
California Advancing and Innovating Medi-Cal (CalAIM) 1915 ...
60
California Advancing and Innovating Medi-Cal (CalAIM) 1915(b) Waiver Overview April 2021 The California Department of Health Care Services (DHCS) will request to renew and amend its Section 1915(b) waiver to consolidate and better align all managed care authorities in order to continue advancing the State’s goal of improving health outcomes for Medi-Cal beneficiaries. Currently, California’s Section 1915(b) waiver authorizes the Specialty Mental Health Services program while other Medi-Cal managed care programs are authorized under California’s current Section 1115 demonstration. Effective January 1, 2022, the CalAIM Section 1915(b) waiver will authorize nearly all of California’s managed care programs, enabling the State to take advantage of flexibilities to implement a more seamless, integrated, and whole person focused delivery system and to support additional benefits for Medi-Cal beneficiaries. See Appendix, Attachment 1 for a table outlining these waiver authority changes. DHCS’ submission of the consolidated Section 1915(b) waiver to the Centers for Medicare & Medicaid Services (CMS) will be in the form of a federally prescribed template, or “waiver pre-print.” To enhance stakeholder understanding, this document summarizes the core components of the CalAIM Section 1915(b) waiver application and the key policies related to the delivery systems that will be authorized under the Section 1915(b) waiver. In coordination with the renewal and amendment of the Section 1915(b) waiver described here, DHCS also will request a five-year renewal and amendment of the State’s current Section 1115 demonstration. The renewal and amendment of the 1115 demonstration—which will be renamed the CalAIM Demonstration—along with the 1915(b) waiver and related contractual and State Plan changes will enable California to provide benefits to certain high-needs, hard-to-reach populations, with the objective of improving health outcomes for Medi-Cal beneficiaries and other low-income people in the State. The proposed Section 1115 demonstration renewal is being released for public comment concurrently with this overview of the Section 1915(b) waiver to offer stakeholders a comprehensive view of and an opportunity to comment on this stage of implementation of the broader CalAIM initiative; visit the DHCS website for an updated overview of CalAIM. Background and Context After extensive stakeholder engagement, DHCS developed a framework that encompasses broad-based delivery system, program, and payment reform across the Medi-Cal program, called California Advancing and Innovating Medi-Cal (CalAIM). CalAIM advances several key priorities of the Newsom administration to help address many of the complex challenges facing California’s most vulnerable residents, such as the growing number of justice-involved populations who have significant clinical needs, and the increasing aging population. CalAIM has three primary goals:
Transcript of California Advancing and Innovating Medi-Cal (CalAIM) 1915 ...

California Advancing and Innovating Medi-Cal (CalAIM) 1915(b) Waiver Overview
April 2021 The California Department of Health Care Services (DHCS) will request to renew and amend its Section 1915(b) waiver to consolidate and better align all managed care authorities in order to continue advancing the State’s goal of improving health outcomes for Medi-Cal beneficiaries. Currently, California’s Section 1915(b) waiver authorizes the Specialty Mental Health Services program while other Medi-Cal managed care programs are authorized under California’s current Section 1115 demonstration. Effective January 1, 2022, the CalAIM Section 1915(b) waiver will authorize nearly all of California’s managed care programs, enabling the State to take advantage of flexibilities to implement a more seamless, integrated, and whole person focused delivery system and to support additional benefits for Medi-Cal beneficiaries. See Appendix, Attachment 1 for a table outlining these waiver authority changes. DHCS’ submission of the consolidated Section 1915(b) waiver to the Centers for Medicare & Medicaid Services (CMS) will be in the form of a federally prescribed template, or “waiver pre-print.” To enhance stakeholder understanding, this document summarizes the core components of the CalAIM Section 1915(b) waiver application and the key policies related to the delivery systems that will be authorized under the Section 1915(b) waiver.
In coordination with the renewal and amendment of the Section 1915(b) waiver described here, DHCS also will request a five-year renewal and amendment of the State’s current Section 1115 demonstration. The renewal and amendment of the 1115 demonstration—which will be renamed the CalAIM Demonstration—along with the 1915(b) waiver and related contractual and State Plan changes will enable California to provide benefits to certain high-needs, hard-to-reach populations, with the objective of improving health outcomes for Medi-Cal beneficiaries and other low-income people in the State. The proposed Section 1115 demonstration renewal is being released for public comment concurrently with this overview of the Section 1915(b) waiver to offer stakeholders a comprehensive view of and an opportunity to comment on this stage of implementation of the broader CalAIM initiative; visit the DHCS website for an updated overview of CalAIM.
Background and Context After extensive stakeholder engagement, DHCS developed a framework that encompasses broad-based delivery system, program, and payment reform across the Medi-Cal program, called California Advancing and Innovating Medi-Cal (CalAIM). CalAIM advances several key priorities of the Newsom administration to help address many of the complex challenges facing California’s most vulnerable residents, such as the growing number of justice-involved populations who have significant clinical needs, and the increasing aging population. CalAIM has three primary goals:

2
• Identify and manage member risk and need through whole person care approaches and addressing social determinants of health;
• Move Medi-Cal to a more consistent and seamless system by reducing complexity and increasing flexibility; and
• Improve quality outcomes, reduce health disparities, and drive delivery system transformation and innovation through value-based initiatives, modernization of systems, and payment reform.
Central to achieving the vision for CalAIM is greater alignment and integration of the Medi-Cal delivery system, which will be enabled by the consolidation of federal managed care authorities into a single waiver vehicle for:
• Medi-Cal Managed Care (MCMC); • Dental Managed Care (Dental MC); • The Specialty Mental Health Services (SMHS) Program; and • The Drug Medi-Cal Organized Delivery System (DMC-ODS).
To date, California has utilized Section 1115 to authorize most parts of Medi-Cal’s managed care delivery system. Section 1915(b) of the Social Security Act provides states with another way to authorize and operate their Medicaid managed care delivery systems. California has long-standing experience with the Section 1915(b) waiver for SMHS. As part of implementing CalAIM, California will transition federal Medicaid managed care authority from the Medi-Cal 2020 Section 1115 demonstration to a renewal and amendment of the Section 1915(b) waiver (“CalAIM 1915(b) waiver” or “consolidated 1915(b) waiver”). This change will enable the State to streamline, align, and simplify federal authorities; maintain flexibilities to further integrate the Medi-Cal delivery system; and fund additional services for Medi-Cal beneficiaries through savings generated by the use of managed care (known as “1915(b)(3) services”). The State is also utilizing this opportunity to update and clarify the SMHS program requirements, including the division of responsibility between Medi-Cal Managed Care Plans (MCPs) and Mental Health Plans (MHPs) and processes related to getting beneficiaries to the right delivery system; modify DMC-ODS program elements to clarify or change policies in order to improve beneficiary access to care; improve administrative efficiency in both SMHS and DMC-ODS; and reform the payment system for behavioral health services. Along with the authorities that DHCS will request through the consolidated 1915(b) waiver, DHCS is requesting authority to continue key elements of its 1115 demonstration to ensure that California has all necessary authorities to implement CalAIM. DHCS is requesting a five-year renewal of some of the waiver and expenditure authorities contained in the expiring Medi-Cal 2020 demonstration as well as certain new authorities to enable the State to complete the transition to the new structure contemplated under CalAIM. The State’s draft 1115 demonstration renewal and amendment request for the renamed Cal-AIM demonstration was posted for a 30-day public comment on the DHCS website.

3
DHCS’ 1915(b) waiver submission to CMS will be made through a federally prescribed template, or “waiver pre-print.” In the pre-print, which DHCS will submit to CMS later this spring, DHCS will:
• Describe the consolidated Medi-Cal managed care delivery system; • Provide assurances on federal Medicaid managed care requirements; • Provide calculations on how spending is cost-effective, efficient, and consistent
with the principles of the Medicaid program; and • Share its plan for active monitoring on program impact, access, and quality of
services in the managed care delivery system.
DHCS will request the CalAIM 1915(b) waiver be effective January 1, 2022, through December 31, 2026. The full 1915(b) waiver pre-print will be posted on the CalAIM website upon submission to CMS. In addition to the pre-print application, California will negotiate various protocols and plans with CMS to govern waiver implementation. Documents will be posted on the DHCS website following approval.
The purpose of this document is to provide an overview of the State’s proposed approach to the CalAIM 1915(b) waiver so that stakeholders continue to be informed about policy developments and can assess how the 1915(b) waiver will work in tandem with the renewal and amendment of the 1115 demonstration (also open for public comment) to achieve the integrated CalAIM vision. Please note that California’s discussions and negotiations with the federal government on the Section 1915(b) waiver, Section 1115 demonstration, and other federal authorities, and California’s state legislative and budget process, could lead to refinements of these proposed policies and financing approaches.
Integrated Delivery System Vision and Approach Medi-Cal—California's Medicaid and Children’s Health Insurance Program (CHIP) —provides comprehensive health care coverage at no or low cost for 13.4 million low-income individuals, or one in three Californians. More than 11 million individuals access their coverage through Medi-Cal’s managed care infrastructure and, depending on their needs, some of these beneficiaries may access multiple delivery systems (e.g., managed care for physical health needs, fee-for-service (FFS), specialty mental health, substance use disorder (SUD), dental, developmental, In Home Supportive Services). As one would expect, the risk of service gaps and the need for care coordination increases with greater system fragmentation, clinical complexity, deeper social needs, and/or decreased patient capacity for coordinating their own care. In order to meet the physical, behavioral, developmental, and oral health needs of all members in an integrated, patient-centered, whole person fashion, DHCS is seeking to—over time—integrate delivery systems and align funding, data reporting, quality, and infrastructure to mobilize, incentivize, and support care delivery toward common goals. Transitioning Medi-Cal’s managed care programs to a single, consolidated 1915(b) waiver, while
4
continuing key 1115 demonstration initiatives, is an important step forward along this path.
The CalAIM 1915(b) waiver will bring each of the delivery systems reviewed below into one federal authority, standardizing federal requirements to the extent possible and reducing administrative complexity. Also, as described below, the State will make changes to the populations, benefits, and financing of Medi-Cal’s managed care delivery that seek to promote consistency and integration across Medi-Cal. (See Appendix, Attachment 1 for an overview of the programs being authorized and the associated program modifications and improvements under the consolidated 1915(b) waiver and delivery system.)
Medi-Cal Managed Care
MCMC operates in all 58 counties in the state, providing coverage for physical health and nonspecialty mental health services for approximately 82 percent of the Medi-Cal population through Medi-Cal MCPs. Six MCMC models operate in the state, varying by county or region:
• County-Organized Health System (COHS): Beneficiaries are served by a single plan that is created and administered by a county’s board of supervisors, or other local health authority.
• Two-Plan: Beneficiaries choose between a single publicly run entity known as a local initiative plan and a single commercial plan.
• Geographic Managed Care (GMC): Beneficiaries choose from multiple commercial health plans.
• Regional: Beneficiaries choose between two or more commercial health plans. • Imperial: Beneficiaries in Imperial County choose between two commercial health
plans • San Benito: Beneficiaries in San Benito County choose between a single
commercial plan and FFS.
The MCMC program is currently authorized under California’s Medi-Cal 2020 Section 1115 demonstration through December 31, 2021. Through the 1915(b) waiver renewal and amendment described here, California will seek to shift the authority for MCMC from Section 1115 to Section 1915(b). California will also seek to continue MCMC-related program authority previously in the 1115 demonstration to:
5
• Require individuals dually eligible for Medi-Cal and Medicare (“dual eligible”) in Coordinated Care Initiative (CCI) counties to enroll in MCMC for Medi-Cal benefits;1 and
• Allow Med-Cal beneficiaries in selected COHS counties to enroll in a Program of All-Inclusive Care for the Elderly (PACE) independent of the COHS MCP.
In addition, DHCS will seek in the CalAIM 1915(b) waiver to require additional populations enroll in MCMC and to further standardize benefits offered through MCMC as described below.
Populations. Currently, most Medi-Cal children, pregnant women, parents/caretaker relatives, and adults without disabilities are required to enroll in MCMC to access their services (“mandatory enrollment”). Seniors and Persons with Disabilities (SPDs) in Two-Plan and GMC counties (16 counties) are also required to enroll in MCMC. American Indians and Alaska Natives, dual eligibles in non-COHS and non-CCI counties, foster children and youth in non-COHS counties, all beneficiaries in San Benito County, and several other populations have the option but are not required to enroll in MCMC (“voluntary enrollment”). Certain populations—such as beneficiaries with other health care coverage in non-COHS counties and beneficiaries in rural zip codes in non-COHS counties—are excluded from MCMC enrollment, meaning they do not have the opportunity to enroll in an MCP and instead access their Medi-Cal services through FFS (“excluded”). Under CalAIM, DHCS is proposing to further standardize MCMC enrollment and require certain additional aid code groups to enroll in MCMC in all counties starting in 2022, and require all dual eligibles to enroll in MCMC in 2023. This will allow MCPs to provide more coordinated and integrated care statewide and provide beneficiaries who have been in FFS or who have not been required to enroll in an MCP with a network of primary care providers and specialists. These aid code groups comprise: Trafficking and Crime Victims Assistance Program (except share of cost); Individuals participating in accelerated enrollment; Child Health and Disability Prevention infant deeming; and Pregnancy-related Medi-Cal (Pregnant Women only, 138-213% citizen/lawfully present). Some American Indians and Alaska Natives may be eligible for Medi-Cal coverage in these additional aid code groups that will be subject to mandatory MCMC enrollment. As is consistent with current policy, all American Indians and Alaska Natives residing in
1 CCI is a Medi-Cal managed care program in seven counties that is designed to provide integrated care across delivery systems and rebalance service delivery away from institutional care and into the home and community. CCI is comprised of two parts: (1) Cal MediConnect (CMC), a Section 1115A demonstration project under the federal Financial Alignment Initiative that combines acute, primary, institutional, and home and community-based services into a single benefit package for Medicaid eligible individuals who are fully or partially eligible for Medicare; and (2) mandatory Medi-Cal managed care enrollment for dual eligibles, and Medi-Cal managed care carve-in for some long-term services and supports.

6
non-COHS counties will continue to have the ability to opt out of MCMC for FFS. In non-COHS counties, beneficiaries with other health coverage and beneficiaries in rural zip codes will no longer be excluded and will be subject to mandatory MCMC enrollment.
DHCS is also proposing to transition both components of CCI (i.e., Cal MediConnect and mandatory MCMC enrollment and LTSS carve-in) into a statewide aligned enrollment structure, in which dual eligible beneficiaries will enroll in a Medi-Cal MCP and have the option to enroll in a dual eligible special needs plan (D-SNP) operated by the same parent company to allow for greater integration and coordination of care. This will be an important step to achieving integration of long-term services and supports (LTSS) into MCMC for dual eligible beneficiaries in all counties. DHCS plans to begin the transition to aligned enrollment in the seven CCI counties starting in 2023, and will expand this approach statewide by 2025.
For a detailed breakdown of managed care enrollment, please see Appendix F of the CalAIM proposal.
Benefits. With certain key exceptions, most Medi-Cal State Plan services are covered under MCMC. However, depending on the MCMC model, certain benefits may be part of the MCP responsibility or provided through another delivery system. Services not covered under MCMC include specialty mental health services, SUD services, and most long-term care services except in CCI and COHS counties. Finally, pursuant to Executive Order N-01-19, the State is in the process of carving out pharmacy benefits from MCPs as a component of the Medi-Cal Rx initiative.2 Under CalAIM, DHCS is proposing to further standardize benefits offered by the MCPs, which will mitigate MCMC enrollee confusion and streamline DHCS administrative rate-setting processes. Effective in 2022, DHCS intends to carve out the Multipurpose Senior Services Program (MSSP, only available in CCI counties) to FFS and carve out specialty mental health services from the MCMC benefit package for Medi-Cal members enrolled in Kaiser in Solano and Sacramento counties. DHCS intends to carve into the MCMC benefit package statewide major organ transplants by 2022 and institutional long-term care services by 2023. Beneficiaries requiring specialty mental health and SUD services will continue to access those services through the SMHS and DMC-ODS or Drug Medi-Cal programs (discussed further below). (For a detailed breakdown of managed care benefit changes, please see Appendix E of the CalAIM proposal.)
2 On February 17, 2021, DHCS announced a delay to the planned April 1, 2021 effective date for Medi-Cal Rx and the carve-out of pharmacy benefits from MCMC contracts. This delay was due to a need to review new conflict avoidance protocols associated with the contracted vendor for Medi-Cal Rx. DHCS anticipates providing further information, including with respect to a revised effective date for the carve-out, in May 2021.

7
A major change going forward for MCMC is the addition of Enhanced Care Management (ECM) and In Lieu of Services (ILOS). Based on the success of the Medi-Cal 2020 Whole Person Care (WPC) pilots and the State’s Health Homes Program (HHP), a key feature of CalAIM is the introduction of ECM as a statewide benefit, as well as ILOS, which, at the option of a plan and member can be offered to members as a cost-effective alternative to State Plan benefits. MCPs will be responsible for administering both ECM and ILOS, by contracting with local community-based providers, with a phased implementation for ECM beginning in 2022 and State-approved ILOS available beginning in 2022. The consolidated 1915(b) waiver will provide the authority for the MCMC program in general, while MCP contracts and other policy guidance will authorize and likely be the vehicle to establish ECM and ILOS. Finally, subject to ongoing deliberations with the State’s contracted vendor for Medi-Cal Rx, DHCS intends to carve pharmacy benefits out of the MCMC benefit package, at an effective date to be subsequently announced.3
Dental Managed Care
Dental services are currently provided through Dental MC plans in two California counties—Sacramento and Los Angeles. In the remaining counties, dental services are available through FFS. While the managed care authority for Dental MC will change, no programmatic changes to Dental MC will be requested in the CalAIM 1915(b) waiver.
Like MCMC, Dental MC in Sacramento County is currently authorized under California’s Medi-Cal 2020 1115 demonstration through December 31, 2021. California will seek to shift Dental MC authority to Section 1915(b) and to shift Los Angeles County, which is currently authorized under Section 1915(a), to Section 1915(b).
Populations. Currently, in Sacramento County, Medi-Cal child and adult enrollees receive their dental services through Dental MC. In Los Angeles County, Medi-Cal child and adult enrollees have the option of enrolling in Dental MC or accessing their dental benefits through FFS. Between the two counties, approximately 836,000 members were enrolled in Dental MC plans as of December 2020. In each county, enrollees choose from three plans.
No changes to eligible populations or counties with Dental MC will be requested as part of the 1915(b) waiver.
Benefits. The Medi-Cal dental services covered under Dental MC are the same as the services provided under Medi-Cal’s FFS program. These include dental exams, x-rays,
3 For further information regarding the carve-out of pharmacy benefits in MCMC, please see All Plan Letter 20-020.

8
and teeth cleanings; fillings; tooth extractions; root canal treatments; orthodontics for children who qualify; and complete and partial dentures.
No changes to benefits will be requested as part of the 1915(b) waiver.
Consistent with State legislation, DHCS has authority for the implementation of a dental integration pilot in San Mateo County as a component of the Medi-Cal 2020 1115 demonstration, or successor thereto. Under the pilot program, Medi-Cal beneficiaries in San Mateo County will be required to access their dental services through the Health Plan of San Mateo. Accordingly, California will seek the authority for the new pilot in the consolidated 1915(b) waiver. The anticipated implementation date for the pilot is January 2022.
Specialty Mental Health Services
SMHS are currently provided by 56 county MHPs covering all 58 counties throughout the state, including two joint-county arrangements in Sutter/Yuba and Placer/Sierra. The MHPs are required to provide or arrange for the provision of SMHS to beneficiaries in their counties who meet criteria for services, consistent with beneficiaries’ mental health treatment needs and goals.
The SMHS program is currently authorized under California’s SMHS 1915(b) waiver through March 31, 2021 and has requested CMS to extend the waiver through December 31, 2021. Through the renewal of the 1915(b) waiver, California will seek to consolidate other Medicaid managed care authorities and SMHS. In tandem with the consolidated 1915(b) waiver, California will also make programmatic changes through contract modifications and guidance to the SMHS delivery system to update the criteria for services, improve access to care prior to formal diagnosis, and move from a cost-based to a rate-based reimbursement approach. Populations. Medi-Cal beneficiaries will receive SMHS if they meet specified criteria for services, which differ for adult beneficiaries and for beneficiaries under age 21. Today, MHPs provide SMHS to approximately 615,000 Medi-Cal beneficiaries. Through the consolidated 1915(b) waiver and implementing contracts and guidance, DHCS is updating the SMHS program requirements for both adults and beneficiaries under age 21 to ensure access to appropriate care and to standardize the access to the SMHS delivery system statewide. These changes include streamlining criteria for services for beneficiaries under age 21, including creating criteria for those under age 21 at high risk of developing mental health conditions due to experiencing trauma, such as involvement in child welfare or homelessness.
Additional SMHS changes include a “no wrong door” policy, clarifying that reimbursement is available for assessments and specified treatment before formal diagnosis in nonresidential settings and allowing beneficiaries to access nonduplicative

9
services in Drug Medi-Cal, DMC-ODS, and SMHS delivery systems; clarifying that treatment in the presence of a co-occurring SUD is appropriate and reimbursable when treatment criteria are met; developing standardized screening and transition tools for both adults and for beneficiaries under age 21; and updating assessment and documentation requirements.
See Appendix, Attachment 2 for a description of the behavioral health policy proposals in CalAIM, including updated criteria for access to specialty mental health services for both adults and beneficiaries under age 21. The updated criteria were developed after extensive stakeholder comment.
Benefits. MHPs will continue to provide the following specialty mental health services in the consolidated 1915(b) waiver:
• Crisis Residential Treatment Services • Adult Residential Treatment Services • Crisis Intervention • Crisis Stabilization • Day Rehabilitation • Day Treatment Intensive • Medication Support Services • Psychiatric Health Facility Services • Psychiatric Inpatient Hospital Services • Targeted Case Management • Intensive Care Coordination (for beneficiaries under age 21) • Mental Health Services (including the following service activities: Assessment,
Plan Development, Therapy, Rehabilitation, and Collateral) • Intensive Home-Based Services (including the following service activities:
Assessment, Plan Development, Therapy, Rehabilitation, and Collateral) (for beneficiaries under age 21)
• Therapeutic Behavioral Services (for beneficiaries under age 21) • Therapeutic Foster Care Services (for beneficiaries under age 21)
Consistent with State legislation, DHCS will be establishing peer support specialist services to expand the use of certified peer support specialists. Peer support specialist services are culturally competent services, provided by certified peer support specialists, that promote recovery, engagement, socialization, self-sufficiency, self-advocacy, development of natural supports, and identification of strengths. DHCS will use the Medicaid State Plan to include peer support specialist services as a distinct service type and, as part of the 1915(b) waiver, request authority to make peer support specialist services available at the option of each county under SMHS and DMC-ODS. (DHCS is submitting a similar Section 1115 waiver request for DMC.)

10
Special Programs for Foster Children and Caregivers. As part of the CalAIM 1915(b) waiver, DHCS will also clarify the authority for county mobile response and stabilization teams to provide SMHS services through the Family Urgent Response System (FURS) to current and former foster children and youth and their caregivers. In addition, DHCS will clarify authority for SMHS delivered as part of the Family First Prevention Services Act (FFPSA) requirements for services to children, youth, and families in the child welfare system, including certain FFPSA programs that are limited to counties that opt to provide them.
Drug Medi-Cal Organized Delivery System
Medi-Cal has long provided coverage of certain SUD treatment benefits through its DMC program, which is authorized through California’s Medicaid State Plan and administered by counties. To improve the SUD delivery system and expand services, the State created the DMC-ODS program under its Medi-Cal 2020 1115 demonstration authority to expand access to treatment, standardize service delivery across participating counties, and provide a broader continuum of high-quality, evidenced-based SUD treatment services.
Since the DMC-ODS pilot program began in 2015, California counties have had the option to participate in the program to provide their resident Medi-Cal beneficiaries with a range of evidence-based SUD treatment services in addition to and including those available under the Medi-Cal State Plan. To date, 37 of California’s 58 counties have implemented DMC-ODS, providing access to 96 percent of the total Medi-Cal population across the state. DHCS is actively engaging with prospective new counties to participate in DMC-ODS, with the goal to eventually expand access to comprehensive SUD services for Medi-Cal beneficiaries statewide.
Critical elements of DMC-ODS include:
• Providing a continuum of care modeled after the American Society of Addiction Medicine (ASAM) Criteria for SUD treatment services;
• Increased local control and accountability; • Greater administrative oversight; • Creation of utilization controls to improve care and efficient use of resources; • Evidence-based practices in substance use treatment; and • Increased coordination with other systems of care.
This approach provides beneficiaries with access to the care and system interaction needed to achieve sustainable recovery.
The DMC-ODS program is currently authorized under California’s Medi-Cal 2020 Section 1115 demonstration through December 31, 2021, and DHCS is currently
11
seeking CMS approval of several DMC-ODS program improvements.4 Under CalAIM, DHCS is continuing and strengthening the SUD treatment system, building on the existing DMC-ODS program. To minimize unnecessary reliance on a Section 1115 demonstration, California will seek to shift the managed care authority for DMC-ODS to the consolidated Section 1915(b) waiver; use the Medicaid State Plan to authorize most benefits; and secure waivers of statewideness and comparability in the 1915(b) waiver to offer these services at county option. California will also seek to use Section 1915(b)(3) authority for Contingency Management services. Authority to provide reimbursable Medi-Cal services for DMC-ODS beneficiaries residing in institutions for mental diseases (IMDs) will remain in the 1115 demonstration.
Population. Currently, to receive services through DMC-ODS, a beneficiary must be enrolled in Medi-Cal and reside in a participating county. Additionally, beneficiaries 21 years of age or older must meet criteria for services after completion of their initial assessment, defined as having at least one diagnosis from the current DSM for Substance-Related and Addictive Disorders, with the exception of Tobacco-Related Disorders and Non-Substance-Related Disorders.5 Today, counties provide DMC-ODS services to 90,600 Medi-Cal beneficiaries.
In tandem with the consolidated 1915(b) waiver, DHCS will update the DMC-ODS criteria for services to clarify that individuals leaving incarceration are eligible to receive DMC-ODS services if they had at least one SUD diagnosis prior to being incarcerated or during incarceration. The consolidated 1915(b) waiver will also clarify that DMC-ODS assessment and treatment services are reimbursable prior to diagnosis in nonresidential settings (similar to SMHS).
Beneficiaries under age 21 are currently, and will remain, eligible to receive DMC-ODS services without a diagnosis. Under the Early and Periodic Screening, Diagnostic, and Treatment Services (EPSDT) mandate, beneficiaries under the age of 21 are eligible to 4 DHCS is currently negotiating with CMS the following proposed programmatic changes: (1) remove the limitation on number of residential treatment episodes that can be reimbursed in a one-year period; (2) clarify criteria for treatment (including determination by a licensed provider and treatment post-incarceration) while reimbursing treatment prior to diagnosis in nonresidential settings; (3) clarify the allowable components of recovery services, including when and how beneficiaries, including justice-involved individuals, may access recovery services and the availability of recovery services to individuals receiving medications for addiction treatment (MAT); and (4) require counties to mandate that DMC-ODS providers demonstrate that they either directly offer or have effective referral mechanisms for MAT. 5 The criteria are: (1) have at least one diagnosis from the Diagnostic and Statistical Manual of Mental Disorders (DSM) for Substance-Related and Addictive Disorders, with the exception of Tobacco-Related Disorders and Non-Substance-Related Disorders, OR (2) have had at least one diagnosis from the DSM for Substance-Related and Addictive Disorders, with the exception of Tobacco-Related Disorders and Non-Substance-Related Disorders, prior to being incarcerated or during incarceration, determined by substance use history.

12
receive all appropriate and medically necessary services needed to correct or ameliorate health conditions that are coverable under Section 1905(a) Medicaid authority. Nothing in the DMC-ODS overrides any EPSDT requirements. Counties are responsible for the provision of services pursuant to the EPSDT mandate. Benefits. Currently, DMC-ODS benefits include a comprehensive continuum of inpatient and outpatient, evidence-based SUD treatment services, which are available only to beneficiaries residing in counties participating in DMC-ODS. Standard DMC services approved through the State Plan are available to all beneficiaries in all counties. DMC-ODS benefits include multiple levels of residential SUD treatment, partial hospitalization, withdrawal management, and recovery services.
Under CalAIM, the comprehensive continuum of benefits offered to DMC-ODS beneficiaries will continue and certain new benefits will be added. The State will use the Medicaid State Plan to authorize most benefits, and will secure waivers of statewideness and comparability in the CalAIM 1915(b) waiver to enable the benefits to be available only in counties that opt to implement DMC-ODS.
Consistent with State legislation, the State also is establishing the peer support specialist provider type and peer support services in DMC-ODS, as described above related to SMHS.
DHCS will also request authority to add Contingency Management as a new component of existing DMC-ODS services with authority under 1915(b)(3). Contingency Management is an evidence-based, cost-effective treatment practice for SUDs, which combines motivational incentives with behavioral health treatments, and it is the only currently effective treatment for stimulant use disorders, for which there is no approved medication.
Additional Program Improvements. In tandem with the transition to the 1915(b) waiver, DHCS will move from a Certified Public Expenditures (CPE)- or cost-based methodology to rate-based financing and payment methodologies for county SUD expenditures. Through a combination of Section 1115 demonstration renewal, State Plan changes, contracts, and guidance, DHCS also plans to make additional program improvements, including the following:
• Pending CMS approval via the Section 1115 demonstration renewal, increasing access to SUD treatment and promoting access to culturally appropriate and evidence-based SUD treatment for American Indians and Alaska Natives through Indian Health Care Providers. DHCS seeks expenditure authority for DMC-ODS services provided by traditional healers and natural helpers, using culturally specific practices. DHCS also plans to require Indian Health Care Providers to use at least two evidence-based practices as defined in DMC-ODS and/or from a list developed by DHCS in consultation with Tribal and Urban Indian partners.

13
• Reiterating the counties’ obligation under the EPSDT mandate to provide early intervention services to beneficiaries under the age of 21 at risk of developing an SUD. Any beneficiary under the age of 21 who is screened and determined to be at risk of developing an SUD may receive the following early intervention services: group counseling, individual counseling, and patient education. A diagnosis from the DSM for Substance-Related and Addictive Disorders is not required for early intervention services. Nothing in this section limits or modifies the scope of EPSDT mandate.
• Renaming the physician consultation service to clinician consultation and clarifying who can bill for the service.
See Appendix, Attachment 2 for a description of the behavioral health policy proposals in CalAIM, including those that may not require a federal waiver and Appendix, Attachment 3 for additional DMC-ODS program details and improvements.
Federal Authorities Requested Under the 1915(b) Waiver
The following is a technical summary of the federal waiver authorities that DHCS will be seeking to enable MCMC delivery systems described above. California has been approved for many of these authorities under the existing 1115 demonstration and 1915(b) waiver.
• Section 1915(b)(3) to allow the State to share cost savings from the use of more cost-effective medical care and provide additional services under the waiver (e.g., Contingency Management).
• Section 1915(b)(4) to allow the State to require beneficiaries obtain services only from specified providers who meet reimbursement, quality, and utilization standards that are consistent with access, quality, and efficient and economic provision of covered care and services.
• Section 1902(a)(1) (Statewideness) to allow the State to offer different Medi-Cal delivery systems in different parts of the state and on a geographically limited or county-by-county basis.
• Section 1902(a)(10)(B) (Amount, Duration, and Scope and Comparability) to allow the State to offer additional benefits for SMHS and DMC-ODS enrollees, and not otherwise available to all beneficiaries in the same eligibility groups.
• Section 1902(a)(23) (Freedom of Choice), 1902(a)(4) (Plan Choice), and relevant federal Medicaid managed care regulations to allow the State to direct that beneficiaries receive their benefits through an applicable managed care entity—i.e., MCP, Dental MCP, MHP, DMC-ODS plan in the state available in the county—and restrict the managed care entity to the option that may be available in the county (i.e., single MCP available in COHS counties, single MHP for SMHS, and single Prepaid Inpatient Health Plan (PIHP) for DMC-ODS).
14
• Relevant federal Medicaid managed care regulations to allow the State to provide informing materials and provider lists to beneficiaries when they first access SMHS through the MHP and on request.
• Relevant federal Medicaid managed care regulations to allow external quality review to commence after completion of the first year of DMC-ODS program implementation in a county.
California’s discussions and negotiations with the federal government on the Section 1915(b) waiver, Section 1115 demonstration, and other federal authorities, as well as California’s state legislative and budget process, could lead to refinements in this list as we work to move the CalAIM initiative forward.
Cost Effectiveness and Funding for Additional Services In order to be granted the 1915(b) waiver, the State must demonstrate the waiver is cost-effective. In the renewal application for the consolidated 1915(b) waiver, the State will share spending calculations and projections under the waiver and, ongoing, the State will document and report on actual spending to the federal government. DHCS is currently developing these spending calculations and projections. Given the decades of years of experience delivering Medi-Cal through managed care, including under Section 1115 demonstration authority, DHCS anticipates California will meet cost-effectiveness to secure approval of the consolidated 1915(b) waiver and be able to demonstrate ongoing cost-effectiveness to maintain authorization of the 1915(b) waiver over the five-year waiver period and beyond.
In addition, DHCS is currently conducting analysis on savings generated by the managed care delivery system, which would enable the State to support additional services for Medi-Cal beneficiaries under the waiver. DHCS anticipates proposing Contingency Management for support as a 1915(b)(3) service and is evaluating inclusion of other services. California’s discussions and negotiations with the federal government on the Section 1915(b) waiver, Section 1115 demonstration, and other federal authorities, as well as California’s state legislative and budget process, could lead to refinements in this list as we work to move the CalAIM initiative forward.
Monitoring Approach The State must actively monitor the effect of the 1915(b) waiver on the accessibility and quality of services as well as the anticipated impact on the State’s Medicaid program. CMS prescribes the major focus areas for monitoring, which are:

15
Program Impact Access Quality
• Choice • Marketing • Enrollment/Disenrollment • Information to Beneficiaries • Grievances/Appeals • Program Integrity
• Timely Access • Primary Care
Provider/Specialist Capacity
• Coordination/Continuity of Care
• Coverage/Authorization • Provider Selection • Quality of Care
For each of the MCMC delivery systems encompassed in the 1915(b) waiver, DHCS will document and maintain data, and report results in these focus areas to CMS. Many of the monitoring activities are tied to existing Medicaid managed care requirements, such as network adequacy validation, programmatic reporting, quality strategy implementation, quality assurance and performance improvement program reviews, and annual external reviews conducted by a qualified organization independent from DHCS and Medi-Cal MCPs.
Under CalAIM, DHCS will also move toward requiring that all MCMC MCPs achieve National Committee for Quality Assurance (NCQA) accreditation by 2026. NCQA will also promote consistency and standardization in MCPs and streamline DHCS monitoring and oversight.
Although DHCS is requesting authority for DMC-ODS using both Section 1115 demonstration and 1915(b) waiver authorities (along with corresponding State Plan Amendments for certain DMC-ODS benefits), DHCS anticipates establishing comprehensive, programwide evaluation and monitoring protocols in the CalAIM Section 1115 demonstration Special Terms and Conditions.

16
Appendices Attachment 1: Overview of CalAIM 1915(b) Waiver Programs
Attachment 2: Overview of CalAIM Behavioral Health Policies
Attachment 3: DMC-ODS Program Description

17
Attachment 1: Overview of CalAIM 1915(b) Waiver Programs
The tables below provide an overview of the programs that will be authorized under the consolidated 1915(b) waiver, including transitions from existing 1915(b) waiver or 1115 demonstration authorities, and program modifications and improvements under the CalAIM 1915(b) delivery system. California’s negotiations with the federal government, as well as California’s state legislative and budget process, could lead to refinements.
Program Current Authority
Future Authority
Duration of Future Authority
Requested
Medi-Cal Managed Care (MCMC) • PACE/COHS • CCI (through 2022,
the duration of the duals demonstration)
1115 1915(b) January 1, 2022 – December 31,
2026
Dental Managed Care (Dental MCMC)
1915(a), 1115 1915(b) January 1, 2022 – December 31,
2026 Specialty Mental Health Services (SMHS)
1915(b) 1915(b) January 1, 2022 – December 31,
2026

18
Program Current Authority
Future Authority
Duration of Future Authority
Requested
Drug Medi-Cal Organized Delivery System (DMC-ODS)
1115 DHCS is seeking a renewal of its
expenditure authority
allowing federal reimbursement
for Medicaid services
provided to short-term
residents of IMDs receiving
DMC-ODS services, and
other programmatic changes noted
above.
1915(b) January 1, 2022 – December 31,
2026
Program Modification/Improvement for 1915(b) Delivery
System Effective Date
MCMC – Mandatory Enrollment of Additional Aid Code Groups and Populations • Trafficking and Crime Victims Assistance Program (except
beneficiaries with a share of cost) • Individuals participating in accelerated enrollment • Child Health and Disability Prevention infant deeming • Pregnancy-related Medi-Cal (pregnant women only, 138–
213 percent FPL citizen/lawfully present) • American Indians and Alaska Natives in non-COHS
counties6 • Beneficiaries with other health care coverage in non-COHS
counties • Beneficiaries living in rural zip codes in non-COHS counties
January 1, 2022
6 As is consistent with current policy, all American Indians and Alaska Natives residing in non-COHS counties will continue to have the ability to opt out of MCMC for FFS.

19
Program Modification/Improvement for 1915(b) Delivery System
Effective Date
MCMC – Mandatory Enrollment of Dual Eligibles • All dual and nondual individuals eligible for long-term care
services • All partial and full dual aid code groups, except share of cost
or restricted scope
January 1, 2023
MCMC – FFS Enrollment • Omnibus Budget Reconciliation Act (OBRA) in Napa,
Solano, and Yolo counties • Share of cost beneficiaries in COHS and CCI counties,
excluding long-term care share of cost
January 1, 2022
MCMC – Pharmacy benefit carved out of benefit package TBD MCMC – MSSP carved out in CCI counties, specialty mental health services carved out for Medi-Cal members enrolled in Kaiser in Solano and Sacramento counties
January 1, 2022
MCMC – Major organ transplants included in the benefit package
January 1, 2022
MCMC – Institutional long-term care services included in the benefit package
January 1, 2023
SMHS • Updated criteria for services for adults and beneficiaries
under age 21 • Peer support specialist services • FURS • FFPSA
January 1, 2022
SMHS – Transition from a cost-based to a rate-based reimbursement approach
No sooner than July 1, 2022
DMC-ODS • Updated criteria for services for adults • Peer support specialist services • Contingency Management services • Additional program improvements
January 1, 2022
DMC-ODS – Transition from a cost-based to a rate-based reimbursement approach
No sooner than July 1, 2022
Additional services supported through 1915(b)(3) savings January 1, 2022

20
Attachment 2: Overview of CalAIM Behavioral Health Policies (including concepts that may not be detailed in the proposed 1915(b) waiver)
Please note that these policies are in development and subject to change.
After extensive consultation with stakeholders, as part of CalAIM, DHCS proposes to implement a suite of improvements to the specialty mental health and SUD treatment delivery systems. These policy changes are summarized at a high level below. To accomplish these policies, DHCS will be making changes through a variety of vehicles: 1115 demonstration, 1915(b) waiver, State Plan Amendments, contracts, information notices, etc.
Summary of Policy Changes
Issue to be addressed
What is changing
Brief summary of change (see following pages for details)
SMHS regulations rely on outdated DSM-IV diagnoses and are complex and confusing. Documentation requirements are complex and could be streamlined with payment reform. Research shows that beneficiaries under age 21 are at high risk of developing mental health conditions after experiencing trauma.
Clarify criteria to access the SMHS delivery system, align medical necessity with federal requirements, clarify documentation requirements, and allow treatment during the assessment period, prior to diagnosis
• Update and clarify criteria for beneficiaries to access SMHS, including streamlining access to children at high risk of developing mental health conditions from trauma (such as being in child welfare or experiencing homelessness)
• Align medical necessity with federal definitions
• Streamline and simplify assessment and documentation requirements
• Align audit processes with updated documentation requirements
• Clarify that it is appropriate to provide specified services during assessment period, prior to completing a diagnosis
Beneficiaries request treatment through a variety of avenues that can be challenging to navigate.
No wrong door • Ensure beneficiaries are assessed and provided treatment regardless of the delivery system where they initially request treatment
• Clarify that beneficiaries may receive nonduplicative, coordinated services in multiple delivery systems
Many beneficiaries have co-occurring
Facilitate treatment of
• Clarify that co-occurring substance use may be addressed as part of a beneficiary’s mental health treatment plan

21
Issue to be addressed
What is changing
Brief summary of change (see following pages for details)
mental health and SUD needs.
co-occurring disorders
Beneficiaries experience differing procedures among MHPs and MCPs when they initially seek treatment.
Standardized statewide screening tool
• Develop a standardized screening tool for MHPs and MCPs to use to guide beneficiaries toward the delivery system that is most likely to meet their needs
Beneficiaries experience differing procedures for transitioning between delivery systems.
Standardized statewide transition tool
• Develop a standardized transition tool for MHPs and MCPs to use when a beneficiary’s condition changes and they would be better served in the other delivery system
The DMC-ODS policies required updating, with lessons learned from first five years.
DMC-ODS updates
Proposed changes during waiver extension (2021): • Remove the limitation on number of
residential treatment episodes that can be reimbursed in a one-year period
• Clarify criteria for services (including diagnosis by a licensed provider and treatment post-incarceration) and allow reimbursement for treatment prior to diagnosis in nonresidential settings
• Clarify the allowable components of recovery services, including when and how beneficiaries, including justice-involved individuals, may access recovery services and the availability of recovery services to individuals receiving MAT
• Require counties to mandate that DMC-ODS providers demonstrate that they either directly offer or have effective referral mechanisms for MAT
Proposed changes during waiver renewal (2022-–26): • Allow reimbursement of culturally specific
services by Indian Health Care Providers

22
Issue to be addressed
What is changing
Brief summary of change (see following pages for details)
• Clarify ASAM 0.5 services for beneficiaries under 21 (early intervention)
• Expand physician consultation to other licensed clinicians
• Add Contingency Management services • Technical edits and minor corrections
Many incarcerated individuals have behavioral health conditions and need connection to behavioral health care upon release.
Facilitated referral and linkage from criminal justice to behavioral health; services in 30 days prior to release
Establish a process for facilitated referral and linkage from county correctional institution release to county specialty mental health, Drug Medi-Cal, DMC-ODS, and Medi-Cal MCPs when the inmate was receiving behavioral health services while incarcerated, to allow for continuation of behavioral health treatment in the community. Seek expenditure authority under 1115 to provide selected services prior to release to facilitate safe re-entry and reduce unnecessary use of health care services upon return to community.
Current behavioral health reimbursement does not allow incentivizing outcomes and quality over volume and cost.
Behavioral Health Payment Reform
DHCS proposes to transition counties from a cost-based reimbursement methodology to fee-for-service reimbursement, using CPT codes (also called HCPCS level 1 codes); reimburse CPT codes with standardized rates; and use inter-governmental transfers for local match.
Small counties could optimize resources through regional administration and delivery of specialty mental health and SUD services to Medi-Cal beneficiaries.
Behavioral Health Regional Contracting
DHCS proposes to encourage counties to collaborate to provide services for a multicounty region, pooling resources to contract with an administrative services organization/third-party administrator or other entity, such as the local Medi-Cal MCP or County Medical Services Program, and providing DMC-ODS or DMC services through a regional approach.
Current contractual, payment and oversight structures do not support
Administrative Behavioral Health Integration
DHCS proposes to streamline the administrative functions for SUD and specialty mental health services to allow a single administrative contract

23
Issue to be addressed
What is changing
Brief summary of change (see following pages for details)
integration of mental health and SUD treatment services.
for behavioral health between DHCS and counties in January 2027.

24
Detailed CalAIM Behavioral Health Policy Descriptions
1. Clarify criteria to access the SMHS delivery system, align medical necessity with federal definition, clarify documentation requirements, and allow treatment during the assessment period, prior to diagnosis.
State Criteria for Access to Specialty Mental Health Services: DHCS is clarifying the current division of responsibilities between Medi-Cal Managed Care Plans (MCPs) and SMHS Mental Health Plans (MHPs), including updates to the criteria for access to specialty mental health services, both for adults and for beneficiaries under age 21. These criteria were developed and continually improved based on significant feedback from stakeholders. The goal of these changes is to update outdated criteria and to improve beneficiaries’ access to medically necessary services.
Medi-Cal Managed Care Plan responsibilities:
The following nonspecialty mental health services are covered by Medi-Cal Managed Care Plans:
1. Individual and group mental health evaluation and treatment (including psychotherapy and family therapy);
2. Psychological testing, when clinically indicated to evaluate a mental health condition;
3. Outpatient services for the purposes of monitoring drug therapy; 4. Psychiatric consultation; and, 5. Outpatient laboratory, drugs, supplies, and supplements (Note: the
pharmacy benefit will be carved out of MCP contracts and transitioned to FFS delivery under Medi-Cal Rx at an effective date to be subsequently announced by DHCS).
Medi-Cal Managed Care Plans are responsible to provide the above nonspecialty mental health services to adult beneficiaries with mild to moderate distress or mild to moderate impairment of mental, emotional, or behavioral functioning resulting from mental health disorders, as defined by the current Diagnostic and Statistical Manual of Mental Disorders. Medi-Cal Managed Care Plans are required to provide nonspecialty mental health services to beneficiaries under the age of 21. Medi-Cal Managed Care Plans are also responsible to provide mental health services to beneficiaries with potential mental health disorders not yet diagnosed.
These services are also available in the FFS delivery system for beneficiaries not enrolled in Medi-Cal managed care.
25
County Mental Health Plan responsibilities: For beneficiaries 21 years and over, Mental Health Plans are responsible for providing specialty mental health services for beneficiaries who meet (A) and (B) below:
(A): The beneficiary must have one of the following: (i) Significant impairment (“impairment” is defined as distress,
disability or dysfunction in social, occupational, or other important activities), OR
(ii) A reasonable probability of significant deterioration in an important area of life functioning.
(B): The beneficiary’s condition in (A) is due to: (i) A diagnosed mental health disorder (according to the current
Diagnostic and Statistical Manual of Mental Disorders and International Statistical Classification of Diseases and Related Health Problems criteria), OR
(ii) A suspected mental disorder that has not yet been diagnosed.
For beneficiaries under age 21, Mental Health Plans are responsible for providing specialty mental health services, including services pursuant to the EPSDT mandate, to beneficiaries who meet either Criteria 1 or Criteria 2: Criteria 1: The beneficiary has a condition that puts the child or youth at high risk for a mental health disorder due to experiencing trauma, evidenced by any of the following: scoring in the high-risk range on a DHCS-approved trauma screening tool, or involvement in the child welfare system, or experience of homelessness. Criteria 2: The beneficiary must meet both (A) and (B), below:
(A): The beneficiary must have at least one of the following: I. A significant impairment (as defined above), or
II. A reasonable probability of significant deterioration in an important area of life functioning, or
III. A reasonable probability of not progressing developmentally as appropriate, or
IV. A less than significant impairment, but requires mental health services that are not included within the mental health benefits that managed care plans are required to provide.
(B): The beneficiary’s condition in (A) is due to:

26
I. A diagnosed mental health disorder (according to the current Diagnostic and Statistical Manual of Mental Disorders and International Statistical Classification of Diseases and Related Health Problems criteria), or
II. A suspected mental disorder that has not yet been diagnosed.
Alignment of California’s Medical Necessity Language with Federal Requirements (for adults and for beneficiaries under age 21 in line with EPSDT protections):
DHCS is proposing to provide medically necessary services, as determined by appropriate clinical providers, to beneficiaries for behavioral services needed to prevent, diagnose, or treat an illness, injury, condition, disease, or its symptoms and that meet accepted standards. In any of those circumstances, if your condition produces debilitating symptoms or side effects, then it is also considered medically necessary to treat those.
Additionally, in accordance with the requirements in Section 1905(r) of the Social Security Act and Title 42 Code of Federal Regulations (CFR) Section 441.50 et seq., for individuals under the age of 21, provide necessary preventive, diagnostic services, treatment, and other measures when it is reasonable and necessary to protect life, to prevent significant illness or significant disability, or to alleviate severe pain, including providing necessary services to correct or ameliorate defects and physical and behavioral health conditions.
Assessments: DHCS proposes to standardize the domains that should be part of assessment, in alignment with current clinical practice. The domains that are likely to be required include:
o Presenting Problem/Changes in Functioning/History of Presenting Problem o Mental Health and Substance Use History o Medical History and Current Medications o Social and Cultural Factors o Risk and Safety Factors o Case Conceptualization and Diagnostic Summary
Documentation: DHCS proposes to update documentation requirements and align with national standards, in preparation for behavioral health payment reform. The shift to CPT codes (also called HCPCS level 1 codes) allows conformity with national code standards and aligns with physical health (medical) practices. DHCS proposes to eliminate documentation requirements based on cost-based reimbursement, such as requiring charts to document each minute of care. In addition, DHCS proposes to

27
remove the following requirements: point-in-time treatment plan, and requiring that each chart note tie to the treatment plan. Instead, DHCS proposes to use problem lists to allow active and ongoing updates of a client’s evolving clinical picture, with progress notes reflecting the care given, aligning with the appropriate billing codes. Finally, DHCS proposes to remove the requirement for clients to sign the treatment plan, as evidence does not show that shared decision-making is achieved through signature requirements.
Audit Processes: DHCS also proposes to revise the clinical auditing protocol to align with the revised documentation requirements. DHCS proposes to use disallowances when there is evidence of fraud, waste, and abuse, and to use quality improvement methodologies (such as oversight from the External Quality Review Organization) for minor clinical documentation concerns.
Treatment During Assessment Period: Unlike screening, which is a brief process with nonlicensed staff to determine which delivery system shall best serve the needs of the beneficiary, assessments are done by licensed providers to determine diagnosis and medical necessity for services. Assessments may require more than one visit to complete. Withholding treatment services until an assessment is complete can be counterproductive to client engagement, especially for patients in crisis or in substance withdrawal. Some medically necessary services may be provided prior to the completion of an assessment, including crisis intervention, medication support services, and certain mental health services (e.g., assessment, plan development, psychotherapy, and collateral). During the assessment period, specialty mental health services specified above are reimbursable, even if it is determined that the beneficiary does not have a mental illness after the assessment is complete.
2. No wrong door
DHCS proposes to ensure that beneficiaries receive the care they need, no matter how they enter the system. Due to parity protection, beneficiaries are entitled to self-refer to see a mental health provider, and they may seek care in multiple ways: through access lines, at walk-in clinics, or through an integrated care site (such as a primary care clinic with embedded behavioral health providers).
Self-referral: Callers to MCP or MHP access lines shall be screened by staff with the statewide screening tool and referred to the appropriate delivery system to meet their needs. If a beneficiary sees an individual clinician directly, without going through the MHP or MCP access lines, the clinician is responsible for determining the beneficiary’s mental health needs, which services are medically necessary, and in which delivery system they should occur. The provider shall provide medically necessary treatment in that visit, and then either continue care or facilitate a referral to another provider if the beneficiary’s needs would be best met in the other delivery system (such as facilitating a referral from nonspecialty mental health to specialty mental health).

28
Services in both delivery systems: Beneficiaries may initiate mental health services in one delivery system and receive ongoing services in another system. Beneficiaries whose mental health needs change, after already establishing care and receiving services in one system, may transition between the delivery systems. In some circumstances, beneficiaries may receive mental health services in more than one delivery system, as long as the care is coordinated between the delivery systems and the services are not duplicated.
3. Co-occurring disorders
Patients with co-occurring mental health and substance use disorder conditions may be treated by providers in each of the behavioral health delivery systems, as long as the covered services are not duplicative and are performed within the provider’s scope of practice, the provider is contracted with the appropriate plan, and the services are billed to the appropriate plan, based on the policies and procedures for that plan: MCP, MHP, DMC-ODS, DMC, and/or FFS.
4. Standardized statewide screening tool
To guide a referral to the behavioral health delivery system that best supports beneficiary needs, DHCS proposes to require MHPs and MCPs to use two standardized screening tools. These tools will determine the appropriate delivery system for mental health services for beneficiaries seeking services for the first time (i.e., nonopen cases): one tool for beneficiaries under 21 and one tool for beneficiaries 21 and over. The tool will be selected in collaboration with stakeholders, and will be designed to be administered by nonlicensed staff, such as on MHP or MCP access lines. If the patient has an SUD, the screening tool shall be used to refer to the appropriate SUD treatment system.
5. Standardized statewide transition tool
Beneficiaries receiving services in one delivery system may have a change in condition requiring care in the other system. To ensure that these beneficiaries requiring a transition between the delivery systems (from the MHP to the MCP, or the MCP to the MHP) receive timely and coordinated care, DHCS plans to standardize the process using two statewide standardized transition tools: one for beneficiaries under 21 and one for beneficiaries 21 years and over. The transition tools will be selected in collaboration with stakeholders, and will be designed to facilitate coordination of care between MHP and MCP delivery systems. The transition tools are designed to be used by the treating provider(s). If the patient has an SUD, the transition tool shall be used to refer to the appropriate SUD treatment system.
6. DMC-ODS updates

29
DHCS proposes to update the DMC-ODS program based on experience from the first several years of implementation. Accordingly, DHCS proposes clarifying and/or changing policies to support the goal of improved beneficiary access to care, quality of care, and administrative efficiency. See Attachment 3 for detail.
7. Facilitated referral and linkage from criminal justice to behavioral health (part of Mandatory Medi-Cal Application Process upon Release from Jail and County Juvenile Facilities)
Justice-involved individuals often receive both medical and behavioral health services while incarcerated. Upon their release from jail or county juvenile facilities, proper coordination is needed to ensure the medical and behavioral health needs of an individual continue to be met, and also to ensure critical nonclinical needs such as housing, and overall integration back into the community are met. Studies have shown these types of coordination activities reduce unnecessary emergency room and inpatient stays, as well as improve treatment and medication adherence upon release from jail. To ensure all county inmates receive timely access to Medi-Cal services upon release from incarceration, DHCS proposes that California mandate the county inmate pre-release Medi-Cal application process by January 2023. Additionally, DHCS proposes mandating that jails and county juvenile facilities implement a process for facilitated referral and linkage from county institution release to county specialty mental health, Drug Medi-Cal, DMC-ODS, and Medi-Cal MCPs when the inmate was receiving behavioral health services while incarcerated, to allow for continuation of behavioral health treatment in the community.
8. Behavioral Health Payment Reform
DHCS proposes to transition counties from a cost-based reimbursement methodology to fee-for-service reimbursement, using CPT codes (also called HCPCS level 1 codes), reimbursing for CPT codes through standardized rates, and using inter-governmental transfers for local match. See the published CalAIM proposal for details, pp. 77–82.
9. Behavioral Health Regional Contracting
Small counties could optimize resources through regional administration and delivery of specialty mental health and SUD services to Medi-Cal beneficiaries. There are a variety of options available to counties, including a Joint Powers Authority to provide services for a multicounty region (e.g., Sutter/Yuba). Counties could also pool resources to contract with an administrative services organization/third-party administrator or other entity, such as the local Medi-Cal MCP or County Medical Services Program, to create administrative efficiencies across multiple counties. Small counties, rural/frontier counties, and counties with shared population centers or complementary resources should consider opportunities for regional partnership. Furthermore, DHCS encourages counties to join DMC-ODS or provide DMC services through a regional approach.

30
DHCS is committed to working with counties to offer technical assistance to help develop regional contracts and establish innovative partnerships.
10. Administrative Behavioral Health Integration
Approximately half of individuals with a SMI have co-occurring substance use, and those individuals would benefit from integrated treatment. The State covers Medi-Cal SUD and specialty mental health services through separate county contracts, which makes it difficult for counties and contracted providers to offer integrated treatment to individuals with co-occurring disorders. For example, counties are subject to two separate annual quality assessments, two separate post-payment chart audits, and two separate reimbursement and cost reporting methods. DHCS proposes to align administrative functions for specialty mental health services and SUD treatment services through a single county contract in January 2027, as part of the next waiver renewal. Throughout the CalAIM waiver renewal period, 2022 through 2026, DHCS plans to work collaboratively with counties to build the foundation for integration, including implementation of the above-listed behavioral health policy and payment reform proposals, to ensure readiness for a single contract. A single contract would require an integrated beneficiary access line; integrated screening, assessment, and referral processes; and integrated beneficiary informing materials, aiming to encourage integration of clinical services, where feasible. A single contract would also streamline administration and oversight, including a single quality improvement program and cultural competence plan (including a single External Quality Review Organization contract), streamlined compliance reviews, audits and oversight, and an integrated network adequacy plan.

31
Attachment 3: DMC-ODS Program Description
This attachment provides a comprehensive description of the DMC-ODS program, which DHCS intends to include as an attachment to its 1915(b) waiver. The DMC-ODS Program Description retains the key elements of the Special Terms & Conditions (STCs) that govern DMC-ODS under the Medi-Cal 2020 1115 demonstration and incorporates the DMC-ODS program improvements outlined in CalAIM and described in the body of this document. The Program Description provides details on DMC-ODS’s county-based delivery system; criteria for services for adults and children; assessment processes to determine medical necessity of services and level of care; covered DMC-ODS benefits; service descriptions, including ASAM level of care and provider type for covered benefits; DMC-ODS provider specifications; DMC-ODS county responsibilities (for counties that participate); and treatment practice requirements. The document also provides details on DMC-ODS implementation planning development and federal approval process; DMC-ODS county oversight, reporting, and monitoring; DMC-ODS financing; and other program details that will govern operation of the program going forward.
The key changes from the 1115 demonstration are proposed as follows:
• Remove two-stay annual limit for residential treatment* • Clarify criteria for services (including determination by licensed provider,
treatment prior to diagnosis, and treatment post-incarceration)* • Expand access to medications for addiction treatment (MAT)* • Expand access to recovery services* • Expand access to Tribal services and natural healers • Add Contingency Management services • Clarify early intervention for beneficiaries under age 21 (ASAM 0.5 services) • Implement various technical updates
*Proposed during demonstration extension period, January – December 2021
Please note that negotiations with the federal government on the Section 1915(b) waiver, Section 1115 demonstration, and other federal authorities, as well as California’s state legislative and budget process, could lead to refinements.
I. Drug Medi-Cal Organized Delivery System – Program Description
A. [Proposed as Attachment (XX) to the 1915(b) Waiver]

32
Drug Medi-Cal Eligibility and Delivery System
The “Drug Medi-Cal Organized Delivery System (DMC-ODS)” is a program for the organized delivery of substance use disorder (SUD) services for Medicaid eligible individuals with SUD. Critical elements of DMC-ODS include providing a continuum of care modeled after the American Society of Addiction Medicine (ASAM) Criteria for SUD treatment services, increased local control and accountability, greater administrative oversight, creation of utilization controls to improve care and efficient use of resources, evidence-based practices in substance use treatment, and increased coordination with other systems of care. This approach provides beneficiaries with access to the care and system interaction needed to achieve sustainable recovery.
Since the DMC-ODS pilot program began in 2015, California counties have had the option to participate in the program to provide their resident Medi-Cal beneficiaries with a range of evidence-based SUD treatment services in addition to and including those not available under the Medi-Cal State Plan. Any county that elects to opt in to the DMC-ODS (hereinafter referred to as “DMC-ODS County”) that does not already have a DHCS-approved implementation plan must submit an implementation plan to the State for approval. Upon DHCS approval, the State will enter into an intergovernmental agreement with the DMC-ODS County to provide, or arrange for, DMC-ODS services through a Prepaid Inpatient Health Plan (PIHP) as defined in 42 CFR 438.2. DMC-ODS services are made available as Medi-Cal benefits for individuals who meet the criteria for services and reside in a DMC-ODS County that opts in to the program. The DMC-ODS County will, in turn, contract with DMC-certified providers or offer DMC-ODS County-operated services to provide all services outlined in the DMC-ODS County’s DMC-ODS Intergovernmental Agreement. DMC-ODS Counties may also contract with an MCP to provide services. DMC-ODS Counties with approval from the State may develop regional delivery systems for one or more of the required modalities or request flexibility in delivery system design. DMC-ODS Counties may act jointly to deliver these services, upon DHCS approval.
EPSDT
In accordance with the Early Periodic Screening, Diagnostic and Treatment (EPSDT) mandate under Section 1905(r) of the Social Security Act, DMC-ODS Counties shall ensure that all beneficiaries under age 21 receive all applicable services needed to correct or ameliorate health conditions that are coverable under Section 1905(a) of the Social Security Act. Nothing in the DMC-ODS limits or modifies the scope of the EPSDT mandate, and a participating DMC-ODS County is responsible for the provision of services pursuant to the EPSDT mandate.
Indian Health Care Providers
American Indian and Alaska Native individuals who are eligible for Medicaid and reside in counties that have opted in to the DMC-ODS can also receive DMC-ODS services

33
through Indian Health Care Providers (IHCPs). IHCP means a health care program operated by the Indian Health Service (IHS) or by an Indian Tribe, Tribal Organization, or Urban Indian Organization as those terms are defined in Section 4 of the Indian Health Care Improvement Act (25 U.S.C. 1603). IHCPs must also have Drug Medi-Cal certification in order to provide services under the DMC-ODS waiver program. As required by 42 CFR 438.14, DMC-ODS Counties must demonstrate that there are sufficient IHCPs participating in the provider network to ensure timely access to DMC-ODS services available. DMC-ODS Counties must adhere to all 42 CFR 438.14 requirements.
IHCPs are required to utilize at least two evidence-based practices or two practices from a culturally responsive list developed by DHCS in consultation with Tribal representatives. In addition to the providers and services that can be provided by all other DMC-ODS providers, IHCPs may additionally utilize Natural Helpers and Traditional Healers to provide allowable services.
DHCS and American Indian/Alaska Native partners continue to explore the development of a Tribal Delivery System. Any Tribal Delivery System developed shall be outlined in an Attachment to this waiver following approval. The provisions in the Attachment shall be consistent with the authorities in the Indian Health Care Improvement Act (including the statutory exemption from state or local licensure or recognition requirements at Section 1621(t) of the Indian Health Care Improvement Act) and shall be developed in consultation with the California tribes, and Tribal and Urban Indian health programs located in the state, consistent with the Tribal Consultation StatePlan Amendment (SPA) and the
CMS Tribal Consultation Policy.
DMC-ODS Program Criteria for Services To receive services through the DMC-ODS, the beneficiary must be enrolled in Medi-Cal, reside in a participating county, and meet the following criteria:
1. Initial Assessment and Treatment Services: DMC-ODS services are reimbursable for up to 30 days following the first visit with a Licensed Practitioner of the Healing Arts (LPHA) or registered/certified counselor, whether or not a DSM diagnosis for Substance-Related and Addictive Disorders is established, or up to 60 days if a provider documents that the client is experiencing homelessness and therefore requires additional time to complete the assessment. If a client withdraws from treatment prior to establishing a DSM diagnosis for Substance-Related and Addictive Disorders and later returns, the 30-day time period starts over.
2. Services After Assessment: a. Beneficiaries 21 years and older: to qualify for DMC-ODS outpatient
services after the initial assessment or residential treatment, beneficiaries 21 years of age and older must meet one of the following criteria:

34
i. Have at least one diagnosis from the Diagnostic and Statistical Manual of Mental Disorders (DSM) for Substance-Related and Addictive Disorders, with the exception of Tobacco-Related Disorders and Non-Substance-Related Disorders, OR
ii. Have had at least one diagnosis from the DSM for Substance-Related and Addictive Disorders, with the exception of Tobacco-Related Disorders and Non-Substance-Related Disorders, prior to being incarcerated or during incarceration, determined by substance use history.
b. Beneficiaries under the age of 21: to qualify for DMC-ODS services after
the initial assessment, beneficiaries under the age of 21 are eligible to receive Medicaid services pursuant to the EPSDT mandate. Under the EPSDT mandate, beneficiaries under the age of 21 are eligible to receive all appropriate services needed to correct or ameliorate health conditions that are coverable under Section 1905(a) Medicaid authority. Nothing in the DMC-ODS overrides any EPSDT requirements. Counties are responsible for the provision of medically necessary DMC-ODS services pursuant to the EPSDT mandate. Beneficiaries under age 21 are eligible for DMC-ODS services without a diagnosis from the DSM for Substance-Related and Addictive Disorders.
c. Beneficiaries of any age: the SUD diagnosis shall be determined by an assessment of the client. The DMC-ODS initial assessment shall be performed either face-to-face or via synchronous telehealth (“synchronous telehealth” throughout this document is defined as live video) by an LPHA or registered or certified counselor and may be done in the community or the home. If the assessment of the client is completed by a registered or certified counselor, then the LPHA shall evaluate that assessment with the counselor and the LPHA shall make the initial diagnosis. The consultation between the LPHA and the registered or certified counselor can be conducted in person, by synchronous video, or by telephone/audio only.
3. Level of Care: The ASAM Criteria assessment shall be used for all beneficiaries
to determine placement into the appropriate level of care. a. For beneficiaries 21 and over, the ASAM Criteria assessment shall be
completed within 30 days of the client’s first visit with an LPHA or registered/certified counselor.
b. For beneficiaries under 21, the ASAM Criteria assessment shall be completed within 60 days of the client’s first visit with an LPHA or registered/certified counselor.
c. If a client withdraws from treatment prior to completing the ASAM Criteria assessment and later returns, the time period starts over.

35
d. A full ASAM Criteria assessment shall not be required to begin receiving DMC-ODS services.
e. The ASAM Criteria assessment does not need to be repeated unless the client’s condition changes.
DMC-ODS Benefits
Currently, standard DMC services approved through the State Plan are available to all beneficiaries in all counties.7 DMC-ODS services are available only to beneficiaries residing in counties participating in the DMC-ODS. Within DMC-ODS counties, most services are required and must be provided as a condition of participating in the DMC-ODS initiative. However, for a few select DMC-ODS services (e.g., partial hospitalization) and/or provider types authorized to offer a service, they are provided at county option.
Table 1 – DMC-ODS Benefits Under CalAIM8
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority 0.5 Screening,
brief intervention, referral to treatment (SBIRT) and Early Intervention services
SBIRT by primary care providers is a service in FFS and managed care. SBIRT by DMC-ODS providers represent components of assessment and treatment services in DMC-ODS. Early intervention services include
FFS and managed care primary care providers DMC and DMC-ODS providers
Medicaid State Plan
Fee-for-service, 1915(b)
7 One exception is that DHCS intends for peer support services to be available in any county that elects to offer them, regardless of whether it is a DMC or a DMC-ODS county. DHCS currently is in the midst of adding peer support services to the State Plan, as well as pursuing 1915(b)(3) (for DMC-ODS counties) and 1115 waiver authority (for DMC counties) to make them available only at county option. 8 This table reflects the proposed state of DMC-ODS benefits, much of which is simply a continuation of existing policy. In some instances, however, as described in the body of this paper, DHCS is working with CMS to secure appropriate authority for adding selected services.
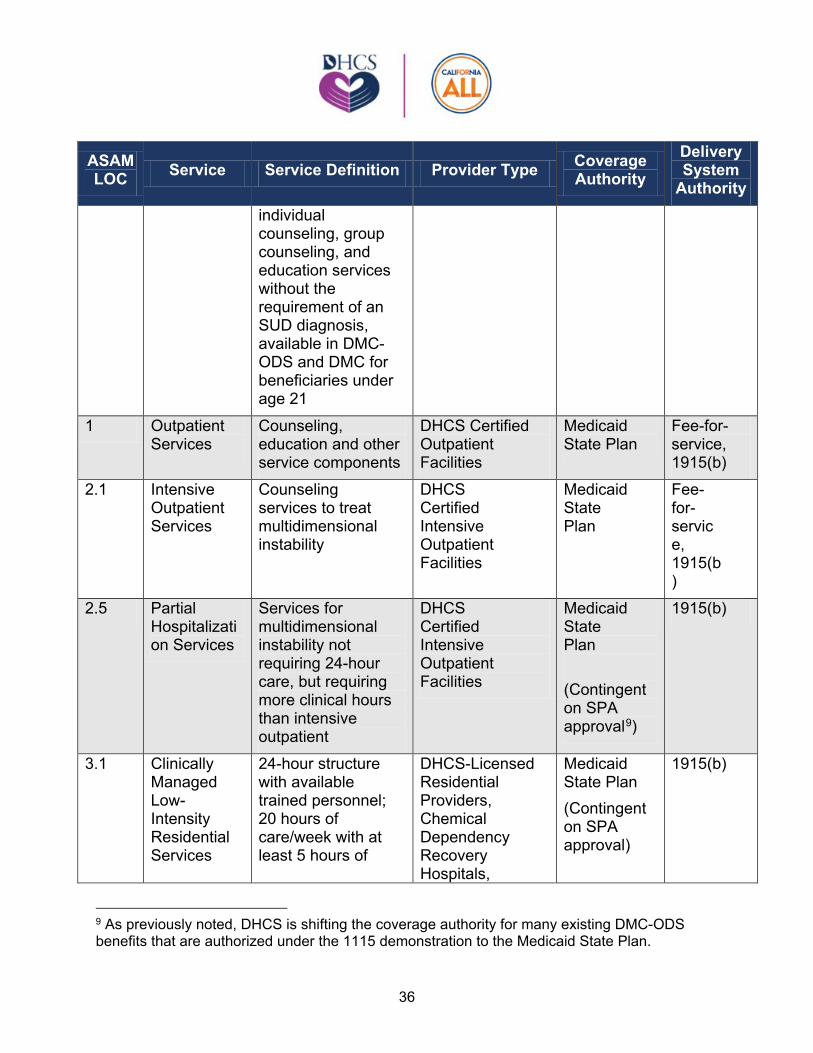
36
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority individual counseling, group counseling, and education services without the requirement of an SUD diagnosis, available in DMC-ODS and DMC for beneficiaries under age 21
1 Outpatient Services
Counseling, education and other service components
DHCS Certified Outpatient Facilities
Medicaid State Plan
Fee-for-service, 1915(b)
2.1 Intensive Outpatient Services
Counseling services to treat multidimensional instability
DHCS Certified Intensive Outpatient Facilities
Medicaid State Plan
Fee-for-service, 1915(b)
2.5 Partial Hospitalization Services
Services for multidimensional instability not requiring 24-hour care, but requiring more clinical hours than intensive outpatient
DHCS Certified Intensive Outpatient Facilities
Medicaid State Plan
(Contingent on SPA approval9
)
1915(b)
3.1 Clinically Managed Low-Intensity Residential Services
24-hour structure with available trained personnel; 20 hours of care/week with at least 5 hours of
DHCS-Licensed Residential Providers, Chemical Dependency Recovery Hospitals,
Medicaid State Plan (Contingent on SPA approval)
1915(b)
9 As previously noted, DHCS is shifting the coverage authority for many existing DMC-ODS benefits that are authorized under the 1115 demonstration to the Medicaid State Plan.

37
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority clinical services/week
Freestanding Acute Psychiatric Hospitals
3.3 Clinically Managed Population-Specific High-Intensity Residential Services
24-hour care with trained counselors to stabilize multidimensional imminent danger. Less intense milieu and group treatment for those with cognitive impairments.
DHCS-Licensed Residential Providers, Chemical Dependency Recovery Hospitals, Freestanding Acute Psychiatric Hospitals
Medicaid State Plan (Contingent on SPA approval)
1915(b)
3.5 Clinically Managed High-Intensity Residential Services
24-hour care with trained counselors to stabilize multidimensional imminent danger
DHCS-Licensed Residential Providers, Chemical Dependency Recovery Hospitals, Freestanding Acute Psychiatric Hospitals
Medicaid State Plan (Contingent on SPA approval)
1915(b)
3.7 Medically Monitored Intensive Inpatient Services
24-hour nursing care with physician availability and 16 hour/day counselor availability
Chemical Dependency Recovery Hospitals; Hospital, Freestanding Acute Psychiatric Hospitals
Medicaid State Plan
Fee-for-service, 1915(b)
4 Medically Managed Intensive Inpatient Services
24-hour nursing care and daily physician care for severe, unstable problems, including
Chemical Dependency Recovery Hospitals, Hospital;
Medicaid State Plan
Fee-for-service, 1915(b)

38
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority counseling services Freestanding
Acute Psychiatric Hospitals
NTP Narcotic Treatment Program
Medications and counseling for opioid and alcohol use disorders
DHCS-Licensed Narcotic Treatment Programs
Medicaid State Plan
Fee-for-service, 1915(b)
1-WM Ambulatory withdrawal management without extended on-site monitoring
Management of mild withdrawal with daily or less than daily outpatient supervision
DHCS Certified Outpatient Facility with Detox Certification; Physician, Licensed Prescriber; or NTP for Opioids
Medicaid State Plan (Contingent on SPA approval)
1915(b)
2-WM Ambulatory withdrawal management with extended on-site monitoring
Management of moderate withdrawal with daytime withdrawal management and support and supervision (not residential)
DHCS Certified Outpatient Facility with Detox Certification; Physician; Licensed Prescriber; or NTP
Medicaid State Plan (Contingent on SPA approval)
1915(b)
3.2-WM
Clinically managed residential withdrawal management
24-hour support for moderate withdrawal symptoms not manageable in outpatient setting
DHCS Licensed Residential Facility with Detox Services; Chemical Dependency Recovery Hospitals; Freestanding Acute Psychiatric Hospitals; Physician; or Licensed
Medicaid State Plan (Contingent on SPA approval)
1915(b)

39
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority Prescriber.
3.7-WM
Medically Managed Inpatient Withdrawal Management
24-hour care for severe withdrawal symptoms requiring 24-hour nursing care and physician visits
General Acute Care Hospital; Chemical Dependency Recovery Hospitals; Freestanding Acute Psychiatric Hospitals
Medicaid State Plan
Fee-for-service, 1915(b)
4-WM Medically managed intensive inpatient withdrawal management
Management of severe, unstable withdrawal requiring 24-hour nursing care and daily physician visits to modify withdrawal management regimen and manage medical instability
General Acute Care Hospital, Chemical Dependency Recovery Hospitals; Freestanding Acute Psychiatric Hospitals
Medicaid State Plan
Fee-for-service, 1915(b)
1-4 1-WM – 4-WM
Clinician Consultation
Consultation services to assist DMC clinicians with seeking expert advice for treating DMC-ODS beneficiaries
DHCS-Certified LPHAs consulting with Addiction Medicine Physicians, Addiction Psychiatrists, or Clinical Pharmacists
Medicaid State Plan
1915(b)
1-4 1-WM – 4-WM
Case Management (component of existing services; can be provided
Coordination of SUD care, including assisting the beneficiary to access needed
DHCS-Certified Providers
Medicaid State Plan (Contingent on SPA approval)
1915(b)
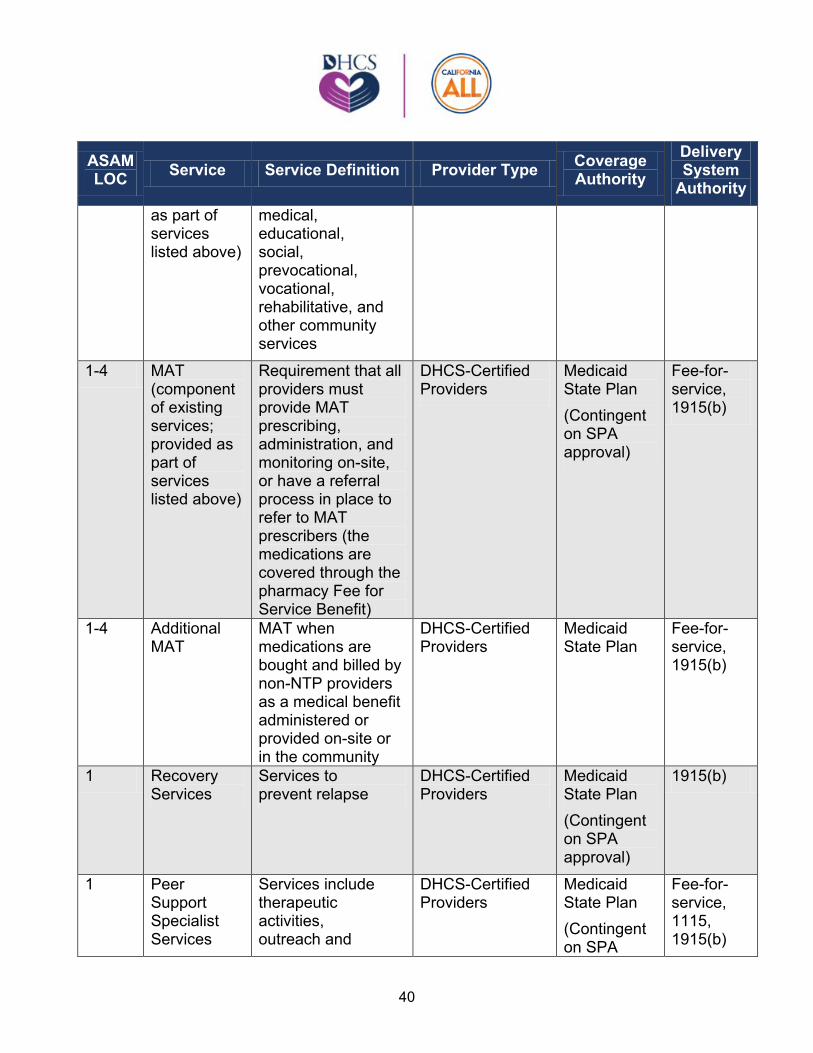
40
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority as part of services listed above)
medical, educational, social, prevocational, vocational, rehabilitative, and other community services
1-4 MAT (component of existing services; provided as part of services listed above)
Requirement that all providers must provide MAT prescribing, administration, and monitoring on-site, or have a referral process in place to refer to MAT prescribers (the medications are covered through the pharmacy Fee for Service Benefit)
DHCS-Certified Providers
Medicaid State Plan (Contingent on SPA approval)
Fee-for-service, 1915(b)
1-4 Additional MAT
MAT when medications are bought and billed by non-NTP providers as a medical benefit administered or provided on-site or in the community
DHCS-Certified Providers
Medicaid State Plan
Fee-for-service, 1915(b)
1 Recovery Services
Services to prevent relapse
DHCS-Certified Providers
Medicaid State Plan (Contingent on SPA approval)
1915(b)
1 Peer Support Specialist Services
Services include therapeutic activities, outreach and
DHCS-Certified Providers
Medicaid State Plan (Contingent on SPA
Fee-for-service, 1115, 1915(b)

41
ASAM LOC Service Service Definition Provider Type Coverage
Authority Delivery System
Authority engagement, and educational groups
approval)
1-2.5 Contingency Management (provided as component of outpatient services)
Motivational incentives combined with counseling
DHCS-Certified providers (the incentives may be delivered through an independent third-party application, to be determined)
1915(b)(3)
1915(b)

42
Table 2 – Required and Optional Services for Participating DMC-ODS Counties Service Required Optional
SBIRT and Early Intervention for under 21
X
Outpatient X Intensive Outpatient X Partial Hospitalization X Residential Treatment X
(At least one ASAM level of service initially; All ASAM levels (3.1, 3.3, 3.5) within three years. Coordination with ASAM Levels 3.7 and
4.0)
X (ASAM levels 3.7 and 4.0)
NTP X Withdrawal Management X
(At least one level) X
(Additional levels) Clinician Consultation X Case Management XMAT X
X
Additional MAT X Recovery Services X Peer Services X Contingency Management X
Screening, Assessment, Brief Intervention, Referral to Treatment and Early Intervention (ASAM Level 0.5)
Screening, brief assessment, brief intervention, and referral to treatment (commonly known as SBIRT) provided by primary care providers is a benefit in the fee-for-service and managed care delivery system for beneficiaries of all ages. These services include screening for alcohol and other drug use, performing brief assessments to confirm the diagnoses, providing brief interventions (such as motivational interviewing or education), and referring to ongoing treatment. SBIRT also represents components of assessment and treatment services when done by DMC-ODS providers.

43
DHCS is reiterating the counties’ obligation under the EPSDT mandate to provide early intervention services to beneficiaries under the age of 21 at risk of developing an SUD. Any beneficiary under the age of 21 who is screened and determined to be at risk of developing an SUD may receive the following early intervention services: group counseling, individual counseling, and educational services. A diagnosis from the DSM for Substance-Related and Addictive Disorders is not required for early intervention services. Completion of the ASAM Criteria assessment is not required to access early intervention services; however, the provider must document the justification for the early intervention services in the beneficiary’s treatment plan. Nothing in this section limits or modifies the scope of the EPSDT mandate.
Early intervention services may be delivered in a wide variety of settings. The initial screening shall be performed in person or by synchronous telehealth. All other early intervention services can be provided in person, by synchronous telehealth, or by telephone (audio-only).
Outpatient Services (ASAM Level 1)
All services provided in the Outpatient Service modality can be provided in person, by synchronous telehealth, or by telephone (audio-only). However, the initial assessment and diagnosis must be conducted in person or by synchronous telehealth. The service components of the Outpatient Services modality include the “Outpatient Drug Free Treatment Services” outlined in the State Plan, and providers are required to either offer medications for addiction treatment (MAT) directly, or have MAT referral processes in place.
In addition to the service components defined in the State Plan, the Outpatient Services modality also includes the following service:
• Family Therapy: The effects of addiction are far-reaching, and the client’s family members and loved ones also are affected by the disorder. By including family members in the treatment process, education about factors that are important to the client’s recovery as well as their own recovery can be conveyed. Family members can provide social support to the client, help motivate their loved one to remain in treatment, and receive help and support for their own family recovery as well.
• Medications for Addiction Treatment (MAT): MAT is the use of medications to treat SUDs, often combined with counseling. MAT is a required service in DMC-ODS for all counties, and all contracted SUD treatment providers must have processes in place to either provide or refer to MAT services (both medication management and counseling) for beneficiaries with diagnoses that are treatable with medications. Licensed prescribers in DMC-ODS programs will be reimbursed for the ordering, prescribing, administering, and monitoring of

44
medications and biologicals utilized to treat SUDs. The medications themselves are available through the Pharmacy benefit.
• Contingency Management (CM): CM uses motivational incentives in combination with behavioral services to treat stimulant use disorders. CM uses positive reinforcement to change behavior by intermittently and randomly rewarding desirable behaviors, such as adherence to program rules, abstinence documented by negative urine drug screens, attendance at counseling, or other positive behaviors. CM is currently the only effective treatment for stimulant use disorder, which has no approved medication treatment.
Providers offering CM must adhere to the following requirements: o The motivational incentives shall be provided in the form of noncash
rewards, such as virtual gift cards managed through an app, with a maximum cumulative allowable amount per beneficiary of $599 per calendar year.
o CM shall be provided in conjunction with counseling or cognitive behavioral therapy in outpatient settings.
o DHCS shall require the motivational incentives to be delivered to the beneficiary independently from the provider through a DHCS-approved mobile or computer application. The mobile or computer application shall have strict safeguards against fraud and abuse, comply with all state and federal privacy statutes and regulations, and integrate periodic questionnaires with patient-reported outcomes to support the evaluation of CM.
o Motivational incentives shall not be utilized to induce an individual into entering treatment.
o Motivational incentives shall only be provided to a beneficiaries after an LPHA determines the diagnosis of stimulant use disorder for this service and that Contingency Management is medically necessary after the ASAM assessment is complete.
Intensive Outpatient Treatment (ASAM Level 2.1)
All services provided in the Intensive Outpatient Treatment modality can be provided in person, by synchronous telehealth, or by telephone (audio-only). However, the initial assessment and diagnosis must be conducted in person or by synchronous telehealth. The service components of Intensive Outpatient Treatment include the Intensive Outpatient Treatment services outlined in the State Plan, and providers are required to either offer MAT directly or have MAT referral processes in place. In addition to the Intensive Outpatient Treatment Services defined in the State Plan, the Intensive Outpatient Treatment modality also includes the following service components:

45
• Family Therapy • MAT • Contingency Management
Partial Hospitalization (ASAM Level 2.5)
Partial Hospitalization services are clinically intensive programming designed to address the treatment needs of beneficiaries with severe SUD requiring more intensive treatment services than can be provided at lower levels of care. Services may be provided in person, by synchronous telehealth, or by telephone (audio-only). However, the initial assessment and diagnosis must be conducted in-person or by synchronous telehealth.
Level 2.5 partial hospitalization programs typically have direct access to psychiatric, medical, and laboratory services, and are to meet the identified needs that warrant daily monitoring or management, but that can be appropriately addressed in a structured outpatient setting. Providing this level of service is optional for DMC-ODS Counties. Contingency Management may be provided as a component of this service. Providers must offer MAT directly or have referral mechanisms for MAT in place.
Residential Treatment (ASAM Level 3.1, 3.3, 3.5, 3.7, and 4.0)
Residential Treatment is a noninstitutional, short-term residential program that provides rehabilitation services. All Residential Treatment services provided to a client while in a Residential Treatment facility can be provided in person, by synchronous telehealth, or telephone (audio-only). However, the initial assessment and diagnosis must be conducted in person or by synchronous telehealth. A client receiving residential services pursuant to DMC-ODS, regardless of the length of stay, is a “short-term resident” of the residential facility in which they are receiving the services. These services are intended to be individualized to treat the functional deficits identified in the ASAM Criteria. Each client shall live on the premises and shall be supported in their efforts to restore, maintain, and apply interpersonal and independent living skills and access community support systems.
Residential Treatment services for adults are provided in DHCS-licensed residential facilities designated by DHCS as capable of delivering care consistent with ASAM treatment criteria. All licensed facilities must have at least one DHCS Level of Care Certification and/or at least one residential ASAM designation Level of Care Certification. All facilities must have a DMC certification. For adolescents, services can be provided in DHCS-licensed residential facilities with an adolescent waiver or in a Department of Social Services licensed facility. Residential (3.7 and 4.0) and withdrawal management services (Levels 3.7-WM and 4.0-WM) may be provided by DMC-ODS Counties and funded through the DMC-ODS waiver in Chemical Dependency Hospitals and/or Acute Free Standing Psychiatric Hospitals. Residential Treatment services within

46
Levels 3.1–4.0 may include facilities that hold a current, valid license from the Department of Public Health or Department of Social Services.
Residential Treatment services can be provided in facilities of any size. The statewide goal for the average length of stay for residential treatment services provided by participating counties is 30 days or less. In furtherance of that goal, DMC-ODS Counties shall adhere to the length of stay monitoring requirements set forth by DHCS and length of stay performance measures established by the external quality review organization. One DHCS ASAM Designation or DHCS Level of Care Designation of Residential Treatment Services is required for approval of a DMC-ODS County implementation plan in the first year of participation in DMC-ODS. The DMC-ODS County must demonstrate all DHCS Level of Care Designations of Residential Treatment Services (Levels 3.1–3.5) within three years of execution of the state-DMC-ODS County Intergovernmental Agreement (managed care contract per federal definition). The DMC-ODS County implementation plan further must describe coordination for ASAM Levels 3.7 and 4.0.
The service components of Residential Treatment services are: • Treatment Services – Services provided to a client to assist the client with the
achievement of self-identified goals including abstinence from the use of alcohol or drugs, achievement of long-term recovery, or achievement of any goal or objective determined by the client or the program to address the client’s SUD. Treatment services include the following: assessment, counseling services, individual counseling sessions, group counseling sessions, educational sessions, prescribing and/or administration of medications for addiction treatment, medication management, and development of a treatment plan.
• Structured Therapeutic Activities – Organized program activities that are designed to meet treatment goals and objectives for increased social responsibility, self-motivation, and integration into the larger community. Such activities would include participation in the social structure of the residential program. It also includes helping the client progress toward increasing levels of responsibility and independence.
• Incidental Medical Services (IMS) – Services including obtaining medical histories, monitoring health status, testing associated with detoxification from alcohol or drugs, overseeing patient self-administered medications, and treating SUDs, including detoxification, if provided at a residential treatment facility licensed by DHCS to provide IMS.
• Medication Services – The prescription or administration related to SUD treatment services, or the assessment of the side effects or results of that medication, conducted by staff lawfully authorized to provide such services within their scope of practice or license.
o Only if the residential facility is licensed by DHCS to provide IMS in accordance with Cal. Health & Safety Code Section 11834.026.

47
o If the residential facility is not licensed by DHCS to provide IMS, then the residential facility shall arrange for the provision of these services when medically necessary.
• Medications for Addiction Treatment o Only if the residential facility is licensed by DHCS to provide IMS in
accordance with Cal. Health & Safety Code Section 11834.026. o If the residential facility is not licensed by DHCS to provide IMS, then the
residential facility shall have a process in place for referral to providers offering MAT.
In addition to the above services, the Residential Treatment Services modality includes the “Perinatal Residential Substance Use Disorder Services” outlined in the State Plan.
Narcotic Treatment Program (ASAM NTP Level 1)
Narcotic Treatment Program (NTP) services are provided in DHCS-licensed NTP facilities pursuant to the California Code of Regulations, Title 9, Chapter 4, Division 4, and title 42 of the CFR. NTPs are required to administer and monitor medications to beneficiaries covered under the DMC-ODS formulary, including methadone, buprenorphine, naltrexone, naloxone, and disulfiram, any other FDA-approved medications, and any other FDA-licensed biologicals for opioid use and alcohol use disorders. The Service Components of NTP include the “Narcotic Treatment Program” services outlined in the State Plan. Counseling services provided in the NTP modality can be provided in person, by synchronous telehealth, or by telephone (audio-only). However, the medical evaluation (which consists of a medical history, laboratory tests, and a physical exam) must be conducted in person. Contingency Management may be provided as a component of this service, for clients who have stimulant use disorder in addition to the opioid use disorder treated by the NTP.
Withdrawal Management (Levels 1, 2, 3.2, 3.7, and 4 in ASAM)
Withdrawal Management (WM) services are provided in a continuum of WM services as per the five levels of WM in the ASAM Criteria. Each client shall reside at the facility, if receiving a residential service, and will be monitored during the detoxification process.
The service components of WM services are:
• Intake – The process of admitting a client into a SUD treatment program. Intake may or may not include the evaluation or analysis of SUD; the diagnosis of SUD; and the assessment of treatment needs to provide medically necessary services. Intake may include a physical examination and laboratory testing necessary for SUD treatment.

48
• Observation – The process of monitoring the client’s course of withdrawal. To be conducted as frequently as deemed appropriate for the client and the level of care the client is receiving. This may include but is not limited to observation of the client’s health status.
• Medication Services – The prescription or administration related to SUD treatment services, or the assessment of the side effects or results of that medication, conducted by staff lawfully authorized to provide such services within their scope of practice or license.
• Medications for Addiction Treatment • Discharge Services – The process to prepare the client for referral into another
level of care, post-treatment return or re=entry into the community, and/or the linkage of the individual to essential community treatment, housing, and human services.
DMC-ODS must provide at least one level of withdrawal management services.
Clinician Consultation Services
Clinician Consultation Services include DMC clinicians consulting with addiction medicine physicians, clinicians, addiction psychiatrists, or clinical pharmacists. Clinician Consultation Services are not with DMC-ODS beneficiaries; rather, they are consultations between clinicians, designed to assist DMC clinicians with seeking expert advice on treatment needs for specific DMC-ODS beneficiaries. Clinicians are LPHAs. These consultations can occur in person or by synchronous or asynchronous telecommunication systems such as telephone, video, or email. Clinician Consultation Services are to support DMC providers with complex cases and may address medication selection, dosing, side effect management, adherence, drug-drug interactions, or level of care considerations. DMC-ODS Counties may contract with one or more physicians, clinicians, or pharmacists specializing in addiction in order to provide consultation services.
Case Management
Case Management services can be provided at DMC provider sites, participating DMC-ODS County locations, regional centers, or in the community. Services can be provided in person, by synchronous telehealth, or by telephone (audio-only). Case Management shall be provided to a client in conjunction with all levels of treatment.
DMC-ODS Counties, through executed memoranda of understanding, shall coordinate a system of Case Management services with physical and/or mental health in order to ensure a client-centered approach to wellness. Case Management services are defined as services that assist a client to access needed medical, educational, social, prevocational, vocational, rehabilitative, or other community services. These services

49
focus on coordination of SUD care, integration around primary care and any needed mental health services, and interaction with the criminal justice system, if needed. Case Management services may be provided anywhere in the community.
Case Management services include:
• Comprehensive assessment and periodic reassessment of individual needs to determine the need for continuation of case management services;
• Transition to a higher or lower level of care for SUD treatment; • Development and periodic revision of a client plan that includes SUD treatment,
medical care, mental health care, and/or social service needs; • Communication, coordination, referral and related activities to connect
beneficiaries to services such as housing supports, food stamps, court appointments, and other needed services to address social determinants of health;
• Monitoring SUD service delivery to ensure ongoing client access to any needed treatment services; and
• Monitoring the client’s ongoing medical and mental health treatment needs and progress in treatment, retention in primary care services, patient advocacy in other systems of care, and linkages to transportation services.
Additional MAT
Additional MAT is an optional service in DMC-ODS and covers MAT for opioid, alcohol, or other use disorders when the medications are purchased and administered or dispensed outside of the pharmacy benefit (in other words, purchased by providers and administered or dispensed on-site or in the community, and billed to the county DMC-ODS plan). Additional MAT may include the ordering, prescribing, administering, dispensing, and monitoring of MAT in provider settings outside of narcotic treatment programs. DMC-ODS counties may choose to reimburse providers for medications, including long acting injectables, in DMC facilities under this optional provision.
Recovery Services
Recovery Services are designed to support recovery and prevent relapse. The recovery community becomes a therapeutic agent through which clients are empowered and prepared to manage their health and health care. Therefore, treatment must emphasize the client’s central role in managing their health, use effective self-management support strategies, and organize internal and community resources to provide ongoing self-management support to beneficiaries.
Client may receive Recovery Services based on self-assessment or provider assessment of relapse risk; the diagnosis of “remission” is not required to access recovery services. Client receiving MAT, including NTP services, may also receive

50
Recovery Services. Clients may receive Recovery Services immediately after incarceration with a prior diagnosis of SUD. Recovery Services may be provided in person, by telehealth, or by telephone (audio only).
The service components of Recovery Services are:
• Individual or group outpatient counseling services; • Recovery Monitoring – Recovery coaching and monitoring delivered in person,
by synchronous telehealth, or by telephone (audio-only); • Relapse Prevention – A behavioral self-control program that teaches individuals
with SUD how to anticipate and cope with the potential for relapse. Relapse prevention can be used as a stand-alone substance use treatment program or as an aftercare program to sustain gains achieved during initial SUD treatment;
• Education and Job Skills – Linkages to life skill services and supports, employment services, job training, and education services;
• Family Support – Linkages to child care, parent education, child development support services, and family/marriage education;
• Support Groups – Linkages to self-help and support services, and spiritual and faith- based support;
• Ancillary Services – Linkages to housing assistance, transportation, case management, and other individual services coordination; and
• Contingency Management
Peer Support Specialist Services
DHCS is establishing a peer support services benefit to expand the use of certified peer support specialists in DMC-ODS and SMHS counties that opt in to participate. Peer Support Specialist Services are culturally competent services, provided by certified peer support specialists, that promote recovery, resiliency, engagement, socialization, self-sufficiency, self-advocacy, development of natural supports, and identification of strengths. Peer Support Specialist Services aim to prevent relapse, empower and inspire beneficiaries through strength-based coaching and role modeling, support linkages to community resources, and educate beneficiaries and their families about their conditions and the process of recovery. Peer Support Specialist Services will include therapeutic activities, outreach and engagement, and educational groups.
Access to Peer Support Specialist Services will improve recovery outcomes and prevent relapses and symptoms of behavioral health disorders. DHCS’ goal is that peer support specialists would receive a peer certification to provide more integrated services between the behavioral health delivery systems. Since an overwhelming percentage of beneficiaries have co-occurring mental health and substance use disorders, DHCS will establish requirements to ensure the workforce will be cross-trained to recognize and refer when a beneficiary needs care in the other corresponding systems.

51
DMC-ODS Provider Specifications
The following requirements will apply to DMC-ODS staff:
Professional Staff
Definition: Professional staff are defined as Licensed Practitioners of the Healing Arts, including, including:
• Physicians • Nurse Practitioners • Physician Assistants • Registered Nurses • Registered Pharmacists • Licensed Clinical Psychologists (LCPs) • Licensed Clinical Social Workers (LCSWs) • Licensed Professional Clinical Counselors (LPCCs) • Licensed Marriage and Family Therapists (LMFTs) • License-eligible practitioners working under the supervision of licensed clinicians
Licensing/Certification/Accreditation Requirements: Professional staff must be licensed, registered, certified, or recognized under the applicable California scope of practice statutes.
Scope of Services: Professional staff shall provide services within their individual scope of practice and receive supervision required under applicable scope of practice laws. Professional staff may provide services in the ODF, IOT, residential treatment, NTP, additional MAT, withdrawal management, case management, partial hospitalization, and physician consultation modalities.
Natural Helpers
Definition: Natural Helpers are health advisors that provide social supports to the beneficiaries that receive DMC-ODS services from an IHCP. Natural Helpers can be relatives, friends, neighbors, spiritual leaders, elected officials, paraprofessionals, and others that are trusted members of their Native American Tribe, Nation, Band, or Rancheria.
Licensing/Certification/Accreditation Requirements: Natural Helpers are credentialed by the IHCP contractor to deliver social supports in the context of Tribal cultures.
Scope of Services: IHCPs may bill for services provided by Natural Helpers. Natural Helpers may provide navigational support, psychosocial skill building, self-management, and trauma support to individuals. Natural Helpers may provide services in the ODF,

52
IOT, residential treatment, NTP, additional MAT, withdrawal management, case management, and partial hospitalization modalities.
Traditional Healers
Definition: A Traditional Healer is a person with knowledge, skills, and practices based on the theories, beliefs, and experiences that are accepted by that Indian community as handed down through the generations and that can be established through the collective knowledge of the elders of the Indian community.
Licensing/Certification/Accreditation Requirements: A Traditional Healer is a person currently recognized by their Tribal leaders as a spiritual leader and in good standing with their American Indian Tribe, Nation, Band, or Rancheria, and has two years of experience as a recognized American Indian spiritual leader practicing in a setting recognized by their American Indian Tribe, Nation, Band, or Rancheria. The Traditional Healer is employed (or contracted) and credentialed by the IHCP contractor.
Scope of Services: Traditional Healers may use an array of Tribally defined, culturally appropriate interventions to treat beneficiaries with SUDs, including music therapy (such as traditional music and songs, dancing, drumming), traditional practices (such as ceremonies, talking circles, sweat lodges, making regalia, prayer, traditional herbs), and other integrative approaches. Traditional Healers may provide services as a component of the ODF, IOT, residential treatment, NTP, additional MAT, withdrawal management, case management, and partial hospitalization modalities.
Registered and Certified Alcohol and Other Drug Counselors
Definition: Registered and certified alcohol and other drug (AOD) counselors are individuals who provide counseling services in a licensed and/or certified AOD program in compliance with the California Code of Regulations, Title 9, Division 4, Chapter 8.
Licensing/Certification/Accreditation Requirements: AOD counselors must be registered or certified in accordance with the California Code of Regulations, Title 9, Division 4, Chapter 8.
Scope of Services: Registered and certified AOD counselors must adhere to all requirements in the California Code of Regulations, Title 9, Division 4, Chapter 8. Registered and certified AOD counselors may provide counseling services, as they are defined in the California Code of Regulations, Title 9, Division 4, Chapter 8. Registered or certified AOD Counselors may provide services in the ODF, IOT, residential treatment, NTP, additional MAT, withdrawal management, case management, and partial hospitalization modalities.

53
Peer Support Specialists
Peer support specialists will be established as a distinct Medi-Cal provider type that will provide defined peer support Medi-Cal services. By July 1, 2021, DHCS will establish statewide requirements for peer support specialist certification for participating counties to use to certify their peer support specialists.
Peer support specialists will be self-identified as having experience with the process of recovery from mental illness or substance use disorder either as a consumer of these services or as the parent or family member of the consumer, and who are issued a certification under a county peer support specialist certification program. Participating counties will provide supervision of their peer support specialists by competent behavioral health professionals trained in the peer recovery model.
DHCS asserts that a peer support specialist program will improve recovery outcomes and prevent relapses and symptoms of behavioral health disorders. DHCS’ goal is that peer support specialists would receive a peer certification to provide more integrated services between the behavioral health delivery systems. Since an overwhelming percentage of beneficiaries have co-occurring mental health and substance use disorders, DHCS will establish requirements to ensure the workforce will be cross-trained to recognize and refer when a beneficiary needs care in the other corresponding systems.
Responsibilities of DMC-ODS Counties for DMC-ODS Benefits
The responsibilities of DMC-ODS Counties for the DMC-ODS benefit shall be included in each DMC-ODS County’s intergovernmental agreement with DHCS and shall require the DMC-ODS Counties to comply with the following.
Selective Provider Contracting Requirements for DMC-ODS Counties
DMC-ODS Counties select which DMC certified providers they include in their DMC-ODS provider networks. DMC-certified providers that do not receive a DMC-ODS County contract cannot receive a direct contract with the State to provide services to residents of DMC-ODS Counties.
Access
Each DMC-ODS County must ensure that all required services covered under the DMC-ODS are available and accessible to enrollees of the DMC-ODS in accordance with the applicable state and federal time and distance standards for network providers developed by the DHCS, including those set forth in 42 CFR 438.68, and Cal. Welf. & Inst. Code Section 14197 and any Information Notices issued pursuant to those requirements. Access to medically necessary services cannot be denied for beneficiaries meeting criteria for DMC-ODS services. DMC-ODS beneficiaries shall

54
receive services from DMC-certified providers. All DMC-ODS services shall be furnished with reasonable promptness in accordance with federal Medicaid requirements and as specified in the State/DMC-ODS County Intergovernmental Agreement. If the DMC-ODS network is unable to provide medically necessary covered services, the DMC-ODS County must adequately and timely cover these services out-of-network for as long as the DMC-ODS County’s network is unable to provide them.
Access to Medications for Addiction Treatment (MAT)
The DMC-ODS County must require that all DMC-certified providers in its DMC-ODS provider network either provide MAT on-site or have an effective referral mechanism/process in place. Beneficiaries needing or utilizing MAT must be served and cannot be denied treatment services or be required to be tapered off medications as a condition of entering or remaining in the program. DMC-ODS Counties will monitor the referral process or provision of MAT services.
Prior Authorization
DMC-ODS Counties must provide prior authorization for residential services within 24 hours of the prior authorization request being submitted by the provider. DMC-ODS Counties will review the DSM and ASAM Criteria to ensure that the client meets the requirements for the service. DMC-ODS Counties may not impose prior authorization or centralized DMC-ODS County-administered ASAM full assessments prior to provision of outpatient assessment and treatment services. Brief ASAM-based screening tools may be used when beneficiaries call the DMC-ODS County’s beneficiary access number to determine the appropriate location for treatment.
Beneficiary Access Number
All DMC-ODS Counties shall have a 24/7 toll free number for both prospective and current beneficiaries to call to access DMC-ODS services. Oral interpretation services must be made available for beneficiaries, as needed.
DMC-ODS County Responsibility
The DMC-ODS County is responsible for ensuring that its residents receive all medically necessary covered services. If a client is able to access all medically necessary covered services, then the DMC-ODS County is not obligated to subcontract with additional providers to provide more choices for that individual client. However, in accordance with 42 CFR §432.206(b)(4), if the DMC-ODS County’s provider network is unable to provide medically necessary services to a particular client, the DMC-ODS County shall adequately and timely cover these services out-of-network for as long as the DMC-ODS County’s network is unable to provide them. Additionally, the DMC-ODS County shall ensure that beneficiaries that work in or travel to a DMC County (a county that does not opt in to the DMC-ODS program) does not experience a disruption of NTP services. The

55
DMC-ODS County shall require all NTP subcontractors to provide any medically necessary NTP services covered by the Medi-Cal State Plan to such beneficiaries. The DMC-ODS County shall require all NTP subcontractors that provide such services to submit the claims for those services to the DMC-ODS County in which the client resides.
If a county participating in the DMC-ODS is removed from DMC-ODS participation by the State, or elects to cease participating in the DMC-ODS, the county shall immediately cease providing DMC-ODS covered services but shall continue to provide DMC State Plan covered services to its beneficiaries.
If a client moves to a new county and initiates an inter-county transfer, the new county is immediately responsible for DMC-ODS treatment services and can claim reimbursement from DHCS through the Short Doyle Medi-Cal System, as of the date of the inter-county transfer initiation. However, out-of-county services used by beneficiaries who do not intend to move to that county and who have not initiated an inter-county transfer are the responsibility of the client’s County of Residence on record with DHCS.
Implementation Planning and Federal Approval Process
DMC-ODS Counties must submit a DMC-ODS implementation plan to the State. The State will provide the template for the implementation plan. DMC-ODS Counties cannot commence services without an implementation plan being approved by the State, a readiness review being completed by the State, and their network being certified by the State. DMC-ODS Counties must also have an executed State/DMC-ODS County intergovernmental agreement with the DMC-ODS County Board of Supervisors and approved by CMS, as well as executed memoranda of understanding with all Medi-Cal MCPs operating within the DMC-ODS County.
DMC-ODS Counties must offer at least one ASAM level of Residential Treatment Services in order to receive approval for their DMC-ODS County implementation plan in the first year. The DMC-ODS County implementation plan must demonstrate ASAM levels of Residential Treatment Services (Levels 3.1–3.5) within three years of implementation. The DMC-ODS County implementation plan must describe coordination for ASAM Levels 3.7 and 4.0 so beneficiaries can access those services, even if not offered by the DMC-ODS County.
Upon CMS approval of an executed intergovernmental agreement, DMC-ODS Counties will be able to bill for all medically necessary DMC-ODS covered services provided to their beneficiaries.
The intergovernmental agreement will provide further detailed requirements, including but not limited to service delivery, access, monitoring, appeals, and other state and federal requirements.

56
Practice Requirements
DMC-ODS Counties shall ensure that providers implement at least two of the following evidenced-based treatment practices (EBPs) based on the timeline established in the DMC-ODS County implementation plan. The two EBPs are per provider, per service modality. DMC-ODS Counties shall ensure the providers have implemented EBPs and are delivering the practices to fidelity. The State will monitor the implementation of EBPs during reviews. The EBPs are:
• Motivational Interviewing – A client-centered, empathic, but directive counseling strategy designed to explore and reduce a person’s ambivalence toward treatment. This approach frequently includes other problem-solving or solution-focused strategies that build on beneficiaries’ past successes.
• Cognitive-Behavioral Therapy – Based on the theory that most emotional and behavioral reactions are learned and that new ways of reacting and behaving can be learned.
• Relapse Prevention – A behavioral self-control program that teaches individuals with SUD how to anticipate and cope with the potential for relapse. Relapse prevention can be used as a stand-alone substance use treatment program or as an aftercare program to sustain gains achieved during initial SUD treatment.
• Trauma-Informed Treatment – Services must take into account an understanding of trauma, and place priority on trauma survivors’ safety, choice, and control.
• Psycho-Education – Psycho-educational groups are designed to educate beneficiaries about substance abuse and related behaviors and consequences. Psycho-educational groups provide information designed to have a direct application to beneficiaries’ lives; to instill self-awareness, suggest options for growth and change, identify community resources that can assist beneficiaries in recovery, develop an understanding of the process of recovery, and prompt people using substances to take action on their own behalf.
DMC-ODS County Oversight, Monitoring, and Reporting
In accordance with the intergovernmental agreement between the state and a DMC-ODS County, the DMC-ODS County shall have a Quality Improvement Plan that includes the DMC-ODS County’s plan to monitor the capacity of service delivery as evidenced by a description of the current number, types, and geographic distribution of SUD treatment services. For DMC-ODS Counties that have an integrated mental health and substance use disorders department, this Quality Improvement Plan may be combined with the Mental Health Plan (MHP) Quality Improvement Plan. DMC-ODS counties must oversee subcontractors’ compliance through on-site monitoring reviews and monitoring report submissions to DHCS. DMC-ODS Counties are also required to comply with compliance monitoring reviews conducted by DHCS and are responsible to develop and implement Corrective Action Plans as needed.

57
DMC-ODS Financing
January 1, 2022 – at least June 30, 2022
Prior to the execution of the DHCS-approved State/county intergovernmental agreement, only DMC State Plan services shall be reimbursable, and only in accordance with the State Plan reimbursement methodologies.
Participating counties shall propose county-specific rates for all covered DMC-ODS services that are provided by contracted providers, except for the NTP modality, and the State will approve or disapprove those rates. NTP reimbursement shall be set pursuant to the process set forth in Cal. Welf. & Inst. Code Section 14021.51. If during the State review process, the State denies the proposed rates, the county will be provided the opportunity to adjust the rates and resubmit to the State. The State shall retain all approval of the rates to assess that the rates are sufficient to ensure access to available DMC-ODS waiver services. Rates will be included in the State and county intergovernmental agreement. For counties participating in a regional model, contracting with Medi-Cal MCPs to administer the DMC-ODS benefit, counties will reimburse the managed care organizations the contracted Per User Per Month (PUPM) rate. The PUPM is reconciled to the lower of actual costs to the managed care plan or prevailing charges for the services rendered. A CMS-approved CPE protocol, based on actual allowable costs, is required before FFP associated with waiver services is made available to the State. This approved CPE protocol must explain the process the State will use to determine costs incurred by the counties under this demonstration.
After services are provided, participating counties shall certify the total allowable expenditures incurred in providing the DMC-ODS services provided either through county-operated providers (based on the county interim rate), contracted fee-for-service (FFS) providers or contracted MCPs (based on actual expenditures). All interim payments are settled to the lower of actual cost or usual and customary charge.
SB 1020 (Statutes of 2012) created the permanent structure for the 2011 Realignment. It codified the Behavioral Health Subaccount that funds programs including Drug Medi-Cal. Allocations of Realignment funds run on a fiscal year of September 1 through August 30. The monthly allocations are dispersed to counties from the State Controller’s Office. The Department of Finance develops schedules, in consultation with appropriate state agencies and the California State Association of Counties (CSAC), for the allocation of Behavioral Health Subaccount funds to the counties.
Subject to the participation standards and process to be established by the State, counties may also pilot an alternative reimbursement structure for a DMC-ODS modality if both the provider of that modality and the county mutually and contractually agree to participate, including use of case rates. The State and CMS will have the final approval of any alternative reimbursement structure pilot proposed by the county, and such pilot structure must continue to meet the terms and conditions expressed herein, including

58
but not limited to the rate approval process described above. Counties may not utilize any alternative reimbursement structure until approval is received from DHCS and CMS.
No earlier than July 1, 2022 – December 31, 2026
Prior to the execution of the DHCS-approved State/county intergovernmental agreement, only DMC State Plan services shall be reimbursable, and only in accordance with the State Plan reimbursement methodologies.
DHCS will use intergovernmental transfers from all participating counties to finance the nonfederal share of all payments. All participating counties receive a monthly allocation from the Local Revenue Fund 2011 (2011 Realignment) that is restricted to providing Medi-Cal Specialty Mental Health Services, Drug Medi-Cal Services, and other non-Medi-Cal SUD services. All participating counties must first meet the needs of Medi-Cal beneficiaries before spending these restricted funds on non-Medi-Cal services. All participating counties will make monthly transfers to DHCS from these funds to finance the nonfederal share of all DMC-ODS payments.
Participating nonregional counties will be reimbursed pursuant to a fee schedule for all covered DMC-ODS services. Participating regional counties that contract with an MCP will be reimbursed a PUPM rate for each beneficiary who uses at least one DMC-ODS service during that month.
Evaluation
The DHCS shall contract with a third party to conduct an evaluation to measure and monitor the outcomes from the DMC-ODS.
Federal 42 CFR Part 438 and Other Managed Care Requirements
Any entity that receives a prepayment from the State to provide services to beneficiaries will be considered, by federal definition, an MCP and held to all applicable federal 42 CFR Part 438 requirements and requirements in this section. The DMC-ODS Counties will be operating as PIHPs as defined in 42 CFR §438.2.
The following provisions of 42 CFR Part 438 are not applicable to DMC-ODS either because they are nonrisk PIHPs or based on CMS’ determination of inapplicability:
i. 42 CFR §438.3(s)(t) – Standard Contract Requirements; ii. 42 CFR §438.4 – Actuarial Soundness; iii. 48 CFR §438.5 – Rate Development Standards; iv. 438 CFR §438.6 – Special Contract Provisions Related to Payment; v. 42 CFR §438.7 – CMS Review and Approval of the Rate Certifications; vi. 42 CFR §438.8 - Medical loss ratio (MLR) standards;
59
vii. 42 CFR §438.9 - Provisions that apply to non-emergency medical transportation PAHPs;
viii. 42 CFR §438.10(g)(2)(ii)(A) and (B) – Information Requirements; ix. 42 CFR §438.50 – State Plan Requirements; x. 42 CFR §438.54(c) – Voluntary Managed Care Enrollment; xi. 42 CFR §438.71(b)(1)(i) and (iii),(c) and (d) – Client Support System; xii. 42 CFR §438.74 – State Oversight of Minimum MLR Requirements; xiii. 42 CFR §438.104 - Marketing Activities; xiv. 42 CFR §438.110 - Member Advisory Committee; xv. 42 CFR §438.114 – Emergency and Poststabilization Services; xvi. 42 CFR §438.116 – Solvency Standards; xvii. 42 CFR §438.206(b)(2) – Women’s Health Services (No women’s health
services are provided through the DMC-ODS waiver); xviii. 42 CFR §438.208(c)(1) – Identification of Individuals with Special Health Care
Needs; xix. 42 CFR §§438.700-730 – Sanctions; xx. 42 CFR §438.802 – Basic Requirements; xxi. 42 CFR §438.808 – Exclusion of Entities; xxii. 42 CFR §438.810 – Expenditures for Enrollment Broker Services; xxiii. 42 CFR §431.51(b)(2) and §441.202 (No family planning services, including
abortion procedures, are provided through the DMC-ODS waiver); and xxiv. 42 CFR §§455.100-104 – Disclosure Requirements
Choice of Providers
Under the DMC-ODS, free choice of providers is restricted. That is, beneficiaries enrolled in this program shall receive DMC-ODS services through the DMC-ODS County, operating as a PIHP.
External Quality Review
DMC-ODS Counties will include in their implementation plan a strategy and timeline for meeting External Quality Review (EQR) requirements (438.310–370). For new DMC-ODS Counties opting into the ODS, EQR requirements must be phased in within 12 months of having an approved implementation plan.
Enrollment
Beneficiaries are enrolled in a single DMC-ODS in each DMC-ODS County. The DMC-ODS meets the criteria set forth in 42 CFR Part 438 for approving waivers for the choice requirement for PIHPs.

60
Disenrollment
The DMC-ODS meets the criteria set forth in 42 CFR Part 438 for approving waivers for the choice requirement for PIHPs. A waiver of choice requirement conversely implies that of disenrollment since both go hand in hand.
Information Requirements
This section establishes specific requirements for the types, content, and distribution of information describing the DMC-ODS program. Waiver of the distribution requirements of subsection (f)(3) allows DMC-ODS Counties to provide informing materials and provider lists that meet the content requirements of Section 438.10 to beneficiaries when they first access SUD services through the DMC-ODS and upon request. The waiver of subsection (f)(3) would apply to the distribution requirements of the subsection only, not to any other provisions of the subsection except as directly related to the issue of distribution.
Network Adequacy Requirements
At least 60 days prior to CMS contract approval, the State shall submit for each participating DMC-ODS County the applicable network adequacy requirements for the State to certify prior to implementation. CMS concurrence with standards is required.
DMC-ODS Counties will be required to submit executed memoranda of understanding with county MCPs and complete the State’s readiness review.


















