California Hospital Supply Planning Guidance and Toolkit · Hospital Emergency Food Supply Planning...
37
Hospital Preparedness Program California Hospital Emergency Food Supply Planning Guidance and Toolkit October 2013
Transcript of California Hospital Supply Planning Guidance and Toolkit · Hospital Emergency Food Supply Planning...
Hospital Preparedness Program
California Hospital
Emergency Food Supply Planning Guidance and Toolkit
October 2013
California Hospital Association – Hospital Preparedness Program Hospital Emergency Food Supply Planning Guidance and Toolkit
Table of Contents
Section ‐ Document Page
Hospital Emergency Food Planning Guidance (Overview Document) 1
Purpose – Overview 1
Regulatory – Accrediting Agency Overview 1
Guidance‐Recommendations 2
Emergency Food Calculations 2
References‐Additional Resources 3
Exhibit 1 – Emergency Food Planning Flow Diagram 4
Exhibit 2 – Emergency Food Plan – Response Flow Diagram 5
Attachments
Attachment A – Hospital Emergency Food Advisory Group 6
Attachment B – Key Guidance and Recommendations 7
Attachment C – Emergency Food Planning Tool* 9
Attachment D ‐ Emergency Food Planning Tool Instructions
Appendices
Appendix A – Key Regulatory References
Appendix B – Key Accrediting Agency References
19
*An Excel Workbook (Planning Calculation Tool) for use in calculating hospital emergency food supply needs is intended to accompany this Guidance and should be saved with a hospital identifier, date and PLAN in the file name. The file name should be updated each time the Plan (tool) is updated. When the tool is used during an actual event to update assumptions and assess resources against demand and circumstances, the file name should include hospital identifier, date and EVENT in the file name (you may wish to include time).
October 2013
California Hospital Association – Hospital Preparedness Program Hospital Emergency Food Supply Planning Guidance and Toolkit
Purpose
This document is intended to provide guidance and tools to hospitals in planning for, and documenting, emergency food supplies, including meeting regulatory requirements. Included are planning guidelines and assumptions, regulatory references, sample planning calculation tools, and other resources intended to support planning efforts.
Overview
Regulatory and accrediting agencies require hospitals to plan for and document an adequate inventory of on‐site assets and resources, including food supplies for patients for normal, day‐to‐day operations and for emergency situations. Hospitals need to consider and prepare for the potential risks and hazards, and the needs that may arise from those risks, specific to their situation. Hospitals have been cited by regulatory agencies for not having adequate food plans, documentation and/or inventories based on differing interpretation of regulations by those agencies and hospitals. This guidance is intended to assist hospitals with emergency food planning and preparedness consistent with emergency operations plans and current regulatory requirements.
The Planning Guidance and Toolkit was developed by the California Hospital Association (CHA) Hospital Preparedness Program (HPP) through the Hospital Emergency Food Advisory Group (Attachment A). The Advisory Group provided valuable input, references, examples and time to this effort. The Guidance and Toolkit have been reviewed by the California Department of Public Health (CDPH) Division of Licensing and Certification.
Regulatory – Accrediting Agency Overview
Following is a summary of key regulatory references relative to emergency food planning. Appendix A includes the full regulatory language at the time of publication for each reference. Appendix B includes key accrediting agency elements related to emergency food supplies at the time of publication. Note that references focus on food supplies and not on food operations and represent those current at the time this document was published.
Title 22 – Section 70277 specifies that at least a one week (7 days) supply of staple foods (non‐perishable) and two (2) days supply of perishable food shall be maintained on the premises. These food supplies are to be appropriate to meet the requirements of the menu; interpreted to mean to meet patient dietary needs and restrictions (e.g., regular, low sodium, liquid, diabetic, infant, etc.).
Title 22 – Section 70741 further specifies that each hospital shall have a disaster and mass casualty program that includes provisions for the availability of adequate basic utilities and supplies, including gas, water, food and essential medical and supportive materials. As each hospital’s services and situation are different, the definition of adequate is subject to those differences.
42 CFR 482.41(c) (2) CMS Interpretive Guidelines specify that supplies must be maintained to ensure an acceptable level of safety and makes a distinction between supplies needed on a day‐to‐day basis and supplies that are likely to be needed during an emergency.
The Joint Commission requires that each hospital have an Emergency Operations Plan that describes key elements applicable to emergency food supplies:
• Hospital capabilities and response procedures for when the hospital cannot be supported by the local community for at least 96 hours (EM 02.02.01‐3)
• A documented inventory of resources and assets on site that may be needed during an emergency (EM 01.01.01 – 8) • How a facility will obtain and replenish non‐medical resources during a disaster (EM 02.02.03‐3)
1
Hospital Emergency Food Guidance and Toolkit
October 2013
• Plan identifying how a facility will monitor quantities of resources and assets during an emergency (EM 02.02.03‐6) • Plan for how a facility will manage staff support needs during an emergency (EM 02.02.07‐5) as well as staff family
support needs (EM 02.02.07‐6)
The Healthcare Facilities Accreditation Program (HFAP) alternative to TJC requires that hospitals have a plan and emergency food supplies to feed patients, staff and visitors for at least three (3) days.
The National Fire Protection Association (NFPA) 99 specifies that hospitals will have contingency plans for disasters, including stockpiling for ensuring immediate, or at least uninterrupted, access to food supplies (11‐5.3.5(c))
Det Norske Veritas (DNV) Healthcare references the need for the hospital to meet NFPA 99 requirements.
Guidance – Recommendations
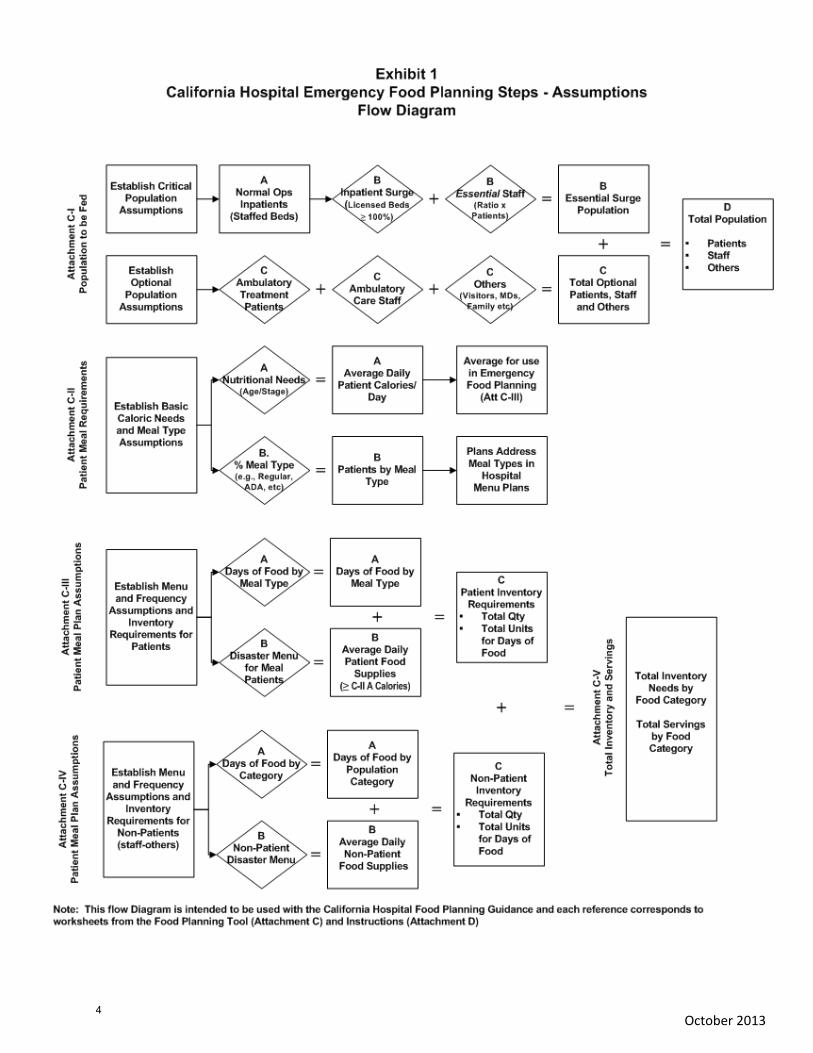
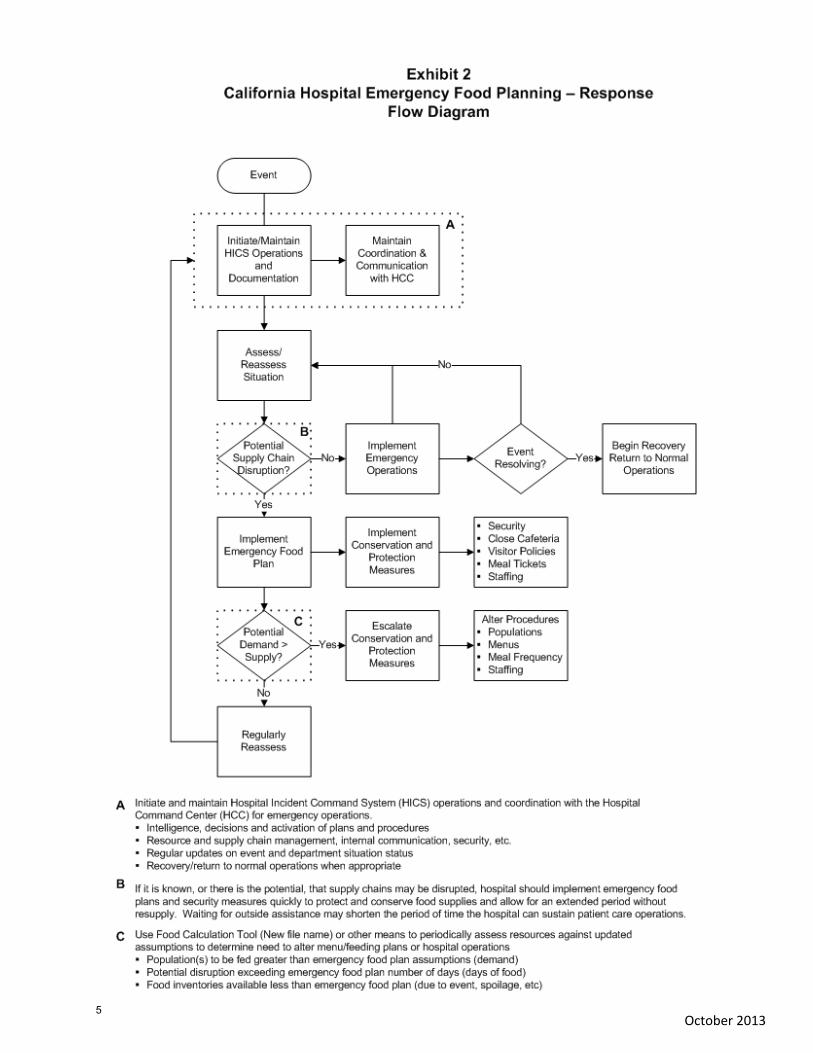
Emergency food plan assumptions should be consistent with the hospital Emergency Operations Plan (EOP) and recognize patient care, and staff who are essential to providing it, as their first priority. This guidance provides a logical process for planning and documenting emergency food plans as outlined in the flow diagram in Exhibit 1. While hospitals may plan based on a logical set of assumptions, disasters may present a different reality and steps may need to be taken during an event to alter plans as outlined in the flow diagram in Exhibit 2. These contingencies should be considered from the outset of an event, keeping the hospitals primary role as a healthcare provider as the focus and priority.
Attachment B includes key recommendations and guidelines for consideration in developing emergency food plans; this document is not a comprehensive checklist for emergency food planning but includes key issues identified by Advisory Group members during their deliberations.
Emergency Food Calculations
Emergency food plans should clearly document calculations and the sources/logic for assumptions used in estimating emergency food needs and inventories. In calculating emergency food supply needs, in addition to consistency with the EOP, there are several practical factors which need to be considered:
Who does the hospital plan to feed (e.g., patients, staff, visitors, physicians, etc) What will each group be fed (meals, MRE, etc) How often will each group be fed (e.g., number of meals, snacks, meal replacements) How food will be delivered (food stations, meal tickets, disposables, security, etc)
Combined, the responses to each question above will result in a calculation of estimated emergency food supply needs. These assumptions should be incorporated into the emergency food plan with the expectation that the hospital will be reviewed by regulatory agencies for compliance against their own plan, even if it exceeds regulatory requirements. Given the costs associated with managing and rotating a large inventory, space limitations and the circumstances that would bring a hospital to activate its emergency food plan, it is recommended that careful consideration be given to developing the assumptions underlying emergency food supply estimates. The recommendations in this guidance incorporate those considerations.
Attachment C is an Emergency Food Planning Calculation Tool and Attachment D includes Instructions for each worksheet in the Calculation Tool. The tool should be modified to be consistent with the hospital’s nutrition care standards and plans and is intended to document emergency food supply assumptions and calculations. It should be saved with a hospital identifier, date and the word “plan” in the file name which should be updated each time the tool is updated. Similarly, the tool assumptions may be updated during an event to assess needs versus inventory and should be saved with a new file name that includes the date and event.
2
Hospital Emergency Food Guidance and Toolkit
October 2013
References – Additional Resources
Following are several references and additional resources related to emergency food supply planning and emergency food operations.
Emergency Food Service: Planning for Disasters, Centre for Emergency Preparedness and Response, Canada Disaster and Emergency Preparedness in Food Service Operations, Puckett and Norton (ISBN‐10: 0880913053) Dietary Reference Intakes (DRI), Institute of Medicine, USDA (www.usda.gov) Emergency Staffing Plan Example (UCSF) www.calhospitalprepare.org/ Example Just‐in‐Time Staff Training Tools (UCSF) www.calhospitalprepare.org/ Patient Emergency Food Menu by Type Example (UCSF) www.calhospitalprepare.org/
3
October 2013 4
October 2013
5
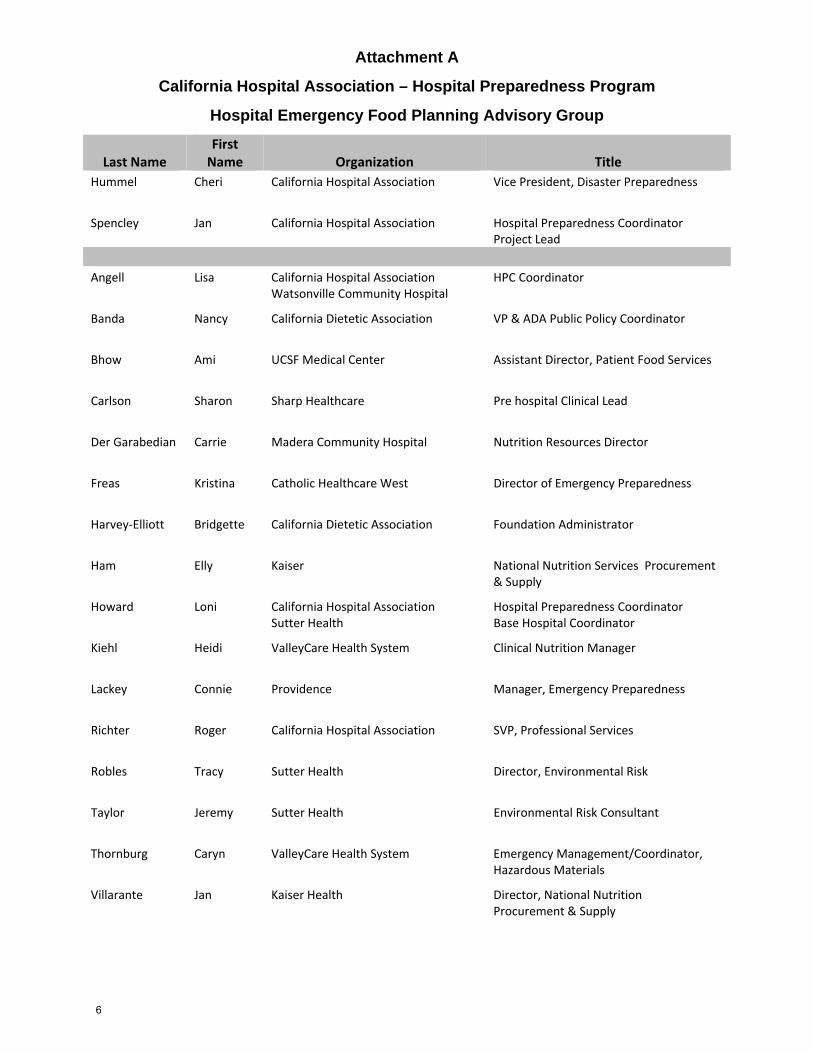
Attachment A
California Hospital Association – Hospital Preparedness Program
Hospital Emergency Food Planning Advisory Group
Last Name First Name Organization Title
Hummel Cheri California Hospital Association Vice President, Disaster Preparedness
Spencley Jan California Hospital Association Hospital Preparedness CoordinatorProject Lead
Angell Lisa California Hospital AssociationWatsonville Community Hospital
HPC Coordinator
Banda Nancy California Dietetic Association VP & ADA Public Policy Coordinator
Bhow Ami UCSF Medical Center Assistant Director, Patient Food Services
Carlson Sharon Sharp Healthcare Pre hospital Clinical Lead
Der Garabedian Carrie Madera Community Hospital Nutrition Resources Director
Freas Kristina Catholic Healthcare West Director of Emergency Preparedness
Harvey‐Elliott Bridgette California Dietetic Association Foundation Administrator
Ham Elly Kaiser National Nutrition Services Procurement & Supply
Howard Loni California Hospital Association Sutter Health
Hospital Preparedness CoordinatorBase Hospital Coordinator
Kiehl Heidi ValleyCare Health System Clinical Nutrition Manager
Lackey Connie Providence Manager, Emergency Preparedness
Richter
Roger California Hospital Association SVP, Professional Services
Robles Tracy Sutter Health Director, Environmental Risk
Taylor Jeremy Sutter Health Environmental Risk Consultant
Thornburg Caryn ValleyCare Health System Emergency Management/Coordinator, Hazardous Materials
Villarante Jan Kaiser Health Director, National Nutrition Procurement & Supply
6
Attachment B
October 31, 2013 AttBEmergFoodGuidelines
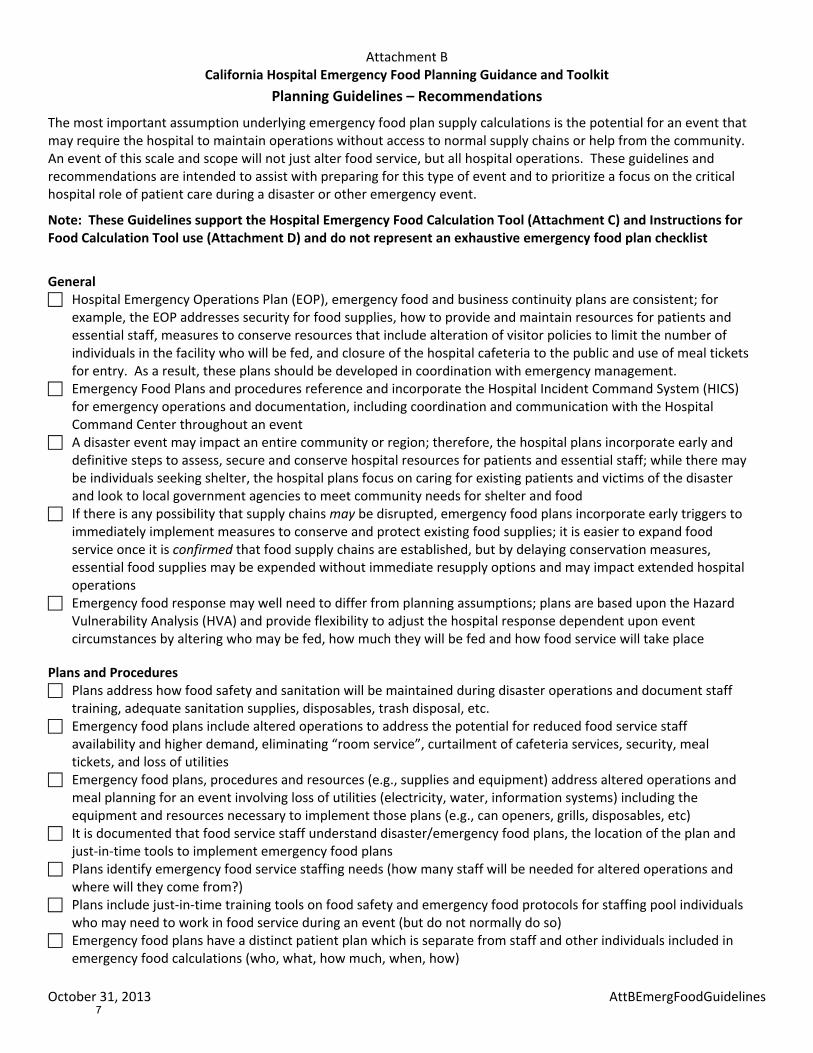
California Hospital Emergency Food Planning Guidance and Toolkit Planning Guidelines – Recommendations
The most important assumption underlying emergency food plan supply calculations is the potential for an event that may require the hospital to maintain operations without access to normal supply chains or help from the community. An event of this scale and scope will not just alter food service, but all hospital operations. These guidelines and recommendations are intended to assist with preparing for this type of event and to prioritize a focus on the critical hospital role of patient care during a disaster or other emergency event.
Note: These Guidelines support the Hospital Emergency Food Calculation Tool (Attachment C) and Instructions for Food Calculation Tool use (Attachment D) and do not represent an exhaustive emergency food plan checklist
General
Hospital Emergency Operations Plan (EOP), emergency food and business continuity plans are consistent; for example, the EOP addresses security for food supplies, how to provide and maintain resources for patients and essential staff, measures to conserve resources that include alteration of visitor policies to limit the number of individuals in the facility who will be fed, and closure of the hospital cafeteria to the public and use of meal tickets for entry. As a result, these plans should be developed in coordination with emergency management.
Emergency Food Plans and procedures reference and incorporate the Hospital Incident Command System (HICS) for emergency operations and documentation, including coordination and communication with the Hospital Command Center throughout an event
A disaster event may impact an entire community or region; therefore, the hospital plans incorporate early and definitive steps to assess, secure and conserve hospital resources for patients and essential staff; while there may be individuals seeking shelter, the hospital plans focus on caring for existing patients and victims of the disaster and look to local government agencies to meet community needs for shelter and food
If there is any possibility that supply chains may be disrupted, emergency food plans incorporate early triggers to immediately implement measures to conserve and protect existing food supplies; it is easier to expand food service once it is confirmed that food supply chains are established, but by delaying conservation measures, essential food supplies may be expended without immediate resupply options and may impact extended hospital operations
Emergency food response may well need to differ from planning assumptions; plans are based upon the Hazard Vulnerability Analysis (HVA) and provide flexibility to adjust the hospital response dependent upon event circumstances by altering who may be fed, how much they will be fed and how food service will take place
Plans and Procedures Plans address how food safety and sanitation will be maintained during disaster operations and document staff training, adequate sanitation supplies, disposables, trash disposal, etc.
Emergency food plans include altered operations to address the potential for reduced food service staff availability and higher demand, eliminating “room service”, curtailment of cafeteria services, security, meal tickets, and loss of utilities
Emergency food plans, procedures and resources (e.g., supplies and equipment) address altered operations and meal planning for an event involving loss of utilities (electricity, water, information systems) including the equipment and resources necessary to implement those plans (e.g., can openers, grills, disposables, etc)
It is documented that food service staff understand disaster/emergency food plans, the location of the plan and just‐in‐time tools to implement emergency food plans
Plans identify emergency food service staffing needs (how many staff will be needed for altered operations and where will they come from?)
Plans include just‐in‐time training tools on food safety and emergency food protocols for staffing pool individuals who may need to work in food service during an event (but do not normally do so)
Emergency food plans have a distinct patient plan which is separate from staff and other individuals included in emergency food calculations (who, what, how much, when, how)
7
Attachment B
October 31, 2013 AttBEmergFoodGuidelines
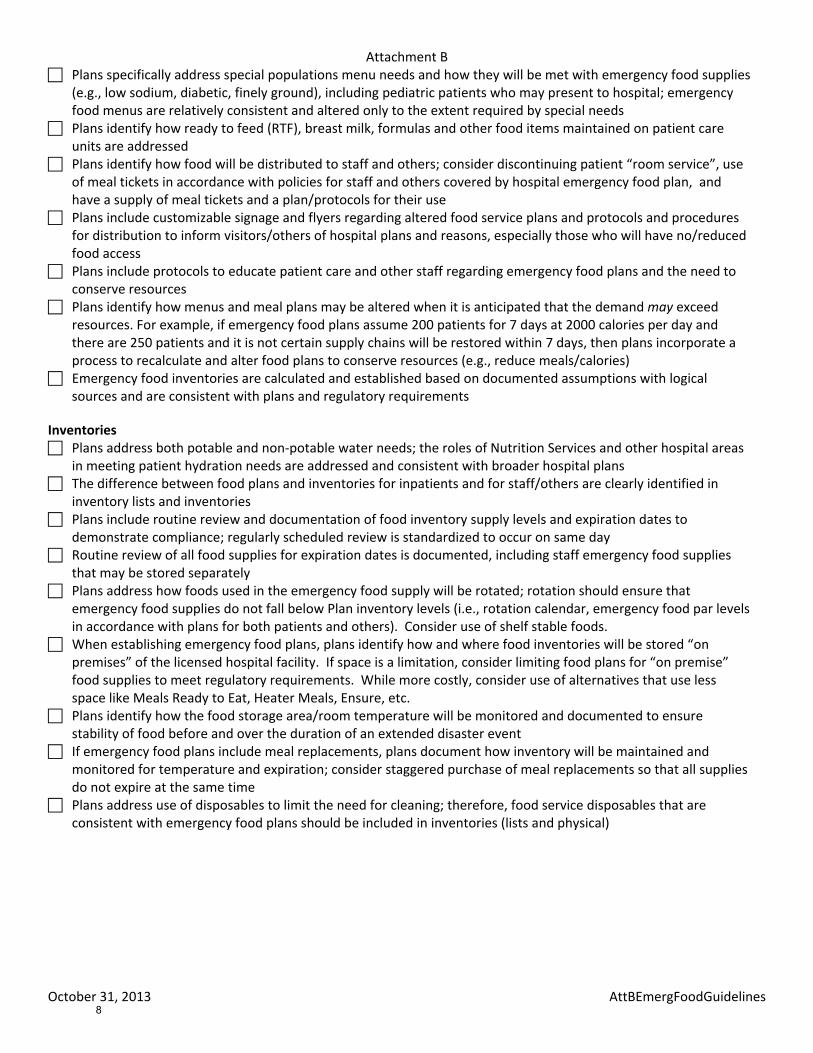
Plans specifically address special populations menu needs and how they will be met with emergency food supplies (e.g., low sodium, diabetic, finely ground), including pediatric patients who may present to hospital; emergency food menus are relatively consistent and altered only to the extent required by special needs
Plans identify how ready to feed (RTF), breast milk, formulas and other food items maintained on patient care units are addressed
Plans identify how food will be distributed to staff and others; consider discontinuing patient “room service”, use of meal tickets in accordance with policies for staff and others covered by hospital emergency food plan, and have a supply of meal tickets and a plan/protocols for their use
Plans include customizable signage and flyers regarding altered food service plans and protocols and procedures for distribution to inform visitors/others of hospital plans and reasons, especially those who will have no/reduced food access
Plans include protocols to educate patient care and other staff regarding emergency food plans and the need to conserve resources
Plans identify how menus and meal plans may be altered when it is anticipated that the demand may exceed resources. For example, if emergency food plans assume 200 patients for 7 days at 2000 calories per day and there are 250 patients and it is not certain supply chains will be restored within 7 days, then plans incorporate a process to recalculate and alter food plans to conserve resources (e.g., reduce meals/calories)
Emergency food inventories are calculated and established based on documented assumptions with logical sources and are consistent with plans and regulatory requirements
Inventories Plans address both potable and non‐potable water needs; the roles of Nutrition Services and other hospital areas in meeting patient hydration needs are addressed and consistent with broader hospital plans
The difference between food plans and inventories for inpatients and for staff/others are clearly identified in inventory lists and inventories
Plans include routine review and documentation of food inventory supply levels and expiration dates to demonstrate compliance; regularly scheduled review is standardized to occur on same day
Routine review of all food supplies for expiration dates is documented, including staff emergency food supplies that may be stored separately
Plans address how foods used in the emergency food supply will be rotated; rotation should ensure that emergency food supplies do not fall below Plan inventory levels (i.e., rotation calendar, emergency food par levels in accordance with plans for both patients and others). Consider use of shelf stable foods.
When establishing emergency food plans, plans identify how and where food inventories will be stored “on premises” of the licensed hospital facility. If space is a limitation, consider limiting food plans for “on premise” food supplies to meet regulatory requirements. While more costly, consider use of alternatives that use less space like Meals Ready to Eat, Heater Meals, Ensure, etc.
Plans identify how the food storage area/room temperature will be monitored and documented to ensure stability of food before and over the duration of an extended disaster event
If emergency food plans include meal replacements, plans document how inventory will be maintained and monitored for temperature and expiration; consider staggered purchase of meal replacements so that all supplies do not expire at the same time
Plans address use of disposables to limit the need for cleaning; therefore, food service disposables that are consistent with emergency food plans should be included in inventories (lists and physical)
8
Attachment C
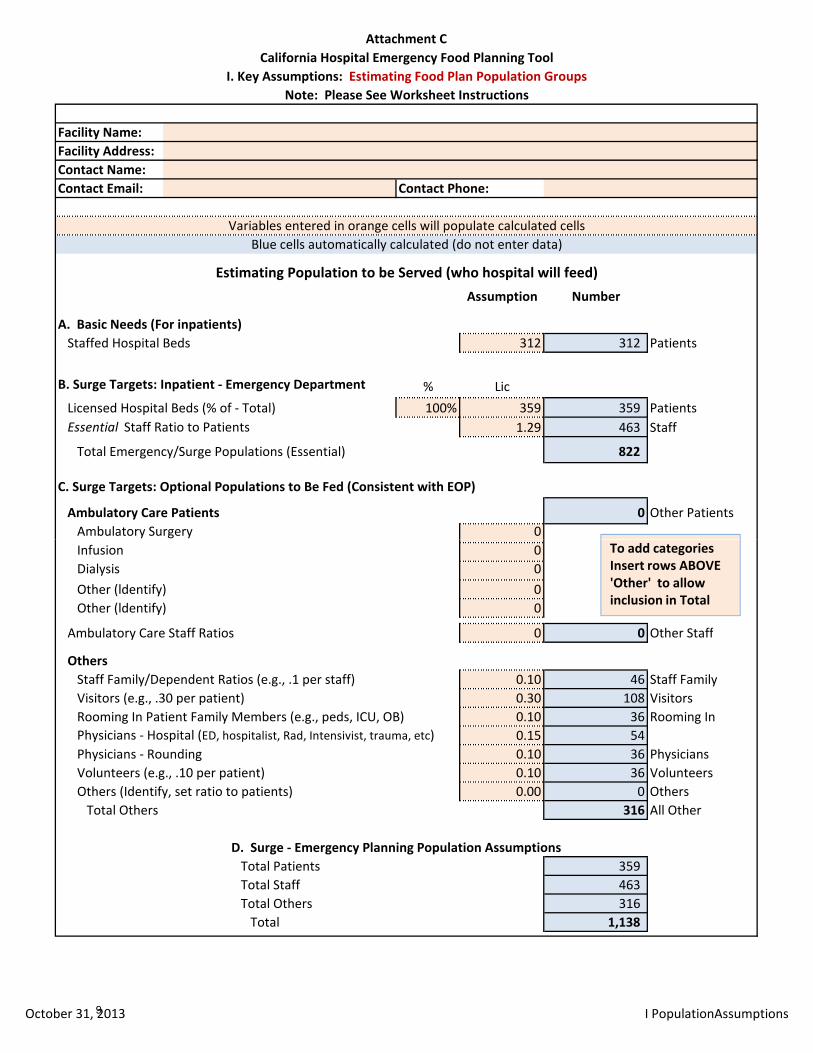
Facility Name:Facility Address:Contact Name:Contact Email: Contact Phone:
Assumption Number
A. Basic Needs (For inpatients)Staffed Hospital Beds 312 312 Patients
B. Surge Targets: Inpatient ‐ Emergency Department % LicLicensed Hospital Beds (% of ‐ Total) 100% 359 359 PatientsEssential Staff Ratio to Patients 1.29 463 Staff
Total Emergency/Surge Populations (Essential) 822
C. Surge Targets: Optional Populations to Be Fed (Consistent with EOP)
Ambulatory Care Patients 0 Other PatientsAmbulatory Surgery 0
Estimating Population to be Served (who hospital will feed)
California Hospital Emergency Food Planning ToolI. Key Assumptions: Estimating Food Plan Population Groups
Note: Please See Worksheet Instructions
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Infusion 0Dialysis 0Other (ldentify) 0Other (ldentify) 0
Ambulatory Care Staff Ratios 0 0 Other Staff
OthersStaff Family/Dependent Ratios (e.g., .1 per staff) 0.10 46 Staff FamilyVisitors (e.g., .30 per patient) 0.30 108 VisitorsRooming In Patient Family Members (e.g., peds, ICU, OB) 0.10 36 Rooming InPhysicians ‐ Hospital (ED, hospitalist, Rad, Intensivist, trauma, etc) 0.15 54Physicians ‐ Rounding 0.10 36 PhysiciansVolunteers (e.g., .10 per patient) 0.10 36 VolunteersOthers (Identify, set ratio to patients) 0.00 0 OthersTotal Others 316 All Other
D. Surge ‐ Emergency Planning Population AssumptionsTotal Patients 359 Total Staff 463 Total Others 316 Total 1,138
To add categories Insert rows ABOVE 'Other' to allow inclusion in Total
October 31, 2013 I PopulationAssumptions9
Attachment C
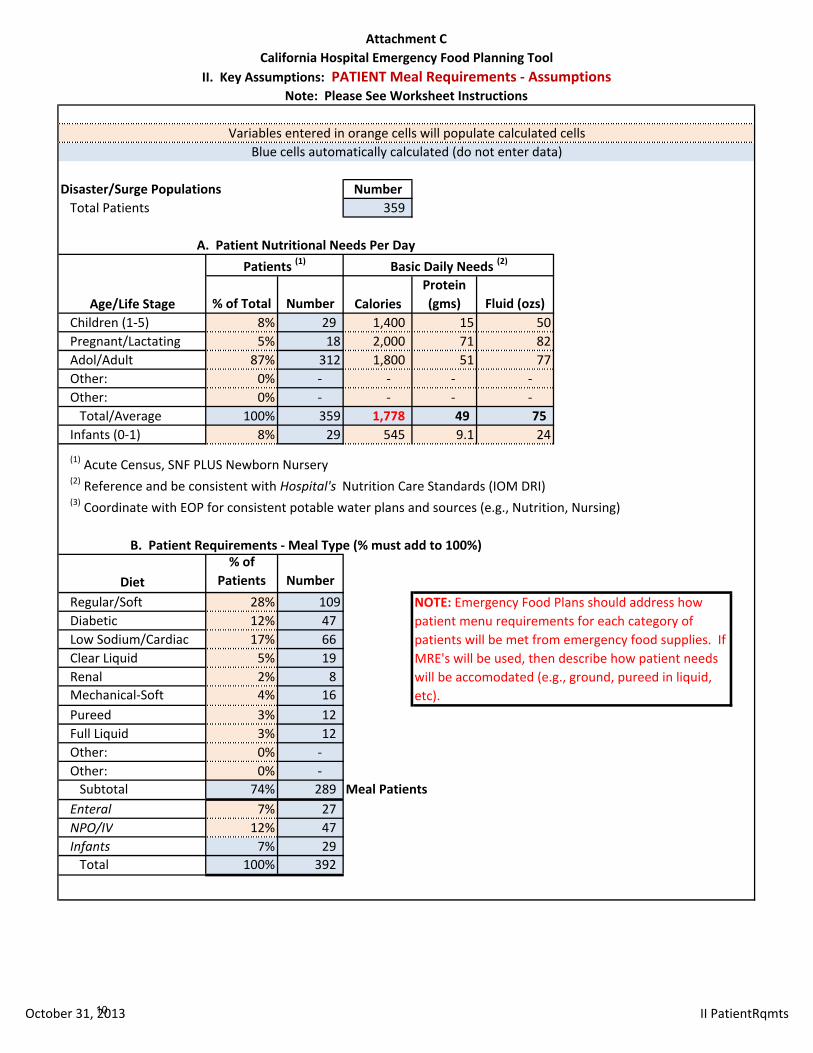
Disaster/Surge Populations NumberTotal Patients 359
% of Total Number CaloriesProtein (gms) Fluid (ozs)
Children (1‐5) 8% 29 1,400 15 50Pregnant/Lactating 5% 18 2,000 71 82Adol/Adult 87% 312 1,800 51 77Other: 0% ‐ ‐ ‐ ‐ Other: 0% ‐ ‐ ‐ ‐ Total/Average 100% 359 1,778 49 75
Infants (0‐1) 8% 29 545 9.1 24
(1) Acute Census, SNF PLUS Newborn Nursery(2) Reference and be consistent with Hospital's Nutrition Care Standards (IOM DRI)(3) Coordinate with EOP for consistent potable water plans and sources (e.g., Nutrition, Nursing)
Diet% of
Patients NumberRegular/Soft 28% 109Diabetic 12% 47 Low Sodium/Cardiac 17% 66 Clear Liquid 5% 19 Renal 2% 8 Mechanical‐Soft 4% 16 Pureed 3% 12 Full Liquid 3% 12 Other: 0% ‐ Other: 0% ‐ Subtotal 74% 289 Meal Patients
Enteral 7% 27 NPO/IV 12% 47 Infants 7% 29 Total 100% 392
NOTE: Emergency Food Plans should address how patient menu requirements for each category of patients will be met from emergency food supplies. If MRE's will be used, then describe how patient needs will be accomodated (e.g., ground, pureed in liquid, etc).
B. Patient Requirements ‐ Meal Type (% must add to 100%)
Age/Life Stage
California Hospital Emergency Food Planning ToolII. Key Assumptions: PATIENT Meal Requirements ‐ Assumptions
Note: Please See Worksheet Instructions
Patients (1) Basic Daily Needs (2)
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
A. Patient Nutritional Needs Per Day
October 31, 2013 II PatientRqmts10
Attachment C
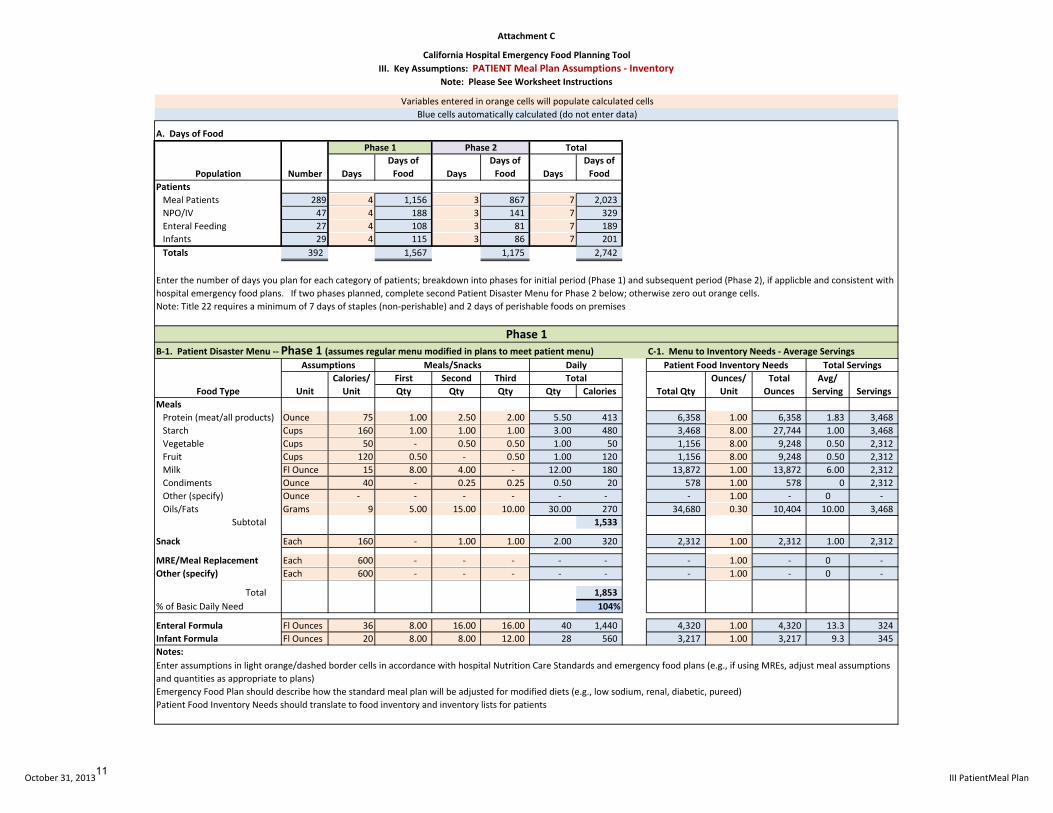
A. Days of Food
DaysDays of Food Days
Days of Food Days
Days of Food
PatientsMeal Patients 289 4 1,156 3 867 7 2,023 NPO/IV 47 4 188 3 141 7 329 Enteral Feeding 27 4 108 3 81 7 189 Infants 29 4 115 3 86 7 201 Totals 392 1,567 1,175 2,742
Note: Title 22 requires a minimum of 7 days of staples (non‐perishable) and 2 days of perishable foods on premises
B‐1. Patient Disaster Menu ‐‐ Phase 1 (assumes regular menu modified in plans to meet patient menu) C‐1. Menu to Inventory Needs ‐ Average Servings
First Second ThirdQty Qty Qty Qty Calories
MealsProtein (meat/all products) Ounce 75 1.00 2.50 2.00 5.50 413 6,358 1.00 6,358 1.83 3,468 Starch Cups 160 1.00 1.00 1.00 3.00 480 3,468 8.00 27,744 1.00 3,468 Vegetable Cups 50 ‐ 0.50 0.50 1.00 50 1,156 8.00 9,248 0.50 2,312 Fruit Cups 120 0.50 ‐ 0.50 1.00 120 1,156 8.00 9,248 0.50 2,312 Milk Fl Ounce 15 8.00 4.00 ‐ 12.00 180 13,872 1.00 13,872 6.00 2,312 Condiments Ounce 40 ‐ 0.25 0.25 0.50 20 578 1.00 578 0 2,312 Other (specify) Ounce ‐ ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Oils/Fats Grams 9 5.00 15.00 10.00 30.00 270 34,680 0.30 10,404 10.00 3,468
Subtotal 1,533
Snack Each 160 ‐ 1.00 1.00 2.00 320 2,312 1.00 2,312 1.00 2,312
MRE/Meal Replacement Each 600 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Other (specify) Each 600 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐
Total 1,853 % of Basic Daily Need 104%
Enteral Formula Fl Ounces 36 8.00 16.00 16.00 40 1,440 4,320 1.00 4,320 13.3 324 Infant Formula Fl Ounces 20 8.00 8.00 12.00 28 560 3,217 1.00 3,217 9.3 345 Notes:
Ounces/ Unit
TotalUnit
Assumptions Meals/Snacks DailyAvg/
Serving Servings
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Total Servings
Phase 1
NumberPopulation
Phase 2 Total
Enter the number of days you plan for each category of patients; breakdown into phases for initial period (Phase 1) and subsequent period (Phase 2), if applicble and consistent with hospital emergency food plans. If two phases planned, complete second Patient Disaster Menu for Phase 2 below; otherwise zero out orange cells.
Total Ounces
Patient Food Inventory Needs
Total QtyFood TypeCalories/Unit
Phase 1
California Hospital Emergency Food Planning ToolIII. Key Assumptions: PATIENT Meal Plan Assumptions ‐ Inventory
Note: Please See Worksheet Instructions
Enter assumptions in light orange/dashed border cells in accordance with hospital Nutrition Care Standards and emergency food plans (e.g., if using MREs, adjust meal assumptions and quantities as appropriate to plans)Emergency Food Plan should describe how the standard meal plan will be adjusted for modified diets (e.g., low sodium, renal, diabetic, pureed)Patient Food Inventory Needs should translate to food inventory and inventory lists for patients
October 31, 2013 III PatientMeal Plan11
Attachment C
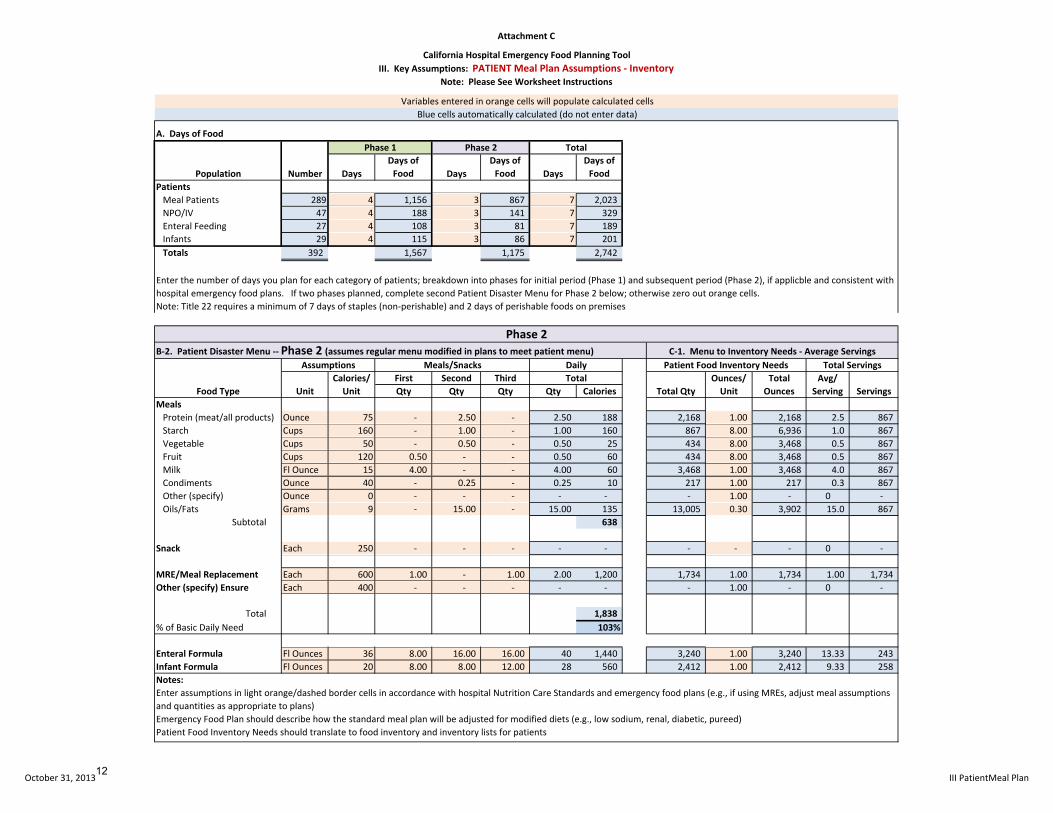
A. Days of Food
DaysDays of Food Days
Days of Food Days
Days of Food
PatientsMeal Patients 289 4 1,156 3 867 7 2,023 NPO/IV 47 4 188 3 141 7 329 Enteral Feeding 27 4 108 3 81 7 189 Infants 29 4 115 3 86 7 201 Totals 392 1,567 1,175 2,742
Note: Title 22 requires a minimum of 7 days of staples (non‐perishable) and 2 days of perishable foods on premises
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Phase 1
NumberPopulation
Phase 2 Total
Enter the number of days you plan for each category of patients; breakdown into phases for initial period (Phase 1) and subsequent period (Phase 2), if applicble and consistent with hospital emergency food plans. If two phases planned, complete second Patient Disaster Menu for Phase 2 below; otherwise zero out orange cells.
California Hospital Emergency Food Planning ToolIII. Key Assumptions: PATIENT Meal Plan Assumptions ‐ Inventory
Note: Please See Worksheet Instructions
First Second ThirdQty Qty Qty Qty Calories
MealsProtein (meat/all products) Ounce 75 ‐ 2.50 ‐ 2.50 188 2,168 1.00 2,168 2.5 867 Starch Cups 160 ‐ 1.00 ‐ 1.00 160 867 8.00 6,936 1.0 867 Vegetable Cups 50 ‐ 0.50 ‐ 0.50 25 434 8.00 3,468 0.5 867 Fruit Cups 120 0.50 ‐ ‐ 0.50 60 434 8.00 3,468 0.5 867 Milk Fl Ounce 15 4.00 ‐ ‐ 4.00 60 3,468 1.00 3,468 4.0 867 Condiments Ounce 40 ‐ 0.25 ‐ 0.25 10 217 1.00 217 0.3 867 Other (specify) Ounce 0 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Oils/Fats Grams 9 ‐ 15.00 ‐ 15.00 135 13,005 0.30 3,902 15.0 867
Subtotal 638
Snack Each 250 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ 0 ‐
MRE/Meal Replacement Each 600 1.00 ‐ 1.00 2.00 1,200 1,734 1.00 1,734 1.00 1,734 Other (specify) Ensure Each 400 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐
Total 1,838 % of Basic Daily Need 103%
Enteral Formula Fl Ounces 36 8.00 16.00 16.00 40 1,440 3,240 1.00 3,240 13.33 243 Infant Formula Fl Ounces 20 8.00 8.00 12.00 28 560 2,412 1.00 2,412 9.33 258 Notes:
ServingsFood Type
Assumptions Meals/Snacks Daily Patient Food Inventory NeedsTotal
Total QtyOunces/ Unit
Total Ounces
Avg/ Serving
Patient Food Inventory Needs should translate to food inventory and inventory lists for patients
Phase 2C‐1. Menu to Inventory Needs ‐ Average ServingsB‐2. Patient Disaster Menu ‐‐ Phase 2 (assumes regular menu modified in plans to meet patient menu)
Enter assumptions in light orange/dashed border cells in accordance with hospital Nutrition Care Standards and emergency food plans (e.g., if using MREs, adjust meal assumptions and quantities as appropriate to plans)Emergency Food Plan should describe how the standard meal plan will be adjusted for modified diets (e.g., low sodium, renal, diabetic, pureed)
Total Servings
UnitCalories/Unit
October 31, 2013 III PatientMeal Plan12
Attachment C
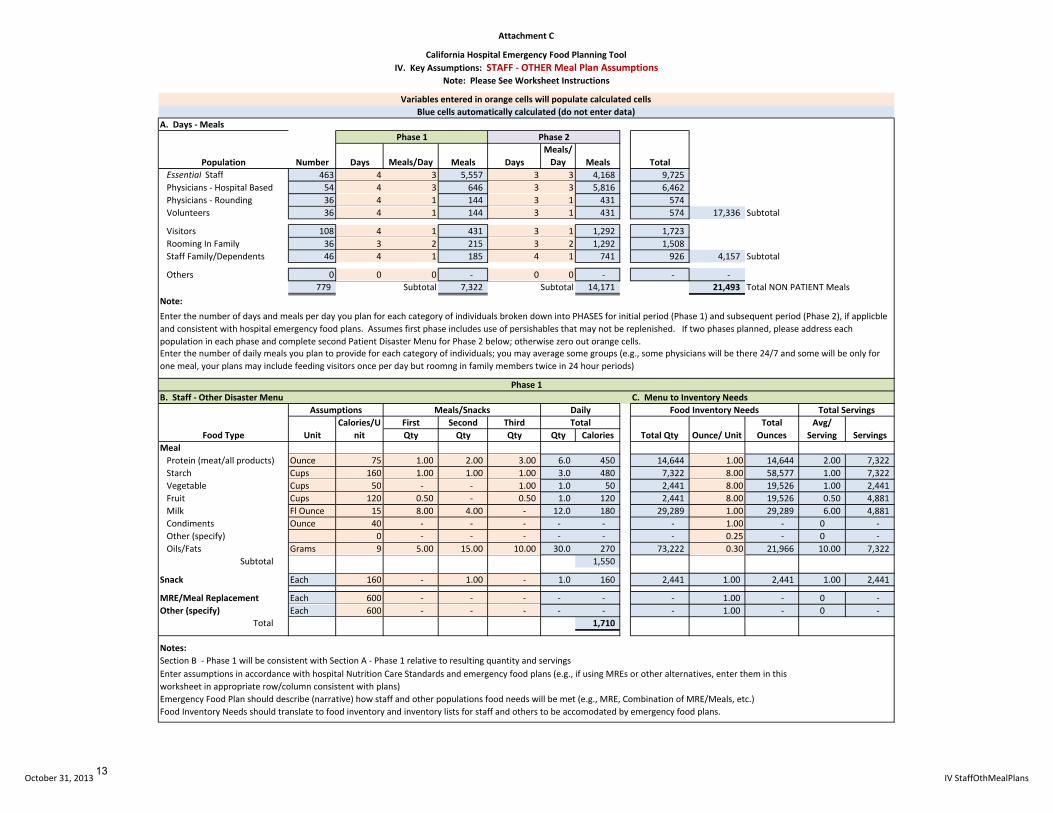
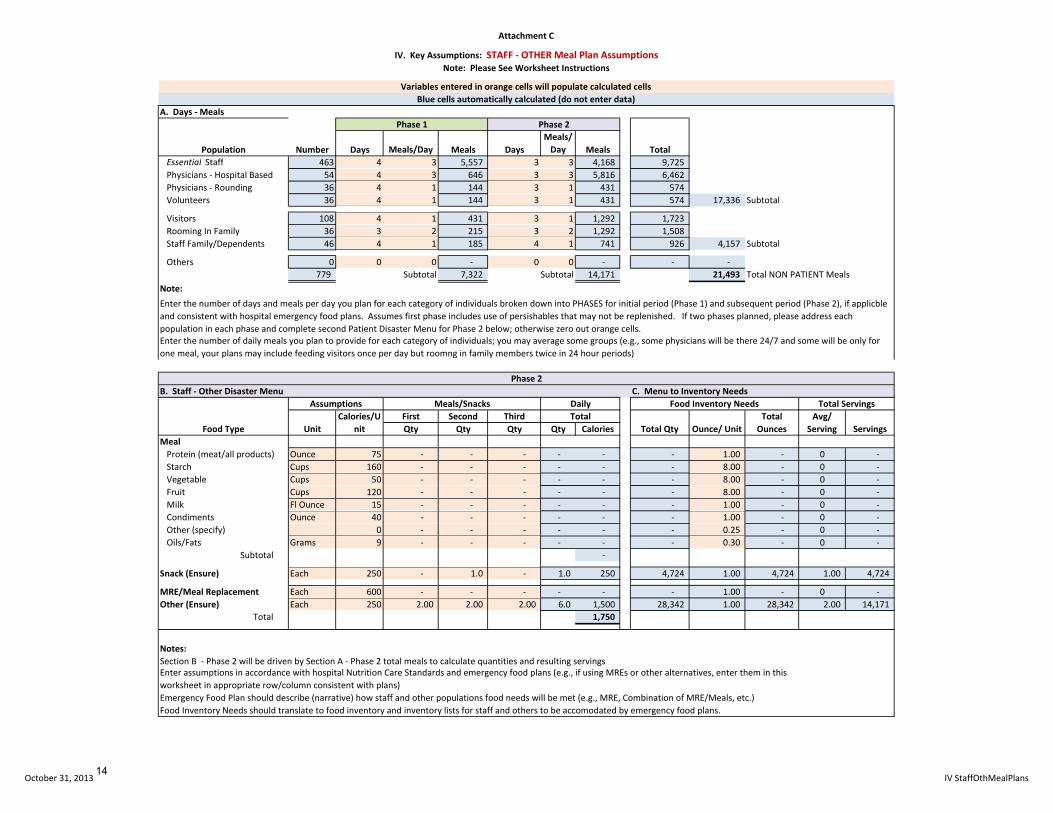
A. Days ‐ Meals
Days Meals/Day Meals DaysMeals/Day Meals
Essential Staff 463 4 3 5,557 3 3 4,168 9,725 Physicians ‐ Hospital Based 54 4 3 646 3 3 5,816 6,462 Physicians ‐ Rounding 36 4 1 144 3 1 431 574 Volunteers 36 4 1 144 3 1 431 574 17,336 Subtotal
Visitors 108 4 1 431 3 1 1,292 1,723 Rooming In Family 36 3 2 215 3 2 1,292 1,508 Staff Family/Dependents 46 4 1 185 4 1 741 926 4,157 Subtotal
Others 0 0 0 ‐ 0 0 ‐ ‐ ‐ 779 Subtotal 7,322 Subtotal 14,171 21,493 Total NON PATIENT Meals
Note:
B. Staff ‐ Other Disaster Menu C. Menu to Inventory Needs
First Second ThirdQty Qty Qty Qty Calories
MealProtein (meat/all products) Ounce 75 1.00 2.00 3.00 6.0 450 14,644 1.00 14,644 2.00 7,322 Starch Cups 160 1.00 1.00 1.00 3.0 480 7,322 8.00 58,577 1.00 7,322 Vegetable Cups 50 ‐ ‐ 1.00 1.0 50 2,441 8.00 19,526 1.00 2,441 Fruit Cups 120 0.50 ‐ 0.50 1.0 120 2,441 8.00 19,526 0.50 4,881 Milk Fl Ounce 15 8.00 4.00 ‐ 12.0 180 29,289 1.00 29,289 6.00 4,881 Condiments Ounce 40 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Other (specify) 0 ‐ ‐ ‐ ‐ ‐ ‐ 0.25 ‐ 0 ‐ Oils/Fats Grams 9 5.00 15.00 10.00 30.0 270 73,222 0.30 21,966 10.00 7,322
Subtotal 1,550
Snack Each 160 ‐ 1.00 ‐ 1.0 160 2,441 1.00 2,441 1.00 2,441
MRE/Meal Replacement Each 600 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Other (specify) Each 600 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐
Total 1,710
Notes:Section B ‐ Phase 1 will be consistent with Section A ‐ Phase 1 relative to resulting quantity and servings
Emergency Food Plan should describe (narrative) how staff and other populations food needs will be met (e.g., MRE, Combination of MRE/Meals, etc.)Food Inventory Needs should translate to food inventory and inventory lists for staff and others to be accomodated by emergency food plans.
California Hospital Emergency Food Planning ToolIV. Key Assumptions: STAFF ‐ OTHER Meal Plan Assumptions
Note: Please See Worksheet Instructions
Avg/ Serving
Phase 2
NumberPopulation
Phase 1
Total
Enter the number of days and meals per day you plan for each category of individuals broken down into PHASES for initial period (Phase 1) and subsequent period (Phase 2), if applicble and consistent with hospital emergency food plans. Assumes first phase includes use of persishables that may not be replenished. If two phases planned, please address each population in each phase and complete second Patient Disaster Menu for Phase 2 below; otherwise zero out orange cells.
UnitCalories/U
nitTotal
Total Qty Ounce/ UnitTotal Ounces Servings
Total Servings
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Enter assumptions in accordance with hospital Nutrition Care Standards and emergency food plans (e.g., if using MREs or other alternatives, enter them in this worksheet in appropriate row/column consistent with plans)
Food Type
Assumptions Meals/Snacks Daily Food Inventory Needs
Enter the number of daily meals you plan to provide for each category of individuals; you may average some groups (e.g., some physicians will be there 24/7 and some will be only for one meal, your plans may include feeding visitors once per day but roomng in family members twice in 24 hour periods)
Phase 1
October 31, 2013 IV StaffOthMealPlans13
Attachment C
A. Days ‐ Meals
Days Meals/Day Meals DaysMeals/Day Meals
Essential Staff 463 4 3 5,557 3 3 4,168 9,725 Physicians ‐ Hospital Based 54 4 3 646 3 3 5,816 6,462 Physicians ‐ Rounding 36 4 1 144 3 1 431 574 Volunteers 36 4 1 144 3 1 431 574 17,336 Subtotal
Visitors 108 4 1 431 3 1 1,292 1,723 Rooming In Family 36 3 2 215 3 2 1,292 1,508 Staff Family/Dependents 46 4 1 185 4 1 741 926 4,157 Subtotal
Others 0 0 0 ‐ 0 0 ‐ ‐ ‐ 779 Subtotal 7,322 Subtotal 14,171 21,493 Total NON PATIENT Meals
Note:
IV. Key Assumptions: STAFF ‐ OTHER Meal Plan AssumptionsNote: Please See Worksheet Instructions
Phase 2
NumberPopulation
Phase 1
Total
Enter the number of days and meals per day you plan for each category of individuals broken down into PHASES for initial period (Phase 1) and subsequent period (Phase 2), if applicble and consistent with hospital emergency food plans. Assumes first phase includes use of persishables that may not be replenished. If two phases planned, please address each population in each phase and complete second Patient Disaster Menu for Phase 2 below; otherwise zero out orange cells.
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Enter the number of daily meals you plan to provide for each category of individuals; you may average some groups (e.g., some physicians will be there 24/7 and some will be only for one meal, your plans may include feeding visitors once per day but roomng in family members twice in 24 hour periods)
B. Staff ‐ Other Disaster Menu C. Menu to Inventory Needs
First Second ThirdQty Qty Qty Qty Calories
MealProtein (meat/all products) Ounce 75 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Starch Cups 160 ‐ ‐ ‐ ‐ ‐ ‐ 8.00 ‐ 0 ‐ Vegetable Cups 50 ‐ ‐ ‐ ‐ ‐ ‐ 8.00 ‐ 0 ‐ Fruit Cups 120 ‐ ‐ ‐ ‐ ‐ ‐ 8.00 ‐ 0 ‐ Milk Fl Ounce 15 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Condiments Ounce 40 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Other (specify) 0 ‐ ‐ ‐ ‐ ‐ ‐ 0.25 ‐ 0 ‐ Oils/Fats Grams 9 ‐ ‐ ‐ ‐ ‐ ‐ 0.30 ‐ 0 ‐
Subtotal ‐
Snack (Ensure) Each 250 ‐ 1.0 ‐ 1.0 250 4,724 1.00 4,724 1.00 4,724
MRE/Meal Replacement Each 600 ‐ ‐ ‐ ‐ ‐ ‐ 1.00 ‐ 0 ‐ Other (Ensure) Each 250 2.00 2.00 2.00 6.0 1,500 28,342 1.00 28,342 2.00 14,171
Total 1,750
Notes:Section B ‐ Phase 2 will be driven by Section A ‐ Phase 2 total meals to calculate quantities and resulting servings
Emergency Food Plan should describe (narrative) how staff and other populations food needs will be met (e.g., MRE, Combination of MRE/Meals, etc.)Food Inventory Needs should translate to food inventory and inventory lists for staff and others to be accomodated by emergency food plans.
Servings
Enter assumptions in accordance with hospital Nutrition Care Standards and emergency food plans (e.g., if using MREs or other alternatives, enter them in this worksheet in appropriate row/column consistent with plans)
Phase 2
Food Type
Assumptions Meals/Snacks Daily Food Inventory Needs Total Servings
UnitCalories/U
nitTotal
Total Qty Ounce/ UnitTotal Ounces
Avg/ Serving
October 31, 2013 IV StaffOthMealPlans14
Attachment C
Total Needed
Avg/ Serving Servings
Total Needed
Avg/ Serving Servings
Total Needed
Avg/ Serving Servings
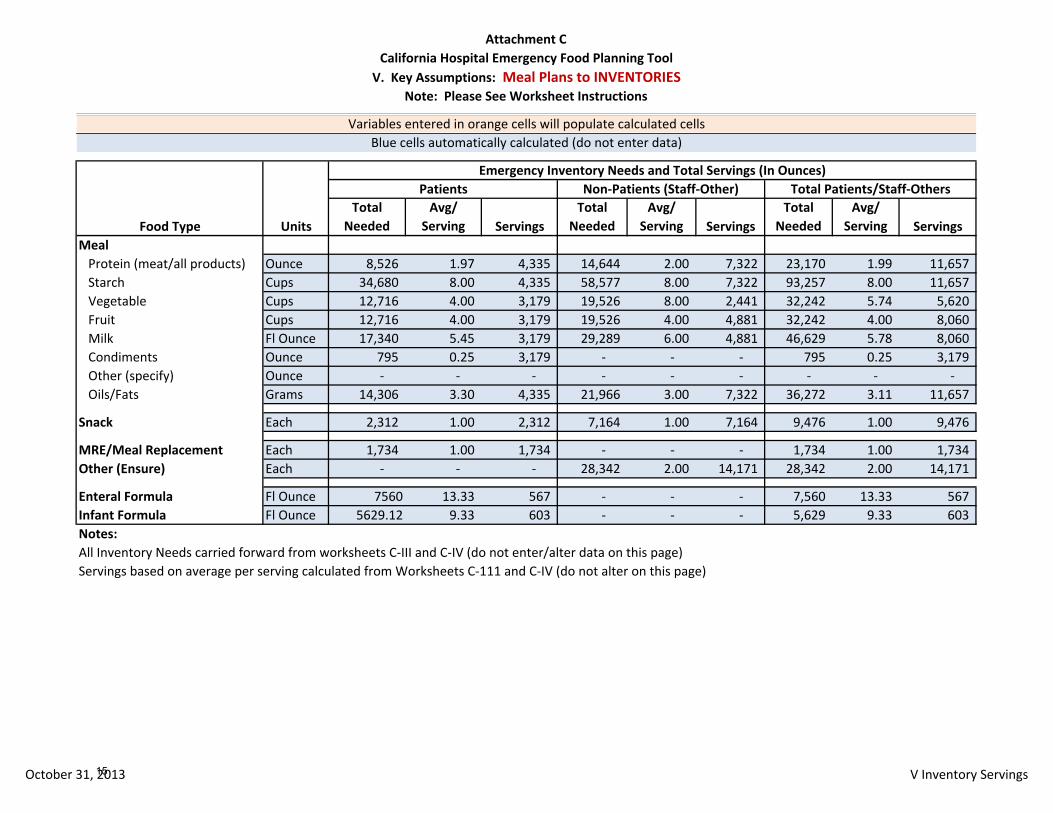
MealProtein (meat/all products) Ounce 8,526 1.97 4,335 14,644 2.00 7,322 23,170 1.99 11,657 Starch Cups 34,680 8.00 4,335 58,577 8.00 7,322 93,257 8.00 11,657 Vegetable Cups 12,716 4.00 3,179 19,526 8.00 2,441 32,242 5.74 5,620 Fruit Cups 12,716 4.00 3,179 19,526 4.00 4,881 32,242 4.00 8,060 Milk Fl Ounce 17,340 5.45 3,179 29,289 6.00 4,881 46,629 5.78 8,060 Condiments Ounce 795 0.25 3,179 ‐ ‐ ‐ 795 0.25 3,179 Other (specify) Ounce ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ Oils/Fats Grams 14,306 3.30 4,335 21,966 3.00 7,322 36,272 3.11 11,657
Snack Each 2,312 1.00 2,312 7,164 1.00 7,164 9,476 1.00 9,476
MRE/Meal Replacement Each 1,734 1.00 1,734 ‐ ‐ ‐ 1,734 1.00 1,734 Other (Ensure) Each ‐ ‐ ‐ 28,342 2.00 14,171 28,342 2.00 14,171
Enteral Formula Fl Ounce 7560 13.33 567 ‐ ‐ ‐ 7,560 13.33 567 Infant Formula Fl Ounce 5629.12 9.33 603 ‐ ‐ ‐ 5,629 9.33 603 Notes:All Inventory Needs carried forward from worksheets C‐III and C‐IV (do not enter/alter data on this page)Servings based on average per serving calculated from Worksheets C‐111 and C‐IV (do not alter on this page)
Emergency Inventory Needs and Total Servings (In Ounces)Patients Non‐Patients (Staff‐Other) Total Patients/Staff‐Others
California Hospital Emergency Food Planning ToolV. Key Assumptions: Meal Plans to INVENTORIES
Note: Please See Worksheet Instructions
Variables entered in orange cells will populate calculated cellsBlue cells automatically calculated (do not enter data)
Food Type Units
October 31, 2013 V Inventory Servings15
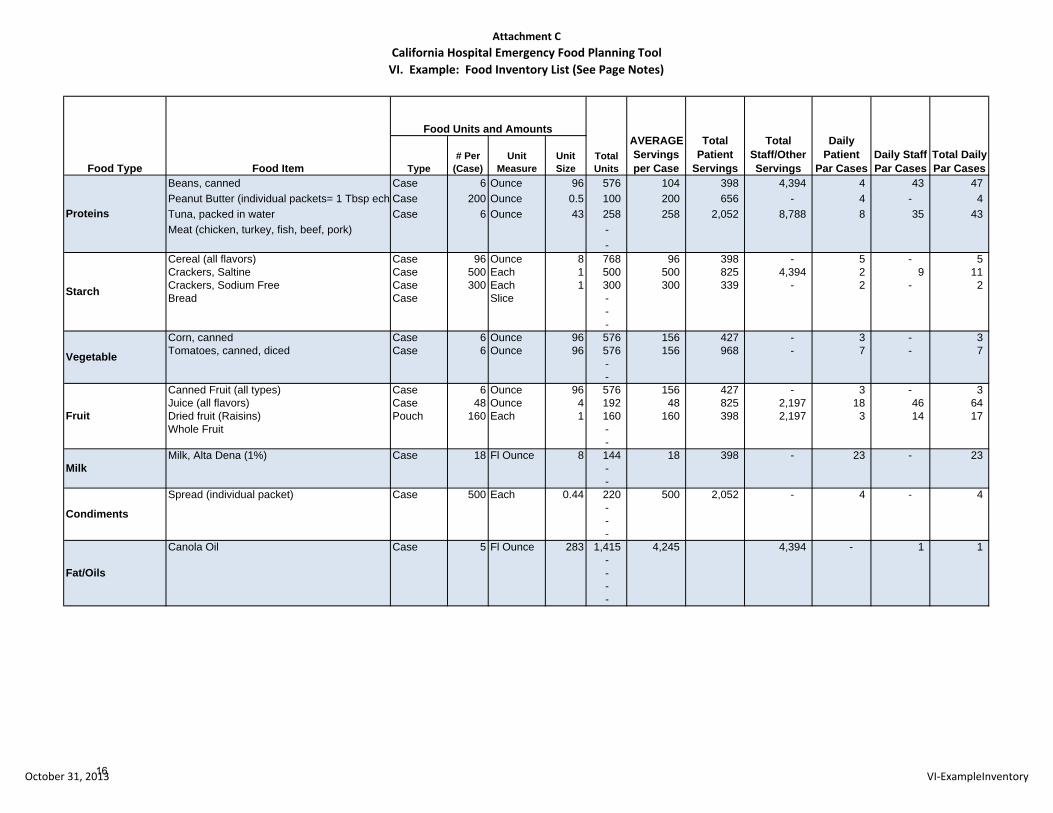
Attachment CCalifornia Hospital Emergency Food Planning ToolVI. Example: Food Inventory List (See Page Notes)
Type# Per
(Case)Unit
MeasureUnit Size
Beans, canned Case 6 Ounce 96 576 104 398 4,394 4 43 47 Peanut Butter (individual packets= 1 Tbsp ech Case 200 Ounce 0.5 100 200 656 - 4 - 4 Tuna, packed in water Case 6 Ounce 43 258 258 2,052 8,788 8 35 43 Meat (chicken, turkey, fish, beef, pork) -
- Cereal (all flavors) Case 96 Ounce 8 768 96 398 - 5 - 5 Crackers, Saltine Case 500 Each 1 500 500 825 4,394 2 9 11 Crackers, Sodium Free Case 300 Each 1 300 300 339 - 2 - 2 Bread Case Slice -
- -
Corn, canned Case 6 Ounce 96 576 156 427 - 3 - 3 Tomatoes, canned, diced Case 6 Ounce 96 576 156 968 - 7 - 7
- -
Canned Fruit (all types) Case 6 Ounce 96 576 156 427 - 3 - 3 Juice (all flavors) Case 48 Ounce 4 192 48 825 2,197 18 46 64 Dried fruit (Raisins) Pouch 160 Each 1 160 160 398 2,197 3 14 17 Whole Fruit -
- Milk, Alta Dena (1%) Case 18 Fl Ounce 8 144 18 398 - 23 - 23
- -
Spread (individual packet) Case 500 Each 0.44 220 500 2,052 - 4 - 4 - - -
Canola Oil Case 5 Fl Ounce 283 1,415 4,245 4,394 - 1 1 - - - -
Total Staff/OtherServings
Daily Patient
Par CasesDaily Staff Par Cases
Vegetable
Fruit
Milk
Condiments
Fat/Oils
Total Daily Par Cases
Proteins
Starch
Food Type Food Item
Food Units and AmountsAVERAGE Servings per Case
Total Patient
Servings Total Units
October 31, 2013 VI‐ExampleInventory16
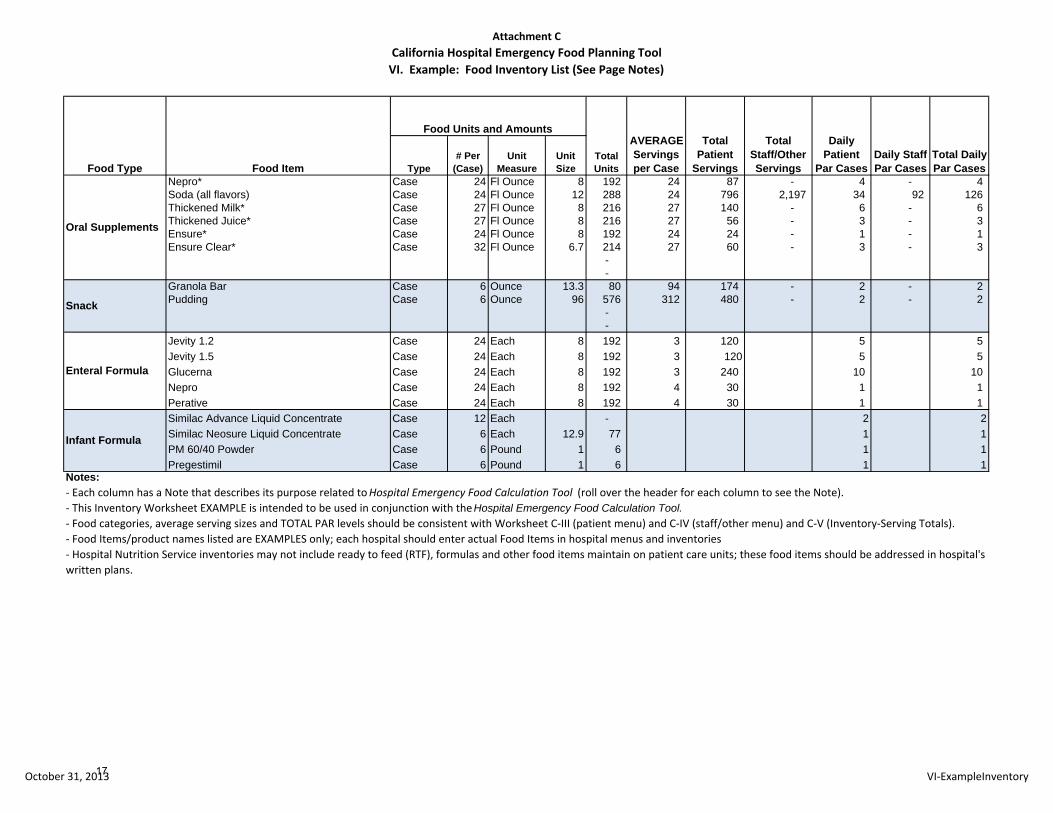
Attachment CCalifornia Hospital Emergency Food Planning ToolVI. Example: Food Inventory List (See Page Notes)
Type# Per
(Case)Unit
MeasureUnit Size
Total Staff/OtherServings
Daily Patient
Par CasesDaily Staff Par Cases
Total Daily Par CasesFood Type Food Item
Food Units and AmountsAVERAGE Servings per Case
Total Patient
Servings Total Units
Nepro* Case 24 Fl Ounce 8 192 24 87 - 4 - 4 Soda (all flavors) Case 24 Fl Ounce 12 288 24 796 2,197 34 92 126 Thickened Milk* Case 27 Fl Ounce 8 216 27 140 - 6 - 6 Thickened Juice* Case 27 Fl Ounce 8 216 27 56 - 3 - 3 Ensure* Case 24 Fl Ounce 8 192 24 24 - 1 - 1 Ensure Clear* Case 32 Fl Ounce 6.7 214 27 60 - 3 - 3
- -
Granola Bar Case 6 Ounce 13.3 80 94 174 - 2 - 2 Pudding Case 6 Ounce 96 576 312 480 - 2 - 2
- -
Jevity 1.2 Case 24 Each 8 192 3 120 5 5 Jevity 1.5 Case 24 Each 8 192 3 120 5 5 Glucerna Case 24 Each 8 192 3 240 10 10 Nepro Case 24 Each 8 192 4 30 1 1 Perative Case 24 Each 8 192 4 30 1 1 Similac Advance Liquid Concentrate Case 12 Each - 2 2Similac Neosure Liquid Concentrate Case 6 Each 12.9 77 1 1PM 60/40 Powder Case 6 Pound 1 6 1 1Pregestimil Case 6 Pound 1 6 1 1
Oral Supplements
Snack
Enteral Formula
Infant Formula
Notes: ‐ Each column has a Note that describes its purpose related to Hospital Emergency Food Calculation Tool (roll over the header for each column to see the Note).‐ This Inventory Worksheet EXAMPLE is intended to be used in conjunction with the Hospital Emergency Food Calculation Tool. ‐ Food categories, average serving sizes and TOTAL PAR levels should be consistent with Worksheet C‐III (patient menu) and C‐IV (staff/other menu) and C‐V (Inventory‐Serving Totals). ‐ Food Items/product names listed are EXAMPLES only; each hospital should enter actual Food Items in hospital menus and inventories‐ Hospital Nutrition Service inventories may not include ready to feed (RTF), formulas and other food items maintain on patient care units; these food items should be addressed in hospital's written plans.
October 31, 2013 VI‐ExampleInventory17

PAGE
INTENTIONALLY
LEFT
BLANK
18
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool I. Key Assumptions: Estimating Food Plan Population Groups
The purpose of this worksheet is to identify the estimated number of individuals by category/group to be included in hospital emergency food supply planning assumptions. These estimates will serve as the basis for subsequent steps in emergency food calculations and should be consistent with the hospital Emergency Operations Plan (EOP). Nutrition managers should work with emergency management in developing the assumptions to ensure consistency.
NOTE: Each hospital should establish and enter assumptions in this and subsequent worksheets based on their specific plans and circumstances, as well as regulatory requirements. For example, a small rural hospital may well have very different emergency food plan assumptions than a large, urban academic medical center. The tool is designed to allow each hospital to consider and document their planning assumptions and meet regulatory requirements, not to impose additional requirements.
Cells in the worksheet colored light orange (dotted line borders) are for hospital data entry. Data should not be entered into cells colored light blue (solid line borders) as these are automatic calculations; entry of data into these cells will result in a loss of automatic calculations and inaccurate results.
A. Basic Needs Population (inpatients)
This section identifies hospital average daily patient census under normal operations. Identification of this base demonstrates that emergency plans take patient surge into consideration. Most California hospitals’ average daily census is between 60‐70% of licensed bed capacity. Therefore, average staffed beds are used to represent a reasonable base for planning purposes; it is best not to use a single day or month for this purpose due to significant variability, but to use a quarter or year unless there are known reasons to use more current estimates (e.g., new beds). These figures are generally available from your finance department and reported quarterly to the State.
B. Surge Targets: Emergency/Surge Populations (inpatients, emergency department and staff)
In this worksheet, estimate the number of individuals to be included in the emergency food plan. How many meals or meal alternatives and for how long will be addressed in subsequent worksheets. Staff ratios to patients include ALL essential staff (not nursing ratios) and are used to allow for easy update of calculations as licensed/surge bed assumptions change.
Licensed Hospital Beds are all inpatient beds under the hospital license, regardless of type (e.g., general acute care, psychiatric, Distinct Part Skilled Nursing Facility) and serve as the basis for estimated emergency/inpatient surge. Enter the number of licensed beds in the worksheet and the percent of licensed beds that your facility’s EOP estimates for surge capacity; if hospital surge capacity estimates are less than 100%, then default to 100% of licensed beds.
Staffing Ratio represents essential hospital staff necessary to providing hospital patient care (Emergency and Inpatient), to continuing essential hospital operations and emergency management. It is recommended that hospitals NOT include non‐essential staff in food planning calculations for any disaster that would require activation of the emergency food plan. Also consider the type of event and ability of staff to come to work (and go home after a shift), modification of staffing ratios due to government emergency declaration and surge, services that will be constrained or limited (e.g., outpatient) and other factors that may impact staffing.
These assumptions should be established in coordination with emergency management, business continuity plans and operations and take alternative treatment area plans for surge into consideration.
19
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
If the hospital operates other, off‐license programs or services (e.g., community center/shelter) not directly related to hospital care, separate plans should be established for those programs or services; they should not be included in hospital plans. This separation is also required by federal agencies who reimburse agencies providing community services to victims during a declared emergency.
The results of this section will be total inpatients, emergency patients and total essential staff to be included in the emergency food plan. Normal Newborn Nursery staff should be included in staffing figures.
C. Surge Targets: Optional Populations
Optional Populations are those that the hospital may decide to include in emergency food plans, but are not required by regulation. It is generally assumed that ambulatory care patients in clinics or ancillary services will leave the hospital campus and receive care and shelter through community resources, if necessary.
The hospital may decide to include Ambulatory Care Patients undergoing treatment or procedures (surgery, infusion, dialysis, etc) at the onset of an event and who cannot leave until they have recovered. Some ambulatory care services may be continued by the hospital during the event (e.g., alternate care areas for surge, ongoing care patients). If the hospital emergency food plan is to feed these populations during an event, then enter the number of patients in each category. Consider whether it is a point in time figure (e.g., how many will actually be in the surgery suite at the onset, not how many cases scheduled throughout the day) unless these services will be continued and/or used for surge and your plan is to feed these patients. It is not required that the hospital feed patients undergoing Ambulatory treatment.
Ambulatory Care Staffing Ratios represents the number of essential staff per Ambulatory Care patient needed to continue care and not included in the inpatient figures above. If you estimate there will be 20 patients and 10 staff, then you would enter .5 in the cell. The results of this section will be estimated Ambulatory Care area patients and staff. Ambulatory Care area staff who may be reassigned to inpatient or emergency services should be included in Section B – Surge Targets – Emergency/Surge Populations above.
At the hospital’s option, there may be Other population groups included in the hospital emergency food plans and the EOP. Review each category in this section and determine both if, and how many, need to be included in emergency food calculations.
Does the hospital EOP include providing Staff Family/Dependent care during a disaster so that staff may come to/remain at work? If so, what are your estimates for how many essential staff would require this support? Enter this figure into the Staff Family/Dependent cell as a ratio to staff. For example, if you have 300 essential staff and your EOP estimates that 50 will need dependent care for a family member, then you would enter .17 into the cell. Staff should be encouraged in advance to make alternative arrangements for family/dependents during a disaster/emergency.
Will the hospital limit Visitors during a disaster? Will the hospital close its cafeteria to the public during a disaster? Both of these steps are recommended at the onset of any event that may require activation of the emergency food plan; it is easier to expand food service if the situation improves, but difficult to implement after scarce resources have already been consumed.
During a disaster, a hospital may well be viewed as a shelter or community resource and must act quickly to implement policies that preserve scarce resources for its primary responsibility to patients and staff. It is anticipated that the hospital may allow one family member to remain with some patients (e.g., pediatrics). It is not necessary to feed other visitors that may be allowed, and it is suggested that policies are limited to a small number that may remain with the patient and, therefore, may not have access to community resources.
20

Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
Does your hospital plan to provide meals to Physicians? If so, estimate the number of hospital‐based physicians that would require meals and enter the number per inpatient. This Hospital‐based physicians should be limited to those physicians expected to be at the hospital for long portions of the day (e.g., emergency, trauma surgeons, hospitalists, intensivists, radiologists, etc). Separately Identify rounding physicians on staff who may come and go for short periods. Enter the total number divided by inpatients for each category of physician (e.g., 20 ÷ 300 = .66).
Will the hospital utilize Volunteers during a disaster response? If so, estimate the number of volunteers per inpatient and enter that figure. For example, if you estimate you will have 300 patients and 20 volunteers per day enter .066 in the cell (20 ÷ 300).
If there are Other essential individuals that are not identified in the sections above, document and estimate the number and enter the ratio per inpatient. As noted previously, it is recommended that estimates be limited to those essential to care/operations.
D. Surge – Emergency Planning Population Assumptions (Summary)
Completing this worksheet will result in a summary of patients, staff and other individuals to be included in the hospital emergency food plan. These figures will carry over to the subsequent worksheets used to identify what, how often and for how long the hospital plans to feed each population category.
21
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool II. Key Assumptions: PATIENT Meal Requirements/Assumptions
The purpose of this worksheet is to identify assumptions for nutritional needs both by patient age/life stage and by meal type (e.g., regular, diabetic, pureed, etc). These estimates will serve as the basis for subsequent steps in emergency food calculations and should be consistent with hospital Nutrition Care Standards as well as emergency meal plan documents describing how specific dietary needs will be met.
Cells in this worksheet colored light orange (dotted line borders) are for hospital data entry. Data should NOT be entered into cells colored light blue (solid line borders) as these are automatic calculations; entry of data into these cells will result in a loss of automatic calculations.
A. Patient Nutritional Needs Per Day
In this section, the hospital will identify the proportion of hospital inpatients in each age/life stage relevant to meal planning and their Basic Daily Nutritional Needs consistent with the hospital Nutrition Care Standards.
Enter the appropriate percentage of total patients in each age/life stage category, include normal newborns in the total. Identify additional categories as appropriate to accommodate hospital specific Nutrition Care Standards.
Enter the Basic Daily Needs for calories, protein and liquid for each age/life stage.
These entries will result in the average Basic Daily Needs for inpatients and will carry over to subsequent worksheets.
B. Patient Dietary Requirements ‐Meal Type
In this table, the hospital will identify the proportion of hospital inpatients by meal type as relevant to meal planning and should be consistent with hospital Nutrition Care Standards and separate emergency meal plans documenting how each need will be met. Enter the appropriate percentage of total patients in each category, include normal newborns in the total. The subtotal, excluding NPO, enteral feeding and infant patients, will serve as the basis for meal and other feeding estimates in subsequent worksheets.
22
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool III. Key Assumptions: PATIENT Meal Plan Assumptions – Inventory
The purpose of this worksheet is to identify PATIENT emergency/disaster menu requirements and translate those requirements to inventory needs. Meal planning assumptions should be consistent with the results of the previous worksheet (II. Patient Meal Requirements), hospital Nutrition Care Standards and emergency meal plan documents describing how specific dietary needs will be met.
Cells in this worksheet colored light orange (dotted line borders) are for hospital data entry. Data should not be entered into cells colored light blue (solid line borders) as these are automatic calculations; entry of data into these cells will result in a loss of automatic calculations.
A. Days of Food
This section will be used to calculate the days of food for patients to be included in emergency food plan calculations. Enter the number of days you plan to feed each category of patient to identify the total days of food required. Two meal planning phases are provided:
Phase 1: Initial period during which hospital may be utilizing more perishables and other food supplies
Phase 2: Subsequent period during which hospital may be limited to staples/non perishables and/or meal replacements.
The Total days for both phases should be no less than 7 days of food for patients to meet Title 22. Patients are broken down by those receiving meals, enteral feeding or infant formula carried forward from previous worksheets.
B. Patient Disaster Menu
This section identifies the average disaster menu for emergency food planning purposes for Phase 1 and Phase 2. Each worksheet is to document the key assumptions underlying the patient menu for each phase, including: • Units of measure to be used in calculating each type of food in the menu (e.g., cups, fluid ounces, grams, etc) • Calories/unit of measure for each type of food (how many calories per ounce of protein, cup of starch, etc) • The units of protein, starch, vegetable, fruit, milk, condiments and oils/fats for each meal provided (per meal) • The calories for snacks, Meals Ready to Eat (MRE) and other meal alternatives and how often they will be used in the
meal plan (each) • Enteral feeding patient and Infant formula assumptions
Based on hospital emergency food plans and Nutrition Care Standards, enter appropriate assumptions into each table. This will result in an average daily unit quantity and calories per patient. For each phase, if you plan to use only MRE or other meal replacements for patients, then populate that row and provide clear documentation of nutritional content in your emergency food plan. If you plan to use a combination, populate the appropriate columns and rows to reflect that plan. For example, if you plan to use MRE for two meal replacements and provide one meal, then you would only enter assumptions for one meal and MRE for two meal replacements into the table (zero out other cells). Daily calories should be at least equal to the average need calculated in Worksheet II ‐ A: Patient Meal Requirements. If the hospital will maintain a single disaster menu, then zero out (do not clear) the servings in the Phase 2 table.
Note: The hospital’s emergency food/meal plan should describe how the regular menu will be modified for different patient menu types (e.g., low sodium, diabetic, etc.) and methods (e.g., ground, pureed). This document addresses emergency food supply calculations, not preparation; however, it is recommended that disaster menus be as consistent as possible across populations and modifications to a basic menu simplified.
23

Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
C. Menu to Inventory Needs and Total Servings
For each worksheet by phase, the final table translates the menu into inventory requirements by taking the daily quantity (e.g., 3 cups of starch) and calculating total ounces for the days of food meal for patients. Enter your assumptions per unit into each table (orange/dotted line cells) and it will calculate the total ounces or quantity required to meet your patient meal plan as well as the average per serving and the number of servings. Because each diet requirement may be met through the use of different resources, the hospital must ensure the food inventory matches the total plan requirements (see later worksheets).
24
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool IV. Key Assumptions: STAFF‐ OTHER Meal Plan Assumptions
The purpose of this worksheet is to identify NON‐PATIENT emergency/disaster menu requirements and translate those requirements to inventory needs. The estimates entered should be consistent with hospital Nutrition Care Standards and emergency meal plan documents describing how specific meal needs will be met for non‐patients. These requirements will differ from patients.
Cells in this worksheet colored light orange (dotted line borders) are for hospital data entry. Data should NOT be entered into cells colored light blue (solid line borders) as these are automatic calculations; entry of data into these cells will result in a loss of automatic calculations and inaccurate results.
A. Meals
This section will calculate the days of food for staff and any other individuals that you may plan for in your emergency food plan. The categories of individuals that could be included in the hospital plan are identified. Two meal planning phases are provided:
Phase 1: Initial period during which hospital may be utilizing more perishables and other food supplies
Phase 2: Subsequent period during which hospital may be limited to staples/non perishables and/or meal replacements.
Enter the number of days in each phase you wish to plan for each category of individual and the number of meals per day to identify the total meals required. For example, your plan may state that you will provide 7 days and 3 meals a day for staff (assuming 3 shifts), 3 a day for hospital physicians but 2 meals per day for rounding physicians and one for volunteers. It is recommended that you plan for a minimum of 4 days for essential staff. Whatever you plan for must be consistent with these calculations and your inventory; therefore, it is recommended that you be prudent but conservative.
B. Staff/Other Disaster Menu
This section identifies the average disaster menu for emergency food planning purposes for Phase 1 and Phase 2 (there is a table for each Phase) The worksheet documents the key assumptions underlying the NON‐PATIENT menu, including:
• Units of measure to be used in calculating each type of food in the menu (cups, grams, etc) • Calories/unit of measure for each type of food (how many calories per gram of protein, cup of starch, etc) • The units of protein, starch, vegetable, fruit, and oils/fats for each meal provided (per meal) • The calories for snacks and Meals Ready to Eat (MRE) and how often they will be used in the meal plan.
Based on hospital emergency food plans, enter your assumptions into the table which will result in an average daily quantity and calories per person. Keep in mind yield versus dry weights when entering as the calculation will result in dry weights needed for inventory. If you plan to use only MRE for non‐patients, then only populate the MRE row and provide clear documentation of their use in your plan (zero out meal cells). If you plan to use a combination of meals and MRE, populate the appropriate columns and rows to reflect that plan. Do this for each Phase. For example, if you plan to use MRE for two meal replacements and provide one meal, then you would enter assumptions for two meals and MRE for one meal (and enter a 0 into the cells in the other columns). Nutritional standards for staff/others should be addressed in your plan.
25
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
C. Menu to Inventory Needs and Average Servings
This table translates the menu into inventory requirements by taking the quantity and translating it to ounces. If the plan calls for an average of 1 cup of starch per meal, then the worksheet will translate that to 8 ounces times the total number of meals. Enter your assumptions per unit into the table and it will calculate the total ounces or quantity required to meet your meal plan, as well as total number of servings (average). Because each diet requirement may be met through the use of different resources, the hospital must ensure the food inventory matches the total plan requirements.
26

Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool V. Key Assumptions: Total Inventory Needs and Servings
The purpose of this worksheet is to summarize both patient and non‐patient (staff and other) emergency/disaster menu food inventory requirements and total servings that inventory should generate. These estimates should be consistent with food inventory lists and actual inventories.
Note: All data in this worksheet is calculated and carried forward from previous worksheets. Data should NOT be entered into cells colored light blue (solid line borders) as these are automatic calculations; entry of data into these cells will result in a loss of automatic calculations.
The data from this worksheet should be utilized to develop/reconcile to food inventory lists and emergency food supplies. This tool should not be integrated into formal emergency food plans until inventory lists and inventories are consistent with the estimated requirements identified through use of the tool.
27
Attachment D Worksheet Instructions
October 31, 2013 EmergFoodWorksheetInstructions
California Hospital Emergency Food Planning Tool VI. Example: Food Inventory and Par List
The purpose of this worksheet is to provide an Example of an inventory format that is linked to the categories of food (Food Type) and calculation methods in the Food Planning Tool.
Note: There are descriptive comments associated with each relevant column header – simply roll your mouse over the column title cell and the comment will pop up. You may also print the page with comments at the end of the page (go to Page Set‐up, Sheet Tab, Comments, and select at End of Sheet from the drop down box).
The information items currently entered into the worksheet are intended to serve as examples only. Each hospital should enter actual inventory items in accordance with their specific plans; however, total items in each Food Type should meet or exceed those calculated using the Tool. For example, if Attachment C‐IV – Meal Plans to Inventories indicates that the hospital needs 91,804 ounces of starch to meet its plan, or 11,476 servings for both patients and others as used in the example, the food inventory should include that amount of starch for that number of servings; again, remember to calculate and document dry versus served amounts for inventory purposes.
28
Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 1
22 CCR Section 70277 Dietetic Service Equipment and Supplies. BARCLAYS OFFICIAL CALIFORNIA CODE OF REGULATIONS
TITLE 22. SOCIAL SECURITY DIVISION 5. LICENSING AND CERTIFICATION OF HEALTH FACILITIES, HOME HEALTH
AGENCIES, CLINICS, AND REFERRAL AGENCIES CHAPTER 1. GENERAL ACUTE CARE HOSPITALS
ARTICLE 3. BASIC SERVICES This database is current through 4/16/10 Register 2010, No. 16.
§ 70277. Dietetic Service Equipment and Supplies. (a) Equipment of the type and in the amount necessary for the proper preparation, serving and storing of food and for proper dishwashing shall be provided and maintained in good working order.
(1) The dietetic service area shall be ventilated in a manner that will maintain comfortable working conditions, remove objectionable odors and fumes and prevent excessive condensation. (2) Equipment necessary for preparation and maintenance of menus, records and references shall be provided. (3) Fixed and mobile equipment in the dietetic service area shall be located to assure sanitary and safe operation and shall be of sufficient size to handle the needs of the hospital. (b) Food Supplies.
(1) At least one week's supply of staple foods and at least two (2) days supply of perishable foods shall be maintained on the premises. Supplies shall be appropriate to meet the requirements of the menu. (2) All food shall be of good quality and procured from sources approved or considered satisfactory by federal, state and local authorities. Food in unlabeled, rusty, leaking, broken containers or cans with side seam dents, rim dents or swells shall not be accepted or retained. (3) Milk, milk products and products resembling milk shall be processed or manufactured in milk product plants meeting the requirements of Division 15 of the California Food and Agricultural Code. (4) Milk may be served in individual containers, the cap or seal of which shall not be removed except in the presence of the patient. Milk may be served from a dispensing device which has been approved for such use. Milk served from an approved device shall be dispensed directly into the glass or other container from which the patient drinks. (5) Catered foods and beverages from a source outside the hospital shall be prepared, packed, properly identified, stored and transported in compliance with these regulations and other applicable federal, state and local codes as determined by the Department. (6) Foods held in refrigerated or other storage areas shall be appropriately covered. Food which was prepared and not served shall be stored appropriately, clearly labeled and dated. (7) Hermetically sealed foods or beverages served in the hospital shall have been processed in compliance with applicable federal, state and local codes.
29
Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 2
Title 24 – Part 2
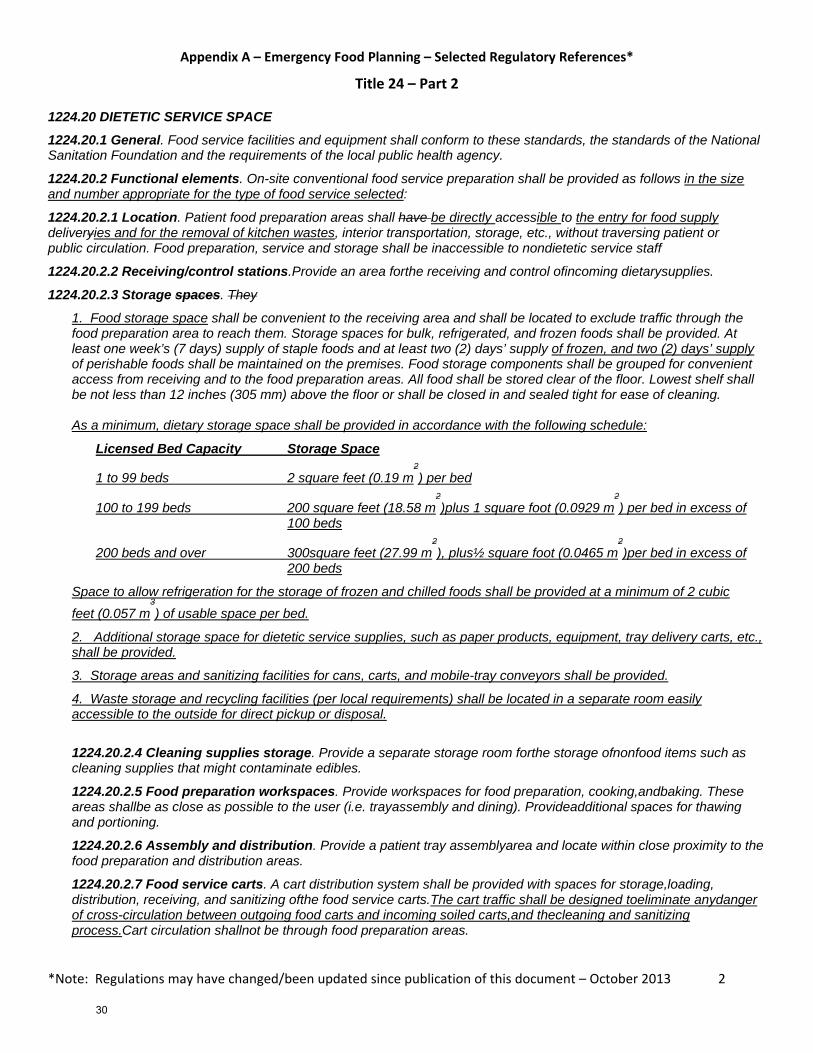
1224.20 DIETETIC SERVICE SPACE 1224.20.1 General. Food service facilities and equipment shall conform to these standards, the standards of the National Sanitation Foundation and the requirements of the local public health agency.
1224.20.2 Functional elements. On-site conventional food service preparation shall be provided as follows in the size and number appropriate for the type of food service selected:
1224.20.2.1 Location. Patient food preparation areas shall have be directly accessible to the entry for food supply deliveryies and for the removal of kitchen wastes, interior transportation, storage, etc., without traversing patient or public circulation. Food preparation, service and storage shall be inaccessible to nondietetic service staff
1224.20.2.2 Receiving/control stations.Provide an area forthe receiving and control ofincoming dietarysupplies.
1224.20.2.3 Storage spaces. They
1. Food storage space shall be convenient to the receiving area and shall be located to exclude traffic through the food preparation area to reach them. Storage spaces for bulk, refrigerated, and frozen foods shall be provided. At least one week’s (7 days) supply of staple foods and at least two (2) days’ supply of frozen, and two (2) days’ supply of perishable foods shall be maintained on the premises. Food storage components shall be grouped for convenient access from receiving and to the food preparation areas. All food shall be stored clear of the floor. Lowest shelf shall be not less than 12 inches (305 mm) above the floor or shall be closed in and sealed tight for ease of cleaning. As a minimum, dietary storage space shall be provided in accordance with the following schedule:
Licensed Bed Capacity Storage Space
1 to 99 beds 2 square feet (0.19 m2) per bed
100 to 199 beds 200 square feet (18.58 m2)plus 1 square foot (0.0929 m
2) per bed in excess of
100 beds
200 beds and over 300square feet (27.99 m2), plus½ square foot (0.0465 m
2)per bed in excess of
200 beds
Space to allow refrigeration for the storage of frozen and chilled foods shall be provided at a minimum of 2 cubic feet (0.057 m
3) of usable space per bed.
2. Additional storage space for dietetic service supplies, such as paper products, equipment, tray delivery carts, etc., shall be provided.
3. Storage areas and sanitizing facilities for cans, carts, and mobile-tray conveyors shall be provided.
4. Waste storage and recycling facilities (per local requirements) shall be located in a separate room easily accessible to the outside for direct pickup or disposal.
1224.20.2.4 Cleaning supplies storage. Provide a separate storage room forthe storage ofnonfood items such as cleaning supplies that might contaminate edibles.
1224.20.2.5 Food preparation workspaces. Provide workspaces for food preparation, cooking,andbaking. These areas shallbe as close as possible to the user (i.e. trayassembly and dining). Provideadditional spaces for thawing and portioning.
1224.20.2.6 Assembly and distribution. Provide a patient tray assemblyarea and locate within close proximity to the food preparation and distribution areas.
1224.20.2.7 Food service carts. A cart distribution system shall be provided with spaces for storage,loading, distribution, receiving, and sanitizing ofthe food service carts.The cart traffic shall be designed toeliminate anydanger of cross-circulation between outgoing food carts and incoming soiled carts,and thecleaning and sanitizing process.Cart circulation shallnot be through food preparation areas.
30
Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 3
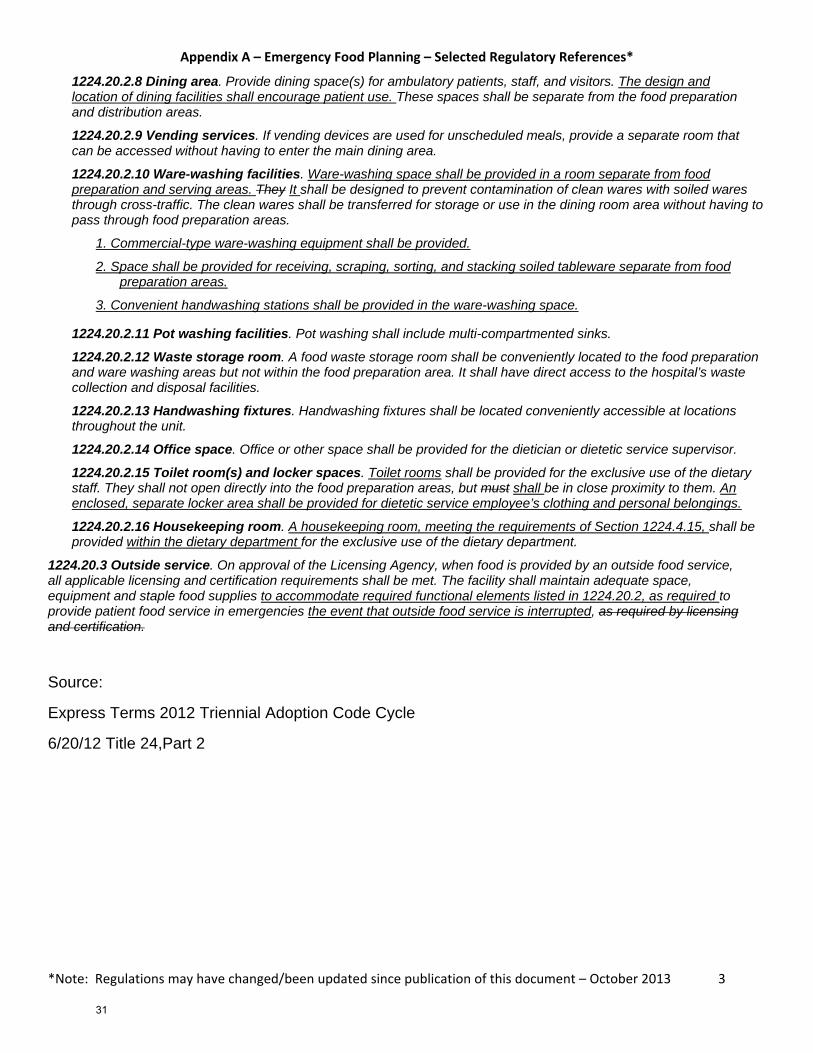
1224.20.2.8 Dining area. Provide dining space(s) for ambulatory patients, staff, and visitors. The design and location of dining facilities shall encourage patient use. These spaces shall be separate from the food preparation and distribution areas.
1224.20.2.9 Vending services. If vending devices are used for unscheduled meals, provide a separate room that can be accessed without having to enter the main dining area.
1224.20.2.10 Ware-washing facilities. Ware-washing space shall be provided in a room separate from food preparation and serving areas. They It shall be designed to prevent contamination of clean wares with soiled wares through cross-traffic. The clean wares shall be transferred for storage or use in the dining room area without having to pass through food preparation areas.
1. Commercial-type ware-washing equipment shall be provided.
2. Space shall be provided for receiving, scraping, sorting, and stacking soiled tableware separate from food preparation areas.
3. Convenient handwashing stations shall be provided in the ware-washing space.
1224.20.2.11 Pot washing facilities. Pot washing shall include multi-compartmented sinks.
1224.20.2.12 Waste storage room. A food waste storage room shall be conveniently located to the food preparation and ware washing areas but not within the food preparation area. It shall have direct access to the hospital’s waste collection and disposal facilities.
1224.20.2.13 Handwashing fixtures. Handwashing fixtures shall be located conveniently accessible at locations throughout the unit.
1224.20.2.14 Office space. Office or other space shall be provided for the dietician or dietetic service supervisor.
1224.20.2.15 Toilet room(s) and locker spaces. Toilet rooms shall be provided for the exclusive use of the dietary staff. They shall not open directly into the food preparation areas, but must shall be in close proximity to them. An enclosed, separate locker area shall be provided for dietetic service employee’s clothing and personal belongings.
1224.20.2.16 Housekeeping room. A housekeeping room, meeting the requirements of Section 1224.4.15, shall be provided within the dietary department for the exclusive use of the dietary department.
1224.20.3 Outside service. On approval of the Licensing Agency, when food is provided by an outside food service, all applicable licensing and certification requirements shall be met. The facility shall maintain adequate space, equipment and staple food supplies to accommodate required functional elements listed in 1224.20.2, as required to provide patient food service in emergencies the event that outside food service is interrupted, as required by licensing and certification.
Source:
Express Terms 2012 Triennial Adoption Code Cycle
6/20/12 Title 24,Part 2
31

Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 4
22 CCR Section 70741 Acute Hospital Disaster Program BARCLAYS OFFICIAL CALIFORNIA CODE OF REGULATIONS
TITLE 22. SOCIAL SECURITY DIVISION 5. LICENSING AND CERTIFICATION OF HEALTH FACILITIES, HOME HEALTH
AGENCIES, CLINICS, AND REFERRAL AGENCIES CHAPTER 1. GENERAL ACUTE CARE HOSPITALS
ARTICLE 7. ADMINISTRATION This database is current through 4/16/10 Register 2010, No. 16.
§ 70741. Disaster and Mass Casualty Program. (a) A written disaster and mass casualty program shall be developed and maintained in consultation with representatives of the medical staff, nursing staff, administration and fire and safety experts. The program shall be in conformity with the California Emergency Plan of October 10, 1972 developed by the State Office of Emergency Services and the California Emergency Medical Mutual Aid Plan of March 1974 developed by the Office of Emergency Services, Department of Health. The program shall be approved by the medical staff and administration. A copy of the program shall be available on the premises for review by the Department. (b) The program shall cover disasters occurring in the community and widespread disasters. It shall provide for at least the following:
(1) Availability of adequate basic utilities and supplies, including gas, water, food and essential medical and supportive materials. (2) An efficient system of notifying and assigning personnel. (3) Unified medical command. (4) Conversion of all usable space into clearly defined areas for efficient triage, for patient observation and for immediate care. (5) Prompt transfer of casualties, when necessary and after preliminary medical or surgical services have been rendered, to the facility most appropriate for administering definite care. (6) A special disaster medical record, such as an appropriately designed tag, that accompanies the casualty as he is moved. (7) Procedures for the prompt discharge or transfer of patients already in the hospital at the time of the disaster who can be moved without jeopardy. (8) Maintaining security in order to keep relatives and curious persons out of the triage area. (9) Establishment of a public information center and assignment of public relations liaison duties to a qualified individual. Advance arrangements with communications media will be made to provide organized dissemination of information. (c) The program shall be brought up-to-date, at least annually, and all personnel shall be instructed in its requirements. There shall be evidence in the personnel files, e.g., orientation checklist or elsewhere, indicating that all new employees have been oriented to the program and procedures within a reasonable time after commencement of their employment. (d) The disaster plan shall be rehearsed at least twice a year. There shall be a written report and evaluation of all drills. The actual evacuation of patients to safe areas during the drill is optional.
32
Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 5
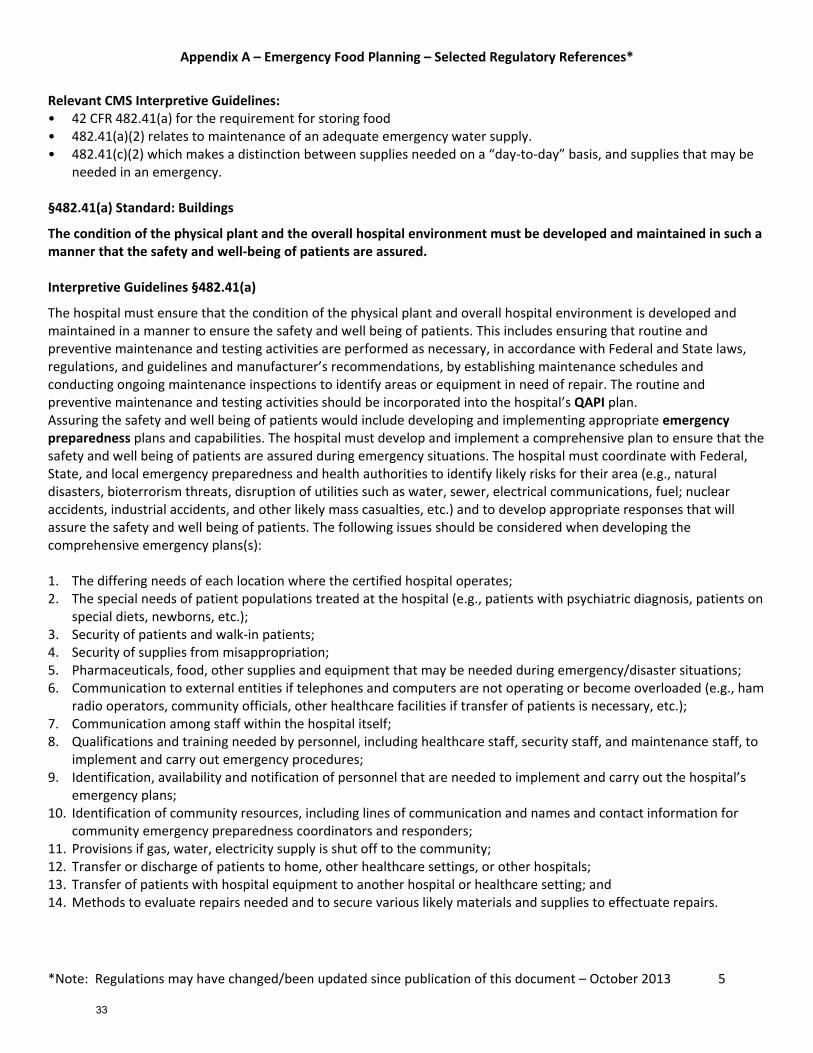
Relevant CMS Interpretive Guidelines: • 42 CFR 482.41(a) for the requirement for storing food • 482.41(a)(2) relates to maintenance of an adequate emergency water supply. • 482.41(c)(2) which makes a distinction between supplies needed on a “day‐to‐day” basis, and supplies that may be
needed in an emergency. §482.41(a) Standard: Buildings
The condition of the physical plant and the overall hospital environment must be developed and maintained in such a manner that the safety and well‐being of patients are assured. Interpretive Guidelines §482.41(a)
The hospital must ensure that the condition of the physical plant and overall hospital environment is developed and maintained in a manner to ensure the safety and well being of patients. This includes ensuring that routine and preventive maintenance and testing activities are performed as necessary, in accordance with Federal and State laws, regulations, and guidelines and manufacturer’s recommendations, by establishing maintenance schedules and conducting ongoing maintenance inspections to identify areas or equipment in need of repair. The routine and preventive maintenance and testing activities should be incorporated into the hospital’s QAPI plan. Assuring the safety and well being of patients would include developing and implementing appropriate emergency preparedness plans and capabilities. The hospital must develop and implement a comprehensive plan to ensure that the safety and well being of patients are assured during emergency situations. The hospital must coordinate with Federal, State, and local emergency preparedness and health authorities to identify likely risks for their area (e.g., natural disasters, bioterrorism threats, disruption of utilities such as water, sewer, electrical communications, fuel; nuclear accidents, industrial accidents, and other likely mass casualties, etc.) and to develop appropriate responses that will assure the safety and well being of patients. The following issues should be considered when developing the comprehensive emergency plans(s): 1. The differing needs of each location where the certified hospital operates; 2. The special needs of patient populations treated at the hospital (e.g., patients with psychiatric diagnosis, patients on
special diets, newborns, etc.); 3. Security of patients and walk‐in patients; 4. Security of supplies from misappropriation; 5. Pharmaceuticals, food, other supplies and equipment that may be needed during emergency/disaster situations; 6. Communication to external entities if telephones and computers are not operating or become overloaded (e.g., ham
radio operators, community officials, other healthcare facilities if transfer of patients is necessary, etc.); 7. Communication among staff within the hospital itself; 8. Qualifications and training needed by personnel, including healthcare staff, security staff, and maintenance staff, to
implement and carry out emergency procedures; 9. Identification, availability and notification of personnel that are needed to implement and carry out the hospital’s
emergency plans; 10. Identification of community resources, including lines of communication and names and contact information for
community emergency preparedness coordinators and responders; 11. Provisions if gas, water, electricity supply is shut off to the community; 12. Transfer or discharge of patients to home, other healthcare settings, or other hospitals; 13. Transfer of patients with hospital equipment to another hospital or healthcare setting; and 14. Methods to evaluate repairs needed and to secure various likely materials and supplies to effectuate repairs.
33
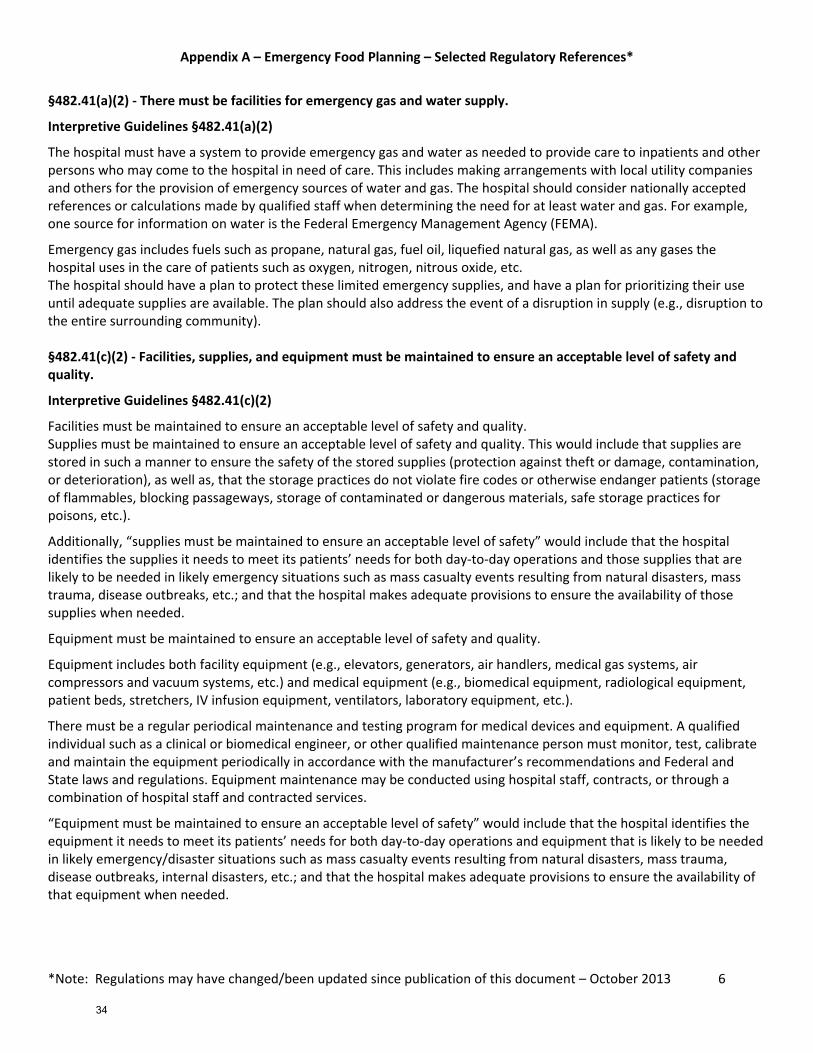
Appendix A – Emergency Food Planning – Selected Regulatory References*
*Note: Regulations may have changed/been updated since publication of this document – October 2013 6
§482.41(a)(2) ‐ There must be facilities for emergency gas and water supply.
Interpretive Guidelines §482.41(a)(2)
The hospital must have a system to provide emergency gas and water as needed to provide care to inpatients and other persons who may come to the hospital in need of care. This includes making arrangements with local utility companies and others for the provision of emergency sources of water and gas. The hospital should consider nationally accepted references or calculations made by qualified staff when determining the need for at least water and gas. For example, one source for information on water is the Federal Emergency Management Agency (FEMA).
Emergency gas includes fuels such as propane, natural gas, fuel oil, liquefied natural gas, as well as any gases the hospital uses in the care of patients such as oxygen, nitrogen, nitrous oxide, etc. The hospital should have a plan to protect these limited emergency supplies, and have a plan for prioritizing their use until adequate supplies are available. The plan should also address the event of a disruption in supply (e.g., disruption to the entire surrounding community). §482.41(c)(2) ‐ Facilities, supplies, and equipment must be maintained to ensure an acceptable level of safety and quality.
Interpretive Guidelines §482.41(c)(2)
Facilities must be maintained to ensure an acceptable level of safety and quality. Supplies must be maintained to ensure an acceptable level of safety and quality. This would include that supplies are stored in such a manner to ensure the safety of the stored supplies (protection against theft or damage, contamination, or deterioration), as well as, that the storage practices do not violate fire codes or otherwise endanger patients (storage of flammables, blocking passageways, storage of contaminated or dangerous materials, safe storage practices for poisons, etc.).
Additionally, “supplies must be maintained to ensure an acceptable level of safety” would include that the hospital identifies the supplies it needs to meet its patients’ needs for both day‐to‐day operations and those supplies that are likely to be needed in likely emergency situations such as mass casualty events resulting from natural disasters, mass trauma, disease outbreaks, etc.; and that the hospital makes adequate provisions to ensure the availability of those supplies when needed.
Equipment must be maintained to ensure an acceptable level of safety and quality.
Equipment includes both facility equipment (e.g., elevators, generators, air handlers, medical gas systems, air compressors and vacuum systems, etc.) and medical equipment (e.g., biomedical equipment, radiological equipment, patient beds, stretchers, IV infusion equipment, ventilators, laboratory equipment, etc.).
There must be a regular periodical maintenance and testing program for medical devices and equipment. A qualified individual such as a clinical or biomedical engineer, or other qualified maintenance person must monitor, test, calibrate and maintain the equipment periodically in accordance with the manufacturer’s recommendations and Federal and State laws and regulations. Equipment maintenance may be conducted using hospital staff, contracts, or through a combination of hospital staff and contracted services.
“Equipment must be maintained to ensure an acceptable level of safety” would include that the hospital identifies the equipment it needs to meet its patients’ needs for both day‐to‐day operations and equipment that is likely to be needed in likely emergency/disaster situations such as mass casualty events resulting from natural disasters, mass trauma, disease outbreaks, internal disasters, etc.; and that the hospital makes adequate provisions to ensure the availability of that equipment when needed.
34
*Note: References only, please review complete, current standards. Standards may have changed/been updated since publication of this document.
Appendix B Emergency Food Planning References
Accrediting Agency References*
Standard ‐‐
Element of Performance Agency ‐ Description
The Joint Commission EM 01.01.01 EP 8
The hospital keeps a documented inventory of the resources and assets it has on site that may be needed during an emergency, including, but not limited to, personal protective equipment, water, fuel, and medical, surgical and medication‐related resources and assets (See also EM.02.02.03, EP6)
EM.02.01.01 EP 3
The Emergency Operations Plan identifies the hospital’s capabilities and establishes response procedures for when the hospital cannot be supported by the local community in the hospitals efforts to provide communications, resource and assets, security and safety, staff, utilities, or patient care for at least 96 hours. Note: Hospitals are not required to stockpile supplies to last for 96 hours of operation.
EM.02.02.03 EP 3
The Emergency Operations Plan describes the following: How the hospital will obtain and replenish non‐medical supplies that will be required through the response and recovery phases of an emergency.
EM.02.02.03 EP 6
The Emergency Operations Plan describes the following: How the hospital will monitor quantities of its resources and assets during an emergency. (See also EM.01.01.01, EP 8)
EM.02.02.07 EP 5
The Emergency Operations Plan describes how the hospital will manage staff support needs (for example, housing, transportation and incident stress debriefing)
EM.02.02.07 EP 6
The Emergency Operations Plan describes how the hospital will manage the family support needs of staff (for example, child care, elder care and communication).
National Fire Prevention Association (NFPA99) Chapter 11 Health Care Emergency Preparedness 11‐5.3.5* Logistics. Contingency planning for disasters shall include as a minimum stockpiling or ensuring
immediate or at least uninterrupted access to critical materials such as the following: (a) Pharmaceuticals (b) Medical supplies (c) Food supplies (d) Industrial and potable (drinking) water
Health Facilities Accreditation Program (HFAP): Nutritional Services 24.00.12 Emergency Preparedness Plan
The Emergency Preparedness Plan of the facilities addresses methods for ensuring the nutritional needs of patients and personnel during an internal or external emergency or disaster. (See accreditation documents for explanation and scoring)
Det Norske Veritas (DNV) Healthcare PE6 SR2
Emergency Management Systems The organization shall meet the requirements set forth in NFPA 99, Chapter 12, Emergency Management (See NFPA99)
CHA Hospital Preparedness Program Emergency Food Planning Guidance Reference – October, 2013
35