C Spine Fractures
90
Cervical Spine Dr. Satendra Raut Resident Department of Radiodiagnosis
-
Upload
satendra-raut -
Category
Documents
-
view
83 -
download
10
Transcript of C Spine Fractures

Cervical Spine
Dr. Satendra Raut
Resident
Department of Radiodiagnosis

Bony Anatomy

Vertebral Anatomy

AnatomySpinal cord
occupies:~35% of canal at the
level of the Atlas~ 50% of the canal
in the lower cervical region (C2-7), thoracolumbar spine

Indications for C-spine Films
TendernessNeurologic defecitForceful Mechanism of injuryDistracting injuryAltered sensorium


Modalities
Plain films – Lateral, AP, and Odontoid
CT
MRI

Interpretation of Lateral Plain Film
Mnemonic AABCSAdequacyAlignmentBonesCartilageSoft Tissue

Interpreting Lateral Plain Film
AdequacyShould see C7-T1
junctionIf not get swimmer’s
view or CT

Swimmer’s View

Interpreting lateral Plain Film
AlignmentAnterior vertebral line
Formed by anterior borders of vertebral bodies
Posterior vertebral lineFormed by posterior borders of vertebral bodies
Spino-laminar LineFormed by the junction of the spinous processes and the
laminae
Posterior Spinous LineFormed by posterior aspect of the spinous processes

Alignment


Bones


Cartilage
Predental Space should be no more than 3 mm in adults and 5 mm in children
Increased distance may indicate fracture of odontoid or transverse ligament injury

Cartilage Cont.
Disc SpacesShould be uniform
Assess spaces between the spinous processes

Soft tissue
Nasopharyngeal space (C1) - 10 mm (adult)
Retropharyngeal space (C2-C4) - 5-7 mm
Retrotracheal space (C5-C7) - 14 mm (children), 22 mm (adults)
Extremely variable and nonspecific
Measurements anterior to the mid-cervical spine up to 7 mm are common. > 7 mm,-a fracture is likely and the neck should be immobilized.

Lateral View - Measurements
1. prevertebral space
< 5 mm
2. atlantodental interval
2.5-3 mm
3. sup-inf vertebral align
< 2.7 mm
4. ant-post body height
< 3 mm
5. spinal canal width
> 13 mm
1.
2.
3.
4.
5.

AP C-spine films
Spinous processes should line up.
Disc space should be uniform
Vertebral body height should be uniform. Check for oblique fractures.

Odontoid view
Adequacy: all of the dens and lateral borders of C1 & C2
Alignment: lateral masses of C1 and C2
Bone: Inspect dens for lucent fracture lines




Fracture and dislocationmost common in the lower cervical spine (C4–
C7), the thoracolumbar junction (T10–L2) and at craniovertebral junction (C1–C2).
manifested by loss of vertebral body heightdisruption of the cortical marginsmalalignment of the spine and loss of the parallel apposing cortical surfaces of
bone at the facet joints or intervertebral disc spaces

Fractures
Classified as stable or unstableStability of cervical spine is provided by two
functional vertical columnsAnterior column: vertebral bodies, the disc spaces,
the anterior and posterior longitudinal ligaments and annulus fibrosus
Posterior column: pedicles, facets and apophyseal joints, laminar spinous processes and the posterior ligament complex
As long as one column is intact the injury is stable.

Fractures of the spine

Compression fractures commonly caused by flexion of the spine anterior wedged deformity of the vertebral body or a
depression limited to the vertebral end-plate, usually the superior end-plate
faint band of sclerosis just beneath the deformed end-plate, indicating a zone of bony impaction
severe compression injuries, a portion of the vertebral body may be displaced into the spinal canal, compromising the spinal cord or nerve roots
most commonly encountered in the form of a teardrop fracture in the cervical spine and in burst fractures at the thoracolumbar junction

Simple wedge compression fracture of C7. Anterior wedging of
the vertebral body involving the superior
end-plate, with a separate fragment
arising from the anterior superior margin of the
body. The posterior elements are intact and
the height of the posterior margin of the
vertebral body is maintained. Note the
normal vertebral apophyseal rings on the
adjacent vertebrae (arrows) in this 13-year-
old boy

Fracture-dislocations
most commonly in the lower cervical spine and at the thoracolumbar junction
Usually the upper vertebral body is displaced anteriorly relative to the lower vertebral body
often an anterior wedged compression fracture of the lower vertebral body and fractures involving the laminae, facets, or spinous processes.

Fracture-dislocation at C4–5. There is a disruption of the
facet joints and the intervertebral disc
with the characteristic
anterior displacement of the vertebra above the
level of the dislocation. The
interspinous ligaments are also
disrupted, as evidenced by the separation of the
spinous processes. The facets above are locked anterior to the
facets below. This therefore represents
a bilateral locked facet.

Fractures of the posterior elements
do not commonly occur without accompanying fractures of the vertebral bodies
Exceptionfractures of the transverse processes of the lumbar
spine the neural arches of the first and second cervical
vertebrae and the spinous processes at the cervicothoracic
junction

Classification of injuries
Flexion creates an anterior wedged deformity of the vertebral body
Extension results in a small triangular fragment separated from the anterior inferior margin of the vertebral body

Distraction creates horizontal fractures in the posterior element and little or no wedging of the vertebral body.
Flexion-distraction creates a horizontal fracture of the posterior elements and anterior wedging of the vertebral body

Axial compression is characterized by anterior wedging of the vertebral body and retropulsion of the posterior superior margin of the vertebral body as in burst fractures.
Shearing results in fracture–dislocations manifested by anterior displacement of the vertebra above the level of dislocation carrying with it a triangular avulsed fragment from the anterior superior margin of the vertebral body below. Fractures of the laminae and superior facets are commonly encountered.

Rotational forces are combined with shearing to produce an anterior lateral dislocation of the spine

The atlas—C1
most common - isolated fracture of the posterior or neural arch of the atlas
from compression of the arch between the occiput and the spinous process of C2 during hyperextension.
commonly non-displaced and bilateral Care must be taken to differentiate these fractures
from gaps in the neural arch that occur as normal variations.
is neurologically benign and mechanically stable

Four types of atlas fractures (I, II, III, IV) result from impaction of the occipital condyles on the atlas
The first 2 types of atlas fracture are stable and include isolated fractures of the anterior and posterior arch of C1
Anterior arch fractures usually are avulsion fractures from the anterior portion of the ring and have a low morbidity rate and little clinical significance.
The third type of atlas fracture is a fracture through the lateral mass of C1.
Radiographically, asymmetric displacement of the mass from the rest of the vertebra is seen in the odontoid view. This fracture also has a low morbidity rate and little clinical significance.
The fourth type of atlas fracture is the burst fracture of the ring of C1 and also is known as a Jefferson fracture This is the most significant type of atlas fracture associated with neurologic impairment.
Initial management of types I, II, and III atlas fractures consists of placement of a cervical orthosis. Type IV fracture, or Jefferson fracture, is managed with cervical traction.

Fracture of the posterior arch of C1
(white arrow) combined with
fracture at the base of the dens. Note the posterior dislocation (black arrow). This is a Type 3 fracture as
it includes the superior articular
facet of C2.

Jefferson fracture uncommon injury characterized by disruption of the
anterior and posterior arches of the atlas bilateral anterior and posterior atlantal arch fractures. results from a force delivered to the top of the skull force is transmitted to the occipital condyles and thence
to the superior articulating surfaces of the lateral masses of the atlas
The latter, which are oblique and superiorly concave to articulate with the occipital condyles, may be driven downward and laterally, with the force dissipated through disruptions of the anterior and posterior arch fractures

Fractures
Commonly - increase in predental space on lateral if transverse ligament is damaged and displacement of C1 lateral masses on odontoid.
the Jefferson fracture may be impossible to distinguish from the isolated fracture of the posterior arch of the atlas caused by hyperextension

(A) Lateral radiograph demonstrates fracture of the posterior arch of atlas indistinguishable from the isolated fracture seen in Figure 46.106 . (B) The open-mouth view demonstrates
bilateral displacement of the lateral masses relative to the lateral border of C1 and relative to the lateral margin of the vertebral body of C2 (arrows). Note also the widening of the space between the dens and medial border of the lateral masses of C1. These findings are characteristic of a Jefferson fracture. (C,D) CT demonstrates a single fracture in the right
portion of the anterior arch (arrowhead) and bilateral fractures of the posterior arch.

The axis—C2
Fractures of the axis are quite common and at times are radiographically obscure
C2 should be scrutinized for evidence of injury in every case of suspected neck injury

Hangman's fracture (traumatic spondylolysis of the axis)
fractures of the neural arch of C2 that are produced by a hyperextension force
bilateral fractures of the neural arch anterior to the inferior facets
same fracture as caused by judicial hanging and it is therefore often referred to as a hangman's fracture

Hangman’s FractureExtension injuryBilateral fractures of
C2 pedicles (white arrow)
Anterior dislocation of C2 vertebral body secondary to ALL tear (red arrow)
Unstable

The fracture lines are usually oblique and tend to be relatively symmetrical and often associated with dislocation of C2 on C3
There may be an avulsion fracture of the anteroinferior margin of C2
Neurological consequences of the hangman's fracture are often less severe than might be anticipated the normal cervical cord occupies only
approximately one-third to one-half of the AP diameter of the normal spinal canal at this level
the bilateral isthmus fracture produces a decompression of the canal.



Undisplaced hangman's fracture. The arrow indicates
the fracture of the pars interarticularis

This is a hangman's
fracture with subluxation of
C2 upon C3 and widely displaced fracture in the
neural arch

Hangman's fracture with wide
separation of the fracture fragments and locking of the
C2 facets anterior to C3. There is also a
small fragment arising from the
anterior margin of the vertebral body
of C2.

Fractures of the odontoid
Odontoid Complex mechanism of injuryGenerally unstableType 1 avulsion fracture of the superolateral portion of
the tip of the dens by the intact alar ligamentrare
Type 2 transverse fracture at the base of the dens Most common
Type 3 superior portion of the axis body with extension through one or both of its superior articular facetsBest prognosis

Fractures
Types 1 and 2 are also known as ‘high’ and Type 3 as ‘low’ dens fractures
most reliable, though non-specific, marker of a dens fracture is soft tissue swelling anterior to the atlanto-axial articulation
Plain film tomography may be superior to CT in the detection of subtle dens fractures because the fracture line may lie precisely in the plane of a CT image and be obscured by volume averaging and therefore not recorded.




High (Type II) dens fracture in frontal (A) and lateral (B) projections. The fracture lines (arrowheads) are confined entirely
to the base of the dens

Low (Type III) dens fracture. (A) AP open-mouth view demonstrates lateral tilting of the dens. No fracture line is
apparent. This is frequently the case in this type of fracture. (B) Lateral view demonstrates disruption of the ring of C2 (arrows).
There is slight anterior tilting of the long axis of the dens. The dens is usually either in neutral or posterior angulation relative to
the body of C2 in lateral projection. (C) A lateral tomogram clearly demonstrates the fracture line and the tilting of the dens

Extension teardrop fracture
fracture of the anteroinferior corner of the body of C2 avulsed by the intact anterior longitudinal ligament
The vertical height of the extension teardrop fragment equals or exceeds its horizontal width
not associated with neurological deficitmay occur in isolation or be associated with a
hangman's fracture

Extension teardrop fracture of C2. Note the
triangular fragment arising from the
anterior inferior margin of the vertebral body
and the marked swelling in the
retropharyngeal tissue representing a
haematoma. The circular lucency within
the soft tissues projected within the retropharyngeal soft tissues represents a snap on the cervical collar. There is slight
posterior subluxation of C2 upon C3 in keeping with the hyperextension
mechanism and disruption of the
intervertebral disc

Sciwora' Syndrome: Unique in Children A special situation involving children deserves mention. In children, it
is not uncommon for a spinal cord injury to show no radiographic abnormalities. This situation has been named "SCIWORA" (spinal cord injury without radiographic abnormality) syndrome. SCIWORA syndrome occurs when the elastic ligaments of a child's neck stretch during trauma. As a result, the spinal cord also undergoes stretching, leading to neuronal injury or, in some cases, complete severing of the cord.This situation may account for up to 70 percent of spinal cord injuries in children and is most common in children younger than eight years. Paralysis may be present on the patient's arrival in the emergency department. However, up to 30 percent of patients have a delayed onset of neurologic abnormalities, which may not occur until up to four or five days after the injury. In patients with delayed symptoms, many have neurologic symptoms at the time of the injury, such as paresthesias or weakness, that have subsequently resolved.

Cont….

The lower cervical spine—C3–C7
Injuries consists of various fractures of the vertebral body
with or without associated dislocation or subluxation
with or without significant fractures of the vertebral body and
fractures limited to the posterior elements without associated dislocation

Teardrop fracture caused by motor vehicle accidents and diving into shallow water is a fracture-dislocation due to flexion and axial compression usually associated with spinal cord injury characterized by a distinct triangular fragment of the anteroinferior
aspect of the vertebral body involved and is said to resemble a teardrop Reduced anterior height of the vertebral body Diffuse prevertebral soft tissue swelling -common posterior displacement of the fractured vertebra and diastasis of the
interfacetal joints indicate disruption of the longitudinal ligaments, intervertebral disc and posterior ligament complex


Flexion teardrop fracture. (A) In the lateral radiograph of the
cervical spine obtained immediately after the injury, the
cervical spine is in the flexed attitude. A single large fragment consisting of the anteroinferior
corner of the body of C5 is present. The fifth vertebral body is posteriorly displaced and, in
addition, widening of the interfacetal and interspinous
spaces between C5 and C6 indicates complete disruption of the posterior ligament complex
and bilateral interfacetal dislocation. (B) In the lateral
examination carried out 2 weeks after the injury, the
characteristic teardrop-shaped fragment is seen. In addition, the
subjacent intervertebral disc space is abnormally widened, as
are the interfacetal and interspinous spaces, indicating
complete soft tissue disruption at the involved level.

Flexion Teardrop fractureFlexion injury
causing a fracture of the anteroinferior portion of the vertebral body
Unstable because usually associated with ligamentous injury

Bilateral locked facets or bilateral interfacetal dislocation (BID)
may occur at any level of the lower cervical spine some degree of neurological deficit Both facet joints at the level of injury are dislocated and all the
interosseous ligaments, including the intervertebral disc- disrupted-marked forward displacement of the involved vertebrae
radiographic features are anterior displacement of the involved vertebrae for a distance of at least one-half the sagittal diameter of a vertebral body and complete dislocation of the articular masses of the involved vertebrae
The articular masses of the vertebra above lie completely anterior to the articular masses of the vertebra below, thus ‘locking’ the facets
accompanied by bilateral laminar fractures of the vertebra above, the laminae and spinous process remaining aligned with the opposing elements of the vertebra below

Unilateral locked facets, or unilateral interfacetal dislocation (UID), is caused by simultaneous flexion and rotation
With flexion and rotation, the involved vertebra moves anteriorly and rotates on its vertical axis, causing dislocation of the interfacetal joint on the side opposite the direction of rotation
dislocated facet comes to rest anterior to the subjacent facet and is thus ‘locked’

Bilateral Facet Dislocation Flexion injury Subluxation of dislocated
vertebra of greater than ½ the AP diameter of the vertebral body below it
High incidence of spinal cord injury
Extremely unstable

Bilateral locked facets at C4–5 (interfacetal
dislocation). Note that the lateral
mass of the inferior facet of
C4 is locked anteriorly to the superior facet of
C5


In the frontal radiograph the spinous processes from the level of the dislocation cephalad are rotated off the midline in the direction opposite that of rotation and therefore point to the side of dislocation.
In the lateral projection , the dislocated vertebra is anteriorly displaced 25% of the sagittal diameter of a cervical vertebral body.
The articular masses and interfacetal joints are no longer superimposed from the level of the dislocation upward.
The spine above the level of dislocation is obliquely oriented, with the spine below in direct lateral orientation.
The oblique orientation gives rise to a ‘bow tie' or ‘butterfly' appearance of the rotated articular masses .
The distance between the posterior surface of the articular mass and the spinolaminar junction line of the vertebrae below the dislocation is greater than that of the vertebrae above with an abrupt change in this distance at the level of the dislocation.
Associated fracture of either the dislocated or contiguous articular mass is common. The anterior displacement of the cephalad vertebra may decrease as a result of the fracture. CT best demonstrates the abnormalities

Unilateral locked facets. In the frontal projection (A), the spinous processes from C6 and above (arrowheads) are rotated off the midline. In the lateral projection (B), the sixth cervical vertebra is displaced slightly anteriorly on C7 by a distance less than half the anteroposterior diameter of a cervical vertebral body. Additionally, from the level of C6 upwards, the posterior cortical margins of the articular masses (arrowheads) are not superimposed, reflecting the rotational components of this injury

Unilateral locked facets at C5–6. In this case the ‘bow tie’ or ‘butterfly’ configuration of the facet is characteristic of this lesion and is clearly depicted by the dashed lines. Note that at the level of dislocation, the vertebrae above are in the oblique projection and those below are in the lateral projection. The distance between the posterior surface of the facets and the spinolaminar line above the level of dislocation is obliterated, whereas the space is preserved below the level of dislocation. This is a very sensitive indicator that the vertebrae above are rotated and those below are in the lateral projection. One can see that the inferior facet of one side (arrow) lies anterior to the vertebra below

Unilateral locked facets of C6 on the left. CT images. The facet joints at C5/C6 are subluxed on the right side (A). The midline images (B) show that C5 is subluxed anteriorly upon C6 approximately 25% of the width of vertebral body. The C5 facet is locked anterior to C6 facet on the left side (C). (Case courtesy of Dr. Raymond F. Carmody, Tucson, Arizona).

Hyperextension fracture-dislocation of C4. The frontal projection (A) shows a comminuted fracture of the articular mass of C4 on the right (*). The lateral projection (B) shows that the body of C4 is anteriorly displaced. The anatomy of the posterior elements at the C4–5 level is completely disorganized. In the right anterior oblique projection (C) the articular mass of C4 is shown to be severely comminuted. The inferior articulating facet of C4 has been completely destroyed (‘flattened facet’ sign). In addition, there is a transverse fracture through the superior articulating facet of C5 (arrowhead). In the left anterior oblique projection (D) there is an interfacetal dislocation of C4 with respect to C5 (stemmed arrow).

Hyperflexion sprain is a pure soft tissue and ligamentous injury caused by acute flexion without
axial compression. The principal radiographic sign is localized kyphotic angulation. This must be differentiated from a reversal of cervical lordosis due to
muscle spasm. Signs of hyperflexion strain on the lateral view include widening of the
interspinous or interlaminar space (‘fanning’), subluxation of the interfacetal joints and posterior widening and anterior narrowing of the intervertebral disc with or without 1–3 mm of anterior displacement of the vertebra.
The findings may be accentuated by carrying out a lateral view in flexion and diminished by doing a similar view in extension.
When performing lateral flexion and extension views, the radiologist must personally control the positioning of the patient's head and preclude forced flexion and extension, which might precipitate or aggravate cervical cord or root injury.

Anterior subluxation of C3 on C4. In the flexed position (A), C3 is anteriorly displaced with respect to C4 by a distance of 2–3 mm. In addition C3 has pivoted upon the anteroinferior corner of its vertebral body, and this, coupled with the anterior translation, has caused a hyperkyphotic angulation at the C2–3 level. The interfacetal joint space is widened posteriorly and the interspinous space is widened (‘fanning’). In the same patient, in the hyperextended position (B) the spine appears normal

Hyperflexion sprain is associated with 30–50% incidence of delayed instability due to failure of ligamentous healing. A posterior fusion is often required to prevent subsequent anterior subluxation or dislocation

Hyperextension injury in spondylosis
Hyperextension of the head upon the neck causes the cord to be pinched between posterior vertebral osteophytes and the thickened ligamentum flavum, resulting in a spinal cord injury.
This is often associated with a retropharyngeal haematoma secondary to a disruption of the anterior longitudinal ligament.
Occasionally, a small fracture of the anteroinferior surface of the vertebra results from an avulsion fracture at the site of the tear in the anterior longitudinal ligament.
Despite the profound neurological deficit, there is often no evidence of fracture or dislocation.
This injury results in the central cervical cord syndrome, characterized by flaccid paralysis from the level of dislocation and sensory changes that are greater in the upper extremity than in the lower.
The extent and nature (oedema or haemorrhage) of the cord injury determine whether the neurological changes are minimal and transitory or severe and permanent.

Spondylosis with quadriplegia following minor trauma (A). The AP and lateral projections demonstrate changes of degenerative arthritis. The lateral projection (B) shows retropharyngeal soft tissue swelling and a small fracture from the anterior inferior margin of C6 (arrow) and a fracture of the spinous process of C3 (open arrow). These two fractures attest to the hyperextension mechanism of injury

Clay shoveller's fracture Isolated fractures of the posterior elements are rare and
difficult to visualize on plain radiographs. The only exception is the ‘clay shoveller's fracture’ an avulsion of the spinous process of C6, C7 or T1 caused
either by rotation of the upper trunk when the cervical spine is relatively fixed or, less commonly, as the result of a direct blow.
CT may demonstrate other fractures of the posterior elements .
Thus CT should be obtained on patients with initial negative plain radiographs who experience continued pain following trauma.

Fractures of the posterior elements. (A) Clay shoveller's fracture (arrow) of the spinous process of C6–7. (B,C) Left pediculolaminar fracture. The plain radiographs were unremarkable. The arrow indicates the fracture of the pedicle and transverse process. The laminar fracture is identified by arrowheads

Clay Shoveler’s FractureFlexion fracture of
spinous process C7>C6>T1stable

Fractures
Burst FractureFracture of C3-C7
from axial loadinngSpinal cord injury is
common from posterior displacement of fragments
Stable if ligaments intact

Whiplash injury The injury is caused by a sudden deceleration of the
body, as occurs when an automobile is stopped suddenly by collision or when a stationary automobile is struck from behind by a moving vehicle.
The head is thus snapped back and forth—‘whiplashed’.
There is considerable difference of opinion about the importance of the whiplash injury as a cause of clinical complaints and disability.

Minor degrees of reversal of the cervical curve, as well as minimal offset of one cervical vertebra on another, may be produced by voluntary muscle contraction and therefore presumably can be produced by muscle spasm secondary to pain, without any actual ligamentous injury of the cervical spine.
This adds to the difficulty in assessing the significance of minor variations in the cervical spine.
Care should be taken not to overemphasize these variations.

Thank you

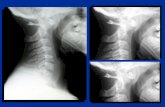
Swimmer’s viewThe swimmers view is all about getting the
humeral heads projected clear of the cervical spine anatomy.
It is usually the humeral heads that obscure the cervico-thoracic junction.
This technique involves moves both humeral heads anteriorly.
This can be achieved by having the patient cross their arms in front of them or by holding onto a bar attached to the upright bucky.