BRAINSTEM AUDITORY EVOKED POTENTIAL RESPONSE
3
Indian J Phyoiol Pharmacol 1990; 34(4): 282-84 LEITER TO THE EDITOR BRAINSTEM AUDITORY EVOKED POTENTIAL RESPONSE IN PERNICIOUS ANAEMIA Sir, (Received on October 15, 1990) During our study of recording auditory evoked potentials in protein-calorie malnutrition in infants and young children (1), we came across a few cases of anaemia. The heamatological investigation- sincluding haemogram, showed that, of the five cases, two had megaloblastic anaemia, two had microcytic hypochromic and one had severe aplastic anaemia. Such neurological complications of various types of anaemias have not been documented except for pernicious anaemia, where classical sub- acuate combined degeneration of the spinal cord was first reported by Russell et al (2). Thereafter associated affection of the cerebral white matter and, more rarely, of the peripheral nerves have been amply documented. Direct relationship bet- ween optic nerve changes in the form of atrophy to the pernicious anaemia was documented by Cohen (3). However it is widely held that optic tract involvement in pernicious anaemia is rare (4-6). Patchy demyelination with affection of axis cylinders in the optic tracts has been reported in two cases of subacute combined degeneration (7). Identical changes have been found in experimental animals with induced B12 deficiency (8). Recently, Troncoso et al (9) have reported changes in visual evoked potentials in pernicious anaemia patients, suggestive of impairment of conduction in visual pathways. Now we repor: involvement of auditory pathways in our two permdous anaemia cases using. evoked potential recording procedure. However of the remaining three cases, two with microcytic hypochromic anaemia and one with severe aplastic anaemia, auditory brainstem evoked responses did not show any gross change and thus were normal. Standard evoked potential recording technique was employed using Ag/AgC1. disc electrodes anchored on scalp (CZ-A1 & A2 positions, 10-20 International System). Monaurally presented click stimuli, 2048 in number at 70 dBHL and 1O/sec were used to evoke brainstem auditory potential responses (BAEPs) as in our other studies (1,10,11). The two male children (GK 3.5 Yr, and RK 4 Yr) had typical megaloblastic bone marrow, showing hypercellular, megaloblastic change with dyserythropoiesis. The BAEP records of one of them are· shown in the figure, before and after therapy. It is clearly seen that before therapy BAEPs trace is of low amplitude, with indistinguish- able wave complexes II, III, IV; the peaks of waves I & V are also not very sharp. After treatment with vitamin B 12 injection and oral vitamin B Complex (Inj-Neurobin 1 ml bwx5 and Syrup vito B forte) for 30 days, the repeat BAEP record shows normal pattern with distinct waves I-V (even the late wave components VI & VII are also clearly visible) with much higher amplitude. The blood picture also improved with nearly normal looking bone marrow after 30 days of therapy. Besides absence of waves II, III, IV or their being inditinct, there is gross abnormality of reduction in amplitude of wave I & V (much so in Rt.side Fig. upper panel 2nd tracing). More than 50% reduction in amplitude reflects impairment in con- duction in the pathways (12). On vit. B complex therapy, there is dramatic increase in amplitude of these waves indicating better neural conduction in auditory pathways. This preliminary report suggests that there is impairment of conduction in brainstem auditory pathways in pernicious anaemia, and that conduction improves on therapy. This is in agreement with the observations of Troncoso et al (9) who found impairment of visual pathways in pernicious anaemia. Further studies using BAEP
Transcript of BRAINSTEM AUDITORY EVOKED POTENTIAL RESPONSE

Indian J Phyoiol Pharmacol 1990; 34(4): 282-84
LEITER TO THE EDITOR
BRAINSTEM AUDITORY EVOKED POTENTIAL RESPONSEIN PERNICIOUS ANAEMIA
Sir,(Received on October 15, 1990)
During our study of recording auditory evokedpotentials in protein-calorie malnutrition in infantsand young children (1), we came across a few casesof anaemia. The heamatological investigationsincluding haemogram, showed that, of the fivecases, two had megaloblastic anaemia, two hadmicrocytic hypochromic and one had severe aplasticanaemia. Such neurological complications of varioustypes of anaemias have not been documentedexcept for pernicious anaemia, where classical subacuate combined degeneration of the spinal cordwas first reported by Russell et al (2). Thereafterassociated affection of the cerebral white matterand, more rarely, of the peripheral nerves havebeen amply documented. Direct relationship between optic nerve changes in the form of atrophyto the pernicious anaemia was documented byCohen (3). However it is widely held that optictract involvement in pernicious anaemia is rare(4-6). Patchy demyelination with affection of axiscylinders in the optic tracts has been reported intwo cases of subacute combined degeneration (7).Identical changes have been found in experimentalanimals with induced B12 deficiency (8). Recently,Troncoso et al (9) have reported changes in visualevoked potentials in pernicious anaemia patients,suggestive of impairment of conduction in visualpathways. Now we repor: involvement of auditorypathways in our two permdous anaemia cases using.evoked potential recording procedure. However ofthe remaining three cases, two with microcytichypochromic anaemia and one with severe aplasticanaemia, auditory brainstem evoked responses didnot show any gross change and thus were normal.
Standard evoked potential recording techniquewas employed using Ag/AgC1. disc electrodes
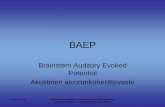
anchored on scalp (CZ-A1 & A2 positions, 10-20International System). Monaurally presented clickstimuli, 2048 in number at 70 dBHL and 1O/secwere used to evoke brainstem auditory potentialresponses (BAEPs) as in our other studies (1,10,11).The two male children (GK 3.5 Yr, and RK4 Yr) had typical megaloblastic bone marrow,showing hypercellular, megaloblastic change withdyserythropoiesis. The BAEP records of one ofthem are· shown in the figure, before and aftertherapy. It is clearly seen that before therapyBAEPs trace is of low amplitude, with indistinguishable wave complexes II, III, IV; the peaks ofwaves I & V are also not very sharp. Aftertreatment with vitamin B 12 injection and oralvitamin B Complex (Inj-Neurobin 1 ml bwx5 andSyrup vito B forte) for 30 days, the repeat BAEPrecord shows normal pattern with distinct wavesI-V (even the late wave components VI & VIIare also clearly visible) with much higher amplitude.The blood picture also improved with nearly normallooking bone marrow after 30 days of therapy.Besides absence of waves II, III, IV or their beinginditinct, there is gross abnormality of reductionin amplitude of wave I & V (much so in Rt.sideFig. upper panel 2nd tracing). More than 50%reduction in amplitude reflects impairment in conduction in the pathways (12). On vit. B complextherapy, there is dramatic increase in amplitudeof these waves indicating better neural conductionin auditory pathways. This preliminary reportsuggests that there is impairment of conduction inbrainstem auditory pathways in pernicious anaemia,and that conduction improves on therapy. This isin agreement with the observations of Troncosoet al (9) who found impairment of visual pathwaysin pernicious anaemia. Further studies using BAEP

Indian J Physiol Pharmacol 1990; 34(4)
L
R
BAEPs IN PA
V
BEFOREV
Letter to the Editor 283
L
R70dBnHL
10/S.C
o 2 4AFTER
10ms~c
Fig. 1 : A representative record of Brainstem auditory evoked potential (BAEP) from a patient(GK 3.5) of pernicious anaemia (PA), before (upper panel) and after vit B complextherapy (lower panel). BAEPs in PA show low amplitude complex with indistinct or absentII, III, IV components. After treatment normal waveform, morphology and amplitudesare restored. L & R stand for left and nght ear. While recording BAEP monoauraUy theother ear was masked by pure white noise (-4OdB).
in a large number of patients with perniciousanaemia may well demonstrate that auditory affection, especially subclinical, is a common and perhapsearly manifestation of the disease, which improveson treatment.
O. P. TANDON AND D. CHOUDHARY
Departments of Physiology and Paediatrics,University College of Medical Sciences &
G. T. B. Hospital, Shahdara, Delhi-110 095

284 Tandan and Choudhary
REFERENCES
Indian J Physiol Pharmacol 1990; 34(4)
1. Tandon OP, Murali YM, Iyer PU, Krishna SVSR, DasD. Brain-stem auditory evoked potentials in malnourishedinfants and children. Brain Dysfunct 1989; 2: 273-78.
2. Russel1 JST, Batten FE, Col1ier JS. Subacute combineddegeneration of the spinal cord. Brain 1900; 23:39.
3. Cohen H. Optic atrophy as the presenting sign in perniciousanaemia. Lancet 1936; 2: 1202-1203.
4. Benham OHH. The visual field defects in subacute combined degeneration of the spinal cord. J Neurol NeurosurgPsychiat 1951; 14:40-46.
5. Holmes J. Cerebral manifestations of vitamin B12 deficiency. Br Med / 1956; 2:1394-98.
6. Lerman S, Feldmahn AL. Centrocecal scotoma as thepresenting sign in pernicious anaemia. Arch Ophthalmol1961; 65:381-85.
7. Adams RD, Kubik CS. Subacute combined degeneration
of the brain In pernicious anaemia. N Engl J Med 1944;231 :1-9.
8. Agamanolis DP, Chester EM, Victor M et al. Neuropathology of experimental vitamin B12 defiency in monkeys.Neurology 1976; 26:905-14.
9. Troncoso J, Mancal1 EL, Schatz NJ. Visual evokedresponses in pernicious anaemia. Arch Neurol 1979;36:168-69.
10. Tandon OP, Krishna SVSR. Brainstem auditory evokedpotentials in children: A normative study. lndian Pediatr1990; 27: 737-40.
11. Tandon OP. Auditory brainstem evoked responses inhealthy north Indians. Ind J Med Res 1990; 92(B): 252-56.
12. Stockard 11, Stockard JE, Sharbrough FW. Brainstemauditory evoked potentials in neurology: Methodology,Interpretation and Clinical application. In 'Electrodiagnosisin clinical Neurology, 2nd Ed: Aminoff AJ (Ed) Churchil1Livingstone New York 1986, 467-503.





![Road Traffic Noise and its Effect on Brain Stem Auditory ... · [2]. Among all objective methods of hearing evaluation, brainstem auditory evoked potential is considered the most](https://static.fdocuments.net/doc/165x107/5f5d38a1dfd4a155386e996d/road-traffic-noise-and-its-effect-on-brain-stem-auditory-2-among-all-objective.jpg)