BPCO: diagnosi e valutazione di gravita’ - Aristea · Firenze 22/23.09.2016 FISIOPATOLOGIA E...
39
Firenze 22/23.09.2016 FISIOPATOLOGIA E IMAGING FUNZIONALE DEL POLMONE BPCO: diagnosi e valutazione di gravita’ Isa Cerveri SC PNEUMOLOGIA IRCCS Fondazione Policlinico San Matteo Universita’di Pavia
Transcript of BPCO: diagnosi e valutazione di gravita’ - Aristea · Firenze 22/23.09.2016 FISIOPATOLOGIA E...

Firenze 22/23.09.2016
FISIOPATOLOGIA E IMAGING FUNZIONALE DEL POLMONE
BPCO: diagnosi e valutazione di gravita’ Isa Cerveri
SC PNEUMOLOGIA
IRCCS
Fondazione Policlinico
San Matteo
Universita’di
Pavia
DIAGNOSIS AND SEVERITY CLASSIFICATION OF COPD
COPD as a complex disease with multiple pathological components ignored when spirometry is used as the only method to evaluate it
FEV1is a crude, not sensitive parameter
It correlates poorly with clinical parameters
Similar FEV1 may have different pathologies
Additional measures are needed to allow a more complete and clinically relevant assessment of the disease
Advances in quantitative CT scanning has emerged
as a noninvasive tool in the “phenotyping of COPD”,
with measures investigating changes in the aiways wall
and lumen and within the lung parenchyma
CT imaging quantitative assessments has shown
associations with parameters of airway physiology

Relationships of emphysema extent by HRCT to
lung elastic recoil and DLCO
Baldi et al., AJRCCM 2001

0
0,1
0,2
0,3
0,4
0,5
Sim
ple
reg
ress
ion
R 2
FEV1
FRC
RV
TLC
RV
/TLC
DL,C
O
DL,C
O/V
A
Chest 2004
Relationships of classical PFT variables to emphysema extent by
HRCT
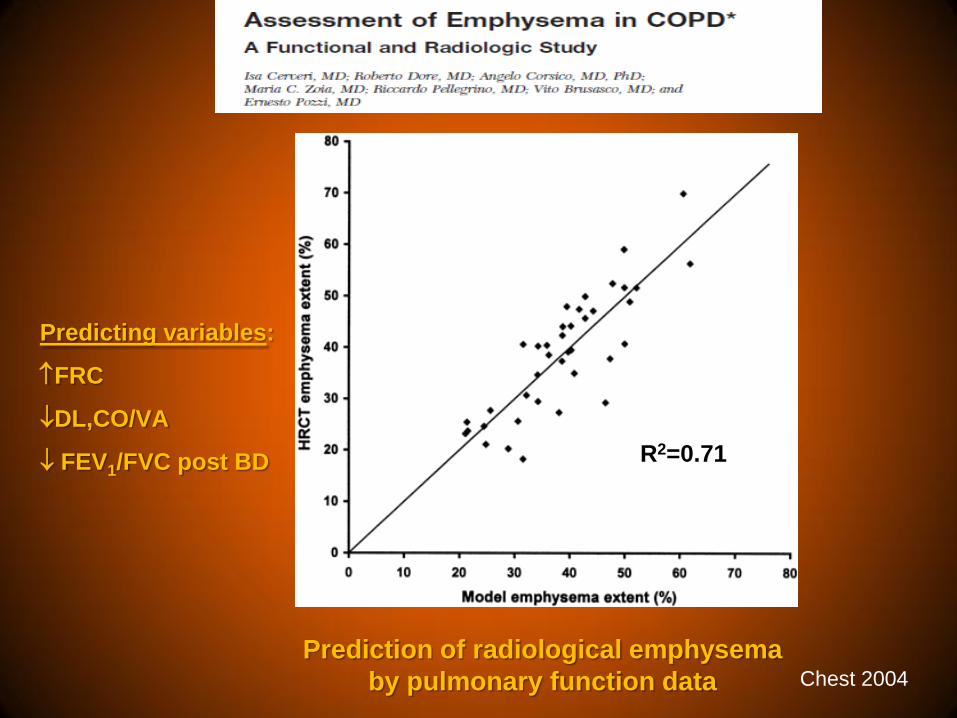
Chest 2004
Predicting variables:
FRC
DL,CO/VA
FEV1/FVC post BD R2=0.71
Prediction of radiological emphysema
by pulmonary function data

Relationships between airway wall area by CT or OCT and
lung function in COPD
Coxson et al AJRCCM 2008
CT
OCT OCT
CT

Bronchodilator response in COPD In some patients, the FVC increases without an increase
in FEV1
Cerveri et al., JAP 2000
1 2 3 4
-1
0
1
2
3
4
Volume (L)
Flo
w (
L/s
)
FEV1 & FVC
responder

Cerveri et al., JAP 2000
1 2 3 4
-1
0
1
2
3
4
Volume (L)
Flo
w (
L/s
)
FVC responder
1 2 3 4
-1
0
1
2
3
4
Volume (L)
Flo
w (
L/s
)
FEV1 & FVC
responder
Bronchodilator response in COPD In some patients, the FVC increases without an increase in
FEV1

Bronchodilator response in COPD The increase in FEV1 is inversely related to the extent of
emphysema
FVC responders
FVC & FEV1 responders
Emphysema extent (%)
Δ F
EV
1 (
% p
red
icte
d)
0
12
24
20 30 40 50 60
Cerveri et al., JAP 2000

Cerveri et al. JAP 2000
Bronchodilator response in COPD Isolated volume responses are associated with a
paradoxical effect of lung volume on airway caliber
FVC & FEV1 responder FVC responder


131 patients firstly diagnosed with moderate COPD
(GOLD stage 2)
Three years follow-up study
Baseline wide multidimensional approach with comprehensive clinical, complete functional and imaging characterisation of the patients

0
10
20
30
40
Presence of emphysema
Frequent exacerbations prestudy
N. of patients
26,1% 24,4%
Baseline clinical characteristics
Cerveri I, COPD 2012

0
20
40
60
80
100
120
140
FRC RV FEV1post
%p
red
62±12
123±24 129±32
91±18
FVCpost
Baseline lung function

The mean FEV1 decline were 42±66 mL/y
0
20
40
60
80
100
Rapid decliners Non rapid decliners
FE
V1 d
eclin
e
(mL/y
)
88±76 mL/y
6±54 mL/y
Cerveri I, COPD 2012

MULTIVARIABLE ANALYSIS
The presence of emphysema at HRCT scan proved to be an
independent prognostic factor of rapid decline in FEV1
When the presence of emphysema was replaced by mean RV, the
model still remained significant
Odds ratios
(95% CI)
p Value
Model 1: <0.0001
● Smoking pack-years 1.02 (1.00, 1.03) 0.047
● Presence of emphysema 17.76 (4.21, 74.93) <0.001
● FEV1 3.64 (1.07, 12.38) 0.038
● Exacerbations per year requiring hospitalization during F/U 4.60 (1.53, 13.86) 0.001
Model 2: 0.002
● Smoking pack-years 1.01 (1.00, 1.02) 0.15
● Residual volume 1.84 (1.04, 3.24) 0.037
● FEV1 2.93 (1.16, 7.43) 0.023
● Exacerbations per year requiring hospitalization during F/U 2.58 (0.99, 6.72) 0.052

The rapid FEV1 decline may be identified by the presence of
emphysema, as assessed by HRCT scans or lung function
testing, in patients with a long smoking history
This supports the importance of lung volume
determination at the first assessment of COPD patients and,
only when needed, further imaging studies
CONCLUSIONS



Quantitative evaluation CT scan in COPD
%LAA-950 AWT-Pi10 (mm)
Vida Diagnostics, Coralville, Iowa,
http://www.vidadiagnostics.com/
Lung Functional Imaging in COPD
244 studies from 1967 to 2016
>200 studies from 2010 to 2016



FEV1 103%pred DLCO 119% pred
FEV165% pred DLCO 17% pred
FEV147% pred DLCO 63% pred




The routine clinical application of serial examinations limited because of the potential risks of cumulative exposure, even in older subjects with COPD
Need to perform CT imaging in patients at the lowest doses possible X ray–dose reduction strategies
Limited spatial resolution possible when low radiation doses are used (evaluation of wall thickeness in the small airways extremely difficult or impossible)

The reconstruction methods affect quantitative measurements and can alter comparability
Standardization of imaging protocols and methods
Availability of sophysticated techniques
Increased costs !!

Excellent safety and tolerability profile Major application of conventional MRI: pulmonary vessel emodynamics Technical problems due to the unique
caracteristics of lung tissue Recent refinements reducing the time
required for imagine acquisition
FEV1:52%; FEV1/FVC 40% FEV1:81%; FEV1/FVC 52%

FEV1:89%; DLCO 64% FEV1:28%; DLCO 32% FEV1:52%; DLCO:55%

A : He MRI
FEV1:46%; FEV1/FVC 53%
B : FDMRI
Patient with COPD and bullous emphysema
Evaluation of regional ventilation Depending on inhaled gas or injected
contrast agents Poor availability of polarized noble gases Expensive !!
Evaluation of regional ventilation and /or perfusion
Not depending on inhaled gas or injected contrast agents
Image registration and analysis complex Important advantages with good potential
for clinical translation

FEV189% pred DLCO 64% pred
FEV1 28% pred DLCO 32% pred
FEV1:52% pred DLCO:55% pred

CT For younger people, even with low dose adaptive iteraction methods, radiation
dose and long-term burden/risk remain a concern
For clinical application continued emphasys on dose reduction is essential
MRI MRI, without exposure to ionizing radiation, could provide an excellent alternative
for clinical application in COPD patients
Semplification of the acquisition and analysis of methods
Improvement of knowledge dissemination
CONCLUSIONS I

CONCLUSIONS II
PULMONARY FUNCTION TESTING
Widely accessible
Easy to implement
Straighforward measurements
They do not tell the whole story for patient populations and individual patient
IMAGING AND PULMONARY FUNCTION TESTING
COPD, as a complex and heterogeneous disease, can not be diagnosed
and treated with simple tools !!
A greater integration is necessary between imaging and pulmonary
function tests both in research, in clinical trials and in clinical practice !!


Reduced parenchymal density (LAA) and airway wall
thickening in asymptomatic smokers and COPD
Nakano et al, Chest 2002

Cerveri et al. JAP 2000
FVC & FEV1 responders
FVC responders
Bronchodilator response in COPD The increase in FEV1 is inversely related to functional
indices of emphysema