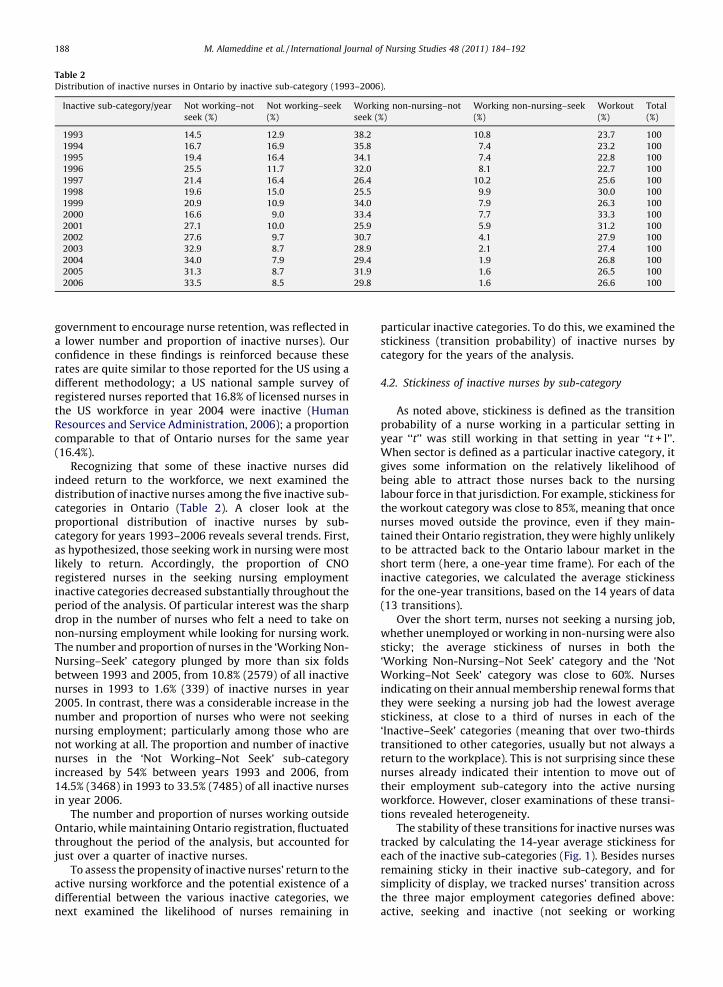
Table 2
Distribution of inactive nurses in Ontario by inactive sub-category (1993–2006).
Inactive sub-category/year Not working–not
seek (%)
Not working–seek
(%)
Working non-nursing–not
seek (%)
Working non-nursing–seek
(%)
Workout
(%)
Total
(%)
1993 14.5 12.9 38.2 10.8 23.7 100
1994 16.7 16.9 35.8 7.4 23.2 100
1995 19.4 16.4 34.1 7.4 22.8 100
1996 25.5 11.7 32.0 8.1 22.7 100
1997 21.4 16.4 26.4 10.2 25.6 100
1998 19.6 15.0 25.5 9.9 30.0 100
1999 20.9 10.9 34.0 7.9 26.3 100
2000 16.6 9.0 33.4 7.7 33.3 100
2001 27.1 10.0 25.9 5.9 31.2 100
2002 27.6 9.7 30.7 4.1 27.9 100
2003 32.9 8.7 28.9 2.1 27.4 100
2004 34.0 7.9 29.4 1.9 26.8 100
2005 31.3 8.7 31.9 1.6 26.5 100
2006 33.5 8.5 29.8 1.6 26.6 100
M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192188
government to encourage nurse retention, was reflected ina lower number and proportion of inactive nurses). Ourconfidence in these findings is reinforced because theserates are quite similar to those reported for the US using adifferent methodology; a US national sample survey ofregistered nurses reported that 16.8% of licensed nurses inthe US workforce in year 2004 were inactive (HumanResources and Service Administration, 2006); a proportioncomparable to that of Ontario nurses for the same year(16.4%).
Recognizing that some of these inactive nurses didindeed return to the workforce, we next examined thedistribution of inactive nurses among the five inactive sub-categories in Ontario (Table 2). A closer look at theproportional distribution of inactive nurses by sub-category for years 1993–2006 reveals several trends. First,as hypothesized, those seeking work in nursing were mostlikely to return. Accordingly, the proportion of CNOregistered nurses in the seeking nursing employmentinactive categories decreased substantially throughout theperiod of the analysis. Of particular interest was the sharpdrop in the number of nurses who felt a need to take onnon-nursing employment while looking for nursing work.The number and proportion of nurses in the ‘Working Non-Nursing–Seek’ category plunged by more than six foldsbetween 1993 and 2005, from 10.8% (2579) of all inactivenurses in 1993 to 1.6% (339) of inactive nurses in year2005. In contrast, there was a considerable increase in thenumber and proportion of nurses who were not seekingnursing employment; particularly among those who arenot working at all. The proportion and number of inactivenurses in the ‘Not Working–Not Seek’ sub-categoryincreased by 54% between years 1993 and 2006, from14.5% (3468) in 1993 to 33.5% (7485) of all inactive nursesin year 2006.
The number and proportion of nurses working outsideOntario, while maintaining Ontario registration, fluctuatedthroughout the period of the analysis, but accounted forjust over a quarter of inactive nurses.
To assess the propensity of inactive nurses’ return to theactive nursing workforce and the potential existence of adifferential between the various inactive categories, wenext examined the likelihood of nurses remaining in
particular inactive categories. To do this, we examined thestickiness (transition probability) of inactive nurses bycategory for the years of the analysis.
4.2. Stickiness of inactive nurses by sub-category
As noted above, stickiness is defined as the transitionprobability of a nurse working in a particular setting inyear ‘‘t’’ was still working in that setting in year ‘‘t + l’’.When sector is defined as a particular inactive category, itgives some information on the relatively likelihood ofbeing able to attract those nurses back to the nursinglabour force in that jurisdiction. For example, stickiness forthe workout category was close to 85%, meaning that oncenurses moved outside the province, even if they main-tained their Ontario registration, they were highly unlikelyto be attracted back to the Ontario labour market in theshort term (here, a one-year time frame). For each of theinactive categories, we calculated the average stickinessfor the one-year transitions, based on the 14 years of data(13 transitions).
Over the short term, nurses not seeking a nursing job,whether unemployed or working in non-nursing were alsosticky; the average stickiness of nurses in both the‘Working Non-Nursing–Not Seek’ category and the ‘NotWorking–Not Seek’ category was close to 60%. Nursesindicating on their annual membership renewal forms thatthey were seeking a nursing job had the lowest averagestickiness, at close to a third of nurses in each of the‘Inactive–Seek’ categories (meaning that over two-thirdstransitioned to other categories, usually but not always areturn to the workplace). This is not surprising since thesenurses already indicated their intention to move out oftheir employment sub-category into the active nursingworkforce. However, closer examinations of these transi-tions revealed heterogeneity.
The stability of these transitions for inactive nurses wastracked by calculating the 14-year average stickiness foreach of the inactive sub-categories (Fig. 1). Besides nursesremaining sticky in their inactive sub-category, and forsimplicity of display, we tracked nurses’ transition acrossthe three major employment categories defined above:active, seeking and inactive (not seeking or working
[(Fig._1)TD$FIG]
Fig. 1. Percent distribution of inactive nurses across major employment
categories (aggregated 1993–2006).
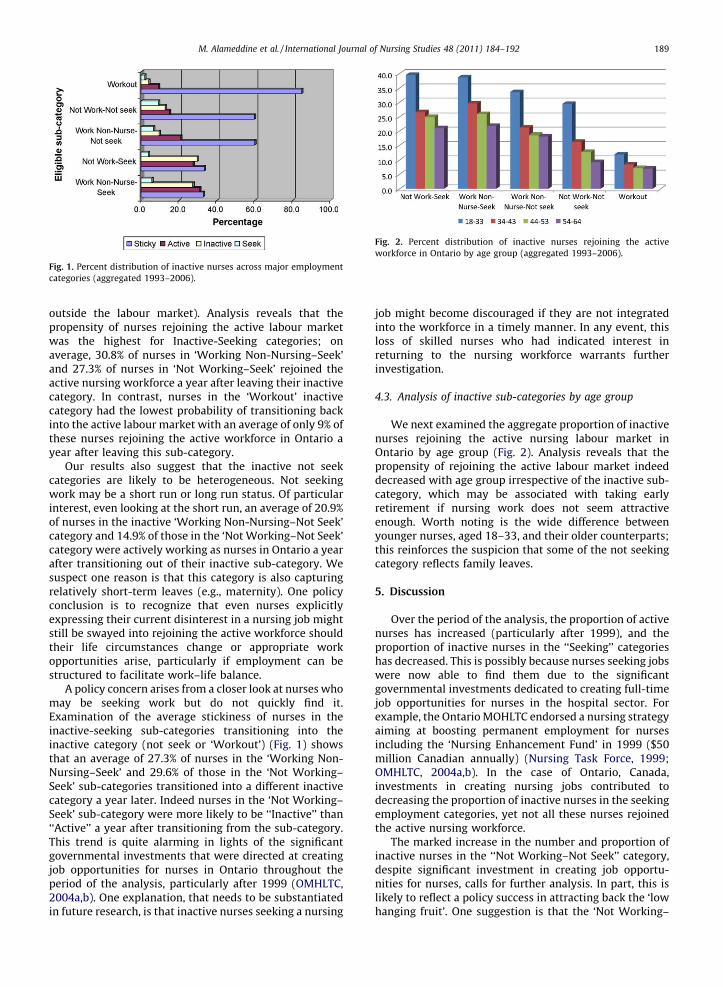
[(Fig._2)TD$FIG]
Fig. 2. Percent distribution of inactive nurses rejoining the active
workforce in Ontario by age group (aggregated 1993–2006).
M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192 189
outside the labour market). Analysis reveals that thepropensity of nurses rejoining the active labour marketwas the highest for Inactive-Seeking categories; onaverage, 30.8% of nurses in ‘Working Non-Nursing–Seek’and 27.3% of nurses in ‘Not Working–Seek’ rejoined theactive nursing workforce a year after leaving their inactivecategory. In contrast, nurses in the ‘Workout’ inactivecategory had the lowest probability of transitioning backinto the active labour market with an average of only 9% ofthese nurses rejoining the active workforce in Ontario ayear after leaving this sub-category.
Our results also suggest that the inactive not seekcategories are likely to be heterogeneous. Not seekingwork may be a short run or long run status. Of particularinterest, even looking at the short run, an average of 20.9%of nurses in the inactive ‘Working Non-Nursing–Not Seek’category and 14.9% of those in the ‘Not Working–Not Seek’category were actively working as nurses in Ontario a yearafter transitioning out of their inactive sub-category. Wesuspect one reason is that this category is also capturingrelatively short-term leaves (e.g., maternity). One policyconclusion is to recognize that even nurses explicitlyexpressing their current disinterest in a nursing job mightstill be swayed into rejoining the active workforce shouldtheir life circumstances change or appropriate workopportunities arise, particularly if employment can bestructured to facilitate work–life balance.
A policy concern arises from a closer look at nurses whomay be seeking work but do not quickly find it.Examination of the average stickiness of nurses in theinactive-seeking sub-categories transitioning into theinactive category (not seek or ‘Workout’) (Fig. 1) showsthat an average of 27.3% of nurses in the ‘Working Non-Nursing–Seek’ and 29.6% of those in the ‘Not Working–Seek’ sub-categories transitioned into a different inactivecategory a year later. Indeed nurses in the ‘Not Working–Seek’ sub-category were more likely to be ‘‘Inactive’’ than‘‘Active’’ a year after transitioning from the sub-category.This trend is quite alarming in lights of the significantgovernmental investments that were directed at creatingjob opportunities for nurses in Ontario throughout theperiod of the analysis, particularly after 1999 (OMHLTC,2004a,b). One explanation, that needs to be substantiatedin future research, is that inactive nurses seeking a nursing
job might become discouraged if they are not integratedinto the workforce in a timely manner. In any event, thisloss of skilled nurses who had indicated interest inreturning to the nursing workforce warrants furtherinvestigation.
4.3. Analysis of inactive sub-categories by age group
We next examined the aggregate proportion of inactivenurses rejoining the active nursing labour market inOntario by age group (Fig. 2). Analysis reveals that thepropensity of rejoining the active labour market indeeddecreased with age group irrespective of the inactive sub-category, which may be associated with taking earlyretirement if nursing work does not seem attractiveenough. Worth noting is the wide difference betweenyounger nurses, aged 18–33, and their older counterparts;this reinforces the suspicion that some of the not seekingcategory reflects family leaves.
5. Discussion
Over the period of the analysis, the proportion of activenurses has increased (particularly after 1999), and theproportion of inactive nurses in the ‘‘Seeking’’ categorieshas decreased. This is possibly because nurses seeking jobswere now able to find them due to the significantgovernmental investments dedicated to creating full-timejob opportunities for nurses in the hospital sector. Forexample, the Ontario MOHLTC endorsed a nursing strategyaiming at boosting permanent employment for nursesincluding the ‘Nursing Enhancement Fund’ in 1999 ($50million Canadian annually) (Nursing Task Force, 1999;OMHLTC, 2004a,b). In the case of Ontario, Canada,investments in creating nursing jobs contributed todecreasing the proportion of inactive nurses in the seekingemployment categories, yet not all these nurses rejoinedthe active nursing workforce.
The marked increase in the number and proportion ofinactive nurses in the ‘‘Not Working–Not Seek’’ category,despite significant investment in creating job opportu-nities for nurses, calls for further analysis. In part, this islikely to reflect a policy success in attracting back the ‘lowhanging fruit’. One suggestion is that the ‘Not Working–

M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192190
Not Seek’ category may not be homogeneous, as thiscategory might includes both nurses taking temporaryleave who may subsequently be likely to return to theworkforce, and those nearing retirement, who will beharder to recruit back. Policy and decision makers areencouraged to assess the attractiveness of created jobs toinactive nurses. Future research initiatives could alsosystematically investigate the enablers and barriers fornurses’ return to the active labour market, and how this fitswith care needs.
Policy makers are also cautioned against assuming thatinvestments in creating nursing jobs is adequate to attractinactive nurses back into the active labour market. In fact,our results suggest that governmental investments increating job opportunities for nurses is a necessary but nota sufficient condition for nurses’ return to the active labourmarket. Other strategies warrant investigation acrossvarious jurisdictions, including: the impact of policieswhich favour full-time employment, particularly sincemany inactive nurses may prefer part-time and flexibleemployment arrangements (Langan et al., 2007; Williamset al., 2006); the effectiveness of providing a convenientlow or no-cost refresher course to ease nurses’ return to theactive nursing workforce (Myers and Bushnell, 2007;Roberts et al., 2005); the effect that improving the qualityof the work environment has on the recruitment of inactivenurses (Cohen et al., 2009; Lavoie-tremblay et al., 2008)and the impact of proving more competitive salary andbenefit packages to enhance the return of inactive nursesinto the labour market (Barron and West, 2005; Langanet al., 2007).
Our analysis further reveals that a significant propor-tion of inactive nurses that are registered and seekingnursing employment are not being effectively integratedinto the labour market in a timely manner. Many of thesenurses are indeed transitioning from seeking employmentcategories into not seeking or working outside categories.A suggestion, that warrant investigation in future researchinitiatives, is that some of these nurses become discour-aged and are lost to the labour market. Some may accept ajob outside the local labour market; many more appear toleave nursing. The attrition of inactive nurses from thenursing profession (e.g., early retirement or working innon-nursing) or from the country (migration) is even moredisconcerting in poorly resourced developing countries,due to an assortment of ‘push’ and ‘pull’ factors that resultin the brain drain of valuable nursing resources from locallabour markets (Dovlo, 2005; Kirigia et al., 2006).
The number of inactive nurses ‘Not Seeking’ employ-ment returning to the active workforce is in the thousandsand could potentially contribute to relieving the reportedshortage of nurses. Our analysis revealed that the ‘‘NotSeeking’’ status might be a temporary one for many nurses.Even if nurses indicate that they are not interested in anursing job at one point in time, many (particularly inyounger age groups) could still be attracted back into theactive labour market should their life circumstanceschange (e.g., end of maternity leave) or attractive workopportunities arise. That conclusion was reinforced by ouranalysis by age group, which concluded that the propensi-ty of attracting inactive nurses back into the active labour
force decreased with age, irrespective of the nursing groupor inactive category. These finding suggest that policymakers should pay careful attention to creating jobopportunities for new nursing graduates to prolong theirprofessional lifespan and prevent their attrition from thelocal labour market.
6. Study limitations
A number of limitations in this study warrantmentioning. First, the registration database utilized inthis analysis includes only nurses that have maintainedtheir registration with CNO; therefore, the analysisunderestimates the attrition of nurses from Ontario’slabour market by omitting those that have dropped theirregistration. Second, it cannot be ascertained whethernurses maintaining CNO registration are different fromthose that let it lapse. We argue that maintenance ofregistration is suggestive of a future intention to resumenursing practice, and that the study is accordingly biasedtowards those most amenable to returning to the labourmarket. Third, although the annual membership registra-tion form defines the various employment sub-sectors andcategories that nurses could pursue, there is no cleardefinition about what is meant by a nursing job. Therefore,it cannot be assured that nurses indicating non-nursingemployment are not using nursing skills and knowledge intheir jobs, although it probably can be assumed that theyare not doing direct patient care. Fourth, because annualregistration forms do not collect information on importantvariables that affect employment decision (e.g., martialstatus, number of children, caring for an elderly), thosevariables cannot be incorporated in the analysis. This isparticularly important when considering short-termleaves (e.g., maternity leaves). Finally, this study analyzesshort-term career transitions, and as such cannot ascertainhow long nurses moving from one employment status(e.g., not working) to the other (actively working) remainthere.
7. Conclusion
At times of shortage, governments need to optimize theuse of all available nursing resources. Inactive nurses are astrategically important pool potentially providing arelatively quick recovery to shortages in a particularlabour market. Longitudinal analysis of short-term careertransitions from Ontario, Canada, reveals that while nursesin certain inactive categories largely remained out of theactive nursing workforce in Ontario (nurses workingoutside), others were more likely to return to practicingnursing in the province. As expected, those nurses whoindicated that they were seeking nursing employmentwere the most likely to return, but also to becomediscouraged if they did not find nursing work in thatjurisdiction and subsequently be lost to the nursing labourforce. We also found that the ‘‘Not Seek’’ inactive categoriesare heterogeneous, with many (particularly those inyounger age groups) eventually returning to the activeworkforce. Optimal reintegration of inactive nursesrequires that payers, professional associations and

M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192 191
employers work collaboratively to formulate carefullycrafted recruitment strategies (e.g., offering part-time andflexible job opportunities, refresher courses, etc.). Some ofthe reported labour trends may be jurisdiction-specific, yetothers almost certainly would apply to other jurisdictions.These findings suggest that policy and decision makersshould examine their pool of inactive nurses, and devisetargeted recruitment strategies to bring back nursescurrently outside the nursing labour market to avoidpermanent loss of such a skilled nursing pool.
Ethical approval
Continuous ethical approval was maintained for theduration of the study from the Institutional Research Boardat the University of Toronto, protocol number 11131.
Funding
This study was funded by a CIHR grant, ‘‘Where donurses work? Work setting and work choice’’ (CIHRreference number MOP-64240). Analysis performed atthe Nursing Health Services Research Unit (NHSRU) -Faculty of Nursing, University of Toronto. Additionalsupport provided by the CIHR Team in Community Careand Health Human Resources (Team Grant referencenumber CTP79849), University of Toronto.
Conflicts of interest
None declared.
References
Aiken, L.H., Clarke, S.P., Cheung, R.B., Sloane, D.M., Silber, J.H., 2003.Educational levels of hospital nurses and surgical patient mortality.JAMA: The Journal of the American Medical Association 290 (12),1617–1623.
Aiken, L.H., Clarke, S.P., Sloane, D.M., 2001. Hospital restructuring: does itadversely affect care and outcomes? Journal of Health and HumanServices Administration 23 (4), 416–442.
Alameddine, M., Baumann, A., Laporte, A., O’Brien-Pallas, L., Levinton, C.,Onate, K., Deber, R., 2009. Career trajectories of nurses leaving thehospital sector in Ontario, Canada (1993–2004). Journal of AdvancedNursing 65 (5), 1044–1053.
Alameddine, M., Laporte, A., Baumann, A., O’Brien-Pallas, L., Mildon, B.,Deber, R., 2006. ‘Stickiness’ and ‘inflow’ as proxy measures of therelative attractiveness of various sub-sectors of nursing employment.Social Science & Medicine (1982) 63 (9), 2310–2319.
Allan, J.D., Aldebron, J., 2008. A systematic assessment of strategies toaddress the nursing faculty shortage. U.S. Nursing Outlook 56 (6),286–297.
Barron, D., West, E., 2005. Leaving nursing: An event-history analysis ofnurses’ careers. Journal of Health Services Research & Policy 10 (3),150–157.
Baranek, P., Deber, R., Williams, P., 2004. Almost Home: Reforming Homeand Community Care in Ontario. University of Toronto Press, Toronto,Ontario, Canada.
Baumann, A., Giovanetti, P., O’Brian-Pallas, L., Deber, R., Blythe, J., Hibberd,J., DiCenso, A., Mallette, C., Brady-Fryer, B., 1998. Restructuring ofhuman health resources: a critical issue. Project 6606-6284-012.
Benjamin, D., Gunderson, M., Riddel, W., 2002. Labour Market Economics.McGraw-Hill Ryerson, Toronto.
Berlin, L.E., Sechrist, K.R., 2002. The shortage of doctorally preparednursing faculty: a dire situation. Nursing Outlook 50 (2), 50–56.
Black, L., Spetz, J., Harrington, C., 2008. Nurses working outside of nursing:societal trend or workplace crisis? Policy, Politics & Nursing Practice9 (3), 143–157.
Blythe, J., Baumann, A., 2009. Internationally educated nurses: profilingworkforce diversity. International Nursing Review 56 (2), 191–197.
Blythe, J., Baumann, A., Rheaume, A., McIntosh, K., 2009. Nurse migrationto Canada: pathways and pitfalls of workforce integration. Journal ofTranscultural Nursing: Official Journal of the Transcultural NursingSociety/Transcultural Nursing Society 20 (2), 202–210.
Buchan, J., 2002. Nursing shortages and evidence-based interventions: acase study from Scotland. International Nursing Review 49 (4), 209–218.
Cohen, J., Stuenkel, D., Nguyen, Q., 2009. Providing a healthy workenvironment for nurses: the influence on retention. Journal of Nurs-ing Care Quality 24 (4), 308–315.
College of Nurses of Ontario. Annual membership renewal—onlineinstruction Guide 2010. Retrieved January 20, 2010 from http://www.cno.org/reg/memb/reg_renew_web.htm.
Crow, S.M., Hartman, S.J., Mahesh, S., McLendon, C.L., Henson, S.W.,Jacques, P., 2008. Strategic analyses in nursing schools: attracting,educating, and graduating more nursing students. Part I. Strengths,weaknesses, opportunities, and threats analysis. The Health CareManager 27 (3), 234–244.
Dovlo, D., 2005. Wastage in the health workforce: some perspectives fromAfrican countries. Human Resources For Health 3, 6.
Duffield, C., Kearin, M., Johnston, J., Leonard, J., 2007. The impact ofhospital structure and restructuring on the nursing workforce. TheAustralian Journal of Advanced Nursing: A Quarterly Publication ofthe Royal Australian Nursing Federation 24 (4), 42–46.
Dussault, G., Fronteira, I., Prytherch, H., Dal Poz, M., Ngoma, D., Lunguzi, J.,Wyss, K., 2007. Scaling up the stock of health workers: a review.
Eastaugh, S.R., 2004. The impact of nurse training funds on the supply ofnurses. Journal of Health Care Finance 30 (4), 1–13.
Hooper, C.R., 2008. Adding insult to injury: the healthcare brain drain.Journal of Medical Ethics 34 (9), 684–687.
Human Resources Service Administration, 2010. The registered nursepopulation: initial findings from the 2008 national sample surveyof registered nurses. U.S. Department of Health and Human Services,Health Resource and Services Administration.
Human Resources and Service Administration, 2006. The RegisteredNurse Population: Findings from the national sample survey ofregistered nurses. U.S. Department of Health and Human Services,Health Resource and Services Administration.
International Centre for Human Resources in Nursing, 2007. An AgeingNursing Workforce. .
Kawi, J., Xu, Y., 2009. Facilitators and barriers to adjustment of interna-tional nurses: an integrative review. International Nursing Review 56(2), 174–183.
Kirigia, J.M., Gbary, A.R., Muthuri, L.K., Nyoni, J., Seddoh, A., 2006. The costof health professionals’ brain drain in Kenya. BMC Health ServicesResearch 6, 89.
Labonte, R.e.a., 2006. The brain drain of health professionals from SubSaharan Africa to Canada. African Migration and Development SeriesNo.2.
Langan, J.C., Tadych, R.A., Kao, C.C., 2007. Exploring incentives for RNs toreturn to practice: a partial solution to the nursing shortage. Journalof Professional Nursing: Official Journal of the American Associationof Colleges of Nursing 23 (1), 13–20.
Lavoie-tremblay, M., Wright, D., Desforges, N., Gelinas, C., Marchionni, C.,Drevniok, U., 2008. Creating a healthy workplace for new-generationnurses. Journal of Nursing Scholarship: An Official Publication ofSigma Theta Tau International Honor Society of Nursing/Sigma ThetaTau 40 (3), 290–297.
McCloskey, B.A., Diers, D.K., 2005. Effects of New Zealand’s health reen-gineering on nursing and patient outcomes. Medical Care 43 (11),1140–1146.
Myers, G., Bushnell, K., 2007. Inactive nurses: making a comeback.Nursing Management 38 (8) 16, 19.
Nursing Task Force, 1999. In: Anonymous (Eds.), Good Nursing, GoodHealth: An investment in the 21st Century. Ontario Ministry of Healthand Long-Term Care, Toronto, Ontario.
O’Brien-Pallas, L., Duffield, C., Alksnis, C., 2004. Who will be there tonurse? Retention of nurses nearing retirement. The Journal of Nurs-ing Administration 34 (6), 298–302.
Ontario Ministry of Health and Long-Term Care. ‘‘McGuinty governmentinvests in nurses’ health and safety.’’ (2004, February 24, News Release)2004. Retrieved January 08, 2010]. Available at: http://ogov.newswire.ca/ontario/GPOE/2004/02/10/c8369.html? lmatch=&lang=_e.html.
Ontario Ministry of Health and Long-Term Care. ‘‘McGuinty governmentimproving health services by investing in better quality nursing care’’(2004, December 8, News Release) 2004. Retrieved January 8, 2010.Available at: http://ogov.newswire.ca/ontario/GPOE/2004/12/08/c2943.html?lmatch=&lang=_e.html.

M. Alameddine et al. / International Journal of Nursing Studies 48 (2011) 184–192192
Pollock, A.M., Dunnigan, M.G., Gaffney, D., Price, D., Shaoul, J., 1999. Theprivate finance initiative: planning the ‘‘new’’ NHS: downsizing forthe 21st century. BMJ (Clinical research ed.) 319 (7203), 179–184.
Roberts, V.W., Brannan, J.D., White, A., 2005. Outcomes-based research:evaluating the effectiveness of an online nurse refresher course.Journal of Continuing Education in Nursing 36 (5), 200–204 quiz234–235.
Steinbrook, R., 2002. Nursing in the crossfire. The New England Journal ofMedicine 346 (22), 1757–1766.
Unruh, L., 2003. Licensed nurse staffing and adverse events in hospitals.Medical Care 41 (1), 142–152.
Williams, K.A., Stotts, R.C., Jacob, S.R., Stegbauer, C.C., Roussel, L., Carter,D., 2006. Inactive nurses: a source for alleviating the nursingshortage? The Journal of Nursing Administration 36 (4), 205–210.


















