
Cancer Medicine Approval In NHS North East Steve Williamson Consultant Pharmacist Northern Cancer...
26
Cancer Medicine Cancer Medicine Approval In NHS North Approval In NHS North East East Steve Williamson Steve Williamson Consultant Pharmacist Consultant Pharmacist Northern Cancer Network Northern Cancer Network & & Northumbria Healthcare NHS Northumbria Healthcare NHS Trust Trust
-
Upload
lenard-reynolds -
Category
Documents
-
view
225 -
download
0
Transcript of Cancer Medicine Approval In NHS North East Steve Williamson Consultant Pharmacist Northern Cancer...
Cancer Medicine Approval Cancer Medicine Approval In NHS North EastIn NHS North East
Steve WilliamsonSteve WilliamsonConsultant PharmacistConsultant Pharmacist
Northern Cancer NetworkNorthern Cancer Network&&
Northumbria Healthcare NHS TrustNorthumbria Healthcare NHS Trust

North Of England Cancer Drug North Of England Cancer Drug Approvals GroupApprovals Group
Who are we?Who are we?
What are we doing? What are we doing?
What Lessons have we learnt?What Lessons have we learnt?
What Challenges do we What Challenges do we allall face? face?
Introducing new cancer drugs -Introducing new cancer drugs -How to get it rightHow to get it right
Resources limited, money, staff to make & give chemo
Cancer drugs have readily identifiable costs and benefits
Can’t have everything, Decisions have to be made Is the drug clinically effective?
Is the drug cost effective?
Can the local healthcare economy afford the budget impact?
Balance tensions between efficiency and equity
Must ensure consistency of approach
Must assess each drugs case on its own merits
Cancer Drug Approvals in the UKCancer Drug Approvals in the UK
NICENICE
SMCSMC
AWMSGAWMSG
LNCDGLNCDG
NECDAG NECDAG
Other Network GroupsOther Network Groups
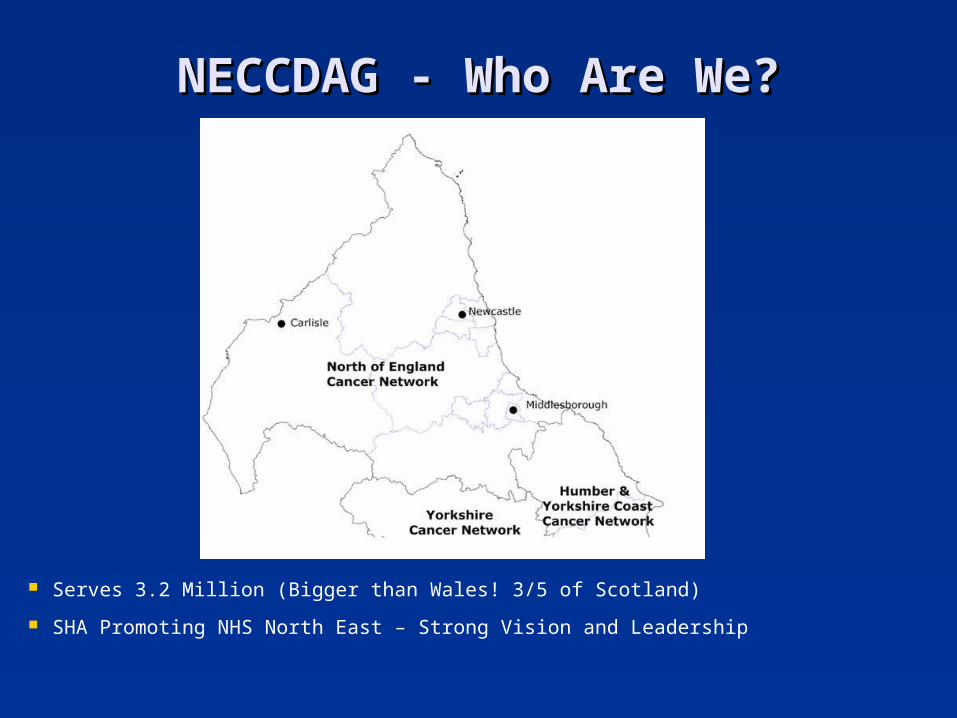
NECCDAG - Who Are We?NECCDAG - Who Are We?
Serves 3.2 Million (Bigger than Wales! 3/5 of Scotland)
SHA Promoting NHS North East – Strong Vision and Leadership
North of England Cancer Drug Approval Group (NE CDAG)
Formed May 2005
Two Cancer Networks in North East
Two sets of decisions = PCT’s making different funding
decisions
Two High profile media drug campaigns highlighted issues to
North East Chief Execs (Herceptin & Alimta)
SHA wanted equity
PCT wanted help with difficult decisions
NECDAG born
North of England Cancer Drug Approval Group (NE CDAG)
Chair – Ian Dalton, Chief Executive of North East NHS
(SHA) Formerly CE of North Tees & Hartlepool Trust
Purpose
To ensure that all patients with cancer in the North East
Cancer Networks receive equitable access to a clinically
defined appropriate range of cancer medicines.
Acts as an expert body within the North East
Make decisions about availability of new and existing
cancer drugs
North of England Cancer Drug Approval Group (NE CDAG)
Accept all NICE recommended Drugs Advise PCTs of financial and service impact
NICE due within 3 to 6 months = not considered Prioritise:
- non NICE recommended potentially curative drug- non NICE Palliative (non curative)
‘Horizon Scan’ Audit, Evaluate, Support Implementation Make dis-investment decisions where appropriate Encourage the use of new drug therapies in clinical Trials
North of England Cancer Drug Approval Group (NE CDAG)
NECDAG Considers New drugs for cancer New indications for old drugs New combinations of drugs Hormonal, supportive and other licensed new / novel
treatments Unlicensed medicines only in exceptional
circumstances Reviewing policy on off-label medicines, e.g. FEC-T
North of England Cancer Drug Approval Group (NE CDAG)
Meets 4 to 5 times per year. Quorm = 3 out of the 5 PCT cluster representatives 75% majority for agreement In event of lack of unity Final Voting rests with PCT
commissioners Submissions sent electronically on the ‘New Product
Request’ form by set deadlines Network Pharmacists provide cost analysis & support Requests presented by a nominated member of the
Tumour Specific Group PCTs / Trusts informed of decisions within 7 days

CANCER DRUG APPLICATION
FORM
Imminent NICE Appraisal
(Financial & Service Impact Assessed)
1. Implementation according to plan in application form undertaken2. Treatment protocol added to NCN/CCA Chemotherapy Approved Lists
North of England Cancer Drug Approval Group (NE CDAG)
Summary of Application Process
Yes
No
Horizon Scanning (Potential
Applications & Applicant identified)
Cancer Drug Approval Group
APPROVED
NO re-submission for 12 months
Unless new evidence
Gateway GroupPrioritises Applications. Adds Financial & Service
Impact information. Advises on Implementation.
Local Chemotherapy
Group
TSG
Decision Communicated to Stakeholders: PCTs, TSG Chairs, Trusts, Network Boards, Network
Chemo GroupsPress Release Prepared
Within 14 days
Clinical & Financial Approval
Approval Group Membership:2 Network Chairs (rotating)2 Network Directors2 Clinical Reps NCN2 Clinical Reps CCA2 Network Medical Directors2 Network Pharmacists1 SHA Executive Director1 SHA Communications Lead2 Network Patient Reps5 PCT Executive Directors(1 Cumbria, 4 from joint SHA area)2 Public Health Reps

Decision making - Simple Approach toDecision making - Simple Approach to Quality Adjusted Life Years Quality Adjusted Life Years
QALY’s combine the Quantity and Quality of Life (QoL). QALY’s combine the Quantity and Quality of Life (QoL).
Utility ValuesUtility Values
One year of perfect health = 1 One year of perfect health = 1
One year of less than perfect Health > 1 (RIP = 0)One year of less than perfect Health > 1 (RIP = 0)
Calculating QALYsCalculating QALYs
Intervention A = patient lives extra 2 years in heath state 0.75Intervention A = patient lives extra 2 years in heath state 0.75
2 years extra life @ 0.75 QoL = 2 x 0.75 = 1.5 QALYs gained2 years extra life @ 0.75 QoL = 2 x 0.75 = 1.5 QALYs gained
Applying QALYS to cost effectiveness decisionsApplying QALYS to cost effectiveness decisions Intervention A, costs £10,000 and generates 1.5 QALYs Intervention A, costs £10,000 and generates 1.5 QALYs Therefore cost per QALY = £10,000/1.5 = £6,667Therefore cost per QALY = £10,000/1.5 = £6,667 Intervention A appears NICE friendly!!Intervention A appears NICE friendly!!
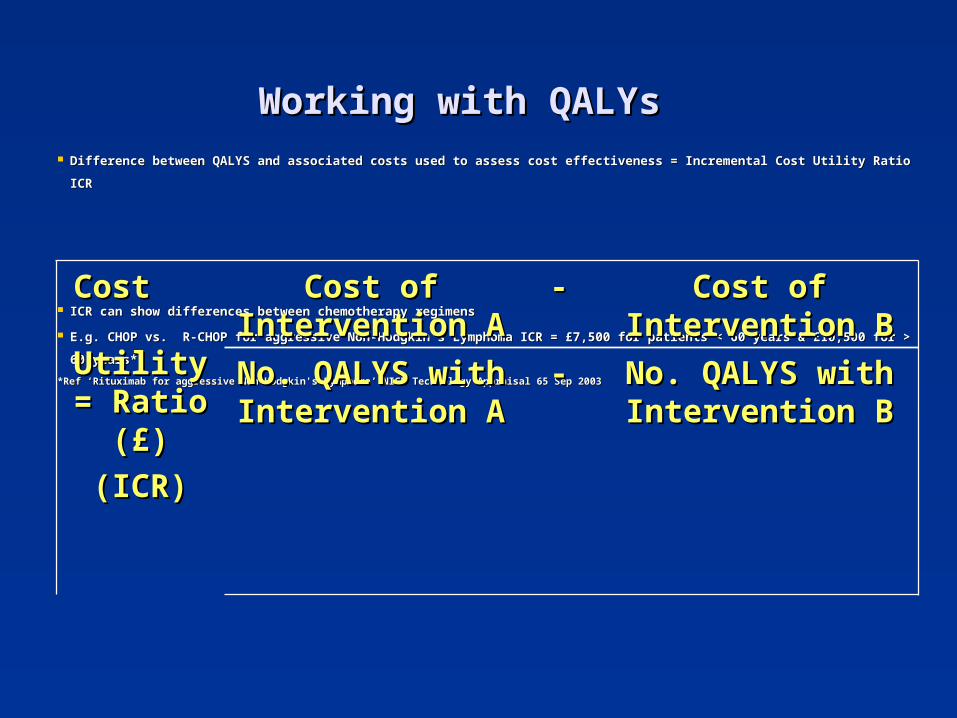
Working with QALYsWorking with QALYs Difference between QALYS and associated costs used to assess cost effectiveness = Incremental Cost Utility Ratio ICRDifference between QALYS and associated costs used to assess cost effectiveness = Incremental Cost Utility Ratio ICR
ICR can show differences between chemotherapy regimensICR can show differences between chemotherapy regimens
E.g. CHOP vs. R-CHOP for aggressive Non-Hodgkin's Lymphoma ICR = £7,500 for patients < 60 years & £10,500 for > 60 E.g. CHOP vs. R-CHOP for aggressive Non-Hodgkin's Lymphoma ICR = £7,500 for patients < 60 years & £10,500 for > 60
years*years*
*Ref ‘Rituximab for aggressive Non-Hodgkin's Lymphoma’ NICE Technology Appraisal 65 Sep 2003*Ref ‘Rituximab for aggressive Non-Hodgkin's Lymphoma’ NICE Technology Appraisal 65 Sep 2003
Cost Cost Utility = Utility = Ratio (£)Ratio (£)
(ICR)(ICR)
Cost of Cost of Intervention AIntervention A
-- Cost of Cost of Intervention BIntervention B
No. QALYS with No. QALYS with Intervention AIntervention A
-- No. QALYS with No. QALYS with Intervention BIntervention B
Working with QALYsWorking with QALYs Not all interventions easily assessed by ICR model
Health Economic studies use robust cost utility models
(computer simulations) e.g. Markov models
Sensitivity analyses crucial to check accuracy of model Sensitivity analysis test affect of changes in clinical
outcomes and resource costs on QALY outcomes (CI’s)
• Changes in Median overall survival benefits
• Changes in Median progression-free survival benefits
• Quality of life (utility) for stable vs. progressive disease
• Drug costs; discounts, No of cycles of drug given etc.

Lessons Learnt Look to NICE to set the standards
Be brave don’t just make easy clinical decisions
Don’t be scared of QALYS
Health economist expertise very rare
Use as a guide only, not the be all and end all
Not perfect, best tool we’ve got
More complex is not necessarily better
Lessons Learnt Why have we been a success?
Action at Chief Executive level
PCT and Commissioner ‘buy in’ from start
Funds follow decisions
Use NICE standards for assessing evidence
Make Tough decisions, i.e. We do say No
Strong Leadership & respected experts
Patient Presence
Still Learning! Want to offer North East patients best medicines
Have to keep commissioners happy
Learn to deal with Phase II evidence & Lack of survival
data
Need good intelligence e.g. ASCO etc
Need credibility with clinicians
Learn to work with industry on prices
Need to manage the media – Press officer vital
We need to encourage NICE to go faster!

NECDAG DecisionsNECDAG Decisions
Adjuvant Temozolomide Approved for PS 0 & Adjuvant Temozolomide Approved for PS 0 & PS1 <50 years (Nov 06) PS1 <50 years (Nov 06)
Revised NICE FAD (March 07) very later similarRevised NICE FAD (March 07) very later similar
Erlotinib initially rejected but to be reviewed in Erlotinib initially rejected but to be reviewed in Nov 07Nov 07
Dasatinib – not approvedDasatinib – not approved
Sunitinib for Renal Cell cancer - ApprovedSunitinib for Renal Cell cancer - Approved
Pemetrexed – approved pre NICE…..Pemetrexed – approved pre NICE…..
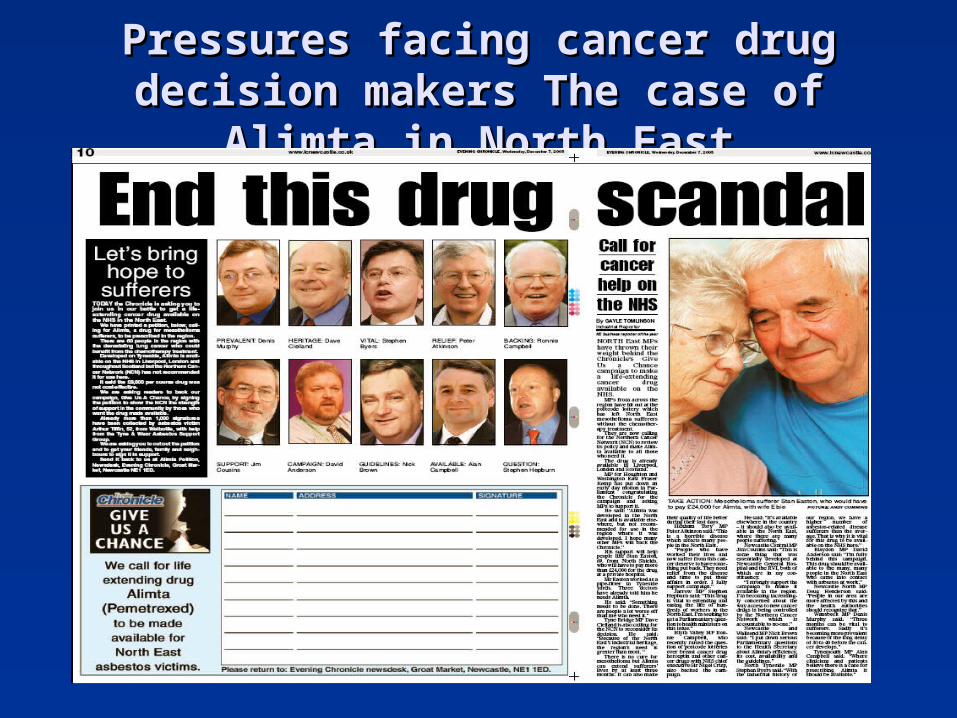
Pressures facing cancer drug decision Pressures facing cancer drug decision makers The case of Alimta in North Eastmakers The case of Alimta in North East
Consequences of cost effectiveness rationing Consequences of cost effectiveness rationing of chemotherapy – The saga of Alimtaof chemotherapy – The saga of Alimta
• 2005 application for to use (Alimta) pemetrexed for mesothelioma in North East England was rejected as not shown to be cost effective.
• (QALY = £36,000 to £47,000)
• Industrial heritage = local population greatly affected
• Patients and their oncologists very unhappy with decision
• Northeast Newspaper Campaign Petition from MP’s, footballers! etc
• Public pressure forces executive action from health bosses
ALIMTA APPROVED
• But…NICE then reject Alimta
• Appeal Hearing Nov 2006
• March 2007 Draft appraisal still negative
• July 2007 – FAD Alimta approved – QALY’s drop from £60K to £34.5
Challenges for the FutureChallenges for the Future
Saying No – Dealing with appealsSaying No – Dealing with appeals
Marginal BenefitMarginal Benefit
Right to NHS treatmentsRight to NHS treatments
Patient and public pressurePatient and public pressure
Exceptional circumstance pathwayExceptional circumstance pathway
Co-PaymentCo-Payment
Challenge of Saying NoChallenge of Saying No BenchmarkingBenchmarking
Same evidence why different decisions?Same evidence why different decisions? Health economist adviceHealth economist advice
Variation in Cost effective AnalysisVariation in Cost effective Analysis NECDAG uses simple in house QALY modelsNECDAG uses simple in house QALY models Do we trust QALYS?Do we trust QALYS? BMJ article showed great variance in NICE QALYS vs IndustryBMJ article showed great variance in NICE QALYS vs Industry11
Threat of litigationThreat of litigation PCTs statutory body – NECDAG advisory PCTs statutory body – NECDAG advisory ? Can we be sued?? Can we be sued? Publication of our decisions - NHS or PublicPublication of our decisions - NHS or Public
1. Comparing estimates of cost effectiveness submitted to the National Institute for Clinical Excellence (NICE) by different organisations: retrospective study A H Miners et al BMJ 2005;330;65
Challenge of Marginal BenefitChallenge of Marginal Benefit
Key is benefitKey is benefit Clinical, Economic, or BothClinical, Economic, or Both
What is marginal ?What is marginal ? ? 3 months extra erlotinib / pemetrexed in lung? 3 months extra erlotinib / pemetrexed in lung < 6 weeks Gem/Cap for pancreas< 6 weeks Gem/Cap for pancreas
Supply and DemandSupply and Demand Cancer medicines Big businessCancer medicines Big business Patients want Patients want hopehope International Market can take premium pricesInternational Market can take premium prices Need to Work Industry on UK pricing Need to Work Industry on UK pricing
Exceptional CircumstanceExceptional Circumstance PCTs have to consider EC requestsPCTs have to consider EC requests Difficult to refuse on grounds of cost Difficult to refuse on grounds of cost How to ensure equity if each PCT make own decision?How to ensure equity if each PCT make own decision? NECDAG has vested interestNECDAG has vested interest Can you have guidance on what is an exception?Can you have guidance on what is an exception? If it can be anticipated then is it an exception?If it can be anticipated then is it an exception? Approvals process needs to anticipate potential EC Approvals process needs to anticipate potential EC
requests, e.g. look at subgroups etc.requests, e.g. look at subgroups etc. More pressure on upfront decisionsMore pressure on upfront decisions
Co- PaymentCo- Payment PCTs need NECDAG advicePCTs need NECDAG advice Can NHS Patients buying their own medicines?Can NHS Patients buying their own medicines? Difficult exceptional CasesDifficult exceptional Cases
Drug rejected on evidence of marginal response and Drug rejected on evidence of marginal response and high cost – i.e. low average response rate… buthigh cost – i.e. low average response rate… but
NHS patient buys drug privately is a responder NHS patient buys drug privately is a responder Runs out of money- can we morally refuse to treat?Runs out of money- can we morally refuse to treat?
Patients Right to NHS treatment Patients Right to NHS treatment vs vs
Access to treatment regardless of ability to payAccess to treatment regardless of ability to pay Will Chemotherapy PBR open this up further?Will Chemotherapy PBR open this up further?
ConclusionsConclusions
North East Group Effective and CredibleNorth East Group Effective and Credible Can be done elsewhereCan be done elsewhere Needs Regional Approach = UnityNeeds Regional Approach = Unity Equity within North East but differences Equity within North East but differences
elsewhere – regional postcode prescribing.elsewhere – regional postcode prescribing. Higher Profile = More scrutinyHigher Profile = More scrutiny Continues to face fresh challengesContinues to face fresh challenges Would be happy to not exist (Fast NICE!)Would be happy to not exist (Fast NICE!)


















