BS Evidence Based Medicine And Atrial Fibrillation.
39
BS Evidence Based Medicine Evidence Based Medicine And Atrial Fibrillation And Atrial Fibrillation
-
date post
22-Dec-2015 -
Category
Documents
-
view
216 -
download
0
Transcript of BS Evidence Based Medicine And Atrial Fibrillation.

BS
Evidence Based MedicineEvidence Based Medicine
And Atrial FibrillationAnd Atrial Fibrillation

BS
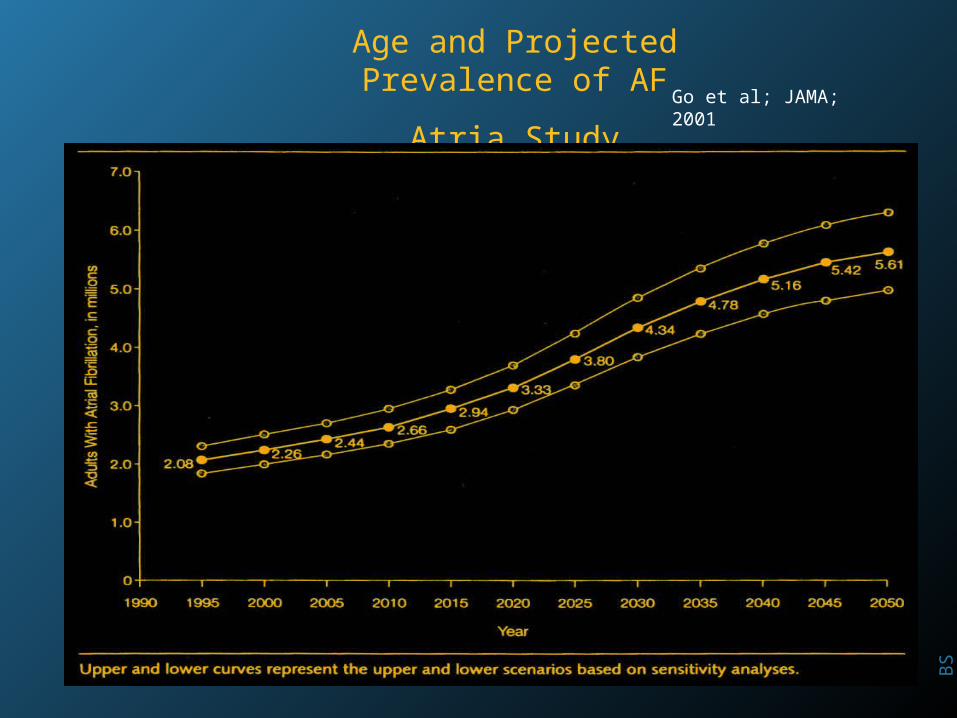
Go et al; JAMA; 2001
Age and Prevalence of AF
Atria Study
1.9 million pts in HMO
17,974 pts with AF
45% > 75 years
BS
Age and Projected Prevalence of AF
Atria Study Go et al; JAMA; 2001

BS
Atrial Fibrillation In The ElderlyAtrial Fibrillation In The ElderlyAre Older Patients Different?Are Older Patients Different?
Younger PatientsYounger Patients Elderly PatientsElderly Patients
Associated DiseaseAssociated Disease +/-+/- ++++++
SymptomsSymptoms ++++++ ++
Intermittent/ChronicIntermittent/Chronic I > CI > C C > IC > I
Thromboembolic RiskThromboembolic Risk ++ ++++++
Hemorrhagic RiskHemorrhagic Risk +/-+/- ++++

BS
Evidence based medicineEvidence based medicine
80 year old male80 year old male
Hypertension for 5 years; Atrial fib ? durationHypertension for 5 years; Atrial fib ? duration
Treated with diuretic and ACE: BP 150/87 mmHgTreated with diuretic and ACE: BP 150/87 mmHg
Electrocardiograph – within normal limitsElectrocardiograph – within normal limits
Echocardiogram – EF 50% early diastolic Echocardiogram – EF 50% early diastolic
relaxation abnormalityrelaxation abnormality
Creatinine 99 umol / lCreatinine 99 umol / l

BS
Atrial Fibrillation In The ElderlyAtrial Fibrillation In The ElderlyThromboembolismThromboembolism
5 year stroke risk is 15%5 year stroke risk is 15%
Aspirin Aspirin risk by 20%; ARR 0.6; NNT 166risk by 20%; ARR 0.6; NNT 166
Warfarin risk Warfarin risk x 70%; ARR 2.1: NNT 47.6 x 70%; ARR 2.1: NNT 47.6
Aspirin major risk 1% pa; warfarin 3% pa Aspirin major risk 1% pa; warfarin 3% pa
P warfarin benefit 100 – (85) + 4.5 = 10.5%P warfarin benefit 100 – (85) + 4.5 = 10.5%
P Aspirin benefit 100 – (85) + 12 = 3%P Aspirin benefit 100 – (85) + 12 = 3%

BS
Computer Decision supportComputer Decision support
BS

BS

BS

BS

BS

BS

BS

BS

BS
Comparison of Decision Model for patients > 75 only with clinical practice
Current treatment N (%)
Recommended
Warfarin Antiplatelet Nil Both
Placebo 5 (38.5) 8 (61.5) 0 0
Warfarin
11 (52.4) 7 (33.3) 3 (14.3) 0
Aspirin
46 (48.4) 41 (43.2) 7 (7.4) 1 (1.0)
Proportion where current treatment = recommended treatment is 41.1% (53/129) 10% (13/129) on some medication when none recommended

BS
Evidence based medicineEvidence based medicine
Decision support can provide evidence based Decision support can provide evidence based
information to assist in clinical decision makinginformation to assist in clinical decision making
Clinicians believe that their decisions on OAC Clinicians believe that their decisions on OAC
for atrial fibrillation are evidence based ?for atrial fibrillation are evidence based ?
However a computer decision support program However a computer decision support program
did not agree that the majority of therapeutic did not agree that the majority of therapeutic
decisions were likely to advantage the patientdecisions were likely to advantage the patient

BS
Evidence based medicineEvidence based medicineRisk benefit ?Risk benefit ?
Balancing the risks of stroke and upper GI tract
bleeding in older patients with atrial fibrillation. Arch
Intern Med 2002: 162(5) ; 541 - 50
For 65-yr with average risks of stroke and upper GI
tract bleeding, warfarin 12.0; aspirin 10.8 and no
antithrombotic Rx, 10.1 QALYs per patient
For 80yr, baseline stroke risk 4.3% pa, warfarin, 7.44;
aspirin, 7.39; and no treatment, 7.21 QALYs per
patient

BS
Evidence based medicineEvidence based medicine
80 year old male80 year old male
Hypertension for 5 years; Atrial fib ? durationHypertension for 5 years; Atrial fib ? duration
Treated with diuretic and ACE: BP 150/87 mmHgTreated with diuretic and ACE: BP 150/87 mmHg
Electrocardiograph – within normal limitsElectrocardiograph – within normal limits
Echocardiogram – EF 50% early diastolic Echocardiogram – EF 50% early diastolic
relaxation abnormalityrelaxation abnormality
Creatinine 99 umol / lCreatinine 99 umol / l

BS



Am Heart J. 2005; 149 (4): 650-656.
Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio

BS
Evidence based medicineEvidence based medicine

BS
Evidence based medicineEvidence based medicine
Warfarin reduces the risk of stroke by about two-thirds Warfarin reduces the risk of stroke by about two-thirds
compared with placebo (ARR, 3.1% per year; NNT, 32) and compared with placebo (ARR, 3.1% per year; NNT, 32) and
by about a third compared with aspirin (ARR, 0.8% per by about a third compared with aspirin (ARR, 0.8% per
year; NNT, 125), but causes at least twice as many intrayear; NNT, 125), but causes at least twice as many intra--
cranial and extracranial and extra--cranial bleeds as aspirin cranial bleeds as aspirin

BS
Evidence based medicineEvidence based medicine

Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio
Predicted event rate in population from calculatorPredicted event rate in population from calculator
Multiply by RRR (Relative risk reduction)Multiply by RRR (Relative risk reduction)
Gives the ARR (Absolute Risk Reduction)Gives the ARR (Absolute Risk Reduction)
1 / ARR = NNT (Patient yr to prevent stroke)1 / ARR = NNT (Patient yr to prevent stroke)
NNH (numbers to harm)NNH (numbers to harm)
1 / Serious ADR1 / Serious ADR

Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio
Warfarin ( NNT – 32 : NNH – 80)Warfarin ( NNT – 32 : NNH – 80)
ARR = 100 / 30 = 3.13%ARR = 100 / 30 = 3.13%
Assumed stroke risk – 3.13 / 0.7 = 4.46%Assumed stroke risk – 3.13 / 0.7 = 4.46%
Bleed assumed rate 100 / 80 = 1.25%Bleed assumed rate 100 / 80 = 1.25%
Assuming risk rate unrelated to warfarin 0.8%Assuming risk rate unrelated to warfarin 0.8%
Total bleed rate 2.1%Total bleed rate 2.1%

Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio
80 yr old male, unCx Atrial fibrillation, BP 150/8780 yr old male, unCx Atrial fibrillation, BP 150/87
Stroke risk – Framingham 5yr (8 points) – 11%Stroke risk – Framingham 5yr (8 points) – 11%
Stroke risk – CHADS2 (4% pa) – 20%Stroke risk – CHADS2 (4% pa) – 20%
Bleeding risk – AFFIRM (2% pa + age 1.05) – 10.1%Bleeding risk – AFFIRM (2% pa + age 1.05) – 10.1%
Stroke risk is 3% and bleed risk 2%Stroke risk is 3% and bleed risk 2%

Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio
80 yr old male, unCx Atrial fibrillation, BP 150/8780 yr old male, unCx Atrial fibrillation, BP 150/87
Stroke risk – on Warfarin (3 – (0.7 * 3)) = 0.9 Stroke risk – on Warfarin (3 – (0.7 * 3)) = 0.9
Absolute risk reduction = 2.1 (NNT 47.6)Absolute risk reduction = 2.1 (NNT 47.6)
Bleeding risk = 2% pa (NNH 83)Bleeding risk = 2% pa (NNH 83)
Applying principle of risk equivalence –Applying principle of risk equivalence –
ADR / Relative risk benefit (1.2 / 0.7 = 1.7)ADR / Relative risk benefit (1.2 / 0.7 = 1.7)
Risk must > 1.7 for a favourable risk profileRisk must > 1.7 for a favourable risk profile

BS
Evidence based medicineEvidence based medicineRisk benefit ?Risk benefit ?
HEMORRHEMORR22HAGESHAGES National Register of Atr Fibrillation National Register of Atr Fibrillation
Anti-thrombotic Rx on individual risks and benefits
Hospitalization for bleed / warfarin was 4.9 per 100
patient-yr, but depended on comorbidity (NNH 24.2)
High-risk patients haemorrhage rate (7.5-15.3) much
greater than the low-risk patients (1.1-2.9)
Previous trial estimates - 2.4 per 100 yr (NNH 62.5)

Am Heart J. 2006;151(3):713-719.
Evidence based medicineEvidence based medicine
Harm (NNH)Harm (NNH)
90.990.9
58.858.8
22.222.2
13.213.2
10.410.4
8.78.7
24.424.4

Calculation of Risk-Benefit RatioCalculation of Risk-Benefit Ratio
80 yr old male, unCx Atrial fibrillation, BP 150/8780 yr old male, unCx Atrial fibrillation, BP 150/87
Stroke risk – on Warfarin (3 – (0.7 * 3)) = 0.9 Stroke risk – on Warfarin (3 – (0.7 * 3)) = 0.9
Absolute risk reduction = 2.1 (NNT 47.6)Absolute risk reduction = 2.1 (NNT 47.6)
Bleeding risk = 4.9% pa (NNH 24.4)Bleeding risk = 4.9% pa (NNH 24.4)
Applying principle of risk equivalence –Applying principle of risk equivalence –
ADR / Relative risk benefit (4.1 / 0.7 = 5.9)ADR / Relative risk benefit (4.1 / 0.7 = 5.9)
Risk must > 5.9 for a favourable risk profileRisk must > 5.9 for a favourable risk profile

BS

BS
Evidence based medicineEvidence based medicineHigh risk and warfarin?High risk and warfarin?
CHAD2 SCORE > 3 - a stroke risk of 9 %CHAD2 SCORE > 3 - a stroke risk of 9 %
Stroke risk – on Warfarin (9 – (0.7 * 9)) = 2.7Stroke risk – on Warfarin (9 – (0.7 * 9)) = 2.7
Absolute risk reduction = 6.3 (NNT 15.9)Absolute risk reduction = 6.3 (NNT 15.9)
The major bleed risk is 4.9% pa (NNH 20.4)The major bleed risk is 4.9% pa (NNH 20.4)
Risk equivalence (4.1 / 0.7) – stroke rate of 5.9%Risk equivalence (4.1 / 0.7) – stroke rate of 5.9%
Warfarin no difference 68.5% - ((100 – 45) + 13.5))Warfarin no difference 68.5% - ((100 – 45) + 13.5))

BS
Evidence based medicineEvidence based medicineIs aspirin a rational choice ?Is aspirin a rational choice ?
Aged 80 yr (atrial fib) has a 5 yr stroke risk of 15%Aged 80 yr (atrial fib) has a 5 yr stroke risk of 15%
Aspirin will reduce that risk by 20%Aspirin will reduce that risk by 20%
No event in 85% + 12 events not preventedNo event in 85% + 12 events not prevented
Aspirin will make no difference 97% of the timeAspirin will make no difference 97% of the time
Absolute risk reduction (ARR) – 0.6 (NNT 166.6)Absolute risk reduction (ARR) – 0.6 (NNT 166.6)
The average bleed risk is 0.2% x 5 = 1%The average bleed risk is 0.2% x 5 = 1%

BS
Evidence based medicineEvidence based medicinePatient preferences ?Patient preferences ?
Malcolm Man-Son-Hing, Malcolm Man-Son-Hing, et alet al, , Medical Decision Medical Decision
MakingMaking 2005: 2005: 2525;; 548-559 548-559 (Systemic review n = 8) (Systemic review n = 8)
FFewer patients ewer patients opt for opt for warfarin compared with warfarin compared with
guidelines ( 5 / 8 studies)guidelines ( 5 / 8 studies)
AspirinAspirin stroke rate of 1 stroke rate of 1 %% , opt for , opt for warfarinwarfarin 50% 50%
Aspirin stroke rateAspirin stroke rate 2 2% ,opt for % ,opt for warfarinwarfarin 66% 66%
Aspirin stroke rate 2 – 6% in 3 to choose warfarinAspirin stroke rate 2 – 6% in 3 to choose warfarin
PPhysicians balance patient preferences with hysicians balance patient preferences with Rx Rx
recommendations recommendations ofof clinical practice guidelines clinical practice guidelines

BS
Evidence based medicineEvidence based medicine
Anyone who believes that the same thing can be suited to everyone is a great fool, since medicine is practiced not on mankind in general but on every individual in particular
Henry De Mondeville circa 1300

BS