Building Blocks Notes

of 38
Transcript of Building Blocks Notes
-
8/3/2019 Building Blocks Notes
1/38
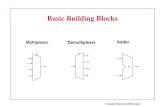
Building Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongBuilding Blocks of A StrongLocal Health SystemLocal Health SystemLocal Health SystemLocal Health SystemLocal Health SystemLocal Health SystemLocal Health SystemLocal Health System
Lectured by
Bien Eli Nillos, MDProject Associate Zuellig Family Foundation
Assistant Professor USLS COM, Family and Community MedicineFormer Doctor to the Barrios Department of Health
HEALTH FINANCING SUMMIT
Nov. 12, 2011
University of Saint La SalleAsian Institute of Management
-
8/3/2019 Building Blocks Notes
2/38
What is a Local Health System?
All the activitieswhose primarypurpose is topromote, restoreor maintainhealth. (WHO,2000)
It involves the formal health services such as primary, secondary and tertiary care,public health services, and public, private for profit and private non-profitinsurance companies and service providers, as well as traditional healers, overthe counter medications, informal or charity home care, health promotion andhealth enhancing interventions like roads, occupational and environmental
safety. It encompasses several political and civil organizations such as healthand social committees, working parties, commissioning bodies, patient advocacygroups and consumer protection agencies as well as national licensing andregulatory bodies. (WHO, 2000).
-
8/3/2019 Building Blocks Notes
3/38
All health systems may be thought of as the articulation to be based on threeelements.(Tobar, 1998): A) management model, B) financing model, C) caremodel. Figure 1 is a diagram showing the components of any health system:
-
8/3/2019 Building Blocks Notes
4/38
The diagram above shows the complex relationship between the health system andits determinants as well as the different sectors and sub-sectors within and outsidethe health system which impact health.
A health system has the following functions:
Financing;Organization and delivery;
Regulation;
Stewardship;
Ability to modify consumer and provider behavior through persuasion;
Ethics and values.
A health sector is smaller in scope than a health system. It is the part of theeconomy related to the demand for health services from different individuals,
communities, organizations and institutions (Bitrn et al, 2010). The health sectorincludes policies, service provision, production or import /export of goods, flow offunds, education of providers, etc. At the core of the health sector are the clients forwhich the health sector exists.
Important health determinants outside the health sector include population,environment, education level, behavior, lifestyle, and infrastructure.
-
8/3/2019 Building Blocks Notes
5/38
To achieve their goals, all health systems have to carry out some basic functions,regardless
of how they are organized: they have to provide services; develop health workersand other
key resources; mobilize and allocate finances, and ensure health system leadershipand
governance (also known as stewardship, which is about oversight and guidance ofthe whole
system).
-
8/3/2019 Building Blocks Notes
6/38
There is mounting evidence that health systems that can deliver services equitablyand efficiently are critical to the achievement of national and global health goals,both in terms of communicable diseases and maternal and perinatal health, butalso, critically, for the prevention and management of chronic and non-communicable diseases. Global health initiatives now incorporate attention to health
systems strengthening into the support provided to countries. However, there is anurgent need for research on all aspects of health system performance, fromunderstanding the dimensions and nature of health system constraints, todeveloping innovative strategies for strengthening health systems, translating theseinto action on the ground and evaluating to assure continuous improvement,enhanced efficiency and effectiveness.
A health system, like any other system, is a set of inter-connected parts that mustfunction
together to be effective. Changes in one area have repercussions elsewhere.Improvements
in one area cannot be achieved without contributions from the others. Interactionbetween
building blocks is essential for achieving better health outcomes.
-
8/3/2019 Building Blocks Notes
7/38
Health services
Good health services are those which delivereffective, safe, quality personal and non-personalhealth interventions to those who need them, whenand where needed, with minimum waste ofresources.
-
8/3/2019 Building Blocks Notes
8/38
When managing health systems and services, the nature of what has to bemanaged is remarkably similar across many different settings. All programmes,projects, facilities and area health authorities, whether public or private, have tomanage the following 3 things:
1. volume and coverage of services to achieve universal access2. inputs or resources (e.g. staff, budgets, information, drugs, supplies, equipment,buildings)3. external relations and partners (e.g. other providers, other sectors, users ofservices, donors)
-
8/3/2019 Building Blocks Notes
9/38
The actions and decisions of health managersinfluence many things: where facilities are located
when they are open
how they are staffed, funded and equipped
the range of services provided including supportservices and outreach activities
use of treatment protocols and guidelines
use of quality systems
referral mechanisms between different services andat different levels of the system.
How to scale up from a pilot project to district or national coverage alsoentails a wide range of management issues and decisions.
-
8/3/2019 Building Blocks Notes
10/38
In many developing countries, people whohave the responsibility to manage servicedelivery often may not have any, or verymuch, management training.
Training to be a doctor, a nurse or apharmacist, usually does not include howto manage finances, or staff, or how to
institute major changes.
Increasing management capacity involves not only building individual managementcompetency, but also, having enough managers in the right places, providing anenabling work environment, and ensuring that managers have suitable functioningmanagement systems to help them to do their job. Thus, focusing primarily onsending managers away for management training will probably not have a
significant impact on improving service delivery and health outcomes, if the otheraspects of building management capacity are not also improved.
(Talked about HLMP of ZFF)
-
8/3/2019 Building Blocks Notes
11/38
Public-private segregation: 70% of ALL health workers employed in the
highly resourced private sector serves 30% ofthe population
30% employed in government services catersto the majority
Emphasis on curative vs. preventivemedicine
Overspecialization in curative services- Dr. Galvez-Tan (2010)
Fragmentation from several perspectives:
public/private segregation
over-specialization
discontinuities between levels of health care
geographic disparities in quality and
quantity of services
Crowding in tertiary care facilities and underutilization of primary health carefacilities due to perceived poor quality and bypassing of the latter.
-
8/3/2019 Building Blocks Notes
12/38
Workforce
A well-performing healthworkforce is one whichworks in ways that areresponsive, fair andefficient to achieve thebest health outcomespossible, given availableresources andcircumstances.
I.e. There are sufficient numbers and mix of staff, fairly distributed; they arecompetent, responsive and productive.
-
8/3/2019 Building Blocks Notes
13/38
Health workers are INDISPENSABLE -the cornerstone of health care deliverysystem, influencing access, quality andcosts of health care, and effective deliveryof interventions for improved healthoutcomes, including progress towards theachievement of the health MillenniumDevelopment Goals and Health For All.
-
8/3/2019 Building Blocks Notes
14/38
The World Health Report 2006estimated a globalshortage of 2.3 million physicians, nurses and midwivesto meet the workforce levels required to strengthenhealth systems and accelerate progress towardsattaining the health related Millennium DevelopmentGoals.
An absolute shortage of human resources for health(HRH) was assessed in 57 countries, mostly in sub-Saharan Africa. Recognizing that pressing health needsacross the globe cannot be met without a competent,adequate and available health workforce, urgent andsustained scale-up of health workforce production was
called upon for both developed and developing countriesto address the health workforce crisis.
Contrary to the tenets of classical economic analysis, as the number of medicalprofessionals in the Philippines has decreased, so has the local wage rate.According to Federico M. Macaranas, PhD, the Executive Director of the AsianInstitute of Management's Policy Center, in his remarks, delivered at the CarnegieCouncil, highlighted the lack of consensus on how to address this problem. ,
Filipino hospital administrators are keen to avoid over-investing in doctors andnurses that are likely to emigrate. As a result, wages are low and employees seethe hospitals as stepping-stones to higher paying jobs overseas. More than 200hospitals have closed in the Philippines in the last five years.
Scaling up the production of health workers means not only increasing the output ofhealth professions education programmes, but also ensuring that the 'pipeline' -from recruitment and selection of students to deployment of new graduates in thehealth labour market - is functional and effective, and that the education and trainingprogrammes are adapted to the changing needs of the population. Given thelengthy periods required to see the effects of certain programmatic efforts (e.g. upto six or even eight years in the case of educating physicians), innovative strategiesmay be required to rapidly increase the capacity of the workforce, notably among
mid-level cadres such as medical officers or nursing assistants, and amongcommunity health workers. At the same time, increased production must be placedin the broader context of ensuring that the quality, distribution and skill mix of thehealth workforce meet national health systems goals.
-
8/3/2019 Building Blocks Notes
15/38
-
8/3/2019 Building Blocks Notes
16/38
No. 1 Exporter of Nurses
An estimated 85% of employed Filipino nurses (more than 150,000) are workinginternationally. (Aiken et al 2004)
70% of all Filipino nursing graduates are working overseas. (Bach 2003)
No. 2 Exporter of Doctors68% of Filipino doctors work overseas, next to India. (Mejia, WHO 1975)
200 hospitals have closed down within the past two years no more doctors and nurses
800 hospitals have partially closed (with one to two wards closed) lack of doctors and nurses
Nurse to patient ratios in provincial and district hospitals now 1: 40 to 1: 60
Loss of highly skilled nurses in all hospitals across the country
-
8/3/2019 Building Blocks Notes
17/38
Information System
A well-functioning health information system isone that ensures the production, analysis,dissemination and use of reliable and timelyinformation on health determinants, healthsystems performance and health status.
-
8/3/2019 Building Blocks Notes
18/38
Several countries are making better use of informationtechnology and geographic informationsystems. Improvements have also been made todisease surveillance systems. In many countries localusers are now involved more closely in the design ofinformation systems.
Nevertheless, most countries still use a wide range ofdata collection and analysis tools, some of which collectthe same data. An increasing volume of data isavailable, but coverage and quality are variable. Linking
information to policy-making at the national level remainscritical, but elusive, goal.
In recent years, WHO and its Member States have placed more emphasis onevidence-based decision-making. Most developing countries in the Region haveattempted to enhance their national health information systems, often with thesupport of partner agencies. However, overall progress has been slow.
(make mention Bago Citys CDSS)
-
8/3/2019 Building Blocks Notes
19/38
Problems faced by developing countries in theRegion include the following: weak organizational support for data collection
systems; lack of standardization and coherence in attempts to
improve health information systems; untimely collection of data; inadequate use of information and evidence for
decision-making; inadequate data analysis and communication skills;
and
overambitious computerization of health informationsystems that countries are unable to maintain.
Underreporting of deaths by national vital registration systems still needs to beaddressed in many countries. If the quality of health information is highly variable, itis unlikely to be widely used.
Rudimentary and ministerial despite its usefulness for decision making
Error prone pen and paper methods at lower levels despite technologicaladvances
Flow is hierarchical with many actors involved
Resulting information is distorted, delayed, withheld
-
8/3/2019 Building Blocks Notes
20/382
Equitable Access
A well-functioning health system ensuresequitable access to essential medicalproducts , vaccines and technologies ofassured quality, safety, efficacy and cost-effectiveness, and their scientifically soundand cost-effective use.
The existing gross inequality in the health status of the people particularly betweendeveloped and developing countries as well as within countries is politically, sociallyand economically unacceptable (Alma Ata)
-
8/3/2019 Building Blocks Notes
21/382
LEB overLEB over 8080 yearsyears
IMR less thanIMR less than 1010
MM less thanMM less than 1515
LEB underLEB under 6060 yearsyears
IMR overIMR over 9090MM overMM over 150150
2
-
8/3/2019 Building Blocks Notes
22/382
Recent essentialmedicines surveysin 39 mainly low-and low-middle-income countriesfound that, whilethere was widevariation, averageavailability was 20%in the public sector,and 56% in the
private sector.
-
8/3/2019 Building Blocks Notes
23/382
An estimated 50% of medical equipment indeveloping countries is not used, either becauseof a lack of spare parts or maintenance, orbecause health workers do not know how to useit.
-
8/3/2019 Building Blocks Notes
24/382
Financing
A good health financing system raises adequate fundsfor health, in ways that ensure people can use neededservices, and are protected from financial catastrophe orimpoverishment associated with having to pay for them.
-
8/3/2019 Building Blocks Notes
25/382
Universal coverage of health services is a widelyaccepted goal of health-financing policies. Yetdespite impressive economic development in theAsia-Pacific region, where growth rates in grossdomestic product (GDP) averaged 72% overthe period 1999 to 2008, about 105 millionpeople suffer financial catastrophe and over 70million are impoverished each year becausethey have to pay for health care Lancet,Health-financing strategy for WHO's Asia-
Pacific Region
-
8/3/2019 Building Blocks Notes
26/382
Many people in the Asia Pacific region, especially thepoor and vulnerable, face severe barriers to accessingquality health care. This is of particular concern during
the current global economic crisis. Appropriate healthfinancing policies can help reduce these barriers toaccess, and thereby extend health gains to those most inneed.
-
8/3/2019 Building Blocks Notes
27/382
The WHO provides technical support to countries in developing such healthfinancing policies. The ultimate aim is universal coverage, where all people haveaccess to appropriate promotive, preventive, curative and rehabilitative services atan affordable cost.
according to National Statistical Coordination Board (NSCB) secretary generalRomulo Virola: The Philippine Star Updated August 15, 2010
Pinoy households continued to bear the heaviest burden in terms of spending fortheir health needs as private out-of-pocket surpassed the 50 percent mark in healthexpenditure share in 2006, reaching 54.3 percent in 2007. Private households thuscontributed an estimated P97.6 billion to the total health expenditure in2005 andP127.3 billion in 2007.
Government came in a far second in health spending contribution, with the National
Government and the local government units (LGUs) footing almost equal shares of13.0 percent and 13.3 percent in 2007, respectively. It is worth noting that the LGUsspent more than the national government in 2006 and 2007. Total governmentexpenditure on health care goods and services increased fromP58.5 billion in 2005to P61.5 billion in 2007, registering an annual growth of only 2.6 percent.
Health expenditure from social insurance barely grew from P19.4 billion in 2005 tonearly P20.0 billion in 2007, indicating an average annual growth of only 1.6percent. Thus, instead of picking up as targeted, the social insurance share inhealth spending went down from 9.8 percent in 2005 to only 8.5 two years later.
-
8/3/2019 Building Blocks Notes
28/382
The global crisis continues toaffect many economies in Asiaand the Pacific. Oftengovernments are under pressureto cut health budgets and expanduser fees, which would furtherreduce access, equity, quality,and utilization of health services.
The 60th Regional CommitteeMeeting held in September 2009discussed the global crisis and itsimpact on health in the region,including action to help mitigateits adverse effects.
-
8/3/2019 Building Blocks Notes
29/382
Focus: Universal coverageThis is defined as securing access for all to appropriate promotive,preventive, curative and rehabilitative services at an affordable cost.
4 target indicators:1. out-of-pocket spending should not exceed30%-40%of total
health expenditure;
2. total health expenditure should be at least4%-5%of GDP;
3. over 90%population should be covered by prepaymentand risk pooling schemes; and
4. close to 100%coverage of vulnerable population with socialassistance and safety net programs.
-
8/3/2019 Building Blocks Notes
30/383
8 strategic areas:1. increasing investment and public spending on heatlh
2. improving aid effectiveness
3. improving efficiency by rationalizing health expenditures
4. increasing the use of prepayment and pooling
5. improving provider payment methods
6. strengthening safety-net mechanisms for the poor andvulnerable
7. improving evidence and information for policymaking, and
8. improving monitoring and evaluation of policy change.
-
8/3/2019 Building Blocks Notes
31/383
-
8/3/2019 Building Blocks Notes
32/383
Inadequate: P 180.8 billion in 2005, which is3.3% of GDP, compared to 5% of GDP asrecommended by WHO
High out of pocket expenditure: 49% in 2005
Inefficient: 11% for cost effective public healthcompared to 78.4% for personal health care
Greater funding for tertiary facilities at theexpense of primary care facilities
- Dr. Galvez-Tan (2010)
-
8/3/2019 Building Blocks Notes
33/383
All of us (former health secretaries) began withthe promise of universal healthcare. I think weshould start getting impatient. The health gapbetween poor and rich has worsened, haswidened, and I dont know anyone else to blameexcept me, because the fact is that weve allfailed. -Sec. Alberto Romualdez (GMA News Online, Nov. 8,
2011)
-
8/3/2019 Building Blocks Notes
34/383
Leadership
Leadership and governance involves ensuringstrategic policy frameworks exist and are
combined with effective oversight, coalition-building, the provision of appropriate regulationsand incentives, attention to system-design, andaccountability.
-
8/3/2019 Building Blocks Notes
35/383
Governance (or stewardship) is responsible attention tosomething entrusted to one's care. In the context ofhealth it refers to the wide range of functions carried outby governments in their work to achieve national healthgoals to improve population health while ensuring equityin access to services, quality of services, and patients'rights.
Governance is also concerned with the roles andresponsibilities of the public, private and voluntarysectors - including civil society - and their relationships
with each other, in the provision and financing of healthcare in pursuit of national health goals.
Effective governance implies leadership in maintaining the strategic direction ofhealth policy development and implementation; detecting and correcting undesirabletrends and distortions; articulating the case for health in national development;regulating the behaviour of actors involved in financing and delivery of healthinterventions; establishing effective accountability mechanisms and promoting
healthy public policy and legislation in other areas of government that impact onpeoples' health. In countries that receive significant amounts of developmentassistance, governance will be concerned with managing these resources in waysthat promote national leadership, contribute to the achievement of agreed policygoals, and strengthen national management systems. While the scope forexercising governance functions is greatest at the national level, the concept canalso cover the steering role of regional and local authorities.
-
8/3/2019 Building Blocks Notes
36/383
Mayor Teodorico Padilla of Sta. Fe, Nueva Vizcaya said learning about
Bridging Leadership taught him that real health service
goes beyond giving away medicines and building clinics.
So he started campaigning to increase his constituents
knowledge about health so that they will start to demand
their right to receive proper healthcare.
-
8/3/2019 Building Blocks Notes
37/383
The values and principles of Primary Health Care remain constant, but there
are lessons from the past, which are particularly important when looking
ahead. First, despite increased funding, resources for health will always be
limited, and there is a responsibility to achieve the maximum possible with
available resources. Second, past efforts to implement a Primary Health
Care approach focused almost exclusively on the public sector. In reality, for
many people poor, as well as rich private providers are the first point
of contact, and responsible health system oversight involves taking account
of private as well as public providers. Third, while keeping its focus on the
community and first contact care, Primary Health Care needs to recognize
the problems associated with relying on voluntarism alone.
-
8/3/2019 Building Blocks Notes
38/38
HEALTH IS EVERYBODYS BUSINESS