Cardiac arrest during surgery and ventilation in the prone position: a case report and systematic...
6
Resuscitation 50 (2001) 233 – 238 Case report Cardiac arrest during surgery and ventilation in the prone position: a case report and systematic review Julian Brown a , James Rogers b , Jasmeet Soar a, * a Aneasthetics Department, Southmead Hospital, North Bristol NHS Trust, Bristol BS10 5NB, UK b Frenchay Hospital, North Bristol NHS Trust, Bristol BS16 1LE, UK Received 14 June 2000; received in revised form 20 July 2000; accepted 19 March 2001 Abstract We present a case report of successful resuscitation following cardiac arrest in a patient undergoing surgery in the prone position. A systematic review of the literature identified 22 further cases. Risk factors for intra-operative cardiac arrest in patients in the prone position include: cardiac abnormalities in patients undergoing major spinal surgery, hypovolaemia, air embolism, wound irrigation with hydrogen peroxide, poor positioning and occluded venous return. Cardiac arrest is also a risk in the increasing number of patients with acute respiratory distress syndrome ventilated in the prone position. Management of prone cardiac arrest may be improved by identification of high-risk patients, careful patient positioning, use of invasive monitoring and placement of self-adhesive defibrillator paddles. Suitable techniques for cardiopulmonary resuscitation including methods for chest compression, defibrillation and the management of air embolism are discussed. © 2001 Elsevier Science Ireland Ltd. All rights reserved. Keywords: Cardiac arrest; Surgery; Prone position; Resuscitation Resumo Apresentamos um caso clı ´nico de uma reanimac ¸a ˜o com sucesso de um doente com paragem cardı ´aca no decurso de cirurgia quando estava em decu ´ bito ventral. Os factores de risco para paragem cardı ´aca intra-operato ´ ria nos doentes em decu ´ bito ventral incluem: cardiopatia em doentes submetidos a cirurgia major da coluna, hipovolemia, embolia gasosa, irrigac ¸a ˜o da ferida com pero ´ xido de hidroge ´nio, mau posicionamento e obstruc ¸a ˜o do retorno venoso. A paragem cardı ´aca e ´ tambe ´m um risco no nu ´ mero crescente de doentes com ARDS ventilados em decu ´ bito ventral. A abordagem da paragem cardı ´aca em pronac ¸a ˜o pode ser melhorada identificando os doentes de alto risco, posicionando os doentes cuidadosamente, utilizando monitorizac ¸a ˜o invasiva e colocando pa ´s auto-adesivas de desfibrilhador. Sa ˜o discutidas as te ´cnicas disponı ´veis para reanimac ¸a ˜o cardio-pulmonar incluindo me ´todos de compressa ˜o tora ´cica, desfibrilhac ¸a ˜o e abordagem da embolia gasosa. © 2001 Elsevier Science Ireland Ltd. All rights reserved. Palaras chae: Paragem cardı ´aca; Cirurgia; Posic ¸a ˜o de pronac ¸a ˜o; Ressuscitac ¸a ˜o www.elsevier.com/locate/resuscitation 1. Introduction The prone position allows access for surgery [1,2]. In the intensive care unit, patients with acute respiratory distress syndrome (ARDS) are increasingly being venti- lated in the prone position [3,4]. Cardiac arrest in these patients is difficult to manage as poor access makes cardiopulmonary resuscitation (CPR) and defibrillation difficult. These difficulties can be further exacerbated in the surgical patient with an open wound, protruding surgical metal work and an unstable spine. There are few case reports of such arrests and few guidelines as to * Corresponding author. Tel.: +44-117-9595114; fax: +44-117- 9595075. E-mail address: [email protected] (J. Soar). 0300-9572/01/$ - see front matter © 2001 Elsevier Science Ireland Ltd. All rights reserved. PII:S0300-9572(01)00362-8
-
Upload
julian-brown -
Category
Documents
-
view
216 -
download
1
Transcript of Cardiac arrest during surgery and ventilation in the prone position: a case report and systematic...

Resuscitation 50 (2001) 233–238
Case report
Cardiac arrest during surgery and ventilation in the proneposition: a case report and systematic review
Julian Brown a, James Rogers b, Jasmeet Soar a,*a Aneasthetics Department, Southmead Hospital, North Bristol NHS Trust, Bristol BS10 5NB, UK
b Frenchay Hospital, North Bristol NHS Trust, Bristol BS16 1LE, UK
Received 14 June 2000; received in revised form 20 July 2000; accepted 19 March 2001
Abstract
We present a case report of successful resuscitation following cardiac arrest in a patient undergoing surgery in the proneposition. A systematic review of the literature identified 22 further cases. Risk factors for intra-operative cardiac arrest in patientsin the prone position include: cardiac abnormalities in patients undergoing major spinal surgery, hypovolaemia, air embolism,wound irrigation with hydrogen peroxide, poor positioning and occluded venous return. Cardiac arrest is also a risk in theincreasing number of patients with acute respiratory distress syndrome ventilated in the prone position. Management of pronecardiac arrest may be improved by identification of high-risk patients, careful patient positioning, use of invasive monitoring andplacement of self-adhesive defibrillator paddles. Suitable techniques for cardiopulmonary resuscitation including methods for chestcompression, defibrillation and the management of air embolism are discussed. © 2001 Elsevier Science Ireland Ltd. All rightsreserved.
Keywords: Cardiac arrest; Surgery; Prone position; Resuscitation
Resumo
Apresentamos um caso clınico de uma reanimacao com sucesso de um doente com paragem cardıaca no decurso de cirurgiaquando estava em decubito ventral. Os factores de risco para paragem cardıaca intra-operatoria nos doentes em decubito ventralincluem: cardiopatia em doentes submetidos a cirurgia major da coluna, hipovolemia, embolia gasosa, irrigacao da ferida comperoxido de hidrogenio, mau posicionamento e obstrucao do retorno venoso. A paragem cardıaca e tambem um risco no numerocrescente de doentes com ARDS ventilados em decubito ventral. A abordagem da paragem cardıaca em pronacao pode sermelhorada identificando os doentes de alto risco, posicionando os doentes cuidadosamente, utilizando monitorizacao invasiva ecolocando pas auto-adesivas de desfibrilhador. Sao discutidas as tecnicas disponıveis para reanimacao cardio-pulmonar incluindometodos de compressao toracica, desfibrilhacao e abordagem da embolia gasosa. © 2001 Elsevier Science Ireland Ltd. All rightsreserved.
Pala�ras cha�e: Paragem cardıaca; Cirurgia; Posicao de pronacao; Ressuscitacao
www.elsevier.com/locate/resuscitation
1. Introduction
The prone position allows access for surgery [1,2]. Inthe intensive care unit, patients with acute respiratory
distress syndrome (ARDS) are increasingly being venti-lated in the prone position [3,4]. Cardiac arrest in thesepatients is difficult to manage as poor access makescardiopulmonary resuscitation (CPR) and defibrillationdifficult. These difficulties can be further exacerbated inthe surgical patient with an open wound, protrudingsurgical metal work and an unstable spine. There arefew case reports of such arrests and few guidelines as to
* Corresponding author. Tel.: +44-117-9595114; fax: +44-117-9595075.
E-mail address: [email protected] (J. Soar).
0300-9572/01/$ - see front matter © 2001 Elsevier Science Ireland Ltd. All rights reserved.PII: S 0 3 0 0 -9572 (01 )00362 -8

J. Brown et al. / Resuscitation 50 (2001) 233–238234
how to manage them. Current methods of CPR aregeared towards supine patients. We describe a casereport of cardiac arrest due to ventricular fibrillationduring surgery in the prone position. We discuss riskfactors and suitable techniques for the management ofpatients with cardiac arrest whilst ventilated in the proneposition.
2. Case report
A 60-year-old female patient (weight 67 kg), under-went thoracic spine decompression surgery for an inva-sive tumour between the T-11 and L-1 vertebral levels.The patient had no other past medical history of noteand no abnormalities in pre-operative investigations.
Anaesthesia was induced with intravenous propofol,fentanyl and rocuronium. The patient was ventilatedwith oxygen, nitrous oxide and isoflurane via a rein-forced 8 mm tracheal tube. Invasive arterial and centralvenous pressures were monitored. The patient wasplaced horizontally into the prone position supported onblocks placed under the upper chest and pelvis. Thepatient’s arms were positioned above her head. Thepatient’s abdomen was allowed to hang freely.
Surgery was prolonged and associated with markedblood loss from epidural veins. Intravenous fluids, andblood were administered to keep the patient haemody-namically stable (pulse 60–70 beats/min, systolic bloodpressure 100–120 mmHg). After 9 h, there was a suddenfall in the patient’s end tidal carbon dioxide levelfollowed by a rapid fall in blood pressure. The electro-cardiograph (ECG) changed from sinus rhythm to abroad complex tachycardia. This deteriorated to a pulse-less ventricular tachycardia. Venous air embolism wasthe suspected cause of cardiac arrest. The surgeonflooded the surgical field with normal saline to prevententrainment of further air into an open epidural vein.The nitrous oxide was turned off and the patient venti-lated with 100% oxygen.
Access for defibrillation was difficult. The fully drapedpatient had an open surgical wound, which was bleedingprofusely and had protruding surgical metalwork. Thepatient also had an unstable spine. It was possible withsome difficulty for a single operator to position defibril-lator paddles in the patient’s right axilla and left apex.A single 200 J DC shock successfully defibrillated thepatient to a sinus tachycardia. Postarrest, the patientrequired increments of epinephrine totalling 1 mg andfluid boluses before cardiovascular stability returned.
Surgery was completed 5 h later. The patient wassedated and ventilated over night and extubated un-eventfully the next day. The patient made a full recoverywith no evidence of cerebral or myocardial injury.
3. Systematic review
3.1. Methods
We conducted a literature search using the MEDLINE
database between 1966 and December 1999 for allpublications in any language. The MeSH search head-ings ‘prone’, ‘spinal’, ‘resuscitation’, ‘cardiac’ and ‘ar-rest’ were used. Abstracts were used to identify relevantarticles. The reference lists of all the identified articleswere also used to capture any articles not identified bythe MEDLINE search.
3.2. Results
We identified 16 suitable articles [5–20] for inclusionin the systematic review (Table 1), which contained 22case reports of CPR in prone positioned patients. Onearticle describes an intensive care patient [17]. Twofurther articles discuss techniques for prone CPR [21,22].
4. Review of literature
Cardiac arrest during surgery in the prone position israre judging from the scarcity of case reports. Themajority of cases describe successful outcomes. Publica-tion bias towards good outcome may underestimate thefrequency of prone cardiac arrest. Interestingly most ofthe survivors are in the more recently published casereports (Table 1). Publication bias will also have had aninfluence on what is published as more extreme cases arelikely to be published [23].
4.1. Pre-operati�e risk factors
The majority of reports have occurred in patientshaving complex spinal and neurological surgery. Youngpatients with congenital spinal abnormalities may haveco-existing cardio-respiratory disease (e.g. Duchennemuscular dystrophy (DMD) [24] or Marfan’s syndrome[25]) and this may predispose to arrest during surgery.
4.2. Intra-operati�e factors
Airway problems are difficult to manage in the pronepatient and can result in cardiac arrest secondary tohypoxaemia [11,14]. Prone positioning can result incompression of the trachea and the tracheal tube inpatients with spinal deformity [14,26]. Tracheobronchialcompression against the vertebral bodies can occur inpatients with severe thoracic lordoscoliosis on pronepositioning. The laryngeal mask airway may be a lifesav-ing option if there is dislodgement of the tracheal tubein the prone patient. It can be rapidly inserted in theprone patient without laryngoscopy [27].

J.B
rown
etal./
Resuscitation
50(2001)
233–
238235
Table 1
AetiologyReferences RhythmAge OutcomeSex Diagnosis Type of surgery Rapid blood loss
Not known ? SurvivedCraniotomy NoEpendymoma?Child[5]Craniotomy Yes GI haemorrhage ? DiedChild ? Medulloblastoma
Retroperitoneal haemorrhage ? DiedYesChild Burr holesMultiple trauma?YesChild ? ? Died? Scoliosis Scoliosis[6]
Scoliosis ? ? ? Died?[7] Scoliosis16Scoliosis Yes Air embolism ?Duchenne[8] Male16
musculardystrophy
? Air embolism ?Idiopathic DiedScoliosisFemale18[9]scoliosis
? Air embolism ? Diedmale Congenital15 Scoliosisscoliosis
Air embolism, air in coronary arteries, probeNo PEA DiedLaminectomy[10] 40 Disc prolapseMaleclosed FO
40 No Air embolism, air in coronary arteries Asystole DiedMale Disc prolapse Laminectomy14 Yes Retractor PEA SurvivedFemale Head injury[11] Craniotomy
Blocked ETT VF SurvivedNoMale Cervical trauma34 LaminectomyYes53 Air embolism Asystole SurvivedFemale Meningioma Craniotomy[12]
[13] Scoliosis Yes ? hypovolaemia Asystole Survived12 Male Spasticquadroplegia
[14] NoFemale Tracheal obstruction due to anatomicalThoracic PEA Survived15 Scoliosiscompressionlordoscoliosis
Yes Air embolism AsystoleAchondroplasia Survived[15] 6 Craniotomy for congenital cervical cordFemalecompression
Male Scoliosis No Hypovolaemia, coronary ischaemia PEA Survived[16] Marfan’s valve15disease
Prone ICU ventilation No ? Asystole Survived[17] 48 Male PneumoniaYes Air embolism, air in LV, closed FO Asystole DiedScoliosisMuscularFemale[18] 8
dystrophy12 Yes Air embolism Asystole DiedFemale Cerebral palsy Scoliosis
Scoliosis[19] YesDuchenne Cardiomyopathy VF SurvivedMale15musculardystrophy
Hydrogen peroxide irrigation and oxygenScoliosis ? DiedKyphoscoliosis No[20] 15 Femaleembolism

J. Brown et al. / Resuscitation 50 (2001) 233–238236
Spinal surgery can be associated with unexpectedblood loss causing hypovolaemia which may itself causecardiac arrest in susceptible patients.
The prone position [1] may exacerbate hypovolaemiaby further reducing venous return and cardiac output.Patients undergoing spinal or posterior fossa surgeryare at risk from gas embolism from two sources: airentrainment and oxygen released from hydrogen perox-ide used for wound irrigation. The clinical effects of airemboli depend on the volume and rate of embolisation[28].
Venous entrainment of air is more likely with lowervenous pressures and when the operative site is abovethe level of the heart [10] as occurs in the proneposition. Venous emboli from any source will tend toexpand with the presence of nitrous oxide [29,30] andshrink with the use of high inspired oxygen concentra-tions. In addition to the effects of venous emboli,patients may be at risk of paradoxical embolisationfrom the venous to the systemic arterial circulation. Amuch smaller volume of gas may have more profoundeffect in either the cerebral or coronary circulations [31]and coronary gas bubbles were found at postmortem intwo of the cases in our series [10]. Paradoxical gasembolism can occur through a patent foramen ovale,which is relatively common 10–30% [32,33] or in thecase of massive embolism in the absence an intra-car-diac shunt.
Cardiac arrhythmias can occur during neurosurgerywith both brain stem manipulation and raised intra-cra-nial pressure as predisposing factors.
A combination of factors was most likely to havecontributed to cardiac arrest in our case report. Venousair embolism in a patient suffering massive blood lossseems to have been the most likely cause.4.3. Management of prone cardiac arrest
In the event of cardiac arrest, resuscitation shouldproceed according to standard protocols. The key areasto consider in prone patients are monitoring and recog-nition of pre-arrest signs, a system for cardiac compres-sions, a technique for defibrillation and the specificmanagement of gas embolism.
Monitoring allows early detection of problems so thatprompt action can be taken. Invasive arterial monitor-ing allows beat by beat measurement of blood pressureand rapid detection of the changes, which may precedecardiac arrest. During CPR the arterial waveform givesan indication of the effectiveness of cardiac compres-sions. Central venous pressure monitoring will help toindicate the volume status of the patient and centralvenous catheters can be used to aspirate air emboli [34].Capnography is now used and a fall in end tidal CO2
(in the expired gas) is an early sign of gas embolism.Transoesophageal echocardiography permits early de-tection of gas embolism.
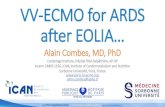
Fig. 1. Reproduced with permission from Ref. [13].
Cardiopulmonary resuscitation : In the event of car-diac arrest, it is essential to start basic life support assoon as possible.
Resuscitation may have to occur in the prone posi-tion if it is not possible to turn the patient. In our case,where surgery was ongoing, it was not been feasible toturn the patient as there was an open wound, ongoingblood loss, unstable spine and protruding metal work.Turning a patient requires several helpers, a trolley,removal of surgical drapes and care to avoid the dis-lodgement of tubes, lines and monitoring cables. Resus-citation therefore needs to start in the prone positionwhilst arrangements are made to turn the patient.
In the prone position, cardiac compression will haveto take place from the back avoiding the surgical field.Several techniques of closed cardiac compression havebeen described, either one or two handed and with[11,17] or without [13] counter pressure on the sternum(Figs. 1 and 2). It may be possible to use open cardiaccompression if there is already a thoracotomy thatallows access to the heart [19].
Fig. 2. Reproduced with permission from Ref. [17].

J. Brown et al. / Resuscitation 50 (2001) 233–238 237
Defibrillation requires an electrical current to bepassed through the heart and a critical mass of my-ocardium to be depolarised, with success decreasingwith increasing delay. Correct positioning of defibrilla-tor paddles may be difficult and potentially dangerousin the prone patient with both single and dual operatortechniques described. We would advocate prior place-ment of self-adhesive pads in the high-risk patient.
The decision as to whether to continue surgery willbe dictated by the nature and duration of cardiacarrest. Surgery may have to be continued to stem severehaemorrhage as in our case.
Management of air embolism during surgery relies onearly detection and prevention of further air entrain-ment by flooding the wound with saline and closure ofopen veins. Positioning in the left lateral and headdown position has been advocated [35] but is difficult inthe prone surgical patient. Cardiac compressions havebeen shown to be effective in pushing air from thepulmonary artery into smaller vessels [36] where, mi-crobubbles are rapidly resorbed [37]. A more directapproach of management is the removal of air from theright heart either percutaneously or via a central venouscatheter. A central venous catheter should therefore bein place in patients having prone surgery where there isrisk of large blood loss and air embolism.
5. Conclusions
Cardiac arrest in patients undergoing surgery in theprone position is rare. Pre-operative risk factors includepre-existing cardiac disease. Intra-operative factors in-clude haemorrhage, gas embolism and diminishedvenous return to the heart. Management of pronecardiac arrest may be improved by identification ofhigh-risk patients, careful patient positioning, use ofinvasive monitoring and placement of self-adhesivedefibrillator paddles. Successful methods for cardiaccompressions and defibrillation have been described inthe patient in the prone position but it may be neces-sary to turn the patient supine if initial resuscitationefforts in the prone position fail.
References
[1] Anderton JM. The prone position for the surgical patient: ahistorical review of the principles and hazards. Br J Anaesth1991;67:452–63.
[2] Graftieaux JP, Ades P, Gomis P, Barre J, Leon A. Etude desposition operatoires pour la chirurgie de la hernie discale lom-baire. Ann Francaise d Anesthesie et de Reanimation1993;12:575–81.
[3] Flaatten H, Aardal S, Hervoy O. Improved oxygenation usingthe prone position in patients with ARDS. Acta AnaesthesiolScand 1998;42(3):329–34.
[4] Blanch L, Mancebo J, Perez M, Martinez M, Mas A, BetbeseAJ, et al. Short-term effects of prone position in critically illpatients with acute respiratory distress syndrome. Intensive CareMed 1997;23(10):1033–9.
[5] Humphreys RP, Creighton EB, Hendrick EB, Hoffman HJ.Advantages of the prone position for neurosurgical procedureson the upper cervical spine and posterior cranial fossa in chil-dren. Child’s Brain 1975;1:325–36.
[6] Winter RB, Moe JH, Lonstein JE. Posterior spinal arthrodesisfor congenital scoliosis. An analysis of the cases of two hundredand ninety patients, five to nineteen years old. J Bone Joint SurgAmer 1984;66(8):1188–97.
[7] Daher YH, Lonstein JE, Winter RB, Moe JH. Spinal deformitiesin patients with arthrogryposis. A review of 16 patients. Spine1985;10(7):609–13.
[8] Lang SA, Duncan PG, Dupius PR. Fatal air embolism in anadult with Duchenne muscular dystrophy during Harringtoninstrumentation. Anaesth Analg 1989;69:132–4.
[9] McCarthy RE, Lonstein JE, Mertz JD, Kuslich SD. Air em-bolism in spinal surgery. J Spinal Disorders 1990;3:1–5.
[10] Albin MS, Ritter RR, Pruett CE, Kalff K. Venous air embolismduring lumbar laminectomy in the prone position: report ofthree cases. Anaesth Analg 1991;73:346–9.
[11] Sun W, Huang F, Kung K, Fan S, Chen T. Successful Car-diopulmonary resuscitation of two patients in the prone positionusing reversed precordial compression. Anesthesiology1992;77(1):202–4.
[12] Loewenthal A, De Albuquerque AM, Lehmann-Meurice C, Ot-teni JC. Efficacite du massage cardiaque externe chez une pa-tiente en decubitus ventral. Ann Francaise d Anesthesie et deReanimation 1993;12:587–9.
[13] Tobias JD, Gregory AM, Atwood R, Gurwitz GS. Intraopera-tive Cardiopulmonary resuscitation in the prone position. JPaediat Surg 1994;29(12):1537–8.
[14] Bagshaw ONT, Jardine A. Cardiopulmonary complications dur-ing anaesthesia and surgery for severe thoracic lordoscoliosis.Anaesthesia 1995;50:890–2.
[15] Kehller A, Mackersie A. Cardiac arrest and resuscitation of a 6month old achondroplastic baby undergoing neurosurgery in theprone position. Anaesthesia 1995;50:348–50.
[16] Gueugniaud PY, Muchada R, Bertin-Maghit M, Griffith N,Petit P. Non invasive continuous haemodynamic PET CO2 mon-itoring during perioperative cardiac arrest. Can J Anaesth1995;42(10):910–3.
[17] Dequin P-F, Hazouard E, Legras A, Lanotte R, Perrotin D.Cardiopulmonary resuscitation in the prone position: kouwen-hoven revisited. Intensive Care Med 1996;22:1272.
[18] Sutherland RW, Winter RJ. Two cases of fatal air embolism inchildren undergoing scoliosis surgery. Acta Anaesthesiol Scand1997;41(8):1073–6.
[19] Reid JM, Appleton PJ. A case of ventricular fibrillation in theprone position during back stabilisation surgery in a boy withDuchenne’s muscular dystrophy. Anaesthesia 1999;54:364–7.
[20] Lopez LM, Traves N, Napal M. Fatal gas embolism duringcorrective surgery for scoliosis using the posterior approach. RevEsp Anestesiol Reanim 1999;46:267–70.
[21] Woo-Ming MO. Cardiopulmonary resuscitation in the proneposition in small children. West Ind Med J 1966;15:197–201.
[22] McNeil EL. Prone CPR aboard an aircraft (McNeil method). JEmerg Nursg 1994;20(6):446.
[23] Easterbrooke PJ, Berlin JA, Gopalan R, Matthews DR. Publica-tion bias in clinical research. Lancet 1991;337:867–72.
[24] Morris P. Duchenne muscular dystrophy: a challenge for theanaesthetist. Paediat Anaesth 1997;7:1–4.
[25] Mesrobian RB, Epps JL. Midtracheal obstruction after Harring-ton rod placement in a patient with Marfan’s syndrome. AnesthAnalg 1986;65:411–3.

J. Brown et al. / Resuscitation 50 (2001) 233–238238
[26] Beals RK, Robbins JR, Rolfe B. Anomalies associated withvertebral malformations. Spine 1993;18(10):1329–32.
[27] McCaughey W, Bhanumurthy S. Laryngeal mask placement inthe prone position. Anaesthesia 1993;48:1104–5.
[28] Adornato DC, Gildenberg PL, Ferrario CM. Pathophysiology ofintravenous air embolism in dogs. Anesthesiology1978;49(2):120–7.
[29] Presson RG, Kirk KR, Haselby KA, Wagner WW. Effect ofventilation with soluble and diffusible gases on the size of airemboli. J Appl Physiol 1991;70(3):1068–74.
[30] Kytta J, Tanskanen P, Randell T. Comparison of the effects ofcontrolled ventilation with 100% oxygen, 50% oxygen in nitro-gen, and 50% nitrous oxide on responses to venous air embolismin pigs. Br J Anaesth 1996;77(5):658–61.
[31] Spencer FC, Rossi NP, Yu SC, Koepke JA. The significance ofair embolism during cardiopulmonary bypass. J Thoracic Car-diovasclar Surg 1965;49:615–34.
[32] Hagan PT, Scolz DG, Edwards WD. Incidence and size ofpatent foramen ovale during the first 10 decades of life: anautopsy study of 965 normal hearts. Mayo Clinic Proceedings1984;59(1):17–20.
[33] Fisher DC, Fisher EA, Budd JH, Rosen SE, Goldman ME. Theincidence of patent foramen ovale in 1000 consecutive patients.A contrast transoesophageal echocardiography study. Chest1995;107(6):1504–9.
[34] Orebaugh SL. Venous air embolism: clinical and experimentalconsiderations. Crit Care Med 1992;20(8):1169–77.
[35] Durant TM, Long, Oppenheimer MJ. Pulmonary venous airembolism. Amer Heart J 1947;33:269–81.
[36] Ericsson JA, Gottlieb JD, Sweet RB. Closed-chest cardiac mas-sage in the treatment of venous air embolism. New Eng J Med1964;270:1353–4.
[37] Presson RG, Kirk KR, Haselby KA, Linehan JA, Zaleski S,Wagner WW. Fate of air emboli in the pulmonary circulation. JAppl Physiol 1989;67(5):1898–902.



![Prone ventilation reduces mortality in patients with acute … · · 2017-08-25prone position, first suggested in 1974 [8], optimizes both lung recruitment and ventilation–perfusion](https://static.fdocuments.net/doc/165x107/5ed80d13cba89e334c672734/prone-ventilation-reduces-mortality-in-patients-with-acute-2017-08-25prone-position.jpg)












