
Cardiovascular Disease in Chronic Renal Failure · Ticking Bomb of CVD in CKD Artery Lp(a) =...
62
Cardiovascular Disease in Chronic Renal Failure Antalya, October 18-22, 2017 Bengt C Fellström, MD, PhD Professor of Nephrology University Hospital Uppsala Sweden
Transcript of Cardiovascular Disease in Chronic Renal Failure · Ticking Bomb of CVD in CKD Artery Lp(a) =...

Cardiovascular Disease in
Chronic Renal Failure
Antalya, October 18-22, 2017
Bengt C Fellström, MD, PhD
Professor of Nephrology
University Hospital
Uppsala
Sweden

USRDS
1000-fold
80 years
Mortality is massively increased in dialysis patients
as compared to the general population

Cardiovascular mortality: transplant patients
Age
(years)
An
nu
al
Mort
ali
ty (
%)
Foley et al AJKD 1998;32 (suppl 3) S112
0.01
0.1
1
1
0
25-34 35-44 45-54 55-64 65-74 75-84
Transplant
Control

Cardiovascular mortality by age group
Jardine A, Gaston R, Fellström B, Holdaas H. Lancet 378:1419-27; 2011

The cardiovascular burden that patients carry with them to transplantation .
Transplantation significantly reduces CV risk in these patients, it does not reduce to background population risk.
–CV risk > gen pop = cardiovascular risk increase as compared with background age adjusted risk. Stage = stage of renal career – CKD = chronic kidney disease;
–HD = haemodialysis; RTR = renal transplant recipient. Factors = stage specific risks – LVH = left ventricular hypertrophy; drugs = immunosuppressive agents.

…, and the development of
cardiovascular disease starts early :
Go A et al. N Engl J Med 2004;351:1296 - 1305
CVD1,120,295 adult
subjects in Kaiser
Permanente health
insurance plan in
Northern California
Median follow-up:
2.8 yrs
*
* MDRD equation

All-cause mortality
p < 0.0001
Cardiac death
p < 0.0001
Non-cardiovascular death
p = 0.0005
MACE
p = 0.0007
Non-fatal MI (NS)
Stroke (NS)
Creatinine (µmol/l)
Endpoint probabilities at baseline
creatinine levels
Pro
babili
ty
0
0.2
0.4
0.6
0.8
50 150 250 350 450 550
Fellström, Holdaas, JArdine, et al. Am J Transplant 2005; 5:1986-9

CVD in CRF
• Endothelial dysfunction
• Acelerated atherosclerosis
• Coronary heart disease
• Left Ventricular Hypertrophy
• Congestive Heart Failure
• Stroke
• Peripheral vascular disease
• Thrombo-embolic disease

Ticking Bomb of CVD in CKD
Artery
Lp(a) = lipoprotein (a); HDL-C = high-density lipoprotein cholesterol
AGEs = advanced glycosylation end products ; Ca x P = calcium-phosphorus product
Small dense LDL-C
Lp (a)
Low HDL-C
Oxidised LDL-C
Inflammation
Oxidant Stress
ROS, AGEs, AOPP
Malnutrition
Ca – P - PTH
Vascular calcification
Diabetes
Insulin resistance
Proteinuria
Renal dysfunction
HypertensionEndothelial
dysfunction


REACTIVE OXYGEN SPECIES
(ROS)
ATHEROSCLEROSIS
Endothelial
Cell
Smooth Muscle
Cell
ROS
ROS
ROSNO
L-
Arginine
BH4
ADMA
NOS
ROS
ROS
LDL-
Chol
Cell
Adhesion
Molecule
Receptor
Guanylyl
Cyclase PDGF-
AA
mRNA
ROS
GTP
cGMP
ROS SMC Proliferation
ECM Synthesis
PDGF-R
Monocyte
Scavang
er
Receptor
oxLDL
IL-1
PDGF
HLA-DR
Foam
Cell

0
,1
,2
,3
,4
,5
,6
,7
,8
,9
1
GS
SG
/GS
H
-10 0 10 20 30 40 50 60
CRP
Correlation between CRP and GSSG/GSH
0
100
200
300
400
500
600
700
800
S-c
rea
-10 0 10 20 30 40 50 60
CRP
Correlation between CRP and serum creatinine
CRP (mg/L)
GSS
G/G
SH
CRP (mg/L)
Ser
um c
reat
inin
e (m
mol
/L)
p= 0.0022
r= 0.50
p = 0.0008
r = 0.53

Relation of MACE with baseline hs CRP and Serum Albumin
Even
t rate
(%
)
16
14
12
10
8
6
hsCRP
Decile
0 2 4 6 8
p<0.0001
Even
t rate
(%
)
16
14
12
10
8
6
Albumin
Decile
0 2 4 6 8
p<0.0001

IL-6 Predicts Poor Outcome in ESRD
AJKD 2005
NDT 2004
NDT 2002
JASN 2006
Bologa et al. AJKD 1998

Oxidative stressInflammation
Retention of
uremic solutes
Decreased renal
function
Decreased clearance of
cytokines and AGEs
Sluggish innate
immune system
Priming of PMNL
Inability to respond
properly to danger
signals
Volume overload and
sympathetic overactivity
Infectious complications
Atherosclerosis
Endothelial
dysfunction
Yilmaz and Stenvinkel. In Press Clin Nephrol 2007

Peter Stenvinkel, MD, PhD
Inflammation in End Stage Renal Disease
- the Fire that Burns Within

Inflammation in CRF & CV effects
One of the strongest markers for CVD in CKD
Strong rel. to CV events in CRF & RTx
Driven by OS, imm-reactivity,
Inv. rel. to telomere shortening senescence
and apoptosis
Influence on other biomarkers ( LDL)
Influences statin effects in CKD

Risk factors for post-transplant
cardiovascular disease
Jardine A, Gaston R, Fellström B, Holdaas H. The Lancet 378:1419-27; 2011

CRP in renal transplant patients
Abedini, S. et al.
CJASN
2009;4:1246-1254

Hyperlipidaemia-
Dyslipidemia

Disturbances in Lipid Metabolism in ESRD
• serum levels of triglycerides, IDL,
VLDL, apo B and Lp(a)
• HDL
• Aggr. Small dense LDL particles
• reverse cholesterol transport
• lipoprotein oxidation,
carbamylation and transformation
by advanced glycation end-
products (AGEs)

Relative risk for all-cause mortality associated with plasma total cholesterol stratified by the presence or absence of inflammation and/or malnutrition in the Choices for Healthy
Outcomes in Caring for ESRD (CHOICE) study
Kwan, et al. Journal of the American Society of Nephrology. 18(4):1246-61, 2007.

Future Treatment of Dialysis patients?
How should the fire
be extinguished ?

Simplified flow schedule of uremia and its complications

Anti-inflammatory and other optionsPresent and future possibilities
Immunemodulation / Anti-Inflammation
Statin treatment
Immunosuppression
T-cells modulation
Vaccination
Cytokine inhibiiton
RAS inhibition
Anti-oxidation
NO-enhancement

Statins
ACEI
PPAR-g activators
Tocopherols
Heparin
Acetylcysteine
Sevelamer
Vitamin D
Aspirin and NSAID
• Thalidomide (TNF-blocker)
• Pentoxifylline (TNF-blocker)
• Etanercept (TNF-receptor blocker)
• Infliximab (TNF-antibodies)
• Anakinra (IL-1 receptor antagonist)
• Tocilizumab (Actemra )
( IL-6R Mo Ab )
• C5 / C3 blockade in the
future ?
Potential Pharmacological Strategies Using
Inflammation and Oxidative Stress as a Target

Anti-inflammatory and other optionsPresent and future possibilities
Immunemodulation / Anti-Inflammation
Statin treatment
Immunosuppression
T-cells modulation
Vaccination
Cytokine inhibiiton
RAS inhibition
Anti-oxidation
NO-enhancement

Statin Therapy Could Benefit Patients with
Kidney Disease at CVD Risk
Stabilisation of
atherosclerotic
plaques
Inhibition of
platelet function
Upregulation of
eNOS function
Reduction in
thrombosis
Decrease in the
hypertensive effects
of angiotensin II
Reduction in C-reactive
protein and inflammation
Reduction in LDL-C
Improvements in
endothelial function
Decrease in circulating
triglycerides
Increase in
circulating
HDL-C
Main action: lower endogenous
cholesterol production by inhibiting
3-hydroxy-3-methylglutaryl
coenzyme A (HMG Co-A) reductase
Statins also have pleiotropic effects
Statins
Ker. SA Fam Practice 2002: http://www.e-doc.co.za

Reductions in inflammatory marker CRP
8 weeks
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
Mean %
change from
baseline in
CRP (%)
Rosuvastatin
Atorvastatin
Rosuvastatin
Atorvastatin
10 mg
16 weeks
20 mg
Comparison of rosuvastatin and atorvastatin in patients with type 2 diabetes
LDL-C = - 51%
LDL-C = - 39%
LDL-C = - 57%
LDL-C = - 46%

Atorvastatin reduces inflammation
within atherosclerotic plaques
0
0,5
1
1,5
2
2,5
3
3,5
4
Control AngII AngII +
Atv
Control TNF TNF + Atv
Ortego et al Atheroscl 1999:
147:253

Holdaas, Fellström, Jardine et al
Lancet 2003; 361:2024–2031

The ALERT trial
• A randomised, placebo controlled trial in 2102
renal transplant recipients
• 5 – 6 years follow-up, fluvastatin 40 – 80
mg/day versus placebo (Holdaas, Fellstrøm, Jardine et al. Lancet
2003:361:2024)
• The Alert core trial was extended by 2 years
during which time all patients were offered
fluvastatin 80 mg/day (Holdaas, Fellstrøm, Cole et al. Am J
Transplant 2005:5.2929)

7
Placebo
Fluvastatin
38%
6
5
4
3
2
1
P=0.031
Proportion
of patients
(%)
Years since randomisation
0 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.00.5
Years since randomisation
1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.00.50
8
0
Years since randomisation
01.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.00.50
Years since randomisation
15
01.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0
Placebo
Fluvastatin
0.50
35%
10
5
Primary Endpoint Cardiac Death
Definite MI Cardiac Death or Definite MI
Proportion
of patients
(%)
Proportion
of patients
(%)
Proportion
of patients
(%)
P=0.005
8
7Placebo
Fluvastatin
32%6
5
4
3
2
1
P=0.050
18
10
6
0
Placebo
Fluvastatin
17%P=0.139
12
14
16
8
4
2
1052
1050
1018
1009
972
974
929
930
878
885
819
791
17
14
1030
1031
1002
1008
971
973
935
938
882
844
18
16
1052
1050
1019
1022
983
991
945
957
900
917
842
821
17
15
1052
1050
1019
1022
983
991
945
957
900
917
842
821
17
15
1052
1051
Placebo
Fluvastatin
Placebo
Fluvastatin
Placebo
Fluvastatin
Placebo
Fluvastatin
Number at risk Number at risk
Number at risk Number at risk
A B
C D
Holdaas, Fellstrøm, Jardine et al Lancet 2003;362:2024

The ALERT extension trial
Holdaas, Fellström, Cole, Jardine et al et al. Am J Transplant 2005:5.2929

p=0.37
4D Study in Diabetic HemodialysisPatients: No Benefit of Statin
Therapy
4D=Die Deutsche Diabetes Dialyse Studie
No. at risk:
Placebo 636 532 383 252 136 51 19
Atorvastatin 619 515 378 252 136 58 29
Wanner C et al. N Engl J Med 2005; 353: 238–248
Cumulative incidence of primary endpoint (%)
Time (years)
Atorvastatin
Placebo60
50
40
30
20
10
0
60 1 2 3 4 5
Primary Endpoint :
CV death , non-fatal MI or stroke

AURORA study design
Matching placebo (n~1350)
Screening
6-monthly6 Final†
Patients (n~2750)Inclusion criteriaESRD, on hemodialysis for
≥3 months 50–80 yearsExclusion criteriaStatin within 6 monthsKidney transplant likely
within 1 yearCreatine kinase >3xULNALT >3xULNTSH >1.5xULN
–14 days1
02
64
Month:Visit:
Rosuvastatin 10 mg daily (n~1350)
33
125
Treatment
†Study medication was administered until 620 patients had experienced a major CV event
Randomization 1:1
Fellström BC, Jardine A, Schmieder R, Holdaas H et al. N Engl J Med 2009; 360: 1395–1407

Study Endpoints
• Primary Endpoint
– time to major CV event (CV death, non-fatal myocardial infarction [MI] or non-fatal stroke) adjudicated by blinded clinical endpoint committee
Fellström BC, Jardine A, Schmieder R, Holdaas H et al. N Engl J Med 2009; 360: 1395–1407

Placebo
AURORA: primary endpointKaplan-Meier estimate of time to
first major CV event
No. at risk:
Rosuvastatin 1390 1152 962 826 551 148
Placebo 1384 1163 952 809 534 153
Cumulative incidence of primary endpoint (%)
Years from randomization
Rosuvastatin
HR=0.96 (95% CI 0.84–1.11)P=0.59
0
5
10
15
20
25
30
35
40
0 1 2 3 4 5
Fellström BC, Jardine A, Schmieder R, Holdaas H et al. N Engl J Med 2009; 360: 1395–1407

Smoking status
Primary endpointForest plot of predefined subgroups
0.90
0.84
0.23
0.87
0.71
<65≥65
Age (years)
NoYes
NoYes
Diabetes
NoYes
History of CVD
MaleFemale
Gender
0.5 0.75 1 1.25 1.5 1.75 2
Favors rosuvastatin Favors placebo
HR(95% CI) p value
Subgroup

127–146
Primary endpointForest plot of predefined subgroups (cont.)
†The three subgroups represent patients whose baseline values fall into tertiles 1, 2 or 3
LDL-C (mg/dL)
Hs-CRP (mg/L)
0.18
0.97
0.27
0.32
0.16
>80
>111
Systolic BP (mm Hg)
Diastolic BP (mm Hg)
Body mass index (kg/m2)
<7171–80
<2.9 2.9–8.5>8.5
<8383–111
<127
>146
<2323.0–26.6>26.6
0.5 0.75 1 1.25 1.5 1.75 2
Favors rosuvastatin Favors placebo
HR(95% CI) p value
Subgroup†
*

Baseline LDL-C as a risk factor according to hsCRP at 3 months
hsCRP <2.0 mg/L hsCRP ≥2.0 mg/L
LDL-C=low-density lipoprotein cholesterol; hsCRP=high-sensitivity C-reactive protein; HR=hazard ratio
Fellström BC et al. ISN-Nexus 2010, 15–18 April, Kyoto, Japan; poster S-10-3-9
0.8
0.6
0.4
0.2
0
-0.2
-0.4
-0.6
-0.8
Baseline LDL-C (mmol/L)
2 3 4 51
HR=1.53
p=0.014
0.6
0.4
0.2
0
-0.2
-0.4
-0.6
Baseline LDL-C (mmol/L)
2 3 4 51
HR=0.83
p=0.015
Log
hazard

Major CV event in relation to post
randomization CRP
HR = 0.71p< 0.018
Fellström , Holdaas, Jardine, Schmieder, Zannad et al. ISN-Nexus 2010, Kyoto, Japan
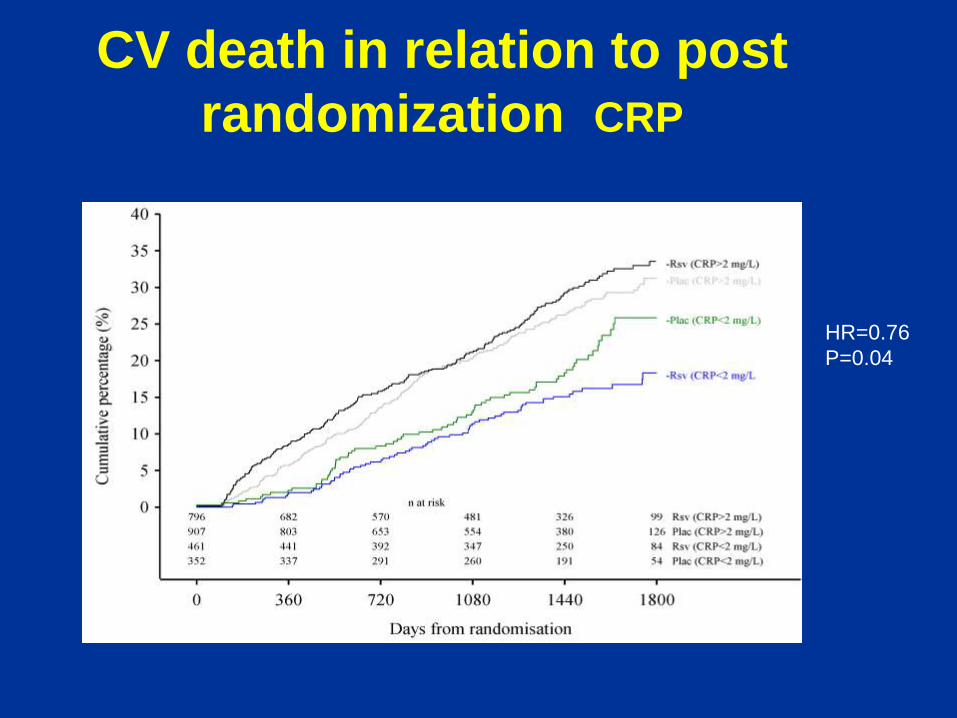
CV death in relation to post
randomization CRP
HR=0.76
P=0.04

Relationship between hsCRP split points and HR for time to first major CV
event
hsCRP=high-sensitivity C-reactive protein; HR=hazard ratio; CV=cardiovascular
Fellström, Holdaas, Jardine, Schmieder, Zannad et al. ISN-Nexus 2010, 15–18 April, Kyoto, Japan
1.2
1.0
0.8
0.6
0.4
0.2
0
hsCRP split points (mg/L)
≥1.0 ≥2.0 ≥3.0 ≥4.0 ≥5.0
n=324
n=2168
p<0.018
n=618
n=1874
p<0.022 n=886
n=1606
p<0.023n=1107
n=1385
p<0.13
n=1203p<0.51
n=1289
<1.0 <2.0 <3.0 <4.0 <5.0
HR

Baigent C, Landray MJ, Reith C, Emberson J, Wheeler DC, Tomson C, Wanner C,
Krane V, Cass A, Craig J, Neal B, Jiang L, Hooi LS, Levin A, Agodoa L, Gaziano
M, Kasiske B, Walker R, Massy Z, Feldt-Rasmussen B, Krairittichai U,
Ophascharoensuk V, Fellström B, Holdaas H, Tesar V, Wiecek A, Haas M, Grobbee
R, de Zeeuw D, Grönhagen-Riska C, Dasgupta T, Lewis D, Herrington W, Mafham
M, Majoni W, Strony J, Musliner T, Grimm R, Pedersen T, Tobert J, Bray C, Knott
C, Collins R, on behalf of the SHARP Investigators.
Effects of lowering LDL-cholesterol with ezetimibe/simvastatin in patients with
chronic kidney disease: the Study of Heart and Renal Protection (SHARP).
The Lancet 2011 Jun 25;377(9784):2181-92.

0 1 2 3 4 5
Years of follow-up
0
5
10
15
20
25
Pro
po
rtio
n s
uff
erin
g ev
ent
(%) Risk ratio 0.83 (0.74 – 0.94)
Logrank 2P=0.0022
Placebo
Eze/simv
SHARP: Major Atherosclerotic Events

Anti-inflammatory treatment optionsPresent and future possibilities
Immunmodulering / Inflammationsdämpning
Statinbehandling
Immunosuppression
T-cells modulering
Vaccination
Cytokinhämning
RAS inhibition
Anti-oxidation
NO-enhancement

Semiquantitative estimation of influence by
immunosuppressive agents on CVD risk factors in
renal transplantation( 0 = neutral effect ; + , ++ , +++ = enhanced effect ; )
IS - drugs Hypertension Hyperlipidemia Diabetes Renal
Dysfunction
Cyclosporine ++ ++ + +
Tacrolimus + + ++ +
Sirolimus
/Everolimus
0 +++ 0 0
Corticosteroids + ++ +++ 0
Mycophenolate
mofetil
0 0 0 0
Monoclonal Ab 0 0 0 0
Fellström , Holdaas , Jardine : Cardiovascular Risk in RTx . Trends in Transplantation , 2009

Control RAPAMUNE
RAPAMUNE Prevents GVD in Monkeys
RE Morris
Et al

Sirolimus Protects Against Aortic Atherosclerosis
in Apo E Deficient Mice
Control Sirolimus 2 mg/kg

Everolimus reduces progression of intimal
thickening in HTxp=0.014
0.04 0.03
0.10
0.0
0.1
0.2
0.3
Max
imu
m i
nti
ma
l
thic
kn
ess
(m
m)
Everolimus
1.5 mg/day
(n=70)
Everolimus
3.0 mg/day
(n=69)
AZA
1–3 mg/kg/day
(n=72)
p=0.491 p=0.003

Proseek Multiplex CVD I 96x96 - Categories
Cardiovascular
Exploratory
Cardiovascular/
Inflammation
Inflammation

Proseek Multiplex CVD I 96x96 - Categories
–67
CA-125CCL20CCL3CCL4CSF-1CTSL1CXCL1CXCL-16ECPFS
GALHB-EGFIL-16IL-27AIL-4IL-6RAIL-8LOX-1mAmPPRLRAGES100A12/EN-RAGESCFTMTNF-R1TNF-R2TNFSF14/LIGHTTRAILTRANCEU-PARYKL-40/CHI3L1
CD40CD40L
CSTBCTSDCXCL-6FGF-23Gal-3GDF-15GHIL-18IL-1raIL-6KLK6MMP-12PAPPAPECAM-1/CD31PSGL-1RETNSELESPON1CASP-8IKBKG/IKK gammaSIRT2SRCTNFRSF10B/TRAIL 2
AGRPAMBeta-NGFCX3CL1Dkk-1EGFESM-1FABP4FASHGFhK11HSP 27LEPMBMCP-1Melusin/ITGB1BP2MMP-1MMP-10MMP-3MMP-7MPONPPBNT-pro-BNP
OPGPAR-1PDGF subunit BPlGFPTX3RENST2TFTIE2TMt-PAVEGF-AVEGF-D

Anti-inflammatory treatment optionsPresent and future possibilities
Immunmodulering / Inflammationsdämpning
Statinbehandling
Immunosuppression
T-cell modulation
Vaccination
Cytokinhämning
RAS inhibition
Anti-oxidation
NO-enhancement

Immunological involvement in
atherosclerosis Tcells & Mac activity
10% T-cells in plaque
reactive to ox-LDL
Tregs downregulate
reactivityt
Tregs contribute to
imm. protection and
attenuation of plaque
inflammation
Antibody driven
protection
Dependence on T-cells
Use of anti CD 25
Tregs drop, protective
effect by Ab blunted
Vaccination against a-s
MoAb ox-LDL

Anti-inflammatory and other optionsPresent and future possibilities
Immunmodulering / Inflammationsdämpning
Statinbehandling
Immunosuppression
T-cells modulering
Vaccination
Cytokinhämning
RAS inhibition
Anti-oxidation
NO-enhancement

Antibodies towards ox-LDL
Antibodies ox-LDL are protective
Vaccination towards ox-LDL in mice
– 50% reduction in atherosclerotic insult
Bojan Cercek, 1997 & Federico Calara, 1998
Jan Nilssons lab , Karolinska Institute, Stockholm

Immunological Targets in
Atherosclerosis
Immunol targets / ag
apoB100 sequences : p21, p 45 , p 210
Ox LDL
Ox PC
AGE , AOPP
Ox LDL , beta-OH –
Now entering into first vaccination studies in man
Lead by Jan Nilsson , Malmö

Zezina, Dimeny, Vessby, Fellström et al. Am J Nephrol 2002
Cut-off level for Ab-oxLDL < !255 l 255–3,533 > l 13,533 U/l
n (%) 30 (32.6%) 53 (57.6%) 9 (9.8%)
Graft loss due to
Chronic rejection 10% (3) 11% (6) 0
Acute rejectiona 20% (6) 6% (3) 0
Thrombosis 0 4% (2) 22% (2)
CHDc 37% (11) 13% (7) 11% (1)
Patient death 23% (7) 11% (6) 22% (2)
I nfluence of extreme Ab-oxLDL serum levels on the outcome of kidney transplantation.
and high but not significantly different incidence of graft loss due to acute rejection (p = 0.06).
Thirty patients (33%) had pre-transplant Ab-oxLDL levels < 256 U/l.
This group had higher frequency of CHD (p < 0.05)
High incidence of graft loss due to acute rejection (p = 0.06).
Antibodies Against Oxidised LDL
in Kidney Graft Recipients

IL-6R blockade ?
IL-1R blockade ?
TNFa blockade ?

Summary and Future Directions
• Uremic patients have a high morbitity & mortality in
Card-Vasc Disease (CKD)
• Uremia / CKD is associated with systemic inflammation
, which is a predictor of CVD
• Statins have a limited effect on CVD in advanced CKD
• Anti-inflammatory or cytokine inibiiton may turn out to
have beneficial effects , but needs to be shown.
• Documentation on the impact of complement
activation is pending.
• Future treatment with complement blockade may turn
out to be an option

Thank You
Questions or Comments
?


















