
Canadian Lung Volume Reduction CLVR Surgery Trial
29
Canadian Lung Volume Reduction CLVR Surgery Trial 2 year report John Miller MD FRCSC MI-GMAC Chair in Thoracic Surgery Richard A Malthaner MD FRCSC FACS Charles H Goldsmith PhD
-
Upload
changezkn -
Category
Health & Medicine
-
view
607 -
download
2
Transcript of Canadian Lung Volume Reduction CLVR Surgery Trial

Canadian Lung Volume Reduction CLVR Surgery Trial
2 year report
John Miller MD FRCSCMI-GMAC Chair in Thoracic SurgeryRichard A Malthaner MD FRCSC FACSCharles H Goldsmith PhD

Hypothesis:LVRS is effective management of symptomatic
patients with large lung volumes and reduced air flow secondary to emphysema
Design:RCT comparing optimal medical management (including rehabilitation) and LVRS to optimal medical management (including rehabilitation)

Trial Design
Eligibility Visit
Rehabilitation
Randomized 1:1
Surgery Median
sternotomyBest Medical Care
3, 6,12, 18, 24 months 3, 6, 12, 18, 24 months
No Crossovers Blinded Assessment No Crossovers Blinded Assessment

Patient SelectionInclusion Criteria:
Disabling dyspnea (CRQ < 4 -dyspnea score)Airflow limitation (FEV1 15-40%)Gas trapping (TLC 120%, RV/TLC > 60%) Radiographic evidence of emphysema
Exclusion Criteria:Ventilated patient Alpha-1 deficiency Chest wall deformityIsolated bullous > 25% of hemithorax pCO2 >55, Pulmonary hypertension Cancer

Primary Outcome: HUI QALY
MortalityPalliation: Quality of Life measurement:
Disease specific: CRQ, MRC, St GeorgesGeneric: MOS, MOS-SF36Health Utility Score: HUI, QWB, SG, TT
We wanted a measure that was generalizeable,And would take mortality into consideration.
We wanted to have an economic assessment

Primary Outcome: HUI QALY1.0
0.5
0.0
HUI: Health Utility IndexScores several health states
1.0 is perfect health
0.0 is death
Examiner administeredMCID 0.05 – 0.10

QALYS (Quality Adjusted Life Years)

Trial Outcomes
Impairment: A loss or abnormality of function at the level of the organ. (Lung Function Studies)
Disability: Any restriction or lack of ability to perform an activity. (exercise capacity, walk tests)
Handicap: A disadvantage for a given individual resulting from an impairment or a disability. (Quality of Life Scores)
(WHO, International Classification of Impairments, Disabilities and Handicaps 1980)

Trial Outcomes
HandicapHUI – QALYs (1o outcome)SF-36, CRQ
ImpairmentPulmonary function tests
Disability6-minute- walk test (6MW)
Economic

Standardized Treatment Arms

London Hamilton

Trial Size
Primary outcome: Health Utility (takes mortality in to account)
HUI3 and QALYsMCID: 0.05 – 0.10 Assuming: alpha of 5% and a power of 90%Size requirement: 350 patients
MCID: determined by a survey of experts and stakeholders
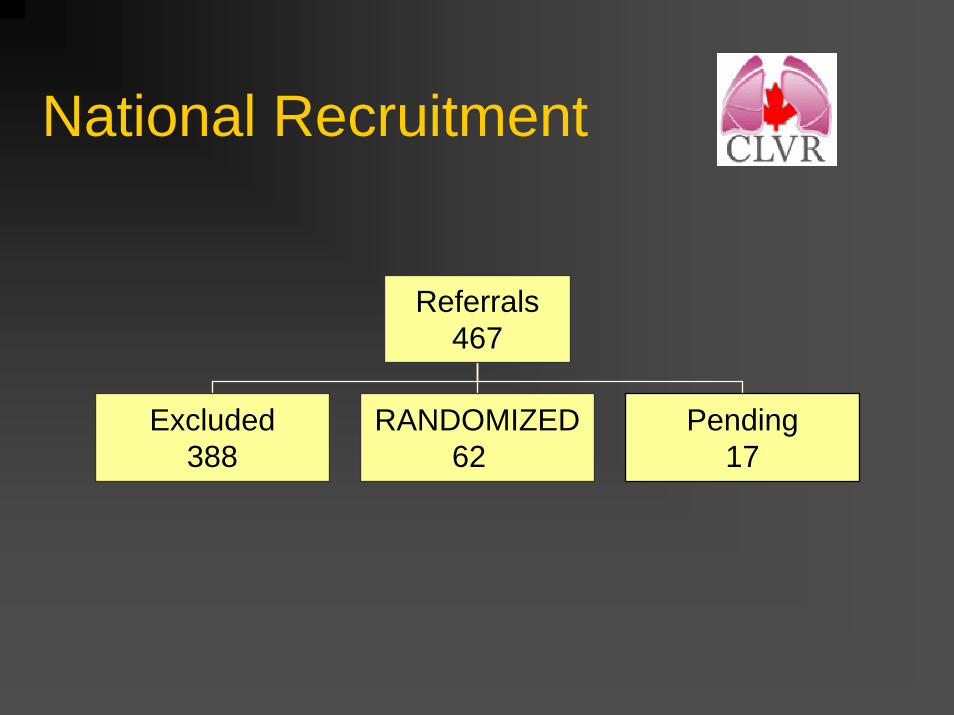
National Recruitment
Referrals467
Excluded388
RANDOMIZED62
Pending17

Reasons for exclusion:
Patient too ill with multi-system illnesses 25%Lung volumes not large enough 24%Patient declined (not sick enough) 17% Lung disease too severe
10%Bullous disease (requires major bullectomy) 9%Alpha 1 anti-trypsin emphysema 6%Lung transplant candidate 5%Patient Ventilator dependant 4%
No patient in any centre underwent LVRS off study
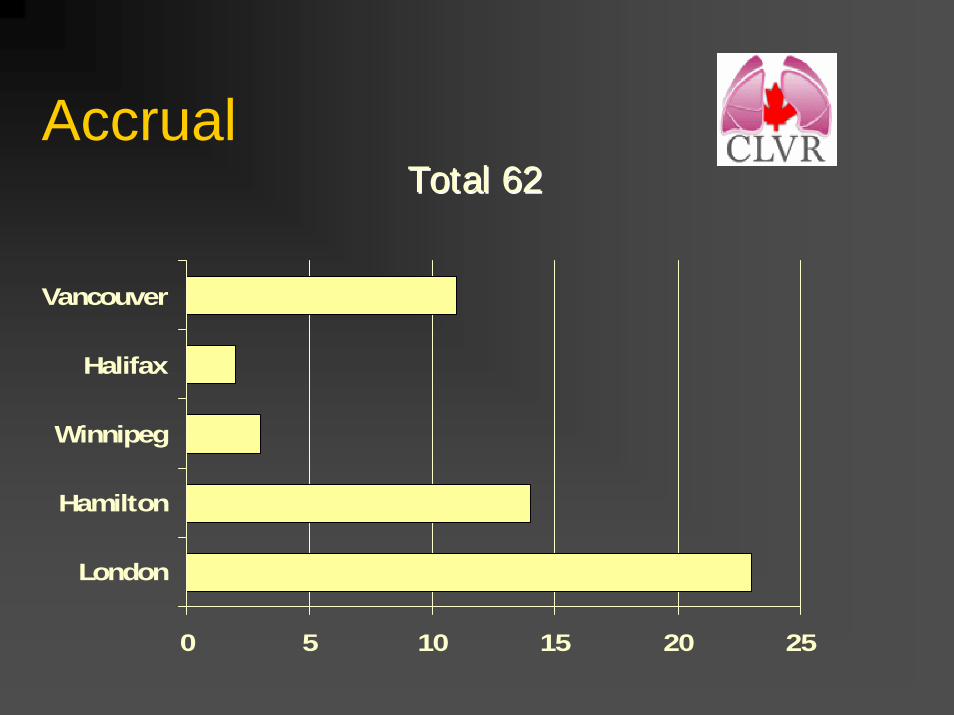
Accrual
0 5 10 15 20 25
London
Hamilton
Winnipeg
Halifax
Vancouver
Total 62Total 62

Accrual:
Struggled to recruit:62/350 = 18% of our anticipated number
Political, economic, strategic issues all worked against reaching our target.

LVRS Medicaln 32 30
Age 64.1 63.7Male: Female 22:10 19:11
Smoked 60 pk-yr 44 pk-yrBMI 24.4 + 4.6 23.6 + 3.7RV 5.4 + 1.0 5.4 + 1.2
TLC 136% 138%FEV1 25% 23%
DLCO 31% 35%6MW 340 319

Mortality
LVRS Medical
30 d 0 0
90 d 6% 3%
2 yr 16%(5)
13%(4)

ImpairmentQuality Adjusted
FEV1 improves over medical Arm by 263 ml (p=0.0001)
LVRS Med
Better 2991%
1027%
worse 3 20P=0.001 32 30
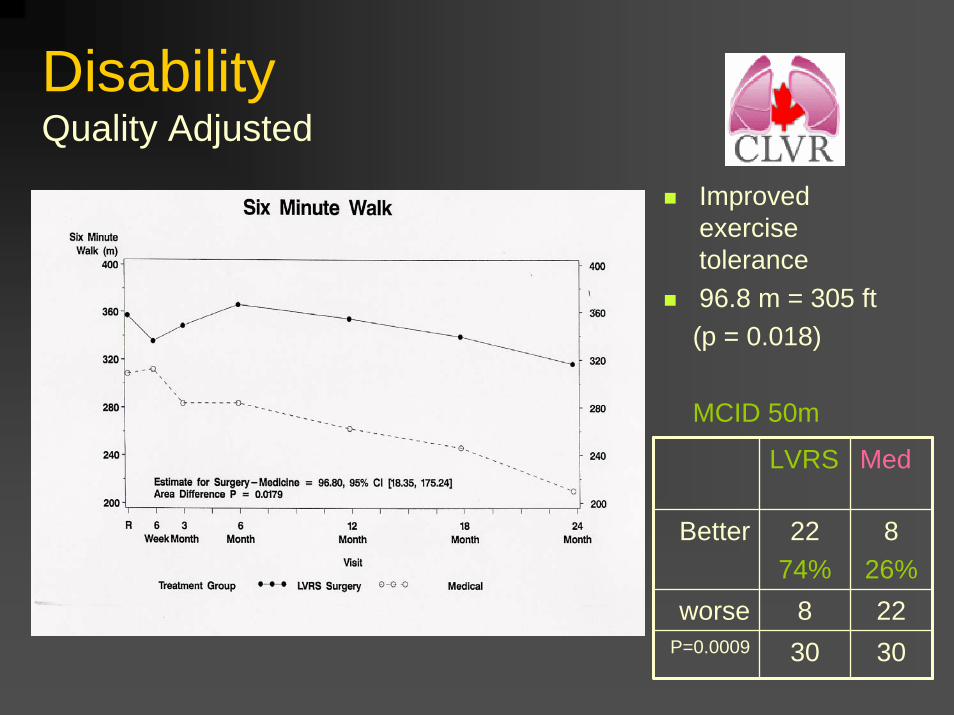
DisabilityQuality Adjusted
Improved exercise tolerance96.8 m = 305 ft(p = 0.018)
MCID 50m
LVRS Med
Better 2274%
826%
worse 8 22P=0.0009 30 30

HandicapQuality Adjusted
Most sensitiveMost meaningfulto patientClinically and statistically better - 1.175
(p = 0.0046)
MCID = 0.5

HandicapQuality Adjusted Life Years
Improved HEALTH UTILITY INDEX Overall health benefitQALY of 0.112Clinically important But small trial size (p = 0.191 )
MCID = 0.10

Costs: hospitalizations
LVRS Arm Medical Arm
Mean 31 daysMedian LOS 17 days
Readmit frequency 0.8 1.6Duration of Hosp 10.3 days 17.2 days

LVRS Medicine Index HospitalizationSurgery Costs 4,6840 Length of stay costs 28,9380 Index Hospitalization 33,6220
Follow-Up Hospitalizations 7,204 12,155 Rehabilitation 3,469 2,647 Oxygen 2,781 3,957 Medications 1,175 1,400Outpatient 1,524 1,498 Total Follow-up Costs 16,154 21,657
Total Costs 49,776 21,657
Quality Adjusted Life Years (QALYs) 1.23 1.02
Cost Effectiveness Ratio COST/QALY $ 133,900.00
( 1.23 -1.02) = 0.2 x (49 -21 ) = 28.1 = $133,000

Cost-Effectiveness 2 years
1.031.23QALYs
$133,000Cost per QALY
$21,657$49,776Cost
Medicaln=28
LVRSn=31
p<0.001 for costs and QALYs (1.23 -1.02) = 0.2 x (49 -21 ) = 28.1 = $133,000

Canadian GuidelinesHow attractive does a new tech need to be to warrant adoption and utilization?
$ 20,000 a good buy for Canadians$ 20,000 - $120,000 considered in a
broader contextgreater than $ 120,000 not in Canadian’s
best interest
Tugwell, Laupacis Feeney Detsky ICES CMAJ 1992

Cost-Effectiveness Other Common Interventions
$133,000LVRS
$177,000 Lung Transplant
$250,000 ICU ventilation (mod risk)
$ 140,000 Lap hernia repair
$ per QALYIntervention

Conclusions
LVRS is an effective treatment for Emphysema:Safe: early surgical mortality off-set by improved mortality later onHandicap: QOL – CRQ, MOS SF36Impairment: PFTs- FEV1Disability: Exercise- 6MWStudy establishes that it can be done in smaller centersCost: challenges us to find savings
clinically important statistically sig.improvement

Thank-you


















