
Practice Guideline update (COPD): 2021 Canadian Thoracic ...

Canadian Guideline on Concussion in Sport

Canadian Guideline on Concussion in Sport
July 2017
Funding provided by: Public Health Agency of Canada
The views expressed herein do notnecessarily representthe views of the Public Health Agency of Canada.
Suggested citation: Parachute. (2017). Canadian Guideline on Concussion in Sport. Toronto: Parachute.
© Parachute –Leaders in Injury Prevention, 2017

Contents EXPERT ADVISORY COMMITTEE ON CONCUSSIONS 5 ADDITIONAL REVIEW AND FEEDBACK 6 PARACHUTE PROJECT TEAM 6
OVERVIEW 7 PURPOSE 7 APPLICATION TO NON-SPORT RELATED CONCUSSION 7 WHO SHOULD USE THIS GUIDELINE? 7 HOW TO READ THIS GUIDELINE 8 ROLE OF CLINICAL JUDGMENT 8 KEY TERMDEFINITIONS 8
GUIDELINE RECOMMENDATIONS 11 1. PRE-SEASON EDUCATION 12 2. HEAD INJURY RECOGNITION 13 3. ONSITE MEDICAL ASSESSMENT 14 4. MEDICAL ASSESSMENT 16 5. CONCUSSION MANAGEMENT 17 6. MULTIDISCIPLINARY CONCUSSION CARE 20 7. RETURN TO SPORT 21
CANADIAN SPORT CONCUSSION PATHWAY 23
GUIDELINE DEVELOPMENT PROCESS EVIDENCE STAKEHOLDERCONSULTATION UPDATES TO THIS GUIDELINE
APPENDIX: DOCUMENTS & TOOLS
25 25 26
27 PRE-SEASON CONCUSSION EDUCATION SHEET 29 MEDICAL ASSESSMENT LETTER 31
25

MEDICAL CLEARANCE LETTER 33 CONCUSSION RECOGNITION TOOL –5THEDITION (CRT5) 35 SPORT CONCUSSION ASSESSMENT TOOL –5THEDITION (SCAT5) 37 CHILD SPORT CONCUSSION ASSESSMENT TOOL –5THEDITION (CHILD SCAT5) 45

Contributors Expert Advisory Committee on Concussions Dr. Charles Tator, Co-Chair, MD, PhD, FRCSC, FACS Professor of Neurosurgery, University of Toronto Division of Neurosurgery and Canadian Concussion Centre, Toronto Western Hospital
Dr. Michael Ellis, Co-Chair, BSc, MD, FRCSC Medical Director, Pan Am Concussion Program Dept. of Surgery and Pediatrics and Section of Neurosurgery, University of ManitobaScientist, Children’s Hospital Research Institute of ManitobaCo-director, CanadaNorth Concussion Network
Dr.Shelina Babul, B.Sc., PhDAssociate Director, Sports Injury Specialist, BC Injury Research & Prevention Unit, BC Children's Hospital Investigator, Djavad Mowafaghian Center for Brain Health, UBC Clinical Associate Professor, Dept. of Pediatrics/Pathology & Laboratory Medicine, UBC
Dr. Shannon Bauman, MD, CCFP (SEM), Dip. Sport Med Medical Director, Concussion North Dept. of Family Medicine, Dept. of Surgery, Royal VictoriaRegional Health Centre
Dr. Michael Cusimano, MD, MHPE, FRCS, DABNS, PhD, FACS Division of Neurosurgery, St. Michael's Hospital Professor of Neurosurgery, Education and Public Health, University of Toronto
Dr.Carolyn Emery, BScPT, PhDAssociate Dean Research and Associate Professor, Faculty of Kinesiology Co-chair, SportInjury Prevention Research Centre, Faculty of Kinesiology Pediatrics and Community Health Sciences, Faculty of Medicine, University of Calgary
Dr. Pierre Frémont, MD, PhD, FCMFFull Professor, Faculty of Medicine, Laval University
Dr.ClaudeGoulet, PhDFull Professor, Faculty of Education, Departmentof Physical Education, Laval University
Louise Logan, BA(Hons), JD President, Logan & Associates
PARACHUTE | Canadian Guideline on Concussion in Sport i5

Dr. Alison Macpherson, PhD Associate Professor, Faculty of Health, School of Kinesiology & Health Science, York University AdjunctScientist, Institute for Clinical Evaluative Sciences
Dr. NickReed, PhD, MScOT, OT Reg (Ont) Clinician Scientist, Bloorview Research Institute Co-Director, Concussion Centre, Holland Bloorview Kids Rehabilitation Hospital AssistantProfessor, Dept. of Occupational Science and Occupational Therapy, University of Toronto
Dr. Kathryn Schneider, PT, PhD, DipManipPT AssistantProfessor, Clinician Scientist, Faculty of Kinesiology, University of Calgary AlbertaChildren’s Hospital Research Institute Clinical Specialist–Musculoskeletal Physiotherapy
Dr. Ash Singhal, BSc, MSc, MD, FRCSC Pediatric Neurosurgeon, BC Children’s Hospital Medical Director, BC Pediatric TraumaProgram Clinical AssistantProfessor, UBC
Dr. Michael Vassilyadi, MD, CM, MSc, FRCS (C), FACS, FAAP Associate Professor of Surgery, University of OttawaDivisionofNeurosurgery, CHEO
Dr. Roger Zemek, MD, FRCPC Associate Professor, Deptof Pediatrics and Emergency Medicine Clinical Research Chair in Pediatric Concussion, University of OttawaDirector, Clinical Research Unit, CHEO
Additional review and feedbackDr. JackTaunton, MSc, MD, DIPL Sports Med (CASEM), FACSM
Federal-Provincial/Territorial WorkGroup on Concussions in Sport
Parachute Project Team Pamela Fuselli, VP, Knowledge Transfer & Stakeholder Relations
Valerie Smith, Director, Solutions
Stephanie Cowle, ProjectManager, Solutions
PARACHUTE | Canadian Guideline on Concussion in Sport i6

Overview PurposeThis guideline covers pre-season education and the recognition, medical diagnosis, and managementof athletes who sustain asuspected concussion during asportactivity. Itaims to ensure thatathletes with asuspected concussion receive timely and appropriate care, and proper managementto allow them to return to their sport. This guideline may notaddress every possible clinical scenario thatcan occur butis intended as ageneral overview thatincludes critical elements based on the latestevidence and currentexpertconsensus.
Application to non-sport related concussion This guideline has been developed based on areview of the currentscientific evidence and expertconsensus on bestpractices for the evaluation and managementof Canadian athletes who sustain aconcussion during asportactivity. However, the managementprinciples described in this guideline should also be applied to children, adolescents and adults who sustain aconcussion outside of asporting environmentand are returning to activity (in school, in the workplace, and so on).
Certain terminology has been used to make this guideline as specific as possible and to directly reflectthe International Consensus Statementon Concussion in Sport.These termsmay be new to some readers and two examples are worth noting. A Return-to-School Strategy is recommended to address the process commonly known as “return to learn”. The Return-to-School Strategy focuses on the individual returning to aformal, structured learning environmentrather thatengaging more broadly in cognitive day-to-day activities. A Return-to-SportStrategy is recommended to address the process known as “return to play”. The Return-to-SportStrategy focuses on individuals returning to training, practice, and competition in organized sport, notunstructured day-to-day activity or play. For further information on terminology used in this guideline, please see the “Key Term Definitions” section.
Who should usethisguideline?This guideline is intended for use by all stakeholders who interactwith athletes inside and outside the contextof school and non-school based organized sports activity, including athletes, parents, coaches, officials, teachers, trainers, and licensed healthcare professionals.
PARACHUTE | Canadian Guideline on Concussion in Sport i7

Howtoreadthisguideline This guideline addresses 7 areas in the prevention, recognition, diagnosis, and managementof sport-relatedconcussion:
1. Pre-season education 2. Head injury recognition 3. Onsite medical assessment4. Medical assessment5. Concussion management6. Multidisciplinary concussion care 7. Return to sport
For each area, recommendations are provided, along with:
‣ Who: Who are the people thatplay akey role to implementthe recommendations in this area.
‣ How: Whatare the key tools and documents people can use to implementthe recommendations in this area. All tools are included directly in this guideline.
Role of clinical judgment Several recommendations in this guideline are aimed atlicensed healthcare professionals with the aim of helping them make informed decisions abouttheir patients. However, this guideline is notintended to take the place of clinical judgmentin diagnosing and treating concussion. Healthcare professionals mustmake their own decisions aboutcare after consultation with their patients, using their clinical judgement, knowledge and expertise.
Key Term Definitions Concussion:A form of traumatic brain injury induced by biomechanical forces thatresultin signs and symptoms thattypically resolve spontaneously within 1-4 weeks of injury.1
Athlete: Any youth or adultparticipating in aschool or non-school based sportactivity, competing atany level of play (amateur or national team). This term refers to all sportparticipants and players. The mostappropriate term will vary across differentsports and settings.
Youth or youth athlete: An athlete or sportparticipantwho is less than 18 years of age.
1McCrory etal. (2017). Consensus statementon concussion in sport–the 5th international conference on concussion in sportheld in Berlin, October 2016. British Journal of Sports Medicine, 51(11), 838-847.
PARACHUTE | Canadian Guideline on Concussion in Sport i8

Sportor sportactivity: A school or non-school based physical activity thatcan be played as an individual or ateam including games and practices.
Recognition: The detection of an event(i.e. asuspected concussion) occurring during sports or asportactivity.
Exercise: Any physical activity thatrequires bodily movementincluding resistance training as well as aerobic and anaerobic exercise or training.
Persistent symptoms: Concussion symptoms thatlastlonger than 2 weeks after injury in adults and longer than 4 weeks after injury in youth.
Licensedhealthcare professional: A healthcare provider who is licensed by anational professional regulatory body to provide concussion-related healthcare services thatfall within their licensed scope of practice. Examples include medical doctors, nurses, physiotherapists, and athletic therapists.
Among licensed healthcare professionals, only medical doctors and nurse practitioners are qualified to conductacomprehensive medical assessmentand provide aconcussion diagnosis in Canada. The types of medical doctors qualified to do such an evaluation are: pediatricians; family medicine, sports medicine, emergency departmentand rehabilitation (physiatrists) physicians; neurologists; and neurosurgeons.
Medical Assessment: The evaluation of an individual by alicensed healthcare professional to determine the presence or absence of amedical condition or disorder, such as aconcussion.
Treatment: An intervention provided by alicensed healthcare professional to address adiagnosed medical condition/disorder or its associated symptoms, such as physical therapy.
Multidisciplinary concussion clinic: A facility or network of licensed healthcare professionals thatprovide assessmentand treatmentof concussion patients and are supervised by aphysician with training and experience in concussion.
Tool: A standardized instrumentor device thatcan be used to help recognize an event(i.e. asuspected concussion) or assess an individual with asuspected medical diagnosis (i.e. SportConcussion AssessmentTool 5).
Document: A standardized written letter or form thatcan help facilitate communication between sportstakeholders.
Concussion Recognition Tool –5th Edition (CRT5): A tool intended to be used for the identification of suspected concussion in children, youth, and adults. Published in 2017 by the Concussion in SportGroup, the CRT5 replaces the previous PocketConcussion Recognition Tool from2013.
PARACHUTE | Canadian Guideline on Concussion in Sport i9

Sport Concussion Assessment Tool –5th Edition (SCAT5): A standardized tool for evaluating concussions in individuals aged 13 years or older, designed for use by physicians and licensed healthcare professionals. Published in 2017 by the Concussion in SportGroup, the SCAT5 replaces the previous SCAT3 from 2013.
Child Sport Concussion Assessment Tool –5th Edition (Child SCAT5): A standardized tool for evaluating concussions in individuals aged 5 to 12 years, designed for use by physicians and licensed healthcare professionals. Published in 2017 by the Concussion in SportGroup, the Child SCAT5 replaces the previous Child SCAT3 from 2013.
Return-to-School Strategy: A graduated stepwise strategy for the process of recovery and return to academic activities after aconcussion. The broader process of returning to cognitive activities has commonly been referred to as “return to learn”.
Return-to-Sport Strategy: A graduated stepwise strategy for the process of recovery and then return to sportparticipation after aconcussion. The broader process of returning to unstructured and structured physical activity has commonly been referred to as “return to play”.
PARACHUTE | Canadian Guideline on Concussion in Sport i10

Guideline Recommendations
PARACHUTE | Canadian Guideline on Concussion in Sport i11

1.Pre-SeasonEducation1.Pre-Season Education
Despite recentincreased attention focusing on concussion there is acontinued need to improve concussion education and awareness. Optimizing the prevention and managementof concussion depends highly on annual education of all sportstakeholders (athletes, parents, coaches, officials, teachers, trainers, and licensed healthcare professionals) on evidence-informed approaches thatcan preventconcussion and more serious forms of head injury and help identify and manage an athlete with asuspected concussion.
Concussion education should include information on: • the definition of concussion, • possible mechanisms of injury, • common signs and symptoms, • steps thatcan be taken to preventconcussions and other injuries from occurring in sport, • whatto do when an athlete has suffered asuspected concussion or more serious head injury,
• whatmeasures should be taken to ensure proper medical assessmentincluding Return-to-School and Return-to-SportStrategies, and
• Return-to-sportmedical clearance requirements.
As an example, this education could be provided using an education sheetthatis reviewed and signed by all stakeholders atthe time of sportregistration or before the beginning of each sports season to confirm thatthe key information has been received by all participants.
In addition to reviewing information on concussion, itis also importantthatall sportstakeholders have aclear understanding of the concussion protocol and policies for their sportand sportsetting atthe beginning of each sportseason. For example, this can be accomplished through pre-season in-person orientation sessions for athletes, parents, coaches and other sportstakeholders.
‣ Who: Athletes, parents, coaches, officials, teachers, and trainers, licensed healthcare professionals
‣ How: Pre-season Concussion Education Sheet
PARACHUTE | Canadian Guideline on Concussion in Sport i12

2.HeadInjuryRecognition2.Head Injury Recognition
Although the formal diagnosis of concussion should be made following amedical assessment, all sportstakeholders including athletes, parents, coaches, officials, teachers, trainers, and licensed healthcare professionals are responsible for the recognition and reporting of athletes who demonstrate visual signs of ahead injury or who reportconcussion symptoms. This is particularly importantbecause many sportand recreation venues will nothave access to on-site licensed healthcare professionals.
A concussion should be suspected in any athlete who sustains asignificantimpactto the head, face, neck, or body and demonstrates ANY of the visual signs of asuspected concussion or reports ANY symptoms of asuspected concussion as detailed in the Concussion Recognition Tool 5. A concussion should also be suspected if aplayer reports ANY concussion symptoms to one of their peers, parents, teachers, or coaches or if anyone witnesses an athlete exhibiting any of the visual signs of concussion.
In some cases, an athlete may demonstrate signs or symptoms of amore severe head or spine injury including convulsions, worsening headaches, vomiting or neck pain. If an athlete demonstrates any of the ‘Red Flags’ indicated by the Concussion Recognition Tool 5, amore severe head or spine injury should be suspected, and Emergency Medical Assessmentshould be pursued (see 3a. Emergency Medical Assessment).
‣ Who: Athletes, parents, coaches, officials, teachers, trainers, and licensed healthcare professionals
‣ How: Concussion Recognition Tool - 5th Edition (CRT5)
PARACHUTE | Canadian Guideline on Concussion in Sport i13

3. Onsite Medical Assessment3. Onsite Medical Assessment
Depending on the suspected severity of the injury and access to medical services, an initial assessmentmay be completed by emergency medical professionals or by an on-site licensed health professional where available. In cases where an athlete loses consciousness or itis suspected an athlete mighthave amore severe head or spine injury, Emergency Medical Assessmentby emergency medical professionals should take place (see 3abelow). If amore severe injury is notsuspected, the athlete should undergo Sideline Medical Assessmentor Medical Assessment, depending on if there is alicensed healthcare professional present(see 3b below).
3a. Emergency Medical Assessment If an athlete is suspected of sustaining amore severe head or spine injury during agame or practice, an ambulance should be called immediately to transfer the patientto the nearestemergency departmentfor further Medical Assessment.
Coaches, parents, trainers and sports officials should notmake any effortto remove equipmentor move the athlete until an ambulance has arrived and the athlete should notbe leftalone until the ambulance arrives. After the emergency medical services staff has completed the Emergency Medical Assessment,the athlete should be transferred to the nearesthospital for Medical Assessment. In the case of youth (under 18 years of age), the athlete’s parents or legal guardian should be contacted immediately to inform them of the athlete’s injury. For athletes over 18 years of age, their emergency contactperson should be contacted if one has been provided.
‣ Who: Emergency medical professionals
3b. Sideline Medical Assessment If an athlete is suspected of sustaining aconcussion and there is no concern for amore serious head or spine injury, the player should be immediately removed from the field of play.
Scenario1:If alicensedhealthcare professionalispresent The athlete should be taken to aquietareaand undergo Sideline Medical Assessmentusing the SportConcussion AssessmentTool 5 (SCAT5) or the Child SCAT5. The SCAT5 and Child SCAT5 are clinical tools thatshould only be used by alicensed medical professional thathas experience using these tools. Itis importantto note thatthe results of SCAT5 and Child SCAT5 testing can be normal in the setting of acute concussion. As such, these tools can be used by licensed healthcare professionals to documentinitial neurological status butshould notbe used to make sideline return-to-sportdecisions in youth athletes. Any youth athlete who is suspected of having sustained aconcussion mustnotreturn to the game or practice and should be referred for Medical Assessment.
PARACHUTE | Canadian Guideline on Concussion in Sport i14

If ayouth athlete is removed from play following asignificantimpactand has undergone Sideline Medical Assessment, butthere are NO visual signs of aconcussion and the athlete reports NO concussion symptoms then the athlete can be returned to play butshould be monitored fordelayed symptoms.
In the case of national team-affiliated athletes (age 18 years and older) who have been removed from play following asuspected concussion, an experienced certified athletic therapist, physiotherapistor medical doctor providing medical coverage for the sporting eventmay make the determination thataconcussion has notoccurred based on the results of the Sideline Medical Assessment. In these cases, the athlete may be returned to the practice or game withoutaMedical Clearance Letter butthis should be clearly communicated to the coaching staff. Players thathave been cleared to return to games or practices should be monitored for delayed symptoms by the licensed healthcare professional. If the athlete develops any delayed symptoms the athlete should be removed from play and undergo Medical Assessmentby amedical doctor or nurse practitioner (see 4. Medical Assessment).
Scenario2:Ifthere isnolicensedhealthcare professionalpresentThe athlete should be referred immediately for Medical Assessmentby amedical doctor or nurse practitioner, and the athlete mustnotreturn to play until receiving medical clearance.
‣ Who: Athletic therapists, physiotherapists, medical doctor
‣ How: SportConcussion AssessmentTool –5th Edition (SCAT5) Child SportConcussion AssessmentTool –5th Edition (Child SCAT5)
PARACHUTE | Canadian Guideline on Concussion in Sport i15

4. Medical Assessment
4. Medical Assessment
In order to provide comprehensive evaluation of athletes with asuspected concussion, the medical assessmentmustrule outmore serious forms of traumatic brain and spine injuries, mustrule outmedical and neurological conditions thatcan presentwith concussion-like symptoms, and mustmake the diagnosis of concussion based on findings of the clinical history and physical examination and the evidence-based use of adjunctive tests as indicated (i.e. CT scan). In addition to nurse practitioners, the types of medical doctors thatare qualified to evaluate patients with asuspected concussion include2: pediatricians; family medicine, sports medicine, emergency department, internal medicine and rehabilitation (physiatrists) physicians; neurologists; and neurosurgeons.
In geographic regions of Canadawith limited access to medical doctors (i.e. rural or northern communities), alicensed healthcare professional (i.e. nurse) with pre-arranged access to amedical doctor or nurse practitioner can facilitate this role. The medical assessment isresponsible for determining whether the athlete has been diagnosed with aconcussion or not. Athletes with adiagnosed concussion should be provided with aMedical AssessmentLetter indicating aconcussion has been diagnosed. Athletes thatare determined to have notsustained aconcussion mustbe provided with aMedical AssessmentLetter indicating aconcussion has notbeen diagnosed and the athlete can return to school, work and sportactivities withoutrestriction.
‣ Who: Medical doctor, nurse practitioner, nurse
‣ How: Medical AssessmentLetter
2 Medical doctors and nurse practitioners are the only healthcare professionals in Canadawith licensed training and expertise to meetthese needs; therefore all athletes with asuspected concussion should undergo evaluation by one of these professionals.
PARACHUTE | Canadian Guideline on Concussion in Sport i16

5. Concussion Management5. Concussion Management
When an athlete has been diagnosed with aconcussion, itis importantthatthe athlete’s parent/legal guardian or spouse is informed. All athletes diagnosed with aconcussion mustbe provided with astandardized Medical AssessmentLetter thatnotifies the athlete and their parents/legal guardian/spouse thatthey have been diagnosed with aconcussion and may notreturn to any activities with arisk of concussion (such as sport) until medically cleared to do so by amedical doctor or nurse practitioner. Because the Medical AssessmentLetter contains personal health information, itis the responsibility of the athlete or their parent/legal guardian to provide this documentation to the athlete’s coaches, teachers, or employers. Itis also importantfor the athlete to provide this information to sportorganization officials thatare responsible for injury reporting and concussion surveillance where applicable.
Athletes diagnosed with aconcussion should be provided with education aboutthe signs and symptoms of concussion, strategies abouthow to manage their symptoms, the risks of returning to sportwithoutmedical clearance and recommendations regarding agradual return to school and sportactivities. Athletes diagnosed with aconcussion are to be managed according to their Return-to-School and Sport-SpecificReturn-to-SportStrategies under the supervision of amedical doctor or nurse practitioner. When available, athletes should be encouraged to work with the team athletic therapistor physiotherapistto optimize progression through their Sport-SpecificReturn-to-SportStrategy. Once the athlete has completed their Return-to-School and Sport-SpecificReturn-to-SportStrategies and are deemed to be clinically recovered from their concussion, the medical doctor or nurse practitioner can consider the athlete for areturn to full sportactivities and issue aMedical Clearance Letter.
The stepwise progressionsfor Return-to-School and Return-to-SportStrategies are outlined below. As indicated in stage 1 of the Return-to-SportStrategy, reintroduction of daily, school, and work activities using the Return-to-School Strategy mustprecede return to sportparticipation.
Return-to-School Strategy The following is an outline of the Return-to-School Strategy thatshould be used to help student-athletes, parents, and teachers to partner in allowing the athlete to make agradual return to school activities (Table 1). Depending on the severity and type of the symptoms present, student-athletes will progress through the following stages atdifferentrates. If the student-athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage. Athletes should also be encouraged to ask their school if they have aschool-specific Return-to-Learn Program in place to help student-athletes make agradual return to school.
PARACHUTE | Canadian Guideline on Concussion in Sport i17

Table 1. Return-to-School Strategy: Graduated Approach3
1
2
3
4
Stage Aim
Daily activities athome thatdo notgive the student-athlete symptoms
School activities
Return to school part-time
Return to school full-time
Activity
Typical activities during the day as long as they do notincrease symptoms (i.e. reading, texting, screen time). Startat5-15 minutes atatime and gradually build up.
Homework, reading or other cognitive activities outside of the classroom.
Gradual introduction of schoolwork. Increase academic May need to startwith apartial activities. school day or with increased breaks during the day.
Gradually progress. Return to full academic activities and catch up onmissedschoolwork.
Goal ofeach step
Gradual return to typical activities
Increase tolerance to cognitive work.
Sport-Specific Return-to-SportStrategyThe following is an outline of the Return-to-SportStrategy thatshould be used to help athletes, parents, coaches, trainers, teachers, and medical professionals to partner in allowing the athlete to make agradual return to sportactivities (Table 2). Activities should be tailored to create asport-specific strategy thathelps the athlete return to their respective sport.
An initial period of 24-48 hours of restis recommended before starting their Sport-SpecificReturn-to-SportStrategy. If the athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage. Itis importantthatyouth and adultstudent-athletes return to full-time school activities before progressing to stage 5 and 6 of the Sport-SpecificReturn-to-SportStrategy. Itis also importantthatall athletes provide their coach with aMedical Clearance Letter prior to returning to full contactsportactivities.
3McCrory etal. (2017).
PARACHUTE | Canadian Guideline on Concussion in Sport i18
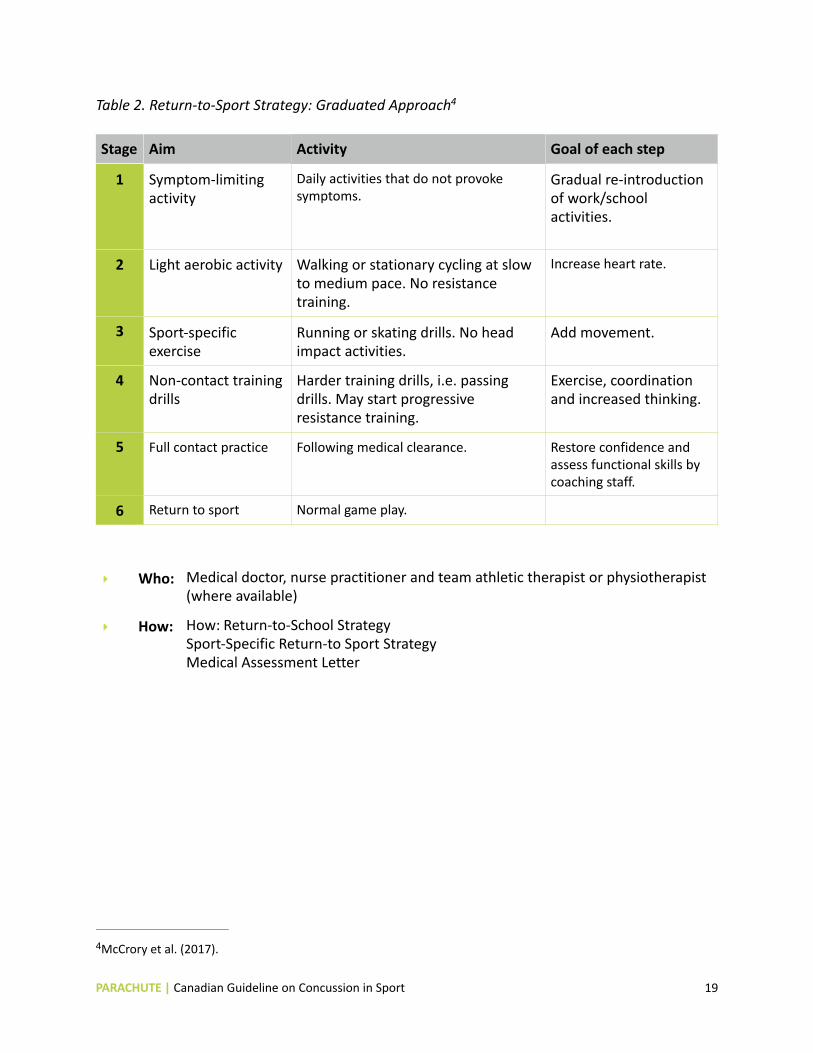
Table 2. Return-to-SportStrategy: Graduated Approach4
1
2
3
4
5
6
Stage Aim
Symptom-limiting activity
Lightaerobic activity
Sport-specific exercise
Non-contacttraining drills
Full contactpractice
Return to sport
Activity
Daily activities thatdo notprovoke symptoms.
Walking or stationary cycling atslow Increase heartrate. to medium pace. No resistance training.
Running or skating drills. No head Add movement. impactactivities.
Harder training drills, i.e. passing drills. May startprogressive resistance training.
Following medical clearance.
Normal game play.
Goal ofeach step
Gradual re-introduction ofwork/schoolactivities.
Exercise, coordination and increased thinking.
Restore confidence and assess functional skills by coaching staff.
‣ Who: Medical doctor, nurse practitioner and team athletic therapistor physiotherapist(where available)
‣ How: How: Return-to-School Strategy Sport-Specific Return-to SportStrategy Medical AssessmentLetter
4McCrory etal. (2017).
PARACHUTE | Canadian Guideline on Concussion in Sport i19

6. Multidisciplinary Concussion Care6. Multidisciplinary Concussion Care
Mostathletes who sustain aconcussion while participating in sportwill make acomplete recovery and be able to return to full school and sportactivities within 1-4 weeks of injury. However, approximately 15-30% of individuals will experience symptoms thatpersistbeyond this time frame. If available, individuals who experience persistentpost-concussion symptoms (>4 weeks for youth athletes, >2 weeks for adultathletes) may benefitfrom referral to amedically-supervised multidisciplinary concussion clinic thathas access to professionals with licensed training in traumatic brain injury thatmay include experts in sportmedicine, neuropsychology, physiotherapy, occupational therapy, neurology, neurosurgery, and rehabilitation medicine.
Referral to amultidisciplinary clinic for assessmentshould be made on an individualized basis atthe discretion of an athlete’s medical doctor or nurse practitioner. If access to amultidisciplinary concussion clinic is notavailable, areferral to amedical doctor with clinical training and experience in concussion (e.g. asportmedicine physician, neurologist, or rehabilitation medicine physician) should be considered for the purposes of developing an individualized treatmentplan. Depending on the clinical presentation of the individual, this treatmentplan may involve avariety of healthcare professionals with areas of expertise thataddress the specific needs of the athlete based on the assessmentfindings.
‣ Who: Multidisciplinary medical team, medical doctor with clinical training and experience in concussion (e.g. asports medicine physician, neurologist, or rehabilitation medicine physician), licensed healthcare professionals
PARACHUTE | Canadian Guideline on Concussion in Sport i20

7.ReturntoSport7.ReturntoSport
Athletes who have been determined to have notsustained aconcussion and those thathave been diagnosed with aconcussion and have successfully completed their Return-to-School and Sport-SpecificReturn-to-SportStrategies can be considered for return to full sportactivities. The final decision to medically clear an athlete to return to full game activity should be based on the clinical judgmentof the medical doctor or nurse practitioner taking into accountthe athlete’s pastmedical history, clinical history, physical examination findings and the results of other tests and clinical consultations where indicated (i.e. neuropsychological testing, diagnostic imaging).
Prior to returning to full contactpractice and game play, each athlete mustprovide their coach with astandardized Medical Clearance Letter thatspecifies thatamedical doctor or nurse practitioner has personally evaluated the patientand has cleared the athlete to return to sport. In geographic regions of Canadawith limited access to medical doctors (i.e. rural or northern communities), alicensed healthcare professional (i.e. anurse) with pre-arranged access to amedical doctor or nurse practitioner can provide this documentation. A copy of the Medical Clearance Letter should also be submitted to sportorganization officials thathave injury reporting and surveillance programs where applicable.
Athletes who have been provided with aMedical Clearance Letter may return to full sportactivities as tolerated. If the athlete experiences any new concussion-like symptoms while returning to play, they should be instructed to stop playing immediately, notify their parents/ legal guardian, coaches, trainer or teachers, and undergo follow-up Medical Assessment. In the eventthatthe athlete sustains anew suspected concussion, the CanadianGuideline onConcussion in Sport should be followed as outlined here.
‣ Who: Medical doctor, nurse practitioner
‣ How: Medical Clearance Letter
PARACHUTE | Canadian Guideline on Concussion in Sport i21

PARACHUTE | Canadian Guideline on Concussion in Sport i22

Canadian Sport Concussion Pathway The figure thatfollows is avisual representation of the decision-making pathway thatreflects the recommendations in this guideline.
PARACHUTE | Canadian Guideline on Concussion in Sport i23

PARACHUTE | Canadian Guideline on Concussion in Sport i24

Guideline Development Process Evidence This guideline was developed using the results of asystematic evidence search and consensus process conducted external to the guideline’s development.
The mostcurrenthigh quality scientific evidence addressing concussion in sportis reviewed roughly every 4 years by the Scientific Committee and ExpertPanel of the International Consensus Conference on Concussion in Sport. The consensus process includes:
• Drafting, feedback, and revision of systematic review questions by the Scientific Committee and ExpertPanel
• Systematic reviews • Submission and review of scientific abstracts to supplementthe systematic reviews with the latestevidence
• Consensus meeting with: public plenary lectures to address the review questions; closed ExpertPanel meeting; and, updating of tools (CRT, SCAT, Child SCAT)
Additional details on the consensus process and methodology are available here: http:// bjsm.bmj.com/content/51/11/873. The results of this process are subsequently published in the form of aconsensus statement, systematic review articles, and tools in the British Journal of Sports Medicine.
The 5th International Consensus Conference on Concussion in Sportwas held October 27-28, 2016 in Berlin, Germany. This iteration of the consensus process included 12 systematic review questions. A new International Consensus Statementon Concussion in Sport, 12 systematic reviews, and updated tools (CRT5, SCAT5, Child SCAT5) were published in April 2017. Three of the lead authors of the Consensus Statement–Dr. Carolyn Emery, Dr. Kathryn Schneider, and Dr. Charles Tator –are members of the ExpertCommittee thatdeveloped this guideline.
The full scope of evidence included in the Consensus Statementand systematic reviews is broader than the scope of this guideline. Selection of the recommendation areas and evidence to include in this guideline was determined by the ExpertCommittee and informed by Russell etal.5’s framework for youth sportconcussion in Canada.
Stakeholder ConsultationA broad group of stakeholders was consulted throughoutthe guideline developmentprocess to ensure the views of end users were considered. The following sectors and professions were included:
5Russell K. etal. (2017). Legislation for youth sportconcussion in Canada: review, conceptual framework and recommendation. Canadian Journal of Neurological Sciences, 44(3), 225-234.
PARACHUTE | Canadian Guideline on Concussion in Sport i25

• Healthcare professionals including: Neurosurgery, Pediatrics, Sports Medicine, Physiotherapy, Occupational Therapy
• Health and sportinjury researchers • National SportOrganization representatives • National MultisportService Organization representatives including coaching • Government• Education
An initial draftof guideline recommendations based on evidence and practice-based expertise was developed by the ExpertCommittee. A national stakeholder eventwas hosted by Parachute in May 2017, where the recommendations were presented to health, sport, and governmentrepresentatives for open discussion. Feedback received was incorporated into subsequentrevisions of the document, which underwentongoing review by the ExpertCommittee and Parachute ProjectTeam.
External review by health, sport, government, and education representatives was the final step for completion of the document.
UpdatestothisGuideline Atthe time of its publication, this guideline reflects the mostcurrenthigh quality evidence on concussion in sport. New scientific evidence and its impacton the areas of recommendation in this guideline will have to be considered as itemerges.
The nextiteration of the consensus conference is expected to occur before December 31, 2020.
PARACHUTE | Canadian Guideline on Concussion in Sport i26

Appendix: Documents & Tools The documents and tools thatfollow are included to supportthe implementation of the recommendations contained in this guideline. They are free to use and distribute.
PARACHUTE | Canadian Guideline on Concussion in Sport i27

PARACHUTE | Canadian Guideline on Concussion in Sport i28

Pre-Season Concussion Education Sheet
WHAT IS ACONCUSSION? A concussion is abrain injury thatcan’tbe seen on x-rays, CT or MRIscans. Itaffects the way an athlete thinks and can cause avariety of symptoms.
WHAT CAUSES ACONCUSSION? Any blow to the head, face or neck, or somewhere else on the body thatcauses asudden jarring of the head may cause aconcussion. Examples include getting body-checked in hockey or hitting one’s head on the floor in gym class.
WHEN SHOULD I SUSPECT ACONCUSSION? A concussion should be suspected in any athlete who sustains asignificantimpactto the head, face, neck, or body and reports ANY symptoms or demonstrates ANY visual signs of aconcussion. A concussion should also be suspected if an athlete reports ANY concussion symptoms to one of their peers, parents, teachers, or coaches or if anyone witnesses an athlete exhibiting ANY of the visual signs of concussion. Some athletes will develop symptoms immediately while others will develop delayed symptoms (beginning 24-48 hours after the injury).
WHAT ARE THE SYMPTOMS OFACONCUSSION? A person does notneed to be knocked out(lose consciousness) to have had aconcussion. Common symptoms include:
‣ Headaches or head pressure ‣ Dizziness ‣ Nauseaand vomiting ‣ Blurred or fuzzy vision ‣ Sensitivity to lightor sound ‣ Balance problems ‣ Feeling tired or having no energy ‣ Notthinking clearly ‣ Feeling slowed down
‣ Easily upsetor angered ‣ Sadness ‣ Nervousness or anxiety ‣ Feeling more emotional ‣ Sleeping more or sleeping less‣ Having ahard time falling asleep ‣ Difficulty working on acomputer ‣ Difficulty reading ‣ Difficulty learning new information
WHAT ARE THE VISUAL SIGNS OFACONCUSSION? Visual signs of aconcussion may include:
‣ Lying motionless on the playing surface ‣ Slow to getup after adirector indirecthitto
the head ‣ Disorientation or confusion or inability to
respond appropriately to questions
‣ Blank or vacantstare ‣ Balance, gaitdifficulties, motor incoordination,
stumbling, slow labored movements ‣ Facial injury after head trauma‣ Clutching head
WHAT SHOULD I DO IFI SUSPECT ACONCUSSION? If any athlete is suspected of sustaining aconcussion during sports they should be immediately removed from play. Any athlete who is suspected of having sustained aconcussion during sports mustnotbe allowed to return to the same game or practice.
It is important that ALL athletes with a suspected concussion undergo medical assessment by a medical doctor or nurse practitioner, as soon as possible. It is also important that ALL athletes with a suspected concussion receive written medical clearancefroma medical doctorornursepractitionerbeforereturningto sport activities.
WHEN CAN THE ATHLETE RETURN TO SCHOOL AND SPORTS? Itis importantthatall athletes diagnosed with aconcussion follow astep-wise return to school and sports-related activities thatincludes the following Return-to-School and Return-to-SportStrategies. Itis importantthatyouth and adultstudent-athletes return to full-time school activities before progressing to stage 5 and 6 of the Return-to-SportStrategy.
PARACHUTE | Canadian Guideline on Concussion in Sport i29

Return-to-School Strategy
1
2
3
4
Stage Aim
Daily activities athome thatdo notgive the student-athlete symptoms
School activities
Return to school part-time
Return to school full-time
Activity
Typical activities during the day as long as they do notincrease symptoms (i.e. reading, texting, screen time). Startat5-15 minutes atatime and gradually build up.
Homework, reading or other cognitive activities outside of the classroom.
Gradual introduction of schoolwork. May need Increase academic activities. to startwith apartial school day or with increased breaks during the day.
Gradually progress. Return to full academic activities and catch up on missed school work.
Goal ofeach step
Gradual return to typical activities
Increase tolerance to cognitive work.
Return-to-Sport Strategy
1
2
3
4
5
6
Stage Aim
Symptom-limiting activity
Lightaerobic activity
Sport-specific exercise
Non-contacttraining drills
Full contactpractice
Return to sport
Activity
Daily activities thatdo notprovoke symptoms.
Walking or stationary cycling atslow to medium Increase heartrate. pace. No resistance training.
Running or skating drills. No head impact Add movement. activities.
Harder training drills, i.e. passing drills. May startprogressive resistance training.
Following medical clearance.
Normal game play.
Goal ofeach step
Gradual re-introduction of work/ school activities.
Exercise, coordination and increased thinking.
Restore confidence and assess functional skills by coaching staff.
HOW LONG WILL IT TAKE FORTHE ATHLETE TO RECOVER? Mostathletes who sustain aconcussion will make acomplete recovery within 1-2 weeks while mostyouth athletes will recover within 1-4 weeks. Approximately 15-30% of patients will experience persistentsymptoms (>2 weeks for adults; >4 weeks for youth) thatmay require additional medical assessmentand management.
HOW CAN I HELP PREVENT CONCUSSIONS AND THEIRCONSEQUENCES? Concussion prevention, recognition and managementrequire athletes to follow the rules and regulations of their sport, respecttheir opponents, avoid head contact, and reportsuspected concussions.
TO LEARN MORE ABOUT CONCUSSIONS PLEASE VISIT: Parachute Canada: www.parachutecanada.org/concussion
SIGNATURES (OPTIONAL): The following signatures certify thatthe athlete and his/her parentor legal guardian have reviewed the above information related to concussion.
________________________________ ____________________________ __________________Printed name of athlete Signature of athlete Date
_________________________________ ____________________________ __________________Printed name of parent Signature of parent
PARACHUTE | Canadian Guideline on Concussion in Sport Date
i30

_____________________________________________________________________________________
_____________________________________________________________________________________________
Medical Assessment Letter
Date: ________________________________
Athlete’s name: ________________________
To whom itmay concern,
Athletes who sustain asuspected concussion should be managed according to the CanadianGuideline onConcussion in Sport. Accordingly, Ihave personally completed aMedical Assessmenton this patient.
Results of Medical Assessment
¨ This patienthas notbeen diagnosed with aconcussion and can resume full participation in school, work, and sportactivities withoutrestriction.
¨ This patienthas notbeen diagnosed with aconcussion butthe assessmentled to the following diagnosis and recommendations:
_____________________________________________________________________________________
¨ This patienthas been diagnosed with aconcussion.
The goal of concussion managementis to allow complete recovery of the patient’s concussion by promoting asafe and gradual return to school and sportactivities. The patienthas been instructed to avoid all recreational and organized sports or activities thatcould potentially place them atrisk of another concussion or head injury. Starting on ___________________(date), Iwould ask thatthe patientbe allowed to participate in school and low-risk physical activities as tolerated and only atalevel thatdoes notbring on or worsen their concussion symptoms. The above patientshould notreturn to any full contactpractices or games until the coach has been provided with aMedical Clearance Letter provided by amedical doctor or nurse practitioner in accordance with the CanadianGuideline on Concussion in Sport.
Other comments:
_____________________________________________________________________________________________
Thank-you very much in advance for your understanding.
Yours Sincerely,
Signature/print____________________________________________ M.D. / N.P. (circle appropriate designation)*
*In rural or northern regions, the Medical AssessmentLetter may be completed by a nurse with pre-arranged access to a medical doctor or nurse practitioner. Forms completed by other licensed healthcare professionals should nototherwise be accepted.
We recommend that this document be provided to the athlete withoutcharge.
PARACHUTE | Canadian Guideline on Concussion in Sport i31

Return-to-School Strategy The following is an outline of the Return-to-School Strategy thatshould be used to help student-athletes, parents, and teachers to partner in allowing the athlete to make agradual return to school activities. Depending on the severity and type of the symptoms present, student-athletes will progress through the following stages atdifferentrates. If the student-athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage.
1
2
3
4
Stage Aim
Daily activities at Typical activities during the day as long as home thatdo not they do notincrease symptoms (i.e. give the student reading, texting, screen time). Startat5-15 athlete symptoms minutes atatime and gradually build up.
School activities
Return to school part-time
Return to school full-time
Activity
Homework, reading or other cognitive activities outside of the classroom.
Gradual introduction of schoolwork. May Increase academic activities. need to startwith apartial school day or with increased breaks during the day.
Gradually progress. Return to full academic activities and catch up on missed school work.
Goal ofeach step
Gradual return to typical activities
Increase tolerance to cognitive work.
1
2
-
Sport-Specific Return-to-SportStrategyThe following is an outline of the Return-to-SportStrategy thatshould be used to help athletes, coaches, trainers, and medical professionals to partner in allowing the athlete to make agradual return to sportactivities. Activities should be tailored to create asport-specific strategy thathelps the athlete return to their respective sport.
An initial period of 24-48 hours of restis recommended before starting their Sport-SpecificReturn-to-SportStrategy. If the athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage. Itis importantthatyouth and adultstudent-athletes return to full-time school activities before progressing to stage 5 and 6 of the Sport-SpecificReturn-to-SportStrategy. Itis also importantthatall athletes provide their coach with aMedical Clearance Letter prior to returning to full contactsportactivities.
Stage Aim
Symptom-limiting activity
Lightaerobic Walking or stationary cycling atslow to Increase heartrate. activity medium pace. No resistance training.
Sport-specific Running or skating drills. No head impact Add movement. exercise activities.
Non-contacttraining drills
Full contactpractice
Return to sport
Activity
Daily activities thatdo notprovoke symptoms.
Harder training drills, i.e. passing drills. May startprogressive resistance training.
Following medical clearance.
Normal game play.
Goal ofeach step
Gradual re-introduction of work/school activities.
Exercise, coordination and increased thinking.
Restore confidence and assess functional skills by coaching staff.
Source: McCrory etal. (2017). Consensus statementon concussion in sport–the 5th international conference on concussion in sportheld in Berlin, October 2016. British Journal of Sports Medicine, 51(11), 838-847.http://dx.doi.org/10.1136/bjsports-2017-097699
PARACHUTE | Canadian Guideline on Concussion in Sport i32
3
4
5
6

_____________________________________________________________________________________________
_____________________________________________________________________________________________
Medical Clearance Letter
Date: __________________________________
Athlete’s name: __________________________
To whom itmay concern,
Athletes who are diagnosed with aconcussion should be managed according to the CanadianGuideline onConcussion in Sport including the Return-to-School and Return-to-SportStrategies (see page 2 of this letter). Accordingly, the above athlete has been medically cleared to participate in the following activities as tolerated effective the date stated above (please check all thatapply):
¨ Symptom-limiting activity (cognitive and physical activities that don’t provoke symptoms)
¨ Light aerobic activity (Walking or stationary cycling at slow to medium pace. No resistance training)
¨ Sport-specific exercise (Running or skating drills. No head impact activities)
¨ Non-contact practice (Harder training drills, e.g. passing drills. May start progressive resistance training. Including gym class activities without a riskof contact, e.g. tennis, running, swimming)
¨ Full-contact practice (Including gym class activities with riskof contact and head impact, e.g. soccer, dodgeball,basketball)
¨ Full game play
What ifsymptomsrecur? Any athlete who has been cleared for physical activities, gym class or non-contactpractice, and who has arecurrence of symptoms, should immediately remove himself or herself from the activity and inform the teacher or coach. If the symptoms subside, the athlete may continue to participate in these activities as tolerated.
Athletes who have been cleared for full contactpractice or game play mustbe able to participate in full-time school (or normal cognitive activity) as well as high intensity resistance and endurance exercise (including non-contactpractice) withoutsymptom recurrence. Any athlete who has been cleared for full-contactpractice or full game play and has arecurrence of symptoms, should immediately remove himself or herself from play, inform their teacher or coach, and undergo Medical Assessmentby amedical doctor or nurse practitioner before returning to full-contactpractice or games.
Any athlete who returns to practices or games and sustains anew suspected concussion should be managed according to the Canadian Guideline on Concussion in Sport.
Other comments:
Thank-you very much in advance for your understanding.
Yours Sincerely,
Signature/print_____________________________________________M.D. / N.P. (circle appropriate designation)*
*In rural or northern regions, the Medical Clearance Letter may be completed by a nurse with pre-arranged access to a medical doctor or nurse practitioner. Forms completed by other licensed healthcare professionals should nototherwise be accepted.
We recommend that this document be provided to the athlete withoutcharge. PARACHUTE | Canadian Guideline on Concussion in Sport i33

1
2
3
4
1
2
Return-to-School Strategy The following is an outline of the Return-to-School Strategy thatshould be used to help student-athletes, parents, and teachers to partner in allowing the athlete to make agradual return to school activities. Depending on the severity and type of the symptoms present, student-athletes will progress through the following stages atdifferentrates. If the student-athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage.
Stage Aim
Daily activities at Typical activities during the day as long as they home thatdo not do notincrease symptoms (i.e. reading, texting, give the student- screen time). Startat5-15 minutes atatime and athlete symptoms gradually build up.
School activities
Return to school part-time
Return to school full-time
Activity
Homework, reading or other cognitive activities outside of the classroom.
Gradual introduction of schoolwork. May need Increase academic activities. to startwith apartial school day or with increased breaks during the day.
Gradually progress. Return to full academic activities and catch up on missed school work.
Goal ofeach step
Gradual return to typical activities
Increase tolerance to cognitive work.
Sport-Specific Return-to-SportStrategyThe following is an outline of the Return-to-SportStrategy thatshould be used to help athletes, coaches, trainers, and medical professionals to partner in allowing the athlete to make agradual return to sportactivities. Activities should be tailored to create asport-specific strategy thathelps the athlete return to their respective sport.
An initial period of 24-48 hours of restis recommended before starting their Sport-SpecificReturn-to-SportStrategy. If the athlete experiences new symptoms or worsening symptoms atany stage, they should go back to the previous stage. Itis importantthatyouth and adultstudent-athletes return to full-time school activities before progressing to stage 5 and 6 of the Sport-SpecificReturn-to-SportStrategy. Itis also importantthatall athletes provide their coach with aMedical Clearance Letter prior to returning to full contactsportactivities.
Stage Aim
Symptom-limiting activity
Lightaerobic Walking or stationary cycling atslow to Increase heartrate. activity medium pace. No resistance training.
Sport-specific Running or skating drills. No head impact Add movement. exercise activities.
Non-contacttraining drills
Full contactpractice
Return to sport
Activity
Daily activities thatdo notprovoke symptoms.
Harder training drills, i.e. passing drills. May startprogressive resistance training.
Following medical clearance.
Normal game play.
Goal ofeach step
Gradual re-introduction of work/school activities.
Exercise, coordination and increased thinking.
Restore confidence and assess functional skills by coaching staff.
Source: McCrory etal. (2017). Consensus statementon concussion in sport–the 5th international conference on concussion in sportheld in Berlin, October 2016. British Journal of Sports Medicine, 51(11), 838-847.http://dx.doi.org/10.1136/bjsports-2017-097699
PARACHUTE | Canadian Guideline on Concussion in Sport i34
3
4
5
6

Concussion Recognition Tool –5th Edition (CRT5) ‣ Available online: http://bjsm.bmj.com/content/bjsports/51/11/872.full.pdf
PARACHUTE | Canadian Guideline on Concussion in Sport i35

PARACHUTE | Canadian Guideline on Concussion in Sport i36

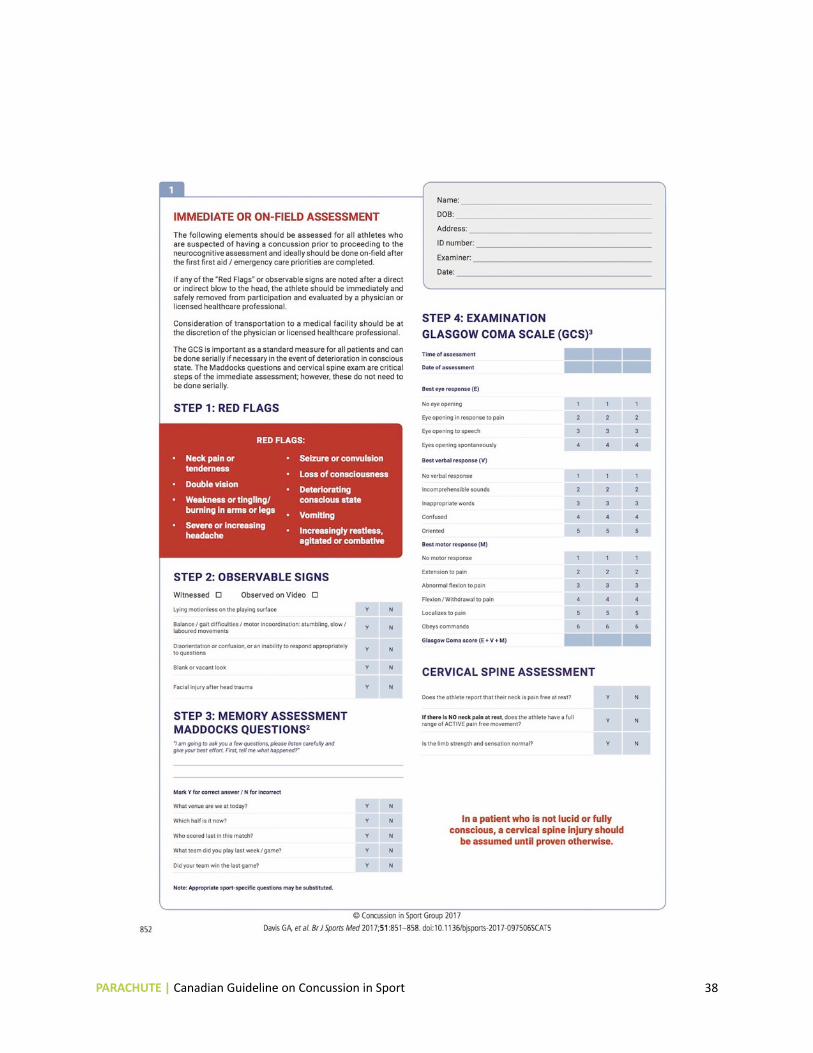
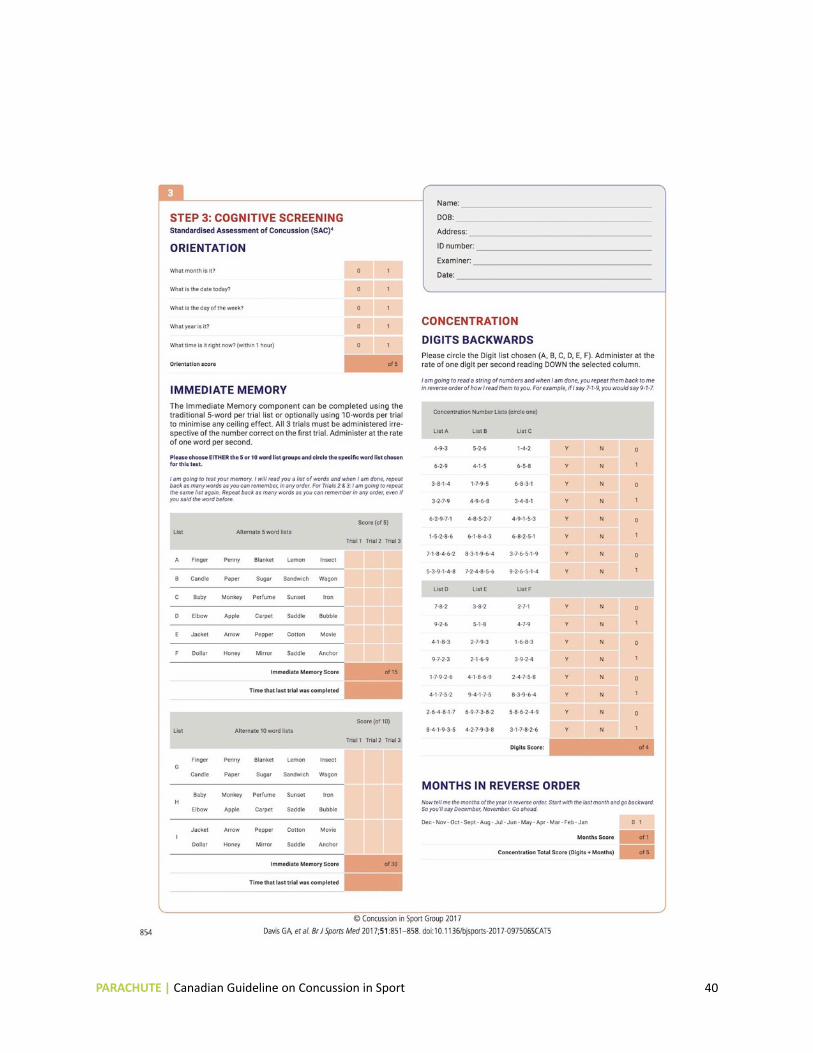
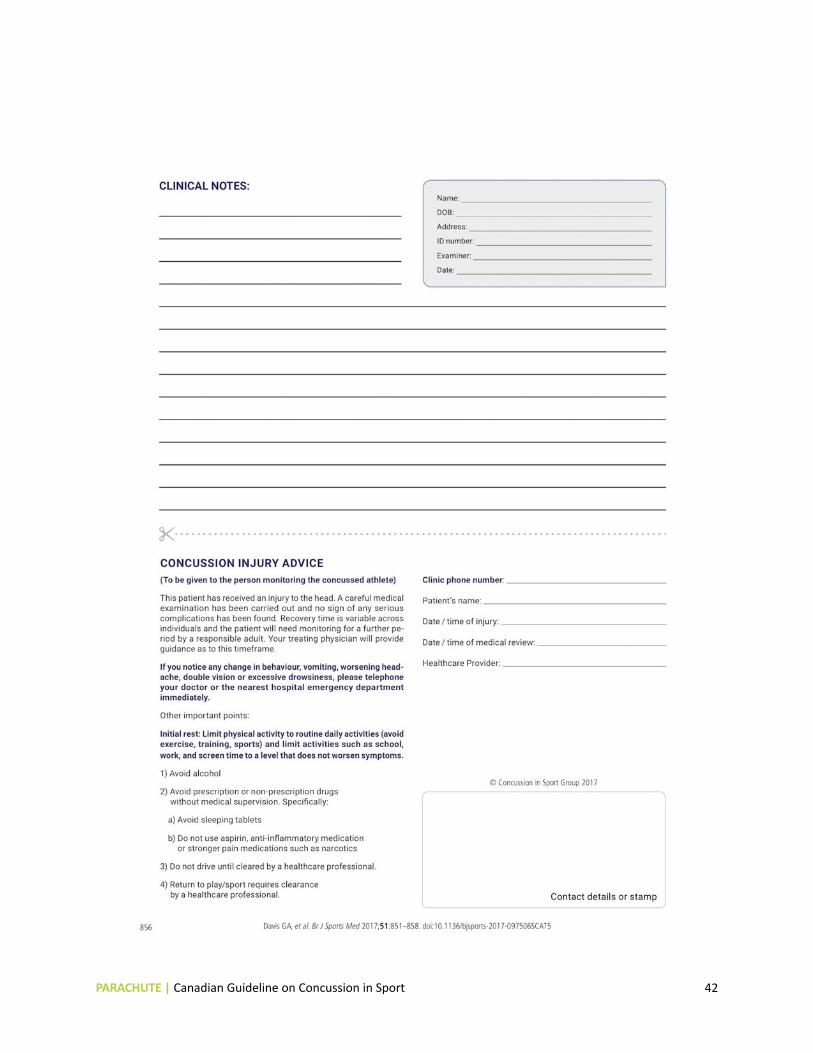
Sport Concussion Assessment Tool –5th Edition (SCAT5) ‣ Available online: http://bjsm.bmj.com/content/bjsports/51/11/851.full.pdf
PARACHUTE | Canadian Guideline on Concussion in Sport i37
PARACHUTE | Canadian Guideline on Concussion in Sport i38

PARACHUTE | Canadian Guideline on Concussion in Sport i39
PARACHUTE | Canadian Guideline on Concussion in Sport i40

PARACHUTE | Canadian Guideline on Concussion in Sport i41
PARACHUTE | Canadian Guideline on Concussion in Sport i42

PARACHUTE | Canadian Guideline on Concussion in Sport i43

PARACHUTE | Canadian Guideline on Concussion in Sport i44

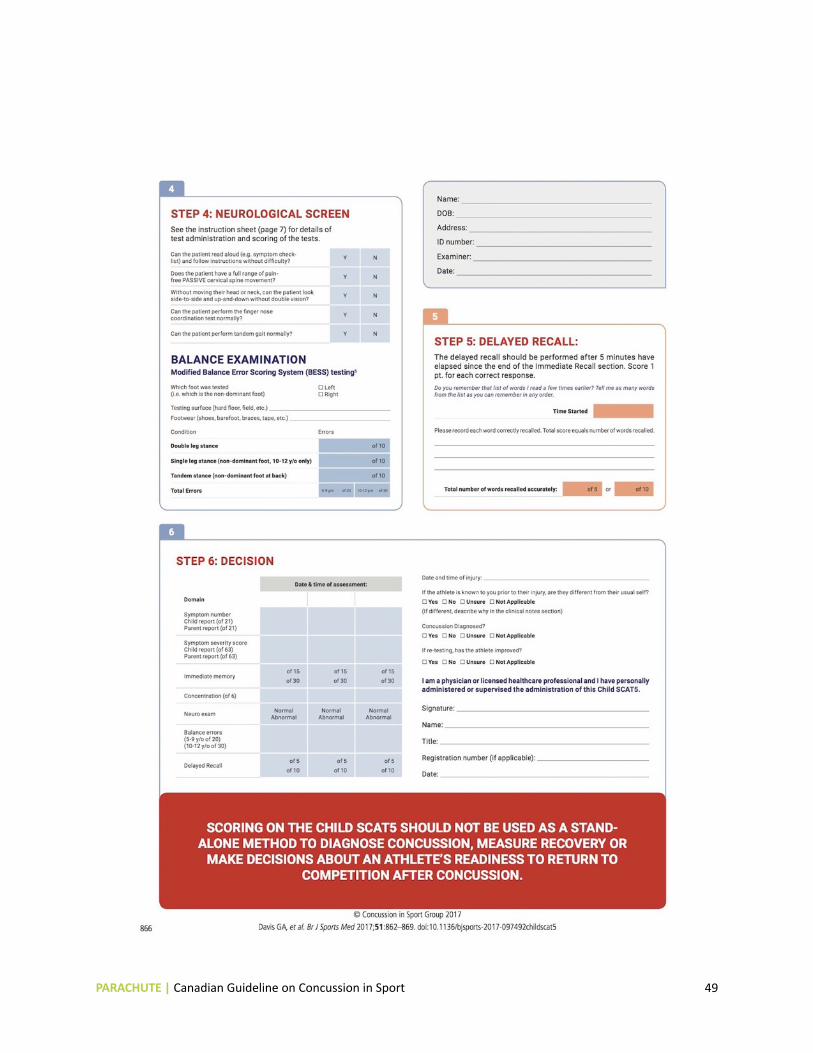
Child Sport Concussion Assessment Tool –5th Edition (Child SCAT5) ‣ Available online: http://bjsm.bmj.com/content/bjsports/51/11/862.full.pdf
PARACHUTE | Canadian Guideline on Concussion in Sport i45

PARACHUTE | Canadian Guideline on Concussion in Sport i46

PARACHUTE | Canadian Guideline on Concussion in Sport i47

PARACHUTE | Canadian Guideline on Concussion in Sport i48
PARACHUTE | Canadian Guideline on Concussion in Sport i49

PARACHUTE | Canadian Guideline on Concussion in Sport i50

PARACHUTE | Canadian Guideline on Concussion in Sport i51

PARACHUTE | Canadian Guideline on Concussion in Sport i52


w w w . p a r a c h u t e . c a


















