(C20) Just Culture: The Critical Paradigm...
15
11/19/2019 1 (C20) Just Culture: The Critical Paradigm Shift Megan Anders, MD, MS, CPPS Assoc. Chair for Anesthesiology Safety and Quality, Univ. of Maryland School of Medicine Rebekah Friedrich, MS, RN, CCRN, CPPS Sr. Performance Improvement Leader, University of Maryland Medical Center Mangla Gulati, MD, CPPS, FACP, SFHM Chief Quality Officer, Associate CMO VP of Patient Safety & Clinical Effectiveness, University of Maryland Medical Center Nothing to Disclose Dr. Megan Anders, Rebekah Friedrich, and Dr. Mangla Gulati have no relevant financial or nonfinancial relationship(s) within the services described, reviewed, evaluated or compared in this presentation. Session Objectives After attending this session, you will be able to: 1. Explain why a Just Culture is an essential precursor to High Reliability 2. Identify key steps in sustaining cultural change 3. Integrate lessons from our model into an implementation strategy for your organization
Transcript of (C20) Just Culture: The Critical Paradigm...
11/19/2019
1
(C20)Just Culture:
The Critical Paradigm ShiftMegan Anders, MD, MS, CPPS
Assoc. Chair for Anesthesiology Safety and Quality, Univ. of Maryland School of Medicine
Rebekah Friedrich, MS, RN, CCRN, CPPS Sr. Performance Improvement Leader, University of Maryland Medical Center
Mangla Gulati, MD, CPPS, FACP, SFHM Chief Quality Officer, Associate CMO VP of Patient Safety & Clinical Effectiveness,
University of Maryland Medical Center
Nothing to Disclose
Dr. Megan Anders, Rebekah Friedrich, and Dr. Mangla Gulati have no relevant financial or nonfinancial relationship(s) within the services
described, reviewed, evaluated or compared in this presentation.
Session Objectives
After attending this session, you will be able to:
1. Explain why a Just Culture is an essential precursor to High Reliability
2. Identify key steps in sustaining cultural change
3. Integrate lessons from our model into an implementation strategy for your organization
11/19/2019
2
Text message
To: 22333
Body: REBEKAHF711
Live PollingTwo (2) Options to Join
Go online
Visit: PollEv.com/rebekahf711
PollEv.com/rebekahf711
• Academic Medical Center• Two campuses in Baltimore• Home of Shock Trauma Center
• 900 licensed beds• 10,400 staff• > 900 residents & fellows• 1,100 clinical faculty physicians
• Annual encounters:• 32,200 inpatient • 441,500 outpatient
University of Maryland Medical Center
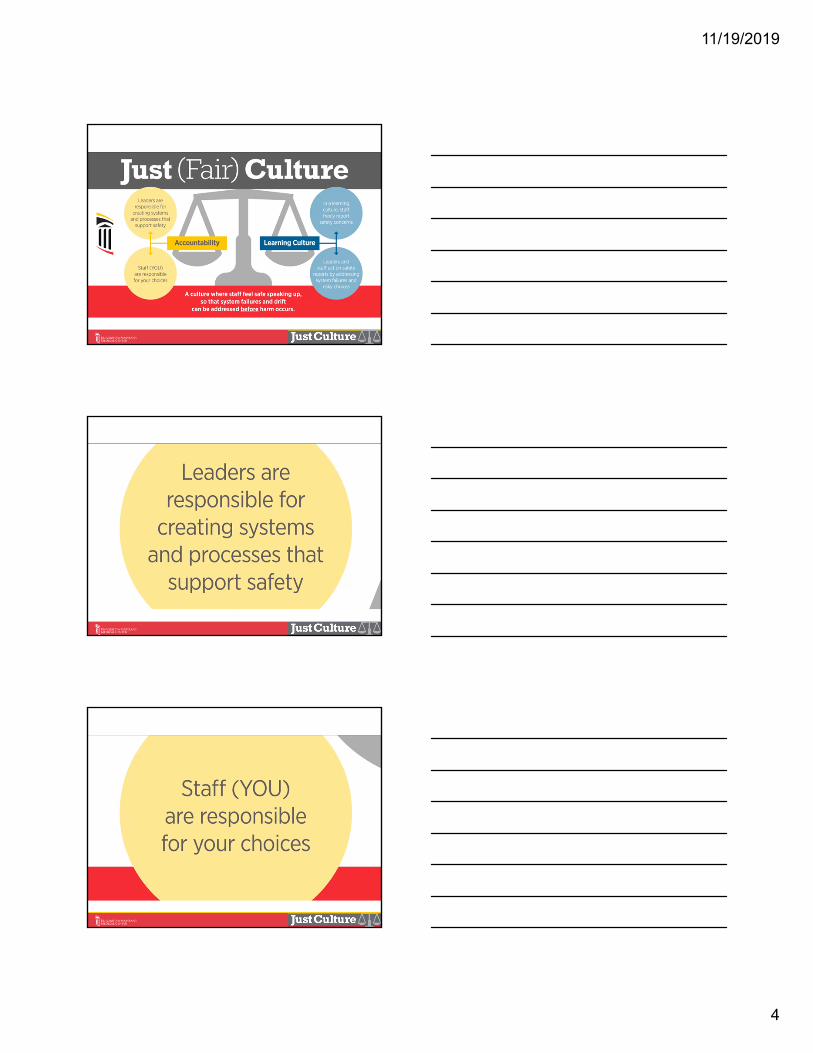
How can we be consistently excellent?
High Reliability Organizations
11/19/2019
3
MidtownDowntown
50
40
30
20
10
0MidtownDowntown
50
40
30
20
10
0
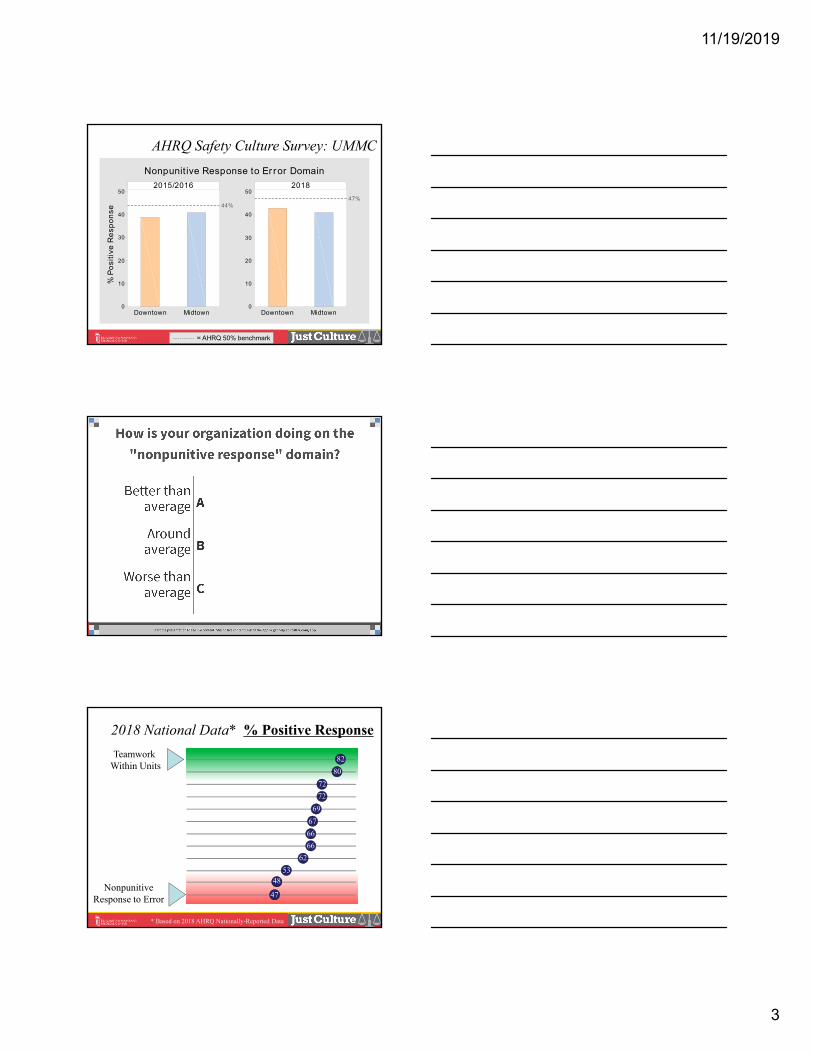
2015/2016
% P
osi
tive
Re
spo
nse
44%
2018
47%
Nonpunit ive Response to Er ror Domain
AHRQ Safety Culture Survey: UMMC
= AHRQ 50% benchmark
47
4853
62
66
66
67
69
72
72
80
82TeamworkWithin Units
NonpunitiveResponse to Error
2018 National Data* % Positive Response
* Based on 2018 AHRQ Nationally-Reported Data
11/19/2019
4
11/19/2019
5
11/19/2019
6
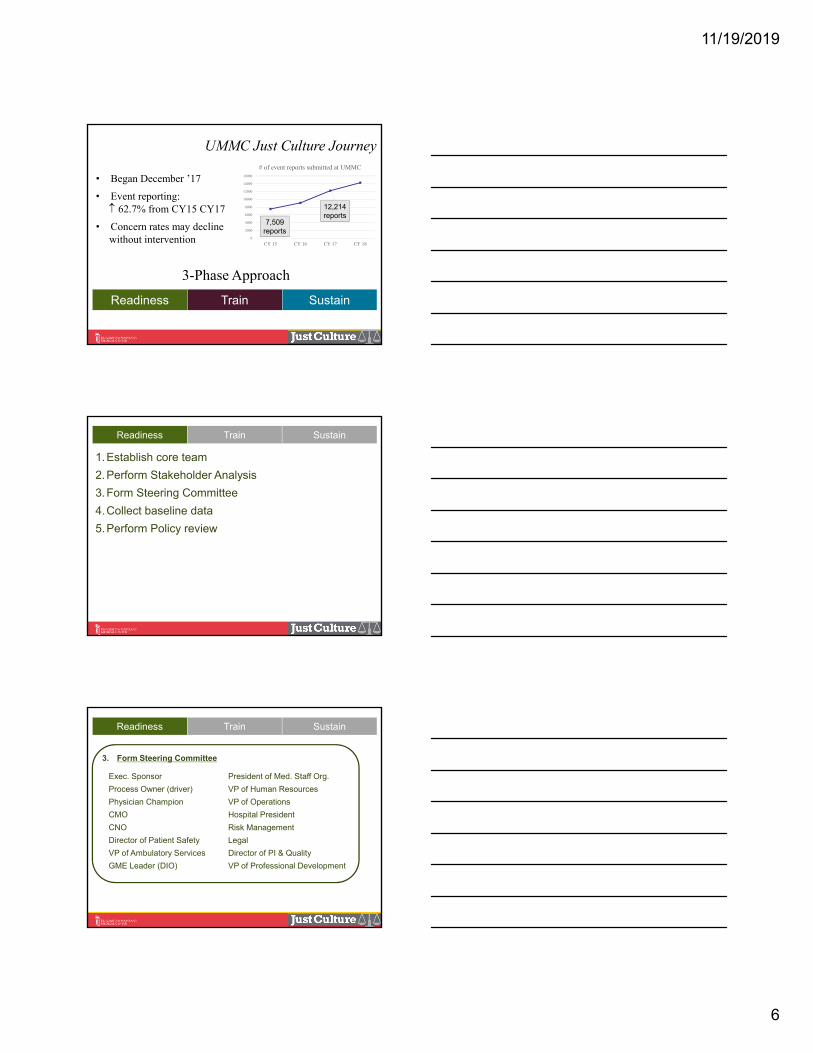
UMMC Just Culture Journey
Readiness Train Sustain
• Began December ’17
• Event reporting: 62.7% from CY15 CY17
• Concern rates may declinewithout intervention 0
2000
4000
6000
8000
10000
12000
14000
16000
CY 15 CY 16 CY 17 CY 18
# of event reports submitted at UMMC
7,509 reports
12,214 reports
3-Phase Approach
Readiness Train Sustain
1.Establish core team
2.Perform Stakeholder Analysis
3.Form Steering Committee
4.Collect baseline data
5.Perform Policy review
3. Form Steering Committee
Exec. Sponsor President of Med. Staff Org.
Process Owner (driver) VP of Human Resources
Physician Champion VP of Operations
CMO Hospital President
CNO Risk Management
Director of Patient Safety Legal
VP of Ambulatory Services Director of PI & Quality
GME Leader (DIO) VP of Professional Development
Readiness Train Sustain
11/19/2019
7
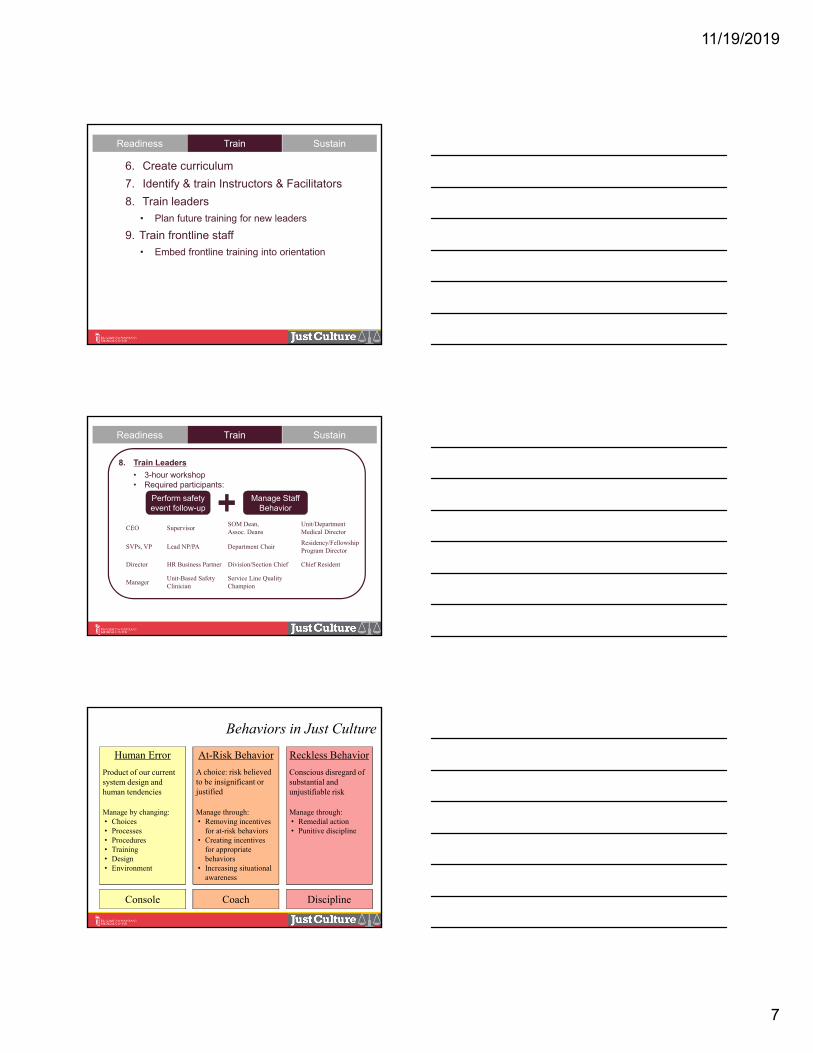
Readiness Train Sustain
6. Create curriculum
7. Identify & train Instructors & Facilitators
8. Train leaders
• Plan future training for new leaders
9. Train frontline staff
• Embed frontline training into orientation
8. Train Leaders
• 3-hour workshop• Required participants:
Perform safety event follow-up
Manage Staff Behavior
CEO SupervisorSOM Dean, Assoc. Deans
Unit/Department Medical Director
SVPs, VP Lead NP/PA Department ChairResidency/FellowshipProgram Director
Director HR Business Partner Division/Section Chief Chief Resident
ManagerUnit-Based Safety Clinician
Service Line Quality Champion
Readiness Train Sustain
Human Error
Product of our current system design and human tendencies
Manage by changing: • Choices• Processes• Procedures• Training• Design• Environment
At-Risk Behavior
A choice: risk believed to be insignificant or justified
Manage through: • Removing incentives
for at-risk behaviors• Creating incentives
for appropriate behaviors
• Increasing situational awareness
Reckless Behavior
Conscious disregard of substantial and unjustifiable risk
Manage through: • Remedial action• Punitive discipline
Console Coach Discipline
Behaviors in Just Culture
11/19/2019
8
• Response is fair, considers:• System failures• THIS situation, context• THIS person’s knowledge• THIS person’s perception of risk
• Response is more fair & consistent • Builds staff trust• Response is more fair & consistent
• Reverse side is “toolkit” (next steps)
Just Culture Algorithm
A Case
Case
Step 1:Determine the action to evaluate
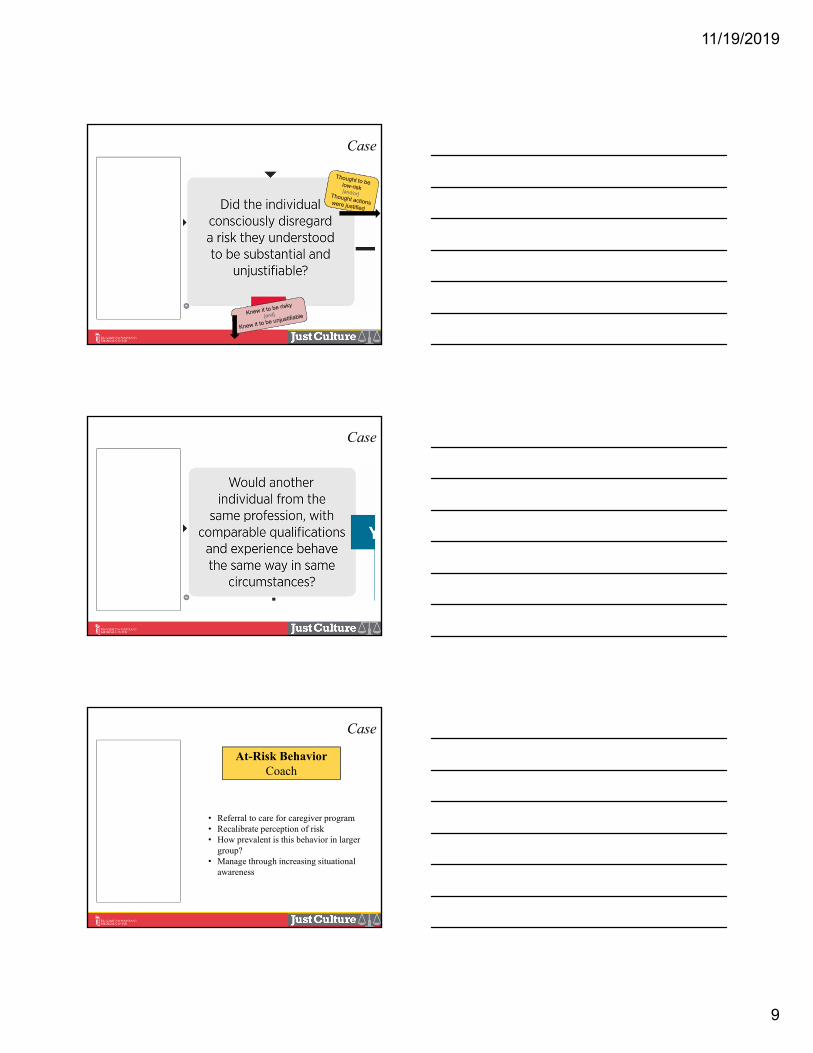
• RN: 1 year experience in ICU
• Sick patient
• 4th dose of rocuronium this shift
• Grabbed medication from wrong bin
• Assumed had selected correct medication
• Didn’t scan or check the med prior to administration
• Administered insulin instead of roc.
11/19/2019
9
Case• RN: 1 year
experience in ICU
• Sick patient
• 4th dose of rocuronium this shift
• Grabbed medication from wrong bin
• Assumed had selected correct medication
• Didn’t scan or check the med prior to administration
• Administered insulin instead of roc.
Case• RN: 1 year
experience in ICU
• Sick patient
• 4th dose of rocuronium this shift
• Grabbed medication from wrong bin
• Assumed had selected correct medication
• Didn’t scan or check the med prior to administration
• Administered insulin instead of roc.
At-Risk BehaviorCoach
• Referral to care for caregiver program• Recalibrate perception of risk• How prevalent is this behavior in larger
group?• Manage through increasing situational
awareness
Case• RN: 1 year
experience in ICU
• Sick patient
• 4th dose of rocuronium this shift
• Grabbed medication from wrong bin
• Assumed had selected correct medication
• Didn’t scan or check the med prior to administration
• Administered insulin instead of roc.
11/19/2019
10
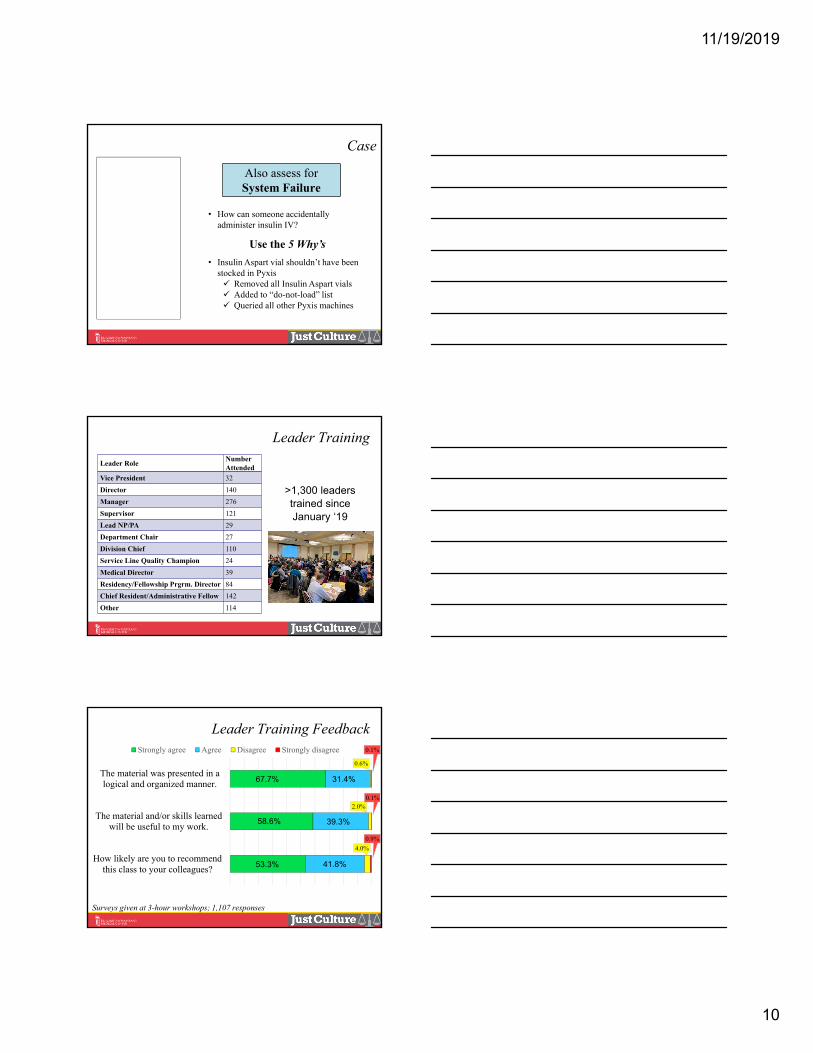
• How can someone accidentally administer insulin IV?
Use the 5 Why’s
• Insulin Aspart vial shouldn’t have been stocked in Pyxis Removed all Insulin Aspart vials Added to “do-not-load” list Queried all other Pyxis machines
Case
Also assess for System Failure
• RN: 1 year experience in ICU
• Sick patient
• 4th dose of rocuronium this shift
• Grabbed medication from wrong bin
• Assumed had selected correct medication
• Didn’t scan or check the med prior to administration
• Administered insulin instead of roc.
Leader Training
>1,300 leaderstrained sinceJanuary ‘19
Leader RoleNumber Attended
Vice President 32
Director 140
Manager 276
Supervisor 121
Lead NP/PA 29
Department Chair 27
Division Chief 110
Service Line Quality Champion 24
Medical Director 39
Residency/Fellowship Prgrm. Director 84
Chief Resident/Administrative Fellow 142
Other 114
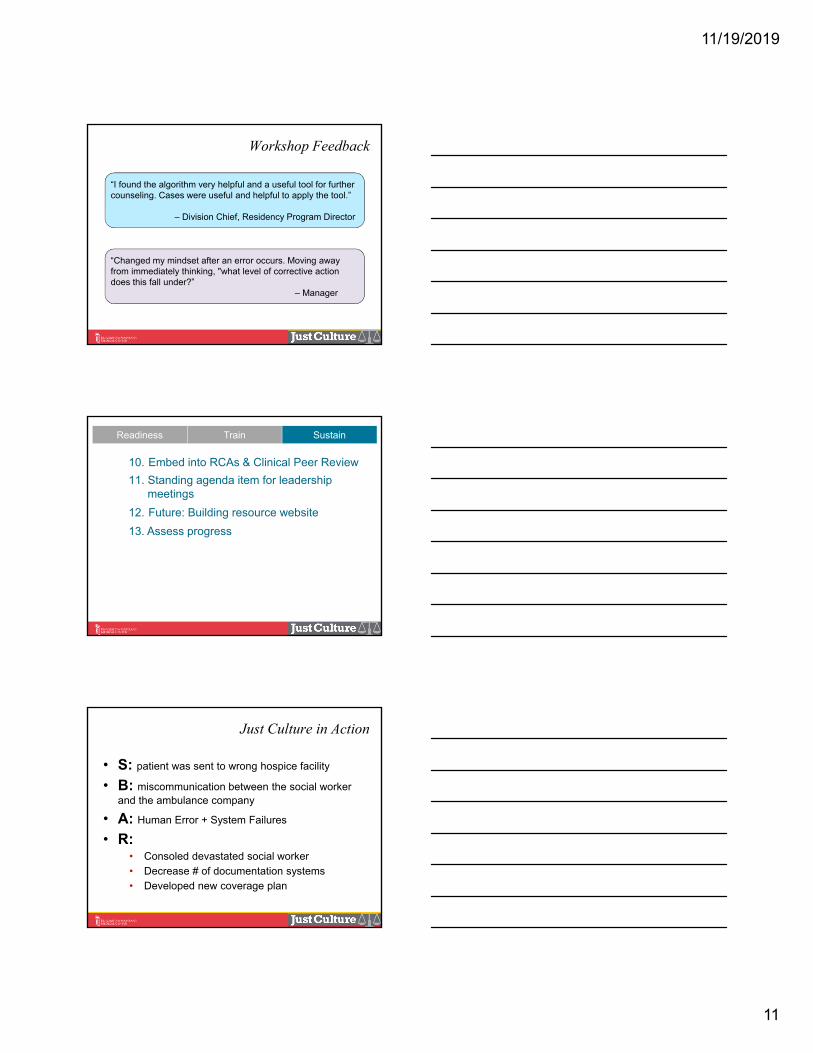
Leader Training Feedback
Surveys given at 3-hour workshops; 1,107 responses
4.0%
2.0%
0.6%
0.9%
0.1%
0.1%
How likely are you to recommendthis class to your colleagues?
The material and/or skills learnedwill be useful to my work.
The material was presented in alogical and organized manner.
Strongly agree Agree Disagree Strongly disagree
67.7%
58.6%
53.3%
31.4%
39.3%
41.8%
11/19/2019
11
Workshop Feedback
“Changed my mindset after an error occurs. Moving away from immediately thinking, "what level of corrective action does this fall under?”
– Manager
“I found the algorithm very helpful and a useful tool for further counseling. Cases were useful and helpful to apply the tool.”
– Division Chief, Residency Program Director
Readiness Train Sustain
10. Embed into RCAs & Clinical Peer Review
11. Standing agenda item for leadership meetings
12. Future: Building resource website
13. Assess progress
Just Culture in Action
• S: patient was sent to wrong hospice facility
• B: miscommunication between the social worker and the ambulance company
• A: Human Error + System Failures
• R: • Consoled devastated social worker
• Decrease # of documentation systems• Developed new coverage plan
11/19/2019
12
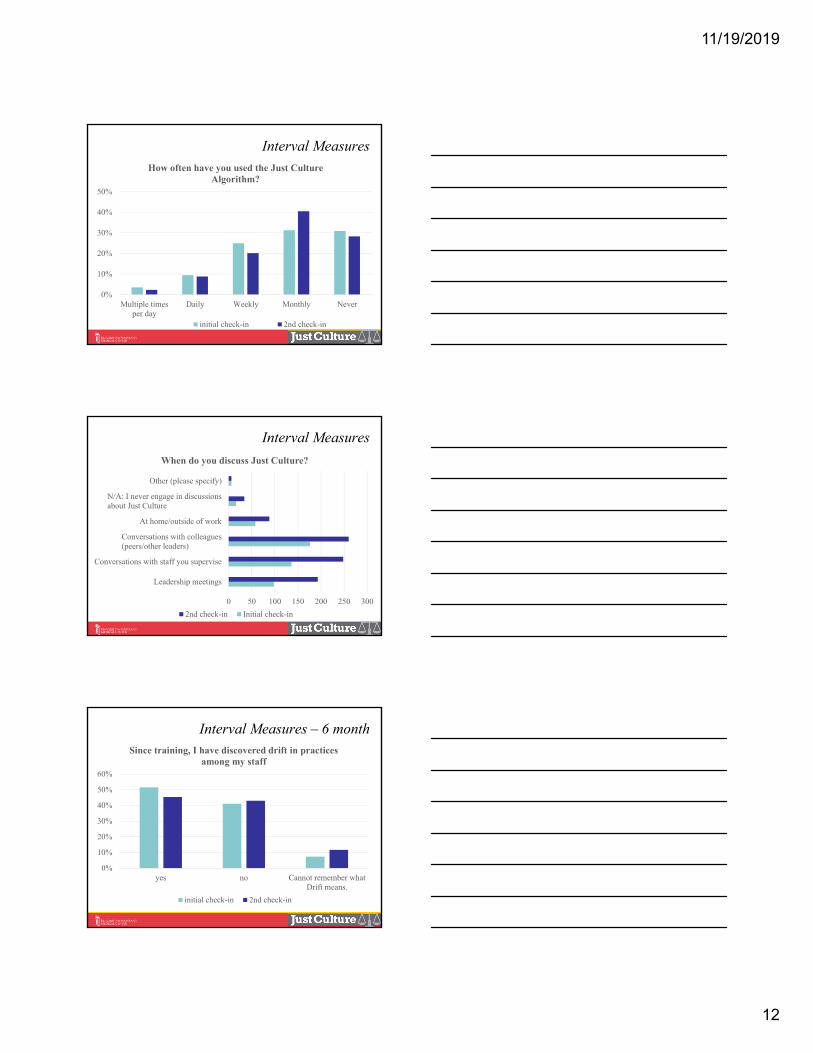
Interval Measures
0%
10%
20%
30%
40%
50%
Multiple timesper day
Daily Weekly Monthly Never
How often have you used the Just Culture Algorithm?
initial check-in 2nd check-in
Interval Measures
0 50 100 150 200 250 300
Leadership meetings
Conversations with staff you supervise
Conversations with colleagues(peers/other leaders)
At home/outside of work
N/A: I never engage in discussionsabout Just Culture
Other (please specify)
When do you discuss Just Culture?
2nd check-in Initial check-in
Interval Measures – 6 month
0%
10%
20%
30%
40%
50%
60%
yes no Cannot remember whatDrift means.
Since training, I have discovered drift in practices among my staff
initial check-in 2nd check-in
11/19/2019
13
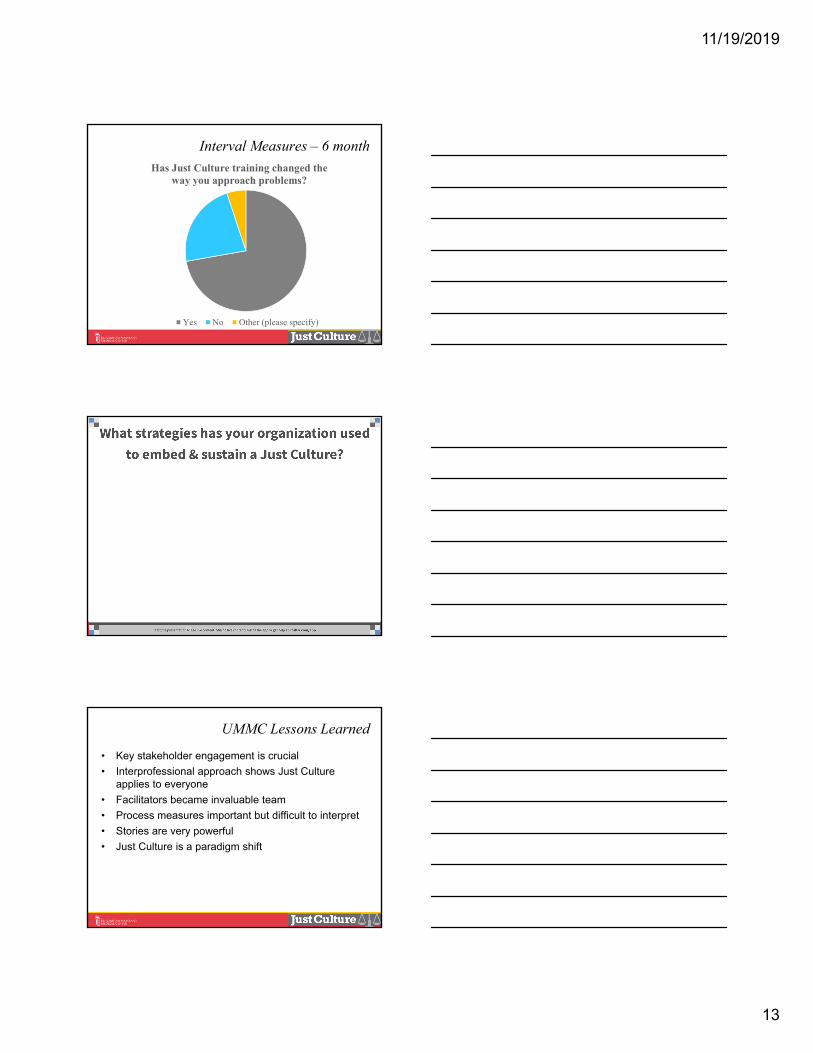
Interval Measures – 6 month
Has Just Culture training changed the way you approach problems?
Yes No Other (please specify)
UMMC Lessons Learned
• Key stakeholder engagement is crucial
• Interprofessional approach shows Just Culture applies to everyone
• Facilitators became invaluable team
• Process measures important but difficult to interpret
• Stories are very powerful
• Just Culture is a paradigm shift
11/19/2019
14
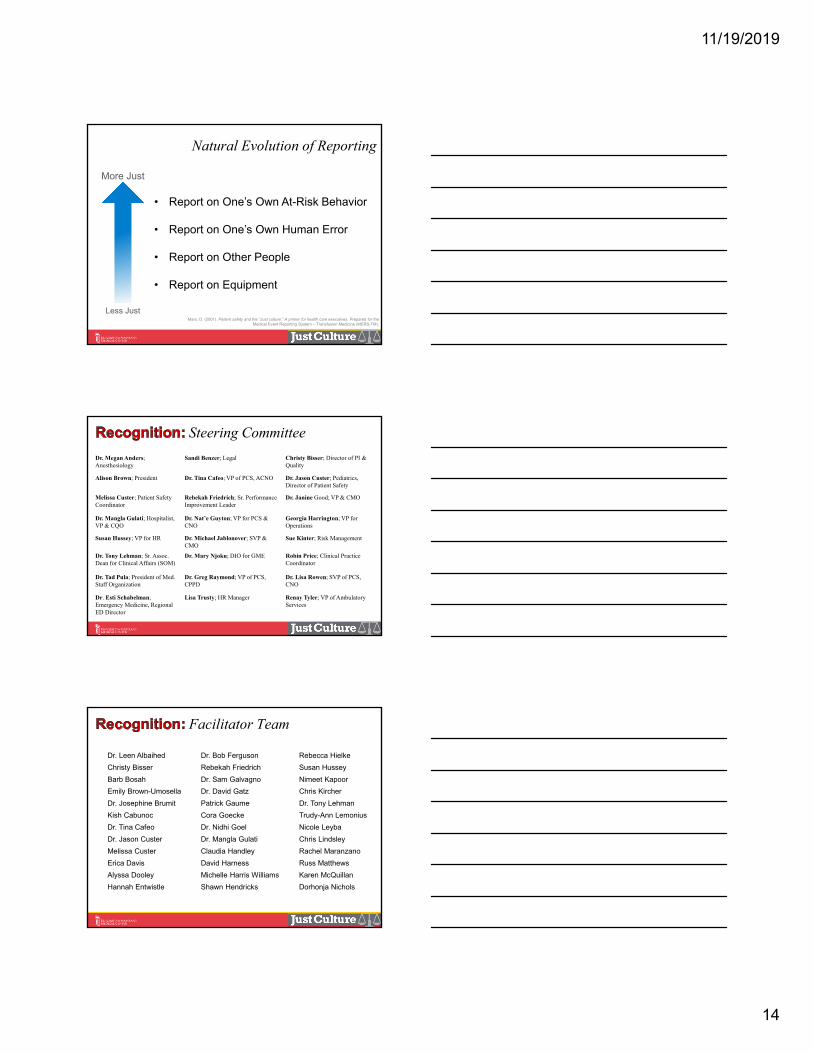
• Report on Equipment
• Report on Other People
• Report on One’s Own Human Error
• Report on One’s Own At-Risk Behavior
Less Just
More Just
Marx, D. (2001). Patient safety and the “Just culture:” A primer for health care executives. Prepared for the Medical Event Reporting System – Transfusion Medicine (MERS-TM).
Natural Evolution of Reporting
Steering Committee
Dr. Megan Anders; Anesthesiology
Sandi Benzer; Legal Christy Bisser; Director of PI & Quality
Alison Brown; President Dr. Tina Cafeo; VP of PCS, ACNO Dr. Jason Custer; Pediatrics, Director of Patient Safety
Melissa Custer; Patient Safety Coordinator
Rebekah Friedrich; Sr. Performance Improvement Leader
Dr. Janine Good; VP & CMO
Dr. Mangla Gulati; Hospitalist, VP & CQO
Dr. Nat’e Guyton; VP for PCS &CNO
Georgia Harrington; VP for Operations
Susan Hussey; VP for HR Dr. Michael Jablonover; SVP & CMO
Sue Kinter; Risk Management
Dr. Tony Lehman; Sr. Assoc. Dean for Clinical Affairs (SOM)
Dr. Mary Njoku; DIO for GME Robin Price; Clinical Practice Coordinator
Dr. Tad Pula; President of Med. Staff Organization
Dr. Greg Raymond; VP of PCS, CPPD
Dr. Lisa Rowen; SVP of PCS,CNO
Dr. Esti Schabelman; Emergency Medicine, Regional ED Director
Lisa Trusty; HR Manager Renay Tyler; VP of Ambulatory Services
Facilitator Team
Dr. Leen Albaihed
Christy Bisser
Barb Bosah
Emily Brown-Umosella
Dr. Josephine Brumit
Kish Cabunoc
Dr. Tina Cafeo
Dr. Jason Custer
Melissa Custer
Erica Davis
Alyssa Dooley
Hannah Entwistle
Dr. Bob Ferguson
Rebekah Friedrich
Dr. Sam Galvagno
Dr. David Gatz
Patrick Gaume
Cora Goecke
Dr. Nidhi Goel
Dr. Mangla Gulati
Claudia Handley
David Harness
Michelle Harris Williams
Shawn Hendricks
Rebecca Hielke
Susan Hussey
Nimeet Kapoor
Chris Kircher
Dr. Tony Lehman
Trudy-Ann Lemonius
Nicole Leyba
Chris Lindsley
Rachel Maranzano
Russ Matthews
Karen McQuillan
Dorhonja Nichols
11/19/2019
15
Facilitator Team (cont…)
Grace Nkonge
Cindi O’Carroll
Cassie O’Malley
Dr. Natalie O’Neill
Dr. Zil Patel
Tacey Penaloza
Michael Anne Preas
Robin Price
Dr. Greg Raymond
Autumn Rosenblum
Mary Jo Simke
Dr. Andrea Smith
Richie Stever
Christine Stough
Dr. Kerri Thom
Dani Thompson
Kerwin Thompson
Dr. Paul Thurman
Lydia Topper
Meg Tripoli
Jessica Wehle
Alison Winter-Lai
Dr. Nicola Zetola
Boysen, P. (2013). Just culture: A foundation for balanced accountability and patient safety. The OschnerJournal, 13, 400-406.
Chassin & Loeb. (2013). High-Reliability health care: Getting there from here. The Milbank Quarterly, 91(3), 459-490.
Dekker, S. (2012). Just Culture- Balancing safety and accountability. Ashgate publishing: Burlington, VT.
Marx, D. (2001). Patient safety and the “Just culture:” A primer for health care executives. Prepared for the Medical Event Reporting System – Transfusion Medicine (MERS-TM).
Meadows, Baker & Butler. (2005). The Incident Decision Tree: Guidelines for Action Following Patient Safety Incidents. Found in Advances in Patient Safety: From Research to Implementation (Vol. 4: Programs, Tools, and Products).
Reason, J. (1997). Managing the risks of organizational accidents. Ashgate publishing: Burlington, VT.
Schmidt, B. (2012). Mitigate drive and organizational change with just culture. Patient Safety & Healthcare Quarterly, May/June. Retrieved from https://www.psqh.com/analysis/mitigate-risk-and-drive-organizational-change-with-just-culture/#
Resources
For more information:
Rebekah Friedrich, MS, RN, CCRN, CPPS
Senior Performance Innovation Leader