Cardiac Glycosides and Therapy of Congestive Heart Failure Philip Marcus, MD MPH.
64
Cardiac Glycosides and Cardiac Glycosides and Therapy of Congestive Therapy of Congestive Heart Failure Heart Failure Philip Marcus, MD MPH Philip Marcus, MD MPH
-
Upload
caitlin-stokes -
Category
Documents
-
view
222 -
download
2
Transcript of Cardiac Glycosides and Therapy of Congestive Heart Failure Philip Marcus, MD MPH.

Cardiac Glycosides and Therapy of Cardiac Glycosides and Therapy of Congestive Heart FailureCongestive Heart Failure
Philip Marcus, MD MPHPhilip Marcus, MD MPH

Pathophysiology of Congestive Heart Pathophysiology of Congestive Heart FailureFailure
Inability of the heart to pump blood in amounts Inability of the heart to pump blood in amounts sufficient to meet metabolic needs of the tissuessufficient to meet metabolic needs of the tissuesWill result in:Will result in:– FatigueFatigue– Decreased exercise toleranceDecreased exercise tolerance– DyspneaDyspnea– OrthopneaOrthopnea– Venous distentionVenous distention– EdemaEdema– CardiomegalyCardiomegaly– HepatomegalyHepatomegaly– TachycardiaTachycardia
Progressive disease that begins long before Progressive disease that begins long before signs and symptoms are evidentsigns and symptoms are evident

Pathophysiology of Congestive Heart Pathophysiology of Congestive Heart FailureFailure
Etiology of Congestive Heart FailureEtiology of Congestive Heart Failure– HypertensionHypertension– Coronary artery diseaseCoronary artery disease– Acute myocardial infarctionAcute myocardial infarction– CardiomyopathyCardiomyopathy
Primary defect in CHF (systolic dysfunction)Primary defect in CHF (systolic dysfunction)– Reduction in contractile force of cardiac muscleReduction in contractile force of cardiac muscle– Decreased Cardiac Output (reduced ejection fraction)Decreased Cardiac Output (reduced ejection fraction)
Diastolic DysfunctionDiastolic Dysfunction– Elevated end-diastolic pressureElevated end-diastolic pressure– Normal-sized chamber (LV)Normal-sized chamber (LV)– Inability to fill and relax ventricleInability to fill and relax ventricle

Physiologic Adaptations to Reduced Physiologic Adaptations to Reduced Cardiac Output (Cardiac Output (to improve perfusionto improve perfusion))
Cardiac DilatationCardiac Dilatation
Increased sympathetic toneIncreased sympathetic tone– Increased heart rateIncreased heart rate– Increased contractilityIncreased contractility– Increase in venous toneIncrease in venous tone
Increase in Increase in preloadpreload– Increase in arteriolar toneIncrease in arteriolar tone
Increase in Increase in afterloadafterload

Physiologic Adaptations to Reduced Physiologic Adaptations to Reduced Cardiac Output (Cardiac Output (to improve perfusionto improve perfusion))
Water retention and increase in blood volumeWater retention and increase in blood volume– Reduction in CO leads to decrease in RBFReduction in CO leads to decrease in RBF– Reduced RBF leads to decrease in GFRReduced RBF leads to decrease in GFR– Decrease in GFR leads to decreased urine productionDecrease in GFR leads to decreased urine production
– Decrease in RBF leads to increase in renin activityDecrease in RBF leads to increase in renin activity– Increase in renin causes increase in Increase in renin causes increase in aldosteronealdosterone– Increased aldosterone leads to sodium and water Increased aldosterone leads to sodium and water
retentionretention


Determinants of Cardiac PerformanceDeterminants of Cardiac Performance
PreloadPreload– Measure of LV filling (stretch)Measure of LV filling (stretch)– Measure LVEDV, LVEDPMeasure LVEDV, LVEDP– In CHF, preload increases and cardiac performance In CHF, preload increases and cardiac performance
(SV, Stroke work) decrease(SV, Stroke work) decrease– Increased preload secondary to:Increased preload secondary to:
Increase in blood volumeIncrease in blood volumeIncrease in venous toneIncrease in venous tone
Reduction of high filling pressure is goal of therapyReduction of high filling pressure is goal of therapy

Determinants of Cardiac PerformanceDeterminants of Cardiac Performance
AfterloadAfterload– Resistance against which the heart must pump bloodResistance against which the heart must pump blood– Represented by aortic impedance and systemic vascular Represented by aortic impedance and systemic vascular
resistanceresistance– SVR increases in CHF secondary to:SVR increases in CHF secondary to:
Increased sympathetic outflowIncreased sympathetic outflow
Increase in circulating catecholaminesIncrease in circulating catecholamines
Activation of renin-angiotensin-aldosterone systemActivation of renin-angiotensin-aldosterone system
– Increase in SVR further reduces C.O.Increase in SVR further reduces C.O.
– Reduction of SVR is one goal of treatmentReduction of SVR is one goal of treatment

Determinants of Cardiac PerformanceDeterminants of Cardiac Performance
ContractilityContractility– Vigor of contraction of heart muscleVigor of contraction of heart muscle
– As contractility decreases, velocity of muscle As contractility decreases, velocity of muscle shortening and rate of intraventricular shortening and rate of intraventricular pressure development decrease (dP/dt)pressure development decrease (dP/dt)
– Goal of inotropic therapy is to increase Goal of inotropic therapy is to increase contractilitycontractility
Heart RateHeart Rate

Left Ventricular Dysfunction
Remodeling
Low Ejection Fraction
Death
Arrhythmia
Pump Failure
Chronic Heart Failure
Congestive Heart Failure: Pathophysiology

Classification of Heart FailureClassification of Heart Failure
Stage AStage A– High risk of developing heart failureHigh risk of developing heart failure– No structural disorder of the heart or signs of No structural disorder of the heart or signs of
symptoms of heart failuresymptoms of heart failure
Stage BStage B– Structural disorder of the heartStructural disorder of the heart– No signs or symptoms of heart failureNo signs or symptoms of heart failure
Stage CStage C– Past or current symptoms of heart failure associated Past or current symptoms of heart failure associated
with underlying structural heart diseasewith underlying structural heart disease
Stage DStage D– End-stage heart failure and need for specialized End-stage heart failure and need for specialized
treatment strategiestreatment strategies

CLASSIFICATION OF CHFCLASSIFICATION OF CHFCongestion at Rest
Low
Perfusion at
Rest
NO YES
NO
YES
Warm/Dry Warm/Wet
PCWP normal PCWP ↑ CI normal CI normal
Cold/Dry Cold/Wet
PCWP normal/↑ PCWP ↑
CI ↓ CI ↓
COMMON
Dry Them Out

Agents used to treat CHF:Agents used to treat CHF:
Inotropic agentsInotropic agents
DiureticsDiuretics– Antialdosterone therapyAntialdosterone therapy
VasodilatorsVasodilators
-blockers-blockers
Salt restrictionSalt restriction
Recent shift from hemodynamic to neurohumoral alterations

Diuretics in CHFDiuretics in CHF
Diuretic therapy results in:Diuretic therapy results in:– Improvement in sodium excretionImprovement in sodium excretion– Improvement in symptoms of fluid overloadImprovement in symptoms of fluid overload– Improvement in exercise toleranceImprovement in exercise tolerance– Improvement of cardiac functionImprovement of cardiac function
Should not be prescribed as monotherapyShould not be prescribed as monotherapy– Start for symptom controlStart for symptom control
Titrate to avoid excess volume depletionTitrate to avoid excess volume depletionUnder-titration can diminish response to ACE Under-titration can diminish response to ACE inhibitors and increase frequency of adverse inhibitors and increase frequency of adverse effects of treatment with effects of treatment with blockersblockers

Possible means of increasing Possible means of increasing myocardial contractilitymyocardial contractility
Increased intracellular CaIncreased intracellular Ca++++
– Increased cAMPIncreased cAMPStimulation of Stimulation of -receptors-receptorsStimulation of adenylate cyclaseStimulation of adenylate cyclaseInhibition of phosphodiesterase IIIInhibition of phosphodiesterase III
– cAMP independent mechanismscAMP independent mechanismsMembrane channelsMembrane channels
– Activation of CaActivation of Ca++++ and Na and Na++ channels channels– Inhibition of KInhibition of K++ channels channels
Membrane pumpsMembrane pumps– Inhibition of NaInhibition of Na++/ K/ K++ ATPase ATPase– Inhibition of NaInhibition of Na++/ Ca/ Ca++++ exchange exchange– Other mechanisms (stimulation of Other mechanisms (stimulation of receptors) receptors)
Increased sensitivity of contractile proteins to CaIncreased sensitivity of contractile proteins to Ca++++

Inotropic agents:Inotropic agents:
Act on heart muscle to improve contractility and Act on heart muscle to improve contractility and increase C.O.increase C.O.
11 adrenergic agonists adrenergic agonists– DopamineDopamine– DobutamineDobutamine
Bipyridine compoundsBipyridine compounds– Inamrinone Inamrinone – MilrinoneMilrinone
Cardiac (digitalis) glycosidesCardiac (digitalis) glycosides– DigoxinDigoxin– Digitoxin (discontinued Oct., 2000)Digitoxin (discontinued Oct., 2000)
Common Foxglove PlantCommon Foxglove PlantD. PurpureaD. Purpurea

Cardiac Glycosides:Cardiac Glycosides:
All compounds exert similar pharmacological All compounds exert similar pharmacological effectseffectsAgents differ in pharmacokinetic Agents differ in pharmacokinetic characteristicscharacteristicsDerived from naturally occurring compounds Derived from naturally occurring compounds obtained from leaves of:obtained from leaves of:– Digitalis purpurea (digitoxin)Digitalis purpurea (digitoxin)– Digitalis lanata (digoxin)Digitalis lanata (digoxin)
Known to ancient EgyptiansKnown to ancient EgyptiansWithering (1785) described effects of extract Withering (1785) described effects of extract of Foxglove plant in patients with of Foxglove plant in patients with dropsydropsy– An Account of the Foxglove, and Some of Its Medical Uses: With An Account of the Foxglove, and Some of Its Medical Uses: With
Practical Remarks on Dropsy and Other DiseasesPractical Remarks on Dropsy and Other Diseases



Cardiac Glycosides (Chemistry):Cardiac Glycosides (Chemistry):
Steroid nucleus combines with unsaturated 5-Steroid nucleus combines with unsaturated 5-member lactone ring at C17 position and series member lactone ring at C17 position and series of sugars linked to C3 of the nucleusof sugars linked to C3 of the nucleusLactone ring and steroid nucleus essential for Lactone ring and steroid nucleus essential for activity (=aglycone)activity (=aglycone)Sugar moiety influencesSugar moiety influences– AbsorptionAbsorption– Half-lifeHalf-life– MetabolismMetabolism

Cardiac Glycosides: Cardiac Glycosides: Pharmacological effectsPharmacological effects
PharmacodynamicsPharmacodynamics– Mechanical effectsMechanical effects– Electrical effectsElectrical effects
DirectDirectIndirect (involve reflex actions)Indirect (involve reflex actions)
Extracardiac effectsExtracardiac effectsDigitalis toxicityDigitalis toxicityPharmacokineticsPharmacokineticsClinical useClinical use

Mechanical Effects:Mechanical Effects:
Acts on cardiac muscle to increase contractile forceActs on cardiac muscle to increase contractile force= = + inotropic action+ inotropic actionMechanism of inotropic actionMechanism of inotropic action– Inhibition of NaInhibition of Na++-K-K++ ATPase ATPase (sodium pump)(sodium pump)
Promotes CaPromotes Ca++++ accumulation accumulation
– Increases force of contraction by facilitating Increases force of contraction by facilitating interaction of myocardial contractile proteinsinteraction of myocardial contractile proteins
Increases intensity of interaction of actin and myosin Increases intensity of interaction of actin and myosin filaments of cardiac sarcomerefilaments of cardiac sarcomereCaused by increases in free [CaCaused by increases in free [Ca++++] in vicinity of contractile ] in vicinity of contractile proteins during systole proteins during systole

Ion Fluxes across the Cardiac Cell Membrane

Relationship of [KRelationship of [K++] to digitalis action] to digitalis action
Potassium competes with digitalis for Potassium competes with digitalis for binding to Nabinding to Na++-K-K++ ATPase ATPase
When Potassium levels low, digitalis When Potassium levels low, digitalis binding increasesbinding increases– Increased binding produces excess inhibition Increased binding produces excess inhibition
of Naof Na++-K-K++ ATPase with resultant toxicity ATPase with resultant toxicity– [K[K++] must be kept within ] must be kept within normal normal rangerange

Digitalis Effects:Digitalis Effects:
In patients with CHFIn patients with CHF– Enhances contractility (inotropic)Enhances contractility (inotropic)– Reduces SVR (which occurred via compensatory processes)Reduces SVR (which occurred via compensatory processes)– Heart size decreasesHeart size decreases– C.O. increasesC.O. increases– As efficiency improves, MVOAs efficiency improves, MVO22 decreases decreases
In normal patientsIn normal patients– Increases SVRIncreases SVR
Increases peripheral vasoconstriction (direct)Increases peripheral vasoconstriction (direct)Increases central sympathetic outflowIncreases central sympathetic outflow
– Increases contractilityIncreases contractility– No change in C.O.No change in C.O.

Electrical Effects:Electrical Effects:
Therapeutic and Therapeutic and ToxicologicalToxicological Importance ImportanceDigitalis glycosides useful for treatment of Digitalis glycosides useful for treatment of arrhythmiasarrhythmias– Atrial fibrillationAtrial fibrillation– Atrial flutterAtrial flutter
May also cause arrhythmiasMay also cause arrhythmiasComplex effectsComplex effects– Direct effectsDirect effects– Indirect effectsIndirect effects

Electrical Effects:Electrical Effects:
Digitalis alters electrical activity of non-contractile Digitalis alters electrical activity of non-contractile tissuetissue– S-A nodeS-A node– A-V nodeA-V node– Purkinje fibersPurkinje fibers
Alters electrical activity of atrial and ventricular Alters electrical activity of atrial and ventricular musclemuscleCan alter:Can alter:– AutomaticityAutomaticity– RefractorinessRefractoriness– Impulse conductionImpulse conduction

Direct Electrical Effects:Direct Electrical Effects:
Result from inhibition of NaResult from inhibition of Na++-K-K++ ATPase ATPase
Alters distribution of ions across cardiac Alters distribution of ions across cardiac cell membranecell membrane
Alters electrical responsiveness of cellsAlters electrical responsiveness of cells
Direct effects heightened by Direct effects heightened by hypokalemiahypokalemia

Direct Electrical Actions:Direct Electrical Actions:
Direct actions on membranes of cardiac cells follow Direct actions on membranes of cardiac cells follow well-defined progression:well-defined progression:– Early, brief prolongation of Early, brief prolongation of action potentialaction potential– Protracted period of shortening of Protracted period of shortening of action potentialaction potential, especially , especially
plateauplateau? Result of inc. K? Result of inc. K++ conductance conductance
Caused by inc. intracellular CaCaused by inc. intracellular Ca++++
Contributes to shortening of atrial and ventricular refractorinessContributes to shortening of atrial and ventricular refractoriness
– Decreased conduction velocity through A-V node and in Purkinje Decreased conduction velocity through A-V node and in Purkinje systemsystem
– Increased refractory period in A-V nodeIncreased refractory period in A-V node

Direct Electrical Actions:Direct Electrical Actions:
Automaticity increases, particularly in ventricular Automaticity increases, particularly in ventricular tissue:tissue:– Decreased activity of normal pacemaker tissueDecreased activity of normal pacemaker tissue– Decreased ventricular refractory periodDecreased ventricular refractory period– Increase A-V blockIncrease A-V block
Ectopic foci can therefore be generated, particularly Ectopic foci can therefore be generated, particularly in Purkinje systemin Purkinje system– PVCs, bigeminyPVCs, bigeminy– Ventricular tachycardiaVentricular tachycardia– Ventricular fibrillationVentricular fibrillation

EKG Effects of Digitalis Glycosides:EKG Effects of Digitalis Glycosides:
P-R interval prolongationP-R interval prolongation– Prolonged A-V nodal conductionProlonged A-V nodal conduction
T-wave depressionT-wave depression– Increase in repolarization of subendocardial Increase in repolarization of subendocardial
tissuetissue
ST depressionST depressionQT interval shorteningQT interval shortening– Decreased time for ventricular systoleDecreased time for ventricular systole

Indirect Electrical Effects:Indirect Electrical Effects:
Digitalis increases Digitalis increases vagal vagal influencesinfluences– Increased rate of vagal firingIncreased rate of vagal firing
Slows spontaneous discharge of SA nodeSlows spontaneous discharge of SA node
Suppresses conduction through AV nodeSuppresses conduction through AV node
Causes reflex reduction in sympathetic toneCauses reflex reduction in sympathetic tone
Increase in vagal firing and decrease in sympathetic Increase in vagal firing and decrease in sympathetic tone causes:tone causes:– Decrease in SA automaticityDecrease in SA automaticity– Decrease in AV conduction (A-V block)Decrease in AV conduction (A-V block)
Actions are complimentaryActions are complimentary

Digital Glycosides: Digital Glycosides: Specific EffectsSpecific Effects
SA NodeSA Node– Slows pacemaker activitySlows pacemaker activity
Increased vagal activityIncreased vagal activityDecreased sympathetic activityDecreased sympathetic activity
AV NodeAV Node– Decreased conduction through AV nodeDecreased conduction through AV node– Increased refractoriness of AV nodeIncreased refractoriness of AV node
– = A-V block= A-V block Purkinje FibersPurkinje Fibers– Increased automaticityIncreased automaticity– Ectopic fociEctopic foci– Ventricular arrhythmiasVentricular arrhythmias

Cardiotoxicity of Digitalis:Cardiotoxicity of Digitalis:Arrhythmia productionArrhythmia production– Most serious adverse effectMost serious adverse effect– Secondary to alteration of electrical propertiesSecondary to alteration of electrical properties– Assess all patients for alterations in Assess all patients for alterations in raterate and and rhythmrhythm
All arrhythmias seenAll arrhythmias seen– BradycardiaBradycardia– A-V block, A-V junctional rhythmA-V block, A-V junctional rhythm– Ventricular tachycardiaVentricular tachycardia– Ventricular fibrillationVentricular fibrillation

Cardiotoxicity of Digitalis:Cardiotoxicity of Digitalis:
Mechanism of arrhythmia generation:Mechanism of arrhythmia generation:– Inc. automaticity of atrial and ventricular tissueInc. automaticity of atrial and ventricular tissue
ectopyectopy
– Dec. conduction through A-V nodeDec. conduction through A-V nodeA-V blockA-V block
– Both factors due to Both factors due to NaNa++-K-K++ ATPase ATPase inhibitioninhibition
Augmented by hypokalemiaAugmented by hypokalemia

Cardiotoxicity of Digitalis:Cardiotoxicity of Digitalis:
Predisposing factors:Predisposing factors:– HypokalemiaHypokalemia– Digitalis toxicityDigitalis toxicity– MyocarditisMyocarditis– HypercalcemiaHypercalcemia– HypomagnesemiaHypomagnesemia– HypothyroidismHypothyroidism– AgeAge– Renal diseaseRenal disease– HypoxemiaHypoxemia

Digitalis Toxicity:Digitalis Toxicity:
Defined solely as elevation in serum Defined solely as elevation in serum digitalis digitalis levellevel– Digoxin > 2.5 ng/mlDigoxin > 2.5 ng/ml– Digitoxin >35 ng/ml (of historical interest)Digitoxin >35 ng/ml (of historical interest)
Digoxin levels may rise secondary to use of:Digoxin levels may rise secondary to use of:– AmiodaroneAmiodarone– VerapamilVerapamil– DiltiazemDiltiazem– Quinidine Quinidine

Digitalis Toxicity: ManagementDigitalis Toxicity: Management
Discontinue drugDiscontinue drugCorrect Correct hypokalemiahypokalemiaAntiarrhythmicsAntiarrhythmics– LidocaineLidocaine– PhenytoinPhenytoin
Pacemaker InsertionPacemaker Insertion
Digibind®Digibind® administration administration– Digoxin-specific Fab fragmentsDigoxin-specific Fab fragments
Prevents tissue binding of digoxinPrevents tissue binding of digoxin30 minute onset of action30 minute onset of actionClearance within 3-4 daysClearance within 3-4 days
– Digoxin + Fab fragments in urineDigoxin + Fab fragments in urine
Dialysis Dialysis ineffectiveineffective

Extracardiac Effects of Digitalis:Extracardiac Effects of Digitalis:
GastrointestinalGastrointestinal– AnorexiaAnorexia– NauseaNausea– Vomiting Vomiting
Central Nervous SystemCentral Nervous System– FatigueFatigue– Visual disturbancesVisual disturbances
Halos around lightsHalos around lightsAlteration of color perceptionAlteration of color perception
– HallucinationsHallucinations– DisorientationDisorientation

Therapeutic Uses of Digitalis:Therapeutic Uses of Digitalis:
Congestive Heart FailureCongestive Heart Failure– Indicated in patients with severe LV dysfunctionIndicated in patients with severe LV dysfunction
Primarily used Primarily used afterafter diuretics and vasodilators diuretics and vasodilatorsNot useful in diastolic dysfunction or right-sided heart failureNot useful in diastolic dysfunction or right-sided heart failureMost efficacious when S3 noted on examinationMost efficacious when S3 noted on examination
Atrial arrhythmiasAtrial arrhythmias– Indicated in atrial fibrillation and atrial flutterIndicated in atrial fibrillation and atrial flutter– Used to slow ventricular responseUsed to slow ventricular response
Therapeutic serum levelsTherapeutic serum levels– Digoxin 0.5-2.2 ng/mlDigoxin 0.5-2.2 ng/ml– Digitoxin 9-25 ng/ml


Digoxin Pharmacokinetics:Digoxin Pharmacokinetics:
Variable oral absorptionVariable oral absorption– Liquid more complete and less variable than tabletsLiquid more complete and less variable than tablets
VVDD = = 6-7 L/kg6-7 L/kg
Binds strongly to proteins in extravascular spaceBinds strongly to proteins in extravascular spaceRenal excretionRenal excretion– Clearance slowed in renal dysfunctionClearance slowed in renal dysfunction– 37% excreted per day37% excreted per day
Minimal hepatic metabolism (<20%)Minimal hepatic metabolism (<20%)Half-life = 1.6 days (30-40 hours)Half-life = 1.6 days (30-40 hours)5xhalf-life to attain plateau (7 days)5xhalf-life to attain plateau (7 days)– DigitalizationDigitalization
Oral and IV administrationOral and IV administration

Digitoxin Pharmacokinetics:Digitoxin Pharmacokinetics:
Absorption almost complete (>90%)Absorption almost complete (>90%)– Less polar and more lipid soluble than DLess polar and more lipid soluble than Digoxinigoxin– Cholestyramine can alter enterohepatic cyclingCholestyramine can alter enterohepatic cycling
Elimination primarily via hepatic metabolism (>80%)Elimination primarily via hepatic metabolism (>80%)– Large capacity of the liver to metabolizeLarge capacity of the liver to metabolize– InducibleInducible
>95% bound to albumin>95% bound to albumin
VVDD = = 0.6 L/kg0.6 L/kg
Half-life = 7 daysHalf-life = 7 days– 4 weeks to reach plateau4 weeks to reach plateau
Oral administrationOral administrationOf Historical Interest: No longer availableOf Historical Interest: No longer available

Bipyridines:Bipyridines:
Inamrinone, formerly amrinoneInamrinone, formerly amrinoneMilrinone (Primacor®) Milrinone (Primacor®) – More potent, higher selectivity for PDEMore potent, higher selectivity for PDE
Phosphodiesterase III inhibitorsPhosphodiesterase III inhibitors– Results in increase in cAMPResults in increase in cAMP– Increases Increases CaCa++++ during action potential during action potential
Similar effects toSimilar effects to receptor stimulationreceptor stimulationVasodilator effects occurVasodilator effects occur
– Decreases preload and afterloadDecreases preload and afterload– Partially responsible for improved C.O.Partially responsible for improved C.O.– Little change in BPLittle change in BP
Used via IV route by continuous infusionUsed via IV route by continuous infusion

BipyridinesBipyridines

Bipyridines: Bipyridines: Inamrinone and MilrinoneInamrinone and Milrinone
Indicated for Indicated for short-termshort-term management of management of severe CHF severe CHF not not responding to digitalis, responding to digitalis, diuretics, vasodilatorsdiuretics, vasodilatorsInamrinone has not been shown to prolong Inamrinone has not been shown to prolong survival or reduce incidence of sudden survival or reduce incidence of sudden deathdeathMilrinone has been shown to Milrinone has been shown to increaseincrease mortality mortality withoutwithout definite benefit definite benefit

Bipyridines: Bipyridines:
Inamrinone metabolized by conjugative pathwaysInamrinone metabolized by conjugative pathways– tt1/21/2 2-3 hours (Milrinone = 30-60 minutes) 2-3 hours (Milrinone = 30-60 minutes)
Excreted in urine as inamrinone and metabolitesExcreted in urine as inamrinone and metabolites
Potentiate arrhythmias in high-risk patients treatedPotentiate arrhythmias in high-risk patients treated
Adverse effects:Adverse effects:– Thrombocytopenia (3% with inamrinone)Thrombocytopenia (3% with inamrinone)– Hepatic toxicityHepatic toxicity

Vasodilators in CHF:Vasodilators in CHF:
Useful in reducing preload and/or afterloadUseful in reducing preload and/or afterloadArterial dilators primarily reduce afterloadArterial dilators primarily reduce afterload– Decrease SVRDecrease SVR– Decrease impedance Decrease impedance
Venous dilators primarily reduce preloadVenous dilators primarily reduce preload– Cause increase in venous capacitanceCause increase in venous capacitance– Pooling of blood in veinsPooling of blood in veins– Decrease in venous returnDecrease in venous return– Relief of congestionRelief of congestion

Vasodilators in CHF:Vasodilators in CHF:
Organic nitratesOrganic nitrates
Direct vasodilatorsDirect vasodilators
Angiotensin-converting enzyme inhibitorsAngiotensin-converting enzyme inhibitors– Beneficial effects in the treatment and Beneficial effects in the treatment and
prevention of heart failureprevention of heart failure– Decrease morbidity and mortalityDecrease morbidity and mortality


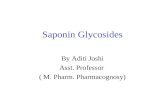
Assessment of LV Function
(Echocardiogram, Radionuclide Ventriculogram)
EF < 40%
Assessment of Volume Status
Signs and Symptoms of
Fluid Retention
Diuretic (Titrate to Euvolemic
State)
No Signs and Symptoms of Fluid
Retention
ACE Inhibitor
-Blocker
Digoxin
Recommended Approach to the Patient with Heart Failure

New VasodilatorsNew Vasodilators
Nesiritide (Natrecor®)Nesiritide (Natrecor®)– Natriuretic peptideNatriuretic peptide
Bosentan (Tracleer®)Bosentan (Tracleer®)– Endothelin receptor antagonistEndothelin receptor antagonist
Epoprostenol (Flolan®)Epoprostenol (Flolan®)– Prostacyclin (PGIProstacyclin (PGI22))

Nesiritide (Natrecor®)Nesiritide (Natrecor®)
Human B-type natriuretic peptide (hBNP)Human B-type natriuretic peptide (hBNP)– Endogenous 32-amino acid peptide hormoneEndogenous 32-amino acid peptide hormone
Structurally similar to atrial natriuretic peptide (ANP)Structurally similar to atrial natriuretic peptide (ANP)
– Manufactured from Manufactured from E. coliE. coli using recombinant DNA using recombinant DNA technologytechnology
– Binds to particulate Binds to particulate guanylate cyclaseguanylate cyclase receptor receptorVascular smooth muscleVascular smooth muscleEndothelial cellsEndothelial cells
– Increases intracellular cGMP » smooth muscle Increases intracellular cGMP » smooth muscle relaxationrelaxation
Relaxes arterial and venous tissue pre-contracted with Relaxes arterial and venous tissue pre-contracted with endothelin-1 or phenylephrineendothelin-1 or phenylephrine

Nesiritide (Natrecor®)Nesiritide (Natrecor®)
Pharmacological ActionsPharmacological Actions– HemodynamicsHemodynamics
VenodilatationVenodilatationArterial DilatationArterial DilatationCoronary Artery DilatationCoronary Artery Dilatation
– NeurohumoralNeurohumoral aldosteronealdosterone norepinephrinenorepinephrine↓ ↓ endothelinendothelin
– RenalRenalDiuresisDiuresis↑↑ GFRGFRNatriuresisNatriuresis
Lusitropic
Anti-fibrotic
Anti-remodeling

Nesiritide (Natrecor®)Nesiritide (Natrecor®)
Pharmacological ActionsPharmacological ActionsProduces dose dependent reductions in PCWP Produces dose dependent reductions in PCWP and systemic arterial pressure in patients with and systemic arterial pressure in patients with heart failureheart failure
Improves dyspneaImproves dyspnea
No effect on cardiac contractilityNo effect on cardiac contractility
No effect of conduction or refractory timesNo effect of conduction or refractory times
Indicated in acutely decompensated CHFIndicated in acutely decompensated CHF

Nesiritide (Natrecor®)Nesiritide (Natrecor®)
PharmacokineticsPharmacokinetics– IV Bolus and InfusionIV Bolus and Infusion– Biphasic disposition from plasmaBiphasic disposition from plasma
Mean terminal elimination half-life = 18 min.Mean terminal elimination half-life = 18 min.Mean initial elimination half-life = 2 min.Mean initial elimination half-life = 2 min.
– Cleared from circulation via 3 independent Cleared from circulation via 3 independent mechanismsmechanisms
Binding to cell surface clearance receptors with cellular Binding to cell surface clearance receptors with cellular internalization and lysosomal proteolysisinternalization and lysosomal proteolysisProteolytic cleavage of peptide by endopeptidaseProteolytic cleavage of peptide by endopeptidaseRenal filtrationRenal filtration

Heart Failure Management Heart Failure Management Recommendations Recommendations
Stage A (High Risk of Developing Heart Stage A (High Risk of Developing Heart Failure)Failure)– Risk-factor managementRisk-factor management
Control of hypertension, diabetes, lipid disordersControl of hypertension, diabetes, lipid disorders
– Use of ACE Inhibitor in patients with Use of ACE Inhibitor in patients with atherosclerotic heart disease, hypertension, atherosclerotic heart disease, hypertension, diabetes, or other risk factorsdiabetes, or other risk factors
– Control of ventricular rate in patients with Control of ventricular rate in patients with supraventricular tachyarrhythmiasupraventricular tachyarrhythmia
– Treatment of thyroid disordersTreatment of thyroid disorders

Heart Failure Management Heart Failure Management RecommendationsRecommendations
Stage B (Left ventricular dysfunction Stage B (Left ventricular dysfunction without symptoms)without symptoms)– Use of ACE inhibitor in patients with history of Use of ACE inhibitor in patients with history of
MI, or reduced ejection fraction regardless of MI, or reduced ejection fraction regardless of history of MIhistory of MI
– Use of Use of ββ-blocker in patients with history of MI, -blocker in patients with history of MI, or reduced ejection fraction regardless of or reduced ejection fraction regardless of history of MIhistory of MI
– Valve replacement or repair in patients with Valve replacement or repair in patients with hemodynamically important valvular diseasehemodynamically important valvular disease
– Long-term use of systemic vasodilator in Long-term use of systemic vasodilator in patients with severe aortic regurgitationpatients with severe aortic regurgitation

Heart Failure Management Heart Failure Management RecommendationsRecommendations
Stage C (Symptomatic left ventricular Stage C (Symptomatic left ventricular dysfunction)dysfunction)– Use of diuretic in patients with fluid retentionUse of diuretic in patients with fluid retention– Use of ACE inhibitor (unless contraindicated)Use of ACE inhibitor (unless contraindicated)– Use of Use of ββ-blocker (unless contraindicated)-blocker (unless contraindicated)– Use of digoxin (unless contraindicated)Use of digoxin (unless contraindicated)– Discontinuation of drugs known to affect Discontinuation of drugs known to affect
patient status adverselypatient status adverselyNSAIDNSAIDAntiarrhythmicsAntiarrhythmicsCalcium channels blockersCalcium channels blockers

Heart Failure Management Heart Failure Management RecommendationsRecommendations
Stage C (Symptomatic left ventricular Stage C (Symptomatic left ventricular dysfunction)dysfunction)– Use of spironolactone in patients with Class IV Use of spironolactone in patients with Class IV
symptoms, preserved renal function, normal potassium symptoms, preserved renal function, normal potassium levelslevels
– Exercise (rehabilitation)Exercise (rehabilitation)– Use of angiotensin II receptor blocker in patients Use of angiotensin II receptor blocker in patients
treated with digoxin, diuretic, or treated with digoxin, diuretic, or ββ-blockers who cannot -blockers who cannot tolerate ACE inhibitors (cough/angioedema)tolerate ACE inhibitors (cough/angioedema)
– Use of hydralazine-nitrate combinationsUse of hydralazine-nitrate combinations– Addition of angiotensin II receptor blocker to ACE Addition of angiotensin II receptor blocker to ACE
inhibitorinhibitor

BosentanBosentan
Indicated for pulmonary hypertensionIndicated for pulmonary hypertension
Approved Nov. 20, 2001Approved Nov. 20, 2001
Endothelin-1 receptor antagonistEndothelin-1 receptor antagonist– Binds to ETBinds to ETAA and ET and ETBB receptors receptors
– Specific and competitive antagonistSpecific and competitive antagonist– Located in endothelium and vascular smooth muscleLocated in endothelium and vascular smooth muscle– ET-1 levels increased in PAH suggesting pathogenic ET-1 levels increased in PAH suggesting pathogenic
role for ET-1role for ET-1

BosentanBosentan
PharmacokineticsPharmacokinetics– Oral administrationOral administration
50% bioavailable50% bioavailable
Unaffected by foodUnaffected by food
– Highly protein bound (albumin)Highly protein bound (albumin)– 3 metabolites, 1 active contributing to 10-20% of 3 metabolites, 1 active contributing to 10-20% of
effecteffect– Inducer of CYP2C9 and CYP3A4Inducer of CYP2C9 and CYP3A4– Eliminated by biliary excretion and hepatic Eliminated by biliary excretion and hepatic
metabolismmetabolism

BosentanBosentan
Pregnancy category XPregnancy category X– Teratogenic in ratsTeratogenic in rats– Pregnancy should be excluded before start of Pregnancy should be excluded before start of
treatmenttreatment
May impair fertilityMay impair fertility
HepatotoxicHepatotoxic
Carcinogenic in miceCarcinogenic in mice