Breast Abscess
13
Breast Abscess Kishore SR Oman Medical College
-
Upload
kishore-rajan -
Category
Health & Medicine
-
view
456 -
download
1
Transcript of Breast Abscess
Breast Abscess
Kishore SROman Medical College
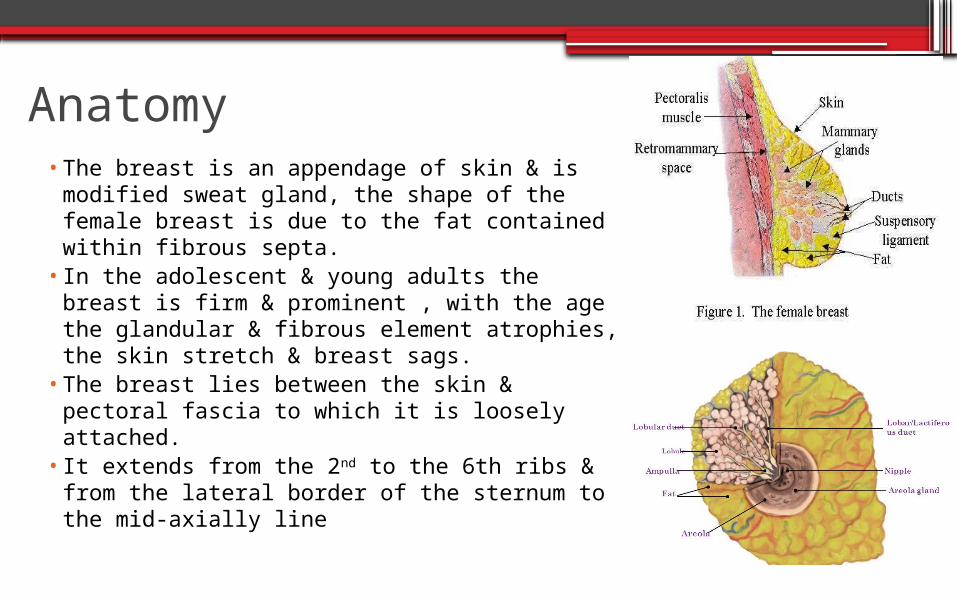
Anatomy •The breast is an appendage of skin & is
modified sweat gland, the shape of the female breast is due to the fat contained within fibrous septa.
• In the adolescent & young adults the breast is firm & prominent , with the age the glandular & fibrous element atrophies, the skin stretch & breast sags.
•The breast lies between the skin & pectoral fascia to which it is loosely attached.
• It extends from the 2nd to the 6th ribs & from the lateral border of the sternum to the mid-axially line
Classification of Breast Abscess
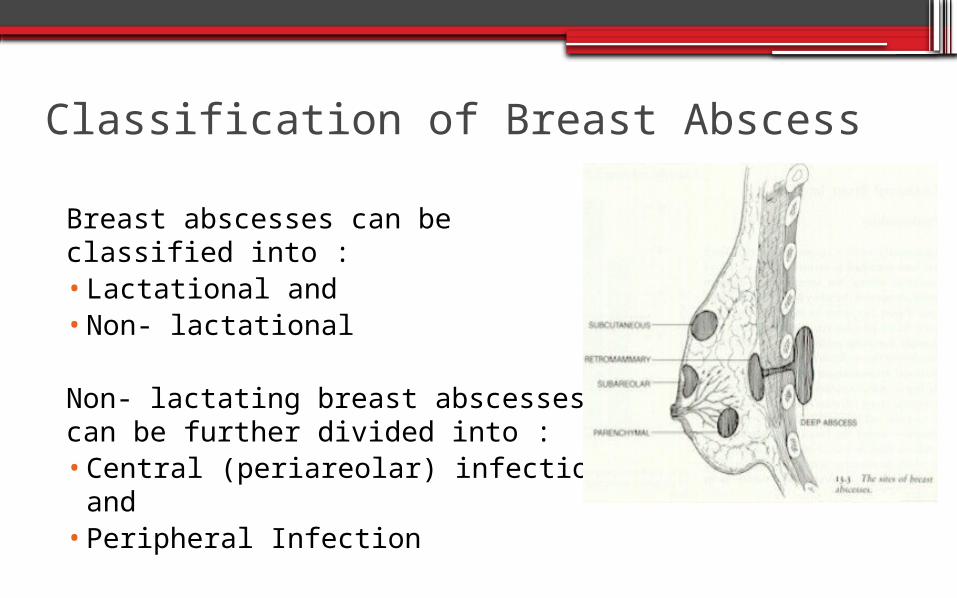
Breast abscesses can be classified into :•Lactational and•Non- lactational
Non- lactating breast abscesses can be further divided into :•Central (periareolar) infection and•Peripheral Infection
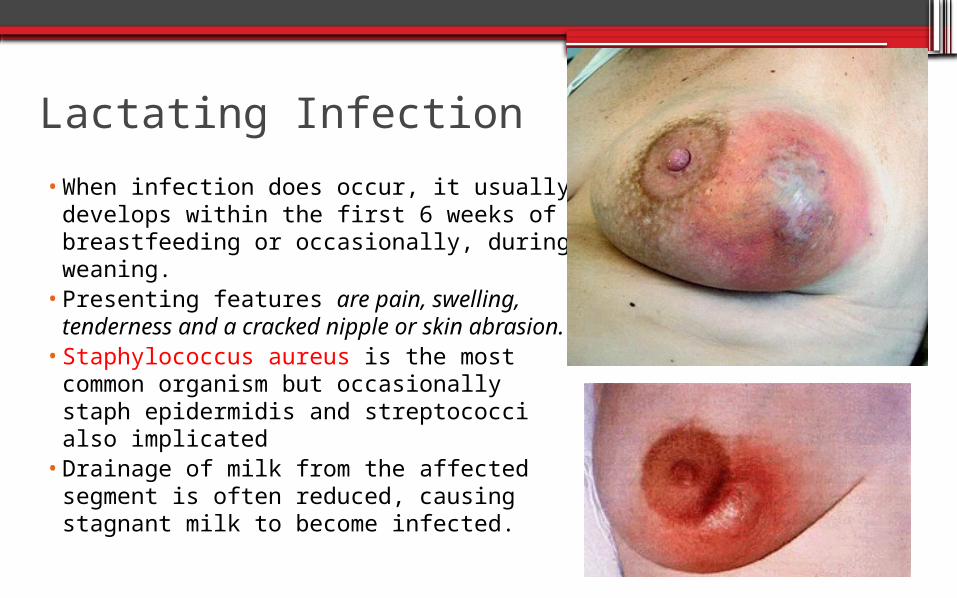
Lactating Infection•When infection does occur, it usually
develops within the first 6 weeks of breastfeeding or occasionally, during weaning.
•Presenting features are pain, swelling, tenderness and a cracked nipple or skin abrasion.
•Staphylococcus aureus is the most common organism but occasionally staph epidermidis and streptococci also implicated
•Drainage of milk from the affected segment is often reduced, causing stagnant milk to become infected.
Non-Lactating Infection
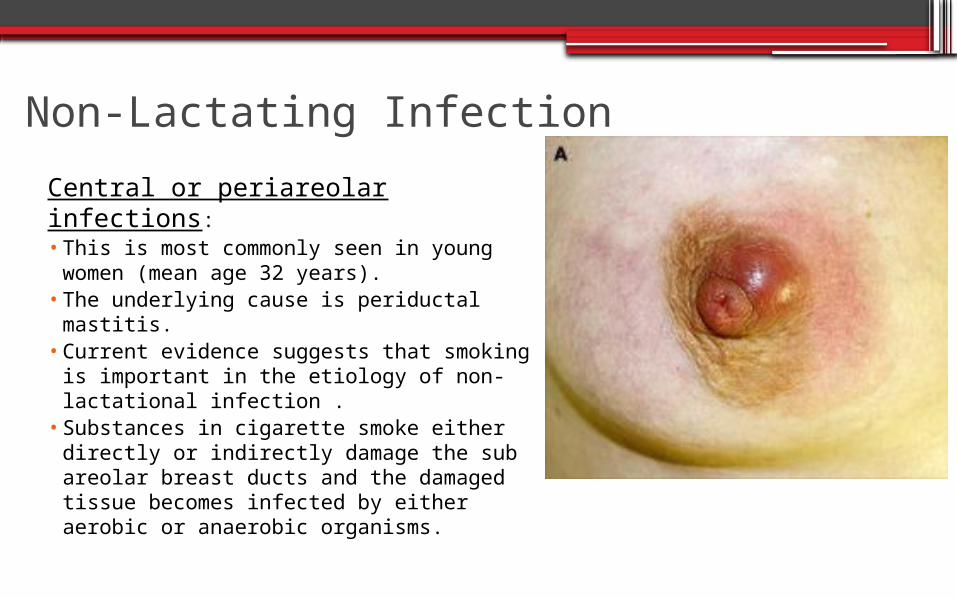
Central or periareolar infections:• This is most commonly seen in young
women (mean age 32 years). • The underlying cause is periductal mastitis. •Current evidence suggests that smoking is
important in the etiology of non-lactational infection .
•Substances in cigarette smoke either directly or indirectly damage the sub areolar breast ducts and the damaged tissue becomes infected by either aerobic or anaerobic organisms.
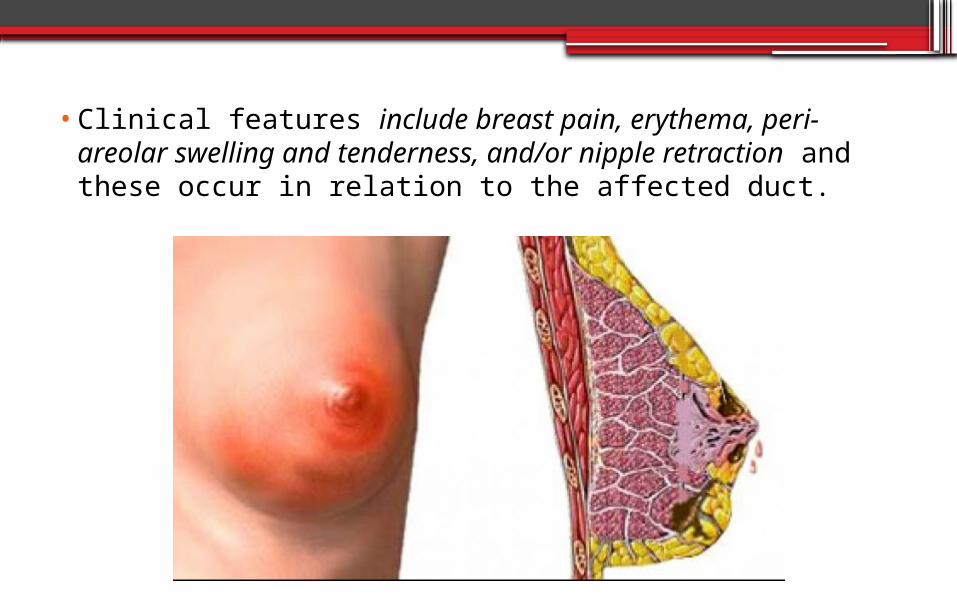
•Clinical features include breast pain, erythema, peri-areolar swelling and tenderness, and/or nipple retraction and these occur in relation to the affected duct.
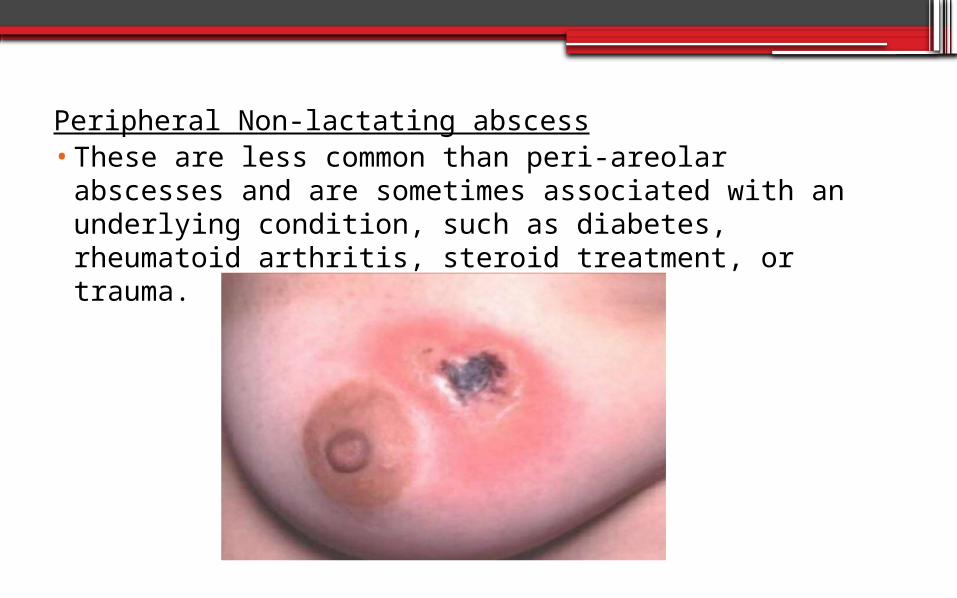
Peripheral Non-lactating abscess•These are less common than peri-areolar abscesses and
are sometimes associated with an underlying condition, such as diabetes, rheumatoid arthritis, steroid treatment, or trauma.
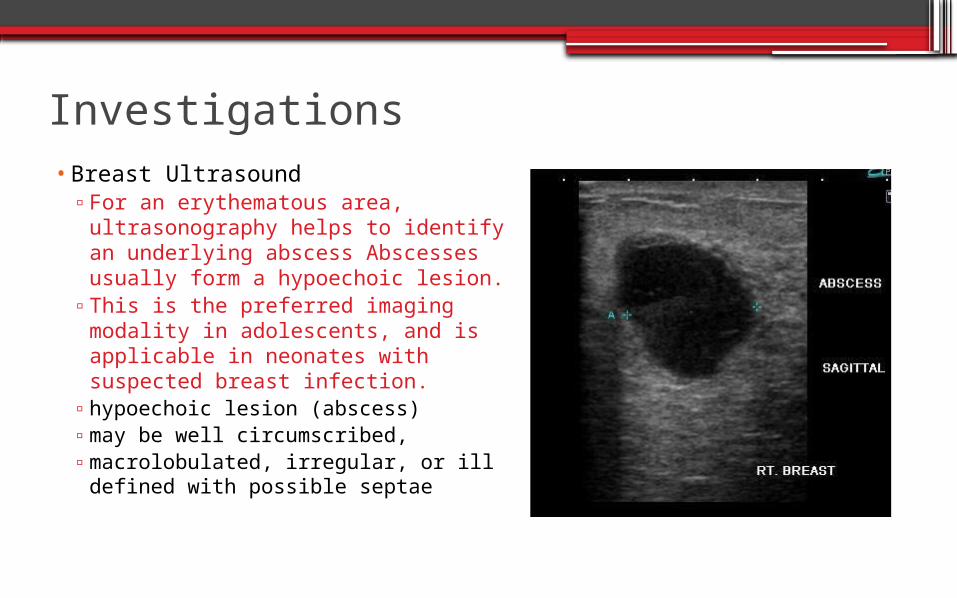
Investigations•Breast Ultrasound▫For an erythematous area,
ultrasonography helps to identify an underlying abscess Abscesses usually form a hypoechoic lesion.
▫This is the preferred imaging modality in adolescents, and is applicable in neonates with suspected breast infection.
▫hypoechoic lesion (abscess)▫may be well circumscribed,▫macrolobulated, irregular, or ill
defined with possible septae
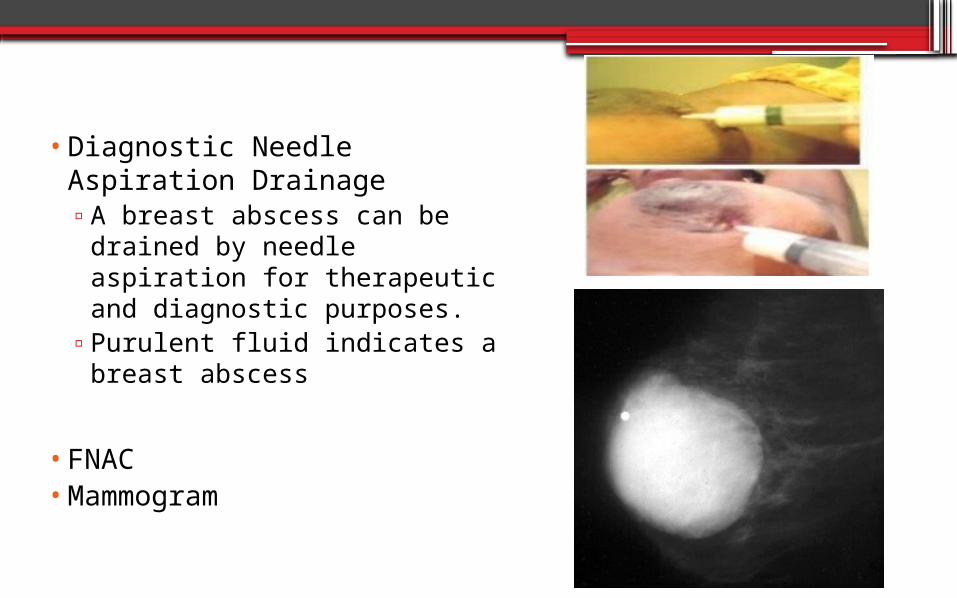
•Diagnostic Needle Aspiration Drainage▫A breast abscess can be drained
by needle aspiration for therapeutic and diagnostic purposes.
▫Purulent fluid indicates a breast abscess
•FNAC •Mammogram
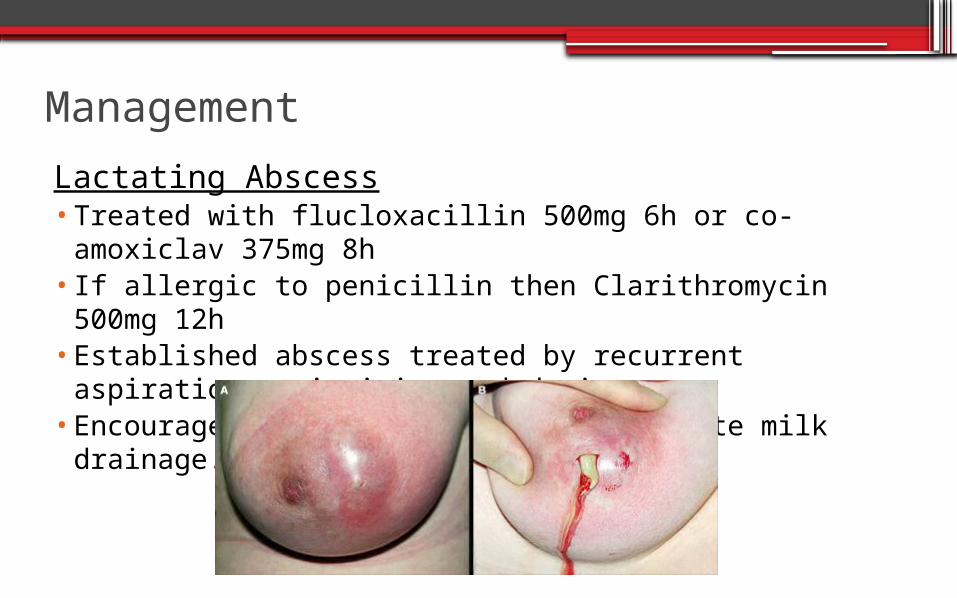
ManagementLactating Abscess•Treated with flucloxacillin 500mg 6h or co-amoxiclav
375mg 8h• If allergic to penicillin then Clarithromycin 500mg 12h•Established abscess treated by recurrent aspiration or
incision and drainage.•Encourage women to breastfeed to promote milk
drainage.
Non- Lactating abscess •Treatment is with appropriate antibiotics.•Co-amox 375mg 8h or combination of clarithromycin and
metronidazole•Abscess are aspirated or incised and drained.•Recurrent infection because the treatment does not
remove the damaged sub areolar duct which requires total duct excision
Prevention•Primary prevention•Good breastfeeding habits (e.g., emptying breasts fully and proper
latching) and proper nipple hygiene may help to minimize the risk of developing lactational mastitis. Sterile equipment and techniques should be used for nipple piercing.
•Secondary prevention•Breastfeeding should be encouraged if feasible during lactation.•Smoking cessation should also be encouraged, to minimize the risk
of recurrence. •Mastitis may increase the risk of transmission of HIV through
breastfeeding. Therefore, if an HIV-positive woman develops mastitis or an abscess, she should avoid breastfeeding from the affected side while the condition persists.

Thank You