
Brentuximab Vedotin. How and When Should it be Used in B and T cell Lymphomas
48
Brentuximab Vedotin. How and When Should it be Used in B and T cell Lymphomas Ranjana Advani MD Professor of Medicine Saul Rosenberg Professor of Lymphoma Stanford University Lymphoma and Myeloma 2014 International Congress on Hematologic Malignancies New York
-
Upload
jared-haynes -
Category
Documents
-
view
21 -
download
3
description
Lymphoma and Myeloma 2014 International Congress on Hematologic Malignancies New York. Brentuximab Vedotin. How and When Should it be Used in B and T cell Lymphomas. Ranjana Advani MD Professor of Medicine Saul Rosenberg Professor of Lymphoma Stanford University. Disclosures. - PowerPoint PPT Presentation
Transcript of Brentuximab Vedotin. How and When Should it be Used in B and T cell Lymphomas
Brentuximab Vedotin.How and When Should it be Used in B and T
cell Lymphomas
Ranjana Advani MDProfessor of Medicine
Saul Rosenberg Professor of LymphomaStanford University
Lymphoma and Myeloma 2014International Congress on Hematologic Malignancies
New York
Disclosures
• Seattle Genetics: Research Funding
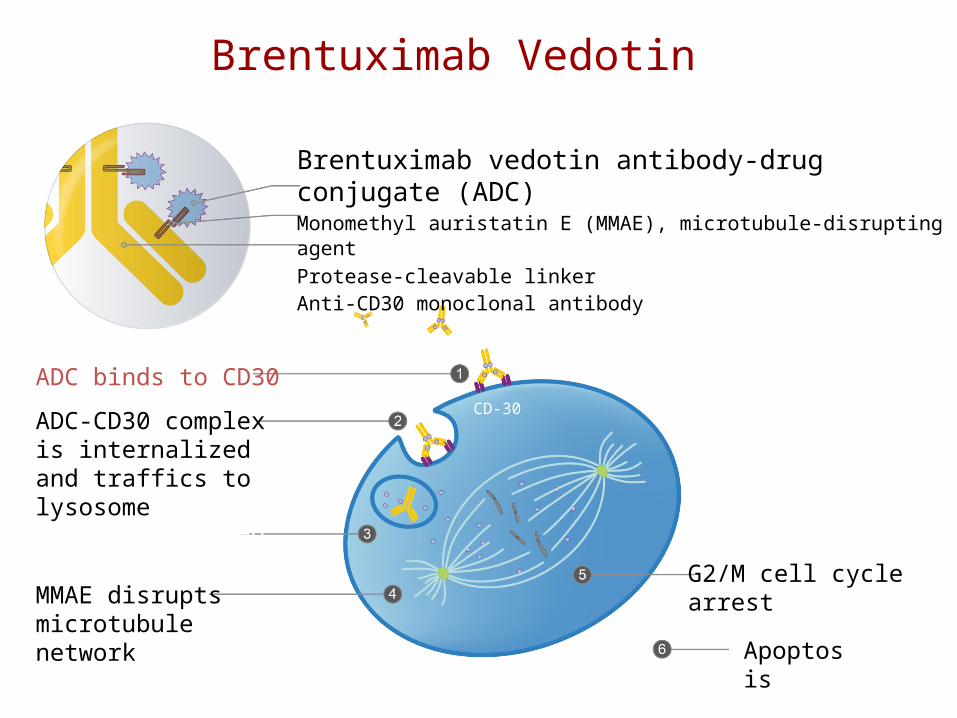
Brentuximab vedotin antibody-drug conjugate (ADC)Monomethyl auristatin E (MMAE), microtubule-disrupting agentProtease-cleavable linker Anti-CD30 monoclonal antibody
ADC binds to CD30
MMAE disruptsmicrotubule network
ADC-CD30 complex is internalized and traffics to lysosome
MMAE is released
Apoptosis
G2/M cell cycle arrest
Brentuximab Vedotin
CD-30

Brentuximab Vedotin Approved Indications
• Treatment of patients with Hodgkin Lymphoma (HL) after failure of autologous stem cell transplant (ASCT) or after failure of at least two prior multi-agent chemotherapy regimens in patients who are not ASCT candidates
• Treatment of patients with systemic Anaplastic Large Cell Lymphoma (ALCL) after failure of at least one prior multi-agent chemotherapy regimen

Outline• Past
– Key data of two pivotal trials which led to approval• Present
– Emerging data of subset experiences from phase 1 and pivotal trials
– Phase 2 trials in other CD 30 + PTCL and DLBCL setting• Future
– Combination with standard chemotherapy to improve cure in front line in HL and CD30 pos PTCL
B cell Lymphoma: Hodgkin Lymphoma and other B NHLT cell lymphoma: PTCL
PastKey data of two pivotal trials which led to approval

Phase II Pivotal trial in relapsed HL All ASCT failures
Toxicity > Gr 3: ANC 20% , sensory neuropathy 8% thrombocytopenia 6%
Individual Patients (n=98)*
Tum
or S
ize (%
Cha
nge
from
Bas
elin
e)
94% (96 of 102) of patients achieved tumor reduction
Younes et al JCO 2012
Med age 31 y, 71% refractory to front line, 66% prior RT
ORR 75% (32% CR)

Phase 2 Relapsed or Refractory HL Pivotal Trial Outcomes According to Best Response
Younes et al JCO 2012
Progression Free Survival Overall Survival

Phase 2 Relapsed or Refractory HL Pivotal Trial PFS in Patients with CR by Subsequent Transplant
Patients Who Achieved a CR N EventsMedian PFS
(95% CI)
Median Number of
Cycles Received
Allogeneic transplant 5 1 21.1 (,) 14
No transplant 30 13 21.7 (9.7, ) 13
• Subsequent transplant did not appear to meaningfully impact PFS in this small dataset
Younes et al JCO 2012

Relapsed or Refractory Systemic ALCL Trial Maximum Tumor Reduction
Pro B, et al. JCO 2012
97% of patients achieved tumor reduction
ORR 86% (57% CR)
72% ALK neg, 62% refractory to front line rx, 22 % prim refr, 26 % prior SCT


Outcomes according to response and ALK status
Pro B, et al. JCO 2012

Summary of “Past”
• High response rate in HL relapsed after ASCT• High response rate in R/R ALCL• More CRs in ALCL• In pts with a CR durable responses• Neuropathy

Present
• Retreatment strategy• Response in chemo refractory transplant naive pts • Can pts get an allogenic consolidation after
responding to brentuximab • Response in pts relapsing after an allogenic
transplant• Experience in elderly pts• Experience in other CD 30 + PTCL• Experience in CD 30+ DLBCL

Retreatment with Brentuximab Vedotin
Bartlett, et al. J Hematol Oncol 2014.
N = 21 (HL), 8 (ALCL), 48% grade 3 neuropathy manageable with dose delay/reduction
ORR 68%, CR: 39%

Retreatment with Brentuximab Vedotin Median DOR 9.5 months
Bartlett, et al. J Hematol Oncol 2014.
CR patients: 45% > 1yr duration
Overall SurvivalProgression Free Survival
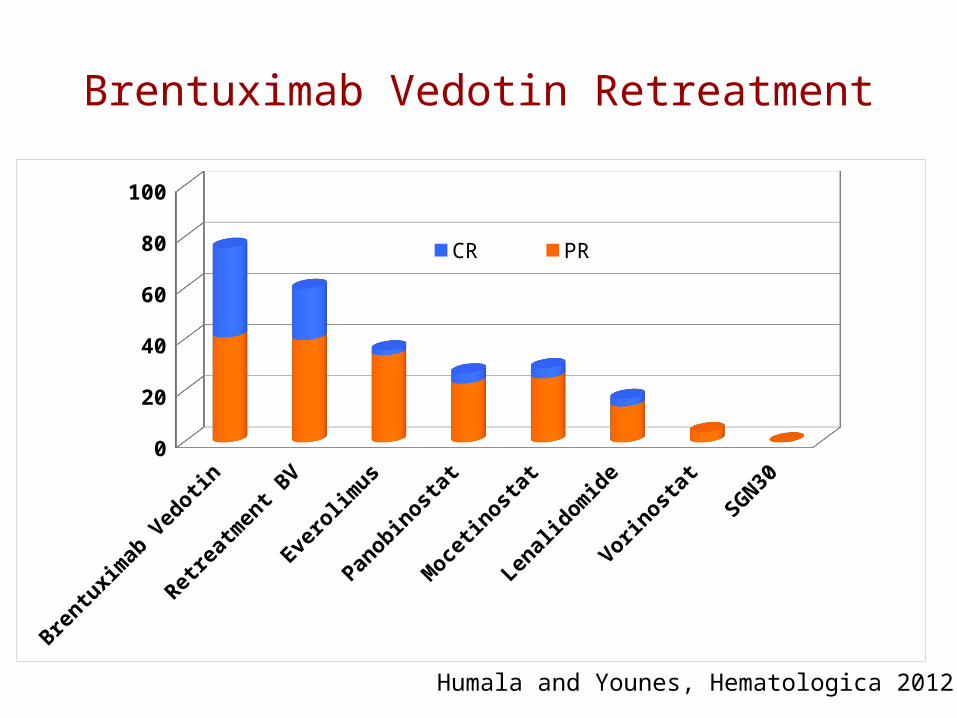
Brentuximab Vedotin Retreatment
Brentu
xim
ab V
edotin
Retre
atm
ent B
V
Evero
limus
Panobin
ostat
Moce
tinost
at
Lenal
idom
ide
Vorinost
at
SGN300
20
40
60
80
100
CR PR
Humala and Younes, Hematologica 2012

Response in Transplant Naïve pts with R/R HLAnalysis of 2 Phase 1 studies
Forero-Torres The Oncologist 2012
3/6 responders subsequent transplant
N=20, median 3 prior regimens, 45% prior RT

Consolidative Allogeneic Transplant Following Brentuximab Vedotin in Patients with R/R HL and
Systemic ALCL from two pivotal trials
Illidge et al Leuk Lymphoma 2014
Progression Free Survival Overall Survival
2 yr estimated 66% 2 yr estimated 80%

Brentuximab vedotin for HL recurring after allogeneic stem cell transplantation
.
Gopal A K et al. Blood 2012

Reduced Intensity Allogeneic Transplantation for HLPre and post brentuximab era
Chen, et al. Biol Blood Marrow Transplant. 2014
2y 59.3 % vs 26%
2y 56.5% vs 23.8%
2y 71 % vs 56.5%
1y 9.5 % vs 17.4%

Experience of Brentuximab Vedotin in pts > 60
Gopal, et al. Leukemia & Lymphoma 2014

Single Agent Brentuximab Vedotin Frontline Therapy for HL in pts > 60 y
• N=19• Antitumor activity: 89%
efficacy-evaluable patients achieved objective response– CR: 12 patients– PR: 5 patients– 2 patients had maximal
response of SD
• Tumor reduction achieved in 100% of patients
• Grade 3 neuropathy n=1
Yasenchak A, et al. ASH 2013. Abstract 4389.
100% of patients achieved tumor reduction
Individual Patients (n = 19)
100
50
0
-50
-100
Tum
or
Siz
e(B
est
% C
han
ge
Fro
m B
asel
ine)
CR CR CR CR
CR CRCR CR CR
CR CR CR
*
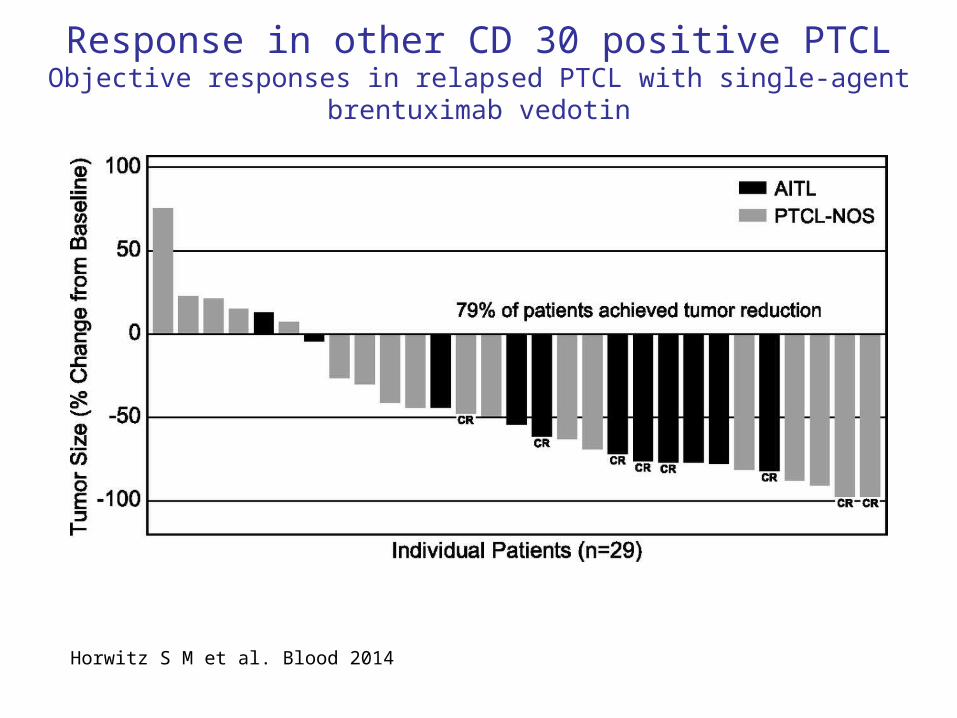
Response in other CD 30 positive PTCLObjective responses in relapsed PTCL with single-agent brentuximab vedotin
Horwitz S M et al. Blood 2014

Outcome by histology and CD30 expression
Horwitz S M et al. Blood 2014

B-Cell Lymphomas• Variable CD30 expression observed in
B-cell lymphomas
– ~14–25% of DLBCL express CD30a,b
– Potentially favorable prognostic factor and unique gene expression profile in newly diagnosed DLBCLa
• Relapsed or refractory DLBCL patients have a poor outcomec
• Autologous transplant of limited efficacy in rituximab era with 3-year EFS of 21%c
• No standard of care for transplant-ineligible patients
Overall survival in DLBCL patients failing second-line therapy
a Hu et al, Blood 121:2715-2724; 2013b Slack et al, ASH Annual Meeting Abstracts 120:1558; 2012c Gisselbrecht et al, J Clin Oncol 28:4184-4190; 2010
Median OS ≈ 4 months
Reprinted from Clin Lymph Myel Leuk, 10; 192, RL Elstrom, et al, (2010) with permission from Elsevier.

A Phase 2 Study of Brentuximab Vedotin in Patients with Relapsed or Refractory CD30-Positive B NHL
Eligibility Criteria
• Relapsed/refractory disease after ≥1 prior systemic therapy• CD30 expression by IHC using the anti-CD30 BerH2 antibody• Age ≥12 years• ECOG ≤2 or Lansky ≥50
Pretreatment Study Treatment
En
d o
f Tre
atm
ent Follow-up
21-Day CyclesBrentuximab vedotin
1.8 mg/kg IVRestage
Dosing on Day 1 (q3wk until disease progressionor unacceptable toxicity)
Screening/Enrollment28 Days
Every 3 months for first 2 years
After Cycles 2, 4, every 3 cycles thereafter, and at EOT

Pathological Diagnoses: N=68
TotalN (%)
DLBCL 50 (74)
DLBCL-NOS 43 (63)
EBV+ DLBCL of the elderly 5 (7)
Plasmablastic lymphoma 1 (1)
T-cell-rich B-cell lymphoma 1 (1)
Other B-cell lymphomas 18 (26)
Grey zone lymphoma 6 (9)
Primary mediastinal B-cell lymphoma (PMBL) 6 (9)
Follicular lymphoma 3 (4)
Post-transplant lymphoproliferative disorder (PTLD) 3 (4)
Bartlett NL, et al. ASH 2013, Abstract 848




Summary of “Present”• Responses seen at re-treatment• Responses seen in primary refractory transplant naïve
pts• Responses seen in pts who have failed allogenic
transplant• Allows for consolidative allogenic transplant• Well tolerated by elderly (> 60 yr) pts• Responses seen in AITL• Responses seen in DLBCL• Response does not correlate with CD30 expression

Brentuximab Vedotin in Malignant Lymphoma
Kumar et al Current Treatment Options in Oncology (2014)
Future
• Combination with standard chemotherapy to improve cure in front line in HL and CD30 positive PTCL

SGN-35 + chemotherapyPreclinical models
Oflazoglu et al BJH 2010

• Major Eligibility– Treatment-naive HL patients– Age ≥18 to 60 years– Stage IIAX or Stage IIb-IV disease
• Treatment Design– 28-day cycles (6 cycles) with dosing on Days 1 and 15
A(B)VD
Brentuximab Vedotin
Cycle 1 Cycle 2 Cycle 3
6 Cycles +/- XRT
Weeks0 2 4 6 8 10 12
Frontline Therapy with Brentuximab Vedotin Combined with ABVD or AVD in Pts with Newly Diagnosed Advanced Stage HL
BV: 1.2 mg/kg IV q 2 weeks
Younes, et al. Lancet Oncology 2013.

Preferred term, n (%)
ABVD with brentuximab vedotin
N=25
AVD with brentuximab vedotin
N=26Any event 11 (44) 0
Pulmonary toxicity 9 (36) 0
Interstitial lung disease 1 (4) 0
Pneumonitis 1 (4) 0
Pulmonary Toxicity
Events generally occurred during Cycles 34 Two patient deaths were associated with pulmonary
toxicity Events resolved in 9 of 11 patients (82%)
Median time to resolution was 2.6 weeks (range, 1.6 to 5 weeks)
8 of 11 patients with events discontinued bleomycin and were able to complete treatment with AVD combined with brentuximab vedotin
Younes, et al. Lancet Oncology 2013.

Outcomes
Younes, et al. Lancet Oncology 2013.

Fanale M A et al. JCO 2014
Brentuximab Vedotin Administered Concurrently or Sequentially with Multi-Agent Chemotherapy as Frontline Treatment of ALCL and other
CD30-Positive Mature T-Cell and NK-Cell Lymphomas

Demographics and Baseline Characteristics
ParameterTotalN=26
Age* , years 56 (21–82)Gender, n 11 M / 15 FIPI score 2, n (%) 17 (65)Stage III/IV disease, n (%) 18 (69)
Diagnosis sALCL, n (%) 19 (73) ALK – / +, n 16 / 3 Other CD30+ T- and NK-cell neoplasms, n (%) 7 (27) Peripheral T-cell lymphoma NOS, n 2 Angioimmunoblastic T-cell lymphoma, n 2 Adult T-cell leukemia/lymphoma, n 2 Enteropathy-associated T-cell lymphoma, n 1
* Median (range)
Fanale M A et al. JCO 2014

Response After Sequential or Combination Treatment
Fanale M A et al. JCO 2014

Outcomes
Combination TreatmentSequential Treatment
Fanale M A et al. JCO 2014

Adapted from Senter and Sievers: Nature Biotechnology 2012
5 years7 years

Major Progress2011-2014 (3 yrs)
• Phase 3 ATHERA trial: Randomized placebo-controlled, post-autologous stem cell transplant maintenance– Press Release 9/26/14 in favor of maintenance arm
• Phase 3 ECHELON-1 frontline Hodgkin lymphoma in combination with chemotherapy– ABVD vs AVD+BV
• Phase 3 ECHELON-2 frontline CD30-positive mature T-cell lymphomas in combination with chemotherapy– CHOP vs CHP+BV
• Phase 3 ALCANZA trial for relapsed CD30-positive cutaneous T-cell lymphoma

• First line salvage (pre ASCT)– Brentuximab Vedotin x 2 +/- ICE using a PET
adapted strategy – Bendamustine + Brentuximab Vedotin
Brentuximab Vedotin Ongoing trials in relapsed HL

Challenges• Need further understanding of mechanism of action
– Does activity correlate with target expression– Defining level of target expression which correlates with response
• Neuropathy is real– Education of physicians and pts imp so that timely dose adjustments can be
made• With the long PFS for patients achieving CR paradigms of care are
being challenged– Role of transplant
• How is BV best used– Front line
• Combination with other targeted agents?• Combination with chemotherapy?• Maintenance for pts with high risk disease?
– Relapse disease• Single agent vs. combination


















