
CARDIAC RESYNCHRONISATION THERAPY (CRT) FOR CHRONIC ... · cardiac resynchronisation therapy (crt)...
32
CARDIAC RESYNCHRONISATION THERAPY (CRT) FOR CHRONIC CONGESTIVE HEART FAILURE (CHF) WHY ? WHEN ? Laurent SABBAH Cardiology Unit, Necker Hospital, Paris 29/04/2014
Transcript of CARDIAC RESYNCHRONISATION THERAPY (CRT) FOR CHRONIC ... · cardiac resynchronisation therapy (crt)...
CARDIAC RESYNCHRONISATION
THERAPY (CRT)
FOR CHRONIC CONGESTIVE HEART
FAILURE (CHF)
WHY ? WHEN ?
Laurent SABBAH
Cardiology Unit, Necker Hospital, Paris
29/04/2014

2

3
Prevalence : 2 - 3 % of population in Europe (1)
12 % > 60 years old in France % (2)
1rst hospitalisation cause after 60 years
5 years mortality : 50 % depending on NYHA class
(1) Dickstein K, Cohen-Solal A & alii. ESC guidelines for the diagnosis and treatment of acute and chronic
heart failure 2008. European Heart Journal
(2) Prévalence et prise en charge de l’insuffisance cardiaque en France - Enquête RS2002-2 février 2002 -
Réseau Sentinelle
CHF: EPIDEMIOLOGY
NYHA
II III IV
Annual Mortality (%) 5 - 15 20 - 50 30 -70
Sudden death mortality 50 - 80 30 - 50 5 - 30
CLASSICAL TREATMENT
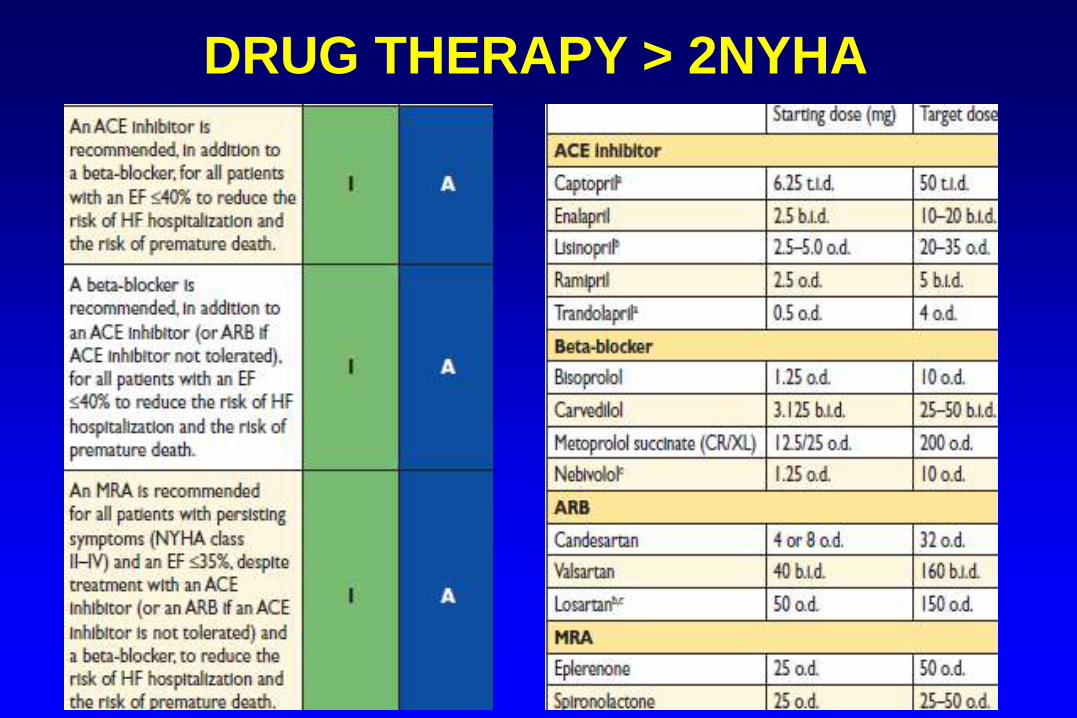
DRUG THERAPY > 2NYHA
6
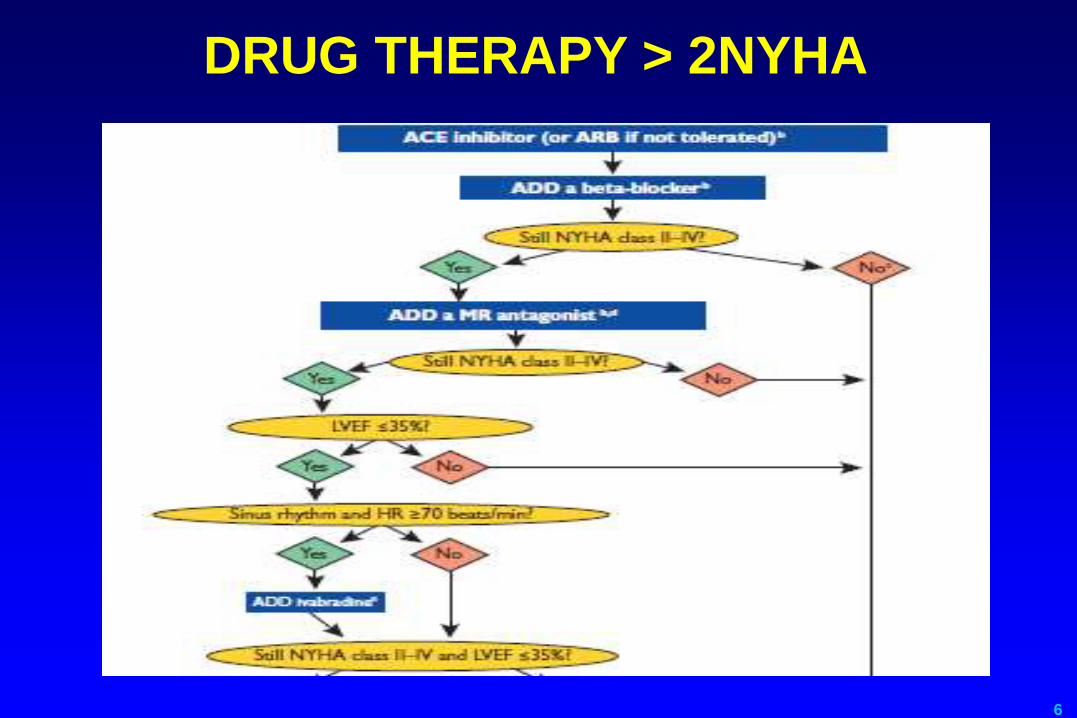
DRUG THERAPY > 2NYHA
7
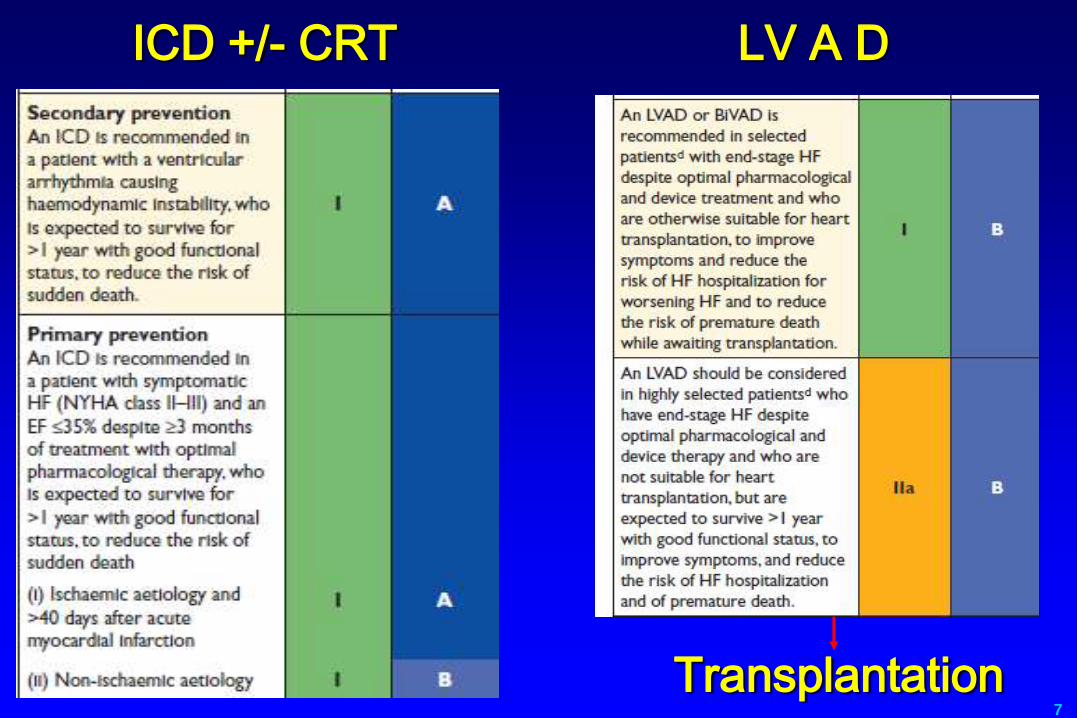
Transplantation
ICD +/- CRT LV A D
8
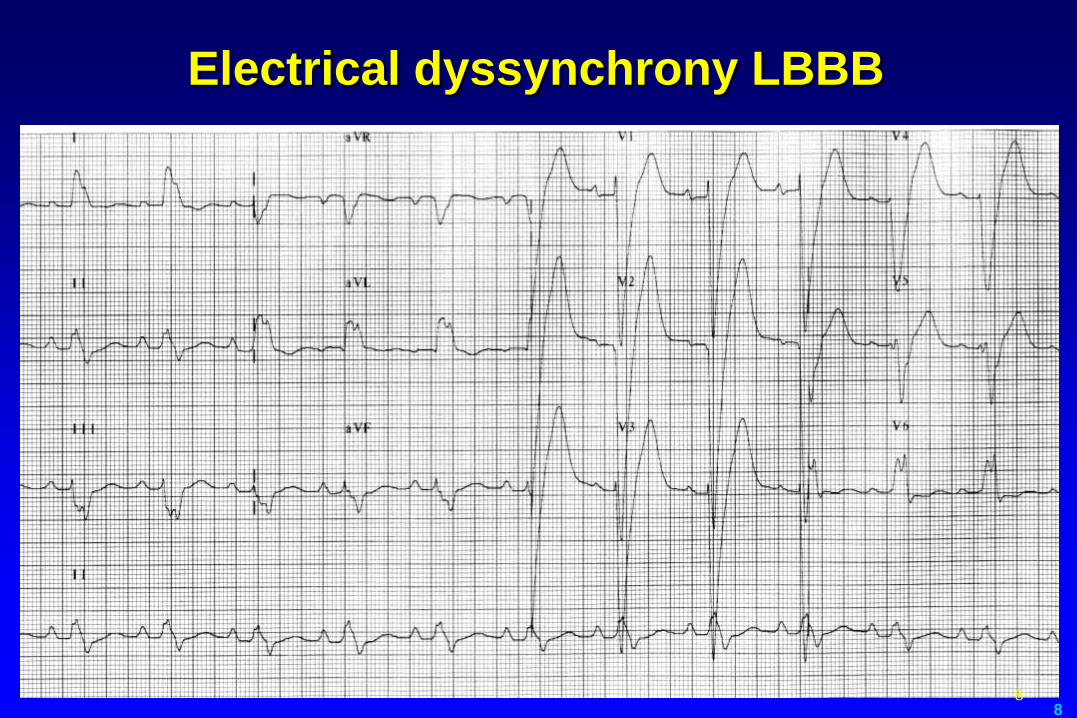
Electrical dyssynchrony LBBB
8
9
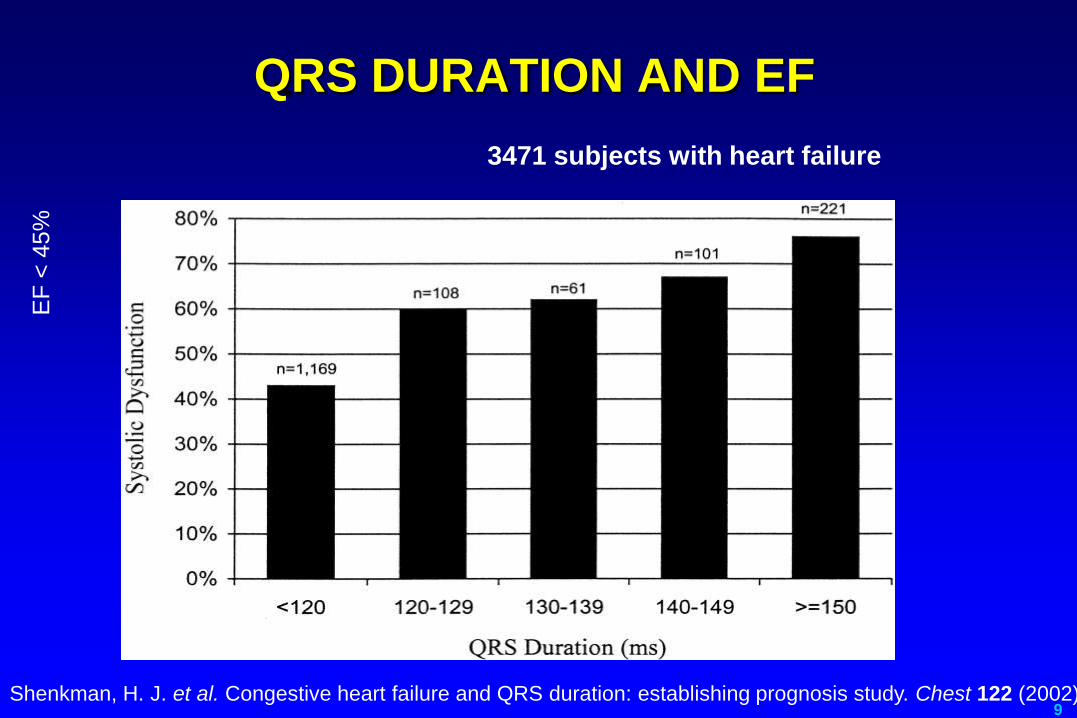
QRS DURATION AND EF
3471 subjects with heart failure
Shenkman, H. J. et al. Congestive heart failure and QRS duration: establishing prognosis study. Chest 122 (2002).
EF
< 4
5%

10
Prevalence and Prognosis of
Ventricular dyssynchrony
LBBB More Prevalent with
Impaired LV Systolic Function
38%
24%
8%
Mod/Sev HF (2)
Impaired LVSF (1)
Preserved LVSF (1)
1. Masoudi, et al. JACC. 2003;41:217-223.
2. Aaronson, et al. Circulation. 1997;95:2660-2667.
Increased All-Cause Mortality with Wide QRS at 45 Months (3)
34%
49%
QRS
< 120 ms
QRS
≥ 120 ms
3. Iuliano, et al. AHJ. 2002;143:1085-1091.
P < 0.001

11
QRS DURATION AND SURVIVAL
60%
70%
80%
90%
100%
0 60 120 180 240 300 360
Jours
Su
rvie
QRS duration (ms)
<90
90-120
120-170
170-220
>220
VEST study (1999)
Dilated CM NYHA>2
3654 ECG scanned
1year mortality
12
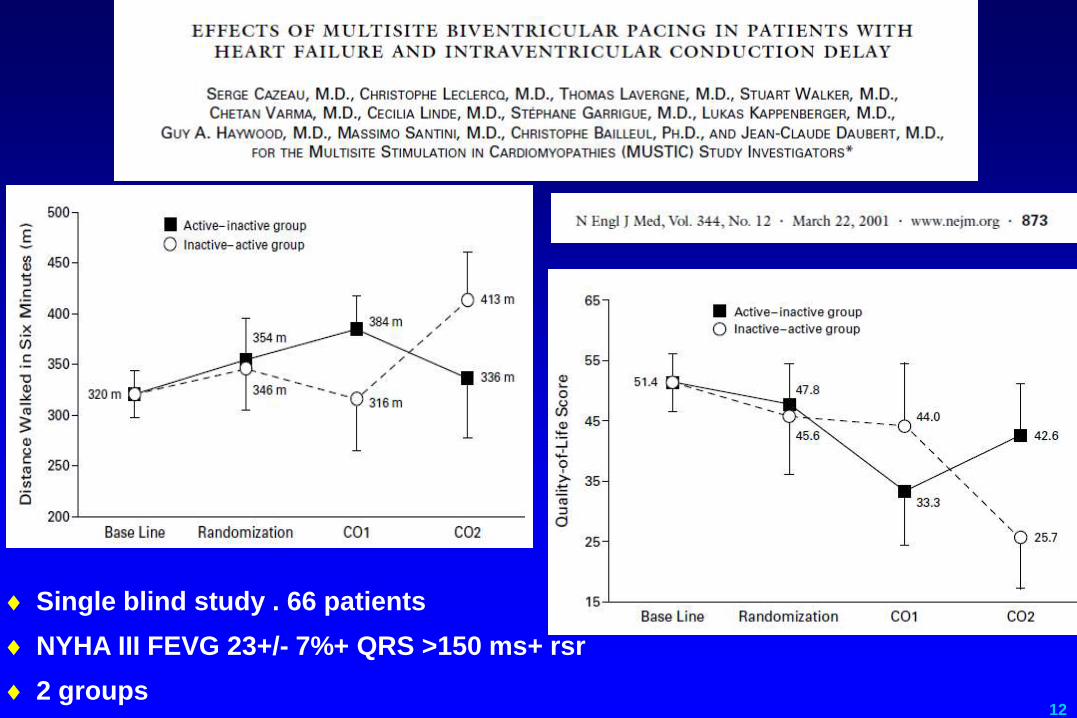
Single blind study . 66 patients
NYHA III FEVG 23+/- 7%+ QRS >150 ms+ rsr
2 groups
13
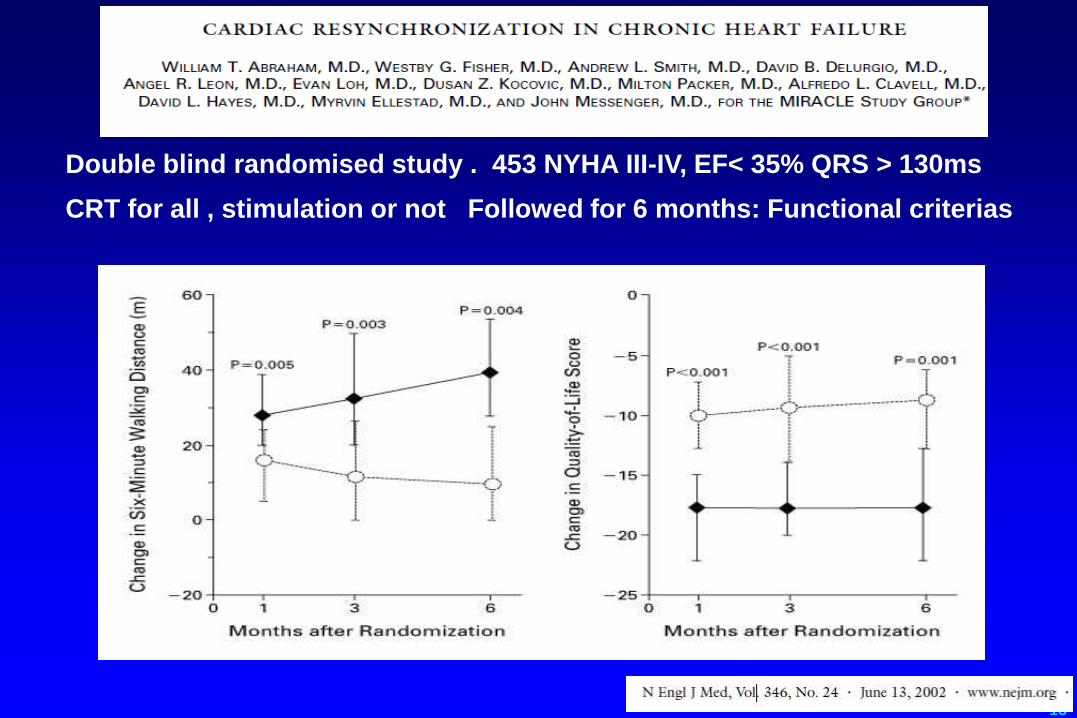
Double blind randomised study . 453 NYHA III-IV, EF< 35% QRS > 130ms
CRT for all , stimulation or not Followed for 6 months: Functional criterias
14
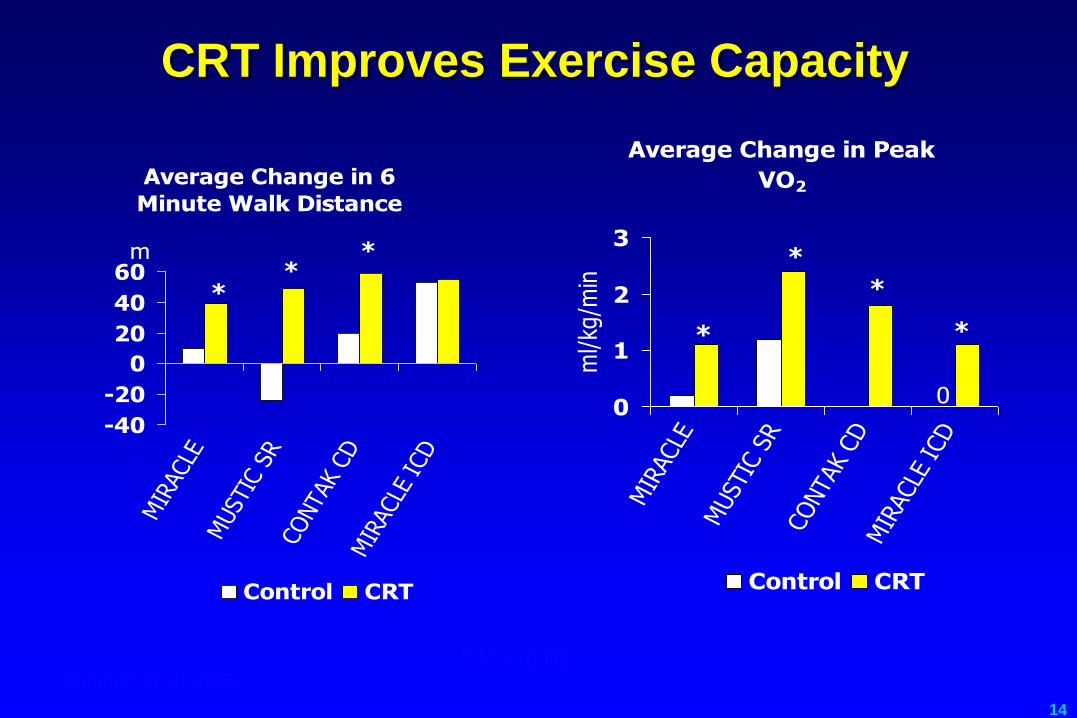
CRT Improves Exercise Capacity
* P < 0.05 Abraham et al., 2003
Average Change in 6
Minute Walk Distance
-40
-20
0
20
40
60
MIR
ACLE
MUST
IC S
RCO
NTA
K CD
MIR
ACLE
ICD
m
Control CRT
**
*
Average Change in Peak
VO2
00
1
2
3
MIR
ACLE
MUST
IC S
RCO
NTA
K CD
MIR
ACLE
ICD
ml/kg
/min
Control CRT
*
*
*
*

15
CRT Improves Quality of Life and
NYHA Functional Class
* P < 0.05 Abraham et al., 2003
Average Change in Score
(MLWHF)
-20
-15
-10
-5
0
MIR
ACLE
MUST
IC S
R
CONTA
K CD
MIR
ACLE
ICD
Control CRT
* * * *
NYHA: Proportion
Improving 1 or More Class
0%
20%
40%
60%
80%
MIRACLE CONTAK
CD
MIRACLE
ICD
Control CRT
**
*

16
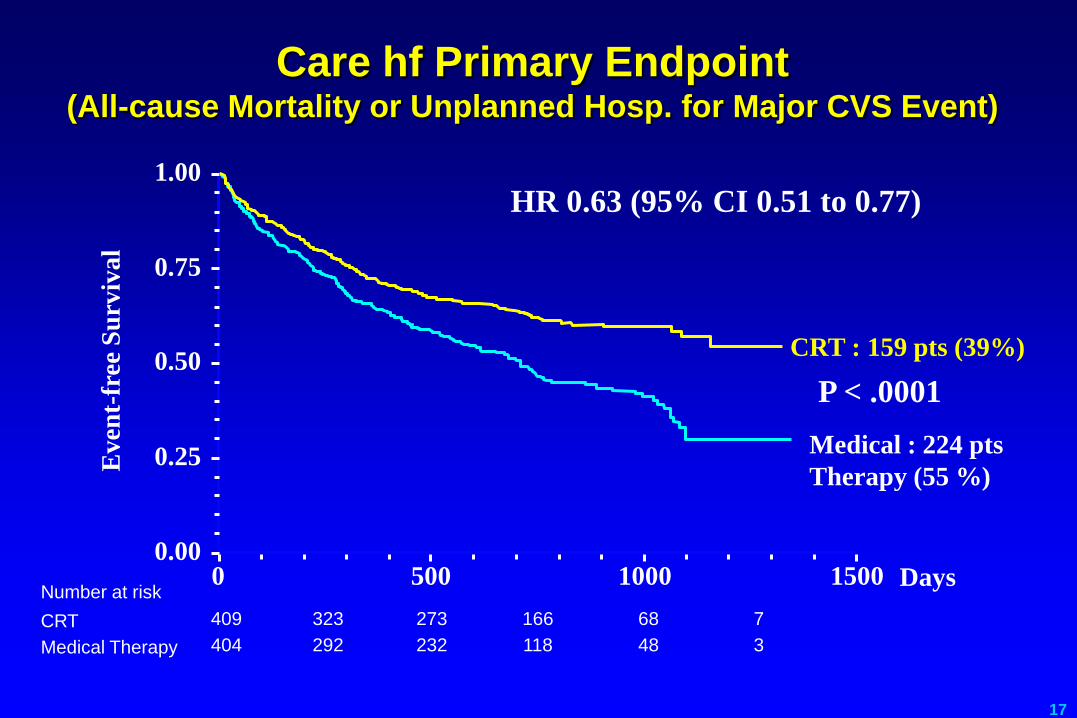
First mortality evaluation study
813 patients NYHA>3 QRS>120MSEC
EF : 25%
CRT VS drug therapy
Follow up : 3 years
17
Care hf Primary Endpoint (All-cause Mortality or Unplanned Hosp. for Major CVS Event)
CRT : 159 pts (39%)
3 48 118 232 292 404 Medical Therapy
7 68 166 273 323 409 CRT
Number at risk 0 500 1000 1500
0.00
0.25
0.50
0.75
1.00
HR 0.63 (95% CI 0.51 to 0.77)
Ev
ent-
free
Su
rviv
al
Days
P < .0001
Medical : 224 pts
Therapy (55 %)
18
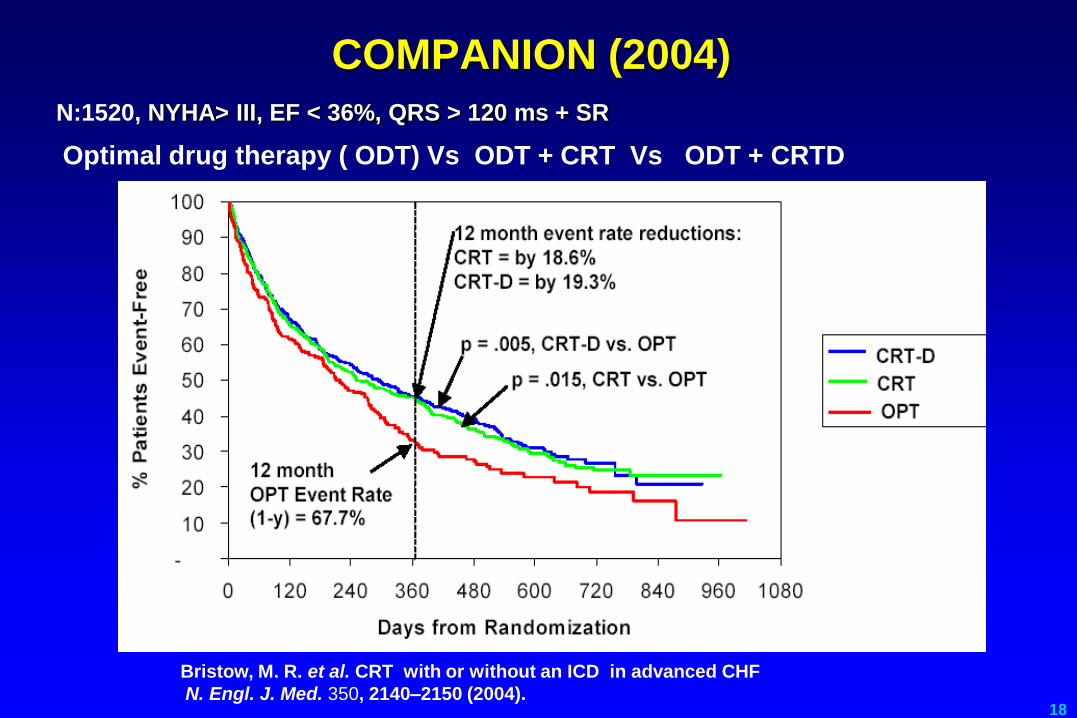
COMPANION (2004)
N:1520, NYHA> III, EF < 36%, QRS > 120 ms + SR
Optimal drug therapy ( ODT) Vs ODT + CRT Vs ODT + CRTD
Bristow, M. R. et al. CRT with or without an ICD in advanced CHF
N. Engl. J. Med. 350, 2140–2150 (2004).
19
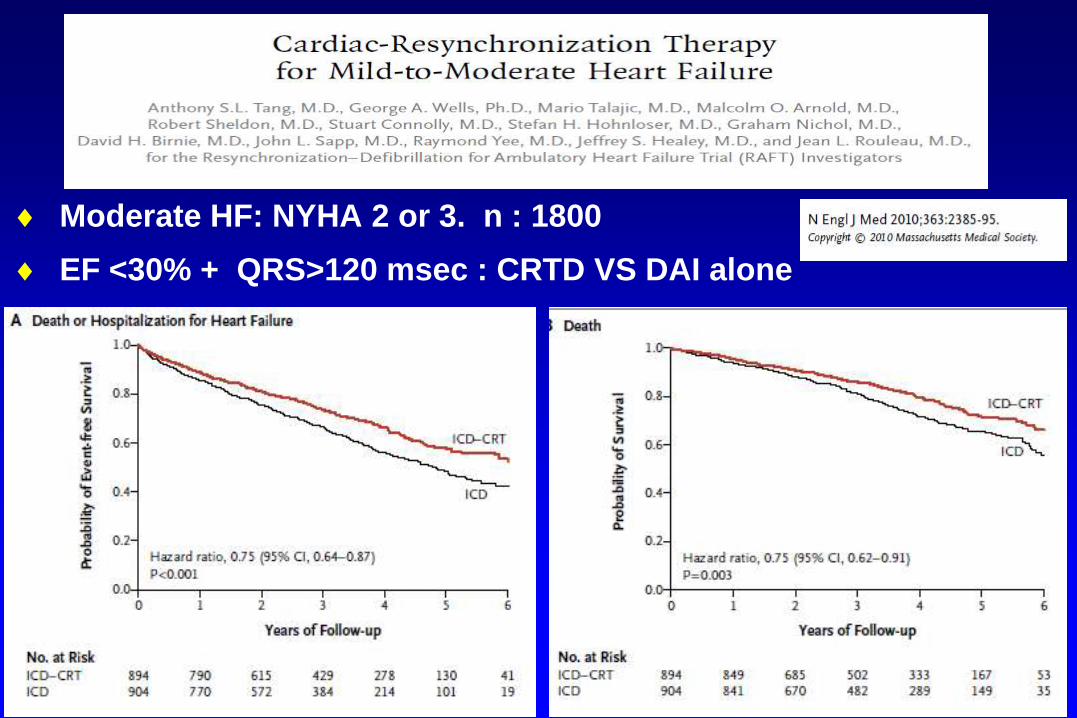
Moderate HF: NYHA 2 or 3. n : 1800
EF <30% + QRS>120 msec : CRTD VS DAI alone
20
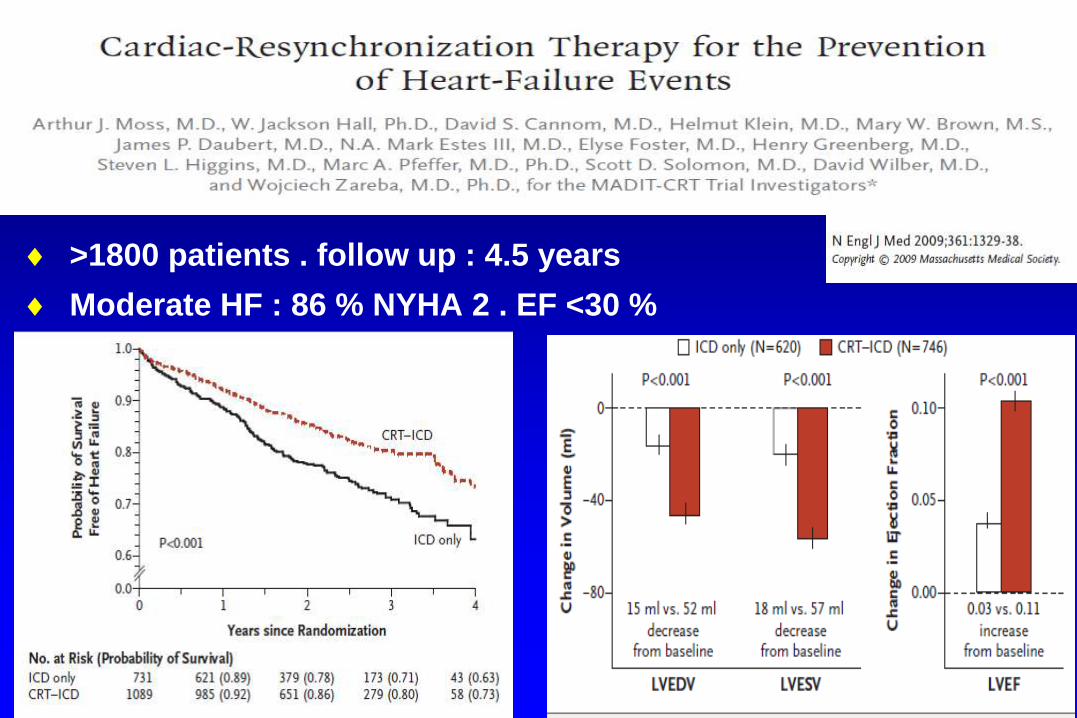
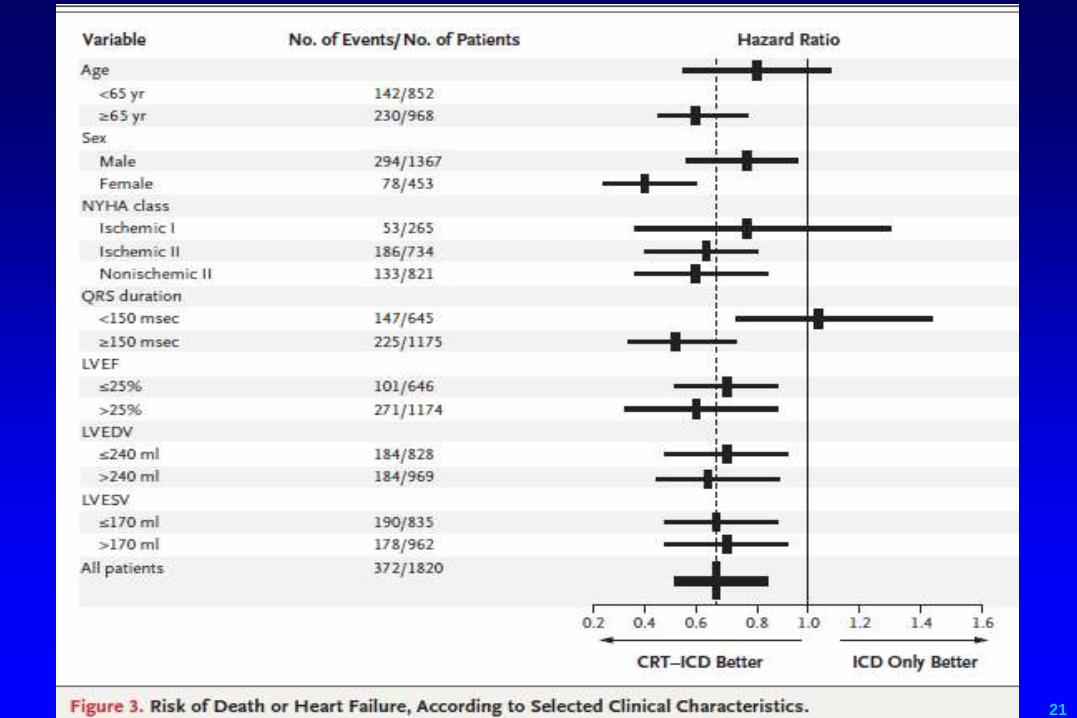
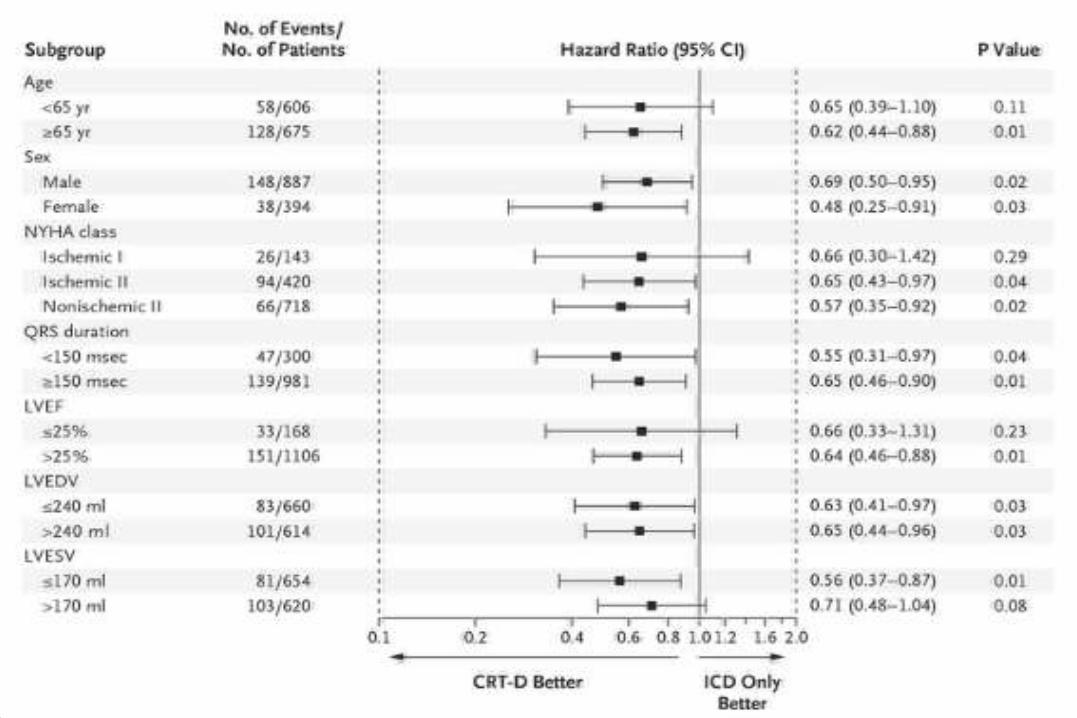
>1800 patients . follow up : 4.5 years
Moderate HF : 86 % NYHA 2 . EF <30 %
ICD VS CRTD
21

22
Goldenberg et al.
Nejm
Mars 2014
Results at 7 years
23
24
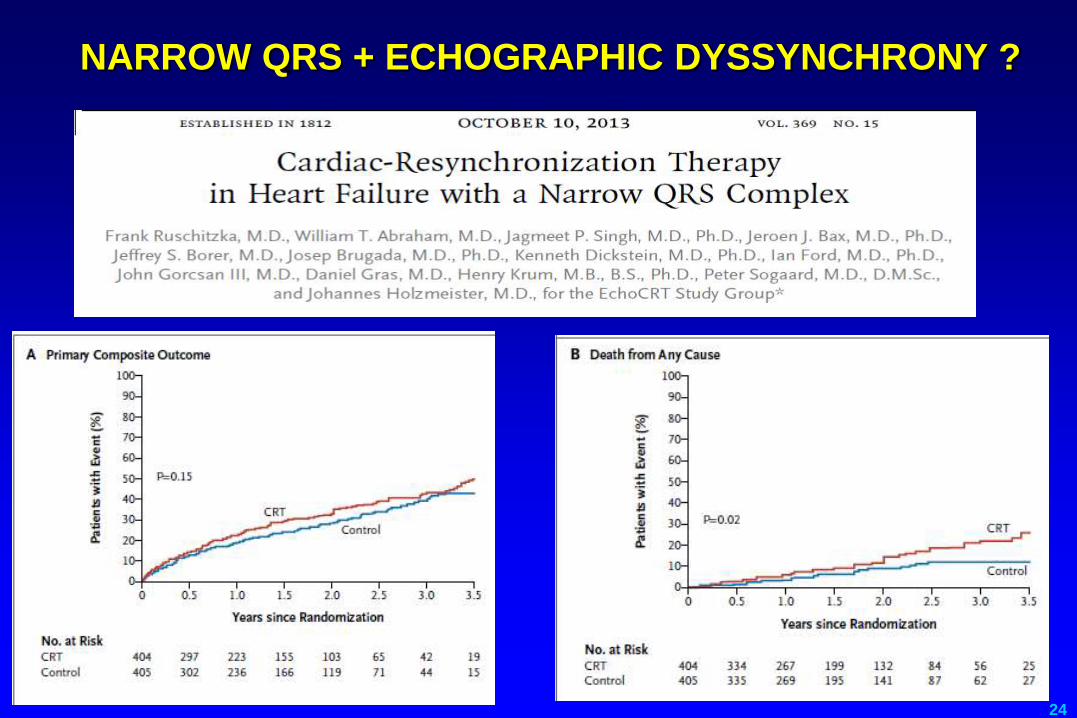
NARROW QRS + ECHOGRAPHIC DYSSYNCHRONY ?
25
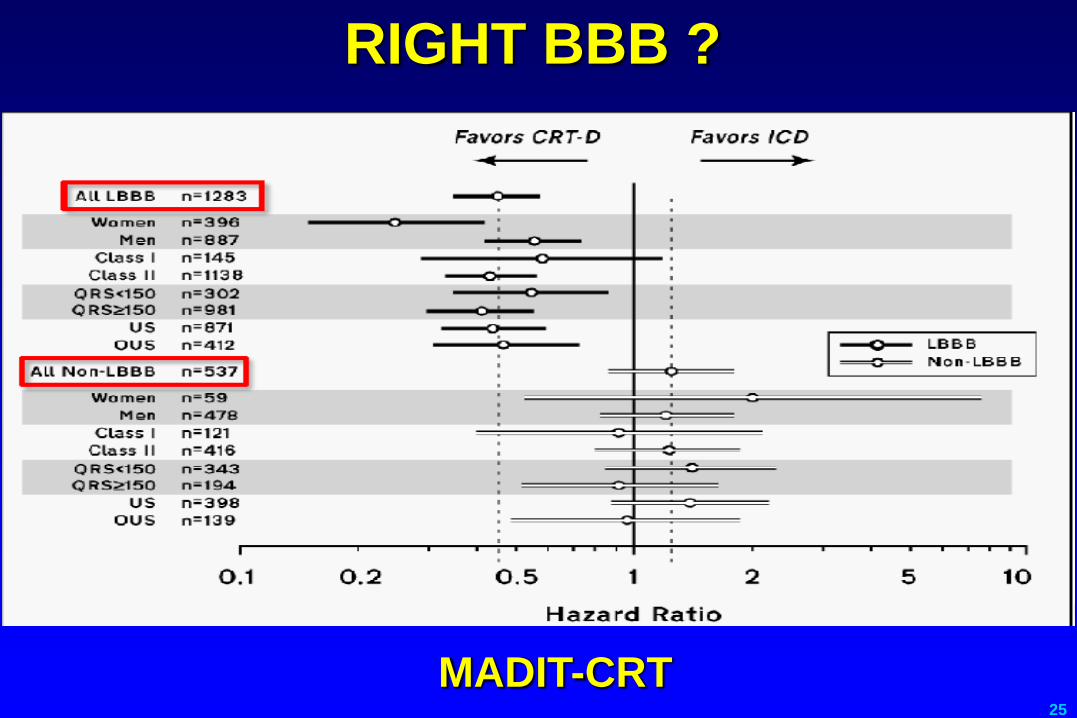
RIGHT BBB ?
MADIT-CRT
Recommandations
27
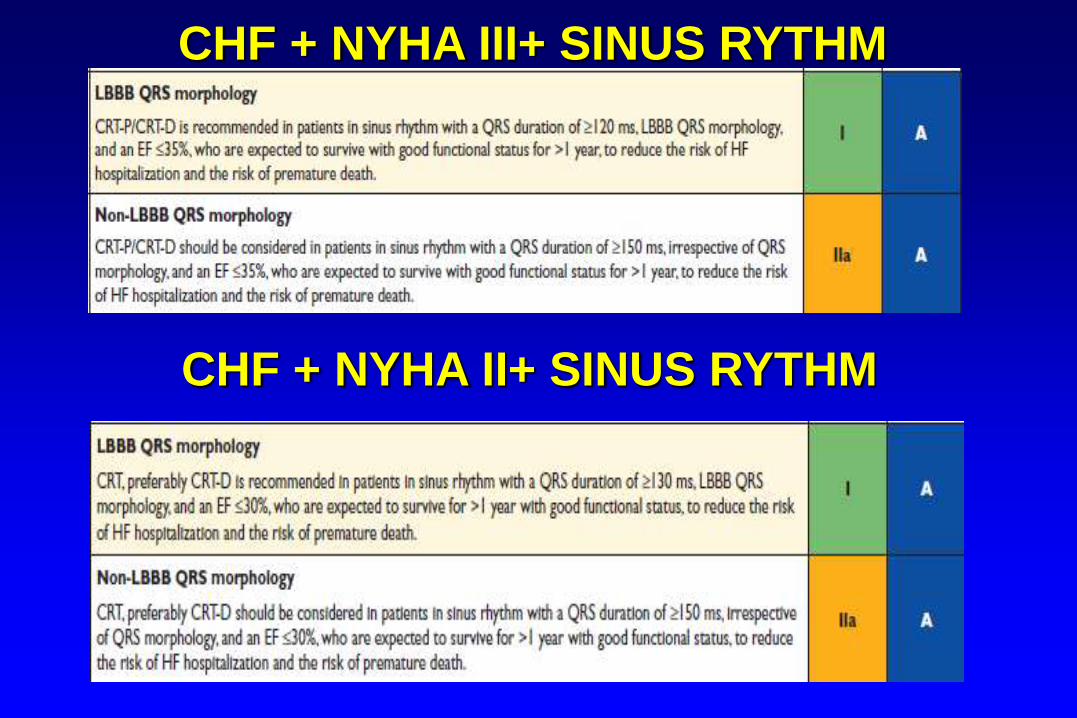
CHF + NYHA III+ SINUS RYTHM
CHF + NYHA II+ SINUS RYTHM
29
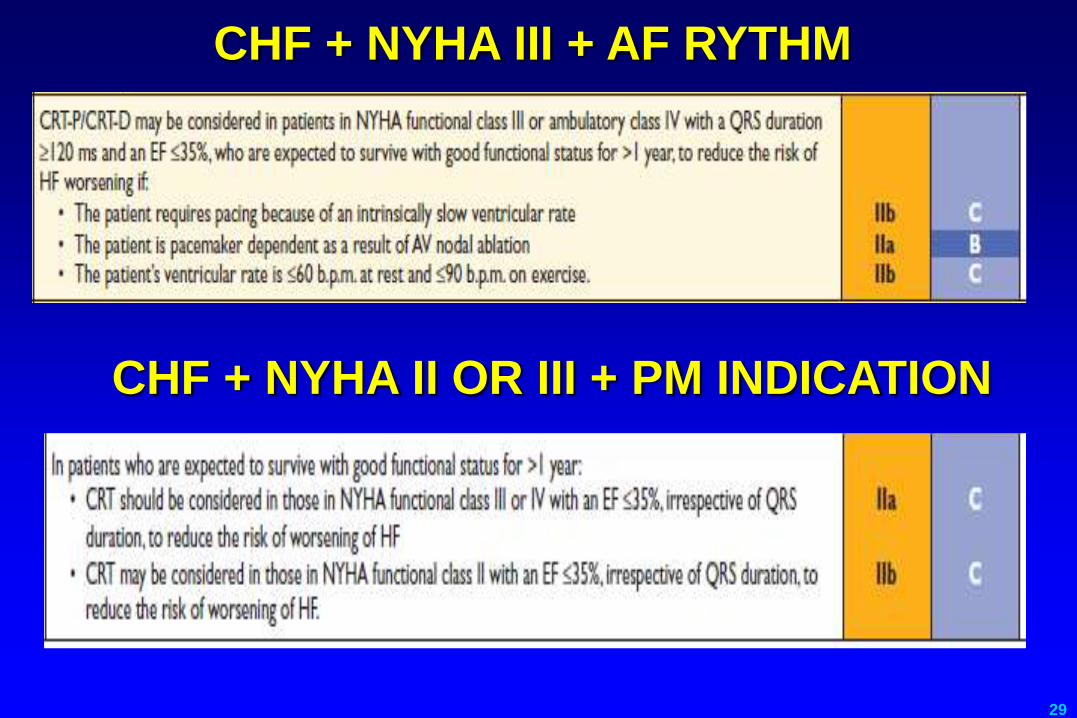
CHF + NYHA III + AF RYTHM
CHF + NYHA II OR III + PM INDICATION
30
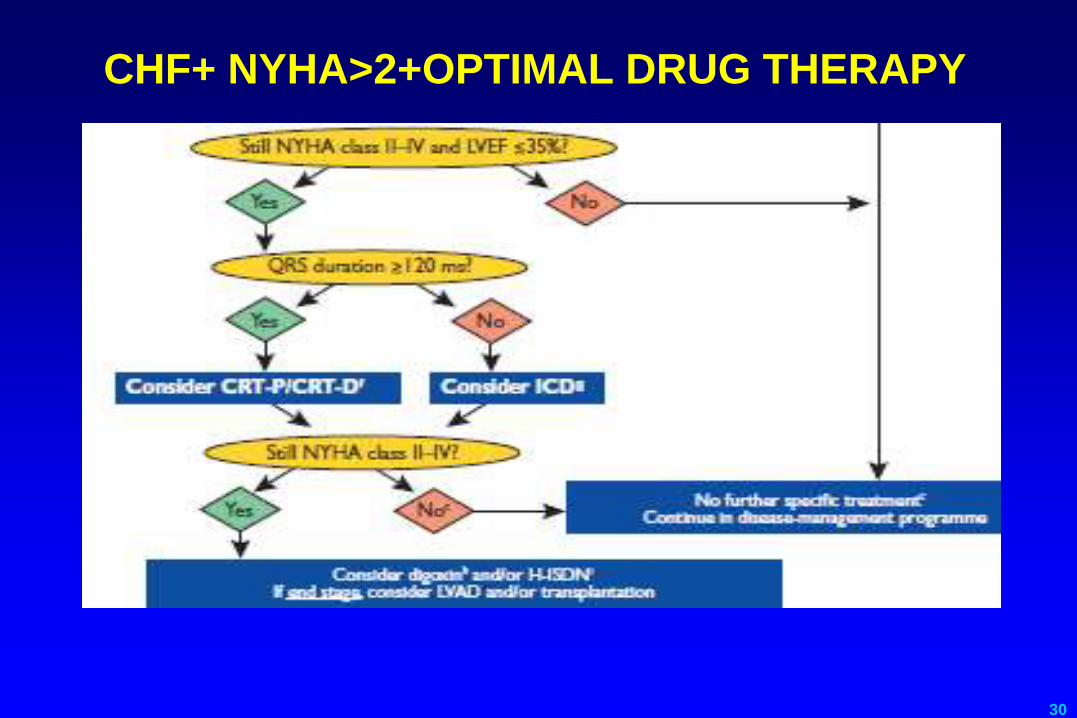
CHF+ NYHA>2+OPTIMAL DRUG THERAPY
31

32


















