
Can we detect prostate cancer in a new way? - Dagens · PDF fileCan we detect prostate cancer...
22
Can we detect prostate cancer in a new way? Urologisk kreft Radiumhospitalet, Oslo, March 31 st , 2016 Tobias Nordström M.D. Ph.D. Danderyds Hospital Dpt Medical Epidemiology and Biostatistics, Karolinska Institutet Tobias Nordström, MEB Karolinska Institutet
Transcript of Can we detect prostate cancer in a new way? - Dagens · PDF fileCan we detect prostate cancer...

Can we detect prostate cancer in a new way?
Urologisk kreft Radiumhospitalet, Oslo, March 31st, 2016
Tobias Nordström M.D. Ph.D. Danderyds Hospital Dpt Medical Epidemiology and Biostatistics, Karolinska Institutet
Tobias Nordström, MEB Karolinska Institutet
Outline
Testing for prostate cancer is common, unstructured and unequal The STHLM3 study – published and unpublished results Next steps – a new diagnostic chain
2 Tobias Nordström, MEB Karolinska Institutet

Data from The Stockholm PSA and Biopsy Registry shows a de-facto, unstructured, screening with PSA in Stockholm
130,000 PSA tests and 5,000 biopsies taken yearly
2,000 prostate cancers/year
65% of all men aged 50-69 has taken at least one PSA-test in the last 5 years
Stockholm PSA and Biopsy Registry Data from 450,000 men All testing in Stockholm since 2003 Complete records • All PSA-test • All biopsy/pathology
results • Detailed information
on all cancers
Ref: “Prostate-specific Antigen (PSA) Testing Is Prevalent and Increasing in Stockholm County, Sweden”, European Urology 2013 3 Tobias Nordström, MEB Karolinska Institutet

But today’s unstructured screening with PSA in Stockholm is not optimal
38% of men with PSA < 1 takes a new test in 2.5 years
60% of all men biopsies are negative
50% of all cancers diagnosed are Gleason 6
Source: Stockholm PSA and Biopsy Registry 4 Tobias Nordström, MEB Karolinska Institutet

Today’s screening with PSA is unequal
Share that had a PSA taken (10 years) Share with increased PSA (4-10 ng/ml) followed-up with biopsy within 12 months
Lower educational level
[≤ 9 years]
54%
27%
Higher educational level
[≥ 13 years]
61%
40%
Ref: “A population-based study on the association between educational length, prostate-specific antigen testing and use of prostate biopsies“, Scand J Urology 2015
5 Tobias Nordström, MEB Karolinska Institutet

The Challenge
Develop a better prostate cancer test than PSA Create structure for prostate cancer testing
6 Tobias Nordström, MEB Karolinska Institutet

Testing for prostate cancer is common, unstructured and unequal The STHLM3 study – published and unpublished results Next steps – a new diagnostic chain
7 Tobias Nordström, MEB Karolinska Institutet

STHLM3 is collaboration between Stockholm County Council and Karolinska Institutet to develop a better prostate cancer test
• Develop a new prostate cancer test that can replace PSA
• Identify at least as many aggressive
cancers as PSA • Significantly reduce number of
biopsies • Demonstrate good health economy • Combine many existing markers
Objective Conditions Method
STHLM3
8 Tobias Nordström, MEB Karolinska Institutet

We have followed a structured process to identify the best markers for the STHLM3 Test
Literature screening of 1,000+ potential plasma and genetic markers
150+ plasma markers evaluated 2011-2012
STHLM3 Test calibrated Collection on PSA 1-3 data Test of logistics 2012
Step 1 Literature Search
Step 2 STHLM2 Cohort [26,000 men]
Step 3 STHLM3 Training [11,130 men]
Step 4 STHLM3 Validation [47,688 men]
Prospective evaluation of STHLM3 Test 2013-2014
9 Tobias Nordström, MEB Karolinska Institutet

STHLM3 combines biomarkers and clinical data into the STHLM3 Test
• Total PSA • Free PSA • Intact PSA • hK2 • MSMB • MIC-1
• Protein markers
• Genetic markers
• Clinical data
STHLM3 Test
= f
Risk factors • Age • Family history • Previous biopsy
* Only measured on biopsied men
Prostate Exam • Prostate volume* • DRE*
10 Tobias Nordström, MEB Karolinska Institutet

STHLM3 in numbers
145,905 men in Stockholm invited
58,818 men recruited 6,777 men biopsied
11 Tobias Nordström, MEB Karolinska Institutet

We have conducted three major analyses
Implement population based screening with the STHLM3 Test What would be the effects of population based screening with the STHLM3 Test? Replace clinical practice using PSA with the STHLM3 Test What would be the effects of replacing current clinical practice with the the STHLM3 Test with equal sensitivity to find aggressive prostate cancer as today? Health Economy What does the STHLM3 Test mean from a health economy perspective?
1
2
3
12 Tobias Nordström, MEB Karolinska Institutet

Population based screening with the STHLM3 Test
13 Tobias Nordström, MEB Karolinska Institutet

In population based screening the STHLM3 Test reduces biopsies with 32% with equal number of aggressive cancers
STHLM3 in population based screening versus PSA≥3
32% less biopsies
Equal number of GS7+
17% less GS6
44% less biopsies in men without cancer
Ref: ”STHLM3: A prospective population-based diagnostic study for prostate cancer screening in men 50-69 years”, Lancet Oncology, 2015 14 Tobias Nordström, MEB Karolinska Institutet

All markers have significant value for the result
Ref: ”STHLM3: A prospective population-based diagnostic study for prostate cancer screening in men 50-69 years”, Lancet Oncology, 2015
Marker Total PSA Age Family history Previous biopsies Genetic score
MSMB MIC1 Free PSA Intact PSA HK2 DRE
Prostate volume
Multivariate P-value
0.008
<0.001 0.004
<0.001
0.006 <0.001 0.047
<0.001 <0.001 <0.001
<0.001 <0.001
Risk factors Biomarkers
Prostate exam
Univariate P-value
<0.001
<0.001 0.005
<0.001
<0.001 <0.001 <0.001 <0.001 0.194
<0.001
<0.001 <0.001
15 Tobias Nordström, MEB Karolinska Institutet

The STHLM3 test identifies more GS7+ versus PSA
PSA 1 - 2 PSA 2 - 3 PSA 3 - 4 PSA 4 - 5 PSA 5 - 10
9%
23%
22%
25%
25%
12%
15%
19%
PSA STHLM3 Test
0%
0%
Share Gleason 7+ for PSA and STHLM3 in different PSA intervalls
Ref: ”STHLM3: A prospective population-based diagnostic study for prostate cancer screening in men 50-69 years”, Lancet Oncology, 2015 16 Tobias Nordström, MEB Karolinska Institutet
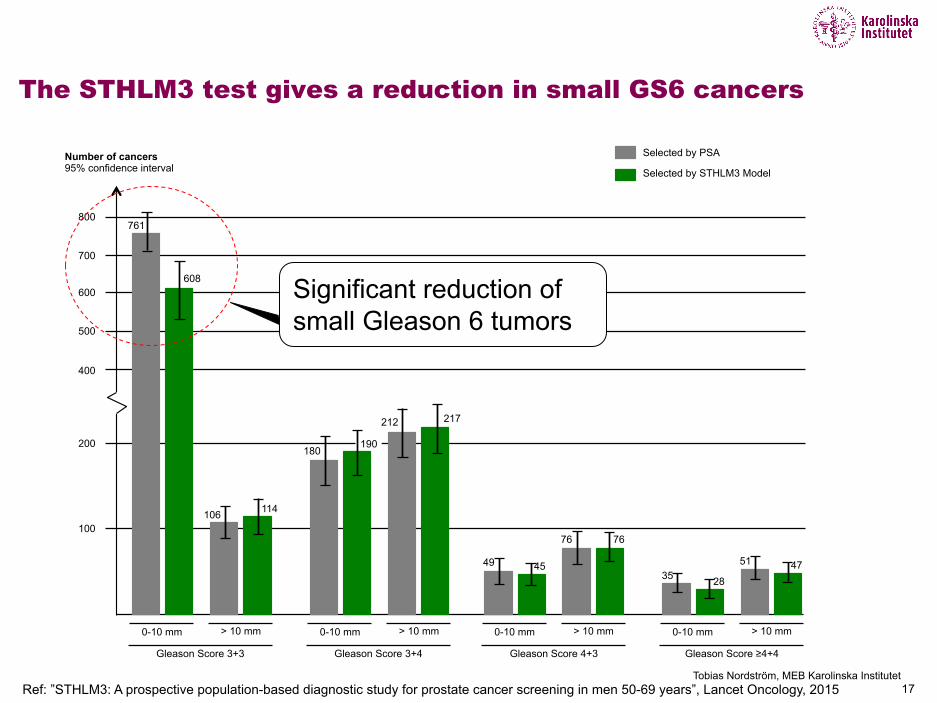
The STHLM3 test gives a reduction in small GS6 cancers
Selected by PSA
Selected by STHLM3 Model
0-10 mm
Gleason Score 3+3
> 10 mm 0-10 mm
Gleason Score 3+4
> 10 mm 0-10 mm
Gleason Score 4+3
> 10 mm 0-10 mm
Gleason Score ≥4+4
> 10 mm
700
600
500
400
200
100
761
608
106 114
180 190
212 217
49 45
76 76
35 28
51 47
Number of cancers 95% confidence interval
800
Significant reduction of small Gleason 6 tumors
Ref: ”STHLM3: A prospective population-based diagnostic study for prostate cancer screening in men 50-69 years”, Lancet Oncology, 2015 17 Tobias Nordström, MEB Karolinska Institutet

The STHLM3 Test works equally well in different age strata
Age 50-54 55-59 60-64 65-69 50-69
Participants
10,276
10,827
11,029
15,478
47,610
Biopsies 466 840 1337 2,304 4,947
Biopsy outcome
Benign 292 (62%) 547 (65%) 845 (63%) 1397 (61%) 3,081
Gleason Score 6
111 (24%) 201 (24%) 295 (22%) 521 (23%) 1,128
Gleason Score ≥7
63 (14%) 92 (11%) 197 (15%) 386 (17%) 738
Saved biopsies
All 35% 41% 30% 34% 32%
Gleason Score 6
30% 26% 16% 16% 17%
Benign 45% 53% 41% 50% 44%
Ref: ”STHLM3: A prospective population-based diagnostic study for prostate cancer screening in men 50-69 years”, Lancet Oncology, 2015 18 Tobias Nordström, MEB Karolinska Institutet

Replace Current Clinical Practice with the STHLM3 Test
Total PSA, Free PSA, Family history, Age, Earlier prostate biopsies, Prostate volume, DRE
19 Tobias Nordström, MEB Karolinska Institutet

Testing for prostate cancer is common, unstructured and unequal The STHLM3 study – published and unpublished results Next steps – a new diagnostic chain
20 Tobias Nordström, MEB Karolinska Institutet

Next steps
Evaluate STHLM3 in clinical practice in primary health care in Stockholm Evaluate STHLM3 in combination with MRI and guided biopsies
21 Tobias Nordström, MEB Karolinska Institutet

Acknowledgements
STHLM3 Core
STHLM3 Scientific Advisory Board Pathology Urology KI Biobank
Henrik Grönberg Martin Eklund Markus Aly Jan Adolfsson Freddie Hamdy Ken Muir Lars Egevad Olof Jansson Magnus Törnblom Christer Kihlfors Lars Häggarth Ulf Leander Lennart Wagrell Anders Hallin Mark Divers James Thompson Anki Carman Amina Said
Funding Mark Clememets Johan Lindberg Astrid Björklund Jan-Erik Damper Jonas Hugosson Anders Bjartell Caroline Elmér Bo Jacobsson Mikael Lagerqvist Lundholm C-G Nettelbladt Renström Peter Arnelöv Cecilia Agarth Carita Björkman
Tobias Nordström Carin Cavalli-Björkman Britt-Marie Hune Peter Wikund Peter Albertsen Ian Thompson Håkan Ageheim Magnus Annerstedt Linnea Ekström Ehn Andreas Thorstenson Dushanka Kristiansson Daniel Altman Ulf Bergerheim Tove Rylander Rudqvist Rafat Samara Staffan Bergh Emma Ridell 22


















