C spine positioning
24
X-RAY CERVICAL SPINE Dr ASHISH KUMAR GUPTA PG 2 nd YEAR Dept. of radiodiagnosis SLIMS
-
Upload
docaashishgupt -
Category
Health & Medicine
-
view
478 -
download
0
Transcript of C spine positioning

X-RAY CERVICAL SPINE
Dr ASHISH KUMAR GUPTA
PG 2nd YEARDept. of radiodiagnosisSLIMS

PROJECTION & IMAGING TECHNIQUE

Cervical spine view

Plain Films
Plain films provide the quickest way to survey the cervical spine. An Adequate spine series includes three views: a true lateral (which must include all seven cervical vertebrae as well as C7-T1 junction), and AP view, and an open mouth odontoid view. These three views do not require the patient to move the neck, and should be obtained without removal of the cervical collar.

POSITIONING AP projection :
Patient - either erect or supine Center the mid-sagittal plane
of patients body to mid line of table.
Adjust the shoulders to lie in the transverse plane
Extend the neck enough so that a line from lower edge of chin to the base of the occiput is perpendicular to the film.
Central beam is directed towards C4 VERTEBRA(thyroid cartilage)
Tube tilt- 15 to 20 degrees cephalad.

Film size-18*22cm or 24*30cm. Kvp-80 Suspended expiration. Collimation-include the lower margin of
mandible to lung apex.

AP View The height of the cervical
vertebral bodies should be approximately equal.
The height of each joint space should be roughly equal at all levels.
Progressive loss of disc height uncinate process impact on the reciprocating fossa,producing osteophytes
Spinous process should be in midline and in good alignment.


LATERAL PROJECTION (grandy method)
Patient position: Place the patient in a lateral position either
seated or standing. Adjust the height of the cassette so that it is
centered at the level of 4th cervical segment Adjust the body in a true lateral position,
with the long axis of cervical vertebrae parallel with plane of film
Elevate the chin slightly to prevent superimposition of mandible.
Ask the patient too look steadily at one spot on the wall to aid in maintaining the position of head
Respiration is suspended at end of full exhalation to obtain max depression of the shoulder.

Lateral view. 1) Anterior arch of atlas 2) Posterior arch of atlas3) Dens 4)Laminae C2 5) Spinous Process C6 6) C7-T1 Intervertebral Foramina 7) Retropharyngeal Space (Normal < 7mm) 8) Retrotracheal
Space (Normal <2cm).


Interpretation of Lateral View

Disc spaces should be equal and symmetric

AD interval Atlas-dens space
– should be 3mm or less(Adult)
1-5mm (children)

Prevertebral soft tissue
C1 –nasopharyngeal space-<10mm
C2-c4 retropharyngeal space-<5-7mm
C5-c7- retrotracheal space-<14mm(children), <22mm(adults).

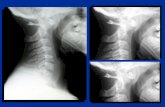
Hyperflexion & hyperextension views Used to Demonstrate normal anterioposterior movement or
fracture/subluxation or degenerative disc disease(vacuum phenomenon).
Spinous process are elevated and widely separated in hyperflexion.
Depressed and closed approximation on the hyperextension position.

HYPERFLEXION HYPEREXTENSION

ODONTOID VIEW SUPINE OR ERECT POSITION. ARMS BY THE SIDE. OPEN MOUTH AS WIDE AS POSSIBLE. ADJUST HEAD SO THAT LINE FROM LOWER EDGE OF
UPPER INCISORS TO THE TIP OF MASTOID PROCESS IS PERPENDICULAR TO THE FILM
Ask to PHONATE ah!!!!!!!!!!

Transoral/AP dens(peg) view An adequate film should include the
entire odontoid and the lateral borders of C1-C2.
Occipital condyles should line up with the lateral masses and superior articular facet of C1.
The distance from the dens to the lateral masses of C1 should be equal bilaterally.
The tips of lateral mass of C1 should line up with the lateral margins of the superior articular facet of C2.
The odontoid should have uninterrupted cortical margins blending with the body of C2.


oblique(ant.&posterior) Patient may be erect or
recumbent. Patient is rotated 45
degree to one side –to left for demonstrating right side neural foramina & to the right to demonstrate left neural foramina.
Central beam directed to c6 vertebra(base of neck) .
Tilt of 15-20 degree caudal for anterior oblique& posterior oblique 15-20 degree cephalad angulation.



job list NAME,AGE, SEX IP NO, INDICATION CONTOUR ALIGNMENT DENSITY IVDS LINES BONES JOINTS PRE AND PARAVERTEBRAL SOFT TISSUE