Candidiasis Jarrod Fortwendel, PhD Department of Microbiology and Immunology...
22
-
Upload
lucas-simpson -
Category
Documents
-
view
218 -
download
0
Transcript of Candidiasis Jarrod Fortwendel, PhD Department of Microbiology and Immunology...

Candida: The most common yeast pathogen of man
• Candida is the 4th most common blood-isolate– i.e., common fungal infection of the circulatory system!
• Candida is a small, thin-walled, ovoid yeast– Measures 4-6 µm in diameter– Reproduces via budding
• Candida species generally occur in 3 forms in tissue:– Blastospores– Pseudohyphae– Hyphae
From left to right - C. albicans yeast colonies, budding yeast (blastospores), and budding yeast interspersed with hyphae and pseudohyphae.

Candida: The human commensal
• The genus Candida encompasses > 150 species:– Only a few are human pathogens:
• C. albicans• C. guilliermondii• C. krusei• C. parapsilosis• C. tropicalis• C. kefyr• C. lusitaniae• C. dubleniensis• C. glabrata
These organisms are ubiquitous in nature and are found as normal human commensals
As commensals, Candida species inhabit the mouth, oropharynx, GI tract, female genital tract and the skin

Candidiasis (Candida infection)• Epidemiology:
– Because they are human commensals, the source of infection is usually endogenous
– Although Candida infections have been recorded since antiquity, infections have become more common due to modern therapeutics
– Candida is now among the most common nosocomial pathogens
– Predisposing conditions for candidiasis are: • 1) Antibacterial therapy (#1 cause of Candidiasis!)
– Destroys normal flora balance allowing Candida to “take over”– Women can often develop vaginal candidiasis on antibacterial therapy
• 2) Indwelling devices (intravascular or urinary) • 3) Altered immune status – e.g., HIV, diabetes, neutropenia• 4) Abdominal and thoracic surgery• 5) Immunosuppressive / cytotoxic therapy

Candidiasis
• C. albicans is the most common etiologic agent of candidiasis
• However, the use of effective antifungal therapies has caused a shift towards non-albicans infections– Non-albicans species now account for almost half of all
Candida blood infections (candidemia)
• This change is clinically important as the various species differ in susceptibility to antifungal agents

Virulence of Candida species
• Candida virulence factors: – Ability to grow at 37°C.– Ability to adhere to host tissues– The yeast-to-hyphal transition (“phenotypic switching”)
• The change from blastospore to pseudohyphal and hyphal stages is generally considered integral to the organism’s penetration into host tissue
• HOWEVER, C. glabrata is associated with extensive infection even through it does not form pseudohyphae or hyphae

Pathogenesis of Candidiasis
• Innate immunity is most important for defense against hematogenous dissemination– Neutrophil is the most important component– Anti-Candida antibodies are produced, but their role in
defense against the organism is unclear
• In the most serious form, Candida disseminates hematogenously and forms microabcesses in major organs– Probably enters bloodstream from mucosal surfaces
where overgrowth has occurred– May enter from the skin

Candidiasis – Clinical AspectsCandidiasis – Clinical Aspects• Clinical Manifestations:
– Severity is largely dependent on immune status of host– In right setting – can cause disease in any organ system– 3 major groups of candidiasis (examples on following slides):
1. Mucocutaneous candidiasis– Cutaneous lesions – skin, nails, intertrigenous areas– Mucous membrane infections – thrush, vaginitis, balanitis– Chronic mucocutaneous candidiasis (CMCC)
2. Deeply invasive candidiasis– Disseminated form affects lungs, kidneys, heart, spleen and others…
3. Candidemia

Mucocutaneous Candidiasis: Cutaneous lesions
2. Intertrigo – erythematous irritation with redness and pustules in the skin folds1. Erosio interdigitalis blastomycetica–
infection between the digits of the hands or feet
3. Folliculitis – pustules developing in the area of the beard (not pictured)

Mucocutaneous Candidiasis:Cutaneous lesions
4. Paronychia (painful swelling at the nail-skin interface) with onychomycosis (fungal nail infection rarely caused by Candida)

Mucocutaneous Candidiasis: Mucous Membrane Infections
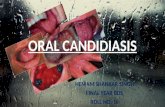
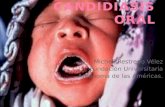
5. Oral thrush – white, adherent, painless, discrete or confluent patches in the mouth, tongue, or esophagus with fissuring at the corners of the mouth.
**Occurrence of thrush in a young, otherwise healthy appearing person should prompt an investigation for underlying conditions affecting the immune system (i.e., HIV)**

Mucocutaneous Candidiasis: Mucous Membrane Infections
6. Vulvovaginal candidiasis - can be accompanied by puritis, pain, and vaginal discharge
7. Perianal candidiasis - puritic, erythematous, pustular infections surrounding the anus
8. Balanitis- erythematous-pustular infections of the glans penis
9. Diaper rash – common erythematous-pustular perineal infection in infants

Mucocutaneous Candidiasis:Chronic Mucocutaneous Candidiasis
CMCC :
-Heterogenous infection of the hair, skin nails and mucous membranes that persist despite therapy
-May be mild or severely disfiguring
-Usually associated with immunologic dysfunction (T-lymphocyte failure to proliferate in response to Candida)

Deeply Invasive Candidiasis
• Deeply invasive candidiasis is commonly the result of hematogenous seeding of various organs as a complication of candidemia (Candida blood infection)
• Candida gains access to the intravascular compartment and spreads hematogenously to brain, chorioretina, heart, kidneys, liver, spleen, endocrine glands, pancreas, heart valves, skeletal muscle, joints, bone, meninges…

Deeply Invasive CandidiasisTwo classic presentations in deeply invasive candidiasis (examples on
next slide):
1. Macronodular skin lesions – Candida can be cultured from the lesions and sometimes seen in prepared biopsies. Painful muscular involvement is also evident beneath affected skin
2. Endophthalmitis – lesion composed mainly of inflammatory cells, may progress to cause loss of the eye, ocular examination is indicated for all patients will candidemia
Chorioretinal and skin involvement are highly significant as both are associated with high probability of abscess formation in deep tissues

Deeply Invasive Candidiasis
Macronodular skin lesions associated with
hematogenously disseminated Candida
Hematogenous Candida endophthalmitis – classic off-white lesion projecting from
the chorioretina into the vitreous causes the surrounding haze

Candidemia
• Candidemia = isolation of Candida from one or more blood specimens
– Associated with high morbidity and mortality
– Although it used to be disputed, current practice dictates that all patients with candidemia should receive antifungal therapy

Candidemia
• Candidemia has become one of the most important nosocomial infections over the last 2 decades
• C. albicans is most common, followed by:– C. troplicalis– C. glabrata– C. parapsilosis (mainly in neonatal settings)
• Clinical manifestations range from fever to overt and life-threatening sepsis

Candidemia
• Treatment of candidemia has 2 elements:
1. Most likely source of fungemia should be identified and treated– In a non-neutropenic patient, an intravascular catheter is the most
likely source and removal of the catheter is often valuable– Other common sources: urinary tract and localized infections
2. Antifungal agent should be employed– Amphotericin B or fluconazole for critically ill patients (never in
combination therapy as they are antagonistic)

Candidiasis – Laboratory Diagnosis
• Laboratory Diagnosis:– Established via visualization of pseudohyphae or hyphae on direct prep:
• KOH prep (with calcofluor white)• Gram’s stain• Periodic Acid-Schiff (PAS) stain• Gimori Methenamine Silver (GMS) stain of infalmmed tissue
“Sausage-shaped” pseudohyphae and true hyphae with septa
***Remember that these are pathogenic forms***

Candidiasis – Laboratory Diagnosis
• Laboratory diagnosis:– Lab culture of Candida:
• Yeast cells with single buds only• Routine culture and sensitivity: Candida will grow on Sheep Blood Agar
(SBA) within 24 hr forming a “staph-like” colony• Fungal culture: SDA positive within 48-72 hr
SBA SDA

Candidiasis – Laboratory Diagnosis
• Speciation achieved via biochemical tests and selective agar:– CHROMagar generates Candida colonies with species-specific colors
– Germ tube test – C. albicans will form germ tubes (the beginning of true hyphal development) under specific culture conditions
– Sugar assimilation tests and the differentiation of developmental structures in culture are also used for speciation of Candida
C. albicans is blue/green
germ tubes