
CAN-ADAPTT AGM 2010 : Population Approaches to Smoking Cessation in Canada October 1 st, 2010...
92
CAN-ADAPTT AGM 2010: Population Approaches to Smoking Cessation in Canada October 1 st , 2010 Ottawa, Ontario
-
Upload
dwain-gibbs -
Category
Documents
-
view
213 -
download
0
Transcript of CAN-ADAPTT AGM 2010 : Population Approaches to Smoking Cessation in Canada October 1 st, 2010...

CAN-ADAPTT AGM 2010:Population Approaches to Smoking
Cessation in Canada
October 1st, 2010Ottawa, Ontario

Welcome/Bienvenue
While we wait to get started Tell people who you are What ‘hat’ you are wearing What you hope to get out of today Favourite vacation location
Name your table……a Fall theme…..

Introduction: CAN-ADAPTT Team
Jess Rogers – Manager Rosa Dragonetti – Clinic manager Janet Ngo – Coordinator, Western Canada Tamar Meyer – Coordinator, Ontario Katie Hunter – Coordinator, Atlantic Canada Stephanie Elliott – Administrative Secretary Dr. Peter Selby – Principal Investigator Dr. John Garcia –Lead, system level
interventions for cessation

Team Members
Executive Committee Evaluation Committee
• Opportunity to get involved
Guideline Development Group Professional Advisory Committee
• Opportunity to get involved

AGENDA
9:00-9:20 Introduction9:20-10:00 Overview of CAN-ADAPTT
progress10:00-10:15 Setting the Stage - P.Selby10:15-10:45 “Population approaches to
tobacco use cessation programming and current capacity in Canada”- J.Garcia
10:45-11:00 Break11:00-12:00 Small group discussion

AGENDA
12:00-12:30 Report back
12:30-1:30 Networking Lunch
1:30-1:45 Where do we go next? – J.Garcia
1:45-3:45 Small group discussion and report back
3:45-4:00 Closing remarks, Next steps - P.Selby and J. Rogers
4:30-6:00 Networking Reception

Objectives for Today
1. Learn about current status of CAN-ADAPTT project: Engagement/Network Membership Dissemination/Implementation Highlights Version 2.0 Launch/Wiki
2. Contribute to development of
CAN-ADAPTT’s population/systems level standards for tobacco use cessation systems

CAN-ADAPTT
Unique guideline development and dissemination project• Practice informed approach• Practice Based Research Network (PBRN)• Dynamic• Online

Dissemination & Engagement• Stakeholders• Professional
Advisory Groups
National Network• Practitioners• Researchers• Policy-makers
Practice-informedResearch Agenda • Seed grants• Discussion board• AGM
Knowledge Translation
• Seed grants• Discussion board
PRACTICERESEARCHCanadian Clinical Practice Guideline

Health Canada Funding
Funding provided by the Drugs and Tobacco Initiatives Program, Health Canada
3 year funding• March 20, 2008 - March 31, 2011

Overview of CAN-ADAPTT Progress
1. Engagement and Network Membership
2. Dissemination/Implementation Highlights
3. Seed Grants and Research Agenda
4. Version 2.0 Launch

1. Engagement and Network Membership

Timeline/Work Plan
March 2008: Focus on provider and practitioner organizations March, 2009: Ontario coordinator October, 2009: Western and Eastern coordinators Spring, 2010: Engagement beyond providers Fall, 2010: Quebec Coordinator

Network Membership
Multi-sectoral
Multi-disciplinary
National

Network Membership
Multi-sectoral
Multi-disciplinary
National
Psychologist
Physician
OT/PT/Chiropractor
Counselor/Therapist/Social Worker
Respiratory Therapist/Asthma Educator
Pharmacist
Dental professional
Nurse professional
Number of Network Members
>700 members across Canada

Network Membership
Multi-sectoral
Multi-disciplinary
National

Member Survey: Reason for Joining the Network
% of participants who identified this reason as their reason for joining “to a great extent”
(n=141)
To conduct practice-informed research to address gaps
To provide input into identifying knowledge gaps
To contribute to promoting the adoption of the guideline
To build relationships/collaboration with tobacco control professionals
To get updates on tobacco control news and events
To gain access to CAN-ADAPTT’s guideline

Moving forward (targets for next 7 months)
Increase Network Membership• Professional representation• Increase regional reach
Launch Version 2.0 on Wiki Platform Translate Version 2.0 in French and launch Launch Version 3.0 Engage Partners, Stakeholders in dissemination
plan Build sustainability around the Network, guideline
and research agenda

2. Dissemination/ Implementation
Highlights

Dissemination/Implementation
National and provincial conferences• Exhibits, poster and oral presentations, workshops
Stakeholder engagement• Regional teleconferences, meetings,
committee/coalition membership
Communications• Stakeholder articles, e-blasts, journals, listservs

Some sense of numbers…..
26 Oral and poster presentations: To a variety of
practitioner and academic audiences
17 Exhibit tables: At a variety of practitioner
conferences across Canada
5 Workshops: Integrating CAN-ADAPTT
guideline in practice/identifying barriers to
implementationPlus, many upcoming dissemination opportunities
confirmed and in development…

CAN-ADAPTT TRAVELS

Western Canada - Highlights
Successes: College of Registered
Dental Hygienists of Alberta (CRDHA)
University of Alberta Dental Hygiene program
Next steps: engagement on applying
the guideline

Ontario - Highlights
Key Successes Canadian and Ontario
Association of Public Health Dentistry conference keynote, workshop
Ontario Respiratory Care Society keynote, workshop

Atlantic Canada – Highlights
Key successes: Significant increase in Atlantic
Canada representation Numerous collaborations/
connections established• across provinces/disciplines
Next Steps: Pursue workshop opportunities

Benefits of Joining
Individuals & organizations
Access to up-to-date clinical practice guideline Opportunities to contribute to the development of Canada’s
first national CPG Links to a variety of resources including websites, projects,
literature reviews and articles Updates on meetings/conferences A discussion board to connect with colleagues, share
resources and comment on the guideline Disseminate and Implement the guideline

3. Seed Grants and Research Agenda

CAN-ADAPTT Seed Grants
23 applications received from across Canada; 12 funded Applicants: researchers, practitioners, and collaborations of
both.
Topic Themes Proposed Products
• Scientific publications• Academic posters• Grant proposals• Collaborative meetings
• Optometry • Women’s health • Addictions• Mental health/ psychiatry• Health sciences
• Specific populations• Role of HCPs• Counselling• Capacity and theory building
Disciplines

Development of a Practice-Informed Research Agenda
Research Agenda
Existing guidelines*
Comprehensive literature
search*
Organizational reports*
CAN-ADAPTT network
feedback*
March 2009-June 2010
Summer 2010 version
Fall 2010 version
Winter 2011 version
Feedback from stakeholders and
collaborating organizations
Ongoing
CAN-ADAPTT Executive committee
September 2010
February 2011
CAN-ADAPTT Network feedback April 2010 (member survey)
October 2010 (AGM)
Ongoing (discussion board)
June 2010- March 2011
Health Canada
submission March 2011
* Details in following section www.can-adaptt.net Updated: June 30, 2010

4. Version 2.0 Launch

Scope of CAN-ADAPTT
Clinical Practice Guideline
Sections Launched• Counselling• Hospital based populations• Youth (Child and Adolescents)• Pregnant and Breastfeeding Women• Mental Health and Other Addictions • Aboriginal Peoples
Upcoming Launches• Pharmacotherapy
Levels of evidence/grade of recommendation

Guideline Development Group
Gerry Brosky, MD (Counselling) Alice Ordean, MD (Pregnant and Breastfeeding Women) Peter Selby, MBBS/ Charl Els, MBChB (Mental Health and
Addictions) Sheila Cote-Meek, PhD (Aboriginal) Bob Reid, PhD (Hospital-based) Jennifer O’Loughlin, PhD (Youth) Paul McDonald, PhD (Pharmacotherapy)

Guideline Development Process

Guideline Development Process
Applied principles of ADAPTE….. Review existing smoking cessation
CPGs (internationally and across disciplines)
CPGs rated using the AGREE instrument Highest-scoring CPGs were used Sections subject to ongoing input by CAN-
ADAPTT network (PBRN, partners etc.)

Version 2.0
Version 2.0
TODAY
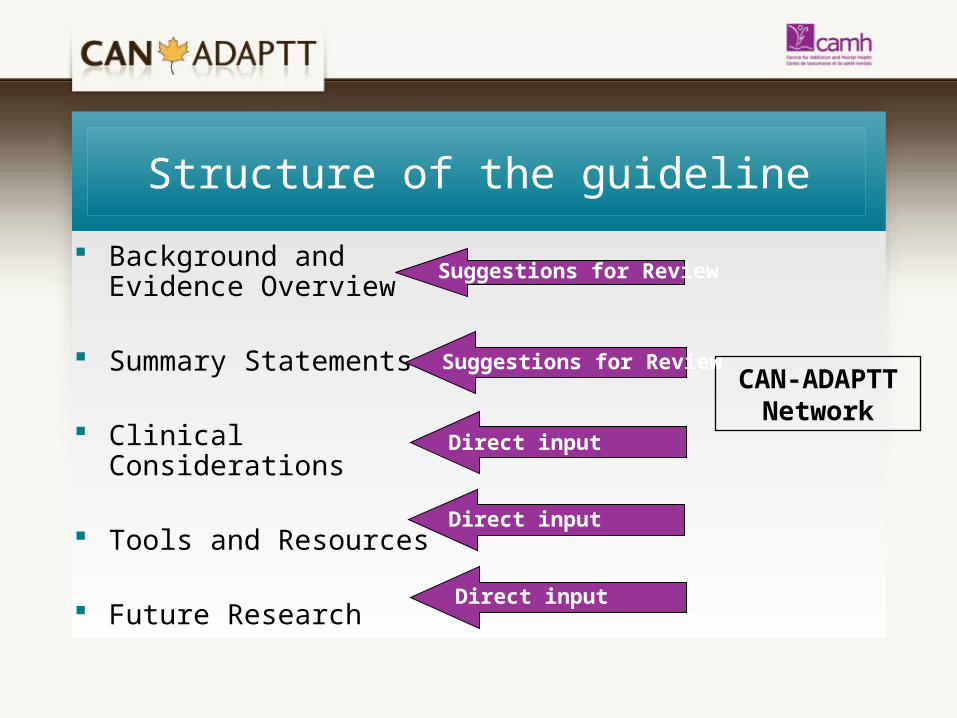
Background and Evidence Overview
Summary Statements
Clinical Considerations
Tools and Resources
Future Research
Structure of the guideline
CAN-ADAPTT Network
Direct input
Direct input
Direct input
Suggestions for Review
Suggestions for Review

Levels of Evidence/Grade of Recommendations
Summary statements are rated based on the GRADE system Required consensus of the Guideline Development Group
Grade of
Recommendation
High
Low
Level of EvidenceWeak Strong
GRADE system of Ratings
1A 1B 1C
2A 2B 2C

Next Steps for the guideline
Integrate outcomes of today’s workshop to create Version 3.0 • Launch date: January 2011
Continue to build clinical considerations• Use of a wiki platform• GDG and network involvement
Continue engagement and dissemination

2.2 Next Steps: Online engagement
Website• New (internal) provider• New website – launching winter 2010
Wiki platform• Launched for AGM (Oct 1)
Twitter• Launching in October

Objective for today….
Inform
CAN-ADAPTT’s guideline on population level approaches for
tobacco use cessation

“Setting the Stage”
Dr. Peter SelbyPrincipal Investigator, CAN-ADAPTT

Setting the Stage…
Opportunity for collaborative approach in developing key principles for an effective smoking cessation system in Canada
Identifying gaps and ways to work together

Society Behaviour and Biology: Making the Case for EBB interventionsT.A. Glass, M.J. McAtee / Social Science & Medicine 62 (2006) 1650–1671

The Smoking Environment in Canada
• About one in five Canadians (5.7 million) 12yrs or older, are daily or occasional smokers*
• Average cigarettes smoked per day = 13.3**
• 37,000 Canadians die from smoking per year
– 100 infants/year• 1 in 5 deaths are due to smoking• 1 in 2 smokers die from smoking-related
diseases
* Canadian Community Health Survey (Statistics Canada), 2010**CTUMS 2009

Burden of Addiction
Smoking rates are higher among:• Young adults• Less than high school education• Blue collar• Mentally ill• Aboriginal• Poor

Never too late to Quit
Quitting smoking at any age may increase life expectancy
Quitting smoking before age 30 = normal life expectancy
Age stop smoking by Life years gained
<30 years 10
<40 years 9
<50 years 6
<60 years 3

“Smoking cessation is a criticalaspect of the management of
many chronic diseases, both interms of treatment outcome,
progression of disease,comorbidities, quality of life, and
survival.”
(Gritz et al., 2007)
“Smoking cessation is a criticalaspect of the management of
many chronic diseases, both interms of treatment outcome,
progression of disease,comorbidities, quality of life, and
survival.”
(Gritz et al., 2007)
Hard things to do….large benefits to doing them….

Providing Smoking Cessation
Many Providers• Physicians, RNs, NPs, Dental Hygenist,
Assistants, Opthalmologists, Chiropractors, Pharmacists, Social Workers, Mental Health Counselors, RTs, etc….
Many Settings• Hospital, Primary Care, Community, Long term
care, Specialty Care, etc.
Opportunities!!!!

Levers and Opportunities
Training of HCPs
Guidelines
Patient/client tools
Provider tools/resources
Incentives
Mass Media
Policy
Priority Setting
Engage community
Research
Clinical Strategies (5A’s, Ottawa Model)
Funding: programs
Funding: pharmacotherapy
Public/Consumers
Existing programmingPartnerships
Opinion leaders/Champions

Need for alignment
Fragmented smoking cessation system across Canada • Information sources (cpg’s, tools etc.)• Settings (clinical, community, hospital, primary
care) • Professionals• Funding• Funding of effective interventions• Educational opportunities in smoking cessation

Provider Approaches
Organizational Level
Population Level Approaches & policy
Importance of alignment and integration of approaches

Intent of the White Paper
Starting point…… Build from evidence, experience and current
capacity to frame the context for smoking cessation guideline
Opportunity today and over Fall 2010 for us to reflect, discuss and revise the White Paper

Today’s Approach
Opportunity to have important conversations in a collaborative way
Helpful hints:• Focus on what matters• Contribute your thinking• Listen to understand• Link and connect ideas• Have FUN! • Be CREATIVE!

Population approaches to tobacco use cessation
programming & current capacity in Canada
60 minutes
John Garcia, PhD

Understand your perspectives on
important components of cessation systems existing challenges and barriers, successes
and where gains can be made emerging opportunities and needs for
smoking cessation system development
What needs to be addressed in a CAN-ADAPTT “System Guideline for Population-based Tobacco Use Cessation”?

Perspectives: Cessation system, What are we talking about?
Clinical Intervention? • Not just a program or intervention
Public Health Approach?• “the organized efforts of society to improve health and well-
being and to reduce inequalities in health” (PHAC)
A goal beyond cessation of tobacco use alone?• Harm reduction – reducing disease, disability and death?
Relationship between tobacco control and cessation?• both a context and the approach?

Exploring Components of Effective Smoking Cessation System(s) Across Canada
CAN-ADAPTT team work to create white paper• Starting place only, stimulate discussion• CDC, IOM, NCI,Ontario (TF, UW, SFO-SAC)
Major components and what we mean:• Goals• Principles• Strategies• Tactics

Tobacco Control – classic goals
1. Preventing tobacco use,
2. Encouraging and motivating quitting tobacco use,
3. Protecting the public from exposure to tobacco smoke, and
4. Denormalization of tobacco and tobacco industry
Tobacco control is not equivalent to cessation Some are questioning this orientation

Cessation System Goals – 6 identified on page 3
Reduce the health consequences (i.e. harm) of the use of tobacco products
Motivate attempts to quit tobacco use Support tobacco users in their efforts to quit
tobacco use

Cessation System Goals (continued)
Facilitate tobacco users stopping use at an earliest age possible
Address the needs of high priority populations to eliminate or reduce inequities in burden of diseases caused by tobacco products (e.g. Aboriginal People, occupational, SES groups), • including those who may be at elevated risk due to
other health conditions (e.g. mentally ill, poly-drug users)

Cessation System Goals (continued)
Encourage repeated sustained quitting and reduction of long-term use in order to reduce health burden among those who have difficulty quitting

Cessation System Goals
Do these goals make sense/resonate?
Alternative goals – for the population-based system?

Key Guiding Principles – page 4 & 5
Tobacco Use Cessation System should be: Continuous – range of interventions,
integrated Goal and Objective Directed Evidence-based Comprehensive and integrated Aligned – across disciplines,
interventions/strategies, decision-makers (across levels)

Key Principles
Build from/include: Strong relationships with smokers
• Not just “one offs”: family members, friends, colleagues
SDOH/Equity and concern for vulnerable populations
Continuous learning cycle• Evidence-inspired, tailoring, continuous improvement
Commitment to invest in research Roles for a range of health care providers, range of
capacities and roles

Proposed structure of a tobacco use cessation system
Strategies
Approaches to achieving the goal(s)
Goals and PrinciplesKey concepts informing the organization and management of the
system
TacticsHow would you go about executing the strategy?
What activities are required? Where would resources be spent?
ActionsPragmatic, action-oriented and implementable tactics necessary to
move toward goals and objectives
This morning
This afternoon
This afternoon

After the break…..Let’s Discuss
1. What is the current status of tobacco use (smoking) cessation systems in Canada?
What’s working well? What are the emerging opportunities for system
development? What are some of the major challenges for
cessation system development?

Evidence and Experience
Focus on areas where there is some degree of evidence around impact, effectiveness and/or trends in practice.
Acknowledge continuous learning cycle and opportunity to build from best practice and experience

BREAK

Small Group Discussion Questions
1. What is the current status of tobacco use (smoking) cessation systems in Canada?
What’s working well? What are the emerging opportunities for system
development? What are some of the major challenges for
cessation system development?
25 minutes

Building from your conversation…..
2. What are the key principles that should be considered in the design of tobacco use cessation systems in Canada?
Please use the White Paper as a starting point only.
Go beyond it and generate new principles.
25 Minutes

Large Group Report Back
Focus your report back on: What were the emerging opportunities? Was there general agreement with the
Principles in the White Paper? What changes/additions did your group
discuss making to the Key Principles?
40 Minutes

Networking Lunch 12:30-1:30
• Visit display tables at the back of the room
• Network with colleagues and meet new people
• Explore CAN-ADAPTT Wiki
• Introduce yourself to the CAN-ADAPTT team!

Welcome Back….
Review discussion from this morning…..

Proposed structure of a tobacco use cessation system
Strategies
Approaches to achieving the goal(s)
Goals and PrinciplesKey concepts informing the organization and management of the
system
TacticsHow would you go about executing the strategy?
What activities are required? Where would resources be spent?
ActionsPragmatic, action-oriented and implementable tactics necessary to
move toward goals and objectives
This morning
This afternoon
This afternoon

Strategies
#1 Planning and Priority Setting
#2 Policy Interventions
#3 Health Communication and Media Interventions for Population Level Tobacco Cessation
#4 Healthcare Setting/Organization and Community Interventions
#5 Population-level Cessation Interventions

Strategies
#6 Training or Building Capacity Among HCP’s in the Provision of Smoking Cessation Interventions
#7 Investment
#8 Evaluation
#9 Surveillance and Monitoring
#10 Alignment and Coordination

White paper….drilling down
World Café Format Opportunity to have important conversations
in a collaborative way
1:40 – 3:45

How does it work?
Discuss specific strategies Round 1: stay at your current table
Quick Report Back Round 2: travel to a new table Round 3: travel to a new table Round 4: return to your original table
Group Discussion

Round #1: Table Talk
Explore the strategy your table has been assigned
Have the important aspects been captured?
Are there additional tactics that could be considered/included?
20 minutes

Report Back
5 minutes/table Introduce the strategy Was there general agreement that the
strategy is important/should be included? What revisions/additions would you
suggest?
40 minutes total

Travel Time
Travel to a NEW table for Round 2 of small group discussion
Table Leads STAY at your first table
5 minutes

Round #2: Table Talk
Have the important and relevant strategies been captured?
What is missing? What needs to be added?
15 minutes

Travel Time
Travel to a NEW table for Round 3 of small group discussion
Table Leads STAY at your first table
5 minutes

Round #3: Table Talk
Table leads take 5 minutes describing what was discussed in Round #2
If there was one thing that hasn’t been said but is needed what is it?
20 minutes

Travel Time
Travel ‘Home’
5 minutes

Large Group Report Back
What key themes emerged?
20 minutes

“Where do we go next?”

Think about….
1. Explore opportunities for collaboration, importance of alignment and how to move forward
2. How might we learn from the experience of different jurisdictions as they implement tobacco use cessation systems across Canada and abroad?

Moving Forward
What needs to happen next week, next month, this year……..beyond?
10 minutes

Wrapping Up
Reflection and Next Steps Evaluation Acknowledgements Thank you Reception

For more information
CAN-ADAPTT
175 College Street
T: 416-535-8501 ext 7427
www.CAN-ADAPTT.net


















