
BPSD: Psychosis in Dementia - sagelink.ca · Case Study: Differential ... individual with dementia,...
16
BPSD – Handbook for Family Physicians Chapter 7 BPSD: Psychosis in Dementia Dr. Ken Le Clair Dr. Marie-France Rivard
-
Upload
hoangnguyet -
Category
Documents
-
view
233 -
download
11
Transcript of BPSD: Psychosis in Dementia - sagelink.ca · Case Study: Differential ... individual with dementia,...
BPSD – Handbook for Family Physicians
Chapter 7
BPSD: Psychosis in Dementia Dr. Ken Le Clair Dr. Marie-France Rivard

BPSD – Handbook for Family Physicians

BPSD – Handbook for Family Physicians
Chapter Index Introduction .........................................................................................1
Part A: Psychosis as Primary Issue ..................................................3
Definition of Psychosis ......................................................................................................3 The Differential Diagnosis (Think P.I.E.C.E.S.) ................................................................3 What Makes Differential Diagnosis More Challenging in People with Dementia?.......3
Examples of Psychosis due to Changes in the Brain, i.e., the “A”s.............................4
Case Study: Differential Diagnosis Dilemma ...................................5Applying U.R.A.F. to the Case Study ................................................................................5
Part B: Psychosis Secondary to Co-Morbid or Associated Mental Illness .................................................................................................10
The Issues and the Relevance ........................................................................................10
Case Studies ......................................................................................10
Case 1 ...............................................................................................................................10 Case 2 ...............................................................................................................................10 Applying U.R.A.F. to Case Studies ................................................................................10

BPSD – Handbook for Family Physicians
1 of 12 Pages
BPSD – Handbook for Family Physicians
Introduction Family physicians who work in Long Term Care homes are often asked to evaluate elderly patients with psychotic symptoms, such as paranoid behaviours and visual hallucinations. Psychotic symptoms can also appear for the first time in elderly patients who live at home; family physicians working in all types of practice settings may be called upon to evaluate these distressing symptoms. Psychosis occurs in:
• The community in over 4% of individuals over the age of 65 (Christenson 1984). • Long-Term Care Homes in approximately 50% of residents (Wragg/Jeste). • 1/3 of all individuals with moderate Alzheimer’s disease.
Risk Factors for Late Life Psychosis The risk factors for late life psychosis include:
• Cognitive impairment, particularly dementia if it is chronic and delirium if it is acute
• Sensory impairment • Early life trauma • Female • Social isolation
The clinical assessment and management of psychosis, perhaps more than any other, highlights the importance of a differential diagnosis, looking for physical, intellectual, and emotional (i.e., psychiatric) causes for the psychosis and the related behavioural disturbances. Often, as with many individuals with complex needs, multiple causes are responsible for the psychosis itself and/or may contribute to the impact of the psychosis on behaviour, risk to self or others and well-being of the person. It is, therefore, helpful to think of P.I.E.C.E.S., using it as a checklist for assessment and management, i.e., what are the Physical, Intellectual, Emotional (psychiatric), Capabilities (functional), Environmental, and Social factors, either causing the psychosis or contributing to the impact and/or translation into behavioural problems. The challenge of psychosis in BPSD also provides an example of the importance of:
1. A shared collaborative approach with various partners in care. 2. The need for understanding how psychosis and its common causes may vary in different settings and at different stages of illness, for example:
• Psychosis due to medical causes is common in hospital and Long-Term Care settings.
• Psychosis due to “intellectual causes,” i.e., due to changes in the brain, is more common in moderate dementia.
3. The careful selection of both non-pharmacological and psychopharmacological interventions to address target symptoms and their impact on behaviour.
4. Shared monitoring of response and side effects.
This chapter provides an approach to understanding and managing psychosis, reviewing differential diagnosis, including psychosis due to medical causes, i.e., delirium (see Chapter 4)
2 of 12 Pages
BPSD – Handbook for Family Physicians
and due to the brain changes as a direct result of the dementia, that alter the way the person understands, perceives and interprets the world around him or her. (see Chapter 5).
The chapter is divided into two sections, focusing on:
A. Differential diagnosis physical/medical/intellectual problems presenting with psychotic symptoms and their pharmacological and non-pharmacological management B. Co-morbid or re-emerging psychiatric disorders that precipitate psychosis in an individual with dementia, i.e., mood disorders and schizophrenia-like syndromes.
3 of 12 Pages
BPSD – Handbook for Family Physicians
Part A: Psychosis as Primary Issue
Definition of Psychosis
Psychosis is a term used by various individuals and health providers to define a different array of phenomena. For the purpose of this chapter it is defined as “a misperception by the individual that does not match the reality and/or is inconsistent with the beliefs and culture of the person.” It is, therefore, a symptom or phenomenon and may be:
a) A visual or auditory hallucination, i.e., a perceptual disturbance that is not triggered by a
stimulus in the environment. b) An illusion, i.e., a misinterpretation of an environmental trigger such as in a delirious
patient with dementia who sees a curtain looking like a snake. c) Other modality misperceptions, i.e., olfactory or tactile/sensory misperceptions such as
bugs crawling under one’s skin. d) A delusion or false fixed belief that cannot be shaken by reasoning.
The Differential Diagnosis (Think P.I.E.C.E.S.)
Psychosis (delusions or hallucinations) in older persons with dementia can be caused or influenced by:
Physical Cause
A delusion caused by a medical problem such as hypo-thyroidism, drug toxicity or withdrawal (e.g. increased dose of Sinemet or rapid cessation of a benzodiazepine), a major sensory change (e.g. loss of vision leading to non-distressing visual hallucinations of the Charles Bonnet Syndrome) or an acute brain “injury” due to stroke or hypoxia.
Intellectual Change
A dementia-related delusion; psychosis due to the brain disorder causing problems with interpretation and understanding of the environment, i.e., the 7 “A”s.
Emotional Disorder Psychiatric delusions (psychosis), associated with major psychiatric disorders or
disturbances such as psychotic depression, delusional disorder or bipolar disorder
The severity of the delusion and/or psychosis and its impacts may vary or be modified by the match of the demands and the Capacities of the person and Environment and Social supports (C.E.S.).
What Makes Differential Diagnosis More Challenging in People with Dementia?
New or acute physical problems and the recurrence of previously diagnosed psychiatric conditions are often considered in non demented patients. However, brain changes due to dementia make the assessment and management of psychosis more complex. The so-called “A”s of dementia described in Chapter 2 can affect the ability of an individual with dementia to interpret his or her world around him, leading to apparent psychotic symptoms.
4 of 12 Pages
BPSD – Handbook for Family Physicians
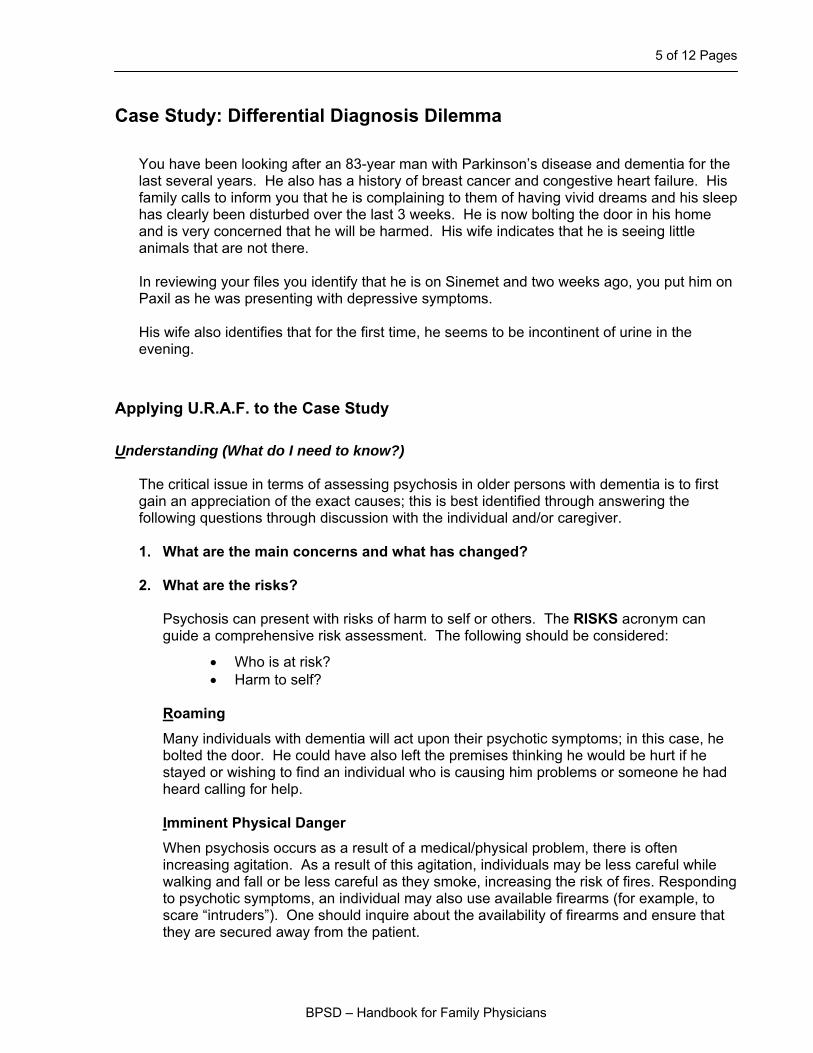
For example, agnosia may lead to the delusion that one’s spouse is an imposter and amnesia may lead to paranoid accusations of stealing. It may be best to consider these “psychoses” as intellectual psychosis, i.e., due to the dementia itself. (See examples in Table 1). This type of psychosis occurs in all stages but tends to be more prevalent in the moderate phase of dementia. Some psychotic symptoms are more common in different phases of the illness, i.e., delusions of stealing may be an early sign of dementia and a red flag for cognitive impairment. Delusions that an individual is in fact an imposter or misinterpreting an individual as someone else who was important in the person’s past tends to be more common in the moderate stages of dementia, or when a specific damage occurs, i.e., a stroke in the R parietal lobe. When dementia has progressed to the point of affecting Activities of Daily Living (ADL) and is moderately advanced, psychotic symptoms secondary to brain changes increase in frequency. It is therefore not surprising to find this type of psychosis particularly in Long Term Care Homes where moderate to severe dementia is more prevalent.
Table 1
Examples of Psychosis due to Changes in the Brain, i.e., the “A”s
• An 82-year old man who does not remember where he placed an object
accuses his wife of stealing (Amnesia).
• A 78-year old woman, Holocaust survivor, screams and yells when people wearing leather jackets approach her (time warp delusions, i.e., individual is living in the present but her ‘terms of reference’ is of the past).
• An 85-year old man looks into the mirror in the bathroom and accuses his wife of having an affair with another man (Agnosia, i.e., does not recognize himself as the person in the mirror).
• An 82-year old woman thinks the T.V. programs are real, that persons are in the room with her and talk to her personally (altered depth/visuo-spatial perception)
• A 78-year old man tries to crawl into bed with his 52-year old daughter (Agnosia + living in a reality of the past– thinks his daughter, who looks like his wife did several years ago, is indeed his current wife since he thinks he is in his fifties as well).
• An 82-year old man screams that there is blood on his bed in the morning. (Altered perception – His wife recently purchased a new bedspread with a bright red rose pattern.)
5 of 12 Pages
BPSD – Handbook for Family Physicians
Case Study: Differential Diagnosis Dilemma
You have been looking after an 83-year man with Parkinson’s disease and dementia for the last several years. He also has a history of breast cancer and congestive heart failure. His family calls to inform you that he is complaining to them of having vivid dreams and his sleep has clearly been disturbed over the last 3 weeks. He is now bolting the door in his home and is very concerned that he will be harmed. His wife indicates that he is seeing little animals that are not there. In reviewing your files you identify that he is on Sinemet and two weeks ago, you put him on Paxil as he was presenting with depressive symptoms. His wife also identifies that for the first time, he seems to be incontinent of urine in the evening.
Applying U.R.A.F. to the Case Study Understanding (What do I need to know?)
The critical issue in terms of assessing psychosis in older persons with dementia is to first gain an appreciation of the exact causes; this is best identified through answering the following questions through discussion with the individual and/or caregiver.
1. What are the main concerns and what has changed?
2. What are the risks?
Psychosis can present with risks of harm to self or others. The RISKS acronym can guide a comprehensive risk assessment. The following should be considered:
• Who is at risk? • Harm to self?
Roaming
Many individuals with dementia will act upon their psychotic symptoms; in this case, he bolted the door. He could have also left the premises thinking he would be hurt if he stayed or wishing to find an individual who is causing him problems or someone he had heard calling for help.
Imminent Physical Danger
When psychosis occurs as a result of a medical/physical problem, there is often increasing agitation. As a result of this agitation, individuals may be less careful while walking and fall or be less careful as they smoke, increasing the risk of fires. Responding to psychotic symptoms, an individual may also use available firearms (for example, to scare “intruders”). One should inquire about the availability of firearms and ensure that they are secured away from the patient.
6 of 12 Pages
BPSD – Handbook for Family Physicians
Suicide
Psychotic and severe depressions can occur during the course of dementia. Individuals who feel they “deserve to be punished for past mistakes or sins” as part of their psychotic depression will be at high risk for suicide (mood-congruent delusion). Individuals who feel, as part of their depression, that they are in an untenable, hopeless situation, will also be at risk for self-harm. Those who have agitated depressions are also at risk of impulsive self-harm despite denying suicidal intent, feeling they cannot cope anymore with this terrible agitation.
Kinship and harm to others
In order to assess the risk to others, one needs to identify whether delusions are “focused” on a particular individual and if the person with psychosis has acted on delusions in the past (e.g. to deal with perceived persecution).
Substance Misuse and Safe Driving Substance and alcohol misuse can cause or worsen psychotic symptoms as well as compound other risks associated with psychosis. Individuals with psychosis, particularly in the context of dementia, may be more distractible with problems of attention and concentration and therefore pose a higher risk in terms of safe driving.
3. What are the possible contributing factors in this case?
Think about the P.I.E.C.E.S. checklist and “check out” causes in the physical, intellectual, emotional, functional, environmental, and social spheres. In Case Study A, the psychosis is of recent onset and should trigger a search for medical causes, i.e. a delirium. The four major causes of medical decline and/or delirium are: 1. Medicines (drugs, in this case, Sinemet, Paxil) 2. Microbial, infections (could a UTI explain recent incontinence?) 3. Myocardial or respiratory illnesses and other medical diseases unique to the
individual (MI with CHF?) 4. Metabolic changes (low sodium secondary to Paxil, hypoglycemia, hypothyroidism,
hypo or hypercalcemia) In this situation, and in any psychotic presentation, sensory impairment and the possibility of partial seizures are also important to consider.
7 of 12 Pages
BPSD – Handbook for Family Physicians
Reflection (How can I explain what’s going on?)
1. What is the most likely explanation? • A medical psychosis; • An intellectual psychosis, i.e. due to an association with the dementia itself; or • A psychiatric psychosis. In this case, medical psychosis is suspected but it is possible for all 3 to be present at the same time.
2. Arrive at a common understanding of the psychosis, the desired outcomes, and the role/support the family physician, person, family, and health professionals will provide.
Actions (What needs to be done?)
1. What is the immediate action?
In this case, focus on the risk to self and others. Treating a delirium in this case is a medically urgent issue. Review the patient factors, his ability to engage in support strategies and the types of supports available. This will enable one to determine the degree of risk and the immediacy of action as well as outline some areas where immediate interventions could be made.
Consider how to collaborate with the person, family, and other care providers in ensuring safety and effective treatment. Arrive at a set of common goals and clearly defined roles, keeping the patient at the centre of the assessment and management strategy.
2. What tests or additional information would be useful?
If, as in these cases, you suspect a medical cause, perform appropriate exams and investigations: • Medicine (i.e., digoxin toxicity, or Sinemet) • Metabolic (changes thyroid function, calcium phosphorous, B12 and folic acid have
been associated with psychosis in late life; in this case, hyponatremia is particularly relevant to consider).
• Microbials (due to recent onset of incontinence in this particular individual, it is important to include a urinalysis; chest X-Rays may be indicated in those susceptible to lung infections).
• Myocardial and other illness should be considered, such as worsening of congestive heart failure, etc.
8 of 12 Pages
BPSD – Handbook for Family Physicians
If this, in fact, a “medical psychosis”, correction of the underlying medical problem(s) is urgently required. Be aware that there is usually more than one medical cause. However, in up to 30% of cases of clinical delirium, no specific medical cause can be found. Even without a specific cause found, consider it a “medical psychosis and/or delirium” and institute effective support strategies and treatments.
3. Non Pharmacological Approaches if Psychosis is due to Delirium The general principles of assisting and intervening in a non pharmacological approach to psychoses that are due to a medical cause and/or delirium can be drawn from the work of Inouye as outlined in Chapter 4. One may consider the acronym CHAOS to remember the critical elements in treatment: Cause (treat it) Hydration (ensure nutrition) Approach (do’s and don’ts; pay most attention to non-verbal communication) Orientation (ensuring appropriate structure) Support for the caregiver and avoidance of sedation
4. Non Pharmacological Approaches, if Cause of Psychosis is due to Changes in the Brain
In this situation, it may be helpful to think of the acronym ERRORS to define non pharmacological approaches. Environment: What is it telling the person? For example, if the environment is triggering a past traumatic event then removing the stimulus may help, i.e., leather jacket triggering fear in a former Holocaust survivor Reception: Vision and hearing Regulation: Over or under stimulation Organization: How do I approach the individual given the changes in his brain or behaviour? (Particular attention to nonverbal interactions) Reality: Various causes unique to this person; think P.I.E.C.E.S. Support the Caregiver
5. Are there other interventions that should be started? 6. Who else might be involved?
7. Interaction Review the Do’s and Don’ts for interacting with the individual with psychosis, i.e.: • Do ensure the person’s and your safety • Do understand this is a response to a “real” perception of the individual • Do focus on the effects on the person not the content
(i.e. validate feelings, concerns) • Do distract • Don’t confront the false beliefs
9 of 12 Pages
BPSD – Handbook for Family Physicians
Follow-Up (How should things be monitored and re-evaluated) A very helpful way to define risks and monitor response is to use the 7 “D”s to characterize the psychosis. The 7 “D”s provide a mechanism for:
1. Determining how immediate action is required 2. Monitoring response 3. Deciding whether or not to use a medication
The “D”s characterize the psychosis/delusion and its impact. The “Ds” are:
1. Dangerousness 2. Distressing 3. Disturbing 4. Disability 5. Directing Action 6. Distant or present 7. Definite (fixed delusion)
The sequence of response to a psychosis and its associated behavioural problems usually follow a similar pattern of resolution. Often, the distressing and disturbing behaviours begin to settle down in the individual; he or she stops acting on the delusion, i.e., bolting doors due to fear of persecution. Then the delusion psychosis may be perceived by the individual as more in the past and finally, the delusion itself may resolve. It is important to consider this usual sequence of response as it may assist the clinician with her or his colleagues in better determining response, whether to increase medication, and prevent premature abandonment of successful strategies.
Usually resolve, initially
Next to resolve
Last to resolve or may never completely disappear
10 of 12 Pages
BPSD – Handbook for Family Physicians
Part B: Psychosis Secondary to Co-Morbid or Associated Mental Illness
(Mood and Anxiety or Schizophrenic-Like Disturbances)
The Issues and the Relevance
• 25% of individuals with dementia have signs and symptoms of a major affective disorder through the course of illness, i.e., Major anxiety and mood disturbances are common.
• Major mental illness, i.e., schizophrenia, bipolar disorder may co-exist with dementia.
Case Studies Case 1
A 79-year old woman hears voices telling her she is rotten and she believes the neighbours are stealing from her and that they are putting odorous gas in her ventilation. She has moved every 3-4 years and recently bolted her doors and taped her windows. She has had memory difficulties for approximately the last 5 years
Case 2
A 92-year old woman noted to have mild memory problems lost her husband of 40 years eight months ago. She is now very irritable and complains of stomach discomfort. She believes she has sinned and is indicated that she has no money and feels people are against her. When questioned, she identifies that she feels that having people against her is certainly deserved.
Applying U.R.A.F. to Case Studies Understanding (What do I need to know?) 1. What are the main concerns and what has changed?
• The major issue in these cases is to identify when and how long the psychosis has been present. As was noted previously, acute onset psychosis tends to be more associated with a medical cause.
• A more progressive, slower onset and, if associated with changes in function and
“moderate” dementia stage, can point the practitioner to thinking more about a psychosis associated with the dementing illness itself.
• The changes associated with the major mental illnesses and/or psychiatric clusters tend
to occur in between the two. One may find in the schizophrenic-like psychosis (Case 1), that there may be some pre-morbid personality issues and odd personality presentations over the person’s lifetime that are now increasing in their severity or emerging now to cause functional issues and distress and disturbing relationships with others in their environment and/or as in Case 2, anxious mood disturbances a family history and/or personal history of mood or anxiety disorder of substance misuse.
11 of 12 Pages
BPSD – Handbook for Family Physicians
• Identify how distressing the behaviours are. At times, and particularly in schizophrenic-like illness, the psychosis may not be causing the person significant distress. This will help in terms of understanding the type of intervention and how to best proceed in a timely and sensitive manner.
• Use the 7 “D”s in the schizophrenic-like psychosis (Case 1) to characterize the degree of
distress and disability associated with the psychosis. Be guided by the results of a collaborative discussion using the 7 “D”s as a collaborative care discussion tool to decide risk, urgency, as well as understanding and appreciating the distressing and disturbing nature of the behaviour, both on the individual and caregiver.
• In Case 2, tools such as the SIG E CAPS and questions from the Cornell Scale for
depression in dementia, a scale developed by Alexopoulos et al for persons who have dementia and depression, may help to identify a possible mood-associated psychosis. Health practitioners, family members may not be aware that psychosis can be part of a major affective disorder and that appropriate treatment can bring significant relief.
2. What are the RISKS and possible causes? • Careful assessment of risks using the RISKS acronym will be helpful to identify
particularly whether there is any suicidal and/or threats to others because of the nature of the disorder.
Reflection (How can I explain what’s going on?)
Once understanding occurs, determine mutually agreed upon goals and outcomes. Reaching common ground and identifying priorities for action will be helpful with the person, the family members, and other providers. Lack of collaborative understanding will often result in failure in both the assessment and management.
Actions (What needs to be done?)
Identify roles that each partner will assume to meet goals and outcomes. 1. What needs to be done right now?
Looking at what needs to be done urgently will be guided by review of risks factors such as suicide, and the results of characterizing the psychosis using the 7 ”D”s, particularly the issue of dangerousness. In addition, this will guide further investigations and looking at information and monitoring processes collaboratively with the individual and his or her caregiving network. In the case of acute psychosis due to delirium, when there is no longstanding delusion or paranoia, one may consider the very short-term use of haloperidol as an emergency measure to allow proper investigations (see delirium chapter). When it is clear that an antipsychotic medication will be required for at least several weeks, we prefer using atypical antipsychotic medications such as Risperidone, Olanzapine or Quetiapine. Given that all antipsychotic medications can cause serious side effects, including an increase risk of death, it is important to document that the drug is clearly indicated (for a psychosis that will likely continue over time and causes much distress to the patient), that it will be used for as short a time as possible (e.g. with a review of its use and possible decrease in the dose or discontinuation every 3
12 of 12 Pages
BPSD – Handbook for Family Physicians
months) and at the lowest possible dose (with a slight decrease in dose as soon as mild side effects or clear benefits occur, to avoid accumulation and significant side effects). It is also important to document how informed consent was obtained (risk-benefit discussion) with the patient or Substitute Decision Maker. Typically, when psychosis occurs as a result of dementia, ongoing use of antipsychotic medication is usually not required and it is possible to discontinue without a return of the psychotic symptoms. However, for psychiatric illnesses such as schizophrenia, antipsychotic medications may have to be continued indefinitely, although a reduction in dose may be possible. The psychotropic laminate provides concise information on starting doses, maximum recommended doses, risk and side effect profile as well as suggested monitoring.
2. Investigations
Investigations depend on the type of associated disorder. If it is a co-existing mood/anxiety disorder refer to Chapter 6. Note: treatment of psychosis as a result of depression often requires both an antipsychotic and an antidepressant and may require Electroconvulsive therapy. If it is co-morbid ‘schizophrenia-like disorder’ or sometimes called a late life paraphrenia, rule out common medical causes that can or have been associated with paranoia in late life: it will therefore be useful to check Ca, P, B12, Folic acid, TSH.
3. Who else should be involved? A common understanding by all involved when psychosis is due to associated mood or anxiety disorder or disturbance or co-morbid late life schizophrenia is necessary for success. Using U.R.A.F. will be very helpful in terms of determining causes and identifying and correcting misunderstandings. Monitoring of response, consider the 7 “D”s.
4. Interaction
• Remember the Do’s and Don’ts. • Keys to interaction are trust, empathy, and understanding. • Non-verbal is 80% of communication. • Establishing an ongoing supportive and therapeutic and trusting relationship with the
patient is fundamental to effective care. Follow-up (How should things be monitored and re-evaluated?)
Identify with the person, family, other providers, the expected/desired outcomes and when to expect them. Define key triggers for review and what re-assessment and actions should take place.


















