
BRONQUIECTASIAS MURRAY.pdf
24
1023 CHAPTER 42 BRONCHIECTASIS Michael D. Iseman, MD • Edward D. Chan, MD INTRODUCTION CLASSIFICATION EPIDEMIOLOGY PATHOGENESIS “VICIOUS CIRCLE” AND MICROBIOLOGY BIOFILMS ASSOCIATED DISORDERS AND PREDISPOSITIONS Lung Injury Due to Acute Infection Cystic Fibrosis Disorders of Immunity Alpha 1 -Antitrypsin Anomalies Ciliated Epithelium Bronchial Cartilage Connective Tissue Congenital and Developmental Anomalies Idiopathic Inflammatory Disorders Aspiration/Inhalation Accidents Postobstructive Disorders Allergic Bronchopulmonary Aspergillosis Miscellaneous DIAGNOSIS MANAGEMENT Airway Hygiene and Hyperosmotic Agents Antimicrobial Therapy Anti-inflammatory Therapy Surgery Miscellaneous INTRODUCTION The condition of bronchiectasis (BXSIS) is defined by dilation, or ectasia, of the airways or bronchos. The primary clinical manifestations of BXSIS are recurrent, chronic, or refractory infections. Other significant seque- lae include hemoptysis, chronic airflow obstruction, and progressive impairment of breathing. In the preantibi- otic era, secondary amyloidosis and embolic brain abscesses were reported as consequences of chronic suppuration in the lungs; such complications are extremely rare now in industrialized nations. There are many and varied pathways that lead to the development of BXSIS (Table 42-1). Broadly, BXSIS may develop due to an incidental event or episode that does not reflect the patient’s intrinsic host defenses. Examples might include a necrotizing pneumonia following aspira- tion or chronic infection distal to an obstructing bron- chial adenoma. Often, however, BXSIS evolves due to conditions that are inherent to the patient’s basic genetic constitution. The most common and dramatic example of this is cystic fibrosis (CF). The distinction between these two models is an important element of prognosis and management. A central issue in understanding the pathogenesis of BXSIS is whether infection is truly the proximate cause of BXSIS or patients develop infections due to an underly- ing predisposing condition. For example, it has been a commonly held adage that many cases of BXSIS in adults are due to childhood bouts of pertussis or measles. 1 Although this is undoubtedly true in some instances, one might be skeptical of this simple construct, asking why formerly common childhood illnesses resulted in BXSIS in only a small proportion of the patients. The question that should be addressed more thoroughly is whether the individuals were particularly vulnerable to complica- tions; for example, did the pertussis or measles result in excessive damage due to innate susceptibility of the hosts? CLASSIFICATION Although there is considerable overlap and coexistence among the various forms of BXSIS, the radiographic pat- terns and distribution may provide clues to diagnosis, management, and prognosis. 2 Thus, characterizing the morphologic features and distribution of BXSIS is a useful
-
Upload
yony-morales-leon -
Category
Documents
-
view
25 -
download
1
Transcript of BRONQUIECTASIAS MURRAY.pdf

1023
C H A P T E R 4 2
BronchiectasisMichael D. Iseman, MD • Edward D. Chan, MD
INTRODUCTION
CLASSIFICATION
EPIDEMIOLOGY
PATHOGENESIS
“VICIOUS CIRCLE” AND MICROBIOLOGY
BIOFILMS
ASSOCIATED DISORDERS AND PREDISPOSITIONSLung Injury Due to Acute InfectionCystic FibrosisDisorders of ImmunityAlpha1-Antitrypsin AnomaliesCiliated EpitheliumBronchial Cartilage
Connective TissueCongenital and Developmental AnomaliesIdiopathic Inflammatory DisordersAspiration/Inhalation AccidentsPostobstructive DisordersAllergic Bronchopulmonary AspergillosisMiscellaneous
DIAGNOSIS
MANAGEMENTAirway Hygiene and Hyperosmotic AgentsAntimicrobial TherapyAnti-inflammatory TherapySurgeryMiscellaneous
INTRODUCTION
The condition of bronchiectasis (BXSIS) is defined by dilation, or ectasia, of the airways or bronchos. The primary clinical manifestations of BXSIS are recurrent, chronic, or refractory infections. Other significant seque-lae include hemoptysis, chronic airflow obstruction, and progressive impairment of breathing. In the preantibi-otic era, secondary amyloidosis and embolic brain abscesses were reported as consequences of chronic suppuration in the lungs; such complications are extremely rare now in industrialized nations.
There are many and varied pathways that lead to the development of BXSIS (Table 42-1). Broadly, BXSIS may develop due to an incidental event or episode that does not reflect the patient’s intrinsic host defenses. Examples might include a necrotizing pneumonia following aspira-tion or chronic infection distal to an obstructing bron-chial adenoma. Often, however, BXSIS evolves due to conditions that are inherent to the patient’s basic genetic constitution. The most common and dramatic example of this is cystic fibrosis (CF). The distinction between these two models is an important element of prognosis and management.
A central issue in understanding the pathogenesis of BXSIS is whether infection is truly the proximate cause of BXSIS or patients develop infections due to an underly-ing predisposing condition. For example, it has been a commonly held adage that many cases of BXSIS in adults are due to childhood bouts of pertussis or measles.1 Although this is undoubtedly true in some instances, one might be skeptical of this simple construct, asking why formerly common childhood illnesses resulted in BXSIS in only a small proportion of the patients. The question that should be addressed more thoroughly is whether the individuals were particularly vulnerable to complica-tions; for example, did the pertussis or measles result in excessive damage due to innate susceptibility of the hosts?
CLASSIFICATION
Although there is considerable overlap and coexistence among the various forms of BXSIS, the radiographic pat-terns and distribution may provide clues to diagnosis, management, and prognosis.2 Thus, characterizing the morphologic features and distribution of BXSIS is a useful

1024 ObstructiveDiseases
AIDS, acquired immunodeficiency syndrome; CF, cystic fibrosis; HIV, human immunodeficiency virus.
discipline. In this era, BXSIS is primarily identified and described by computed tomography (CT; see later).
Cylindrical BXSIS is described as failure of the involved airways to taper progressively in their distal course. Usually, in this condition, the bronchial walls are smooth or regular (Fig. 42-1). Varicoid BXSIS is an allusion to
varicose veins and is marked by irregular dilation, nar-rowing, and outpouching of the airways (Fig. 42-2). Sac-cular BXSIS includes focal or cystic distortion of the distal airways; it may be isolated (Fig. 42-3) or may form confluent “honeycomb” patterns (Fig. 42-4).
A traditional clinical distinction within BXSIS has been “wet” versus “dry.” Historically, it was observed that some patients with BXSIS had continuous or frequent
FIGURE 42-1 n Cylindrical bronchiectasis (BXSIS). In the anterior segment of the right upper lobe is an extended nontapering airway with moderately thickened and generally regular walls (arrow). The patient is a 50-year-old white woman with a slender body habitus and subtle scoliosis but no other identified risk factors for BXSIS. In addition, she had severe varicoid and “honeycomb” BXSIS involving her right middle lobe (see Figs. 42-2 and 42-4).
FIGURE 42-2 n Varicoid BXSIS. The right middle lobe of this 50-year-old woman is involved with severe atelectasis and dense, side-by-side varicoid BXSIS involving the conducting airways. Distal to this pattern are dramatic honeycomb changes of the terminal air spaces (see Fig. 42-4).
TABLE 42-1. Conditions Associated with Bronchiectasis
POSTINFECTIOUS CONDITIONSChildhood lower respiratory tract infections
Granulomatous infections
Necrotizing pneumonias in adults
Other respiratory infections
PRIMARY IMMUNE DISORDERSHumoral defects
Cellular and/or mixed disorders
Neutrophil dysfunction
Other
CYSTIC FIBROSISClassic CF
Variants of CF
Young’s syndrome
ALPHA1-ANTITRYPSIN SYSTEMDeficiencies
Anomalies
HERITABLE STRUCTURAL ABNORMALITIESCiliated epithelium
Cartilage
Connective tissue
Sequestration, agenesis, hypoplasia
Dwarfism
IDIOPATHIC INFLAMMATORY DISORDERSSarcoidosis
Rheumatoid arthritis
Ankylosing spondylitis
Systemic lupus erythematosus
Sjögren’s syndrome
Inflammatory bowel disease
Relapsing polychondritis
INHALATION AND OBSTRUCTIONGastroesophageal reflux/aspiration
pneumonia
Toxic inhalation/thermal injury
Postobstruction accident
Foreign body
Tumors, benign and malignant
Extrinsic airway compression
Allergic bronchopulmonary aspergillosis/mycosis
MISCELLANEOUSHIV infection/AIDS
Yellow-nail syndrome
Radiation injury
42 brOnchiectasis 1025
productive cough that typically yielded copious, often purulent secretions—hence “wet.” Others who carried the diagnosis of BXSIS rarely experienced cough, and if they did so, rarely was their cough productive—hence “dry.” Independent of etiology, the most frequent pat-terns associated with wet or dry BXSIS are anatomic localizations. BXSIS involving dependent zones (lower lobes, the right middle lobe, or the lingular segment of the left upper lobe) tends to entail frequent or chronic infections and to be “wet” in nature. By contrast, chronic BXSIS isolated to the upper lobes is less commonly involved with infection and to be “dry” in terms of sputum production. Presumably, this is related in large measure to gravity-driven drainage of the upper zones in contrast to pooling of secretions in the dependent regions.
EPIDEMIOLOGY
There are no systematic data on the incidence or preva-lence of BXSIS. Historically, it has been thought that as antibiotics and vaccines were introduced in the 20th century, there has been a declining rate of BXSIS.3,4 The presumed mechanism was that these modalities lessened the frequency, severity, and duration of lower respira-tory tract infections that might result in BXSIS. In this regard, it is suggested that BXSIS remains relatively more common in regions where prompt and effective medical care is not available.5 However, it should be stressed that there are no careful quantitative studies documenting these trends.
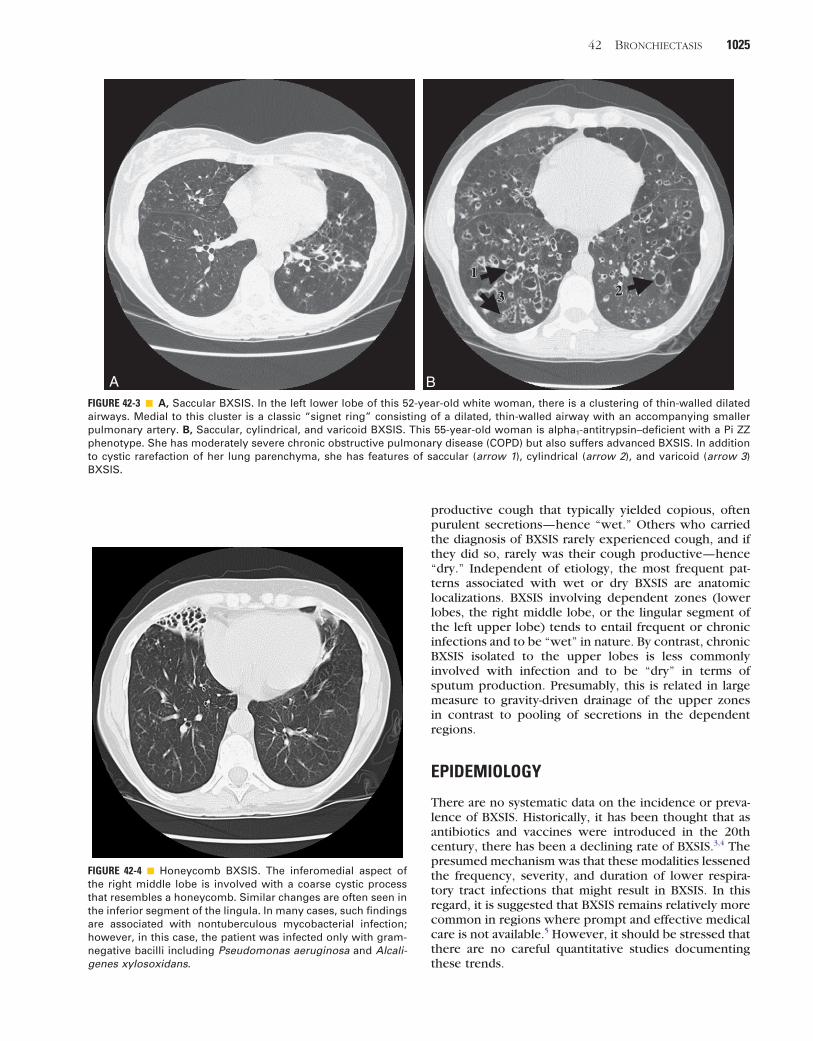
A BFIGURE 42-3 n A, Saccular BXSIS. In the left lower lobe of this 52-year-old white woman, there is a clustering of thin-walled dilated airways. Medial to this cluster is a classic “signet ring” consisting of a dilated, thin-walled airway with an accompanying smaller pulmonary artery. B, Saccular, cylindrical, and varicoid BXSIS. This 55-year-old woman is alpha1-antitrypsin–deficient with a Pi ZZ phenotype. She has moderately severe chronic obstructive pulmonary disease (COPD) but also suffers advanced BXSIS. In addition to cystic rarefaction of her lung parenchyma, she has features of saccular (arrow 1), cylindrical (arrow 2), and varicoid (arrow 3) BXSIS.
FIGURE 42-4 n Honeycomb BXSIS. The inferomedial aspect of the right middle lobe is involved with a coarse cystic process that resembles a honeycomb. Similar changes are often seen in the inferior segment of the lingula. In many cases, such findings are associated with nontuberculous mycobacterial infection; however, in this case, the patient was infected only with gram-negative bacilli including Pseudomonas aeruginosa and Alcali-genes xylosoxidans.

1026 ObstructiveDiseases
impact of airway collapsibility on the effectiveness of the cough mechanism. Coughing is an essential, primary element of lung defense. An effective cough sends columns of air rushing upward through the bronchial tree at peak speeds measured in the range of 600 mph.12 To generate these high flow rates, the cartilaginous rings must have the structural integrity to remain patent while the posterior membranous element invaginates into the lumen of the airway to lessen the cross-sectional diam-eter of the airway and accelerate airflow. While perform-ing bronchoscopy on patients with BXSIS, it is common to observe extraordinary collapsibility of the airways, virtually obstructing the bronchi. It seems likely that such amplified airway compressibility impedes the air-driven propulsion of secretions out of the bronchial tree and helps propagate the chronic or recurring infections that mark most cases of BXSIS.
“VICIOUS CYCLE” AND MICROBIOLOGY
The other major element in the pathogenesis of BXSIS is the destructive effect of chronic airway infections, the vicious cycle theory as described by Cole.13 Briefly, it is reasoned that once airways are “damaged,” they become vulnerable to chronic colonization, which merges into an inflammatory condition; this results in further injury and lessened capacity to resist infection. Analysis of cellular and noncellular constituents in the bronchiec-tatic airways typically demonstrates intense infiltration by neutrophils as well as mononuclear cells and lymphocytes.14
Although there is a burgeoning literature on mecha-nisms of inflammation and airway damage, the relevance of these findings to the diagnosis and clinical manage-ment is not currently apparent and is not addressed in detail in this chapter.
It is apparent that simple colonization and infection of the airways are not sufficient to produce true BXSIS. Sputum from patients with smoking-related chronic bronchitis typically yields organisms such as Haemo-philus influenzae, Haemophilus parainfluenzae, Strep-tococcus pneumoniae, and Moraxella catarrhalis, a microbial spectrum similar to that seen with BXSIS.15 In addition, there is heavy cellular traffic and the presence of a variety of inflammatory mediators. However, signifi-cant BXSIS does not appear commonly among patients with simple chronic bronchitis. Hence, it is probable that systemic conditions or focal disturbances as noted later are required for the development of classic BXSIS. Notably, however, the appearance in respiratory secre-tions of Pseudomonas aeruginosa on a chronic or recurring basis does pose the risk of deleterious effects on ciliary function and other host defenses.16 Pseudomo-nal infections may be of particular importance due to their role in the formation of biofilms (see later). Two reports note worsened lung function16 and quality of life17 among BXSIS patients who become infected with P. aeruginosa. In a longitudinal study of the microbiol-ogy of 89 patients with BXSIS over a 5-year period, 47% were colonized with H. influenzae, 12% with P. aerugi-
In the United States, there appear to be increasing numbers of BXSIS cases associated with environmental or nontuberculous mycobacteria (NTM).6,7 Based on serial observations in a cohort now numbering approxi-mately 2000, our group believes that in the majority of cases, the mycobacterial infections both initiate and “drive” the evolution of BXSIS. Of interest, this disorder seems disproportionately to involve women, predomi-nantly slender white women.8,9 It is not possible to determine whether this is an accurate picture or an arti-fact of increased awareness and improved diagnostic techniques.
PATHOGENESIS
Various mechanisms operate to produce permanent, pathologic dilation and damage of the airways. In sim-plest terms, they may be thought of in terms of traction, pulsion, and weakened tensile strength of the airways. In most cases, the pathogenesis becomes inextricably linked with and propelled by the destructive effects of chronic infection.
In normal lungs, airways are held patent by a combi-nation of negative intrapleural pressure (which main-tains the lungs in an inflated state) and the cartilaginous rings of the trachea and the large and medium airways. The distending forces of the negative intrapleural pres-sure are transmitted to the airways by a diffuse system of interstitial tethering. As the lung undergoes fibrotic changes consequent to disorders such as sarcoidosis, interstitial lung disorders, or infections such as tubercu-losis, local retractile forces result in fixed dilation of the airways, or “traction” BXSIS.
The prototypic “pulsion” BXSIS occurs with allergic bronchopulmonary aspergillosis (ABPA). In ABPA, there are intense, immunologically mediated reactions to inhaled Aspergillus that has lodged in the airways. The proliferating fungi form large mucoid conglomerates that fill and distend the central airways. It is probable that this airway dilation is potentiated by focal damage medi-ated by inflammatory products that weaken the bronchi.
Weakness of the airways contributing to the develop-ment of BXSIS may take many forms. Classic postinfec-tious BXSIS presumably is mediated in part by chronic damage to the walls of the airways, resulting in second-ary loss of structural integrity.10,11 This is coupled with scarring and loss of volume of the local lung units, leading to regional increases in retractile forces. Exam-ples of primary weakness of the airways contributing to BXSIS includes Mounier-Kuhn syndrome (congenital tracheobronchiomegaly), Williams-Campbell syndrome (absence of cartilaginous rings in the segmental and subsegmental generations of bronchi), Marfan syndrome, or relapsing polychondritis. A case is made later that the apparent propensity of slender women for BXSIS may be based in part on mechanisms analogous to Marfan syndrome.
One particular component of the posited role of “weakened airways” in the pathogenesis of BXSIS that has not received adequate attention is the potential

42 brOnchiectasis 1027
ing story of recurring, localized infections following a discrete episode of “pneumonia” in their childhood or early adult years that presumably produced irreversible damage leading to BXSIS.1
Specific traditional pathogens to which BXSIS has been ascribed include Bordetella pertussis, mucoid strains of S. pneumoniae, Staphylococcus aureus, Kleb-siella pneumoniae, adenoviruses, rubeola (measles), and influenza. Chronic granulomatous pathogens com-monly related to BXSIS include Mycobacterium tubercu-losis, Histoplasma capsulatum, and NTM such as Mycobacterium avium complex (MAC). In addition, mixed infection, including anaerobic mouth flora related to aspiration, may result in extensive damage to the parenchyma (“lung abscesses”) with subsequent BXSIS.
Cystic FibrosisCF and CF variants are arguably the most common causes of BXSIS in the United States and other industrialized nations of the Western Hemisphere today. Being the most common autosomal recessive disorder among whites (1 in 2000–2500 live births),26 CF is increasingly prevalent as improved therapies allow those who are afflicted to live longer. At present, there are approxi-mately 30,000 CF patients in the United States with 40% to 45% of them estimated to be over 18 years old or roughly 12,000 to 14,000 adults with CF. In the next decade, it is predicted that about 50% of all CF patients will be adults.27 The specific manifestations, severity, and rapidity of progression of CF vary highly according to the genotype and other modifying factors. However, the majority of those with childhood-onset CF who survive into their adolescence or early adult years have manifest BXSIS. (See Chapter 41 for details.)
In addition to these “typical” cases in which CF is recognized early in life, among a large series of adult patients seen at the National Jewish Health (NJH) in Denver with BXSIS associated with NTM, 117 of 865 (13.5%) were found to have one or more abnormal alleles of their cystic fibrosis transmembrane regulator (CFTR) gene,28 well in excess of the anticipated carrier rate of 6% in the general population. In 19 of the NJH patients (2.1% overall), there were two abnormal alleles, and 98 (11.4%) had only one mutation. Of note, the mean age of these patients was 61 years. The clinical importance of these heterozygous mutations may be disputed; however, patients in this cohort had a high frequency of chronic airflow obstruction, sinusitis, difficulties with conception, and coinfection with pathogens typical of CF, including mucoid strains of P. aeruginosa—all fea-tures compatible with clinical CF. Among another series of patients with BXSIS and/or NTM lung disease, 24 of 50 (48%) had one or more CFTR mutations.29 Similarly, among a cohort of 63 patients with NTM lung disease studied at the National Institutes of Health (NIH), 36% had mutations in the CFTR gene.30 Consistent with the assertion that these heterozygous mutations are clinically relevant is a series of 30 patients with clinical features of CF who were reported to have normal CFTR alleles on comprehensive gene sequencing.31 The authors
nosa, and 21% had no identifiable pathogen. After 5 years, there was a slight increase in the number of those colonized with P. aeruginosa. As expected, those with the mildest disease had no pathogen whereas those with the worst disease were colonized with P. aeruginosa.18
As previously noted, NTM can colonize bronchiec-tatic airways as well as cause BXSIS. Based on two recent studies from the United Kingdom, the prevalence of NTM isolated from a heterogeneous group of bronchiec-tatic patients was approximately 2% to 10%.19 Further-more, bronchiectatic patients with NTM infections also have a greater likelihood of having concomitant Aspergil-lus lung disease.20
BIOFILMS
Costerton in 198421 hypothesized that P. aeruginosa in human infections “attaches to solid or tissue surfaces and grows predominantly in biofilms that release mobile swarmer cells into the surrounding fluid phase. These natural and pathogenic biofilms are covered by an exopolysaccharide matrix (glycocalyx) that serves as a barrier against hostile environmental factors such as host defense mechanisms and antibiotics.”21 Since this discov-ery, there has been clear evidence for the clinical sig-nificance of biofilms in promoting chronic infection in the airways of CF patients22 as well as a variety of other infections.23 P. aeruginosa, among its various attributes, enjoys cilia-driven motility, which appears critical in the aggregation phase of early biofilm formation.24 Once biofilm formation has commenced, features of growth and gene activation that release virulence factors are influenced by “quorum sensing.” Owing to a combina-tion of physicochemical factors that deny access to the microbes by host defense cells and/or antibiotics, infec-tion may persist despite aggressive treatment. In vitro testing indicates that bacteria embedded in biofilms can survive despite exposure to concentrations of antimicro-bials that exceed the minimal inhibitory concentration in a suspension culture by 1000-fold.25 We may antici-pate that future understanding and optimal management of patients with chronic BXSIS will entail interventions to modify or interfere with biofilms.24
ASSOCIATED DISORDERS AND PREDISPOSITIONS
Lung Injury Due to Acute InfectionIn the traditional model of lung injury due to acute infec-tion, patients are deemed to have normal airways and lungs until they experience a specific lower respiratory tract infection that results in irreversible damage to their airways. In the modern era in industrialized nations, most episodes of lower respiratory tract infection—ade-quately treated—resolve without residual damage even-tuating in BXSIS. However, among the older generations who were not protected by readily available antibiotics and vaccines, there are individuals who offer a convinc-

1028 ObstructiveDiseases
Other, less common primary immune disorders that may result in recurrent or refractory respiratory infec-tions leading to bronchiectasis include hyper-IgM or hyper-IgE (Job’s) syndrome and thymic hypoplasia result-ing in abnormal cellular immunity (DiGeorge syndrome). There are two forms of the hyper-IgE syndrome: an auto-somal dominant form caused by mutations in the signal transducer and activator of transcription 3 (STAT-3) gene, resulting in STAT-3 deficiency, and an autosomal recessive form, for which the precise genetic cause is not known.38 The susceptibility of such individuals with dominant hyper-IgE syndrome to pyogenic bacteria and NTM organisms may be due to impaired production of cytokines secreted by type 1 helper T cells such as interferon-γ, tumor necrosis factor-α, and interleukin-17 (IL-17), cytokines known to be important in controlling such infections.39 Genetic anomalies that may result in combined humoral and cellular impairment include severe combined immunodeficiency syndrome (SCIDS), “bare lymphocyte” syndrome, Wiskott-Aldrich (an X-linked recessive illness associated with small platelets and eczema), cartilage-hair hypoplasia (associated with short-limbed dwarfism), ataxia-telangiectasia syndrome, and a variety of other rare disorders.
Alpha1-Antitrypsin AnomaliesVarious phenotypic abnormalities of alpha1-antitrypsin (AAT) appeared prominently in a recent series of patients seen at the NJH with BXSIS associated with NTM.40 Pre-viously, there have been reports of the relationship between AAT deficiency and BXSIS.41,42 However, in the great majority of cases in the NJH series, the patients were not deficient in AAT but had heterozygous pheno-types (mainly MS; to a lesser extent MZ) with normal AAT levels. The prevalence of AAT anomalies in the overall cohort of NJH patients with various NTM infec-tions was 17%40; even more striking was the 27% preva-lence of AAT anomalies in the patients with rapidly growing mycobacterial disease.43 Based on various surveys, AAT anomalies would be anticipated in roughly 8% to 9% of the U.S. population.44 However, the role of heterozygous anomalies of the AAT system in the patho-genesis of lung disease is controversial.45 The majority of the NJH patients did not have significant chronic obstruc-tive lung dysfunction or grossly visible emphysema on CT scanning. Hence, we postulate that the AAT anoma-lies render the patients more vulnerable to respiratory tract infections. Inferential evidence in support of this hypothesis includes an informal survey done among emphysema patients being repleted with Prolastin46; 74 of the 89 responding patients described a perceptible benefit, and 56 of the 74 identified a reduction in the frequency of infectious exacerbations of their chronic obstructive pulmonary disease. Possibly relevant to the development of BXSIS is the observation that AAT is produced in airway epithelium (as well as the liver) and “Z” AAT may polymerize in the lung and act as a chem-oattractant.47 Direct evidence in support of the effect of AAT on infection includes evidence that aerosolized Prolastin suppresses P. aeruginosa lung infection in an
concluded that the modifying factors outside the CFTR genome could result in a clinical condition consistent with CF. It is our contention that heterozygous anoma-lies in the CF gene acts as a predisposing factor for BXSIS.
Based on contemporary understanding of the complex and diverse features of CF, there appear to be two groups in whom BXSIS occurs. The first and obvious group includes those with classic infancy/childhood-onset disease in whom clinical and laboratory data readily confirm the diagnosis of CF. The other group involves those with less severe disease that manifests later in life and for whom diagnostic testing is ambiguous.32 Sweat chloride testing may or may not be abnormal, and geno-typing may demonstrate heterozygous or even normal CFTR alleles. We might include under this rubric persons carrying the label of Young’s syndrome (males with BXSIS, sinusitis, and obstructive azoospermia) and males with congenital bilateral absence of the vas deferens,33 who have not been consistently regarded as having variant CF.
There are a wide variety of genetic factors lying outside the CFTR region that influence the clinical phe-notypes of the patients.34 (See Chapter 41 for additional discussion.)
Disorders of ImmunityImmunologic deficiencies are also associated with the development of BXSIS. Primary diseases that result in immunodeficiency may devolve from mutations that impair B or T lymphocytes and cause abnormal humoral immunity, cellular immunity, or both. Less frequent anomalies may involve natural killer (NK) lymphocytes, neutrophils, or complement proteins. Some specific immune disorders are noted later.
Common variable immunodeficiency (CVID), or acquired hypogammaglobulinemia, is the most frequent syndrome recognized in this group of diseases. Clini-cally, it is seen equally among males and females, distin-guishing it from X-linked agammaglobulinemia (Bruton’s disease), which exclusively involves young males. It may occur throughout all age groups, although it is most commonly recognized in early childhood. Although there are normal numbers of circulating B lymphocytes, they fail to differentiate into antibody-producing cells. This results in particular vulnerability to infections with encapsulated bacteria such as S. pneumoniae, H. influ-enzae, S. aureus, and P. aeruginosa. Recurring infec-tions of the airways with these and other organisms frequently result in BXSIS.35 The diagnosis is established by demonstrating low levels of gamma globulin and failure to produce appropriate antibody responses fol-lowing vaccination. A variant of the hypogammaglob-ulinemic disorders is selective deficiency of subclasses of immunoglobulin G (IgG), notably IgG2 and IgG4.
36 Because repletion with gamma globulin is so useful in controlling the recurrent infections, pursuit of the diag-nosis of deficient antibody production (CVID or Bruton’s disease) is strongly indicated. By contrast, selective defi-ciency of secretory IgA, another cause of recurrent res-piratory infections, cannot be controlled by repletion.37

42 brOnchiectasis 1029
Ciliated EpitheliumCongenital structural and functional disturbances of the ciliated epithelial cells are seen in association with BXSIS as well as with frequent and severe upper respiratory tract problems.52a,52b These disorders appear to be an autosomal recessive process, with an estimated fre-quency between 1 in 12,500 to 1 in 40,000.53 Primary ciliary dyskinesia (PCD) embraces a heterogeneous group of ultrastructural deficits involving the axoneme or central functional element of the cilia.54 The normal axoneme is composed of nine paired or doublet micro-tubules arrayed peripherally around two central, single microtubules; attached to the peripheral doublet micro-tubules are outer and inner dynein arms as well as radial spokes (Fig. 42-5). The direction in which the cilia beat is determined by the orientation of the two central microtubules. In a local sheet of bronchial ciliated epi-thelium, the axes of the central microtubules are arrayed within a fairly narrow range, typically deviating 25 degrees or less from each other along the long axis of the airway. A variety of abnormalities have been described, including the complete or partial absence of
animal model48 and the observation by Shapiro and col-leagues49 of the inhibitory effects of AAT on replication of the human immunodeficiency virus (HIV) in whole blood. Further support for a role of AAT in direct resist-ance to infection is the observation in an African popula-tion that two polymorphic variants of the AAT haplotype were associated with significantly greater risks of HIV infection when compared with the other nine haplo-types common in sub-Saharan African populations.50 Chan and coworkers43 showed that AAT inhibits phago-cytosis of Mycobacterium abscessus by human macro-phages, partially denying the mycobacteria their preferred intracellular milieu. It should be noted that a group from France studied AAT alleles in a large cohort of BXSIS patients and reached a different conclusion.51 They found the following phenotypes in their patients: MS 11.9%, MZ 3.5%, SS 1.5%, SZ 0.5%, ZZ 0.5%. In this study, the distribution of these phenotypes was not sig-nificantly different in their controls, and they inferred that AAT anomalies did not contribute to the risk for BXSIS. In a study of 74 patients with severe AAT defi-ciency (PiZ phenotype), 70 had bronchiectatic changes on CT scan.52
Ciliary ultrastructure
Nexin links
Radialspokes
InnerDynein arm
OuterDynein arm
Microtubule doublets
Two centralsingle microtubules
Central microtubulesorientation definesaxis of beating cilia
Membrane encased axoneme
Axis
Membrane
FIGURE 42-5 n Ultrastructure of the cilia. The structure and function of cilia are elegant and complex. Each ciliated epithelial cell possesses approximately 200 cilia. The direction of ciliary beating is determined by the orientation of the inner pairs of microtubules. Dysfunction of the ciliary apparatus may involve a variety of structural abnormalities in the cilia or disorganization of the ciliary axes. The cilia beat in a relatively fluidic periciliary medium; above that, adherent by a thin physicochemical junction, is a gelatinous layer of mucus.

1030 ObstructiveDiseases
outer or inner dynein arms, a lack of radial spokes, dis-ordered microtubule arrangements, ciliary disorienta-tion, and other rare disturbances. Functionally, these disturbances result in reduced or disorganized beating of the ciliated epithelial cells or, in some cases, gross immo-tility. There may also be inversion of the normal ana-tomic locations for the organs of the thorax and abdomen, situs inversus universalis or partialis; PCD with situs inversus universalis is known eponymically as Kartage-ner’s syndrome. In the absence of normal ciliary activity, organ orientation appears random, resulting in situs inversus in roughly half of the cases. Evidence in support of this theory includes discordant organ orientation in monozygotic twins with disordered ciliary motility.55
The ineffectual beating of the ciliated cells results in stagnation and accumulation of mucus, which classically is associated with early-onset refractory or recurrent infections of the airways including otitis media, mastoidi-tis, sinusitis, and bronchitis. BXSIS is a common sequelae of PCD, typically involving the dependent zones includ-ing the lower lobes, right middle lobe, and/or the lingu-lar segment of the left upper lobe (Fig. 42-6). The defect also involves the flagella of the spermatozoa, resulting usually, although not universally, in male infertility.
Diagnosing PCD is often problematic.56 Consideration should be given in the setting of early-onset upper and lower respiratory infections (see earlier). Male infertility, although suggestive, is more likely due to Young’s syn-drome in a North American population. A suggestive feature on high-resolution CT is predominant BXSIS in the lower lobes, with or without right middle lobe or
FIGURE 42-6 n Dependent-zone BXSIS in primary ciliary dyski-nesia (PCD). This 35-year-old white woman has classic PCD. She has atelectasis and saccular BXSIS involving the right middle lobe, the medial basilar segment of the right lower lobe, and the anteromedial aspects of her left lower lobe. She has previ-ously been treated for Mycobacterium avium complex (MAC) and now has refractory infections with P. aeruginosa.
lingular involvement and sparing of the upper lobes (unpublished data). Diffuse, softly marginated flocculent centrilobular opacities in the lower lobes is typical of PCD, reflecting chronic bronchiolitis. Electron micro-scopic analysis of the ultrastructure of the cilia or clearly documented ciliary dysfunction via high-speed video microscopy are the “gold standard” for diagnosis. However, such testing is complicated by the following factors: (1) chronic infection may denude the airways of ciliated epithelium and (2) chronic infection may damage cilia, resulting in nondiagnostic findings. One report demonstrated that computer-assisted analysis can increase the diagnostic yield significantly over conven-tional transmission electron microscopy for inner dynein arm disturbances.57 Direct measurements of ciliary beat frequency or coordination is available only in selected research centers. Among males, dysmotile or immotile spermatozoa may be demonstrated, and ultrastructural analysis of the sperm flagella may confirm the diagnosis. The “saccharine test” has also been employed as an infer-ential test of ciliary dysfunction. The primary utility of the saccharine test is to exclude PCD by a normal value. An abnormal saccharine test is consistent with, but not diagnostic of, PCD, as individuals with other disorders that result in chronic rhinosinusitis may have denuded their ciliated epithelium or have inflammatory factors that impair ciliary beating. Thus, the test should not be done within a month of an upper respiratory infection.
The latest test for the diagnosis of PCD is nasal nitric oxide (NO) levels.56 In a large cohort with proven PCD, nasal NO levels were significantly lower than in normals or subjects with CF. Of interest, parents of PCD patients had lower than normal nasal NO levels, intermediate between controls and patients, despite the absence of clinical disease.
Patients with PCD, sinusitis, and BXSIS also have a marked tendency toward colonization and infection with H. influenzae.56 The mechanism(s) for this predilection is unknown. Defective adaptive immunity is a plausible candidate.34
Bronchial CartilageCartilaginous “C-rings” are present throughout the entire trachea as well as the large and medium-sized airways, typically down to the fourth through sixth generations of the ramifying bronchi. The primary functional role of these structures is to maintain airway patency during expiration including cough. There are two well-described heritable syndromes that involve these cartilaginous structures.
Mounier-Kuhn syndrome, or congenital tracheobron-chomegaly, is a rare disorder associated with gross enlargement or dilation of the C-rings in the trachea and segmental bronchi58 (Fig. 42-7). The underlying defect is atrophy and even absence of elastic fibers and smooth muscle tissues of the large airways.59 In addition, primary or secondary atrophy of the connective tissue between the rings may result in outpouchings or diverticula, potentially serving as reservoirs for recurrent infections. Distal to the involved airways, bronchial structures gen-

42 brOnchiectasis 1031
infections when tracheal diverticula are present and difficulty with bronchial anastomosis due to discrepancy in the airway diameters between the donor and the recipient lungs.
Williams-Campbell syndrome, or congenital bronchial cartilage deficiency syndrome, is another rare disorder that tends to present early in life with recurring infection and BXSIS.60 The absence of cartilage from lobar through the first few generations of segmental airways is the typical finding in Williams-Campbell syndrome, although main-stem bronchi may be affected as well. Characteris-tic findings on CT scan include more extensive periph-
erally appear normal. Clinically, Mounier-Kuhn patients may present in their early years or as late as the fourth decade with recurring lower respiratory infections. In advanced stages, airway collapsibility may result in severe airflow obstruction. The diagnosis is readily made by finding extraordinary dilation of the trachea and central bronchi on CT scans, with airway dimensions 3 standard deviations greater than normal. Special consid-erations in management include positive end-expiratory pressure support and silicone or metallic stenting. Lung transplantation is an option, although unique issues asso-ciated with Mounier-Kuhn syndrome include recurrent
A
B
CFIGURE 42-7 n Congenital tracheobronchomegaly (Mounier-Kuhn syndrome) with BXSIS. This 73-year-old woman has had recurring respiratory infections throughout her adult life, most recently associated with Mycobacterium avium complex. A, On the poster-oanterior view, a massively dilated trachea (arrow) is seen. B, The dilated trachea with prominent cartilaginous rings is confirmed on a computed tomography (CT) scan. C, Not only is the trachea enlarged, but the main-stem bronchi are dilated.

1032 ObstructiveDiseases
notypic findings among these patients that are mindful of these connective tissue disorders are various combina-tions of scoliosis, straight-back syndrome, pectus exca-vatum or unusually narrowed anteroposterior chest diameter, pectus carinatum, and/or mitral valve pro-lapse. Among a series of 63 patients reported from the NIH with NTM lung disease, predominantly manifested by BXSIS, careful morphometric studies were per-formed.30 Compared with the women in the National Health and Nutrition Examination Survey (NHANES) database, patients with NTM lung disease were found to be significantly taller and more slender. In addition, pectus excavatum, scoliosis, and mitral valve prolapse were found in excess of expected rates. However, the patients did not have dolichostenomelia (a long, narrow frame), hyperdistensible joints, arachnodactyly, or overt aortic root involvement to suggest classic Marfan syn-drome.30 Neither do they have the cutaneous or joint abnormalities typical of Ehlers-Danlos syndrome. Our supposition is that the fundamental “defect” having to do with a propensity for BXSIS is “weakness” of the con-nective tissue of the bronchial tree. Notable among our patients, as well as other series of females with BXSIS associated with environmental mycobacteria, is bron-chiectatic involvement of the right middle lobe and lin-gular segment of the left upper lobe. Our hypothesis does not identify the “prime factor” in the pathogenesis of the BXSIS: do the airways dilate in response to the high intra-airway pressures generated during coughing that is incidental throughout life, or is there an underly-ing structural or functional defect that increases the risks for infections that set in motion the coughing and inflam-mation that lead to BXSIS?
Could slenderness itself—independent of malnutri-tion or any underlying illness—predispose individuals to mycobacterial infections? One intriguing hypothesis for the increased susceptibility to mycobacterial infections in thin individuals is due to a relative deficiency of leptin, which is normally produced by fat cells. Experimental corroboration for the leptin hypothesis comes from studies showing that leptin-deficient (ob/ob) mice are more susceptible to M. tuberculosis and M. abscessus lung infections.65
In view of the preponderance of females in recent series with BXSIS associated with MAC, two theories have been proposed. “Lady Windermere’s syndrome,” named after a character in a novel by Oscar Wilde, posits that women—in the effort to be demure or elegant—voluntarily suppress their cough, leading to accumula-tion of secretions and chronic infections.66 However, it has been our observation that these patients cough fre-quently.67,68 Rather than voluntary suppression, it seems more plausible that their coughing may be ineffectual due to airway collapsibility, which interrupts movement of secretions out of the bronchial tree.
An alternative proposition came from Japan where they, too, have noted a particular female vulnerability to BXSIS with MAC, largely among elderly, postmenopausal women.69 Tsuyuguchi and associates69 demonstrated that among female mice, oophorectomy led to higher mycobacterial loads in the lungs and spleen following intravenous challenge with MAC. Furthermore, estrogen
eral BXSIS than would be anticipated by the clinical history and more proximal extension of BXSIS than usual (Fig. 42-8). Inspiratory ballooning and expiratory col-lapse of the airways on chest CT scan is characteristic of Williams-Campbell syndrome.61 The degree of peripheral airway distortion suggests that this disorder entails more than simply the absence of proximal cartilage. Patients with Williams-Campbell syndrome are particularly pre-disposed to proximal bronchomalacia after transplanta-tion due to the combined effects of cartilage deficiency in the main-stem bronchi plus decreased blood supply to the proximal airways due to loss of collateral circula-tion of the transplanted lung.62
Connective TissueAmong the various formally described heritable disor-ders of the connective tissues, BXSIS and other structural abnormalities including extensive cystic degeneration of the lungs have been noted most extensively in those with Marfan syndrome.63,64 In addition to airway and parenchymal abnormalities, persons with Marfan syndrome have various other anomalies, including pectus excavatum, pectus carinatum, scoliosis, straight-back syndrome, and mitral valve prolapse. Two of these con-ditions, scoliosis and mitral valve prolapse, are found often in patients with two other connective tissue disor-ders, Ehlers-Danlos syndrome and cutis laxis.
This constellation of findings is mindful of the proto-typic female patients we and others are seeing with BXSIS, most commonly in association with NTM. Based on analogy to these heritable disorders, we believe that there may be subtle anomalies or polymorphic variants of connective tissue that predispose to their BXSIS. Phe-
FIGURE 42-8 n Williams-Campbell syndrome. This 50-year-old man had a lifelong history of recurring respiratory infections and productive cough. The airways are massively dilated with collections of respiratory secretions pooling in some of the cystic spaces. Notable are the normal dimensions of the main-stem bronchi.

42 brOnchiectasis 1033
resulting in traction and airway distortion, endobron-chial granulomatous inflammation including stricture with poststenotic infection, or compression secondary to hypertrophic peribronchial lymphadenopathy.70
Rheumatoid arthritis (RA) may entail a variety of pul-monary manifestations. In two early series, BXSIS was seen in 3.2%71 and 5.2%72 of referral populations of RA patients. More recently, BXSIS has been described in considerably higher percentages of RA patients undergo-ing high-resolution CT scanning: 20% to 35%73; surely, these studies were skewed by selecting patients with respiratory problems to undergo CT scanning. However, BXSIS was seen in 8% of RA patients without respiratory symptoms.74 Notably, the majority of the patients in the previously discussed series did not have RA-associated interstitial fibrosis as a presumed cause of the BXSIS. Potential causal mechanisms include increased propen-sity for infections, either intrinsic to RA or secondary to steroid or cytotoxic therapy. Sjögren’s syndrome in asso-ciation with RA has also been proposed as a risk factor, but the evidence is inconsistent.73 Clinically, it should be noted that the presence of BXSIS in RA patients was associated with an unfavorable prognosis in one series.75
Ankylosing spondylitis has been classically associated with upper lung zone fibrocystic degeneration and anky-lotic fusion of the junctions of the ribs and vertebrae, resulting in restricted ventilation. However, in a large series from the Mayo Clinic, pulmonary involvement was described in only 1.2% of the patients.76 BXSIS independ-ent of apical fibrocystic disease has been seen in a small series from the United Kingdom.77 Ankylosing spondyli-tis was reported in association with MAC in an early series from the NJH.78
Systemic lupus erythematosus (SLE) may involve an assortment of pulmonary complications, including those intrinsic to SLE and others related iatrogenically (see Chapter 58). BXSIS, as such, was described in 21% of SLE patients studied with high-resolution CT in one series79; factors related to BXSIS were not well studied. As with RA, the presence of Sjögren’s syndrome may be a comor-bid element.
Sjögren’s syndrome (SS), keratoconjunctivitis sicca and xerostomia (dry eyes and mouth), may exist in the primary form or in association with other collagen vas-cular diseases such as RA or SLE. Pulmonary complica-tions of SS include lymphocytic interstitial pneumonia, lymphoma or pseudolymphoma, and/or pulmonary hypertension (see Chapter 58). BXSIS has also been noted.80–82 It is reasoned that lymphocytic inflammation results in impaired function of mucous glands, in turn resulting in decreased volumes and increased viscosity of mucus. This leads to airway obstruction, poor clear-ance, and chronic infection. There have not been large surveys employing the CT lung scan in SS patients to quantify the risk for BXSIS. However, we have recently seen several elderly female patients with primary SS in whom BXSIS was prominently involved.
Inflammatory bowel disease (IBD) has been related directly to BXSIS.83 IBD-associated BXSIS appears to be more common with ulcerative colitis than Crohn’s disease.84 In the majority of cases, the IBD antedates the lung manifestations, but in some cases, the pulmonary
repletion normalized the bacillary burden, and ex vivo macrophages supplemented by estrogens were more competent at limiting mycobacterial growth.
However, neither the putative relationship to connec-tive tissue disorders nor the alleged role of estrogen deficiency can explain the striking disparity of females in recent reports of MAC-related BXSIS. In these series, 80% to 95% of patients described have been women.6–8 Certainly, this might reflect referral or reporting bias. Furthermore, we cannot exclude the possibility of sex-associated effects on connective tissue strength/integrity or cellular immunity.
An additional remarkable element of the reported cases of MAC-associated BXSIS is the strong preponder-ance of whites. White females constitute 80% to 95% in recent series, including those compiled in communities/areas with large African American, Hispanic, or other minority populations.6–8 Again, given the potential for referral, reporting, or ascertainment biases, we cannot be sure of the validity of these observations. However, among the specialists with whom we correspond, this is a strongly held perception. The relatively higher preva-lences of CF and AAT anomalies in European-derived populations may partially, but not wholly, explain this apparent imbalance.
Congenital and Developmental AnomaliesConditions such as sequestration, agenesis, hypoplasia, and atresia may result directly in BXSIS or may predis-pose to infections that eventuate in this condition. Sequestrations presumably develop due to accessory pri-mordial lung buds, which may be invested within normal lung tissue (intralobar) or external to the normal lungs (extralobar). Sequestrations may or may not connect with the bronchial tree and often derive their blood supply directly from the aorta. Clinically, they most com-monly present with recurrent and/or chronic lower res-piratory tract infections beginning in the second or third decade of life. Radiographically, they usually appear as irregular, peculiar densities abutting the diaphragm in the posterior basal regions. Unilateral hyperlucent lung (Swyer-James-MacLeod syndrome) is characterized by unilateral bronchiolitis leading to hyperinflation. In some cases, BXSIS is present. The etiology(ies) and pathogenesis of this rare disorder are uncertain but may involve developmental or acquired disturbances of the bronchial tree.
Idiopathic Inflammatory DisordersThere are a wide array of conditions associated with BXSIS that might be included under the rubric of idio-pathic inflammatory disorders. They are all systemic ill-nesses that variably involve the lungs and, in such cases, may or may not result in BXSIS.
Sarcoidosis is by far the most common of these disor-ders. (See Chapter 59 for a comprehensive review.) Broadly, sarcoidosis may involve the airways by several fundamental mechanisms: diffuse parenchymal scarring

1034 ObstructiveDiseases
so high that one might question whether the esophageal findings were the cause of recurring infections/BXSIS or, in some cases, an effect. In the latter regard, it is impor-tant to note that among series of patients with chronic asthma and idiopathic pulmonary fibrosis, the incidence of demonstrated esophageal dysfunction ranged from 80% to 95%.88,89 It is plausible that labored breathing with wide disparities between intra-abdominal and intratho-racic pressure and/or chronic coughing, which stresses and dilates the diaphragmatic ring, might disrupt the LES and subject the esophagus to distending forces.90 An additional factor that could contribute to GER is the medications employed for these pulmonary disorders, including anticholinergics, β-agonists, theophylline, and corticosteroids, all of which impair LES function,91 and broad-spectrum antibiotics which alter gastroesophageal flora.
In any case, clinicians should be alert to the potential of GER/aspiration as a primary or contributing role in the development of BXSIS. For those suspected of disordered deglutition, tailored hypopharyngography employing contrast materials of varying consistency may identify unsuspected aspiration. It is important to note that some patients spill contrast material into their trachea without any awareness or coughing. Such studies may be performed with a speech therapist, who can also aid patients with safer techniques for eating, drinking, and swallowing.
Impaired esophageal motility may be suggested on CT scans of the lungs in which the esophagus is grossly dilated, there is excessive air present along the course of the esophagus, or the walls of the esophagus are thick-ened. Impaired motility may often be demonstrated on a simple barium swallow. The extent of impaired contrac-tility may be measured by esophageal manometry; this is critical if reconstitution of the LES is contemplated. Dem-onstrating actual reflux may be problematic. If gross reflux is demonstrated on a routine study, it is sufficient for a presumptive diagnosis. However, if symptoms or other clinical features suggest GER and the upper gas-trointestinal series is negative, a 18- to 24-hour pH probe with or without measurement of impedence may both identify and quantify reflux episodes.88 Recent studies have documented that nonacid reflux may result in chronic cough and even lung injury.92 Among the impli-cations of these findings is that acid-inhibition measures may not be sufficient to protect the airways. For indi-viduals with evidence of recurrent aspiration, elevation of the head of the bed should be done routinely.
Toxic inhalation or thermal injury may also be associ-ated with BXSIS. Acute and chronic inflammation of the tracheobronchial tree, bronchiolitis, bronchiolitis oblit-erans, and diffuse alveolar damage may occur after expo-sure to toxic metal fumes (e.g., aluminum, cadmium, chromium, nickel) or toxic gases (e.g., ammonia, chlo-rine, phosgene, sulfur dioxide) (see Chapter 68). In severe cases, BXSIS may ensue due to either infectious complications of the exposure, denuding of the ciliated epithelium, or progressive fibrosis. Similarly, chronic airway damage and BXSIS may evolve following thermal or smoke injury.
symptoms may herald the IBD. Proposed pathogenic relationships include a cryptogenic infection that incites both airway and intestinal inflammation, common epi-thelial targets of autoimmunity, or sensitizing agents that are inhaled and/or ingested.
Relapsing polychondritis (RP) is identified essentially as progressive inflammation, weakness, and deformity of cartilaginous structures including the ears, nose, larynx, and tracheobronchial tree, typically associated with nonerosive polyarthritis. In addition, there may be inflammatory and/or functional disturbances of the eyes or the auditory/vestibular components of the ears. Res-piratory involvement is a common clinical element of RP and a major cause of mortality. BXSIS in such patients may be due to primary bronchial damage and/or recur-rent infection.85
Aspiration/Inhalation AccidentsSpillage of foreign matter into the airways may result in BXSIS. There are two fairly distinct scenarios in which such matter might be aspirated into the lungs and cause sufficient damage to result in chronic deformity of the airways. One is the direct spillage of secretions from the oropharynx, infamous for a plethora of microorganisms including microaerophilic and anaerobic bacteria which can produce necrotizing pneumonia. The other is intro-duction of materials refluxed from the esophagus and/or stomach, which, in addition to the microorganisms noted earlier, contain food particles, hydrochloric acid, biliary or pancreatic secretions, and microbes indige-nous to the gut including Helicobacter pylori.86
Laryngeal protective functions are imperfect, and “microaspiration” occurs frequently. Thus, we might presume that aspiration leading to lower respiratory tract infections involves greater than usual volumes and/or more noxious contents. Also, it is reasonable to posit that once the airways have been damaged, a lesser inoc-ulum can have more substantial clinical effects, a variant of the “vicious circle” theory.
Many factors influence the likelihood/frequency of aspiration. They include (1) depressed sensorium (trauma, alcohol or drug abuse, postictal, general anesthesia); (2) altered brain-stem function (post–cerebrovascular accident, postpolio, primary neurologic diseases such as multiple sclerosis, amyotrophic lateral sclerosis, or syringomyelia); (3) altered laryngeal structure/function (postsurgery, postirradiation); (4) esophageal disorders (dysmotility, obstruction by tumors or strictures, muscu-lar dystrophy, achalasia, tracheoesophageal fistulas, or lower esophageal sphincter (LES) incompetence); and (5) gastric dysfunction (dysmotility or outlet obstruction).
Although all of these elements may contribute to the risk of infection (and BXSIS), it seems likely that gastro-esophageal reflux (GER) is the most common factor. Among a cohort of BXSIS patients noted previously from the NIH, approximately three fourths of them had dem-onstrated abnormalities of esophageal morphology (dila-tion and thickening), function (dysmotility), anatomy (hiatal herniation), or competence (overt reflux).87 Indeed, the frequency of esophageal disturbances was

42 brOnchiectasis 1035
ABPA/M typically occurs in the setting of recurrent/refractory (steroid-dependent) asthma, clinicians should be aware that these episodes may also include fever, malaise, pleuritic chest pain, and cough productive of purulent secretions. Such episodes may be confused with pneumonia, acute bronchitis, and/or exacerbations of simple BXSIS, especially if the asthmatic component is absent or minimal. The picture may be particularly obscure if the ABPA/M occurs in individuals with CF, a disorder in which ABPA/M is relatively more common. Features mindful of ABPA/M include characteristic find-ings on CT scanning, eosinophilia, elevated IgE levels, and dramatic responses to corticosteroids.
The other pathway to BXSIS occurs in the setting of long-standing, inadequately controlled ABPA/M. In such cases, extensive fibrosis and airway distortion may evolve due to uncontrolled inflammation (Fig. 42-10). In these cases, the patients may acquire secondary airway patho-gens including P. aeruginosa or other gram-negative bacilli as well as NTM. In these “burned-out” cases, the patients may not demonstrate asthma, eosinophilia, or elevated levels of IgE.
MiscellaneousThere are numerous other causes of BXSIS including such diverse entities as HIV infection/acquired immuno-deficiency syndrome (AIDS), yellow-nail syndrome, or radiotherapy injury.
Among persons with AIDS, BXSIS has been identified in a significant proportion of those undergoing CT scans, including children.93,94 Obviously, this is skewed by the selection of those with respiratory problems for scan-ning. Presumably, the pathogenesis of the BXSIS involves
Postobstructive DisordersForeign bodies may be aspirated into the airways in association with infants and children putting foreign objects in their mouths, choking events while eating, trauma, or loss of consciousness including seizures. In some cases, the obstructing object may be radiopaque (teeth, bone, or metal objects), but in most instances, the obstructing material (e.g., peanuts, vegetables) is not discernible by radiographic study. Tumors, benign or malignant, may also result in airway obstruction, poor drainage, recurrent/chronic infection, and BXSIS. The more common tumor types include bronchogenic carci-nomas (particularly the squamous cell variety), bronchial adenomas, and papillomas. Extrinsic airway compres-sion due most often to hypertrophic lymphadenitis from granulomatous diseases such as sarcoidosis or infections such as tuberculosis or histoplasmosis may severely narrow or even occlude large airways. In patients with “focal” BXSIS (particularly those with disease limited to only one region, one segment, one lobe, or even one lung), bronchoscopic examination to exclude an obstructing lesion should be performed early if other causes are not evident.
Allergic Bronchopulmonary AspergillosisIn acute or subacute bronchopulmonary aspergillosis (or other mycoses), ABPA/M, patients develop mucoid plugs in the medium-sized bronchi. The inflammation and dis-tention typically results in thin-walled BXSIS of the central and mid-lung airways (Fig. 42-9). Although
BAFIGURE 42-9 n Allergic bronchopulmonary aspergillosis with mucus-plugging and thin-walled BXSIS. This 44-year-old woman with steroid-dependent asthma reported coughing up gray-green mucus plugs. She had immunoglobulin E (IgE) levels over 1000 IU/mL, 10% to 15% eosinophilia, and precipitins to Aspergillus fumigatus. A, A classic serpentine mucus plug in the anterior segment of the right upper lobe. B, A more cephalad axial CT image of the same patient, showing central thin-walled BXSIS, presumably residual to the more distal mucus plugging.

1036 ObstructiveDiseases
severe, chronic, and recurrent infections with a variety of opportunistic pathogens. An additional element that has not been fully addressed is the potential impact of oxidative damage associated with infection or other stressors on the AAT system.95,96 Impairment of AAT function may contribute to the accelerated lung damage, including BXSIS, in persons with AIDS.97,98
Yellow-nail syndrome is an uncommon disorder marked by the triad of yellow, thick, dystrophic nails; chronic lymphedema of the face, hands, and lower extremities; and pleural effusions.99 Females are more often involved than males; the median age of onset is 40 years, with cases ranging from infancy to the seventh decade. The most prominent pulmonary finding is bilat-eral exudative pleural effusions.100 Recurrent sinusitis and lower respiratory tract infections are common.101 BXSIS presumably evolves due to chronic infection. Contributing factors may entail abnormal lymphatic structure, increased vascular permeability, deficient immunoglobulin production, and/or ciliary dysfunction.
Radiation therapy (XRT), typically delivered for carci-noma of the breast or mediastinal tumors including lym-phomas, may result in profound damage to the central airways. This reaction is not part of the postirradiation bronchiolitis obliterans syndrome but a distinctive condi-tion marked by focal damage to the cartilage and mucosa of the airways leading to patulous distention and irregu-larities of the major bronchi in the field of irradiation. In our experience, BXSIS secondary to XRT given for neo-plasms has become less common in the recent era when the control of dosage and field has become more refined. In some cases, this condition may be recognized by lung parenchymal scarring in the field of irradiation (Fig. 42-11).
FIGURE 42-10 n Late fibrocystic damage from allergic broncho-pulmonary aspergillosis (ABPA). The patient is a 70-year-old man with a 30-year history of poorly managed ABPA. CT scan shows residual central thin-walled BXSIS (arrow) in addition to fibrotic and cystic damage.
FIGURE 42-11 n BXSIS in a field of therapeutic x-irradiation. This 68-year-old woman had been diagnosed with a non–small cell carcinoma of the lung. She received radiotherapy to the right hilar region approximately 18 months previously. Her CT scan shows dense fibrosis and BXSIS in the radiation field. Inferior to this process she had a necrotic, cavitary process associated with Mycobacterium avium complex infection.
DIAGNOSIS
In the great majority of cases, BXSIS is recognized in the context of chronic or recurring lower respiratory tract infections (deemed to be “bronchitis” or “pneumonia”) over many months or years. Some BXSIS patients in whom wheezing is a prominent element may have been identified and treated as “asthmatics” for many years. Occasionally, patients come to attention following an episode of hemoptysis. Less frequently, BXSIS is identi-fied on CT scans done for other considerations.
Although the plain chest radiograph can suggest BXSIS with “tram tracks” (Fig. 42-12) or multiple ring shadows (Fig. 42-13), CT scanning is the current diag-nostic study of choice. The finding on the plain lateral chest radiographs of atelectasis of the right middle lobe and/or lingula (Fig. 42-14) is highly suggestive of coexisting BXSIS and should be followed by CT scanning in patients with persistent abnormalities and chronic symptoms.
Once BXSIS has been identified on CT scan, what studies should be performed to help direct management and classify the disease? Certainly, a careful family history may be useful in identifying genetic risk factors; however, the family pattern is rarely specific for a particular disor-der unless there is a clear story for CF.
Past medical history and review of systems should focus on the various disorders noted in Table 42-1 and delineated earlier in the discussion of associated disor-ders and predispositions.

42 brOnchiectasis 1037
Airway Hygiene and Hyperosmotic AgentsAirway hygiene consists of nonantibiotic therapies directed toward mobilizing and eliminating inflamma-tory secretions from the tracheobronchial tree and from the paranasal sinuses. Also included under this rubric are steps to prevent/limit aspiration of oropharyngeal or gas-troesophageal contents into the airways.
Hypertonic saline, 7% twice or four times daily, has been shown to accelerate mucus clearance, decrease exacerbations, and improve lung function in CF patients.110 However, its role in non-CF BXSIS remains to be seen. Inhaled dry powder mannitol appears promis-ing in airway clearance in bronchiectatic patients,111 although more definitive studies are needed.
Antimicrobial TherapyAntimicrobial therapy historically has been the center-piece of BXSIS care. However, there is no clear consen-sus on the major questions in this area including whether treatment should be given on a routine, periodic sched-ule (“rotating”) or an as-needed basis for clinical exacer-bations. In a meta-analysis that studied the use of prolonged oral antibiotics for purulent BXSIS, sputum volume/purulence was shown to decrease, but there were no significant beneficial effects in regards to rates of exacerbations, lung function, or death.112 As well, there are limited data on the preferability of empirical selection of an antimicrobial agent or treatment guided by species identification and in vitro susceptibility testing.
Laboratory testing may variously include the studies noted in Table 42-2. These tests need not all be per-formed on initial assessment but may be done sequen-tially, with the more probable disorders being checked initially.
MANAGEMENT
The care of patients with BXSIS typically involves many layers, which may be partitioned into five broad components: airway hygiene, antimicrobial treatment, anti-inflammatory therapy, surgery, and miscellaneous. These modalities are delineated in Table 42-3. Although most patients with BXSIS require various elements of each of these components to enjoy optimal health, there is not a standard formula for treating this disorder. The great majority of recurrently or chronically sympto-matic patients benefit from a regular mucus-clearing regimen and periodic antibiotic therapy. For most patients, a pragmatic or “trial-and-error” approach is required to determine individual needs, preferences, and tolerances.
It is important to note that most elements described in this section have not been proved to be efficacious by randomized, controlled clinical trials. Thus, meta-analy-ses (such as the Cochrane Database of Systematic Reviews) generally cannot confirm the benefits or dysu-tility of such approaches.102–109 Perhaps because BXSIS is such a complex mix of varying conditions and/or has been an underappreciated “orphan” disease, a paucity of systematic research has been directed at this very trou-blesome disorder.
A BFIGURE 42-12 n “Tram tracks” on the routine chest radiograph in BXSIS. A, In the right lower lobe are parallel, nontapering shadows, “tram tracks” (arrow), representing BXSIS. B, The airway is seen as cylindrical BXSIS (arrow).

1038 ObstructiveDiseases
Anti-inflammatory TherapyThe obvious rationale for using the anti-inflammatory agents in BXSIS is that they may reduce the inflammatory cascade, with the goals not only of reducing symptoms but also to limit the progression of disease and decline in lung function. Anti-inflammatory agents that have been examined in BXSIS include the nonsteroidal anti-
Aerosolized antibiotics also appear promising in treating or preventing exacerbations. In patients with CF, inhaled tobramycin twice daily given in alter-nating months decreased the frequency of exacer-bations due to P. aeruginosa.113 Even in patients without CF, inhaled tobramycin was found to be efficacious.114
C
BA
FIGURE 42-13 n Multiple ring shadows on the plain chest radiograph in BXSIS. A, On the posteroanterior view, thin-walled cystic shadowing is seen in the right mid-lung field. The trachea and mediastinum are shifted to the right, indicating extensive volume loss. B, The lateral view confirms the presence of multiple ring shadows in the mid-zone. C, CT scan of this 65-year-old white woman indicates severe varicoid BXSIS involving her entire right middle lobe and the anterior segment of the right upper lobe.

42 brOnchiectasis 1039
acin significantly decreased the amount of sputum by half as well as the perceived dyspnea.115 Another mecha-nism by which indomethacin may help in BXSIS is via inhibition of neutrophil chemotaxis and neutrophil deg-radation of fibronectin, thereby decreasing airway inflam-mation and purulence.116
In a comprehensive Cochrane Database review of ran-domized trials of NSAIDs in CF patients, high-dose ibu-profen has been shown to slow the progression of lung disease, especially in children.117 In contrast, there have been no randomized, controlled trials on the use of NSAIDs in bronchiectatic patients without CF.118
inflammatory drugs (NSAIDs), inhaled corticosteroids, and intermittent macrolides to exploit their anti- inflammatory and other nonmicrobicidal activities.114a
NSAIDs
Because prostaglandins may play a role in augmenting airway secretions, the NSAIDs—by blocking the cyclooxygenase pathway—have been studied in BXSIS. In a double-blind, placebo-controlled study in patients with bronchorrhea due to chronic bronchitis, diffuse panbronchiolitis, and bronchiectasis, inhaled indometh-
A
B
CFIGURE 42-14 n Atelectasis and BXSIS involving the right middle lobe and lingula on plain chest radiographs and a CT scan. This 60-year-old woman has had recurring “pneumonia” throughout life. A, Posteroanterior view shows subtle effacement of the right heart border and cardiophrenic sulcus as well as a hazy opacity at the left heart border. B, On the lateral view, there are two oblique densities representing the atelectatic right middle lobe (arrow 1) and lingula (arrow 2). C, CT scan demonstrates BXSIS and atel-ectasis of the right middle lobe and inferior segment of the lingula.

1040 ObstructiveDiseases
TABLE 42-2. Diagnostic Studies for the Classification and Management of Patients with Bronchiectasis
Test Comments
ROUTINE, UNIVERSAL STUDIESComputed tomography
lung scan (CTLS)If bronchiectasis (BXSIS) is suspected, CTLS is the definitive test. Thin-section, high-resolution images may help
detect subtle airway dilation before bronchial walls are grossly thickened. Contrast is generally not helpful and may, in fact, compromise the overall resolution of the study. CTLS may also identify esophageal abnormalities.
Pulmonary function tests (PFTs)
For patients with significant BXSIS, comprehensive PFTs, including spirometry, bronchodilator responsiveness, lung volumes, and diffusion capacity, are important studies that aid in management and prognosis. PFTs may also provide useful hints regarding predisposing conditions.
Complete blood count Anemia may reflect effects of chronic infection or blood loss (consider inflammatory bowel disorders).
Leukocytosis may mark severity of infection.
Eosinophilia may suggest ABPA/M.
ESR, C-reactive protein Nonspecific markers of inflammation; very high levels may suggest underlying connective tissue disease or vasculitis.
Routine sputum culture
Antibiotic therapy in BXSIS should generally be directed against specific pathogens and guided by in vitro susceptibility. The presence of mucoid strains of Pseudomonas aeruginosa and Staphylococcus aureus may raise suspicions for CF. Stenotrophomonas maltophilia, Alcaligenes xylosoxidans, and Burkholderia cepacia are gram-negative bacilli that may prove problematic pathogens in patients with long-standing BXSIS. Isolation of B. cepacia and Helicobacter pylori require special laboratory techniques.
Mycobacterial sputum culture
Environmental mycobacteria such as Mycobacterium avium complex, M. chelonae, and M. abscessus appear to be increasingly common in contemporary BXSIS. May be commensal but often are pathogenic.
Fungal sputum culture Especially in patients with an asthmatic component, the presence of Aspergillus species (or other molds including Pseudallescheria or penicillium) may suggest etiology.
CT scan of sinuses Many BXSIS patients also suffer chronic rhinosinusitis. The presence of extensive sinus involvement suggests possible CF, immunoglobulin deficiencies, or ciliary disorders. Also, optimal management often entails aggressive sinus care.
SPECIFIC, DIRECTED STUDIESSweat chloride, CF
genotyping, and nasal potential differences
For BXSIS patients with bilateral disease, sinusitis, and no other identified risk factor, mild variants of CF appear to be relatively common (see text and Chapter 41). Sweat chloride is regarded as the primary screening test for CF, but a considerable portion of adults with CF have borderline or normal results. Nasal potential difference may be useful for identifying CF in equivocal cases (see Chapter 41).
Alpha1-antitrypsin (AAT) levels and phenotype
AAT anomalies appear to be a substantial risk factor for BXSIS, especially with white females. Abnormal proteinase inhibitor (Pi) phenotypes, even heterozygous patterns such as MS, appear to confer risk even with normal levels of AAT (see text). Repletion of AAT may enhance resistance to lower respiratory tract infections.
Immunoglobulin (Ig) levels
Deficiencies of IgG or IgA may promote BXSIS; IgG subclass deficiencies may also be a factor. Elevated levels of IgE may suggest ABPA/M or Job’s syndrome. Hyper-IgM may be associated, as well, with chronic infections.
Ciliary morphology or function
For individuals with suggestive stories (see text), a nasal ciliated epithelium biopsy with transmission electron microscopy may identify primary ciliary dyskinesia. Other studies including ex vivo ciliary activity, the saccharine test, or spermatozoa analysis may aid in this diagnosis (see text).
Nasal nitric oxide (NNO) levels
Patients with documented PCD have significantly lower levels of NNO than normals or patients with CF.56 Although not universally available, such testing may prove highly useful in identifying PCD. Paradoxically, exhaled NO levels have been elevated in BXSIS of diverse etiologies125 except CF.
Barium swallow (BaS) The BaS may detect disturbed deglutition, esophageal diverticula, obstructing lesions (tumors or strictures), hypomotility, achalasia, hiatal hernias, or lower esophageal sphincter (LES) incompetence with reflux. Note that the absence of reflux on a BaS does not exclude this problem (see pH probe).
pH probe For patients suspected of gastroesophageal reflux, an 18- to 24-hour study with a transnasal pH probe may identify, quantitate, and characterize reflux. Obviously, medications that inhibit acid production must be stopped before such tests.
Esophageal manometry For patients being considered for surgical repair of the LES, manometry should be performed to determine that the esophagus generates sufficient pressure to propel food and liquids through the tightened sphincter.
Tailored hypopharyngography (TH)
TH is useful in detecting abnormalities of the initial phase of swallowing, deglutition. Persons particularly prone to problems include those with prior strokes, Parkinson’s disease, bulbar disorders including postpolio syndrome, and those with prior laryngeal or pharyngeal surgery. Note that some patients have gross aspiration without clinical manifestations (choking, coughing); this may occur in individuals with none of the above risk factors.
LESS COMMON, EXOTIC STUDIESCollagen vascular
disease (CVD) serologies
Various CVDs may contribute to the risk for BXSIS, including RA, ankylosing spondylitis, and systemic lupus erythematosus. Thus, for patients with compatible histories or physical findings, assays for rheumatoid factor, HLA-B27, and ANA may provide insight into predisposing conditions. CVD serologies may also suggest the diagnosis of Sjögren syndrome, particularly SSA/Ro and/or SSB/La.
Schirmer’s test For patients with histories suggestive of “sicca syndrome” (dry eyes, dry mouth, oral ulcers), a positive Schirmer test may indicate the presence of either primary or secondary (associated with a CVD) Sjögren’s syndrome.
ABPA/M, allergic bronchopulmonary aspergillosis/other mycoses; ANA, antinuclear antibody; CF, cystic fibrosis; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; PCD, primary ciliary dyskinesia; RA, rheumatoid arthritis.

42 brOnchiectasis 1041
TABLE 42-3. Elements for Management of Patients with Bronchiectasis
Procedure Comments
AIRWAY HYGIENE
Tracheobronchial Clearance TechniquesMechanical “valve” devices
(Flutter, Pep, Acapella, and others)
A variety of these devices exist that are designed to transmit agitating forces to the airways to physically loosen and help propel tenacious secretions out of the bronchial passages. By retarding expiratory flow, they may also stent the airways open. For optimal results, respiratory therapists should assess individual patients’ needs and abilities and train them in proper usage.
Postural drainage and chest physiotherapy
For patients with dependent-zone bronchiectasis (BXSIS), positioning in the prone head-down, Trendelenburg, and/or lateral decubitus postures may promote local drainage. This might be optimized by pretreatment with mucus-mobilizing methods (see later) and clapping or vibrating techniques while in these postures.
Therapeutic vest The pneumatically powered jacket produces high-energy vibrating forces throughout the entire thorax. Of proven utility in CF,126 the vest may also be useful with BXSIS of other etiologies.
Mucus-Mobilizing Methods
Inhaled β-agonists (IBAs) and/or anticholinergic bronchodilators (ACBs)
IBAs may accelerate ciliary beat frequency as well as relieve the bronchospasm present in some BXSIS patients. Although the parasympathomimetic ACBs pose a theoretical risk for “drying” secretions, some BXSIS patients tolerate them and enjoy modest benefits not provided by IBAs.127,128
Hypertonic saline or mannitol inhalation
Nebulizing hypertonic solutions including saline or mannitol into the airways appears to aid patients in the clearance of tenacious secretions.129 Hypertonic saline is considerably less expensive than dornase alfa (see later). Mannitol has not yet been approved for use in the United States.
Dornase alfa (Pulmozyme) This product hydrolyzes neutrophil DNA, which contributes to the viscosity of inflammatory secretions. Of proven utility in CF patients,130,131 it was not beneficial in BXSIS of differing etiology in one trial.132 Extended administration in CF patients has been shown to reduce neutrophilic inflammation of the airways.133 However, we have found it useful in some patients with diagnoses other than CF. It is quite expensive and should be used judiciously.
N-Acetylcysteine (Mucomyst) Also used primarily in CF patients, it has been generally supplanted by dornase alfa.126 Its side effects include airway irritation when used in high concentrations. Given orally in Europe, this approach has not been proved efficacious, nor is it approved in the United States.
Anti-inflammatory Airway ManagementSystemic steroids Mucosal edema and the production of inflammatory secretions may be partially alleviated by
corticosteroids. Randomized, controlled trials in young patients with CF have shown improvements in clinical and physiologic parameters with extended courses of alternate-day steroids134,135 (see Chapter 41 for details). However, there were significant adverse effects, particularly on growth rates in males.136 Given these and other deleterious effects of long-term systemic steroids, such treatment arguably should be reserved for refractory cases.
Inhaled steroids (ISs) To avoid some of the complications of systemic steroids, inhaled treatment is a logical approach.137 Modest evidence of efficacy has been shown in some but not all trials with CF.119 ISs may also improve the airway hyperreactivity common among BXSIS patients.
Macrolide antibiotics (MLAs) In addition to their antimicrobial effects, MLAs have demonstrated host defense–modifying activities that include anti-inflammatory effects.86,140 Azithromycin, an azolide, given over many months has resulted in clinical and physiologic improvement among CF patients infected with Pseudomonas aeruginosa.141–143 These effects must be balanced against the considerable expense and potential for producing drug resistance among bacterial and mycobacterial pathogens common to BXSIS. (Patients should be screened for mycobacterial infections before use.)
Nonsteroidal anti-inflammatory drugs (NSAIDs)
Among young CF patients, long-term administration of ibuprofen has shown some benefits.144 However, these results may not be generalized, and NSAID therapy should be approached cautiously given the potential side effects and their expense.
Anti-aspiration MeasuresAnti-GER management Teaching patients to alter their dietary practices (reduced food and liquid intake in the evening), elevated
the head of the bed, or most drastically, surgical revision of the LES or hiatal hernia may lessen the risk of recurrent airway soilage.
Improved deglutition For patients who aspirate on swallowing, changing the consistency of foods or employing maneuvers such as the “chin tuck” may lessen the risk of airway soilage.
Reducing gastric acid Although lowering gastric acidity with proton-pump inhibitors or H2-blockers may diminish the symptoms of reflux, it is illogical to think that it should protect against aspiration. Theoretically, lowered acidity of the aspirated matter might result in reduced damage to the lungs; however, it should not be regarded as a lung-protective intervention.
ANTIMICROBIAL THERAPYEpisodic, targeted antibiotics Rather than administering “rotating” or “empirical” agents, this approach involves sampling respiratory
secretions during clinical exacerbations and employing antimicrobials on the basis of species identification and in vitro susceptibility. Although logically an attractive option, it entails inevitable delays in treatment and may be confounded by the presence of multiple, potential pathogens.
Continued

1042 ObstructiveDiseases
Procedure Comments
Rotating antibiotic therapy A popular practice, clinicians might treat BXSIS patients with a 1 wk/mo cycle of arbitrarily selected antimicrobials such as, for example, amoxicillin, a fluoroquinolone, and a macrolide. There is some evidence of utility for long-term antibiotic therapy145; however, the potential for selecting for drug-resistant strains is a consideration. Imperfect evidence reported in a recent analysis suggests that patients with chronic P. aeruginosa infection do better with targeted therapy.146
Initial empirical followed by targeted antibiotics
This approach offers the advantage of prompt treatment for an exacerbation, followed by a more narrowly focused regimen based on the results of the initial sputum cultures. To be representative, sputum sampling should be done before initiating empirical antimicrobial therapy.
Role of inhaled antibiotics The model of inhaled tobramycin in controlling pseudomonal infections in CF patients147,148 (see Chapter 41) is an attractive model for non-CF BXSIS as well.149 Certainly, for those patients with chronic or recurrent gram-negative bacillary infections, this approach might be considered. However, our early experience suggests less favorable tolerance of tobramycin in elderly subjects.
Therapy for exotic pathogens
Patients may either acquire secondary infections of preexisting BXSIS or primarily develop BXSIS due to exotic microbes such as environmental mycobacteria or fungi. In such cases, specific therapy may be indicated.
SURGERYResectional surgery There are no systematic studies of surgical interventions in BXSIS. However, anecdotal observations suggest
that extirpation of severely damaged lobes may confer considerable benefit. Disease limited to the right middle lobe or lingula may be particularly amenable.150–152 Whether such resections should be done through the lateral thoracotomy or VATS approach is unresolved, although our group strongly prefers the former.
Transplantation For younger patients with BXSIS-associated respiratory insufficiency, the question of transplantation may arise. Based on the model of CF, it is a plausible consideration.
MISCELLANEOUSVaccination vs. Streptococcus
pneumoniaeAlthough not specifically proved in BXSIS, this vaccine seems an obvious adjunct.
Vaccination vs. influenza In addition to vaccination, BXSIS patients should be considered for antiviral therapy if they develop clinical influenza.
Smoking cessation A priority for all pulmonary patients.
Alpha1-antitrypsin (AAT) repletion
Among COPD patients receiving AAT repletion, there was a perception of reduced frequency of infectious exacerbations (see text). For BXSIS associated with AAT anomalies, repletion might confer protection against recurrent infections.
Oxygen Patients with BXSIS, especially extensive lower lobe disease, may become hypoxic with exertion or with sleep. Early detection and O2 supplementation may improve exercise tolerance and physical conditioning. Nocturnal O2 may lessen pulmonary hypertension and delay the appearance of cor pulmonale.
Methylxanthines (Mx) Oral Mx (theophylline) theoretically might augment bronchodilation, enhance mucus clearance, and enhance diaphragmatic contractility. However, the side effects, variable pharmacokinetics including interactions with macrolide antibiotics, and GER-promoting effects make Mx a problematic element in most BXSIS patients.
Cromolyn, nedocromil, or leukotriene modifiers
Although these various asthma medications may have some theoretical roles in BXSIS, there have been no studies demonstrating efficacy.
CF, cystic fibrosis; COPD, chronic obstructive pulmonary disease; GER, gastroesophageal reflux; VATS, video-assisted thoracoscopic surgery.
TABLE 42-3. Elements for Management of Patients with Bronchiectasis—cont’d
Inhaled Corticosteroids
A review of clinical trials have shown that the use of inhaled corticosteroids in CF did not cause improvement.119
Intermittent Macrolide Therapy
Independent of their antimicrobial properties, macrolide antibiotics hold great promise in inhibiting disease activ-ity in BXSIS due to their nonantimicrobial immunomod-ulatory effects.120 Intermittent macrolide therapy may help in BXSIS via different mechanisms including decreas-ing chloride diffusion potential gradient across the airway mucosa (resulting in decreased sputum volume), reducing airway levels of the neutrophil chemotactic factor IL-8, inhibiting both neutrophil and Pseudomonas
migration, suppressing Pseudomonas quorum sensing, and disrupting the established biofilm layer.121 Clarithro-mycin but not amoxacillin or cefaclor was shown to significantly reduce sputum production in patients with chronic bronchitis or BXSIS. In a study of a small number of patients with BXSIS122 randomized to standard care for 6 months followed by the addition of azithromycin given at a dose of 500 mg twice weekly for 6 months or vice versa, azithromycin significantly decreased the incidence of exacerbations and sputum volume compared with standard care.123 Similar beneficial effects plus improve-ment in lung function have been shown in various trials using intermittent azithromycin therapy in CF patients chronically infected with P. aeruginosa but also in younger CF patients before they have been colonized with P. aeruginosa.124

42 brOnchiectasis 1043
SurgerySurgery remains a controversial issue in the management of BXSIS. No formal systematic studies of the indications and efficacy of resectional surgery have been conducted among patients with BXSIS. Traditional indications for resectional surgery have included chronic disabling infection, recurrent infections of intolerable frequency, or irreversible lung damage distal to a foreign body or benign tumor. Life-threatening hemoptysis may also provoke consideration of surgery, although therapeutic bronchial artery embolization may be the initial treat-ment of choice. A historical adage has been that surgery does not cure BXSIS. If true, it is likely due to our evolv-ing understanding that most cases of BXSIS are due
to innate risk factors that predispose to recurrence. However, surgery is still an appropriate palliative measure in selected cases.
MiscellaneousAdditional measures, such as vaccination against pneu-mococcal disease or influenza and smoking cessation, are appropriate for all patients. Intuitively, these meas-ures seem particularly important for those with BXSIS; however, no systematic information is available to confirm their usefulness. On the other hand, early rec-ognition of exercise and sleep-related hypoxia has sub-stantially demonstrated benefits in regard to morbidity and mortality.
Key Points
• BXSIS is defined by the presence of permanent dilation of the medium to large bronchi. The main clinical significance of BXSIS is recurrent airway infections by bacterial and fungal organisms resulting in chronic cough, sputum, weight loss, and respiratory compromise.
• Most BXSIS occurs owing to a combination of host susceptibility factors—which may be overt or covert—and the recurrent infections and the largely neutrophilic inflammatory response that perpetuate the airway injury.
• Localized BXSIS is most often due to suboptimally treated bacterial infections. BXSIS due to nontuberculous mycobacteria is increasingly recognized: the two predominant phenotypic presentations are elderly men with upper lobe fibrocavitary disease in a background of emphysema, and postmenopausal women with lingular and right middle lobe BXSIS and nodules.
• BXSIS that is more diffuse is generally due to an underlying host disorder such as cystic fibrosis, primary ciliary dyskinesia, disorders of cartilage as seen with the Mounier-Kuhn and Williams-Campbell syndromes, common variable immune deficiency, and allergic bronchopulmonary aspergillosis.
• BXSIS has also been associated with extrapulmonary disorders such as ulcerative colitis and collagen vascular diseases. Severe fibrotic lung diseases from any cause may also result in a form of BXSIS known as traction BXSIS.
• The linchpins in the management of BXSIS are the timely institution of antimicrobials to treat the culprit pathogens isolated and diligent airway clearance measures to improve symptoms and to decrease the frequency of such infections. Surgical lung resection should also be considered for patients with severe localized disease that are recalcitrant to medical treatment.
• Anti-inflammatory agents such as the NSAIDs and the low-dose intermittent macrolides are promising in helping to alleviate symptoms and reduce the rate of disease progression, but recommendations for their use remain to be defined.
References1. Pasteur MC, Helliwell SM, Houghton SJ, et al: An investigation
into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med 162:1277–1284, 2000.
2. Reiff DB, Wells AU, Carr DH, et al: CT findings in bronchiectasis: Limited value in distinguishing between idiopathic and specific types. AJR Am J Roentgenol 165:261–267, 1995.
3. Trucksis M, Swartz MN: Bronchiectasis: A current view. Curr Clin Top Infect Dis 11:170–205, 1991.
4. Barker AL, Bardana EJ: Bronchiectasis: Update of an orphan disease. Am Rev Respir Dis 137:969–978, 1988.
5. Singleton R, Morris A, Redding G, et al: Bronchiectasis in Alaska native children: Causes and clinical courses. Pediatr Pulmonol 29:182–187, 2000.
6. Kennedy TP, Weber DJ: Nontuberculous mycobacteria: An under-appreciated cause of geriatric lung disease. Am J Respir Crit Care Med 149:1654–1658, 1994.
7. Prince DS, Peterson DD, Steiner RM, et al: Infection with Myco-bacterium avium complex in patients without predisposing conditions. N Engl J Med 321:863–868, 1989.
8. Iseman MD, Buschman DL, Ackerson LM: Pectus excavatum and scoliosis: Thoracic anomalies associated with pulmonary disease due to M. avium complex. Am Rev Respir Dis 144:914–916, 1991.

1044 ObstructiveDiseases
9. Wallace RJ Jr: Mycobacterium avium complex lung disease and women: Now an equal opportunity disease. Chest 105:6–7, 1994.
10. Westcott JL, Cole SR: Traction bronchiectasis in end-stage pulmo-nary fibrosis. Radiology 161:665–669, 1986.
11. Shum DKY, Chan SCH, Ip MSM: Neutrophil-mediated degradation of lung proteoglycans: Stimulation by tumor necrosis factor-alpha in sputum of patients with bronchiectasis. Am J Respir Crit Care Med 162:1925–1931, 2000.
12. Comroe JH Jr (ed): Special acts involving breathing. In Physiology of Respiration: An Introductory Text (2nd ed). Chicago: Year Book, 1974, pp 229–233.
13. Cole PJ: A new look at the pathogenesis, management of persist-ent bronchial sepsis: A “vicious circle” hypothesis and its logical therapeutic connotations. In Davies RJ (ed): Strategies for the Management of Chronic Bronchial Sepsis. Oxford: Medicine Pub-lishing Foundation, 1984, pp 1–20.
14. Gaga M, Bentley AM, Humbert M, et al: Increases in CD4 T lym-phocytes, macrophages, neutrophils and interleukin 8 positive cells in the airways of patients with bronchiectasis. Thorax 53:685–691, 1998.
15. Tager I, Speizer FE: Role of infection in chronic bronchitis. N Engl J Med 292:563–571, 1975.
16. Evans SA, Turner SM, Bosch BJ, et al: Lung function in bron-chiectasis: The influence of Pseudomonas aeruginosa. Eur Respir J 9:1001–1004, 1996.
17. Wilson CB, Jones PW, O’Leary CJ, et al: Effect of sputum bacte-riology on the quality of life of patients with bronchiectasis. Eur Respir J 10:1754–1760, 1997.
18. King PT, Holdsworth SR, Freezer NJ, et al: Microbiologic follow-up study in adult bronchiectasis. Respir Med 101:1633–1638, 2007.
19. Fowler SJ, French J, Screaton NJ, et al: Nontuberculous mycobac-teria in bronchiectasis: Prevalence and patient characteristics. Eur Respir J 28:1204–1210, 2006.
20. Kunst H, Wickremasinghe M, Wells A, Wilson R: Nontuberculous mycobacterial disease and Aspergillus-related lung disease in bronchiectasis. Eur Respir J 28:352–357, 2006.
21. Costerton JW: The etiology and persistence of cryptic bacterial infections: A hypothesis. Rev Infect Dis 6:S608–S616, 1984.
22. Singh PK, Schaefer AL, Parsek MR, et al: Quorum-sensing signals indicate that cystic fibrosis lungs are infected with bacterial bio-films. Nature 407:762–764, 2000.
23. Costerton JW, Stewart PS, Greenberg EP: Bacterial biofilms: A common cause of persistent infections. Science 284:1318–1320, 1999.
24. Stewart PS, Costerton JW: Antibiotic resistance of bacteria in biofilms. Lancet 358:135–138, 2001.
25. Ceri H, Olson ME, Stremick C, et al: The Calgary biofilm device: New technology for rapid determination of antibiotic suscepti-bilities of bacterial biofilms. J Clin Microbiol 37:1771–1776, 1999.
26. National Institutes of Health Consensus Development Confer-ence: Genetic testing for cystic fibrosis. Arch Intern Med 159: 1529–1539, 1999.
27. Boyle MP: Adult cystic fibrosis. JAMA 298:1787–1793, 2007.28. DeGroote MA, Huitt G, Fulton K, et al: Retrospective analysis of
aspiration risk and genetic predisposition in bronchiectasis patients with and without non-tuberculous mycobacteria infec-tion. Am J Respir Crit Care Med 163:A763, 2001.
29. Ziedalski TM, Kao PN, Henig NR, et al: Prospective analysis of cystic fibrosis transmembrane regulator mutations in adults with bronchiectasis or pulmonary nontuberculous mycobacterial infection. Chest 130:995–1002, 2006.
30. Kim RD, Greenberg DE, Ehrmantraut ME, et al: Pulmonary non-tuberculous mycobacterial disease: Prospective study of a distinct preexisting syndrome. Am J Respir Crit Care Med 178:1066–1074, 2008.
31. Groman JD, Meyer ME, Wilmott RW, et al: Variant of cystic fibro-sis phenotypes in the absence of CFTR mutations. N Engl J Med 347:401–407, 2002.
32. Kerem E, Corey M, Kerem BS, et al: The relation between genotype and phenotype in cystic fibrosis—Analysis of the most common mutation (delta F508). N Engl J Med 323:1517–1522, 1990.
33. Gilljam M, Moltyaner Y, Downey GP: Airway inflammation and infection in congenital bilateral absence of the vas deferens. Am J Respir Crit Care Med 169:174–179, 2004.
34. Accurso FJ, Sontag MK: Seeking modifier genes in cystic fibrosis. Am J Respir Crit Care Med 167:289–293, 2003.
35. Cunningham-Rundles C, Bodian C: Common variable immunode-ficiency: Clinical and immunological features of 248 patients. Clin Immunol 92:34–48, 1999.
36. Hill SL, Mitchell JL, Burnett D, et al: IgG subclasses in the serum and sputum from patients with bronchiectasis. Thorax 53:463–468, 1998.
37. Chipps BE, Talamo RC, Winkelstein JA: IgA deficiency, recurrent pneumonias, and bronchiectasis: Clinical conference in pulmo-nary disease from the Department of Pediatrics, the Johns Hopkins University School of Medicine. Chest 73:519–526, 1978.
38. Freeman AF, Holland SM: The hyper-IgE syndromes. Immunol Allergy Clin North Am 28:277–291, 2008.
39. Holland SM, DeLeo FR, Elloumi HZ, et al: STAT3 mutations in the hyper-IgE syndrome. N Engl J Med 357:1608–1619, 2007.
40. Chan ED, Feldman NE, Chmura K: Do mutations of the alpha-1-antitrypsin gene predispose to non-tuberculous mycobacterial infection? Am J Respir Crit Care Med 169:A132, 2004.
41. Shin MS, Ho K-J: Bronchiectasis in patients with alpha-1- antitrypsin deficiency: A rare occurrence? Chest 104:1384–1386, 1993.
42. Tomashefski JF Jr, Crystal RG, Wiedemann HP, et al and the Alpha 1-Antitrypsin Deficiency Registry Study Group: The bronchopul-monary pathology of alpha-1 antitrypsin (AAT) deficiency: Find-ings of the death review committee of the national registry for individuals with severe deficiency of alpha-1 antitrypsin. Hum Pathol 35:1452–1461, 2004.
43. Chan ED, Kaminska AM, Gill W, et al: Alpha-1-antitrypsin (AAT) anomalies are associated with lung disease due to rapidly growing mycobacteria and AAT inhibits Mycobacterium abscessus infec-tion of macrophages. Scand J Infect Dis 39:690–696, 2007.
44. De Serres FJ: Worldwide racial and ethnic distribution of alpha-1-antitrypsin deficiency: Summary of an analysis of published genetic epidemiologic surveys. Chest 122:1818–1829, 2002.
45. Dahl M, Tybjaerg-Hansen A, Lange P, et al: Change in lung func-tion and morbidity from chronic obstructive pulmonary disease in alpha-1-antitrypsin MZ heterozygotes: A longitudinal study of the general population. Ann Intern Med 136:270–279, 2002.
46. Lieberman J: Augmentation therapy reduces frequency of lung infections in antitrypsin deficiency: A new hypothesis with sup-porting data. Chest 118:1480–1485, 2000.
47. Mulgrew AT, Taggart CC, Lawless MW, et al: Z alpha1-antitrypsin polymerizes in the lung and acts as a neutrophil chemoattractant. Chest 125:1952–1957, 2004.
48. Cantin AM, Woods DE: Aerosolized prolastin suppresses bacterial proliferation in a model of chronic Pseudomonas aeruginosa lung infection. Am J Respir Crit Care Med 160:1130–1135, 1999.
49. Shapiro L, Pott GB, Ralston AH: Alpha-1-antitrypsin inhibits human immunodeficiency virus type 1. FASEB J 15:115–122, 2001.
50. Hayes VM, Gardiner-Garden M: Are polymorphic markers within the alpha-1-antitrypsin gene associated with risk of human immu-nodeficiency virus disease? J Infect Dis 188:1205–1208, 2003.
51. Cuvelier A, Muir J-F, Hellot M-F, et al: Distribution of alpha-1-an-titrypsin alleles in patients with bronchiectasis. Chest 117:415–419, 2000.
52. Parr DG, Guest PG, Reynolds JH, et al: Prevalence and impact of bronchiectasis in alpha1-antitrypsin deficiency. Am J Respir Crit Care Med 176:1215–1221, 2007.
52a. Amirav I, Cohen-Cymberknoh M, Shoseyov D, Kerem E. Primary ciliary dyskinesia: prospects for new therapies, building on the experience in cystic fibrosis. Paediatr Respir Rev 10:58–62, 2009.
52b. Leigh MW, Zariwala MA, Knowles MR. Primary ciliary dyski-nesia: improving the diagnostic approach. Curr Opin Pediatr 21:320–325, 2009.
53. Lillington GA: Dyskinetic cilia and Kartagener’s syndrome: Bron-chiectasis with a twist. Clin Rev Allergy Immunol 21:65–69, 2001.
54. Geremek M, Witt M: Primary ciliary dyskinesia: Genes, candidate genes and chromosomal regions. J Appl Genet 45:347–361, 2004.

42 brOnchiectasis 1045
82. Vitali C, Tavoni A, Viegi G, et al: Lung involvement in Sjögren’s syndrome: A comparison between patients with primary and with secondary syndrome. Ann Rheum Dis 44:455–461, 1985.
83. Camus P, Colby TV: The lung in inflammatory bowel disease. Eur Respir J 15:5–10, 2000.
84. Sharma S, Eschun G. What are the pulmonary manifestations of inflammatory bowel disease? J Respir Dis 28:227–234, 2007.
85. Tillie-Leblond I, Wallaert B, Leblond D, et al: Respiratory involve-ment in relapsing polychondritis: Clinical, functional, endo-scopic, and radiographic evaluations. Medicine (Baltimore) 77:168–176, 1998.
86. Tsang KW, Lam WK, Kwok E, et al: Helicobacter pylori and upper gastrointestinal symptoms in bronchiectasis. Eur Respir J 14:1345–1350, 1999.
87. De Groote MA, Huitt G, Fulton K, et al: Retrospective analysis of aspiration risk and genetic predisposition in bronchiectasis patients with and without non-tuberculous mycobacteria infec-tion. Am J Respir Crit Care Med 163:A763, 2003.
88. Harding SM: Recent clinical investigations examining the associa-tion of asthma and gastroesophageal reflux. Am J Med 115: 39S–44S, 2003.
89. Raghu G: The role of gastroesophageal reflux in idiopathic pul-monary fibrosis. Am J Med 115:60S–64S, 2003.
90. Zerbib F, Guisset O, Lamouliatte H, et al: Effects of bronchial obstruction on lower esophageal sphincter motility and gastro-esophageal reflux in patients with asthma. Am J Respir Crit Care Med 166:1206–1211, 2002.
91. Lagergren J, Bergstrom R, Adami H-O, et al: Association between medications that relax the lower esophageal sphincter and risk for esophageal adenocarcinoma. Ann Intern Med 133:165–175, 2000.
92. Halsey KD, Wald A, Meyer KC, et al: Non-acidic supraesophageal reflux associated with diffuse alveolar damage and allograft dys-function after lung transplantation: A case report. J Heart Lung Transplant 27:564–567, 2008.
93. McGuinness G, Naidich DP, Garay SM, et al: AIDS associated bronchiectasis: CT features. J Comput Assist Tomogr 17:260–266, 1993.
94. Verghese A, al-Samman M, Nabhan D, et al: Bacterial bronchitis and bronchiectasis in human immunodeficiency virus infection. Arch Intern Med 154:2086–2091, 1994.
95. Lee WL, Downey GP: Leukocyte elastase: Physiological functions and role in acute lung injury. Am J Respir Crit Care Med 164:896–904, 2001.
96. Meyer KC, Nunley DR, Dauber JH, et al: Neutrophils, unopposed neutrophil elastase, and alpha-1-antiprotease defenses following human lung transplantation. Am J Respir Crit Care Med 164:97–102, 2001.
97. Diaz PT, King MA, Pacht ER, et al: Increased susceptibility to pulmonary emphysema among HIV-seropositive smokers. Ann Intern Med 132:369–372, 2000.
98. Bard M, Couderc L-J, Saimot AG, et al: Accelerated obstructive pulmonary disease in HIV infected patients with bronchiectasis. Eur Respir J 11:771–775, 1998.
99. Cordasco E: Clinical features of the yellow nail syndrome. Cleve Clin J Med 57:472–476, 1990.
100. Brofman JD, Hall JB, Scott W, et al: Yellow nails, lymphedema and pleural effusion: Treatment of chronic pleural effusion with pleuroperitoneal shunting. Chest 97:743–745, 1990.
101. Varney VA, Cumberworth V, Sudderick R, et al: Rhinitis, sinusitis and the yellow nail syndrome: A review of symptoms and response to treatment in 17 patients. Clin Otolaryngol 19:237–240, 1994.
102. Corless JA, Warburton CJ: Leukotriene receptor antagonists for non-cystic fibrosis bronchiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
103. Lasserson T, Holt K, Evans DJ, et al: Anticholinergic therapy for bronchiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
104. Crockett AJ, Cranston JM, Latimer KM, et al: Mucolytics for bron-chiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
105. Corless JA, Warburton CJ: Surgery vs. non-surgical treatment for bronchiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
55. Noone PG, Bali D, Carson JL, et al: Discordant organ laterality in monozygotic twins with primary ciliary dyskinesia. Am J Med 82:155–160, 1999.
56. Noone PG, Leigh MW, Annuti A: Primary ciliary dyskinesia: Diagnostic and phenotypic features. Am J Respir Crit Care Med 169:459–467, 2004.
57. Escudier E, Couprie M, Duriez B, et al: Computer-assisted analysis helps detect inner dynein arm abnormalities. Am J Respir Crit Care Med 166:1257–1262, 2002.
58. Woodring JH, Howard RSI, Rehm SR: Congenital tracheobron-chomegaly (Mounier-Kuhn syndrome): A report of 10 cases and review of the literature. J Thorac Imaging 6:1–10, 1991.
59. Abdallah EG, Ashton RW: Mounier-Kuhn syndrome: Overcoming a lack of recognition. South Med J 101:14–15, 2008.
60. Jones VF, Eid NS, Franco SM, et al: Familial congenital bronchiectasis: Williams-Campbell syndrome. Pediatr Pulmonol 16:263–267, 1993.
61. George J, Jain R, Tariq SM: CT bronchoscopy in the diagnosis of Williams-Campbell syndrome. Respirology 11:117–119, 2006.
62. Palmer SM Jr, Layish DT, Kussin PS, et al: Lung transplantation for Williams-Campbell syndrome. Chest 113:534–537, 1998.
63. Foster ME, Foster DR: Bronchiectasis and Marfan’s syndrome. Postgrad Med J 56:718–719, 1980.
64. Wood JR, Bellamy D, Child AH, et al: Pulmonary disease in patients with Marfan syndrome. Thorax 39:780–784, 1984.
65. Ordway D, Henao-Tamayo M, Smith E, et al: Animal model of Mycobacterium abscessus lung infection. J Leukoc Biol 83:1502–1511, 2008.
66. Reich JM, Johnson NR: Mycobacterium avium complex pulmonary disease presenting as isolated lingular or middle lobe pattern: The Lady Windermere syndrome. Chest 101:1605–1609, 1992.
67. Iseman MD: That’s no lady (letter). Chest 109:1411, 1996.68. Iseman MD: That’s no lady, revisited (letter). Chest 111:255,
1997.69. Tsuyuguchi K, Suzuki K, Matsumoto H, et al: Effect of oestrogen
on Mycobacterium avium complex pulmonary infection in mice. Clin Exp Immunol 123:428–434, 2001.
70. Olsson T, Bjornstad-Pettersen H, Stjernberg N: Bronchostenosis due to sarcoidosis: A cause of atelectasis and airway obstruction simulating pulmonary neoplasm and chronic obstructive pulmo-nary disease. Chest 75:663–666, 1979.
71. Walker WC: Pulmonary infections and rheumatoid arthritis. Q J Med 142:239–250, 1967.
72. Solanki T, Neville E: Bronchiectasis and rheumatoid disease: Is there an association? Br J Rheumatol 31:691–693, 1992.
73. Perez T, Remy-Jardin M, Cortet B: Airways involvement in rheumatoid arthritis. Am J Respir Crit Care Med 157:1658–1665, 1998.
74. Remy-Jardin M, Remy J, Cortet B, et al: Lung changes in rheuma-toid arthritis. Radiology 193:375–382, 1994.
75. Swinson DR, Symmons D, Suresh U, et al: Decreased survival in patients with co-existent rheumatoid arthritis and bronchiectasis. Br J Rheumatol 36:689–691, 1997.
76. Rosenow CE, Strimlan CV, Muhm JR, et al: Pleuropulmonary manifestations of ankylosing spondylitis. Mayo Clin Proc 52:641–649, 1977.
77. Casserly IP, Fenlon HM, Breatnach E, et al: Lung findings on high-resolution computed tomography in idiopathic ankylosing spondylitis: Correlation with clinical findings, pulmonary func-tion testing and plain radiography. Br J Rheumatol 36:677–682, 1997.
78. Davidson PT, Khankjo V, Goble M, et al: Treatment of disease due to Mycobacterium intracellulare. Rev Infect Dis 3:1052–1059, 1981.
79. Fenlon HM, Doran M, Sant SM, et al: High-resolution chest CT in systemic lupus erythematosus. AJR Am J Roentgenol 166:301–307, 1996.
80. Constantopoulos SH, Padadimitriou CS, Moutsopoulos HM: Res-piratory manifestations in primary Sjögren’s syndrome: A clinical, functional, and histologic study. Chest 88:226–229, 1985.
81. Robinson DA, Meyer CF: Primary Sjögren’s syndrome associated with recurrent sinopulmonary infections and bronchiectasis. J Allergy Clin Immunol 94:263–264, 1994.
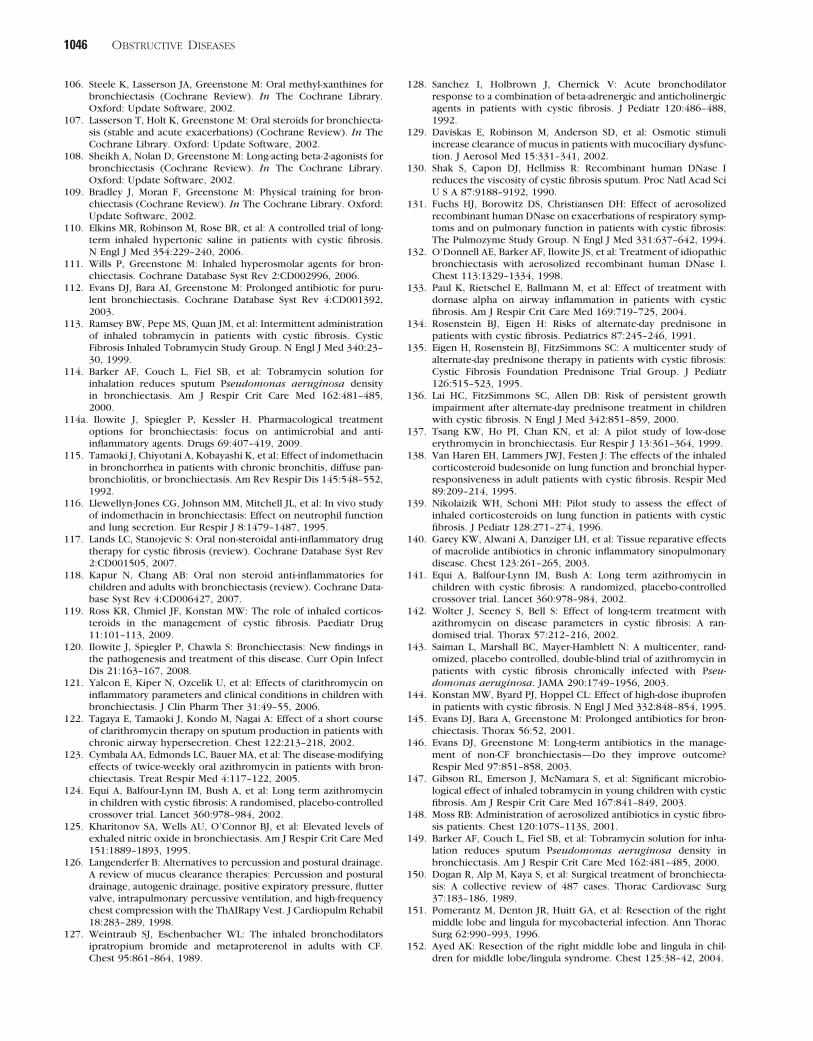
1046 ObstructiveDiseases
128. Sanchez I, Holbrown J, Chernick V: Acute bronchodilator response to a combination of beta-adrenergic and anticholinergic agents in patients with cystic fibrosis. J Pediatr 120:486–488, 1992.
129. Daviskas E, Robinson M, Anderson SD, et al: Osmotic stimuli increase clearance of mucus in patients with mucociliary dysfunc-tion. J Aerosol Med 15:331–341, 2002.
130. Shak S, Capon DJ, Hellmiss R: Recombinant human DNase I reduces the viscosity of cystic fibrosis sputum. Proc Natl Acad Sci U S A 87:9188–9192, 1990.
131. Fuchs HJ, Borowitz DS, Christiansen DH: Effect of aerosolized recombinant human DNase on exacerbations of respiratory symp-toms and on pulmonary function in patients with cystic fibrosis: The Pulmozyme Study Group. N Engl J Med 331:637–642, 1994.
132. O’Donnell AE, Barker AF, Ilowite JS, et al: Treatment of idiopathic bronchiectasis with aerosolized recombinant human DNase I. Chest 113:1329–1334, 1998.
133. Paul K, Rietschel E, Ballmann M, et al: Effect of treatment with dornase alpha on airway inflammation in patients with cystic fibrosis. Am J Respir Crit Care Med 169:719–725, 2004.
134. Rosenstein BJ, Eigen H: Risks of alternate-day prednisone in patients with cystic fibrosis. Pediatrics 87:245–246, 1991.
135. Eigen H, Rosenstein BJ, FitzSimmons SC: A multicenter study of alternate-day prednisone therapy in patients with cystic fibrosis: Cystic Fibrosis Foundation Prednisone Trial Group. J Pediatr 126:515–523, 1995.
136. Lai HC, FitzSimmons SC, Allen DB: Risk of persistent growth impairment after alternate-day prednisone treatment in children with cystic fibrosis. N Engl J Med 342:851–859, 2000.
137. Tsang KW, Ho PI, Chan KN, et al: A pilot study of low-dose erythromycin in bronchiectasis. Eur Respir J 13:361–364, 1999.
138. Van Haren EH, Lammers JWJ, Festen J: The effects of the inhaled corticosteroid budesonide on lung function and bronchial hyper-responsiveness in adult patients with cystic fibrosis. Respir Med 89:209–214, 1995.
139. Nikolaizik WH, Schoni MH: Pilot study to assess the effect of inhaled corticosteroids on lung function in patients with cystic fibrosis. J Pediatr 128:271–274, 1996.
140. Garey KW, Alwani A, Danziger LH, et al: Tissue reparative effects of macrolide antibiotics in chronic inflammatory sinopulmonary disease. Chest 123:261–265, 2003.
141. Equi A, Balfour-Lynn IM, Bush A: Long term azithromycin in children with cystic fibrosis: A randomized, placebo-controlled crossover trial. Lancet 360:978–984, 2002.
142. Wolter J, Seeney S, Bell S: Effect of long-term treatment with azithromycin on disease parameters in cystic fibrosis: A ran-domised trial. Thorax 57:212–216, 2002.
143. Saiman L, Marshall BC, Mayer-Hamblett N: A multicenter, rand-omized, placebo controlled, double-blind trial of azithromycin in patients with cystic fibrosis chronically infected with Pseu-domonas aeruginosa. JAMA 290:1749–1956, 2003.
144. Konstan MW, Byard PJ, Hoppel CL: Effect of high-dose ibuprofen in patients with cystic fibrosis. N Engl J Med 332:848–854, 1995.
145. Evans DJ, Bara A, Greenstone M: Prolonged antibiotics for bron-chiectasis. Thorax 56:52, 2001.
146. Evans DJ, Greenstone M: Long-term antibiotics in the manage-ment of non-CF bronchiectasis—Do they improve outcome? Respir Med 97:851–858, 2003.
147. Gibson RL, Emerson J, McNamara S, et al: Significant microbio-logical effect of inhaled tobramycin in young children with cystic fibrosis. Am J Respir Crit Care Med 167:841–849, 2003.
148. Moss RB: Administration of aerosolized antibiotics in cystic fibro-sis patients. Chest 120:107S–113S, 2001.
149. Barker AF, Couch L, Fiel SB, et al: Tobramycin solution for inha-lation reduces sputum Pseudomonas aeruginosa density in bronchiectasis. Am J Respir Crit Care Med 162:481–485, 2000.
150. Dogan R, Alp M, Kaya S, et al: Surgical treatment of bronchiecta-sis: A collective review of 487 cases. Thorac Cardiovasc Surg 37:183–186, 1989.
151. Pomerantz M, Denton JR, Huitt GA, et al: Resection of the right middle lobe and lingula for mycobacterial infection. Ann Thorac Surg 62:990–993, 1996.
152. Ayed AK: Resection of the right middle lobe and lingula in chil-dren for middle lobe/lingula syndrome. Chest 125:38–42, 2004.
106. Steele K, Lasserson JA, Greenstone M: Oral methyl-xanthines for bronchiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
107. Lasserson T, Holt K, Greenstone M: Oral steroids for bronchiecta-sis (stable and acute exacerbations) (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
108. Sheikh A, Nolan D, Greenstone M: Long-acting beta-2-agonists for bronchiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
109. Bradley J, Moran F, Greenstone M: Physical training for bron-chiectasis (Cochrane Review). In The Cochrane Library. Oxford: Update Software, 2002.
110. Elkins MR, Robinson M, Rose BR, et al: A controlled trial of long-term inhaled hypertonic saline in patients with cystic fibrosis. N Engl J Med 354:229–240, 2006.
111. Wills P, Greenstone M: Inhaled hyperosmolar agents for bron-chiectasis. Cochrane Database Syst Rev 2:CD002996, 2006.
112. Evans DJ, Bara AI, Greenstone M: Prolonged antibiotic for puru-lent bronchiectasis. Cochrane Database Syst Rev 4:CD001392, 2003.
113. Ramsey BW, Pepe MS, Quan JM, et al: Intermittent administration of inhaled tobramycin in patients with cystic fibrosis. Cystic Fibrosis Inhaled Tobramycin Study Group. N Engl J Med 340:23–30, 1999.
114. Barker AF, Couch L, Fiel SB, et al: Tobramycin solution for inhalation reduces sputum Pseudomonas aeruginosa density in bronchiectasis. Am J Respir Crit Care Med 162:481–485, 2000.
114a. Ilowite J, Spiegler P, Kessler H. Pharmacological treatment options for bronchiectasis: focus on antimicrobial and anti- inflammatory agents. Drugs 69:407–419, 2009.
115. Tamaoki J, Chiyotani A, Kobayashi K, et al: Effect of indomethacin in bronchorrhea in patients with chronic bronchitis, diffuse pan-bronchiolitis, or bronchiectasis. Am Rev Respir Dis 145:548–552, 1992.
116. Llewellyn-Jones CG, Johnson MM, Mitchell JL, et al: In vivo study of indomethacin in bronchiectasis: Effect on neutrophil function and lung secretion. Eur Respir J 8:1479–1487, 1995.
117. Lands LC, Stanojevic S: Oral non-steroidal anti-inflammatory drug therapy for cystic fibrosis (review). Cochrane Database Syst Rev 2:CD001505, 2007.
118. Kapur N, Chang AB: Oral non steroid anti-inflammatories for children and adults with bronchiectasis (review). Cochrane Data-base Syst Rev 4:CD006427, 2007.
119. Ross KR, Chmiel JF, Konstan MW: The role of inhaled corticos-teroids in the management of cystic fibrosis. Paediatr Drug 11:101–113, 2009.
120. Ilowite J, Spiegler P, Chawla S: Bronchiectasis: New findings in the pathogenesis and treatment of this disease. Curr Opin Infect Dis 21:163–167, 2008.
121. Yalcon E, Kiper N, Ozcelik U, et al: Effects of clarithromycin on inflammatory parameters and clinical conditions in children with bronchiectasis. J Clin Pharm Ther 31:49–55, 2006.
122. Tagaya E, Tamaoki J, Kondo M, Nagai A: Effect of a short course of clarithromycin therapy on sputum production in patients with chronic airway hypersecretion. Chest 122:213–218, 2002.
123. Cymbala AA, Edmonds LC, Bauer MA, et al: The disease-modifying effects of twice-weekly oral azithromycin in patients with bron-chiectasis. Treat Respir Med 4:117–122, 2005.
124. Equi A, Balfour-Lynn IM, Bush A, et al: Long term azithromycin in children with cystic fibrosis: A randomised, placebo-controlled crossover trial. Lancet 360:978–984, 2002.
125. Kharitonov SA, Wells AU, O’Connor BJ, et al: Elevated levels of exhaled nitric oxide in bronchiectasis. Am J Respir Crit Care Med 151:1889–1893, 1995.
126. Langenderfer B: Alternatives to percussion and postural drainage. A review of mucus clearance therapies: Percussion and postural drainage, autogenic drainage, positive expiratory pressure, flutter valve, intrapulmonary percussive ventilation, and high-frequency chest compression with the ThAIRapy Vest. J Cardiopulm Rehabil 18:283–289, 1998.
127. Weintraub SJ, Eschenbacher WL: The inhaled bronchodilators ipratropium bromide and metaproterenol in adults with CF. Chest 95:861–864, 1989.


















