BYPASS GRAFTING OPERATIONS USING CONVENTIONAL … · the anastomosis by purse - stringing it. ........
37
BYPASS GRAFTING OPERATIONS USING CONVENTIONAL TECHNIQUE WITH OFF-PUMP CORONARY ARTERY BYPASS GRAFTING IN TWO IDENTICAL GROUPS CONDUCTED AT THE PENANG HOSPITAL (1999-2000) BY DR. V ASANTHA KASINATHAN M .B. B.S. (MYSORE) Dissertation Submitted In Partial Fullfilment Of The Requirement For The Degree Of Master Of Medicine (General Surgery) , UNIVERSITI SAINS MALAYSIA YEAR 2001
Transcript of BYPASS GRAFTING OPERATIONS USING CONVENTIONAL … · the anastomosis by purse - stringing it. ........
BYPASS GRAFTING OPERATIONS USING CONVENTIONAL TECHNIQUE WITH OFF-PUMP
CORONARY ARTERY BYPASS GRAFTING IN TWO IDENTICAL GROUPS CONDUCTED AT THE
PENANG HOSPITAL (1999-2000)
BY
DR. V ASANTHA KASINATHAN
M.B.B.S. (MYSORE)
Dissertation Submitted In Partial Fullfilment Of The Requirement For The Degree Of Master Of Medicine (General Surgery) ,
UNIVERSITI SAINS MALAYSIA YEAR 2001

II SUPERVISORS
UNIVERSITI SAINS MALAYSIA
1. Dr Anas Sjahroeddin Ressang
Pakar Bedah Dan Pensyarah
J abatan Surgeri
Universiti Sains Malaysia
Kubang Kerian
Kelantan
2. Dr. Lin Naing
Pakar Statistics
J abatan Perubatan Masyarakat
Universiti Sains Malaysia
Kubang Kerian
Kelantan
MINISTRY OF HEALTH
1. Mr. Mohd. Hamzah KamaruIzamam Md (UKM), FReS (Edin)
Pakar Bedah Kardiothorasik
J abatan Pembedahan Kardiothorasik
Hospital Pulau Pinang
ii

III ACKNOWLEGEMENTS
I would like to express my thanks to Mr. Mohd Harnzah Bin Karnarulzarnan and Mr
Prashant Joshi for all their guidance and advice during my training in the Department of
Cardiothoracic surgery at Penang Hospital. They had suggested this topic for research and
it was subsequently presented at the Biannual Cardiothoracic Surgery Conferrence on
16th - 18th February 2001. I would also like to express a special thanks to Dr. Lin Naing
for being so helpful and guiding me with the statistical analysis of this study. I would like
to thank all the staff of the Cardiothoracic surgery clinic, CICU, Al ward, operation
theatre staff, record office staff and all my colleagues and friends for their co-operation
and valuable suggestions.
iii

IV TABLE OF CONTENTS
CONTENTS PAGE
I FRONTISPIECE ........................................................................................................... i
II SUPERVISORS ........................................................................................................... ii
m ACKNOWLEGEMENTS ........................................................................................... iii
IV TABLE OF CONTENTS ............................................................................................ iv
V LIST OF TABLES ...................................................................................................... vi
VI LIST OF FIGURES ................................................................................................... viii
VIT ABSTRACT IN BAHASA MALAYSIA .................................................................... x
VITI ABSTRACT IN ENGLISH ........................................................................................ xii
IX QUOTATIONS: ........................................................................................................ xiii
1 INTRODUCTION ........................................................................................................ 1
2 LITERATURE REVIEW ............................................................................................. 3
2.1 HISTORY ........................................................................................................ 3
2.2 ANATOMY ..................................................................................................... 7
2.3 INCIDENCE .................................................................................................. 11
2.4 INDICATIONS OF OFF-PUMP CABG ....................................................... 11
2.6 ADVERSE EFFECTS OF CPB CABG ......................................................... 12
2.6.1 Renal Failure ...................................................................................... 14
2.6.2 Cerebral Damage ................................................................................ 14
2.6.3 Hepatic Failure ................................................................................... 17
2.6.4 Hematological Disorders .................................................................... 17
2.6.5 Other Factors ...................................................................................... 19
2.7 INCIDENCE OF MAJOR POST-OPERATIVE COMPLICATIONS WITH AND WITHOUT CPB IN A STUDY DONE BY ENIO BUFFALO IN 1995 .......................................................................................................... 19
2.8 COST- EFFECTIVENESS ............................................................................ 20
3 OBJECTIVE OF STUDy .......................................................................................... 22
4 MATERIALS AND METHOD ................................................................................. 24
4.1 GENERAL DESCRIPTIONS ........................................................................ 24
4.1.1 Pre-operative preparation ................................................................... 25
4.1.2 Laboratory assessment ....................................................................... 26
4.1.3 Pre-operative checklist ....................................................................... 26
4. 1.4 Intra operative procedure ................................................................... 27
4.1.5 Post-operative monitoring at the coronary intensive care unit. .......... 38
iv

4.2 IN"CLUSION CRITERIA ............................................................................... 39
4.3 EXCLUSION CRITERIA .............................................................................. 39
4.4 STATISTICAL ANALYSIS .......................................................................... 40
4.5 NULL HYPOTHESIS (Ho) ............................................................................ 40
4.6 ALTERNATNE HYPOTHESIS (Hd ........................................................... 40
5 RESULTS .................................................................................................................. 41
5.1 Pre and post operative renal status ................................................................. 51
5.2 Renal profile ................................................................................................... 58
5.3 Duration of CICU stay ................................................................................... 60
5.4 Treatment with inotropes ............................................................................... 63
5.5 Gross neurological status ............................................................................... 67
5.6 Post operative bleeding .................................................................................. 69
5.7 Post operative blood transfusion .................................................................... 74
5.8 Post operative wound infection ...................................................................... 77
5.9 Post operative chest complications ................................................................ 82
5.10 Angina ............................................................................................................ 82
5.11 Pericardial effusion ........................................................................................ 86
5.12 Ejection fraction of the heart .......................................................................... 90
5.13 Preoperative risk factors ................................................................................. 95
6 DISCUSSION .......................................................................................................... III
7 CONCLUSION ........................................................................................................ 120
8 FUTlJRE TREND .................................................................................................... 121
9 LIMITATIONS, RECOMMENDATIONS AND SUGGESTIONS ........................ 124
10 REFERENCES ........................................................................................................ 126
11 APPENDICES ......................................................................................................... 139
11.1 Appendix I (Clinical findings related to coronary heart disease) ................. 139
11.2 Appendix IT (Clinical findings related to lung collapse) .............................. 140
11.3 Appendix ill (Risk factors of interest) ......................................................... 141
11.4 Appendix N (Definition of risk factors) ..................................................... 142
11.5 Appendix V (Radiological findings of pneumonia) ..................................... 148
11.6 Appendix VI (Radiological findings of lung collapse) ................................ 149
11.7 Appendix VII (Radiological findings of pleural effusion) ........................... 150
11.8 Appendix VIn (Coronary angiogram) .......................................................... 150
11.9 Appendix IX (A glossary of tenns used in the study) .................................. 151
11.10 Appendix X (Patients name and RIN, VC) . ................................................. 155
v

V LIST OF TABLES
Table 2.1 Incidence of major post-operative complications with and without CPB in a study done by Enio Buffalo in 1995 ............................................. 20
Table 2.2 Showing the cost of OPCAB and CPB CABG at Penang Hospital, Penang .......................................................................................................... 21
Table 5.1 Showing the age and sex distribution among the CPB and OPCAB CABG patients ............................................................................................. 42
Table 5.2 Showing the distribution of race, sex and age group among the CPB and OPCAB CABG patients ........................................................................ 43
Table 5.3 Shows the youngest and oldest patients in OPCAB and CPB CABG ......... 46
Table 5.4 Shows the mean age in the male (a) and female (b) patients in OPCAB and CPB CABG ............................................................................................ 47
Table 5.5 The univariate and multivariate analysis of OPCAB (50 cases) and CPB ( 50 cases) CABG operation performed the Cardiothoracic surgery unit at Penang Hospital, Penang ...................................................... 49
Table 5.6 Shows pre-operative serum creatinine level in OPCAB and CPB CABG patients ............................................................................................. 52
Table 5.7 Shows post operative serum creatinine level in CPB and OPCAB CABG patients ............................................................................................. 55
Table 5.8 Shows pre-operative renal failure in CPB and OPCAB CABG patients ......................................................................................................... 59
Table 5.9 Shows the extubation time in CPB and OPCAB CABG patients ............... 61
Table 5.1 0 The intra-operative use of inotrope in CPB and OPCAB CABG patients ......................................................................................................... 63
Table 5.11 Shows the age and sex distribution in pre-operative stroke in CPB and OPCAB CABG patients .............................................................................. 67
Table 5.12 Shows post-operative bleeding in CPB and OPCAB CABG patients ........ 70
Table 5.13 Shows the type of transfusion of blood products in the post-operative period in CPB and OPCAB CABG patients ............................................... 75
Table 5.14 Shows the incidence of sternal wound infection in CPB and OPCAB CABG patients ............................................................................................. 78
Table 5.15 Shows the incidence of leg wound infection in CPB and OPCAB CABG patients ............................................................................................. 80
Table 5.16 Shows a comparison of stable angina and unstable angina in pre-operative CPB and OPCAB CABG patients ................................................ 83
Table 5.17 Shows the pre-operative pericardial effusion in CPB and OPCAB CABO patients ............................................................................................. 86
vi

Table 5.18 Shows the post-operative pericardial effusion in CPB and OPCAB CABG patients ............................................................................................. 88
Table 5.19 Shows the pre-operative ejection fraction of the heart in CPB and OPCAB CABG patients ............................................................................... 91
Table 5.20 Shows the pre-operative incidence of smoking in CPB and OPCAB CABG patients ............................................................................................. 96
Table 5.21 Shows the comparison of pre-operative risk of family history of heart disease in CPB and OPCAB CABG patients ............................................... 99
Table 5.22 Shows the comparison of pre-operative risk of diabetes mellitus in CPB and OPCAB CABG patients .............................................................. 1 01
Table 5.23 Shows the pre-operative risk factor of hypercholesterolemia in CPB and OPCAB CABG patients ...................................................................... 1 05
Table 5.24 Shows the pre-operative risk factor of hypertension in CPB and OPCAB CABG patients ............................................................................. 107
Table 5.25 Shows the pre-operative incidence of chronic obstructive airway disease (COAD) in CPB and OPCAB CABG patients .............................. 109
vii

VI LIST OF FIGURES
Figure 2.1
Figure 2.2
Figure 2.3
Figure 4.1
Figure 4.2
Figure 4.3
Figure 4.4
Figure 4.5
Figure 4.6
Figure 4.7
Figure 5.1
Figure 5.2
Figure 5.3
Figure 5.4
Figure 5.5
Figure 5.6
Figure 5.7
Figure 5.8
Figure 5.9
Diagram A ...................................................................................................... 8
Diagram B .................................................................................................... 10
Pathophysiology of pump syndrome ............................................................ 13
Shows the removal of the long saphenous vein from the leg ....................... 28
Shows the incision being enlarged with a pair of fine scissors ................... .32
The reversed scissors are helpful to enlarge the incision in the other direction ........................................................................................................ 33
Graduated probes can be passed into the artery to measure the internal diameter, which in this case is 2 mm. The probes are also useful in detecting narrowings in the vessel and distal artery ..................................... 34
Two further bites of this continuous suture are inserted before sliding the vein down into position .......................................................................... 35
Once the continuous suture has been inserted, the knot is tied and the suture is cut. In using Prolene , which is designed to pull through very easily, care must be taken not to tie the knot too tight and thus narrow the anastomosis by purse - stringing it. ........................................................ 36
Just before closing the chest, the grafts to the right and left anterior descending coronary arteries are checked to ensure that there is no leak from the anastomoses ................................................................................... 3 7
Shows the race distribution of patients who had undergone CPB CABG ........................................................................................................... 44
Shows the distribution of race in OPCAB CABG ....................................... 45
The pre-operative levels of serum creatinine in CPB and OPCAB CABG patients ............................................................................................. 54
The post operative levels of serum creatinine in CPB and OPCAB CABG patients ............................................................................................. 57
Shows the extubation time in OPCAB CABG and CPB CABG patients ......................................................................................................... 62
Shows the age, sex distribution and the incidence of inotropes use in CPB and OPCAB CABG patients ................................................................ 64
Shows the age distribution and the incidence of inotrope use in female CPB and OPCAB CABG patients ................................................................ 65
Shows the age distribution and the incidence of inotrope use in male CPB and OPCAB CABG patients ................................................................ 66
Shows the age and sex distribution of post-operative stroke in CPB and OPCAB CABG patients ........................................................................ 68
viii

Figure 5.10 A comparison of post operative bleeding in CPB and OPCAB CABG male patients ................................................................................................. 72
Figure 5.11 A comparison of post operative bleeding in CPB and OPCAB CABG female patients .............................................................................................. 73
Figure 5.12 Shows the types of blood products tranfused in the CPB and OPCAB CABG patients ............................................................................................. 76
Figure 5.13 Shows the incidence sternal wound infection in CPB and OPCAB CABG patients ............................................................................................. 79
Figure 5.14 Shows the incidence of post operative leg wound infection in CPB and OPCAB CABG patients .............................................................................. 81
Figure 5.15 Shows the incidence of stable angina in CPB and OPCAB CABG patients ......................................................................................................... 84
Figure 5.16 Shows the incidence of unstable angina in CPB and OPCAB CABG patients ......................................................................................................... 85
Figure 5.17 Shows the incidence of pre-operative pericardial effusion in CPB and OPCAB CABG patients ............................................................................... 87
Figure 5.18 Shows the incidence of post-operative pericardial effusion in CPB and OPCAB CABG patients ............................................................................... 89
Figure 5.19 Shows the incidence of pre-operative ejection fraction in CPB and OPCAB CABG patients ............................................................................... 93
Figure 5.20 Shows the incidence of post operative ejection fraction in CPB and OPCAB CABG patients ............................................................................... 94
Figure 5.21 A comparison of smoking in CPB and OPCAB CABG patients ................. 97
Figure 5.22 A comparison of smoking in CPB and OPCAB CABG patients ................. 98
Figure 5.23 Shows the incidence of family history of heart disease in CPB and OPCAB CABG patients ............................................................................. 100
Figure 5.24 A comparison of the pre-operative risk factor of diabetes mellitus in CPB and OPCAB CABG patients .............................................................. 102
Figure 5.25 A comparison of diabetes mellitus in CPB and OPCAB CABG patients with respect tho the different age group ....................................... .1 03
Figure 5.26 A comparison of the pre-operative risk factor of hypercholesterolemia in CPB and OPCAB CABG patients .......................................................... 106
Figure 5.27 A comparison of pre-operative risk factor of hypertension in CPB and OPCAB CABG patients ............................................................................. 1 08
Figure 5.28 Shows the incidence of chronic obstructive airway disease (COAD) in CPB and OPCAB CABG patients .............................................................. 110
Figure 6.1 Shows the Medtronic (Inc) Tm Octopus II Tissue Stabilizer which is utilized in OPCAB CABG ......................................................................... 112
Figure 6.2 Shows an earlier model of the tissue stabilizer used in OPCAB CABG ... 113
Figure 6.3 Showing a second type of tissue stabilizer ................................................. 114
ix
ABSTRACT IN BAHASA MALAYSIA
Ini adalah suatu kajian prospektif yang telah dikendalikan di Jabatan Pembedahan
Kardiotorasik, Hospital Penang, Pulau Pinang, melibatkan sebanyak seratus orang,
sepanjang setahun daripada bulan Januari 1999 ke Januari 2000. Lima puluh pesakit telah
menjalani pembedahan secara "off-pump" (OPCAB), yang telah dibandingkan dengan
lima puluh pesakit lain yang telah menjalani pembedahan secara "on-pump" (CPB)
dengan alat "heart-lung machine". Pesakit yang sedang menghadapi penyakit seperti sakit
buah pinggang, penyakit lumpuh, penyakit lelah, dan serangan sakit jantung bam-bam ini
telah diasingkan dan di beri rawatan secara pembedahan "off-pump (OPCAB)".
Pesakit di dalarn kumpulan ini telah mengalarni masalah yang sarna; seperti sakit jantung,
kekurangan daya upaya semasa berkerja, iaitu NYHA kelas II, ill dan N. Sebelum
menjalani pembedahan, pesakit-pesakit yang didapati mengidap sakit kencing manis,
darah tinggi, darah berlemak tinggi, merokok dan yang mempunyai penyakit yang sarna di
kalangan ahli keluarga dari kedua-dua golongan telah di teliti. Pemeriksaan yang sarna,
sehelum pembedahan, telah dilakukan di kedua-dua kumpulan pesakit. X -ray dada,
pemeriksaan ECG, Echocardiography, angiogram telah dilakukan untuk seratus pesakit
1n1. Pendarahan semasa dan selepas pembedahan, keadaan huah pinggang,
Echocardiography, ECG dan X-ray dada telah dibandingkan. Perbelanjaan diantara
OPCAB dan CPB pembedahan telah dibandingkan. Kajian telah menunjukkan bahawa
x

pesakit yang telah menjalani pembedahan jantung secara "off-pump" (OPCAB) telah
menerima faedah yang lebih baik daripada pesakit yang telah menjalani pembedahan
secara CPB. Ini menunjukkan bahawa lebih banyak lagi pembedahan akan dilakukan
secara OPCAB pada masa yang akan datang.
xi

ABSTRACT IN ENGLISH
This is a prospective study conducted at the Department of Cardiothoracic Surgery,
Penang Hospital, Penang, with a total of one hundred patients were studied over a period
of one year between January 1999 to January 2000. Fifty patients who had undergone
coronary artery bypass surgery off-pump (OPCAB) were compared with fifty patients who
had undergone coronary artery bypass surgery on the heart-lung machine (CPB). Patients
who had associated problems of renal failure, stroke, bronchial asthma and recent
myocardial infarction were included in the off-pump CABG surgery. The symptoms did
not differ in both the groups. They had experienced angina, decreased effort tolerance,
palpitations, with NYHA class IT, ill and IV. The predisposing factors of diabetes
mellitus, hypertension, hyperlipidemia, smoking, previous family history of heart disease
were studied in both these groups. The same pre-operative investigations were performed
in both groups of patients. Chest x-ray, ECG, echocardiography, femoral angiogram were
done for these one hundred patients. The intra-and post operative bleeding, pre and post
operative renal status, echocardiogram, ECG and chest X-rays were compared. The cost
effectiveness of both the OPCAB and CPB procedures were reviewed. There was,
generally, a better outcome in patients who had undergone a coronary bypass by the off
pump (OPCAB) method as when compared to those by the CPB method. This indicates
that more cases can be done by the OPCAB method in the future.
xii

Quotations:
"Its pretty easy to go upstairs and point at the patients that have been on
pump and the patients that have been off pump"
- James C. Hart, M.D.
" The patients respond to beating heart Cabg so much better and are
extubated within 2-6 hours"
- David Perkowski,M.D.
" I saw my two post - op patients today in the unit. Both were awake ,
smiling, no bleeding, no strokes, sitting up, and delined. As they sat up,
swung their legs over the side of the bed, and begged me to listen to how
good their lungs sounded, they told me how appreciative they were. I
could not think of another time EVER that an on-pump patient had EVER
looked this good this quickly"
- Michael D, Moran M.D , Cardiologist
xiii

1 INTRODUCTION
Suitable techniques for cardiopulmonary by-pass has in the last 15 years become a
realistic standard procedure. The pump oxygenator taking over the function of the lungs,
permits operation on intracardiac defects as it provides a quiet, peaceful heart and a clear
view of the heart unobscured by blood. This procedure is not without its complications
and hence has led to the alternative method of CABG operations using off-pump
technique and minimally invasive procedures. Originally, only short periods of CPB was
feasible but now up to 6 hours are possible. Nevertheless, there are several grave
complications associated with on-pump CABG. This has lead to the resurgence of the off
pUl!lP technique in several centers. Everyday, all over the world, approximately 2000 off
pump operations are being performed. New fields are being explored, such as prolonged
partial bypass, to assist the action of the heart in episodes of acute heart failure. Video
assisted minimally invasive coronary operations without cardiopulmonary bypass is
indeed going to be the mainstay of management in the near future. A multicenter study
from the Benetti Foundation in Argentina was carried out by Frederico et al in 1994. The
aim of this study was to avoid the risks associated with CPB. It has led to the interest in
off-pump CABG. The incision used was through a small anterior thoracotomy. The
results showed that this method is a new promising technique that can be considered an
alternative to most angioplasty and complementary to the conventional CABG operations
[Frederico et all. The main issues in "beating heart" coronary operations are the reduced
medical costs and the avoidance of the CPB associated risks. There is a dramatic decrease
in costs due to both the decrease of disposable materials and to the reduction in total

hospital stay and intensive care stay. Frederico et al proved this in their study with zero
morbidity level for non cardiac complications and to a faster recovery post-operatively. A
few of our cases needed to be on PTCA right from the pre-operative stage of
management. Studies have shown that the outcome is favourable even for these patients if
the CABG is done off-pump. This study also emphasises the advantages of a combined
right and left small thoracotomies. 'Off pump' CABG operations have led surgeons to
learn the use of tissue stabilising techniques to stabilize the target vessels on the
epicardium. A stable myocardial function is maintained, ensuring adequate total body
perfusion. The use of Medtronic Octopus Tissue Stabilising System (OTS) allows for
improved exposure, with minimal hemodynamic compromise. It enables the surgeon to do
multi-vessel 'off-pump' (OPCAB) CABG [1. Hart et aI, 1997]. The economic outcome of
'off-pump' (OPCAB) CABG has led to the revival of this technique [Asci one et aI, 1999].
2

2 LITERA TURE REVIEW
2.1 History
• Early 20th century: Lehrbuch der Chirurgie, edited by Wullstein and Wilms,
contained a short chapter describing heart wounds.
• 1910: Alexis Carrel: performed the 1 st experimental coronary artery procedure
(shunt between the descending aorta and coronary artery using a free carotid
artery graft).
• Nevertheless, full-fledged experimental studies directed to the clinical use of
coronary artery bypass grafting did not appear until the middle of that century.
• Early experiments: In 1940, Murray developed a number of direct suture
anatomosis of systemic arteries including the internal mammary artery to the
coronary artery involving a free arterial graft.
• 1956-1965: experiments aimed at solving the immediate problems, and to
protect against jeopardizing the coronary circulation were dealt with. These
studies first used blood perfusion or autoperfusion to prevent cardiac
fibrillation. Then, the study moved on to cardiopulmonary bypass and
cardioplegia method to achieve a motionless arterial target for the suturing
process.
• 1953: V.P. Demikhov in Moscow, used LIMA to LAD graft by means of a
cannula on the beating heart of a dog.
3

• 1965: Amosova Sinyakin demonstrated suturing techniques with automatic
suturing instruments (circular vessel suturing apparatus called VCA-4 or
ASC-4) in experimental dogs.
• During the mid 1950s, Prof. Vasili I. Kolesov started work on coronary
revascularization for the treatment of heart disease (ligation of both internal
mammary arteries, in the hope of increasing collateral flow to the mediastinal
coronary arteries). This was called the Fieschi operation. Next he used the
tunneling of bleeding internal mammary arteries to the L ventricular wall.
This was called the Vineberg procedure.
• 1950s: W.Longmire was one of the pioneers of coronary bypass surgery. He
had to perform a couple of earliest internal mammary artery to coronary
anastomosis during a thrombo-endarterectomy. It later proved to be a good
operation.
• 1961: Goetz and colleagues conducted experiments with non sutured
mammary artery anastomosis Goining of the internal mammary artery to the R
coronary artery on the beating heart by means of a tantalum ring. It took 17
minutes. Catheterization was done 2 weeks after the surgery and it confirmed
the patency of the anastomoses.
• 1964: Prof. Kolesov introduced direct suturing between the internal mammary
artery and coronary arteries (done in 1964).
• 1965: Khan and colleagues showed the use of vascular staplers for
anastomosis in calf. Further work was delayed until recent renewed efforts by
Tulleken and colleagues, Nataf and colleagues and others.
4

• 1966: Prof. Kolesov used the gastroepiploic artery for the Vineberg
procedure, retrograde (1966) and bilateral internal mammary artery
anastomosis (1969) and the use of abdominal artery grafting on experimental
basis. He pioneered the use of internal mammary artery to coronary artery
anastomosis for the treatment of acute myocardial infarction and pre
infarction conditions. He retired in 1976, his research group carried on with
his work. He died in 1992.
• 1973: Garrett et al used the saphenous vein graft to perform CABG on a
beating heart.
• Despite the widespread use of CPB bypass, Prof. Kolesov prefered to avoid
CPB or to simplify it. He advocated that for ill patients, on-pump bypass must
be avoided as it is a heavy burden for the patients heart.
• 1975: Trapp and Bisarya and Anekey reported successful cases operated by
the off-pump method.
• 1982: Benetti et al (Argentina, South America) pioneered the off-pump
CABG Lower morbidity, mortality and reduced costs were reported. This was
particularly true of high -risk patients. Similar findings were reported by
several other centres.
• *Minimally invasive direct coronary artery grafting was demonstrated by
Subrmaniam, Robinson et aI, Califiore et aI, Janssen, Vim et al.
• Mack and Nataf introduced the video-assisted cardiac surgery. They showed
how this method greatly reduced the invasiveness of the procedure and they
developed it further. Despite the initial uncertainty, the quality of the
anastomosis and the benefits of the procedure, this off-pump direct
5

visualization has received increasing acceptance. The advent of mlnl
thoracotomy, done off-pump, on a beating heart where LIMA is anastomosed
to the LAD as originally proposed by Benetti and popularised by Califiore et
al represented an important development in coronary surgery in recent years.
This is limited to patients with single LAD lesions.
• Recent progress: Development of myocardial tissue stabilizers, flow
occluders, etc, video-assisted dissection of LIMA have been developed.
• The use of robotics have emerged to expand these teclmiques and complete
the thoracoscopic coronary surgery. The develpoment of coronary artery
surgery spans practically throughout the entire 20th century with intervals
between the breakthroughs becoming progressively shorter. However, there
was a distressing gap between the origination and the acceptance of ideas
regarding less invasive coronary artery surgery.
• Under research now: The MIDCAB operation performing LIMA to LAD
anastomosis by percutaneous angioplasty or other methods to provide
effective myocardial revascularization via a non-invasive approach and at a
lower cost.
6
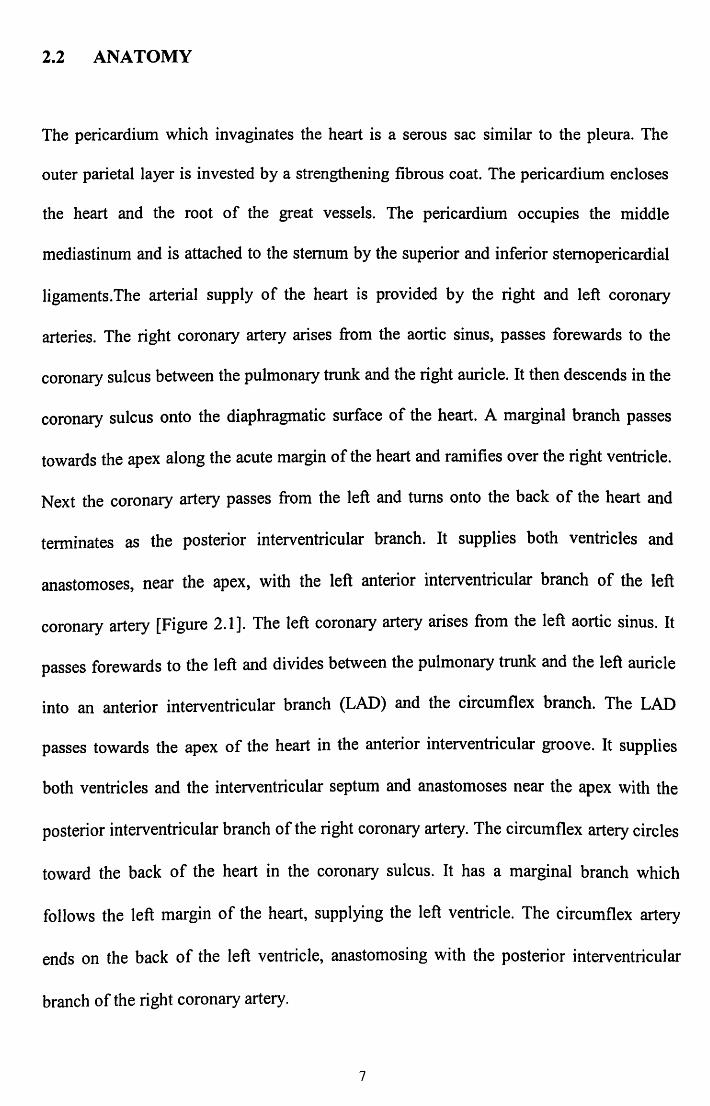
2.2 ANATOMY
The pericardium which invaginates the heart is a serous sac similar to the pleura. The
outer parietal layer is invested by a strengthening fibrous coat. The pericardium encloses
the heart and the root of the great vessels. The pericardium occupies the middle
mediastinum and is attached to the sternum by the superior and inferior sternopericardial
ligaments.The arterial supply of the heart is provided by the right and left coronary
arteries. The right coronary artery arises from the aortic sinus, passes forewards to the
coronary sulcus between the pulmonary trunk and the right auricle. It then descends in the
coronary sulcus onto the diaphragmatic surface of the heart. A marginal branch passes
towards the apex along the acute margin of the heart and ramifies over the right ventricle.
Next the coronary artery passes from the left and turns onto the back of the heart and
terminates as the posterior interventricular branch. It supplies both ventricles and
anastomoses, near the apex, with the left anterior interventricular branch of the left
coronary artery [Figure 2.1]. The left coronary artery arises from the left aortic sinus. It
passes forewards to the left and divides between the pUlmonary trunk and the left auricle
into an anterior interventricular branch (LAD) and the circumflex branch. The LAD
passes towards the apex of the heart in the anterior interventricular groove. It supplies
both ventricles and the interventricular septum and anastomoses near the apex with the
posterior interventricular branch of the right coronary artery. The circumflex artery circles
toward the back of the heart in the coronary sulcus. It has a marginal branch which
follows the left margin of the heart, supplying the left ventricle. The circumflex artery
ends on the back of the left ventricle, anastomosing with the posterior interventricular
branch of the right coronary artery.
7

Diagram A 1. Left main. 2. Left anterior descending (LAD) . 3 . Diagonal. 4. Circumflex . 5. Obtuse marginal. 6. Right. 7 . Right ventricular branch. 8 . Acute marginal branch . 9 . Posterior interventricular.
Figure 2.1 Diagram A
8

A posterior artery of the left ventricle frequently swings down the back of the left
ventricle near the tennination of the circumflex, matching the distribution of the posterior
vein of the left ventricle. The branch supplying the SA node arises from the right coronary
artery in 54% of cases, distal to its conal branch. It supplies the deep aspect of the right
atrium, circles the base of the superior vena cava and ends in the SA node at the cephalic
end of the sulcus terminalis.
An intermediate artery arises from the right coronary artery nearly opposite its right
marginal branch and ascends over the right atrial surface. An anastomotic atrial branch
arises from the circumflex artery near its origin and passes towards the right, towards the
internal surface of the left atrium. It may anastomose with the terminals of the right
sinuatrial artery and is usually involved in the variant cases in which the sinuatrial artery
is a left coronary branch. The circumflex also gives rise to an intermediate atrial branch
which distributes along the left atrium above the coronary sulcus. The A V node artery
arises from the right coronary artery opposite the origin of the posterior interventricular
artery (85%) and penetrates deeply to the AV node (LAD) and posterior interventricular
arteries. Of these, those from the LAD pass two-thirds of the way into the septum, those
from the posterior interventricular arteries pass one third of the way into the septum. The
terminal anastomoses between the arteries are usually small and require enlargement for
survival in case of occlusion of any of the larger branches of the coronary arteries.
Interference with the coronary circulation results in ischemia and pain (angina pectoris) or
a varying amount of pennanent damage to the myocardium. A small area of damage
usually allows recovery by connective tissue replacement in the infracted area, but
massive damage is likely to be fatal. The coronary artery bypass surgery in which the
venous autografts are inserted to bridge the affected areas, has saved many lives. The
three most common locations of coronary occlusion, in descending order of frequency, are
proximally in the LAD, proximally in the right coronary artery and proximally in the
circumflex artery. The veins, for most part of the heart, follow the arteries [Fig 2.2].
9
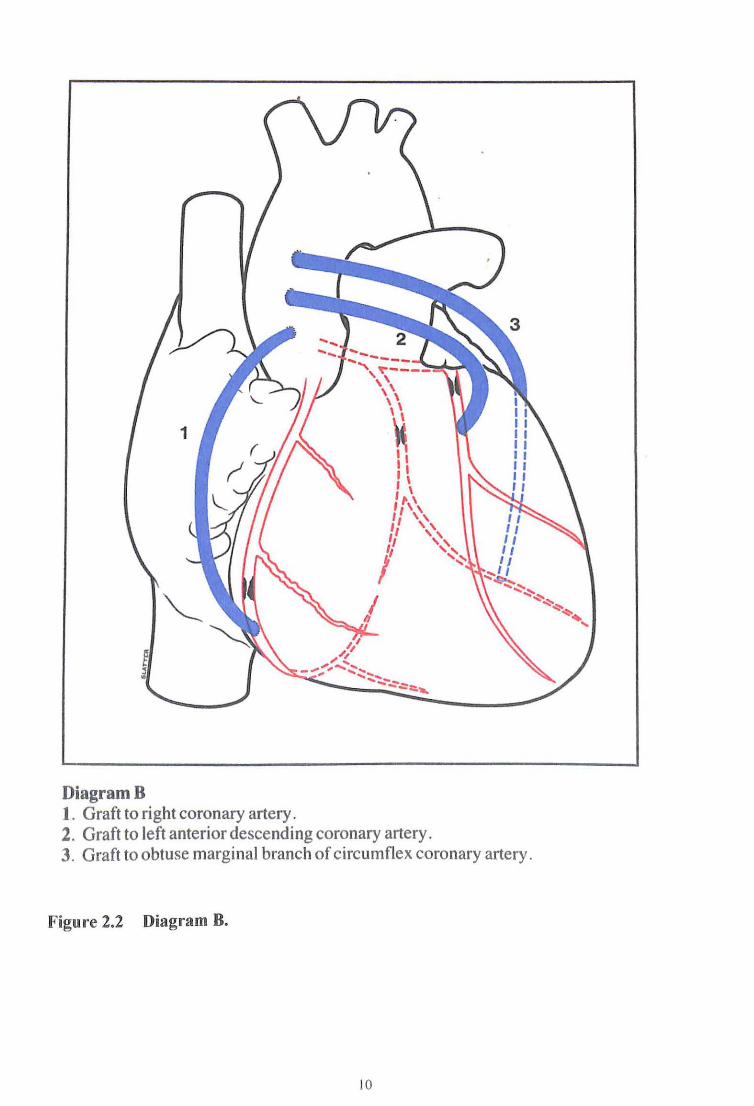
DiagramB 1. Graft to right coronary artery . 2. Graft to left anterior descending coronary artery. 3. Graft to obtuse marginal branch of circumflex coronary artery.
Figure 2.2 Diagram B.
10

2.3 INCIDENCE
The incidence of coronary artery disease is more in males than in women but the odds are
equal in both sexes in the post-menopausal women and men of the same age.
2.4 INDICATIONS OF OFF·PUMP CABG
The following are the indications for performing an off-pump CABG:
• Coronary artery disease
• Severely calcified aorta, especially the ascending aorta
• Renal disease, renal insufficiency
• Pulmonary disease, emphysema
• Previous stroke, cerebrovascular accident
• Diffuse peripheral vascular disease
• elderly patients
• Poor ventricular function
• Re-operations
• Jehovah's witness religious group (refuse blood transfusion based on religious
beliefs)
11

2.5 CONTRAINDICATIONS OF OFF-PUMP CABG
There are several contraindications to off-pump CABG and these are as follows:
• Deep intramyocardial vessels
• Small distal targets
• Hemodynamic instability due to cardiac manipulation or ischaemic precondition
• Acute myocardial infarction with cardiogenic shock
2.6 ADVERSE EFFECTS OF CPB CABG
On-pump CABG (CPB), has several adverse effects affecting mUltiple organs. The
pathophysiology of this "pump syndrome" is illustrated in Fig. 2.3 below.
12

CPB
~ (controlled shock)
~ Inflammatory reaction
~ Activation ofC', Kallikrein, kinnins, Tumor necrosis
~ factor, alpha systems
~ Alters coagulation functions
~ vasoplegic syndrome
~ Increased capill~ permeability
~ Sequestration of neutrophils
~ MICROEMBOLI
~ (to brain, kidneys, lungs, liver etc)
Figure 2.3 Pathophysiology of pump syndrome.
13
2.6.1 Renal Failure
After CPB CABG, renal failure is usually due to acute tubular necrosis. This is due to
renal vasoconstriction. The exact local mechanism is not understood as yet. It is believed
to be due to a physiological shunt which diverts blood from the artery to the vein, thereby
depriving the renal tissue of its blood supply. Acute tubular necrosis can occur in the
event of a brief hypotensive episode intraoperatively. Other mechanisms may be involved
including the intravascular (glomerular) thrombosis, tubular obstruction and the renin
angiotensin system. Incompatible blood transfusion damage in the extracorporeal
apparatus, long perfusions, septicaemia, hypoxia and acidosis have also been implicated
in the etiology of renal failure in CPB CABG. The plasma haemoglobin released by red
cell trauma after CPB operations can pass through the kidney and appear in the urine
without any sign of renal disturbance. Renal embolism with clot, air or airfoam is a rare
cause of renal failure. The acute tubular necrosis usually causes oliguria (less than 400
ml/day). Anuria is rare in acute tubular necrosis and if present, it suggests the presence of
bilateral renal embolism or bladder neck obstruction due to an associated prostatic
hyperplasia. Renal failure can occur without oliguria, as seen in non-oliguric renal failure
in valve replacement done on CPB.
2.6.2 Cerebral Damage
Cerebral damage after CPB CABG is due to embolism and cerebral ischemia. eNS
complications due to cerebral embolisation occurs at the time of decannulation, aortic
clamping and declamping. A common complication is the development of a stroke.
14

Intracranial hemorrhage, hypothermia, metabolic derrangements can also contribute to
cerebral disturbances after CPB CABG. It is manifested as psychiatric disorder or present
with post-operative neurological signs which may be so severe as to result in coma and
death. Embolism may be due to air trapped within the left side of the heart after open
heart surgery. The nitrogen content of air is absorbed slowly. Thus air embolism is more
dangerous than oxygen or carbon dioxide embolism. This can occur if frothing occurs in
the oxygenator or if cold blood comes into contact with warm tissues. De-airing of the
grafts and the chambers of the heart is very important at the end of the anastomosis of the
grafts.
The presence of a preoperative mitral valve lesion will predispose the patient to the risk of
developing a cerebral thrombo-embolism from the left atrium and appendage. Left
ventricular aneurysms often contain clots which can embolise. Thrombosis along the left
atrial suture lines and prosthetic valves is another cause of post-operative thrombo
embolism. Fat embolism can occur due to the release of fat globules from the pericardium
after median sternotomy incisions or due to trauma to mediastinal fat by suction injury of
the coronary aspirators into the extracorporeal equipment. Fibrin embolism has been
shown to be common with certain oxygenators resulting in diffuse brain damage.
Occasionally, foreign materials such as sutures, patches can reach the brain as emboli.
Cerebral ischemia can cause severe cerebral damage. The ischemic event could manifest
are noted in hypoglycemia, diabetic coma, gross electrolyte imbalance or a very low pH.
Drugs added due to a very low intraoperative cardiac output, a low flow from the pump
oxygenator. This can also result from using pure oxygen in the pump oxygenator leading
to a low arterial carbon dioxide tension. It is also seen if the patient is hyperventilated
intraopeartively. Cerebral anoxia develops faulty oxygenation techniques by the
15

anaesthetist, with large left to right shunts, pulmonary complications and ventilatory
inadequacies result in cerebral damage. Other causes of cerebral damage in CPB CABG is
due to raised intracranial pressures from subdural hemorrhage, hypertensive crisis,
cerebral dehydration with hypertonic solutions and with obstruction to one jugular vein. In
this instance, the venous cross communications cannot be relied upon to overcome the
resultant raised intracranial pressure. Profound hypothermia can cause cerebral damage
due to ischemia rather than from direct damage from hypothermia. Cerebral symptoms
may be seen due to metabolic disturbances but it is rare. Mental and neurological changes
can occur due to the pump oxygenator. The psychological disturbances are of various
degrees ranging from slight disorientation to frank psychoses. Treatment postoperatively
at the CICU can bring about a fear of impending death with its unsureal atmosphere. They
can have a lack of sleep, anxiety fragmented speech and use the wrong words while
attempting to talk. Hallucinations occur when the cardiac output improves. Patients can
also experience disorders of conciousness, unequal pupils, hemiparesis, convulsions,
hyperpyrexia, hyperreflexia and extensor responses. Slowing pulse, spreading hemi
paresis or hemi-sensory loss could point to the evolvement of cerebral oedema. An
associated papilloedema will definitely indicate a CT scan of the brain with further
neurological assessment. The pathology of cerebral damage is due to changes brought
about by ischemia and anoxia. It consists of diffuse neuronal loss in the cerebral cortex
with less changes in the medulla. Cerebral odema mayor may not be present. Clot and
calcium embolism may cause cerebral infarcts. Diffuse local areas of cerebral damage
may be seen due to air or fibrin embolism.
16

2.6.3 Hepatic Failure
Jaundice may occur after cardiac surgery for vanous reasons. Older patients with
pulmonary hypertension and myocardial insufficiency are likely to develop hepatic
failure. Hepatic function could be depressed during and after the surgery. Anaesthesia,
especially halothane, hypothermia, a low flow with poor tissue perfusion from the pump
oxygenator and raised plasma hemoglobin aggravate these effects. The kidneys will also
suffer from a reduced renal blood flow. Thus renal and hepatic failure can occur
simultaneously.
Post-operatively a low cardiac output with a high venous pressure may worsen hepatic
damage. Drugs and sepsis also playa role. Transfusion viral hepatitis may occur after
cardiac surgery with an incubation period of 14-100 days. Cytomegalovirus hepatitis may
also occur.
2.6.4 Hematological Disorders
Blood damage in extracorporeal circulation is of a complex nature and causes accelerated
destruction of red blood cells in the post-perfusion period. Hemoglobin levels can fall to
as low as 3-5 gmJdL.Subacute bacterial endocarditis or protracted low grade infection
may cause anemia. Gastrointestinal bleeding may occur from anticoagulant therapy and
result in anemia. Post operatively, despite good drainage variable amount of blood lies in
the chest cavity. Post operative chest X-ray will show a widening of the mediastinum.
Intravascular hemolysis will occur due to artificial materials used in CPB. A patient with
17

sickle cell disorder will do well with off-pump CABG with a preoperative spleenectomy
before the CABG. The amount of blood to be transfused (packed cells) is calculated with
the following formula:
Vol. of blood = 3.5 X (Desired level of Hb - Actual Hb level) X body weight
Failure of the hemostatic mechanism after CPB is a major problem requiring chest
reopening. The circulating heparin may not have been neutralised well with protamine.
Recrudescence of heparin activity after effective neutralization can occur. It is called
heparin rebound phenomenon. The cause is unknown. Heparinised blood returns into
circulation from stagnant peripheral vessels or to fibrinolytic degradation of the heparin
protamine complex. An increase thrombin time due to a decrease in levels, allows heparin
to reappear. Excessive dose of protamine prolongs coagulation, but fortunately this rare.
Qualitative platelet defects are seen when platelets are exposed to the CPB circuit with
alpha- granule release. Alteration of platelet membrane receptors occurs. The degree of
platelet dysfunction co-relates with the duration of CPB and the degree of hypothermia
after bypass. Hemodilution on CPB and consumption in extracorporeal circuit will
decrease platelet count by 30%-50%. The thrombocytopenia worsens as the CPB time
increases. These are the quantitative platelet defects. A transient fall in the platelet count
to 30% is noted on giving protamine. CPB lowers most of the coagulation factors by 50%,
especially factor V by 80%. Hemodilution is more pronounced if patients have a small
blood volume. The use of intra-operative cell-savers will eliminate clotting factors.
Fibrinolysis occurs due to activation of the plasminogen during CPB.
18

2.6.5 Other Factors
CPB predisposes to the development of paradoxical septal wall motions of the cardiac
musculature. There is an increased rate of morbidity and mortality .It involves increased
utilization of resources. There is an increased incidence of reopening of the chest for
blood loss and bleeding. The post-operative stay is prolonged as when compared to the
off-pump CABG. Peri-operative incidence of myocardial infarct is more with CPB.
2.7 INCIDENCE OF MAJOR POST-OPERATIVE COMPLICATIONS WITH AND WITHOUT CPB IN A STUDY DONE BY ENIO BUFFALO IN 1995.
The above study conducted by Enio Buffalo et al has established that complications of
CABG with CPB is more than with off-pump CABG (Table 2.1). Patients benefit from an
off-pump CABG. A similar study was done by the cardiothoracic teams of three hospitals
in the USA i.e. Allegheny University HospitaV Medical College of Pennsylvania,
Harrisburg Hospital and Park Nicolet CliniclHealth System Minnesota. They had similar
results showing that off-pump CABG had many advantages over the CPB CABG.
19

Table 2.1 Incidence of major post-operative complications with and without CPB in a study done by Enio Buffalo in 1995.
Complication With CPB WithoutCPB (509 cases) (200 cases)
Perioperative MI 18 (3.5%) 2 (1%)
Arrythmias 25 (5.6%) 5 (2.5%)
eVA 3 (0.6%) 0(0%)
Acute renal failure 8 (5.1%) 0(0%)
GIT bleed 7 (1.4%) 2 (1%)
Excessive bleeding 16 (3.0%) 3 (1.5%)
Prolonged intubation 40 (7.8%) 9 (4.5%)
Vasoplegic syndrome 10 (2.1 %) 2 (1%)
Total 127 (24.90/0) 23 (11.50/0)
2.8 COST - EFFECTIVENESS
Costs are reduced when CABG is performed by the off-pump method. CPB patients
require a prolonged CleU stay, and general ward stay post operatively due to all the
above mentioned complications. With CPB, time spent in the hospital is reduced, with
fewer post operative complications. Thus more number of patients can be treated by the
off-pump technique using the available resources. It also decreases the waiting list for
coronary surgery. The estimated cost of coronary artery bypass operation at the
Cardiothoracic Surgery Unit at Penang Hospital is as follows (Table 2.2):
20

Table 2.2 Showing the cost of OPCAB and CPB CABG at Penang Hospital, Penang.
Type of operation Off-pump (OPCAB) CPB
Cost (in ringgit Malaysian) RM3,200.00 RM 4,864.00
The cost of utilizing the extracorporeal equipment alone being RM2064.00.
21
3 OBJECTIVE OF STUDY
1. The primary aim of this study is to assess the usefulness of the off-pump coronary
artery bypass surgery for elective patients with coronary artery disease.
2. The secondary aim is to assess the following parameters in these patients:
a) Morbidity
1. Infection
11. Ventilation time
iii. Cost effectiveness
b) Mortality
c) Peri-operative infarcts based on ECG findings
d) Clinical outcome
1. Renal status pre and post operatively (assessed with serum creatinine)
11. Duration of CICU stay ( assessed with time of extubation)
iii. Treatment with inotroph
IV. Gross neurological status
v. Post operative bleeding
VI. Post operative blood transfusion
V11. Post operative wound infection of the chest and the leg.
VIlt. Post operative lung complications
IX. Angina
22

x. Pericardia! effusion
Xl. Ejection fraction
xu. Pre-operative risk factors
xiii. Incidence of wound infection
23
4 MATERIALS AND METHOD
4.1 GENERAL DESCRIPTIONS
Suitable techniques for cardiopulmonary bypass has in the last fifteen years become a
realistic standard procedure. The pump oxygenator takes over the functions of the heart
and the lungs, thus pennitting a quiet, non-beating heart with a clear view unobscured by
blood. Originally only short periods of bypass were feasible. Now periods of up to 6 hours
are possible. Nevertheless, there are several grave complications associated with the use
of the CPB machine. This has led to the use of the off-pump method of CBG using the
Octopus IT tissue stabilizer (by Medtronics Inc.) in several centres around the world.
A total of 100 patients were involved in this prospective study. Fifty of them were
operated using the CPB method and another fifty patients were operated by the off-pump
method. Patients were selected randomly into the two groups of study. Those with pre
operative risk factors of arrythmias were excluded from this study. Both groups had
patients with various other medical problems such as diabetes mellitus, hypertension,
gastrointestinal bleeding, gastritis, ischaemic heart disease, chronic obstructive airway
disease, renal disease, and others. They were all assessed pre operatively by the same
parameters. Baseline blood investigation of full blood count, blood urea and electrolytes,
serum creatinine, coagulation profile were done. Routinely, blood was grouped and cross
matched prior to surgery. A pre-operative angiogram was perfonned. All the 100 patients
had under gone investigations such as ECG, echocardiography, chest x-ray preoperatively.
They were all grouped together and given a "pump talk" i.e. a briefing about the
24