
Workforce Modernisation in the NW Helen Kilgannon Assistant Director Workforce and Modernisation.

July 2013
Business Case for the Health and Care Modernisation
Transition Programme

2
You may re-use the text of this document (not including logos) free of charge in any format or medium, under the terms of the Open Government Licence. To view this licence, visit www.nationalarchives.gov.uk/doc/open-government-licence/
© Crown copyright
Published to gov.uk, in PDF format only.
www.gov.uk/dh
3
Business Case for the Health and Care Modernisation
Transition Programme

Business Case for the Health and Care Modernisation Transition Programme
4
Contents
Introduction ................................................................................................................................ 5
Executive Summary ................................................................................................................... 6
The Case for Change ............................................................................................................... 10
Key Changes ........................................................................................................................... 15
Financial Case ......................................................................................................................... 31
Economic Case ........................................................................................................................ 41
Commercial Case .................................................................................................................... 46
Management Case ................................................................................................................... 49
Appendix A - Changes Adopted Following the NHS Future Forum's Report ........................... 63
Appendix B - Accountabilities in the New Structures ............................................................... 65
Appendix C - Other Arm's length Bodies .................................................................................. 67
Business Case for the Health and Care Modernisation Transition Programme
5
Introduction
The health and care transition programme was established by the Department of Health (DH) in September 2010 to co-ordinate the implementation of the Health and Care reforms outlined in the White paper, “Equity and Excellence: Liberating the NHS”. The programme provided a governance framework to co-ordinate a number of distinct programmes of work across the health and care system to deliver the Government's vision to reshape healthcare so that it is more patient-centred, led by health professionals and focused on delivering world-class health outcomes. The reforms affected around 45,000 staff and more than 400 organisations across the NHS, local government, public health, DH and its arm’s length bodies (ALBs). The health and care reforms came into operation on 1 April. They reshaped the NHS so that it is more patient-centred, led by health professionals and focused on delivering world-class health outcomes. The abolition of SHAs and PCTs, and the establishment of CCGs, puts commissioning in the hands of GPs and local clinicians. New, more autonomous Arm’s Length Bodies are empowered to deliver services according to national priorities. Local government has an important new role in addressing local community health needs. Local authorities are also working with the NHS to deliver integrated health and care services. The new system provides a stronger voice for people and communities, empowering patients and local communities by ensuring services are responsive to their needs. This business case reflects the original proposals as captured in the Health and Social Care Bill 2011, updated to include the changes introduced in response to the report of the NHS Future Forum. The costs and benefits outlined in the business case reflect those included in the revised Impact Assessment for the Bill published in September 2011. In May 2012, the Department published a Transition Scheme for Publication. In this it made a commitment to publish the business case once the transition programme closed in April 2013. As the transition programme has now closed, this business case is being published to fulfil that commitment. What follows, therefore, is the case for change and the costs and benefits of reform as they were assessed in 2011. Parliament has also been given an up-to-date assessment of the costs and benefits of the reforms, alongside the Department’s annual report and accounts for 2012-13.
Business Case for the Health and Care Modernisation Transition Programme
6
Executive Summary
1. The reforms of the NHS and wider health and care system, as set out in the NHS White Paper Equity and Excellence: Liberating the NHS and the Social Care Bill 2011 are fundamental and wide ranging. Aspects of the policy intent will take years to fully implement. The first and most significant stage of the delivery of reforms is setting up the new organisational infrastructure for managing the NHS and Public Health.
2. The transition programme was established in September 2010 to manage the
implementation of the organisational and structural changes, which will largely be implemented by 1 April 2013. This Business case for the Transition Programme is essentially focused on the delivery of the organisational changes rather than all the longer term transformation and full policy intent behind the reforms.
3. The business case is not the document which was used to justify and approve the
reforms, or the Transition Programme or its funding. However, it sets out a summary of the case for change, a description of the main changes, and the costs and benefits of the programme. We are using the business case to provide the baseline of costs and benefits, so we can track their delivery through the life of the programme.
The Case for Reform
4. The current NHS architecture of the health and care system has evolved in a piecemeal way, which is now unwieldy and involves duplication. Costs are increasing at a rate which is unaffordable in the current financial climate, due to an ageing population, increased expectations, and the costs of treatment and technology. Its centralised management structure run out of the Department of Health tends to result in centrally driven changes and process targets which impact on the NHS ability to focus on local service delivery and outcomes.
5. The reforms aim to create a more responsive patient-centred NHS which delivers
outcomes that are amongst the best in the world. In order to deliver the full policy reforms, a new management infrastructure is required which:
puts commissioning in the hands of GPs and local clinicians
puts management of commissioning at arm’s length from the Department and focuses on delivery of outcomes
puts Local Government at the heart of ensuring local community needs are addressed. The Key Changes
6. The main structural changes to organisational infrastructure across the Health and Care system will be implemented by 1 April 2013. By then:
A full system of Clinical Commissioning Groups will have been established and ready to commission services for their patients;
Business Case for the Health and Care Modernisation Transition Programme
7
the NHS Commissioning Board will be running to manage commissioning to deliver NHS outcomes through CCGs;
Health Education England will have taken over SHAs’ (and part of the Department’s) responsibilities for education and training;
Public Health England (PHE) will have been established as the lead body accountable for delivery of Public Health outcomes, and will take on functions from the National Treatment Agency (NTA) and the Health Protection Agency (HPA), which will be abolished;
Health and Wellbeing Boards will be established in every upper tier local authority in England as the local system leaders for health and wellbeing;
Healthwatch England and Local Healthwatch will have been established, and
Local Authorities will have taken on local public health responsibilities from PCTs;
Primary Care Trusts (PCTs) and Strategic Health Authorities (SHAs) will have been abolished.
7. Altogether about 50,000 staff, currently in SHAs, PCTs, DH and other ALBs, will be
affected, either by moving with their functions into another part of the system or through leaving the system. All the current NHS estate and the majority of the other resources, processes and systems which are managed, owned or controlled by SHAs and PCTs will transfer into some part of the new system.
Financial Case
8. The key purpose of the reforms is to deliver the best possible patient services and the Government has committed to a one third reduction in administrative spending to release resources of £4.5 billion (in 2010-11 prices, or £4.9 billion in nominal terms) to the front line by the end of 2014-15. The annual savings from 2014-15 onwards will be £1.5 billion (in 2010-11 prices).
Business Case for the Health and Care Modernisation Transition Programme
8
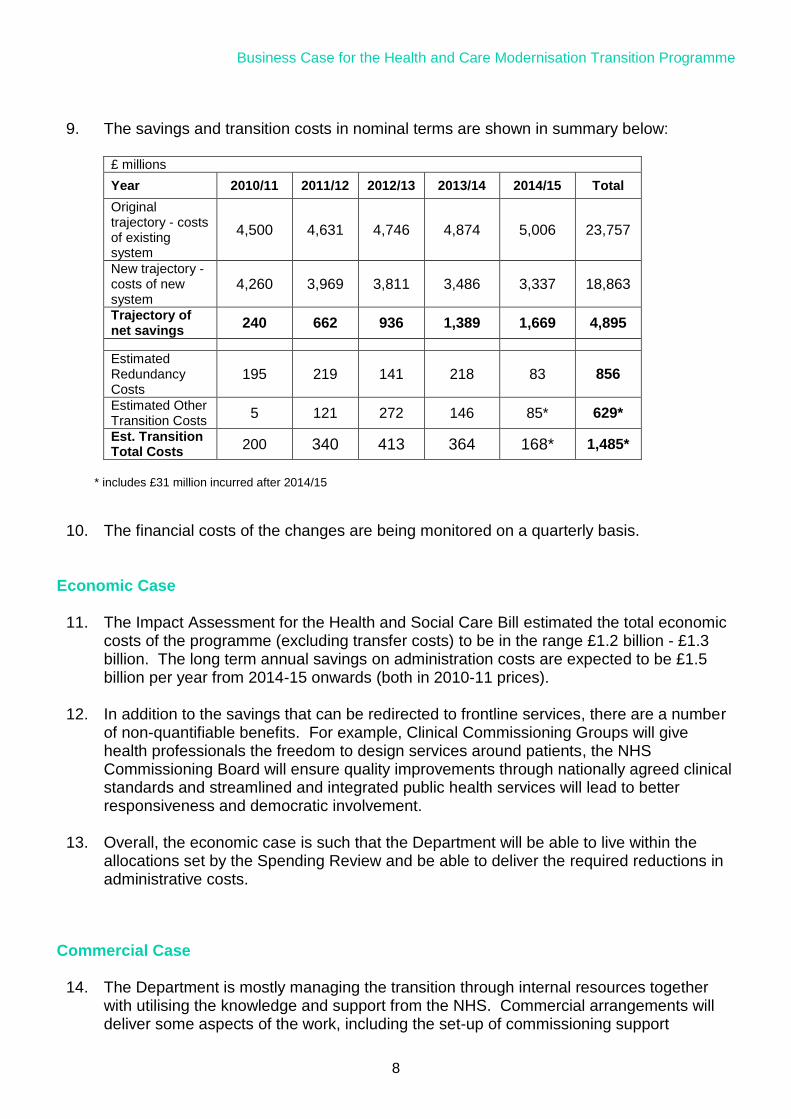
9. The savings and transition costs in nominal terms are shown in summary below:
£ millions
Year 2010/11 2011/12 2012/13 2013/14 2014/15 Total
Original trajectory - costs of existing system
4,500 4,631 4,746 4,874 5,006 23,757
New trajectory - costs of new system
4,260 3,969 3,811 3,486 3,337 18,863
Trajectory of net savings
240 662 936 1,389 1,669 4,895
Estimated Redundancy Costs
195 219 141 218 83 856
Estimated Other Transition Costs
5 121 272 146 85* 629*
Est. Transition Total Costs
200 340 413 364 168* 1,485*
* includes £31 million incurred after 2014/15
10. The financial costs of the changes are being monitored on a quarterly basis.
Economic Case
11. The Impact Assessment for the Health and Social Care Bill estimated the total economic costs of the programme (excluding transfer costs) to be in the range £1.2 billion - £1.3 billion. The long term annual savings on administration costs are expected to be £1.5 billion per year from 2014-15 onwards (both in 2010-11 prices).
12. In addition to the savings that can be redirected to frontline services, there are a number
of non-quantifiable benefits. For example, Clinical Commissioning Groups will give health professionals the freedom to design services around patients, the NHS Commissioning Board will ensure quality improvements through nationally agreed clinical standards and streamlined and integrated public health services will lead to better responsiveness and democratic involvement.
13. Overall, the economic case is such that the Department will be able to live within the
allocations set by the Spending Review and be able to deliver the required reductions in administrative costs.
Commercial Case
14. The Department is mostly managing the transition through internal resources together with utilising the knowledge and support from the NHS. Commercial arrangements will deliver some aspects of the work, including the set-up of commissioning support

Business Case for the Health and Care Modernisation Transition Programme
9
organisations, establishing a publicly owned company to manage and disposal of the surplus primary care estate, and developing shared service arrangements to achieve service efficiencies and financial savings. In addition, reviews have been commissioned to assess commercial efficiencies at the NHS Business Services Authority, the NHS Litigation Authority and the NHS Blood and Transplant.
Management of the Change
15. This programme is the largest and most radical ever undertaken in the NHS, as it fundamentally changes the way the NHS is managed and run. It is being managed through an integrated programme run out of the Department. The programme SRO and Transition Director are professional and experienced change programme managers, who ensure the programme is subject to best practice assurance by the Cabinet Office Major Projects Authority. The programme is organised into 24 separate programmes, each with an SRO, Programme Board and team, responsible for managing the delivery of a major change.
16. The Permanent Secretary and NHS Chief Executive each chair the two main oversight
Transition Boards, and hold individual programme SROs to account for delivery of their programmes.

Business Case for the Health and Care Modernisation Transition Programme
10
The Case for Change Summary The current NHS architecture of the Health and Care system has evolved in a piecemeal way, which is now unwieldy and involves duplication. Costs are increasing at a rate which is unaffordable in the current financial climate, due to an ageing population, increased expectations, and the costs of treatment and technology. Its centralised management structure run out of the Department of Health tends to result in centrally driven changes and process targets which impact on the NHS ability to focus on local service delivery and outcomes. The reforms aim to create a more responsive patient centred NHS which delivers outcomes that are amongst the best in the world. In order to deliver the full policy reforms, a new management infrastructure is required which:
puts commissioning in the hands of GPs and local clinicians
puts management of commissioning at arm’s length from the Department and focuses on delivery of outcomes
puts local government at the heart of ensuring local community needs are addressed.
Vision
17. The Government plans to create a more responsive, patient-centred NHS, which achieves outcomes that are among the best in the world.
18. Their plans have been formulated in a series of White Papers and
Consultations leading up to the publication of the Health and Social Care Bill 2011, which sets out a series of structural reforms to the way the health and care system in order to:
Improve outcomes. Secretary of State’s over-arching ambition is to create a healthcare system that achieves results amongst the best in the world. The current system focuses too narrowly on process targets.
Give patients more power, so that the health and social care services better respond to patients’ and service users’ own needs and wishes.
Focus more on prevention, to tackle the rising incidence of ‘lifestyle disease’ including obesity and alcohol dependency.
Increase the local democratic legitimacy of local commissioning to foster integrated local service planning and commissioning across the NHS, social care and public health, and local government and address the wider determinants of health and wellbeing.

Business Case for the Health and Care Modernisation Transition Programme
11
Improve NHS commissioning so that there is less variability of commissioning arrangements.
Liberate the provider sector to create locally accountable and efficient NHS providers.
Drive quality and productivity improvements so that the NHS can meet the challenging financial position over the coming period as a result of rising demand, rising healthcare inflation, and pressure on social care funding.
Develop a workforce which is more flexible and responsive to changing service needs.
The Structural Problems of the Health and Social Care System
19. The current architecture of the health and social care system has developed piecemeal, involves duplication, and is unwieldy. The Health and Social Care Bill aims to put more power in the hands of patients and clinicians, and remove layers of management, while building on key aspects of the existing arrangements.
20. The main structural problems being addressed are as follows:
Improving public health and tackling health inequalities by setting up a dedicated new public health service - Public Health England (PHE).
Increasing the democratic involvement in commissioning and planning across health and social care through establishing Health and Wellbeing Boards to ensure services develop more around the needs of patients and communities.
Improving commissioning so that it is more patient focused by establishing Clinical Commissioning Groups that will comprise consortia of GP practices, patients, carers and the public as well as other health and care professionals, to work in partnership with local communities and local authorities to commission the great majority of NHS services for their patients.
Ensuring there is national leadership in commissioning and improved quality across the country by creating a statutory NHS Commissioning Board.
Strengthening the accountability of local commissioners and the responsiveness of local services by bringing elected representatives, local health, public health and social care commissioners and a representative of Local Healthwatch, together in local health and wellbeing boards.
Improving the economic regulation of Foundation Trusts in the new system by developing an economic regulator for all providers by
Business Case for the Health and Care Modernisation Transition Programme
12
changing the functions of Monitor, the current regulator for Foundation Trusts.
Streamlining the system to work more effectively and to reduce overheads so that maximum resources can be diverted to front line services by reducing the number of Arms Length Bodies (ALBs) and abolishing Strategic Health Authorities (SHAs) and Primary Care Trusts (PCTs), transferring functions as appropriate to the new bodies.
Strengthening and embedding the voice of patients and the public at both the local and national level through the establishment of Healthwatch England (as a committee of the regulator CQC) and Local Healthwatch (sharing local intelligence with Healthwatch England to inform the national picture).
21. The Key Changes section sets out a high level model for the future health
and care system and the functions of the new bodies in more detail. Financial Context
22. The Autumn 2010 Spending Review protected healthcare funding in real terms over the Spending Review period. However, even with this increase the NHS will need to achieve significant efficiency gains to meet the future costs of an ageing population, increased expectations and changes in technology.
23. The three core commitments to meet this challenge are to:
radically de-layer and simplify the number of NHS bodies, and the Department’s own NHS functions;
make up to £20 billion of NHS annual efficiency savings by March 2015 through the Quality, Innovation, Productivity and Prevention (QIPP) programme; and
reduce the costs of the Department and its arms length bodies (ALBs) by at least 33% in real terms by March 2014.
24. Up to £20 billion of annual efficiency savings over the next four years will
be reinvested to meet rising levels of demand, to meet rising costs in some areas, and to support improvements in quality and outcomes. QIPP delivery is outside the Transition Programme, however higher quality care is often better value in the long term, compared to unsafe or ineffective care that can cost money to put right, or require more care and treatment than is necessary.
25. The scale of the efficiency challenge is such that it can only be met by
system-wide reform. Improving quality and productivity is inextricably linked with implementing the transition programme’s structural reform, for

Business Case for the Health and Care Modernisation Transition Programme
13
example through bringing together responsibility for clinical decisions with the financial consequence of those decisions.
26. The Government has committed to reducing administrative spending by
one-third in order to free up resources for frontline services. The NHS and the Department of Health will therefore realign the entire system to make functions more efficient, or could remove some non-essential functions entirely.
Transition Programme Scope and Objectives
Scope
27. The modernisation and reform of the health and social care system
encompasses a range of policy developments that go beyond the structural changes. In particular, the Health and Social Care Bill includes cross-cutting themes on developing a patient led-NHS, improving quality of care, developing choice and competition and tackling health inequalities.
28. The Transition Programme will oversee the structural design of the new
system and the associated policy development, so that by 2013 the main components of the new Health and Care system will have been properly defined and understood, and the new organisations established to take them forward. In addition, there are a range of policy areas that will also be developed and implemented by 2014 and while the Department is taking these forward they fall outside the specific scope set for the Transition Programme. Examples from the White Papers include personal health budgets, NHS Outcomes Framework, payment by results reform, wider Information Strategy, Social Care funding reform and the changes to Foundation Trusts.
29. The new bodies will continue with the implementation and delivery of
benefits after April 2013 to complete the delivery of the Government’s vision, as set out in the Health and Social Care Bill, and secondary legislation.
Objectives
30. The objectives of the Transition Programme are to:
reform the health and care system such that it will deliver the Secretary of State’s vision;

Business Case for the Health and Care Modernisation Transition Programme
14
deliver the structural changes on time and within the programme’s budget;
ensure the transition of activities from the old system to the new system occur smoothly, including the closure of entities and transfer of appropriate accountabilities;
ensure the future system runs within the cost envelopes set by the 2010 Spending Review; and
ensure the Health and Care system maintains operational and clinical performance, and emergency preparedness throughout the transition.
Business Case for the Health and Care Modernisation Transition Programme
15
Key Changes Summary This section describes the new health and social care system and the changes from the current structure, how these will be implemented, and the timescales. The main structural changes to organisational infrastructure across the Health and Care system will be implemented by 1 April 2013. By then:
A full system of Clinical Commissioning Groups will have been established and ready to commission services for their patients;
the NHS Commissioning Board will be running to manage commissioning to deliver NHS outcomes through CCGs;
Health Education England will have taken over SHAs’ (and part of the Department’s) responsibilities for education and training;
Public Health England (PHE) will have been established as the lead body accountable for delivery of Public Health outcomes, and will take on functions from the National Treatment Agency (NTA) and the Health Protection Agency (HPA), which will be abolished;
Health and Wellbeing Boards will be established in every upper tier local authority in England as the local system leaders for health and wellbeing;
Healthwatch England and Local Healthwatch will have been established; and
Local Authorities will have taken on local public health responsibilities from PCTs;
Primary Care Trusts (PCTs) and Strategic Health Authorities (SHAs) will have been abolished.
Altogether about 50,000 staff, currently in SHAs, PCTs, DH and other ALBs will be affected, either by moving with their functions into another part of the system or through leaving the system. All the current NHS estate and the majority of the other resources, processes and systems which are managed, owned or controlled by SHAs and PCTs will transfer into some part of the new system. Overview of the new Health and Social Care System
31. The Secretary of State for Health remains responsible for promoting a comprehensive health service, and retains ultimate accountability for securing the provision of services. However, instead of directly managing providers or commissioners Ministers will transparently set objectives for the NHS through a mandate to the NHS Commissioning Board. Ministers will hold to account all of the national bodies, with powers to intervene in the event of significant failure, or in an emergency.
Business Case for the Health and Care Modernisation Transition Programme
16
32. The Department of Health will provide system leadership, setting strategic
outcomes and the regulatory, policy and legal framework. It will assure delivery through the stewardship of the system, securing the resources required and allocating those resources across the health and social care system.
33. The NHS Commissioning Board will allocate the funding received from the
Department to clinical commissioning groups, who will commission services from GPs and other clinicians. The Board will also commission some national and regional specialist services, including family health dentistry and community pharmacy.
34. Clinicians will lead commissioning for their local population, with clinical
senates and networks providing additional expertise to improve the design and delivery of patient care.
35. Local authorities will also have a much stronger role in shaping services
and will take over responsibility for local population health improvements. The new health and wellbeing boards will bring together local commissioners of health and social care, elective representatives and Healthwatch to come to a joint view of the health and wellbeing needs of local people and a joint strategy for addressing those needs, which will drive local commissioning across the NHS, social care and public health. At a national level, Public Health England will bring together a range of organisations, integrate the functions and bring public health to centre stage.
36. NHS providers will no longer be performance managed by Strategic
Health Authorities. There will be a consistent system of regulation for all providers: the Care Quality Commission will ensure services meet safety and quality requirements while Monitor will promote efficiency, with powers to set prices, and support service continuity. Patients will be able to choose the best service for themselves, from any qualified provider, with competition on quality not price and with Monitor overseeing compliance with regulations and tackling specific abuses and restrictions that act against patients’ interests. Monitor will temporarily also retain oversight of Foundation Trusts while the NHS Trust Development Authority will help the remaining NHS trusts achieve foundation status.
37. Health Education England will provide oversight and leadership for
professional education and training. It will ensure that the health workforce has the right skills, behaviours and training and is available in the right numbers to support the delivery of excellent healthcare and healthcare improvement.

Business Case for the Health and Care Modernisation Transition Programme
17
38. The National Institute for Health and Care Excellence will continue to
provide independent advice and guidance to the NHS and will extend its role to social care. The Information Centre will continue to act as an authoritative source of health and social care information.
39. The diagram below shows the health and social care system in 2013,
including the relationship between the national and local structures.
The key accountabilities in the new structures are set out in the Accountabilities Statement for the Department of Health. An overview summary is in Appendix B.
Organisation structure changes
40. The main structural changes for each of the organisations are set out below, which include the changes since the Bill was originally introduced in January 2011 from both the Commons Committee and Government’s response to the NHS Future Forum report (Appendix A sets out changes from the report).
Business Case for the Health and Care Modernisation Transition Programme
18
NHS Commissioning Board
What the organisation is for:
The NHSCB’s overarching role is to ensure that the NHS delivers better outcomes for patients within its available resources. The NHSCB can fulfill this role through its leadership on delivering the NHS Outcomes Framework, supported by its accountability framework for clinical commissioning groups, its framework for choice and competition, and its framework for emergency planning and resilience.
Key changes:
The Board will be an independent non-departmental public body (NDPB); it will have its own powers and it will be accountable to Secretary of State. It will commission national and regional specialised services, the family health services of dentistry, community pharmacy and primary ophthalmic services, and allocate and account for NHS resources. It will also take over the current CQC responsibility of assessing NHS commissioners and will hold GP consortia to account for their performance and quality.
How these will be implemented:
The NHSCB will be organised to ensure that each member of staff is working to improve health outcomes as well as taking on a particular functional responsibility. It will be organised nationally around the five outcome domains of the NHS Outcomes Framework (reducing mortality, long-term conditions, acute episodes, patient safety and patient experience) and there will be national professional leads for each of these areas, reporting to a national medical director or nursing director.
Timeline / Key stages:
It will operate in shadow form as a Special Health Authority from October 2011. Subject to the passage of the Health and Social Care Bill, in May 2012, the NHSCB will be established as an independent statutory body and take on some formal statutory accountabilities, including the authorisation of Clinical Commissioning Groups and the planning for 2013–14. The NHSCB will be fully operational by April 2013.

Business Case for the Health and Care Modernisation Transition Programme
19
Clinical Commissioning Groups
What the organisation is for:
Establishing groups of GPs, other health and social care professionals and patients and the public to commission the great majority of NHS services. They will not be directly responsible for commissioning services that GPs themselves provide but they will become increasingly influential in driving up the quality of general practice. This role will be transferred from Primary Care Trusts (PCTs) which will close by 31 March 2013. Clinical Commissioning Groups will be responsible for the functions that directly support commissioning healthcare services, including:
population health needs assessment;
strategy development;
patient and public engagement;
procurement and contracting; and
validation and reimbursement.
Key changes:
By April 2013, there will be a comprehensive system of Clinical Commissioning Groups, supported by and accountable to the new independent NHS Commissioning Board. The legislative framework will be designed to make sure that these groups are able to focus on improving quality of care within the resources available to them.
How these will be implemented:
Pathfinders are currently testing the new commissioning arrangements to ensure they are working well before shadow arrangements come into place. The pathfinders will also be involved in the design and testing of the authorisation processes, accountability, and support and intervention in readiness for authorisation to start from October 2012.
Timeline / Key stages:
The NHS Commissioning Board will be able to authorise Clinical Commissioning Groups from October 2012, and SHAs and PCTs will be abolished by April 2013. However the Board will only authorise CCGs when it is satisfied that they are ready to take on the commissioning functions.

Business Case for the Health and Care Modernisation Transition Programme
20
Health Education England and Local Education and Training Boards
What are the organisations for:
Health Education England (HEE) will be established to provide oversight and national leadership for education and training. HEE will bring together the interests of healthcare providers, the professions, patients and staff and take over the advisory role of Medical Education England and the professional advisory boards for education and training of nurses and allied health professionals.
Key changes:
The healthcare providers, with their local clinical leadership, will take a lead role in planning and developing their workforce, with responsibility for many of the workforce functions currently led by the Strategic Health Authorities (SHAs). Funding arrangements would be reformed to provide a fairer and more transparent approach. Oversight and national leadership for education and training will be provided by Health Education England (HEE).
How these will be implemented:
HEE will promote and ensure high quality workforce planning, education and training that is responsive to the changing needs of patients and local communities, providing national leadership on planning and developing the health workforce. It will allocate and account for most NHS Education & Training resources, support the development of provider-led networks and hold the local networks to account for the use of Education & Training resources.
Timeline / Key stages:
The Health Education England will be established as a Special Health Authority in shadow form in 2012 and will take over most SHA responsibilities for education and training in April 2013, when the Boards come into full operation.
Monitor
What the organisation is for:
Monitor will carry out the following functions as regulator for providers of health services:
setting, in conjunction with the NHS Commissioning Board, and regulating prices for NHS-funded services, and preventing anti-competitive behaviour that acts against patients’ interests;
supporting the continuity of vital services in the event of the financial failure; and

Business Case for the Health and Care Modernisation Transition Programme
21
licensing providers.
It will have a vital role in making sure that the system works together to give patients choices about their health and care. It will tackle specific abuses and restrictions that act against patients’ interests to ensure a level playing field between providers. Monitor will also have a duty to support commissioners to provide care in an integrated way where this best meets the needs of patients.
Key changes:
The Bill turns Monitor into a regulator for providers of NHS-funded health services, from it’s current role of determining whether NHS trusts are ready to become foundation trusts, ensuring foundation trusts comply with the conditions of their authorisations, and supporting their development.
How these will be implemented:
Monitor’s core duty will be to protect and promote patients’ interests. It will do this by promoting the provision of care that is economic efficient and effective and ensure that quality is maintained and where possible increased.
Timeline / Key stages:
It is anticipated that, subject to Parliamentary approval, foundation trusts will be subject to Monitor’s licensing regime from April 2013. From April 2013 Monitor will also issue guidance for commissioners on good procurement practice; protecting patient choice and preventing conflict of interest and anticompetitive behaviour.
NHS Trust Development Authority
What the organisation is for:
The NHS Trust Development Authority will provide governance and accountability for NHS Trusts in England. It will be responsible for overseeing the performance management of NHS Trusts including clinical quality, and driving their progress towards Foundation Trust status. It will be accountable nationally for performance and maintaining financial balance of NHS Trusts, the management of the foundation trust pipeline, monitoring clinical quality, governance and risk in NHS Trusts, and public appointments to NHS Trusts and NHS Charities. It will also be responsible for public appointments to NHS Trusts and some NHS charities.

Business Case for the Health and Care Modernisation Transition Programme
22
Key changes:
The NTDA will take on performance management role previously undertaken by the Strategic Health Authorities. It will also take over the work of the Appointments Commission in relation to appointments for NHS Trusts. The NTDA will exist until all NHS trusts are a Foundation Trust in their own right, part of an existing Foundation Trust or in another organisational form.
How these will be implemented:
NTDA will be a time-limited Special Health Authority of the Department of Health.
Timeline / Key stages:
NTDA will be established in shadow form in October 2012 and will take over SHAs’ responsibilities for the foundation trust pipeline and for the overall governance of NHS trusts from April 2013.
Health and Wellbeing Boards
What the organisation is for:
Health and wellbeing boards will be a forum for local commissioners across the NHS, public health and social care, as well as elected representatives and representatives of Local Healthwatch, to develop robust joint strategies, based on local need, which will drive integrated local commissioning, and securing better outcomes for local people.
Key changes:
Local authorities and clinical commissioning groups will perform Joint Strategic Needs Assessments through health and wellbeing boards, and develop joint health and wellbeing strategies which will drive local commissioning. From April 2013, local authorities will receive their public health ring-fenced budgets for the first time, and the health and wellbeing boards will assume their statutory powers to improve commissioning.
How these will be implemented:
Clinical commissioning groups and local authorities will assume joint responsibility for performing Joint Strategic Needs Assessments (currently undertaken by local authorities and PCTs) through health and wellbeing boards. There will be a new duty on boards to develop a joint health and wellbeing strategy, based on local need and setting out priorities for collective action, which will drive joint local commissioning and integrated service provision across the NHS, public health and social care.

Business Case for the Health and Care Modernisation Transition Programme
23
Timeline / Key stages:
Subject to the passage of the Health and Social Care Bill, health and well being boards will be established in every upper tier authority from April 2013. It is intended that they will run in shadow form from 2012.
Healthwatch England and Local Healthwatch
What the organisation is for:
Local Healthwatch and Healthwatch England will strengthen the voice of patients and the public locally, and will enable the collective views of users of health and social care services to influence national policy.
Key changes:
Local Healthwatch will carry forward the current functions of Local Involvement Networks (LINks) such as entering and viewing services, and will take on further functions, supporting individuals by providing information to promote choices, and potentially providing or signposting to NHS complaints advocacy. It will give local people the opportunity to make their views on their experiences known to commissioners and providers of services, and will provide feedback to Healthwatch England. Healthwatch England will provide leadership to Local Healthwatch organisations and will provide advice and information to the Secretary of State, the NHS Commissioning Board, Monitor, local authorities and the Care Quality Commission on the views and experiences of patients and the public. Local authorities and clinical commissioning groups will perform Joint Strategic Needs Assessments through health and wellbeing boards, where Local Healthwatch will be represented, and develop joint health and wellbeing strategies which will drive local commissioning. Boards are intended to operate in shadow form in 2012-13, and will be established on a statutory basis from April 2013.
How these will be implemented:
Healthwatch England will be established as a statutory committee of the Care Quality Commission. Local Healthwatch organisations will be funded via local authorities, and will have a seat on health and wellbeing boards. The Health and Social Care Bill creates various duties on the Secretary of State, Monitor, the Care Quality Commission, the NHS Commissioning Board and local authorities to respond in writing to the advice of Healthwatch England; and for commissioners and providers to respond in writing to the advice of Local Healthwatch.
Business Case for the Health and Care Modernisation Transition Programme
24
Timeline / Key stages:
Subject to the passage of the Health and Social Care Bill, Healthwatch England will be established in October 2012 and Local Healthwatch will be established in April 2013.
Public Health England
What the organisation is for:
Public Health England (PHE) will be a new integrated public health organisation – bringing together a number of existing bodies – that will strengthen the national response on emergency preparedness and health protection. It will support delivery across the three domains of public health – health improvement, health protection, and population health services – through information, evidence, surveillance and professional leadership. The Secretary of State is ultimately accountable to Parliament and the public for the delivery of the functions for which Public Health England is responsible PHE will drive improved outcomes in health and wellbeing, and protect the population against existing and future threats to health.
Key changes:
Setting up a dedicated new public health service - PHE - in the Department and taking on the functions of the Health Protection Agency (HPA); the National Treatment Agency for Substance Misuse (NTA); public health and intelligence functions; and national commissioning of health promotion and improvement campaign activity. PCT responsibilities for local health improvement will transfer to local authorities, who will employ the Director of Public Health jointly appointed with PHE.
How these will be implemented:
PHE will be an executive agency of the Department of Health. Its chief executive will be accountable to the Permanent Secretary for how the agency delivers against its business plan. PHE will also be accountable to the Department for the public funding it receives.
Timeline / Key stages:
Public Health England will be established on 1 April 2013, alongside the establishment of the NHS Commissioning Board and local authorities taking on their new statutory responsibilities for both public health and the Directors of Public Health.
Business Case for the Health and Care Modernisation Transition Programme
25
This timing ensures that the transition is separated from the Olympic and Paralympic Games, where responsibilities for health protection through this crucial period will remain with the existing statutory bodies.
Department of Health
What the organisation is for:
The role of the Department of Health is to maximise the health and wellbeing gain for the population through its stewardship of the adult social care, public health and NHS systems, and its work with other government departments.
It will do this by:
setting strategic outcomes for the health and adult social care system and assuring delivery through its stewardship of the systems;
securing resources for the health and social care system;
setting the regulatory, policy and legal framework for the health and social care system; and
providing system leadership for the whole system.
Key changes:
Commissioning policy and the allocation and accounting for NHS resources will move the NHS Commissioning Board, and tariff work will move to Monitor.
How these will be implemented:
A detailed mapping of functions is in progress, together with design of jobs within the future DH. Staff moves into confirmed posts will be completed in accordance with the HR framework.
Timeline / Key stages:
The top level structure for the Department was announced in July 2011. Function and people moves will be aligned with receiving organisations and will be completed by April 2013.
Other Arm’s Length Bodies
Overall aim:
In future the arm’s length bodies’ sector will mirror the reformed NHS and social care landscape, creating institutions that have clear duties, are transparent in their accountabilities and their responsibilities to patients, users and the public, and are more streamlined, with no overlap of functions between organisations.

Business Case for the Health and Care Modernisation Transition Programme
26
Key changes:
The following changes are being implemented following the review of the Department’s ALBs published in July 2010. Eight of the ALBs will leave the sector either becoming self-funding or being abolished and having their services transferred/delivered elsewhere:
Alcohol and Education Research Council (AERC)
Appointments Commission (AC)
Council for Healthcare Regulatory Excellence (CHRE)
Human Fertilisation and Embryology Authority (HFEA)
Human Tissue Authority (HTA)
General Social Care Council (GSCC)
National Patient Safety Agency (NPSA)
NHS Institute for Innovation and Improvement) (NHSIII).
Three ALBs are undergoing commercial reviews with likely consequences to each organisation's business from 2012-13 onwards:
NHS Business Services Authority (NHS BSA)
NHS Blood and Transplant (NHS BT)
NHS Litigation Authority (NHS LA).
Four other ALBs will continue, but each has some element of transition to manage:
Medicines and Healthcare products Regulatory Agency (MHRA)
Care Quality Commission (CQC)
National Institute for Health and Clinical Excellence (NICE)
The Health and Social Care Information Centre (HSCIC).
NICE and HSCIC will change status from Special Health Authorities to be non-departmental public bodies, which will give them greater autonomy. The remaining three ALBs included in the ALB review are:
Health Protection Agency (HPA)
National Treatment Agency (NTA)
Monitor (see separate section). The Health Protection Agency (HPA) and the National Treatment Agency (NTA) will be abolished with functions will be transferred to become part of Public Health England (PHE). In addition Health Research Authority (HRA) is a newly formed NHS organisation from December 2011 to protect and promote the interests of patients and the public in health research. It brings together the functions previously provided by the National Patient Safety Agency and the Research Ethics Committee.

Business Case for the Health and Care Modernisation Transition Programme
27
How these will be implemented:
Some organisations will be abolished or move to self-funding status, and some functions will cease or transfer. Savings and efficiencies will be made by streamlining the number of bodies and changing the way that they deliver their functions. Business support services across ALBs will be aggregated, helping to reduce duplication and bureaucracy through shared services initiatives for back office functions such as HR, finance and procurement. The continuing and new arm’s length bodies will formally set out their roles and responsibilities through framework agreements, including how the Department will seek assurance on the delivery of their objectives within their available resources.
Timeline / Key stages:
The ALB transition timetable continues until transition is complete. The majority of those ALBs leaving the sector will be closed during 2012-13. The exceptions being the transfer of functions from and closure of HFEA and HTA, which are subject to passage of the Public Bodies Bill and future primary health legislation, where closure is planned for 2015. Further details on the future roles, timings and function transfers are included in Appendix C.

Business Case for the Health and Care Modernisation Transition Programme
28
High Level Timeline
41. The sequence of key transition events is outlined below on the current plans:
Design and Policy Phase: To April 2011
White Paper ‘Equity and Excellence: Liberating the NHS’ published in July 2010.
Public Health White Paper published November 2010.
Command Paper (response to White Paper consultation) published December 2010.
House of Commons Bill Committee Stage.
Publication of HR framework for transition to the new system.
Publication of the NHS Operating Framework and PCT allocations for 2011-12.
Identification of the first wave of “pathfinder” Clinical Commissioning Groups.
DH confirms the design framework, subject to Parliamentary approval.
DH gives permission to pathfinders and early implementers to model some elements of the new arrangements and explore key issues for wider roll-out.
Listening Exercise: April 2011 – June 2011
Pause to undertake more engagement with stakeholders and consider improvements.
Government response to the NHS Future Forum report.
Preparation and Early Implementation: July 2011 – March 2013
SHA cluster arrangements in place by October 2011.
NHS Commissioning Board established in shadow from as a Special Health Authority from November 2011.
PCT provider-arm divestments largely completed; Community FTs come on stream.
Health Research Authority created as a Special Health Authority in 2011.
Health Education England and the NHS Trust Development Authority are established in shadow form as Special Health Authorities during 2012.

Business Case for the Health and Care Modernisation Transition Programme
29
Public Health England set up in shadow form for preparatory work before establishment in April 2013. Shadow allocations to local authorities for public health.
NHSCB is established as an independent statutory body by October 2012, carrying out limited functions, in particular, establishing and authorising clinical commissioning groups
Monitor starts to take on economic regulation powers and functions in October 2012.
Healthwatch England and local Healthwatch are established in October 2012.
Health and wellbeing boards operate in shadow form during 2012-13
Implementation – first full year of new system: April 2013 – March 2014
PCTs and SHAs abolished by April 2013.
NHS Commissioning Board takes on its full functions.
A full system of clinical commissioning groups is established. But the NHS Commissioning Board will not authorise clinical commissioning groups to take on their responsibilities until ready.
Health Education England takes over SHAs’ responsibilities for education and training.
Establishment of Public Health England and abolition of NTA and HPA.
Local Authorities take on local public health responsibilities and functions.
Most changes to ALBs implemented.
The NHS Trust Development Authority takes over SHAs’ responsibilities for the foundation trust pipeline and for the overall governance of NHS trusts.
Health and wellbeing boards established on a statutory basis.
Monitor will regulate all providers of NHS care.
The timeline is shown in chart form below:

Business Case for the Health and Care Modernisation Transition Programme
30
Transition High Level timeline from November 2010 to April 2013

Business Case for the Health and Care Modernisation Transition Programme
31
Financial Case Summary The key purpose of the reforms is to deliver the best possible patient services, and the Government has committed to a one third reduction in administrative spending, to release £4.5 billion resources to the front line by the end of 2014/15. The annual savings from 2014-15 onwards is £1.5 billion. The savings and transition costs in nominal terms are shown in summary below:
£ millions,
Year 2010/11 2011/12 2012/13 2013/14 2014/15 Total
Original trajectory
- costs of existing
system
4,500 4,631 4,746 4,874 5,006 23,757
New trajectory -
costs of new
system
4,260 3,969 3,811 3,486 3,337 18,863
Trajectory of net
savings 240 662 936 1,389 1,669 4,895
Estimated
Redundancy
Costs
195 219 141 218 83 856
Estimated Other
Transition Costs 5 121 272 146 85* 629*
Est. Transition
Total Costs 200 340 413 364 168* 1,485*
Financial costs are being monitored on a quarterly basis. * includes £31 million incurred after 2014/15. Reduction in Administrative Spending
42. The Government has committed to a reduction of one third in administrative spending across Whitehall. In the health sector, this covers all functions within the Department of Health, SHAs, PCTs and ALBs that do not constitute the direct delivery of a frontline service. The changes introduced by the Health and Social Care Bill will deliver these planned reductions in administrative expenditure.
43. The one third real terms reduction in administrative spending has been
measured against a 2010-11 baseline and is to be fully achieved by 2014-15. The Department estimated a baseline for administrative expenditure in January 2011 at £5.1 billion and subsequently adjusted it in September
Business Case for the Health and Care Modernisation Transition Programme
32
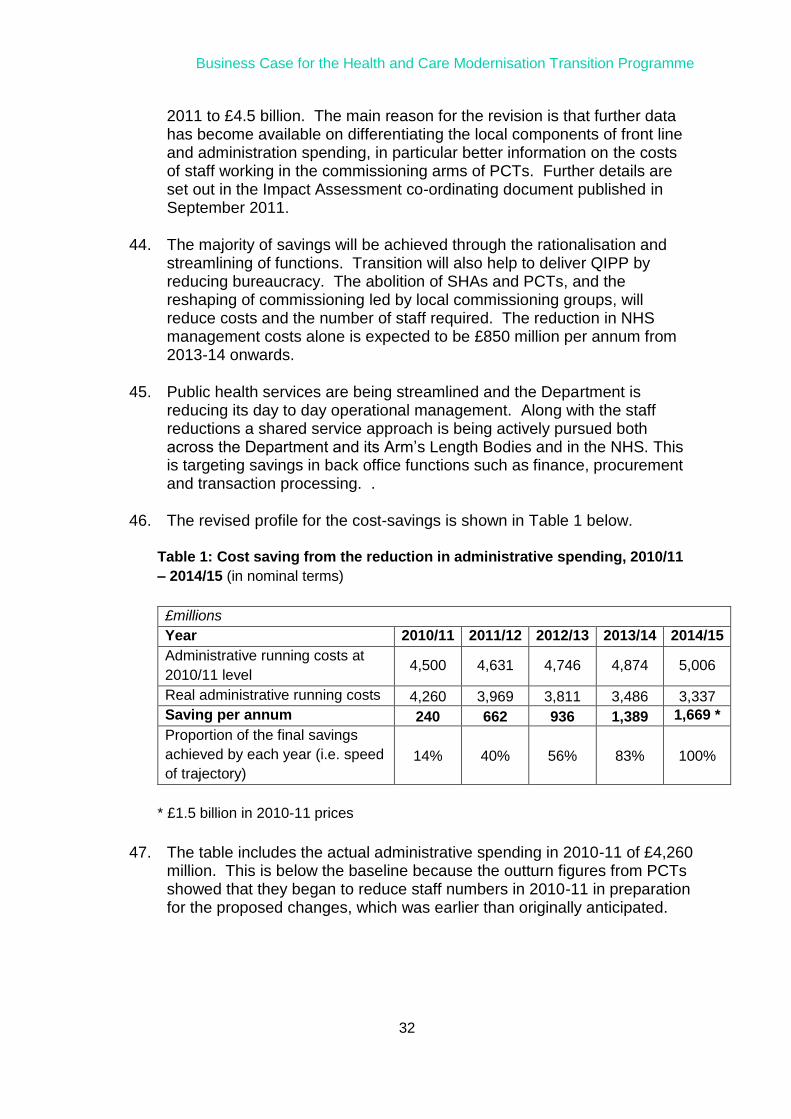
2011 to £4.5 billion. The main reason for the revision is that further data has become available on differentiating the local components of front line and administration spending, in particular better information on the costs of staff working in the commissioning arms of PCTs. Further details are set out in the Impact Assessment co-ordinating document published in September 2011.
44. The majority of savings will be achieved through the rationalisation and
streamlining of functions. Transition will also help to deliver QIPP by reducing bureaucracy. The abolition of SHAs and PCTs, and the reshaping of commissioning led by local commissioning groups, will reduce costs and the number of staff required. The reduction in NHS management costs alone is expected to be £850 million per annum from 2013-14 onwards.
45. Public health services are being streamlined and the Department is
reducing its day to day operational management. Along with the staff reductions a shared service approach is being actively pursued both across the Department and its Arm’s Length Bodies and in the NHS. This is targeting savings in back office functions such as finance, procurement and transaction processing. .
46. The revised profile for the cost-savings is shown in Table 1 below.
Table 1: Cost saving from the reduction in administrative spending, 2010/11
– 2014/15 (in nominal terms)
£millions
Year 2010/11 2011/12 2012/13 2013/14 2014/15
Administrative running costs at
2010/11 level 4,500 4,631 4,746 4,874 5,006
Real administrative running costs 4,260 3,969 3,811 3,486 3,337
Saving per annum 240 662 936 1,389 1,669 *
Proportion of the final savings
achieved by each year (i.e. speed
of trajectory)
14% 40% 56% 83% 100%
* £1.5 billion in 2010-11 prices
47. The table includes the actual administrative spending in 2010-11 of £4,260 million. This is below the baseline because the outturn figures from PCTs showed that they began to reduce staff numbers in 2010-11 in preparation for the proposed changes, which was earlier than originally anticipated.

Business Case for the Health and Care Modernisation Transition Programme
33
Redundancy costs
48. The Health and Social Care Bill proposals involve a major de-layering in the NHS, and recognise that some staff who are currently employed by PCTs, SHAs, ALBs, NHS Leadership and DH will be made redundant.
49. Table 2 below shows the estimated redundancy numbers and costs from
April 2011 onwards, and how this is broken down across those organisational groups. These numbers assume that the new organisations recruit all of their staff from existing organisations. Further reductions in staff numbers will be achieved through natural wastage. The differences in the predicted future staff reductions across different organisations are based on high-level modelling of the skills that the new organisations might require. The percentage reduction includes both the staff numbers from redundancy and those occurring from natural wastage.
Table 2: Lower estimate redundancy costs and numbers from April 2011
onwards
Future expected
redundancy
numbers
Predicted
wastage
numbers
Future expected
redundancy cost
(£m)
Total future
reduction in
staff (%)
SHAs 600 400 51 27%
PCTs 7,900 3,500 343 33%
ALBs 200 600 11 15%
NHS
Leadership
plus DH
400 500 32 21%
Total 9,100 5,000 437 29%
50. The costs and figures in Table 2 are based on the following assumptions:
The extent of redundancies will be different across organisational groups;
Redundancies are phased over the transition period. So, in comparison to the initial Impact Assessment figures in January 2011, more of the reduction in the workforce is achieved through natural wastage rather than redundancy. This is, however, offset by higher unit costs of redundancy as a result of increased pay pressures in the system;
A one third real reduction in running costs is achieved over 4 years for the whole non-provider administrative spend;
The redundancy multipliers (the number of times their salary an individual can expect to receive if they are made redundant) are 1.5 for DH, SHAs and ALBs, and 1.2 for PCTs. These are based on the

Business Case for the Health and Care Modernisation Transition Programme
34
information available at this stage, including from the Electronic Staff Records database;
Redundancies are spread evenly throughout the wage structure, across all levels of employment; and
Natural wastage (the proportion of staff that leave of their own accord, for example through finding new jobs or through retirement) is 3% per annum (see also paragraph 54 below).
51. The strongest drivers of cost in this table are the redundancy cost
multiplier and the wastage assumption. The redundancy cost multiplier is applied at the higher point of the salary scale, making this a high-end estimated cost; this has been adopted because redundancy packages are usually more attractive to higher paid, longer serving staff and because some staff have pension protection included in the redundancy package. Reducing the multiplier for DH, SHAs and ALBs to 1, and the PCT multiplier to 0.8, would reduce the redundancy costs by £154 million.
52. The wastage assumption figure is derived from current levels of natural
wastage (around 6%) being reduced by the anticipation of the prospect of redundancy packages being made available. The current turnover of managers within the NHS is estimated to be around 12.5%; the working assumption is that this level would halve during an economic downturn, as managers have transferable skills but fewer opportunities. This is then halved again as fewer staff will choose to leave when there is the prospect of redundancy packages, giving the assumption of 3% used here. For example, wastage fell by a half in 2006-7 when PCTs were being reorganised and redundancy was made available; increasing the wastage to 6% would reduce costs by £243 million.
53. Some redundancies occurred in 2010-11 and the payments recorded in
the 2010-11 accounts are shown in the table below (excluding provisions for future years), along with the remaining staff numbers as at April 2011.
Table 3: Current staff numbers and redundancy costs incurred so far
Remaining staff
(April 2011)
Redundancy costs
incurred 2010/11 (£m)
SHAs 3,800 3
PCTs 34,500 142
ALBs 5,800 29
NHS Leadership plus DH 4,200 21
Total 48,300 195
54. With the £195m redundancy costs already incurred in 2010-11, this makes a total projected redundancy cost of £632m. This is a theoretical minimum total cost as there are likely to be extra redundancy costs because of:
Business Case for the Health and Care Modernisation Transition Programme
35
Friction – skill and geography mismatches between the staff available and those required in the new organisations; and
Flexibility – future organisations may decide to employ staff that are not employed in the current system.
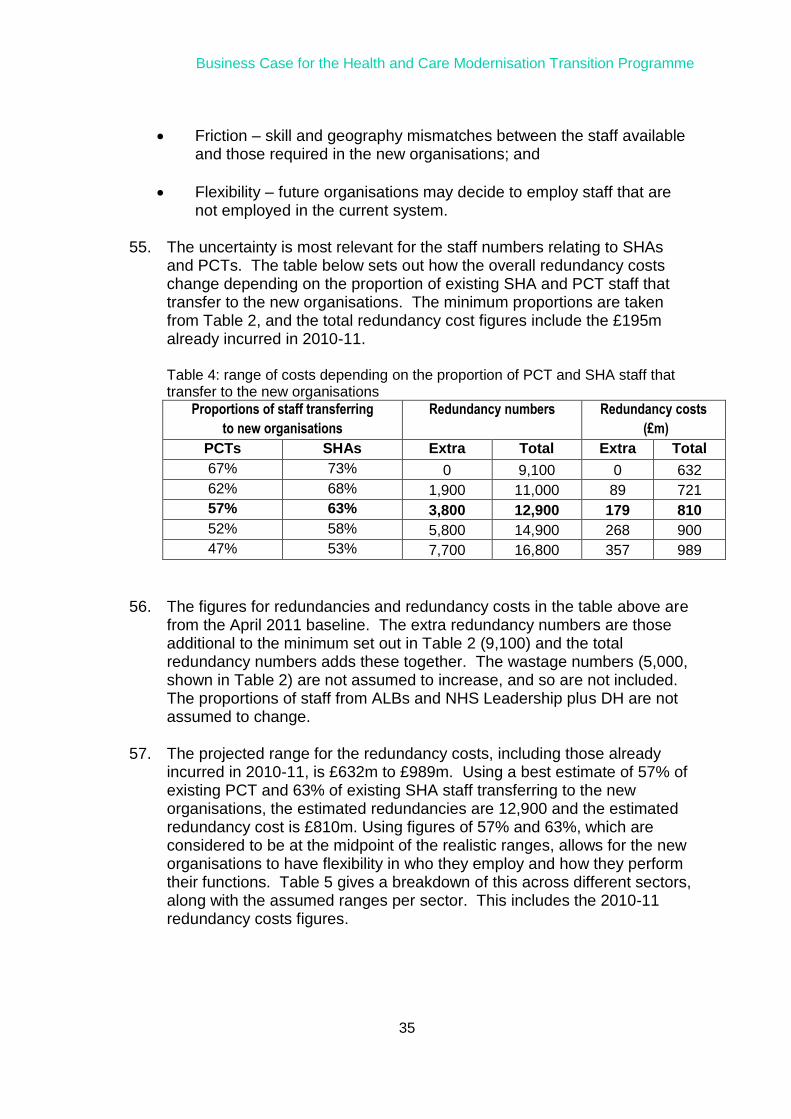
55. The uncertainty is most relevant for the staff numbers relating to SHAs
and PCTs. The table below sets out how the overall redundancy costs change depending on the proportion of existing SHA and PCT staff that transfer to the new organisations. The minimum proportions are taken from Table 2, and the total redundancy cost figures include the £195m already incurred in 2010-11. Table 4: range of costs depending on the proportion of PCT and SHA staff that transfer to the new organisations
Proportions of staff transferring
to new organisations
Redundancy numbers Redundancy costs
(£m)
PCTs SHAs Extra Total Extra Total
67% 73% 0 9,100 0 632
62% 68% 1,900 11,000 89 721
57% 63% 3,800 12,900 179 810
52% 58% 5,800 14,900 268 900
47% 53% 7,700 16,800 357 989
56. The figures for redundancies and redundancy costs in the table above are from the April 2011 baseline. The extra redundancy numbers are those additional to the minimum set out in Table 2 (9,100) and the total redundancy numbers adds these together. The wastage numbers (5,000, shown in Table 2) are not assumed to increase, and so are not included. The proportions of staff from ALBs and NHS Leadership plus DH are not assumed to change.
57. The projected range for the redundancy costs, including those already
incurred in 2010-11, is £632m to £989m. Using a best estimate of 57% of existing PCT and 63% of existing SHA staff transferring to the new organisations, the estimated redundancies are 12,900 and the estimated redundancy cost is £810m. Using figures of 57% and 63%, which are considered to be at the midpoint of the realistic ranges, allows for the new organisations to have flexibility in who they employ and how they perform their functions. Table 5 gives a breakdown of this across different sectors, along with the assumed ranges per sector. This includes the 2010-11 redundancy costs figures.

Business Case for the Health and Care Modernisation Transition Programme
36
Table 5: Predicted range of total redundancy costs
All figures are in £millions in 2010/11 prices
Minimum redundancy
cost
Most likely
redundancy cost
Maximum redundancy
cost
SHAs 54 84 114
PCTs 485 634 782
ALBs 40 40 40
NHS Leadership
plus DH 53 53 53
Total 632 810 989
58. Table 6 shows an initial profile of the redundancy costs and the conversion from 2010-11 prices to cash figures. The modelling is to be further developed to reflect emerging data on the transfer of functions and people between ‘sender’ and ‘receiver’ organisations, revised timings and the end state budgets.
Table 6: Redundancy Expenditure Profile in nominal and 2010-11 prices
Year £m 2010/11 2011/12 2012/13 2013/14 2014/15 Total
Estimated
Redundancy Costs –
2010-11 prices
195 194 156 213 52 810
Redundancy Costs –
nominal prices 195 219 141 218 83 856
Non-Redundancy costs
59. Table 7 sets out the non-redundancy costs and each of the components is explained in more detail in the sections below.

Business Case for the Health and Care Modernisation Transition Programme
37
Table 7: Non-redundancy costs
Year £m 2010/11 2011/12 2012/13 2013/14 2014/15 Total
Estates Costs 5 20 85 85 195*
IT Costs 13 114 40 167
Internal Costs 5 38 43 86
Other External
Costs 65 95 21 181
Total Other
Transition Costs 5 121 272 146 85 629*
* includes £31 million estates costs estimated to be incurred after 2014-15
Estates Costs
60. The Department’s and ALB’s administration estates baseline has been
taken as £90m, based on the running costs in 2009-10 (excluding specialist estates operated by the Health Protection Agency and NHS Blood and Transplant).
61. The SHA and PCT admin estate comprises over 500 separate buildings
with an annual running cost in excess of £150m. The budget for these properties, and the staff currently required to manage them, are held by SHAs and PCTs. In October 2011 the current 10 SHAs and 152 PCTs were consolidated administratively into 4 SHA clusters and 50 PCT clusters. For some time into the future staff are likely to continue in most of the locations, although they will require less space than the current offices provide.
62. The main estates transition cost relates to the legacy costs of surplus
office space, and is dependent on how much of the estate will be reused for the new CCGs and other sub-national structures. NHS estate cost data is available for the SHA estate (£16m excluding hosted functions), but for PCTs it has been estimated on the basis of 63% of their estate total being used for commissioning activity, with the remaining 37% being used for provider activity. Excluding provider activity, the total NHS administrative office cost was circa £106 million per annum in 2009-10. This estimate will be revised once further data collected by the Property Services (Propco) programme in the summer of 2011 is analysed.
Business Case for the Health and Care Modernisation Transition Programme
38
63. In line with the proposed governance regime, it is anticipated that the large majority of CCGs and Commissioning Support Groups (CSGs) will continue to use existing estate. However, these costs will rise substantially, both in terms of capital investment and additional legacy costs, if there is significant acquisition of new property rather than utilisation of existing property, resulting in a larger surplus. The timing of these costs (and therefore the profile of the net saving) is still uncertain given the dependency on the details of the individual buildings to be retained or made surplus. This is not yet known but could stretch over a period of years as leased property is managed out.
64. The scale of the costs (and therefore how quickly the savings are accrued)
depend critically on how much of the existing SHA and PCT estate can be recycled and how much needs to be replaced.
65. By analysing the current lease profiles, and assuming that between a half
and one-third of the current PCT estate is retained, the transition cost for estates is estimated to be between £80 million to £200 million. This includes between £10 million to £20 million for the DH and ALB estate changes, including preparing buildings for new organisations. The range reflects the uncertainty about where, in terms of buildings, new organisations are likely to be based and how the existing estate will be used.
66. The £195 million in Table 7 represents a high end estimate together with
the related costs for ICT (information, communication and telephony) such as cabling and core computer equipment and networks for the new organisations.
Information Technology
67. The organisational changes to the NHS will impact on the operation of the
informatics systems across the Department, its Arms Length Bodies and the NHS.
68. Costs are likely to arise in the following areas:
changes to existing national systems owned by Connecting for Health;
changes to DH and ALB systems;
changes to / transfer of existing systems operated by SHAs, PCTs and the wider NHS; and
new requirements may emerge from the operational design of the economic regulator, NHS Commissioning Board and other organisations.

Business Case for the Health and Care Modernisation Transition Programme
39
69. The main cost is expected to be incurred on PCT systems and their transfer to successor organisations. In the Impact Assessment it was assumed that the cost would be equivalent of 6 months of the average IT spend per year for setting up new IT and transferring from the old one. This gave a figure of £950,000 per PCT (in 2010-11 prices) or £151 million in total as an estimate (£167 million in nominal terms).
Internal Costs
70. The Department of Health will incur costs to fund the teams that develop the way that the new bodies will operate and in designing the new systems and organisations, as well as managing the implementation. For most of these teams, specific budgets have been established to contain the costs. However, for a few areas where costs are being incurred within recurrent directorate allocations, an apportionment basis has been used to identify transition costs.
71. These internal costs cover all the significant work programmes, although
they do not cover some support areas (e.g. finance) where there is no clear distinction between transition work and business as usual.
72. Table 7 shows the internal costs incurred in 2010-11, expected to be
incurred in 2011-12, and an initial estimate for 2012-13. It is anticipated that costs for 2012-13 will be broadly consistent with 2011-12.
Other External Costs
73. In addition to estates and IT costs, other set-up costs for the new
organisations will include those for design and recruitment, and for establishing internal systems. Costs are also expected to be incurred on establishing the new organisations’ identities and brands, and harmonising pay and conditions for staff transferring from other organisations.
74. Such costs falling outside the Department are currently estimated to be £181 million, of which about £100 million has been identified for the setup of Clinical Commissioning Groups. The cost profile for Other External Costs is shown in Table 7.
Funding for Transition Costs
75. Most of the financial resources to support transition are held at local level.
SHAs and PCTs are expected to fund their redundancy and other

Business Case for the Health and Care Modernisation Transition Programme
40
transition costs within the 2% headroom for non-recurrent spending they have been required to create. This 2% headroom is worth approximately £1.6 billion per annum and is recognised in current NHS plans. However non-recurrent spending within this amount is not restricted to transition costs.
76. Funds are also held centrally for transition costs. The initial estimate for centrally-held programme revenue and capital resources is shown in Table 8.
Table 8: Original Central Programme Resources for transition (£m)
2011/12 2012/13 Notes
Capital 107
Redundancy - Central 80 102 For DH and ALBs,
SHAs are assumed self-
financing.
Non Redundancy -
Central
50 100
Total 237 202
77. In 2011 the Department established new arrangements to govern the allocation of non-recurrent administration funds to those DH directorates and newly-established arm’s length bodies which were incurring costs on developing or setting up the new arrangements. A Special Allocations Group (SAG), comprising three DH finance directors and a representative from the Integrated Programme Office of the Transition Programme, considered cases for non-recurrent funding against criteria of affordability, value for money and alignment to Transition Programme priorities. For 2012-13 the Transition Costs Group has been established to carry out an analogous role.

Business Case for the Health and Care Modernisation Transition Programme
41
Economic Case
Summary
The total economic costs of transition in 2010-11 prices are estimated to be in the range £1.2bn - £1.3bn (excluding transfer costs), and the long term annual savings are expected to be £1.5bn per year from 2014-15 onwards. In addition to the savings that can be redirected to frontline services, there are a number of non-quantifiable benefits. For example, Clinical Commissioning Groups will give health professionals the freedom to design services around patients, the NHS Commissioning Board will ensure quality improvements through nationally agreed clinical standards, and streamlines and integrated public health services will lead to better responsiveness and democratic involvement. Overall, the economic case is such that the Department will be able to live within the Spending Review allocations, and be able to deliver the management cost reductions.
Summary of the Impact Assessments
78. The Impact Assessments (IA) for the Health and Social Care Bill 2011
assessed the benefits, costs and risks of implementing the policies that require primary legislation. It was originally published in January 2011 and revised in September 2011 for when the Bill entered the House of Lords.
79. Table 9 below shows the total costs set out in the Impact Assessment that
were assumed to be attributable to the changes in the system architecture. The full range is £1,001 million to £1,478 million, from the estimated best case to the estimated worst case. These costs are assumed to be incurred predominantly in 2011-12 and 2012-13, when SHAs and PCTs are abolished, and the NHS Commissioning Board and clinical commissioning groups are set up.

Business Case for the Health and Care Modernisation Transition Programme
42
Table 9: Impact Assessment Figures (in 2010-11 prices)
Savings and Costs £million Notes
Savings 11,989 £4.5bn in first 5 years and £1.5bn in
each of next 5 years. Para 48.
Redundancy 632 - 989 Breakdown in table 5. £195m
incurred in 2010-11.
Estates 80 - 200 Outlined in Paras 65-71.
Other Non-redundancy 289 Costs from Para 64 et seq. but
excludes items commented on
below
Total Costs 1001 - 1478
80. The best estimate of transition costs, based on the most likely level of redundancy costs is £1,179 million to £1,299 million. This includes the £195 million already spent. This is compared to a total predicted saving over the 10-year period of £11,989 million. These figures are financial costs rather than opportunity costs, are in 2010-11 prices, and are not discounted.
81. The overall savings arise from the reduction in administrative costs set out in Table 2. The benefits figures do not include the health benefits associated with the proposed changes. The Impact Assessment overall shows that the anticipated monetarised benefits are significantly larger than the associated costs.
Business Case for the Health and Care Modernisation Transition Programme
43
Table 10 Summary of the Impact assessment (2010-11 prices)
September 2011
Figures
Total costs of transition (best estimates) £1.2bn - £1.3bn
Long-term annual savings (from 2014/15 onwards) £1.5bn per year
Long-term annual admin spending (2014/15 onwards) £3.0bn
Gross savings over the transition (2010/11 – 2014/15) £4.5bn
Net savings over the transition (2010/11 – 2014/15) £3.2bn - £3.3bn
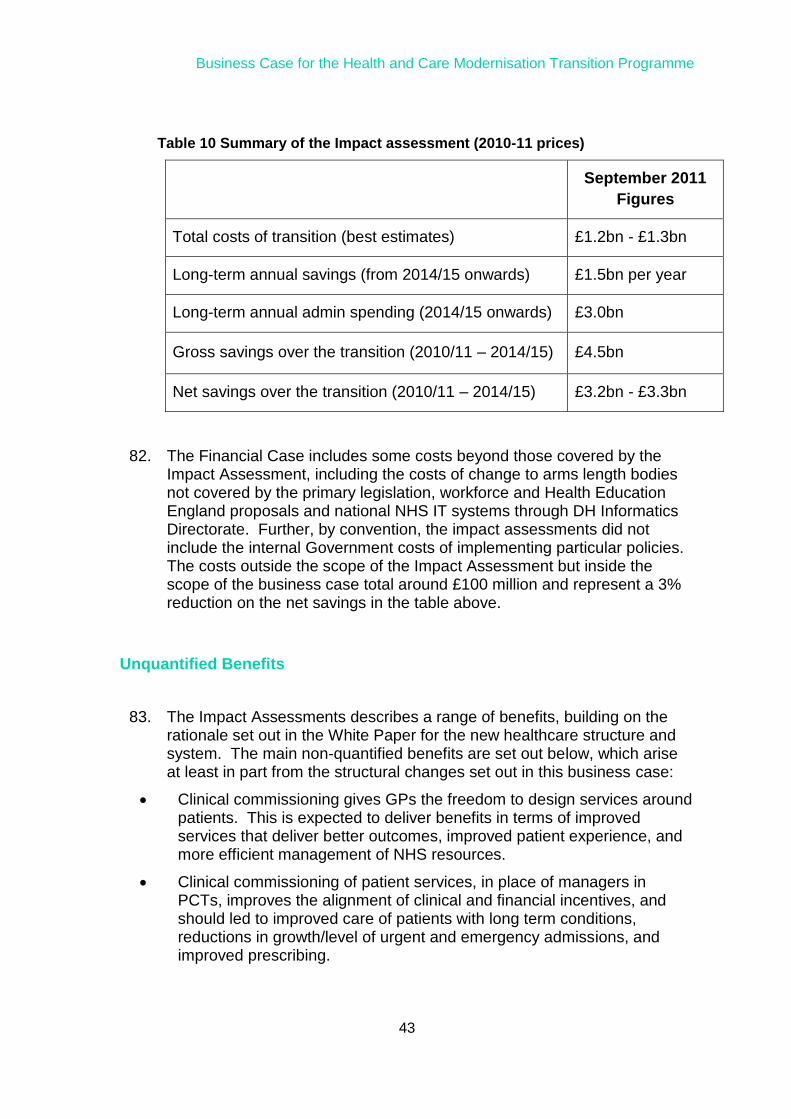
82. The Financial Case includes some costs beyond those covered by the Impact Assessment, including the costs of change to arms length bodies not covered by the primary legislation, workforce and Health Education England proposals and national NHS IT systems through DH Informatics Directorate. Further, by convention, the impact assessments did not include the internal Government costs of implementing particular policies. The costs outside the scope of the Impact Assessment but inside the scope of the business case total around £100 million and represent a 3% reduction on the net savings in the table above.
Unquantified Benefits
83. The Impact Assessments describes a range of benefits, building on the rationale set out in the White Paper for the new healthcare structure and system. The main non-quantified benefits are set out below, which arise at least in part from the structural changes set out in this business case:
Clinical commissioning gives GPs the freedom to design services around patients. This is expected to deliver benefits in terms of improved services that deliver better outcomes, improved patient experience, and more efficient management of NHS resources.
Clinical commissioning of patient services, in place of managers in PCTs, improves the alignment of clinical and financial incentives, and should led to improved care of patients with long term conditions, reductions in growth/level of urgent and emergency admissions, and improved prescribing.
Business Case for the Health and Care Modernisation Transition Programme
44
NHS Commissioning Board will ensure quality improvements through nationally agreed clinical standards, with a new legal duty for quality improvements. The Board will also be able to make additional payments in the form of a quality reward to reflect the performance of commissioning groups in relation to the quality of services, reductions in inequalities and outcomes achieved.
NHS Commissioning Board will streamline decision-making, planning and commissioning of all specialist services, providing greater consistency and reducing inequitable access to specialised services across the country. This will enable a consistent approach to service specifications to contain costs and get best value for money (e.g. agreeing single tariffs across providers).
The economic regulator will develop a more independent, transparent and stable regulatory framework for providers, increase certainty on the structure and level of prices, and strongly police anti-competitive practices to restrain the market power of large incumbent providers, which is expected to support efficiency gains in the NHS, encourage providers to be more flexibly to patient needs and support innovation.
A streamlined and integrated public health service will lead to better responsiveness, for example removing the potential for delays in responding to public health threats and emergencies and enhance the use of evidence.
Less central control and reduced bureaucracy means there is less need for intermediate tiers to communicate instructions down through the system and manage delivery.
Greater local democratic involvement in commissioning through health and wellbeing boards should ensure stronger joint working and more responsive local services. The strengthened voice of patients and the public in decisions at both the national and local level through Local Healthwatch and Healthwatch England will further ensure that services better address local needs, ultimately leading to higher levels of patient satisfaction, improved quality of services and more cost effective commissioning.
HEE will provide an opportunity to embed a single, multi-professional approach to provide professional leadership and focus on quality of education and training being commissioned, improving on the current fragmented approach. Health Education England (HEE) will also reinforce national co-ordination of education and training activity, and provide better leadership across the whole system, bringing together the interests of the professions and providers of NHS services.
Employers will have clearer ownership and involvement in the education, training and planning of their workforce through the creation of local education and training boards. They will be able to better link service planning and workforce planning, focusing on the whole workforce, while
Business Case for the Health and Care Modernisation Transition Programme
45
recognising the levels of contact with patients and service users and the varying local needs.
The Education Outcomes Framework (EOF) being developed will set out the high level principles and outcomes for achieving a world class health care education system, so for the first time the investment in education and training will be directly linked to improvements in patient care.
84. Most of these benefits will be delivered in the longer term following the transitional structural changes. The benefit realisation will be achieved through the framework agreements and NHSCB mandate and the system levers embedded into the new operating arrangements.
Business Case for the Health and Care Modernisation Transition Programme
46
Commercial Case
Summary
The Department is mostly managing the transition through internal resources together with utilising the knowledge and support from the NHS. Commercial arrangements will deliver some aspects of the work, including the set up of commissioning support organisations, establish a publicly owned company to manage and disposal of the surplus primary care estate, and developing shared service arrangements to achieve service efficiencies and financial savings. In addition, reviews have been commissioned to assess commercial efficiencies at the NHS Business Services Authority, NHS Litigation Authority and NHS Blood and Transplant, which are due to report later in 2011.
Introduction / Approach
85. The Department is mostly managing the transition through internal
resources together with utilising the knowledge and support from the NHS. This section sets out the aspects of the transition programme that require commercial procurements or the transfer of personnel and assets, with reference to their core documents.
Commercial Arrangements across the Transition Workstreams
Commissioning Support Arrangements
86. It is anticipated that Clinical Commissioning Groups will buy in, or share with other organisations, support to assist them to carry out their commissioning functions. Potential areas include business support such as finance, accounting and administration; transactional support such as planning, performance modelling and contract management; and commissioning support such as pathway redesign, service specification and establishing best practice around cost effectiveness and clinical quality.
87. Support could be bought in from commissioning support organisations,
local authorities, private and third sector bodies or joint ventures. The Department is developing a national framework and a range of support tools, and is also actively working with the PCT clusters to reshape commissioning and develop their commissioning support offerings.

Business Case for the Health and Care Modernisation Transition Programme
47
Commercial Reviews
88. A key finding of the 2010 Arm’s Length Bodies review identified that the bodies had under-exploited potential commercial opportunities. Commercial reviews were subsequently commissioned for the NHS Business Services Authority, NHS Blood and Transplant and NHS Litigation Authority. Within each of these organisations there are activities which are either similar to those already delivered by the private sector, or which could be traded in a market type environment. The reviews aim to identify commercial opportunities which can improve value for money, drive up operational efficiency and increase income
NHS Property Vehicle
89. NHS administrative estate which is not transferred to existing healthcare providers will be transferred to an NHS property vehicle (NHS PV) established as a company wholly owned by the Secretary of State for Health. Its prime focus will be efficient property management, reducing running costs and maximising the value achieved from the sale of any surplus assets.
Shared Services
90. The management of non-core services into a shared or standardised service is a cross-government strategy to help reduce administrative costs. A Shared Service Programme has been established to maximise the savings across Department, its new public health arm Public Health England (PHE) and the remaining and newly created Arms Length Bodies (ALBs), including the NHS Commissioning Board. Savings will be made by aggregating volumes of activity, standardising service specifications and, in some areas, using external skills to improve efficiency.
91. The shared services are being initially developed in the following areas:
Financial Transactions – for payroll, accounting, invoice processing and supplier maintenance, cash and debt management, and VAT returns;
HR – starters, leavers, changes, absence management, policy development, HR support; and
Procurement – contract management, e-procurement tools, catalogue data maintenance, and government procurement card admin.
Business Case for the Health and Care Modernisation Transition Programme
48
92. Each area is expected to develop separate business cases in due course.
Information Technology
93. The Information Technology elements of the transition programme are still in development and the commercial approach for any procurements will be established in the coming months. A number of IT contracts will need to be reviewed and potentially novated to different organisations.

Business Case for the Health and Care Modernisation Transition Programme
49
Management Case
Summary
This Management Case sets out how we are managing the Transition Programme, and how the Programme fits in to the wider Health and Social Care system, and the key Governance processes that are in place.
There are also sections on the functions of key Boards, Delivery Plan, Risk Management, stakeholder engagement and Gateway Review. The key decisions are taken at a hierarchy of programme boards which include the permanent secretary and NHS chief executive and senior DH and NHS directors. Each transition workstream has an SRO, programme plan, milestones and risk management arrangements. An ongoing series of stakeholder events also ensures there is wider consultation and engagement.
The programme is the largest ever undertaken in the NHS, and is being managed through best practice in Project and Programme Management, with full scrutiny by the Cabinet Office Major Projects Authority.
Transition Programme Structure
94. The Transition Programme was established by the Department to oversee and coordinate the work to design and implement the new Health and Care system to April 2013. There are 24 separately managed programmes of work, led by A Senior Responsible Owner, Programme Director and supported by a programme team. The Transition Programme governance structure, operating from September 2011, has been revised to reflect the move from system design to programme development and delivery, and is set out below:

Business Case for the Health and Care Modernisation Transition Programme
50
95. The following paragraphs describe the different work strands in more detail:
NHS Transition
96. The NHS facing programme includes:
Commissioning Board: Establishing the new NHS Commissioning Board.
Commissioning Development: responsible for ensuring a smooth transition from the current commissioning system to a new structure of Clinical Commissioning Groups. The team will oversee the development and implementation of the new commissioning architecture and the transition in the Department of Health and NHS to the new commissioning arrangements.
SHA Transition: Transition and closure of Strategic Health Authorities (SHAs) and Primary Care Trusts (PCTs), ensuring the effective

Business Case for the Health and Care Modernisation Transition Programme
51
transfer of services to new organisations and close down of discontinuing functions.
Health Education England: provision of sector-wide leadership and oversight of workforce planning, education and training in the NHS.
NHS Trust Development Authority (NTDA) and FT Pipeline: a short-life special health authority for transition that will ensure continued governance and performance management for NHS trusts who have yet to achieve Foundation Trust (FT) status, and help to manage the approval of Trusts to achieve Foundation Trust status (FT Pipeline).
Sector Regulation: creation of a new Regulator to promote patient choice and competition, set efficient prices and support continuity of service.
NHS Development: provision of overall strategic direction for the QIPP Programme, including National Clinical Workstreams such as Long Term Conditions and Urgent Care, working with the NHS and the Department on improvement, and work on commissioning for primary care.
Future State Informatics: supporting the NHS in delivering better, safer care to patients, by bringing in new computer systems and services
DH Transition Programmes
97. These programmes include:
DH Transformation and Shared Services: creation and implementation of the new Department of Health, and the delivery of shared services arrangements for business support services across DH and the ALBs.
Public Health England: creation of Public Health England, and the new Public Health system.
Local Government: establishing the new Local Government arrangements, including the design and implementation of Health and Wellbeing Boards, the establishment of Healthwatch England and local public health services.
Health Research Authority (HRA): forming the Health Research Authority (HRA) to provide a new pathway for the regulation and governance of health research, streamline regulation, create a unified approval process, and promote proportionate standards for compliance and inspection within a consistent national system of research governance.
ALB Transition: structural reorganisation of the Arm’s Length Bodies following the ALB review.
Emergency Preparedness, Resilience and Response (EPRR): setting clear principles for emergency preparedness, resilience and response.

Business Case for the Health and Care Modernisation Transition Programme
52
Social Care Programme: making services more personalised, more preventative and more focused on delivering the best outcomes for people using services.
Workforce Transition: design and safe transfer of health and social care workforce functions in the new system.
Governance and Accountabilities: establishment of the overall chain of accountability for the proper stewardship of Parliamentary funds and the accountability structures and processes in the new system.
Cross-cutting Functional Workstreams
98. The implementation programmes are supported by cross-cutting functional
workstreams. They will work in partnership with business leads in the implementation programmes to provide specialist professional advice during the design stage, and deliver the requisite changes during the implementation phase, ensuring joined-up working across the DH, ALBs and the NHS. The workstreams are as follows:
Finance
NHS Estates and establishing a NHS Property Vehicle
Informatics Transition
IT enabled Estates for DH and ALBs
HR
Communications and Stakeholder management
Equalities.
Executive Board
99. The Executive Board’s purpose when considering Transition business is:
to oversee the overall design, strategic approach, planning and implementation of the new direction for the health and care system, ensuring the phased alignment of system-wide organisational changes, mitigation of risks to business continuity and financial control and co-ordinated engagement and communications. It ensures that at a strategic level, effective people and programme disciplines are in place across all parts of the Transition Programme with the aim of ensuring successful delivery of the new health and care system.
Business Case for the Health and Care Modernisation Transition Programme
53
100. In particular, the Executive Board:
ensures transition is coordinated between NHS, DH, ALBs and local government as part of an integrated plan;
provides a single point for joint decision making for all aspects of Transition, which require senior level decisions; and
provides the overall governance of the Transition Programme ensuring the programme delivers successfully, managing the risks and issues effectively, though most routine programme governance is delegated to the Transition Programme SRO.
Transition Board for Cross Cutting Functions
101. This Board oversees and assures the delivery of the cross cutting functional work programmes, ensuring they deliver the necessary functional change, and are fully integrated with the DH and NHS programmes they support. It meets monthly, providing reports and escalating issues to the Executive Board or other bodies as appropriate, and is chaired by the Transition SRO (DH’s Director General of Policy, Strategy and Finance). Its remit is to:
ensure functional designs, transition policies and decisions are aligned to the system needs, and agreed as necessary by the right decision makers;
ensure each workstream is making good progress to the overall integrated programme and implementation plan, and dependencies across the programme are identified, tracked and managed;
ensure risks to progress, costs and benefits are being managed effectively;
escalate risks, issues to Executive Board as necessary; and
formally report status and progress to plan to the Executive Board every month.
DH, Social Care and Public Health Transition Board
102. This Board oversees the design and delivery of each of the DH, Public
Health and Local Government component programmes. Specifically, it ensures the design and implementation of the DH, Public Health and Social Care structures and systems, and the transition to Local Government, are consistent with the needs of the new Health and Care system, and with the transition to the new NHS system.
Business Case for the Health and Care Modernisation Transition Programme
54
103. The Board covers the following workstreams in support of the transition:
DH Transformation and the delivery of shared services across the system;
delivery of Public Health England and the wider Public Health system, including the PH transition into Local Government;
transition of the wider health and care changes for Local Government, including establishment of Health and Wellbeing Boards, and new Healthwatch;
development and implementation of Social Care changes;
implementation of the new Health Research Authority;
transition of the current DH ALBs.
NHS Future Systems Executive (and NHS Transitional Executive Forum)
104. This Board oversees the design and delivery of each of the NHS
component programmes, ensuring they design and implement the new NHS organisations and structures as required to meet the policy intention, and that they work consistently as part of one new aligned NHS system.
105. This Board feeds into the NHS Transitional Executive Forum, which will
ensure the new NHS structures work together as an integrated whole, interact effectively as part of the wider Health and Care system, and that the current NHS structures transition effectively to the new system and close down effectively.
106. The NHS Future Systems Executive covers the following workstreams in
support of the Transition:
NHS Commissioning Board;
commissioning development, including commissioning architecture;
NTDA and FT pipeline;
Monitor changes and economic regulation regime;
HEE and education and training;
Future Informatics organisation;
future design of shared services for the NHS; and
development of leadership and systems across the system.

Business Case for the Health and Care Modernisation Transition Programme
55
Implementation Programme Boards
107. Each of the implementation programmes have their own governance
arrangements and associated boards (e.g. Commissioning Development Board and Public Health Programme Board).
108. The role of each Board is to govern and drive the design and delivery of
each of the Programmes according to the policy and legislative framework set by Ministers, and within the design framework and context set by the Executive Board. Each Board identifies risks and interdependencies and escalates issues to the DH Transition Programme Board, NHS Future System Executive or Transition Board for Cross Cutting Functions as appropriate, and if necessary, to the Executive Board.
Delivery Plan
109. There is a high level Transition Programme Roadmap, as well as more
detailed delivery plans for each of the individual programmes and workstreams. The following is a snapshot of the high level summary that shows the complexity of the programme and the inter-relationships between the different workstreams.
2011 2012 2013
Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May
QH Initial Occupation
Health & Care Transition Programme – High Level RoadmapHSC Transition Programme Plan Update Annex A
PROTECT: Management
Full System of Health & Wellbeing Boards
Fully Operational
NTDA SpHA Established
NTDA Commence Formal Role
Dev. Implementation Plan
Establish Health & Wellbeing Network Health & Wellbeing Board JSNA/JHWS Guidance Available
NTDA Fully Staffed
LA & local Healthwatch
Organisations take on
NHS Advocacy
Olympics & Para Olympics
Develop Governance Guidance
Run Programme of Continuous Learning & Support
Staff Consultation Response – TBC
NTDA Preparatory Running
Local Healthwatch Organisations Established
Healthwatch England Organisation Established
Local Healthwatch Organisations Preparatory Running
Senior Recruitment Exec Team Appointed - TBC
PHE Commence Formal Role
NTA & HPA Abolished
PHE Established in Shadow Form
Agree 2013/14 Business Plan & Budget
IT In Place
HQ Building Accommodation In Place
Exec Agency Business Case Agreed by CST & MCO
Publish draft Framework, Operating
Model, Org. Structure
PTP Agreed
CEO & Exec Team Appointed
Full Staff Consultation on
Structure
PHE Staff Appointed
System Testing & Training
Parliamentary Passage
Health and Social Care Bill Receives Royal Assent - TBC
Re-committal Lords 3rd Reading - TBCCommons 3rd Reading
Inst. Issued & Regulations Drafted
NHS CB & HRA Regs Laid
HRA SpHA Est’d – 1 Dec
NTDA & HEE Regs Laid - TBC
NTDA HEE SpHA Est’ed – TBC
Health and Social Care Act/ Secondary Legislation - TBC
Appointments Commission Abolished
Shadow Health & Wellbeing Boards In Place
HEE SpHA Established
HEE Commence Formal Role
Agreed Framework
DH Staff Consultation
Completed
Chair, NEDs and CEO Recruitment
Chair & NEDs Appointed
Agreed Operating Model
HEE Business Plan 2012/13 Agreed
Staff Consultation Response Published –
29 Aug
Transfer of Staff - Main
Transfer of Functions from NPSA & Appointing Authority Functions from SHAs
Commence Organisational Design Work
Monitor/Regulator Fully Operational
FT Provider Licenses In Place
Monitor Distress & Failure Regime Go Live for FTsTransition Dates Agreed
NHS CB Re-Established as NDPB
NHS CB able to Authorise Commissioning Groups
NHS CB Chair, NED & Directors Appointed
NHS CB Full Go Live -takes on Full Statutory
Functions & Financial
Responsibility
All SHAs & PCTs Abolished
NHS CB Staffed
Launch Discrete NHS CB Accounting System
Mandate Published – for 2013/14
Agree 2012/13 Budget baseline
Staff Consultation
Response
Published
NDPB Framework Agreement Agreed
Internally Agreed Framework
Executive Team & Board Recruitment
NHS CB Establishes & Authorises Commissioning Groups
NHS CB Preparatory Running
NHS Institute & NPSA Abolished - TBC
DH MoU Signed-off
Maple Street Refurb Completed
Staff Recruitment & TransfersFunctions Proposals Presented to Senior Team
STATUS
Build, Implement & Test EPRR Arrangements (PHE & NHS CB)New EPRR Arrangements Live
HEE Preparatory Running
Produce Detailed Operating Model
PHE Preparatory Running
Tfr Staff & Recruitment
Emergency Preparedness - Pre Olympics Testing
HRA Preparatory Running
Take On NPSA Functions - TBC
H&SC Bill
Dilnot Report Published SC WP & Draft Bill Published - TBC Parliamentary Passage - TBC
Decision on Buildings for NTDA in -London & Leeds
NHS CB SpHA Est’d – 31 Oct
NHS CB SpHA Established
Working Draft Framework
Approach to Competition Agreed
Interim DH Accountabilities Framework In Place
Network MGT Boards In Shadow
HEE & Networks Financial Roles & Responsibilities Agreed
Network’s Go Live
CEO Appointed
Exec Team AppointedExec Team Recruitment
Staff Consultation
HEE Functions Agreed
Agreed Org. Structure Design
V1.2 15-09-2011
SC&H Bill
NHS Commissioning
Board
NHS Other
Legislation &
Finance
Secondary
Finance
Monitor
DH
NTDA
HEE/Networks
Public Health England
Emergency Preparedness
DH Other
HRA
Informatics
Healthwatch
(England & Local)
Health & Wellbeing
Boards
Working Draft Framework
Chief Exec & Exec Team Appointed - TBC
Monitor Essential Services Regime Go LivePricing Roles & Responsibilities Agreed - TBC MoU In Place with NHSCB - TBC
New Operation Model in Place for CCP
Working Draft Framework
Network DevelopmentNetworks Mirror End State Operations
Agreed Costing & Tariff Management Process
First JHWS JSNA for 2014/15
Action Learning Sets – for early Imkplementor BoardsSupport for Elected Members
Develop Benchmarking Measures
Self Assessment of Local Government Readiness (SALGR)
SALGR SALGR SALGR SALGR
Acting Chief Exec & Acting Finance Director
HRA Established (Health Service Purposes)
Framework/MoU In PlaceShadow Term Arrangements Agreed
Shared Service Functions In PlaceNRES Financial Processes & Budget transferred to HRANew HO
Location
identified
NRES HO Tfrs to New Location
Current IRAS & RED contracts Tfr to HRA
Commence Shared Services Engagement
Website Development
Development Work
DG Structure SCS 1 AppointedDH Staff Moves
Redraft of Business Case Completed Majority of Bus. Case Costs Confirmed Bus. Case update – Interim Cost Outturn Bus. Case update – Interim Cost Outturn
Recruitment Process
Lords 2nd Reading 10 Oct TBC
Agreed Framework
Agreed IT Spec.
PTP Published
Chair & 1 NED Appointed CEO Appointed 5 NEDs Appointed
Commence HR Staff Process Tfr of Appointment Commission Staff
Location ready for occupancy
Working Draft Framework
Decision on Location - TBC
Monitor Additional Accommodation Available
HEE Decision on Location
Abolish GSCC Abolish CHRE
HEE Draft Operating Model
Sign-off EPRR Model
Concordat
Procurement Business Case Signed off
Directors Appointed
CEO In Post
Section 28 Staff Consultation Commences
Final DH Accountabilities Framework In Place
Informatics Key Organisational Transition .
Informatics Systems Transition (NHS)
Clarify budgets for routine and programme operation in
2012-13
Define arrangements for InformaticsDesign support arrangements for continuity of
local informatics capability
Latest date to get org design for coding into specification
Latest date to get funding approval for org design changes
IMS 3 Contract Award
Decision on national informatics functions destination/futures Closure of Informatics Directorate
and transfer of all continuing
informatics functions to new host
organisations completeClarification of main organisation design assumptions by the NHS CB
Latest dates for cross DH/NHS HR announcement on destination
organisations
HEE SRO Appointment
NHS PVFull Business Case Signed-off
High Level Commercial Strategy Completed
Senior Board Appts.
Commence HR ConsultationWaves of Staff Transfers
Narrative Narrative Narrative Narrative NarrativeNarrative
Activity Milestone Critical Activity Critical Milestone Go Live/Est Milestone Key Sequencing Completed Milestones & Activities At Risk Milestones Slipped Milestones & ActivitiesNarrative Narrative Narrative
Narrative

Business Case for the Health and Care Modernisation Transition Programme
56
110. The Listening Exercise and the subsequent Government Response to the NHS Future Forum’s report did impact quite significantly on the original timetable for change. The new timings allow for a more phased approach to transition as follows:
October 2011: NHS Commissioning Board established in shadow form as a special health authority, and SHA cluster arrangements in place.
During 2012: Health Education England and the NHS Trust Development Authority are established as Special Health Authorities, but in shadow form, without full functions.
April 2012: The next step in extending the choice of Any Qualified Provider, which will be phased in gradually.
By October 2012: NHS Commissioning Board is established as an independent statutory body, but initially only carries out limited functions – in particular, establishing and authorising Clinical Commissioning Groups.
October 2012: Monitor starts to take on its new regulatory functions, and HealthWatch England and local HealthWatch are established.
April 2013: SHAs and PCTs are abolished and the NHS Commissioning Board takes on its full functions. Health Education England takes over SHAs’ responsibilities for education and training. The NHS Trust Development Authority takes over SHA responsibilities for the FT pipeline and for the overall governance of NHS Trusts. Public Health England is established, and a full system of Clinical Commissioning Groups is established. But the NHS Commissioning Board will not authorise groups to take on their responsibilities until they are ready. Health and wellbeing boards are established in upper tier local authorities in England and Local HealthWatch established.
April 2014: Our expectation is that the remaining NHS Trusts will be authorised as Foundation Trusts by April 2014. But if any Trust is not ready, it will continue to work towards FT status under new management arrangements.
April 2016: Monitor’s transitional powers of oversight over Foundation Trusts will be reviewed (except for newly authorised FTs, where Monitor’s oversight will continue until two years after the authorisation date if that is later).
Business Case for the Health and Care Modernisation Transition Programme
57
Business Assurance Arrangements
Internal review
111. All deliverables will be reviewed and regularly approved by:
the relevant Programme/ Workstream Board; and
the Transition Board for Cross Cutting Functions, which confirms that proposals are consistent and integrated with all programmes and workstreams.
112. Some key deliverables will also require sign off by:
NHS Transitional Executive Forum, DH, Social Care and Local Government Board and / or DH Management Committee; and
(Transition) Executive Board.
113. An independent programme management expert, Ian Andrews, provides advice and Non-Executive Director scrutiny to the SROs and Transition Director.
114. Progress on transition is a standing item on the Department Board, and
the Board receives a regular status report on the Programme.
External review and assurance
115. The programme is subject to review from several sources:
Ministers review the programme on a regular basis, with Earl Howe PS(Q) appointed as lead Minister on Transition.
The programmes comprising the Transition Programme are subject to peer review through the long-established Gateway Review process, and the overall Transition Programme through the Cabinet Office Major Projects Authority and Major Projects Review Group (MPRG) processes.
Within Cabinet Office, the Major Projects Authority (MPA) oversees the Gateway Process to ensure best value for money and efficient delivery of major government projects. The Transition Programme is included within the Government Major Programmes and Project (GMPP) Portfolio, and quarterly reports are provided to the MPA by the Department of Health.
The OGC Gateway Process examines programmes and projects at key decision points in their lifecycle. It looks ahead to provide delivery confidence that they can progress to the next stage; the process is best practice in central government, including the health sector.

Business Case for the Health and Care Modernisation Transition Programme
58
Risk Management
116. Each SRO and Programme Board is responsible, supported by their
project support team, for determining, establishing and managing risks and issues within the wider programme framework and governance. They will maintain a risk and issues register covering their areas of responsibility and report these at regular intervals – alongside their Programme Status Reports which are submitted to their relevant senior Board. Risks and issues can be escalated through this process for consideration by the senior board, executives and the Transition SRO. To support the senior boards in their responsibility for coordinating risks and issues the Integrated Programme Office has established, and maintains, Transition Programme-wide risk and issues registers, incorporating key risks across the programme.
117. This register is updated on a cyclical basis, using monthly updates which
have been approved by the respective SROs and Programme Boards, discussing areas of concern with representatives from each of the programme teams or workstreams. A number of key strategic risks are included in the Departmental Risk Register, which is reviewed by the Executive Board and Transition risks are also escalated to the Departmental Board as appropriate.
Stakeholder engagement
118. As part of the staff engagement and stakeholder plans each SHA has
hosted a ‘Transition Event’. SHAs have also hosted a series of assurance events, where DH leaders held sessions with representatives of local stakeholders, including PCTs, acute NHS and FTs, community and independent sector providers, local authorities and GP consortia, to explore the key challenges in the region.
119. Regular engagement events continue with Local Government and third
sector organisations, along with a series of ministerial visits.
120. Consultations: Significant stakeholder and public engagement has taken place around the NHS White paper with the following associated consultations:
Healthy lives, healthy people: consultation on the funding and commissioning routes for public health.
Healthy lives, healthy people: transparency in outcomes, proposals for a public health outcomes framework.
Healthy lives, healthy people: our strategy for public health in England – White Paper consultation.
Liberating the NHS: developing the healthcare workforce.

Business Case for the Health and Care Modernisation Transition Programme
59
A consultation on proposals - transparency in outcomes: a framework for adult social care.
Liberating the NHS: Greater choice and control. a consultation on proposals.
Equity and excellence: liberating the NHS.
Liberating the NHS: commissioning for patients - consultation on proposals.
Liberating the NHS: increasing democratic legitimacy in health.
Liberating the NHS: regulating healthcare providers
Benefit Realisation Plan
121. The main quantifiable benefits from the planned structural reforms are
financial, primarily from the reduction in administrative costs from the closure of SHAs and PCTs, releasing some 24,500 staff. Indirect benefits will arise from the organisation changes, as they will facilitate or stimulate broader changes in clinical quality and efficiency (including the QIPP initiatives), across the NHS.
122. The intended wider benefits are:
better patient outcomes;
better alignment to patient demands and needs, and more clinical input;
improvement in response to public health threats and emergencies
improved public health outcomes and a reduction in health inequalities
reduced numbers of people living with preventable ill health and people dying prematurely whilst reducing the gap between communities
more responsive system, with stronger levers, and
more local decisions.
123. The ability to monitor and measure the benefits is the responsibility of the new organisations operations, through their Operating Frameworks and Mandates. In particular, the NHS Commissioning Board will need to monitor overall NHS performance and track the improvements, and the Bill’s duty to secure quality improvements will be incorporated into the design of Clinical Commissioning Groups, and evaluated as part of their authorisation process.

Business Case for the Health and Care Modernisation Transition Programme
60
124. The NHS Outcome Framework is a key part of the future NHS system to provide macro quality performance measures, and corresponding indicators.
125. During transition, an NHS early warning system is being developed to
monitor NHS performance on a monthly / quarterly basis.
Delivering Cost Benefits
126. Budgets are being set for the Health and Care System on the basis there
will be a reduction of one-third in administrative spending covering the functions of the Department of Health, SHAs, PCTs and ALBs that are not directly frontline services.
127. The one-third real reduction in administrative spending is equivalent to a
25.8% nominal reduction in total resources for the management of the system.
128. To achieve these reductions, PCTs and SHAs will be abolished and
Clinical Commissioning Groups and the NHS Commissioning Board will be created, together with Health and Wellbeing Boards, and new public health responsibilities in local authorities.
129. These cost benefits will be realised by the system keeping in financial
balance, and living within the reduced financial envelopes.
Realising Non-financial Benefits by key area
130. In addition to realising cost benefits as above, there are a substantial
number of non financial benefits. In many areas it is difficult to attribute these to a particular part of the system, however the following does provide an indicative benefits realisation for the key areas of activity:
Commissioning for Patients (Clinical Commissioning Groups and the National Commissioning Board)
131. While the main monetised benefit for this area are the reductions in
administration savings referred to above, the main non-monetised benefits are from improved clinical engagement, improved outcomes and more responsive and co-ordinated care. There are further additional benefits from the reduced variation in outpatient referrals and elective activity, improved care of patients with long term conditions, reductions in the level of urgent and emergency admissions, and improved prescribing.
Business Case for the Health and Care Modernisation Transition Programme
61
Provider Regulation
132. The new more stable and transparent regulatory regime will support
quality gains as providers face a clear set of incentives to improve.
Increasing local democratic legitimacy in Health (Health and Well Being Boards)
133. Greater democratic involvement, and requiring the attendance of key commissioning partners, elected representatives and local HealthWatch, will ensure stronger joint working, with services being tailored more towards local needs and priorities. This will be supported by the enhanced Joint Strategic Needs Assessment and joint health and wellbeing strategy, which should serve to identify and address needs across an area. Ultimately, this will lead to higher levels of patient satisfaction, improved quality of services and more cost effective commissioning.
Healthwatch
134. The main non financial benefits will be from improvements in the patient
experience, and health outcomes stemming from stronger public voice. Complaints advocacy will also lead to improved services and patient confidence in the Health and Social Care system. There should also be a reduced likelihood of significant ‘adverse events’ through better information flows.
Public Health:
135. Incorporating both national and local structures should provide a
streamlined and efficient service, which will make a positive impact on health and improve health outcomes.
Delivery of Non-Financial Benefits
136. The DH will publish a set of Outcomes Frameworks which will define the
outcomes for which we will hold the health and care system to account. Each year the Secretary of State will set out his objectives for the NHS Commissioning Board in the Mandate. The Department's ALBs, including the NHS Commissioning Board will be held to account to deliver the outcomes and objectives set out by the Department effectively, efficiently and economically. Transparent, outcome-focused indicators will enable the DH and the NHS and the public to understand progress. Each year

Business Case for the Health and Care Modernisation Transition Programme
62
the Secretary of State will publish an annual report on the NHS which will set out a review of the NHS's achievements, that will provide evidence of financial and non financial benefits realisation.

Business Case for the Health and Care Modernisation Transition Programme
63
Appendix A
Changes adopted following the NHS Future Forum’s report
The NHS Future Forum was set up by the Secretary of State in April 2011, comprising of a group of 45 leading professionals across health and social care. It focused on four themes:
how advice from a range of healthcare professions can improve patient care;
how to ensure public accountability and patient involvement in the new system;
the role of choice and competition in improving the quality of care; and
how new arrangements for education and training can support the modernisation process.
The Forum reported to the Government in June 2011 and the key changes set out in the Government response to the Future Forum report are below:
GP consortia will now be called “clinical commissioning groups”, and will have governing bodies with at least one nurse, one specialist doctor and lay members;
where a clinical commissioning group is ready and willing, it will take on commissioning responsibility from April 2013; if it is not ready by that date, the local arms of the NHS Commissioning Board will commission on its behalf;
commissioners will be supported by clinical networks and clinical senates, both hosted by the NHS Commissioning Board;
there will be clearer duties across the system to involve patients, the public and carers;
foundation trusts will have public board meetings;
a strengthened role for health and wellbeing boards in driving local commissioning;
strengthening the role of HealthWatch England by ensuring that other bodies at the national level need to respond in writing to its advice;
Monitor’s core duty will be to protect and promote the interests of patients – not to promote competition as if it were an end in itself;
there will be further safeguards against price competition, cherry picking and privatisation;
there will be stronger duties on commissioners to promote, and Monitor to support, care that is integrated around the needs of users; and

Business Case for the Health and Care Modernisation Transition Programme
64
Public Health England will be established as an Executive Agency rather than a core part of the Department of Health.

Business Case for the Health and Care Modernisation Transition Programme
65
Appendix B
Accountabilities in the New Structure
The key accountabilities in the new structures are set out in the Accountabilities Statement for the Department of Health. A brief overview summary is provided below. Ministers will retain ultimate accountability for the health service: as now, they will be responsible for setting strategic direction, overseeing the system and for accounting to Parliament. The Bill, however, significantly reduces their role and that of the Department, in day-to-day operational management. Department of Health’s the Permanent Secretary is accountable to Parliament for the proper stewardship of the resources assigned to the Department by the Treasury through the Spending Review and voted by Parliament. Her responsibilities are set out in the Treasury guidance Managing Public Money. The Department’s Accounting Officer appoints an Accounting Officer for each ALB, with the exception of the NHS Commissioning Board where the Health and Social Care Bill provides directly for the Chief Executive of the Board to be its Accounting Officer. Each ALB Accounting Officer will be held to account for the stewardship of public money and assets and the delivery of the ALB’s objectives and outcomes as agreed with the Department. For all ALBs, a framework agreement will set out their responsibilities and delegations, and ALBs are expected to hold open board meetings and make papers available on their websites. CCGs will be accountable to the NHSCB for the outcomes they deliver for patients and their stewardship of public resources. The NHSCB Accounting Officer will appoint an Accountable Officer for each CCG, and they will hold specific responsibilities for promoting continuous improvement in the quality of the services it commissions and providing good value for money.
Business Case for the Health and Care Modernisation Transition Programme
66
Appendix C
Other Arm’s Length Bodies – roles from April 2013
Key: ENDPB = Executive Non Departmental Public Body
SpHA = Special Health Authority
ALB Category Role
Care Quality
Commission
(CQC)
ENDPB CQC is the independent regulator of health and adult
social care providers in England. All providers of
regulated activities, including NHS and independent
providers, have to register with CQC and meet a set
of essential requirements of safety and quality. CQC
has independent enforcement powers where
providers are not meeting the requirements and
operate a joint licensing regime with Monitor. Current
responsibility of assessing NHS commissioning
moves to the NHS Commissioning Board. In the
future, it will receive functions from NIGB, and may
also receive functions from other organisations, e.g.
HTA and HFEA
It will also be the host organisation for Healthwatch
England, which will operate as a statutory committee
of CQC and act as the independent national
champion for health and social care consumers.

Business Case for the Health and Care Modernisation Transition Programme
67
Health Research
Authority (HRA)
ENDPB The role of the HRA is to protect and promote public
and patient interests in health research, streamlining
regulation to facilitate appropriate research, improving
health and helping to make it cost-effective to do
research in the UK.
It has been initially established as a Special Health
Authority from December 2011. HRA has the National
Research Ethics Service (NRES) as its core and has
taken on the functions which have been the
responsibility of the National Patient Safety Agency. In
due course, it will perform the Secretary of State’s
function of approving the processing of patient
information for medical research. Subject to
legislation, HRA will be established as a Non
Departmental Public Body (NDPB), which will enable
it to take on more functions. There will be a
consultation on the future of the Human Fertilization
and Embryology Authority to determine if its research-
related functions should pass to the HRA.
Health & Social
Care Information
Centre (HSCIC)
ENDPB The Information Centre is the national repository for
information collected from NHS and social care
organisations in England. It collects, joins up and
publishes information in an anonymised and de-
identified form so that it can be used for many
purposes (including to enable more integrated
provision of care, for public accountability and to
support research.) HSCIC will change status from a
special health authority to an ENDPB in April 2013.
Human
Fertilisation &
Embryology
Authority (HFEA)
ENDPB The Human Fertilisation & Embryology Authority
licences and monitors in vitro fertilisation (IVF), donor
insemination and human embryo research in clinics,
regulates the storage of sperm, eggs and embryos.
The ALB review recommended that HFEA should be
abolished as an ALB and its functions transferred to
other regulators by the end of the current Parliament.
DH is examining the practicalities and legal
implications of how to divide the functions between the
proposed Health Research Authority and the CQC.

Business Case for the Health and Care Modernisation Transition Programme
68
Human Tissue
Authority (HTA)
ENDPB The Human Tissue Authority is responsible for
implementing the Human Tissue Act and is a
Competent Authority for the EU Tissue and Cells
Directive. It regulates activities such as anatomical
and post-mortem examinations, transplantations and
the storage of human material for education, training
and research. The ALB review recommended that
HTA should be abolished as an ALB and its functions
transferred to other regulators by the end of the
current Parliament. DH is examining the practicalities
and legal implications of how to divide the functions
between the proposed Health Research Authority and
the CQC.
National Institute
for Health & Care
Excellence (NICE)
ENDPB NICE provides guidance, sets quality standards and
manages a national database of best practice for the
NHS in England to improve people's health, prevent
and treat ill health. Its remit is being extended to
adults and children’s social care. NICE will change
status from a special health authority to an ENDPB in
April 2013.
NHS Blood &
Transplant
(NHS BT)
SpHA NHSBT is responsible for the provision of a reliable,
efficient supply of blood to hospitals in England and
North Wales. It is also the organ donation
organisation for the UK and is responsible for
matching and allocating donated organs. NHSBT will
seek opportunities to become more commercially
effective.
NHS Business
Services Authority
(NHS BSA)
SpHA BSA is the main processing facility for payment,
reimbursement, remuneration and reconciliation for
NHS patients, employees and affiliated parties. This
includes the remuneration of Community Pharmacists,
Dentists and administration of the NHS pensions
scheme alongside a range of other transactional
functions. It has been subject to a review examining
its potential for increased commercial opportunities.
NHS Litigation
Authority (NHS LA)
SpHA NHSLA’s main role is to administer five indemnity
schemes on behalf of Secretary of State under which
NHS bodies pool some of their clinical and non-
clinical liabilities. It has been subject to a review
examining commercial efficiencies.

Business Case for the Health and Care Modernisation Transition Programme
69
Medicines &
Healthcare
Products
Regulatory Agency
(MHRA)
Executive
Agency
The MHRA protects public health through regulation
of medicines and devices, by helping users to
understand their risks and benefits, and by
encouraging and facilitating developments in products
that will benefit people. It will take on the Central
Alerting System (CAS) from NPSA; the Research
Capability Programme (RCP); and, the National
Institute for Biological Standards and Control (NIBSC)
from HPA.
Arm’s Length Bodies leaving the system
ALB Name Category Function Transfers
Alcohol Education and Research Council
AERC
ENDPB The assets of AERC have been transferred to a new independent charity, Alcohol Research UK, which was launched in September 2011, as part of the cross-government policy to reduce the harm from alcohol misuse. The residual body will be abolished by the end of July 2012.
Appointments Commission
AC
ENDPB Will close by the end of October 2012 as an ALB in view of the substantial reduction in the number of appointments required. The remaining appointment work will transfer to DH, the NHS CB and the NTDA. Secretary of State and Privy Council will, in future, retain powers of appointment
Council for Healthcare Regulatory Excellence
CHRE
ENDPB This will be made a self-funding body, by charging a levy on regulators by the end of September 2012. Its role will be extended role to set standards for and quality assure voluntary registers. It will be renamed the Professional Standards Authority (PSA)
General Social Care Council
GSCC
ENDPB The role of the regulation of social workers in England to the Health Professions Council (HPC) will be transferred to and will be renamed the Health and Care Professions Council (HCPC) to reflect its remit across health and social care. GSCC will close at the end of July 2012
Health Protection Agency
HPA
ENDPB HPA will close as a statutory organisation by April 2013 and transfer functions to the Secretary of State as part of the new Public Health England (PHE)
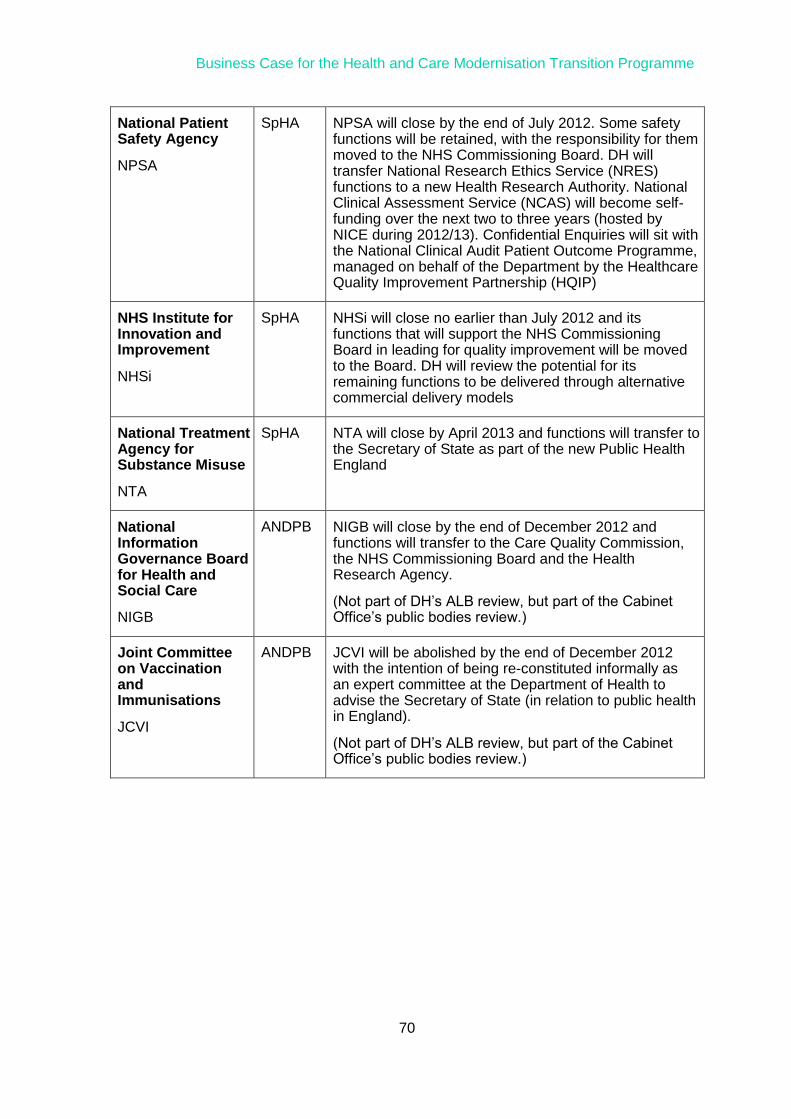
Business Case for the Health and Care Modernisation Transition Programme
70
National Patient Safety Agency
NPSA
SpHA NPSA will close by the end of July 2012. Some safety functions will be retained, with the responsibility for them moved to the NHS Commissioning Board. DH will transfer National Research Ethics Service (NRES) functions to a new Health Research Authority. National Clinical Assessment Service (NCAS) will become self-funding over the next two to three years (hosted by NICE during 2012/13). Confidential Enquiries will sit with the National Clinical Audit Patient Outcome Programme, managed on behalf of the Department by the Healthcare Quality Improvement Partnership (HQIP)
NHS Institute for Innovation and Improvement
NHSi
SpHA NHSi will close no earlier than July 2012 and its functions that will support the NHS Commissioning Board in leading for quality improvement will be moved to the Board. DH will review the potential for its remaining functions to be delivered through alternative commercial delivery models
National Treatment Agency for Substance Misuse
NTA
SpHA NTA will close by April 2013 and functions will transfer to the Secretary of State as part of the new Public Health England
National Information Governance Board for Health and Social Care
NIGB
ANDPB NIGB will close by the end of December 2012 and functions will transfer to the Care Quality Commission, the NHS Commissioning Board and the Health Research Agency.
(Not part of DH’s ALB review, but part of the Cabinet Office’s public bodies review.)
Joint Committee on Vaccination and Immunisations
JCVI
ANDPB JCVI will be abolished by the end of December 2012 with the intention of being re-constituted informally as an expert committee at the Department of Health to advise the Secretary of State (in relation to public health in England).
(Not part of DH’s ALB review, but part of the Cabinet Office’s public bodies review.)


















