
C LINICAL S TAFF T RAINING P RESENTATION 1 Crystal Blais, Ph.D. Scientific Affairs Liaison Training...
40
CLINICAL STAFF TRAINING PRESENTATION 1 Crystal Blais, Ph.D. Scientific Affairs Liaison Training Program Manager © 2014 Nuraleve, Inc. Proprietary and Confidential. 13-11-2014 SOP-LI-03-57 Rev C
-
Upload
vanesa-maxfield -
Category
Documents
-
view
213 -
download
0
Transcript of C LINICAL S TAFF T RAINING P RESENTATION 1 Crystal Blais, Ph.D. Scientific Affairs Liaison Training...

CLINICAL STAFF TRAINING PRESENTATION
1
Crystal Blais, Ph.D.Scientific Affairs LiaisonTraining Program Manager
© 2014 Nuraleve, Inc. Proprietary and Confidential.13-11-2014
SOP-LI-03-57 Rev C

Defining Chronic Pain
2

Definitions: Pain
Pain
An unpleasant sensory or emotional experience associated with potential or actual tissue damage, or described in terms of such damage
33© 2014 Nuraleve, Inc. Proprietary and Confidential.
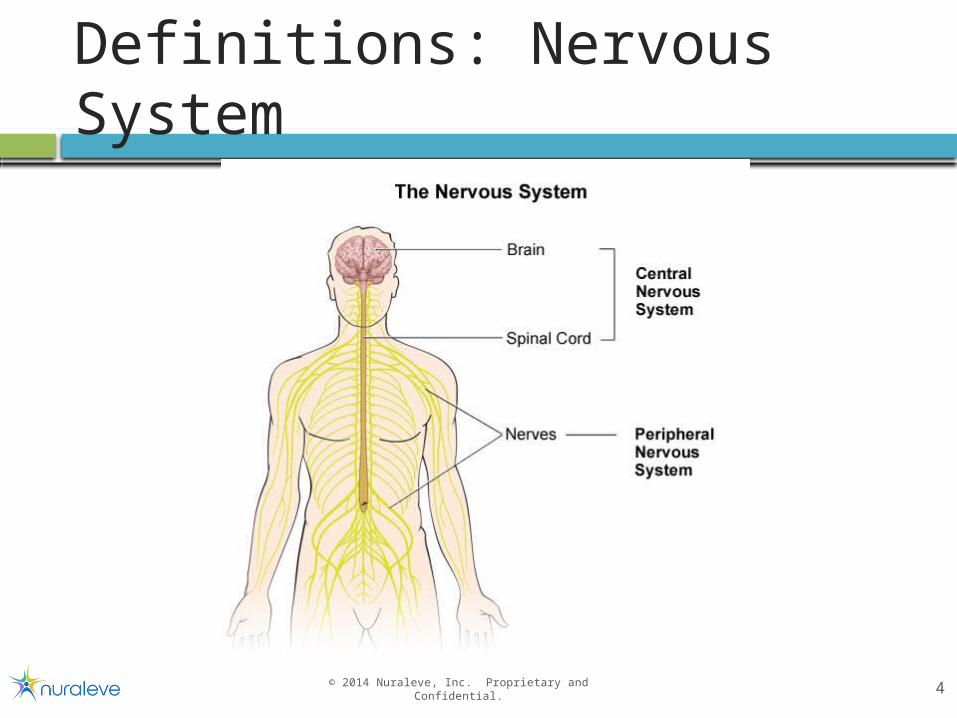
Definitions: Nervous System
44© 2014 Nuraleve, Inc. Proprietary and Confidential.

Definitions: Nociception
55

How injury leads to pain
Steps: Transduction: from noxious stimuli at nociceptors to nerve
impulses
Transmission: nerve impulses from periphery to CNS
Perception: the experience of pain
Modulation: modulation of pain from brain to spinal cord
Sensitization – important for chronic pain development
Peripheral sensitization: nociceptors generate nerve impulses easier
Central sensitization: spinal neuron hyper-excitability
66© 2014 Nuraleve, Inc. Proprietary and Confidential.

Classes of pain
Acute pain
Chronic pain (or chronic non-cancer pain)
Cancer pain
Acute pain Occurs in response to tissue trauma
Goes away when injury heals
Serves an important biological function
77© 2014 Nuraleve, Inc. Proprietary and Confidential.

Chronic Pain: Definition
Chronic pain features: Pain that persists past the normal time of healing
Pain lasting longer than 12 weeks*
Low levels of underlying pathology that do not explain the presence and/or extent of the pain
Perpetuated by factors remote from the cause
Pain continues to occur (continuous or intermittently) without acute exacerbations
A persistent pain that “disrupts sleep and normal living, ceases to
serve a protective function, and instead degrades health and
functional capability”
88© 2014 Nuraleve, Inc. Proprietary and Confidential.

Causes of Chronic Pain
Acute injury (e.g., whiplash)
Chronic conditions (e.g., multiple sclerosis)
In some cases: no discernable cause
99© 2014 Nuraleve, Inc. Proprietary and Confidential.

tDCS: How It Works
10

Background
Transcranial direct current stimulation (tDCS)
Non-invasive technique
Administered using scalp electrodes
Low amounts of current (DC)
standard dose: 2 mA
Stimulates select regions of the brain
For chronic pain: motor cortex (M1)
Session duration: 20 minutes
1111© 2014 Nuraleve, Inc. Proprietary and Confidential.

Background
1212© 2014 Nuraleve, Inc. Proprietary and Confidential.
Two electrodes:
Anode Cathode
Current flows from anode to cathode
Two methods of stimulation:
Anodal stimulation
Cathodal stimulation

Cortical Excitability
1313© 2014 Nuraleve, Inc. Proprietary and Confidential.
Anodal stimulation
Increased cortical excitability
Cathodal stimulation
Decreased cortical excitability
tDCS changes how our neural circuits respond to stimuli

tDCS & Neuromodulation
1414© 2014 Nuraleve, Inc. Proprietary and Confidential.
Long-term brain changes via tDCS occur due to:
1. Modulation of neurotransmitter activity glutamate GABA
2. Neuronal excitation Long-term potentiation (LTP) Increased synaptic strength/efficacy
3. Neuroplasticity Functional changes

tDCS & Chronic Pain
1515© 2014 Nuraleve, Inc. Proprietary and Confidential.
Anodal stimulation of the motor cortex (MI1)results in decreased pain due to:
Decreased processing of pain signals Via suppression of sensory neurons in thalamus
Decreased activity in somatosensory cortex Via direct pathway with M1
Endogenous opioid release

tDCS & Chronic Pain
1616© 2014 Nuraleve, Inc. Proprietary and Confidential.
Anodal stimulation of the motor cortex (MI1)results in decreased pain due to:
Decreased processing of pain signals Via suppression of sensory neurons in thalamus
Decreased activity in somatosensory cortex Via direct pathway with M1
Endogenous opioid release

Safe Use
tDCS is safe when applied within standard safety guidelines
Minor adverse events include: Mild tingling sensation Drowsiness Itching/burning Headache Light headedness
No major side effects or serious adverse events have been reported
1717© 2014 Nuraleve, Inc. Proprietary and Confidential.

Contraindications
Patients may not be eligible for Painrelief if they:
Are under 18 years of age
Have had a recent (<6 months ago) head injury
Have a history of seizures/epilepsy
Have metal embedded in the skull
Have a pacemaker and/or other implanted electrical devices
Have lesions, lipomas, open wounds or bruising on the scalp at the electrode site
1818© 2014 Nuraleve, Inc. Proprietary and Confidential.

tDCS & Chronic Pain: Studies
19

tDCS & Chronic Pain: Indications
Fibromyalgia
Migraines
Diabetic neuropathy
Chronic back pain
Trigeminal neuralgia
Polyneuropathy
Atypical face pain
Arthrosis
Post-stroke pain
Phantom pain
2020© 2014 Nuraleve, Inc. Proprietary and Confidential.

tDCS & the Motor Cortex (M1)
2121© 2014 Nuraleve, Inc. Proprietary and Confidential.
Decreased pain intensity Decreased pain frequency Decreased pain duration Improved quality of life Improved sleep quality
Beneficial effects are both acute and long-lasting Effects seen up to 4 months post-treatment
Anodal stimulation of M1 results in:

Anodal tDCS of M1: Studies
2222© 2014 Nuraleve, Inc. Proprietary and Confidential.
Study Population SampleSize Sessions Efficacy % Responders
Gonçalves et al., 2014
Chronic lower back and/or lower limb
pain20 5 →80% responders (i.e., reduction of 50% or more
in pain intensity) in the active group 80%
Kim et al., 2013
Painful diabetic polyneuropathy
(PDPN)60 5
After 5th session:→20-50% reduction (from baseline) in pain scores →65% of participants reported ≥30% decrease)→Illness severity decreased (from baseline) 31.5%
→Pain reduced up to 4 weeks post-treatment
65%
Wrigley et al., 2013
Neuropathic pain due to
spinal cord injury 10 5 None 10%

Anodal tDCS of M1: Studies
2323© 2014 Nuraleve, Inc. Proprietary and Confidential.
Study Population SampleSize Sessions Efficacy %
Responders
DaSilva et al., 2012 Chronic migraine 13 10
From baseline to 4 months post-stimulation:→migraine intensity: from 4.6 to 2.9→length of migraine (hrs): from 8 to .9
From baseline to 30 days post-stimulation:→75% of patients saw moderate improvement with partial remission of symptoms
75%
Mendonca et al., 2011 Fibromyalgia 30 1 None N/A
Antal et al., 2010
Therapy-resistant chronic pain
syndrome12 5
After 5 sessions: →63% responders (i.e., reduction of 30% or more in pain intensity)
Decrease in pain intensity (change from baseline): →After 5th session: 33.5%→7 days post-study: 11%→14 days post-study: 28%→28 days post-study: 27%
63%

Anodal tDCS of M1: Studies
2424© 2014 Nuraleve, Inc. Proprietary and Confidential.
Study Population SampleSize Sessions Efficacy %
Responders
Valle et al., 2009
Fibromyalgia (women only) 41 10
Pain scores: values not given
Quality of life: →28% improvement
Not reported
Roizenblatt et al., 2007 Fibromyalgia 32 5
Pain scores:→59% decrease
Sleep measures:→decreased arousal: 35%→increased sleep efficacy: 12%
Not reported
Fregni et al., 2006a
Central pain after traumatic spinal
injury17 5
Pain scores:→After 5 sessions: 58% decrease→During follow-up (16 days post-treatment): 37%
5 sessions: 63%Follow-up: 36%
Fregni et al., 2006b Fibromyalgia 32 5
Quality of life scores:→"Pain" item: 49% improvement→Overall quality of life: 36% improvement
Not reported

tDCS & Chronic Pain: Considerations
25

Treatment Outcomes
Factors that affect treatment outcomes:
Age
Circadian rhythms
Resting brain states
Hormone levels
Underlying mechanisms of pain
Central sensitization
2626© 2014 Nuraleve, Inc. Proprietary and Confidential.

The Motor Cortex (M1)
The homunculus:
2727© 2014 Nuraleve, Inc. Proprietary and Confidential.

tDCS & Painrelief™
28

Painrelief™ Program
2929© 2014 Nuraleve, Inc. Proprietary and Confidential.
Chronic pain reduction program:
10 consecutive sessions
20 minutes each
2 mA

Painrelief™ System
3030© 2014 Nuraleve, Inc. Proprietary and Confidential.

Painrelief™ Accessories
Accessories you will use: Skin markers
Measuring tape
Alcohol swabs
Electrodes & lead wires
Sponges
Saline solution
Electrode prep container
Batteries and chargers
3131© 2014 Nuraleve, Inc. Proprietary and Confidential.

3232© 2014 Nuraleve, Inc. Proprietary and Confidential.
32
Determining electrode placement
International 10-20 System

Determining electrode placement
3333© 2014 Nuraleve, Inc. Proprietary and Confidential.
33
Cathode (right forehead)
Anode (left motor cortex)
Cathode (left forehead)
Anode (right motor cortex)
Pain on right side of body Anode: left M1 Cathode: right
forehead
Pain on left side of body Anode: right M1 Cathode: left
forehead
Pain on both sides of body
Anode: dominant hemisphere

1. Measure head midline from the nasion to the inion,
marking 10% (Fpz)
Determining electrode placement
3434© 2014 Nuraleve, Inc. Proprietary and Confidential.
34
10% Depression between eyes
Bump at back of head

Determining electrode placement
3535© 2014 Nuraleve, Inc. Proprietary and Confidential.
35
1. Measure head midline from the nasion to the inion, marking
10% (Fpz)
2. Align the cap so that the marked point is in the center of
the Fpz point.

Determining electrode placement
3636© 2014 Nuraleve, Inc. Proprietary and Confidential.
36
1. Measure head midline from the nasion to the inion,
marking 10% (Fpz)
2. Align the cap so that the marked point is in the center
of the Fpz point.
3. Mark the points C3/Fp1 (right
side pain) and C4/Fp2 (left
side pain) on the cap
Fp2Fp1
C4C3

Tips and Tricks
Hair: Split the hair around the target location. Pre-wet hair if necessary by rubbing the sponge in
the target location. Then, re-apply saline on sponge Use alcohol swab to remove marker dots from scalp
at end of session
Electrodes: Red electrode: middle should be at exact
location, with uniform pressure. Black electrode: the more contact area, the
merrier.
3737© 2014 Nuraleve, Inc. Proprietary and Confidential.

Tips and Tricks
WHAT YOU DON’T WANT:
Shifting of electrodes (especially red)
Shifting of electrode during initial installation at any point during the session
will result in stimulation of an incorrect brain region
Prevention:
Adjust electrode under cap as needed
3838© 2014 Nuraleve, Inc. Proprietary and Confidential.

Tips and Tricks
WHAT YOU DON’T WANT:
Dripping electrodes
If liquid leaks around the contact area, it may: Short the contact between electrodes (ineffective session) Change the area of contact between electrodes (modifies
effectiveness)
Too much or too little liquid affects the current density
Prevention:
Squeeze out excess saline before patient application3939© 2014 Nuraleve, Inc. Proprietary and Confidential.

Questions?
40© 2014 Nuraleve, Inc. Proprietary and Confidential.
1.888.792.7922 Ext. 103


















