Bpac Polypharmacy Poem 2006 Pf
20
nz bpac better edicin m e POLYPHARMACY
-
Upload
jacob-alexander-marpaung -
Category
Documents
-
view
15 -
download
4
description
polifarmasi
Transcript of Bpac Polypharmacy Poem 2006 Pf

nzbpacbetter edicin m e
POLYPHARMACY

bpacnz Development Team: RachaelClarke
SoniaRoss
DrTrevorWalker
DavidWoods
Acknowledgement:
bpacnzwouldliketothankProfessorJohnCampbell,AssociateProfessorNgaireKerseandDrNeilWhittakerfortheirhelpandguidance
onthedevelopmentofthisresource.
Developedbybpacnz
Level8,10GeorgeStreet
POBox6032
Dunedin
Phone034775418
Fax0800bpacnz(0800272269)
www.bpac.org.nz
©bpacnzMay2006
Allinformationisintendedforusebycompetenthealthcareprofessionalsandshouldbeutilisedinconjunctionwithpertinentclinical
data.
www.bpac.org.nz
Soonyouwillreceiveamultimeds self-administered patient questionnairetoidentifypeopleathigherriskof
drugrelatedproblems,amedicinesgridtoprovideavisualrepresentationofmedicationuseandaSIMPLEschema
formedicinesreview.

“But know also, man has an inborn
craving for medicine ...the desire to
take medicine is one feature which
distinguishes man the animal, from
his fellow creatures. It is really one
of the most serious difficulties with
which we have to contend.”
WilliamOsler1894
Contents
Background,GoalandObjectives.......................................................................................................................2
Polypharmacy-weighingupthebenefitsandharms.............................................................................................3
Elderlypeopleareatincreasedriskofdrugrelatedproblems...............................................................................4
Drugsassociatedwithincreasedriskofadversedrugreactionsinelderlypeople...................................................6
Commondruginteractionsinelderlypeople........................................................................................................7
Recognisingadversedrugreactions...................................................................................................................8
Riskfactorsfordrugrelatedproblemsinelderlypeople.................................................................................... 10
AreallygoodrecipeforDRP............................................................................................................................ 11
Drugrelatedharm;termsanddefinitions........................................................................................................... 12
Hospitaladmissionsforadversedrugreactions................................................................................................. 14
CARMcomment.............................................................................................................................................. 16
References,Bibliography................................................................................................................................. 17
bpacnzPolypharmacyIPage1
POLYPHARMACY

Goal
Thegoalofthiscampaignistodecreasedrugrelatedproblemsinelderlypeoplebyreducingprescribing
factorsassociatedwithincreasedrisk.
Background
Drugrelatedproblemscausesignificantpreventablemorbidityandmortality.Theireconomiccostis
estimatedtorankfourthinthedevelopedworld,behindcardiovasculardisease,canceranddiabetes.
Drugrelatedproblems includeadversedrugevents,adversedrugreactionsanddrug interactions.
Polypharmacyhasvariousdefinitionsandconnotationsintheliteraturerangingfromtheuseof4,5,
6ormoredrugsincombinationtothemoresimplisticadditionofjustoneinappropriatedrugtoan
existingdrugregimen.Theadditionofanydrugisonetoomanyifitprovidesnobenefitandcauses
potentialharm.Ourdefinitionofpolypharmacyforthepurposeofthiscampaignis:“theadditionofone
ormoredrugstoanexistingregimenwhichprovidesnoadditionaltherapeuticbenefitand/orcauses
drugrelatedharm”.Elderlypeopleonmultiplemedicationsareatparticularlyhighriskofdrugrelated
problems.
Objectives
To raise awareness of the increased risk of drug related problems associated with
polypharmacyand toprovide tools, includingmedicines review, to identify andmanage
highriskpatients.
Identifyandraiseawarenessofmajorcategoriesofadversedrugreactionsandhighrisk
drugcombinationsinNewZealand.
Reducetheinappropriateuseofhighriskdrugsanddrugcombinationsespeciallyinelderly
people.
Reducethe“prescribingcascade”phenomenon.
•
•
•
•
Page2 IbpacnzPolypharmacy
“Don’t treat risk factors. Don’t even treat disease. Treat patients, and treat them as individuals”
ProfessorJohnCampbell,2005
POLYPHARMACY

Polypharmacy
Potentialbenefits Riskofharm
Synergisticcombinationsallowlowerdosesandthereforeless
adverseeffectsthanindividualdrugs.
e.g.treatmentofhypertension
Synergisticadverseeffectsincreaseriskofharm.
e.g.mayincreaseriskoffallsduetoposturalhypotension
Supplementaldrugmaydecreaseadverseeffectofinitialdrug.
e.g.anticholinergicaddedfordruginducedextrapyramidaleffects
Increasedcomplexityoftheregimencanleadtoconfusion,error
andpooradherence.
e.g.multipletablets,multipledoses,increasedriskofsideeffects
Additionaldrugmayimproveoutcomes.
e.g.additionofspironolactonetoACEinhibitorforheartfailure
Increasedopportunitiesfordruginteractions.
e.g.increasedriskofhyperkalaemia
Multipledrugsmaybeneededformultipleconditions.
e.g.diabetesplusosteoarthritis
Moredrugs=moreopportunityforadverseeffects.Difficultto
predictinteractionswithinacomplexregimen.
e.g.ACEinhibitorplusNSAIDincreasestheriskofrenalfailure
Polypharmacy - weighing up the benefits and harms
“First do no harm”
Hippocrates,460-355BC
Theuseofmultipledrugsisacceptedbestpracticeforcommon
chronicconditionssuchashypertensionanddiabetes.Conscientious
clinicians,whoadheretoevidence-basedguidelines,willoftenfind
themselvesprescribingsixormoredrugsforpeoplewithseveral
chronic conditions. However, trials investigate populations and
clinicianstreatindividuals.
Manypeopleon fiveormoredrugswill be takinganunfamiliaroreven
uniquecombination (Bjerrum,1998). Thepotential benefits and risksof
harmofsuchregimenswillnothavebeensubjecttoresearchandareoften
difficulttopredict.
The difficulty is balancing the potential benefits of these drugs,
as described in the guidelines, with the risk of harm from the
highnumberofdrugsused.Cliniciansneedtoconsidercarefully
numbers needed to treat, numbers needed to harm, long term
prognosisandthewishesofindividualpatients.
bpacnzPolypharmacyIPage3

Riskofevent
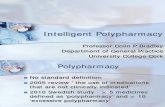
Figure 1. Risk of harm increases with number of drugs taken
The risk of an adverse drug event has been
estimated at 13% for two drugs, 58% for five
drugsand82%forsevenormore(Fulton&Allen,
2005).
0 %
20 %
40 %
60 %
80 %
100 %
0 %
20 %
40 %
60 %
80 %
100 %
2drugs 5drugs 7+drugs
Elderly people are at particular risk of drug related problems
becauseofcomplexdrugregimensinvolvingmultipledrugsandthe
physiologicalchangeswhichaccompanyaging.Upto30percent
ofhospitaladmissionsintheelderlymaybeassociatedwithdrug
relatedproblems(Hanlon,1997).
Large clinical trials often exclude elderly people and those with
co-morbidities. Thismeans that subjects of trials are often very
differentfromtheelderlypatientswithmultipleco-morbiditiesseen
inpractice.AUKstudyfoundstrokepatientsinprimarycarewere
on average 12 years older than patients in the research which
formedthebasisofnationalguidelinesforbloodpressurelowering
for patientswith stroke (Mant, 2006). Theguidelines, therefore,
cannotbeapplieduncriticallytothepatientsofthesepractices.
Elderly people are at increased risk of drug related problems
Prescribersneedtoconsiderthespecialneedsofelderlypatients
whenfollowingclinicalguidelines.Iftheydonot,theyarelikelyto
exposetheirpatientstoincreasedriskofdrugrelatedproblems.
Changes which accompany aging make people particularly susceptible to drug related problems.
Physiological changes associated with aging affect a person’s
handling and response to drugs. Changes in the excretion and
metabolism of drugs lead to increased drug concentrations,
changesinreceptorsensitivitycauseexaggerationorbluntingof
drugeffects,anddeclineincognitivefunctionmakesadherenceto
acomplexdrugregimendifficult.
Page4 IbpacnzPolypharmacy

Some examples of age related changes to drug effects include:
increasedposturalswaywithbenzodiazepines
increasedsensitivitytoCNSdrugs,e.g.benzodiazepines,opioids,antipsychoticsandantiparkinsondrugs
posturalinstabilitypre-disposingtodruginducedhypotensionanddrugrelatedfalls
increasedanalgesiceffectofmorphine
reducedpeakdiureticresponsetofrusemide
increasedanticoagulanteffectofwarfarin,and
impairedthermoregulatorymechanismspredisposingtodruginducedhypothermia
MangoniandJackson,2003
•
•
•
•
•
•
•
Age related changes which increase the risk of drug related problems
bpacnzPolypharmacyIPage5
Receptor sensitivities changeRenal function declines
Cognitive function declinesGastro-protection reduced
Liver metabolism slowsCirculatory instability
Increasing age

Some drugs associated with adverse drug reactions in the elderly
Drugordrugclass Comments
AlldrugsStartlow,goslow.Manydrugs,e.g.oxybutynin,antipsychotics,TCAs,
antihypertensivesneedmuchlowerdosesinelderlypeople.
benzodiazepines
Thosewithalonghalf-life,suchasdiazepam,nitrazepamcauseexcessiveand
prolongedsedation.Temazepamisabetterchoiceifnecessarybutallarebest
avoided.
cimetidine Moredruginteractionsandagreaterpotentialforconfusionthanranitidine.
dextropropoxyphene Cancauseconfusionandexcessivesedationintheelderly.
digoxinUselowdosesinitially.Extravigilancerequiredforthosewhoneedtobeonhigher
doses.
indomethacin ThisNSAIDhasahighincidenceofCNSeffectsandgastrotoxicity.
nefopam(Acupan) CNSeffectsandmarkedanticholinergicactions;avoid.
NSAIDsUselowestdosenecessaryfortheshortestperiod.Avoidlong-termuseoffulldose,
longerhalf-lifedrugssuchasnaproxenandpiroxicam.
tricyclicantidepressants(TCAs)Doxepinandamitriptylineareverysedatingandhavestronganticholinergicactions.
Notpreferredasfirstchoicefordepressionintheelderly.
thioridazine(Aldazine) GreaterpotentialforCNSandextrapyramidaleffects.
Drugs associated with increased risk of adverse drug reactions in elderly people
Because of age related changes in drug handling described on
page5certaindrugsareassociatedwithincreasedriskofadverse
drugreactionswhengiventoelderlypeople.
If the potential benefits of these drugs for an individual patient
appear to outweigh the risks of harm they should be used with
caution;otherwisetheyshouldbeavoided.
Page6 IbpacnzPolypharmacy

Common Drug Interactions
Drugcombination Riskofharm Prevention
warfarin/NSAIDs
increasedriskofbleeding
reviewneedforNSAIDconsider
paracetamolasanalternative
warfarin/amiodaronemonitorINRandadjustwarfarindose
accordingly
warfarin/sulfadrugs
usealternativeantibioticwarfarin/macrolides
warfarin/norfloxacin
warfarin/phenytoin
increasedorpossibledecreasedeffectsof
warfarin
phenytoinconcentrationpossiblyincreased
monitorphenytoinlevelandINR
ACEinhibitors/K+supplements elevatedpotassiumlevelsmonitorpotassiumlevels
discontinueK+supplementifnotneeded
ACEinhibitors/spironolactoneelevatedpotassiumlevels
renalfailuremonitorpotassiumlevelsandrenalfunction
ACEinhibitors/NSAIDs renalfailure
re-evaluateneedforNSAID
monitorrenalfunction
avoidhypovolaemia
digoxin/amiodarone digoxintoxicity
decreasedoseofdigoxinby50%when
addingamiodaroneandcheckdigoxin
levelsweeklyuntilstable
digoxin/verapamildigoxintoxicity
bradycardia,heartblock
checkECG
re-evaluateneedforthesedrugs
theophylline/norfloxacinandciprofloxacin theophyllinetoxicityre-evaluateneedforthesedrugs
monitortheophyllinelevels
anticholinergiccombinationse.g.TCA,
sedatingantihistamine,antipsychotic,
oxybutynin,orphenadrine,benztropine,etc
sedation,confusion,blurredvision,fallsreducenumbers,strengthordosesof
thesedrugs
drugsactingontheCNS
combinationsofantiepileptics,
antipsychotics,analgesics,
antidepressants,etc
sedation,confusion,fallsreducenumbers,strengthordosesof
thesedrugs
“The ingenuity of man has ever been fond of exerting itself to varied forms and combinations of medicines.” WilliamWithering,1785
Common drug interactions in elderly people
It is impossible to remember all possible drug interactions; see
howlongthelistisinappendixoneoftheBNF!Anumberofdrug
combinationsarefrequentlyusedbuthavethepotentialtocause
significant harm if notmanaged appropriately.Not every elderly
adult who takes these medications together will experience an
adversereaction.
bpacnzPolypharmacyIPage7

Recognising adverse drug reactions
Common presentations of adverse drug reactions in the elderly
Symptom Possiblecausativeoraggravatingdrugs
Confusion
benzodiazepines,phenothiazines(e.g.chlorpromazine,promethazine,methotrimeprazine),anticholinergic
drugs,TCAs,opioids,antiparkinsondrugs,anticonvulsants,corticosteroids,NSAIDs,cimetidine,ranitidine
orsuddenbenzodiazepinewithdrawal
Unsteadinessandfallscombinationsofdrugswithsedatingproperties(e.g.TCAs,anticonvulsants,phenothiazines,sedatinganti-
histamine,antipsychotic,benztropine,opioids)anticholinergics
Constipationcalciumchannelblockers(especiallydiltiazemandverapamil),phenothiazines,tricyclics,anticholinergic
drugs
Depression longtermbenzodiazepineuse,highdosesofTCAs(especiallyamitriptylineanddoxepin)
Dyspepsia NSAIDs
Electrolytedisturbancesloopandthiazidediuretics(hypokalaemia,hyponatraemia),potassiumsparingdiuretics(hyperkalaemia),
antidepressants(SSRIs,venlafaxine-hyponatraemia,syndromeofinappropriateantidiuretichormone)
Heartfailure,
hypertensionNSAIDs
Hypotensionandfalls combinationsofdrugsactingonthecirculation
Hypothermia phenothiazines,risperidone,benzodiazepines,alcohol,opioids
Insomnia theophyllineanddecongestants
Parkinsoniansymptoms metoclopramide,methotrimeprazine,prochlorperazine
Urinaryretention anticholinergicdrugs.Manydrugs,includingOTCdecongestants,cancauseoraggravateurinaryproblems
Stressincontinence alpha-blockers(e.g.doxazosin),calciumchannelblockers
Adversedrugreactionsareoftenunrecognisedandthereforenot
managed.Evenworseanewdrugmaybeprescribed to treata
symptomwhichhasnotbeenrecognisedasbeingcausedbyan
existingmedication.
This leads to a prescribing cascade where the additional drug
prescribed increases the risk of more adverse reactions raising
therisksoffurtherprescribingtotreatthesenewsymptoms.
People with communication difficulties such as those with
Alzheimer’s disease, dysphasia or intellectual disabilities are at
particularriskofhavingunrecognisedadversedrugreactions.
Page8 IbpacnzPolypharmacy

Examples of the prescribing cascade:
Ankleoedemaduetoacalciumchannelblockerleadstoprescribingofadiuretic.
This type of oedema does not respond to a diuretic.
Prescribedorover-the-counterNSAIDdrugcausesanincreaseinbloodpressureandtheaddition
ofanantihypertensivedrug.
NSAIDs cause a small rise in BP and may tip the balance into the hypertensive category. Review the
need for the NSAID in these patients.
Apatientonamitriptyline50mgnocteforpain.Afteradoseincreasefrom25–50mgthepatient
complainsof incontinenceandoxybutynin isprescribed.The incontinenceworsensandthedose
ofoxybutynin is increased.Thepatientalsocomplainsofconstipationandastimulant laxative is
prescribed.
Amitriptyline has anticholinergic actions and can cause urinary retention leading to overflow
incontinence which was not recognised. Oxybutynin also has anticholinergic actions but is used for
urge incontinence. The situation worsens, the person gets constipated and a laxative is prescribed.
“I do not want two diseases – one nature-made, one doctor-made”NapoleonBonaparte,1820
bpacnzPolypharmacyIPage9

Useofnarrowtherapeuticindexdrugs,suchasdigoxin,warfarin,lithium,anticonvulsantsincreasesthe
riskofdrugtoxicityanddruginteractions.
Useofmultipledrugsincreasesrisksofunpredictedinteractions.
Useofdrugscommonlyassociatedwithdrugrelatedproblemsrequiringhospitaladmissions,suchas
warfarin,NSAIDs,ACEinhibitorsandopioidanalgesics.
Useofdrugsthathavesynergisticadverseeffects,suchashypotensionorsedation.
Useofdrugsfrommultipleprescribers.
Recentcommencementofnewmedicine.
Recentdischargefromhospital.
Unsuperviseduseofover-the-counterorcomplementarymedicines.
When a patient cannot communicate effectively, for example because of Alzheimer’s disease or
intellectualhandicap.
•
•
•
•
•
•
•
•
•
Risk factors for drug related problems in elderly people
Page10 IbpacnzPolypharmacy

Rx: Gli anziani cadono
Buona Salute!
A really good recipe for DRP
Ingredients
6ormoredrugs
12ormoredailydoses
2ormorechronicconditions
2ormoreprescribers
1ormoreofthefollowing:
highriskdrugs
highriskdrugcombinations
highriskdrug-conditioncombinations
Optional
Variousherbaloralternativeremedies
•
•
•
Anyoneoftheseingredientsorseveralcombinedcan,iflefttosimmer,
produceasurprisingconcoctionthatmakeselderlypeoplegoweakat
thekneesandmakestheirheadsspin.
To increase the risk of an unfortunate outcome you can leave the
mixture tostand,without regularchecking,or throw inanadditional
ingredientwithout first assessing the effects of the ones already in
thepot.
Unlikekitchenrecipesyoucanremoveingredientswhichdon’tappear
tobeworking.
Simplifying the recipe, assessing the need for the ingredients, and
monitoring their effectsare thesecrets toachieving thebenefitsof
drugtherapywhilstavoidingunfortunateoutcomes.
“Elderly people all overNewZealandare falling for thisdeceptively easy recipe. Its
basicingredientsarecommonineverydaypracticeasprescriberstrytobalancethe
possiblebenefitsofdrugtherapywiththepotentialforunfortunateoutcomes.”
bpacnzPolypharmacyIPage11

Drug related harm; terms and definitions
Adverse drug event (ADE)
Examples:
Severe bronchospasm following use of metoprolol in an
asthmatic patient with a history of beta-blocker induced
bronchospasm.Thisisamedicationerrorasthehistorywas
not recognised. The metoprolol unmasked and aggravated
thebronchospasmratherthancausingitdirectly.
Metoprolol stopped suddenly resulting in tachycardia and
hypertension.This is alsoamedicationerror resulting from
abrupt discontinuation of the metoprolol and associated
rebound effects. The dose should have been gradually
reduced.
1.
2.
Severebradycardiaresultingfromtheadministrationofthree
timestheintendeddoseofmetoprolol(47.5mgTIDinstead
ofdaily).Anothermedicationerrorwhichcouldbeduetoan
incorrectprescriptionorincorrectreadingorinterpretationof
theprescription.
NBthetermadversedrugeventdoesnotincludesituationswhen
adrugisnotusedwhenthepatientcouldpotentiallybenefitfrom
it.Forexample,failuretouseabeta-blockerinapatientwithstable
wellcontrolledCOPDandheartfailureorpostmyocardialinfarction.
Thisisan“untreatedindication”.
3.
An injury resulting from the use of a drug
Anadversedrugeventisabroadertermwhichincludesadversedrugreactionsplusharmfromtheuseofthedrugincluding
prescribing,administration,overdoses,dosereductionsanddiscontinuationsoftherapy(medicationerrors).
Page12 IbpacnzPolypharmacy
An event or circumstance involving a patient’s drug treatment (or lack of drug treatment) that actually or potentially
interferes with the achievement of an optimal outcome. AdaptedfromHeplerandStrand,1990.
DRPsinclude:
Untreatedindications
Drugusewithoutaclearindication
Sub-therapeuticdosage
Excessivedosage
Adversedrugreaction
Druginteraction
Drugwithdrawalreaction
Medicationerror
Non-adherencetodrugtreatment
Therapeuticfailure
(AdaptedfromHanlonetal,2004)
•
•
•
•
•
•
•
•
•
•
DRPs cause significant morbidity and mortality in the general
population.Someauthorshaveestimatedthattheeconomiccost
ofDRPrankaroundfourthbehind,cardiovasculardisease,cancer
and diabetes in the developed world (Johnson and Bootman,
1995).
Arecentsystematicreviewreportedthatamedian7.1%(range
5.7–16.2) of hospital admissions result from drug related
problems,ofwhich59%wereconsideredpreventable(Winterstein
etal,2002).
Drug related problem (DRP) nowsometimesreferredtoasMedicinesrelatedproblem

Adversedrugreactionsfallintooneoftwomaincategories:
Type A reactions arepredictable,dose-relatedreactionswhere
theintensityoftheeffectincreaseswithdoseorreducedclearance
ofthedrugfromthebody,i.e.increasedbloodconcentrations.For
example,theanticholinergiceffects(constipation,blurredvision)of
amitriptylinewilltendtoworsenifthedoseisincreasedfrom25
mgto50mgdaily.Inadditionthepatientwilltendtobecomemore
drowsyandsedated.
Type B reactions are not related to dose and are largely
unpredictable (idiosyncratic). These represent many potentially
serious adverse reactions such as blood dyscrasias and
ADRs
ADEs
DRPs
A response to a drug which is noxious and unintended and which occurs at doses normally used in man for prophylaxis, diagnosis or therapy of a disease or for the modification of physiological function.
Inotherwords,harmdirectlycausedbythedrugatnormaldoses.Forexample,depressioncausedbyabeta-blocker.
hepatotoxicity.
Forsomeadversedrugreactionsthereappearstobeathreshold
drugdoseorconcentrationatwhichatypeBreactionbecomes
more likely. For example, it is difficult to predict who will get
confusionduetocimetidineorranitidine,buttheelderlyseemtobe
moresusceptibleespeciallyifthedoseisnotreducedaccordingto
thedeclineinrenalfunction.Similarly,theriskoftherareallopurinol
hypersensitivitysyndromeisincreasedifthedoseisnotadjusted
inrenalimpairment.
bpacnzPolypharmacyIPage13
Adverse drug reaction (ADR)

Hospital admissions foradverse drug reactions
3000
2500
2000
1500
1000
500
050-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90+
NumberofADRhospitaladmissions
Admissionsper50,000population
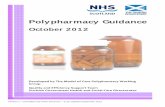
We identified hospital admissions in 2005 for adverse drug
reactions in people over 50 years of age by extracting ICD-10
codesandpatientdemographicdatafromtheHospitalSeparation
Diagnosis Database. International literature suggests that these
dataarelikelytounderestimatetheactualnumberofadmissions
foradversedrugreactionsbecauseofincompletecoding.
Overtheyear,therewere15,254admissionsfor17,806adverse
drugreactions.Therewere146differentadversedrugreactions
recorded.Adversedrugreactionsincreasewithage(graphbelow).
Fiftysixpercentwere female.Only8%ofoverall admissions for
adverse drug reactions were for Māori people although Māori
represent approximately 15%of the population.However, in the
youngerage-bands50-59,Māorirepresentedagreaterproportion
ofadmissionsprobablyduetobeingonmoredrugsatayounger
agecausedbyearlieronsetofchronicdisease.
Hospital admissions for adverse drug reactions increase with age
Page14 IbpacnzPolypharmacy
Age
A
dmis
sion
s

Anticoagulantswerethemostfrequentlyimplicateddrugsfollowedbydiuretics,opioids,nonsteroidalanti-inflammatorydrugsandbeta
blockers.
Number of admissions for ADR by drug group
Maindruggroup Admissions Sub-group Admissions
Cardiovascular
(43.3%)7711
anticoagulants 1779
diuretics 1552
beta-blockers 1023
ACEinhibitors 810
antiarrhythmics 703
vasodilators 577
calciumchannelblockers 434
antihypertensive 288
aspirin 230
α-adrenoceptorblocker 155
lipid-lowering 153
other 7
Nervous system
(17.4%)3107
opioids 1289
antidepressants 424
antipsychotics 362
anaesthetic 180
benzodiazepines 159
antiepileptics 143
analgesics 121
other 429
Anti-inflammatory
(11.6%)2074
NSAIDs 1124
corticosteroids 950
Anti-infectives
(10.3%)1826
penicillin 698
cephalosporin 192
other 936
Oncology agents
(6.4%)1139
anti-neoplasm 978
immunosuppressant 152
other 9
Alimentary tract
(4.5%)805
insulin&oralhypoglycaemics 440
other 365
Other
(6.4%)1144
musculo-skeletal 178
hormonepreparations 106
respiratory 81
topical 38
sensorysystem 25
vaccine 13
other 703
TOTAL 17806
bpacnzPolypharmacyIPage15

Hyponatraemia is an adverse reaction that can be serious and
is reported most often in the elderly with fluoxetine, paroxetine
andbendrofluazideindividuallyorincombination.Inaseriesof11
patientsaged65yearsandolderwithhyponatraemiaattributedto
bendrofluazide,fourweretakingothermedicinesalsolikelytocause
hyponatraemia, these were frusemide, fluoxetine and paroxetine,
and in one case both frusemide and fluoxetine. Presenting
symptomsweresometimesvagueandincludedlethargy,confusion
andnausea.Oneyoungerpatientdevelopedconvulsions.Sixofthe
eleven patients required hospital admission and in one case the
conditionwaslife-threatening.Onepatientwasalsotakingquinine
anddevelopedatrialfibrillation,probablyanadverseeffectofquinine
mademorelikelybecauseoftheelectrolytedisturbance.Thepatient
takingbendrofluazide,frusemideandfluoxetinealsotookenalapril
androfecoxiband,aswellashyponatraemia,developedacuterenal
failureduetothecombinationofdiuretics,ACEinhibitorandanon
steroidalanti-inflammatoryagent(bpacnz,ACEInhibitors).
Interactions with simvastatinarealsocommonlyreported.Myalgia
occursfrequentlywithsimvastatinbuthighdosesorco-prescription
offibratesormedicinesthatinhibitsimvastatinmetabolismcanlead
to myopathy, including on rare occasions, rhabdomyolysis which
isoftenfatal.Reportshavebeenreceivedofsuchreactionswhen
otherpotent inhibitorsofhepaticCYP3A4 isoenzymeshavebeen
prescribedsuchasazoleantifungals,erythromycinandciclosporin.
Ofnote is thatdiltiazem,aweak inhibitorofCYP3A4,appearsto
haveprecipitatedrhabdomyolysiswhengivenwithhighdoses(80
mg daily) of simvastatin or at lower doses where there were a
numberofco-morbidities.Theseinteractionsalsoaffectatorvastatin
(Savage,2006).
Interactions with warfarin continue to be commonly reported.
Thereareanumberofrecentreportsofroxithromycin increasing
theeffectofwarfarin.Thisislikelytobetoalesserdegreethanwith
erythromycinbuttheproductinformationforroxithromycinindicates
that the effect may be clinically significant in patients receiving
polytherapy or in the elderly (Medsafe, 2006). The interaction
betweenmiconazoleandwarfariniswell-recognisedbutreportsto
CARM,someserious,indicatethatitisnotalwaysrecognisedthat
miconazoleoralgelwillalsointeract.
ReportstoCARMofhypotension in the elderlydemonstrate in
particular that the addition of psychoactive medicines that lower
bloodpressuretoanantihypertensiveregimemaymeanthatsome
antihypertensive medicines need to be discontinued or the dose
lowered if the psychoactive medication is considered necessary.
A combination of trifluoperazine, atenolol and amlodipine in one
patient led to ataxia, hypotension and syncope. A patient with
bradycardia and heart block probably due to the combination of
diltiazemandmetoprolol,wasalsotakingdonepezilandthismay
have contributed to the dizziness and hypotension the patient
alsoexperienced.Apatienttakingnortriptyline,timolol,nifedipine,
captopril and hydrochlorothiazide developed hypotension and
syncope and recovered when nortriptyline and nifedipine were
withdrawn.
Where the prescription of potentially interacting medicines is
unavoidable, careful follow up for indicators that an unwanted
outcomeisdevelopingisessential.
CARMCentreforAdverseReactionsMonitoring
TheCentreforAdverseReactionsMonitoring(CARM)hasidentifiedsomecommonlyreportedadversedrugreactions
inthelast10yearsoccurringinpatientsaged65yearsandolderandoftenresultingfrominteractingmedicines.
Page16 IbpacnzPolypharmacy
Commonly reported adverse drug reactions

References
BjerrumL,J.Sogaard,J.Hallas,J.Kragstrup.Polypharmacy:correlationswithsex,ageanddrugregimen,EurJClinPharmacol.1998;54(3):197–202.
FultonMM,AllenER.Polypharmacyintheelderly:ALiteratureReview.JAmerAcadNursePract.2005;17(4):123-131.
JohnsonJA,BootmanJL.Drug-relatedmorbidityandmortality:acost-of-illnessmodel.ArchInternMed.1995;155:1949-1956.
MangoniAA,JacksonSHD.Age-relatedchangesinpharmacokineticsandpharmacodynamics:basicprinciplesandpracticalimplications.BrJClinPharmacol.
2003;57(1):6-14.
HanlonJT,SchmaderKE,KornkowskiMJ,etal.Adversedrugeventsinhighriskolderoutpatients.JAmGeriatrSoc.1997;45:945-948.
HanlonJT,LindbladCI,GraySL.Canclinicalpharmacyserviceshaveapositiveimpactondrugrelatedproblemsandhealthoutcomesincommunitybased
olderadults?AmJGeriatrPharmacother.2004;2:3-13.
Mant,J.,McManus,J.,&Hare,R.(2006).Applicabilitytoprimarycareofnationalclinicalguidelinesonbloodpressureloweringforpeoplewithstroke:cross
sectionalstudy.BMJ,332,635-637.
WintersteinAG,SauerBC,HeplerCD,etal.Preventabledrug-relatedhospitaladmissions.AnnPharmacother.2002;36:1238–48.
Bibliography
BeersMH,Ouslander JG, Rollingher I, ReubenDB,Brooks J, Beck JC. Explicit criteria for determining inappropriatemedication use in nursing home
residents.ArchInternMed.1991;151:1825-1832.
bpacnz:BestPracticeAdvocacyCentre,(2006).ACEinhibitors.Availablefromhttp://www.bpac.org.nz/default.asp?action=article&id=27&category=247
(AccessedMay2006).
BootmanJL,HarrisonDL,CoxE.Thehealthcarecostofdrug-relatedmorbidityandmortalityinnursingfacilities.ArchInternMed.1997;157:2089-2096.
DavisP,Lay-YeeR,BriantRetal.AdverseeventsinNewZealandPublicHospitalsI:occurrenceandimpact.NZMedJ.2002:115(1167).Availablefrom:
http://www.nzma.org.nz/journal/115-1167/271/(AccessedApril2006).
FickDM,CooperJW,WadeWE,WallerJL,MacleanJR,BeersMH.UpdatingtheBeersCriteriaforPotentiallyInappropriateMedicationUseinOlderAdults.
ArchInternMed.2003;163:2716-2724.
HeplerCD,StrandLM.OpportunitiesandResponsibilitiesinPharmaceuticalCare.AmJHospPharm.1990;47:533-43.
HoechstMarionRousselNZLtd.Rulide™productinformation.March1996.www.medsafe.govt.nz/DatasheetPage.htm.
KellyWN.Firstdonoharm:Reducingmedicationerrorsinlong-termcare.AnnLong-TermCare2002;10:49-56.
KlarinI,WimoA,FastbomJ.Theassociationofinappropriatedrugusewithhospitalisationandmortality;Apopulationbasedstudyoftheveryold.Drugs
Aging.2005;22(1):69-82.
MedicinesandOlderPeople,2001.NationalServiceFramework:Dept.ofHealth(UK).
Availablefrom:http://www.dh.gov.uk/assetRoot/04/06/72/47/04067247.pdf(AccessedApril2006).
Nebeker JR, Barach P, Samore MH. Clarifying adverse drug events; A clinician’s guide to terminology, documentation and reporting. Ann Intern Med
2004;140:795-801.
NPSNews;2004No34.NationalPrescribingServiceLimited,Canberra,Australia.Availablefrom;http://www.nps.org.au/site.php?content=/html/news.
php&news=/resources/NPS_News/news34(AccessedMarch2006).
Prescribingfortheolderperson.MeReCBulletin.2000;11(10):37.Availablefrom:http://www.npc.co.uk/MeReC_Bulletins/2000Volumes/pdfs/vol11n10.
pdf(AccessedApril2006).
RochonPA,GurwitzJH.Optimisingdrugtreatmentforelderlypeople:theprescribingcascade.BMJ.1997;315:1096-9.
Room forReview.Aguide tomedication review:MedicinesPartnership. (updated31/03/2006)Available from:http://www.medicines-partnership.org/
medication-review/room-for-review.
SavageRandTatleyM.Myopathywithstatins:checkCKlevelsandinteractions.PrescriberUpdate2004;25(1):4-5.
StuckAE,BeersMH,SteinerA,etal.Inappropriatemedicationuseincommunityresidingolderpersons.ArchInternMed.1994;154:2195-2200.
ZiereG,DielemanJP,HofmanA,PolsHAP,vanderCammenTJM,StrickerBHCH.Polypharmacyandfallsinthemiddleageandelderlypopulation.BrJ
ClinPharmacol.2005;61(2):218-223.
bpacnzPolypharmacyIPage17

nzbpacbetter edicin m e