Bowel Obstruction in Advanced cancer - Island...
43
Bowel Obstruction in Advanced cancer Bowel Obstruction in Advanced cancer Practical management Practical management Dr. Robin Love March 2015
Transcript of Bowel Obstruction in Advanced cancer - Island...

Bowel Obstruction in Advanced cancerBowel Obstruction
in Advanced cancerPractical management Practical management
Dr. Robin LoveMarch 2015

2
ObjectivesObjectives
Understand the causes of obstruction in cancer Be able to discuss goals of care with
patients and family Plan various treatments depending on
the goals of care and clinical context
Understand the causes of obstruction in cancer Be able to discuss goals of care with
patients and family Plan various treatments depending on
the goals of care and clinical context

3
OutlineOutline
Case Epidemiology Pathophysiology Clinical Diagnosis Treatment
Surgical Medical
Case Epidemiology Pathophysiology Clinical Diagnosis Treatment
Surgical Medical

4
Case 1 Norman Case 1 Norman
78 year old man , lives on GabriolaIsland Cecal carcinoma resected 3 years later: recurrent obstructive Sx
several admissions Admitted via ER with mild nausea,
moderate abdominal pain, no flatus or stool for days
78 year old man , lives on GabriolaIsland Cecal carcinoma resected 3 years later: recurrent obstructive Sx
several admissions Admitted via ER with mild nausea,
moderate abdominal pain, no flatus or stool for days

5
Epidemiology: Bowel ObstructionEpidemiology: Bowel Obstruction
Occurs in 3-10% of all cancer-related terminally ill Most common Ovary 25% (10-42%) Colorectal 15% (5-25%)
Less common Pancreas, gynecological, prostate, gastric,
bladder
Occurs in 3-10% of all cancer-related terminally ill Most common Ovary 25% (10-42%) Colorectal 15% (5-25%)
Less common Pancreas, gynecological, prostate, gastric,
bladder

6
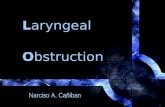
Typical Locations of Obstructions Esophageal Biliary
Gastro duodenal Small Bowel Colorectal
Typical Locations of Obstructions Esophageal Biliary
Gastro duodenal Small Bowel Colorectal
Gastro-intestinal Tract Anatomy

7
Pathophysiology…Pathophysiology…
Small bowel (61%) or large bowel (33%) or both (20%) Single or multiple sites Partial or complete Malignant or benign causes
Final common path: occlusion of the lumen of the bowel
Small bowel (61%) or large bowel (33%) or both (20%) Single or multiple sites Partial or complete Malignant or benign causes
Final common path: occlusion of the lumen of the bowel

8
Etiology: Related to the Cancer
Etiology: Related to the Cancer
Tumour Mass Single or multiple Intraluminal Intramural Extraluminal Separate from the
bowel Tumour invasion of
mesentery, muscle or nerve plexus
Tumour Mass Single or multiple Intraluminal Intramural Extraluminal Separate from the
bowel Tumour invasion of
mesentery, muscle or nerve plexus
Volvulus/torsion Around tumour Around adhesions Around fistula
Massive ascites Paraneoplastic
syndrome
Volvulus/torsion Around tumour Around adhesions Around fistula
Massive ascites Paraneoplastic
syndrome
Often Multifactorial

9
Etiology: Related to the Cancer treatment
Etiology: Related to the Cancer treatment
Adhesions PostoperativeMalignant Post radiation
Radiation enteritis Chemotherapy (ileus)
Adhesions PostoperativeMalignant Post radiation
Radiation enteritis Chemotherapy (ileus)

10
Etiology: unrelated or indirectly related to the cancer
Etiology: unrelated or indirectly related to the cancer
Constipation / Impaction
Ileus Infection Drugs Diabetes
Peritonitis Bowel infarction
Constipation / Impaction
Ileus Infection Drugs Diabetes
Peritonitis Bowel infarction
Other unrelated Hernia Diverticulitis Pancreatitis… Inflammatory bowel
disease Adhesions
a significant number are benign causes
Other unrelated Hernia Diverticulitis Pancreatitis… Inflammatory bowel
disease Adhesions
a significant number are benign causes

11
Diagnosis of Bowel ObstructionDiagnosis of Bowel Obstruction History Physical
examination Imaging of the
abdomen Plain films CT Contrast studies
History Physical
examination Imaging of the
abdomen Plain films CT Contrast studies

12
Clinical: History and symptoms…Clinical: History and symptoms…
Rarely an acute event- usually develops slowly and often is partial Cramps, nausea, vomiting, abdominal
distension Gradually become more severe and
continuous
Rarely an acute event- usually develops slowly and often is partial Cramps, nausea, vomiting, abdominal
distension Gradually become more severe and
continuous

13
…symptoms and signs…symptoms and signs
Constant abdominal pain in 90% (related to the underlying tumor ?)
Intermittent colic in 75% Vomiting early and in large amounts in
proximal (gastric,duodenal and small bowel) and later in large bowel
Constant abdominal pain in 90% (related to the underlying tumor ?)
Intermittent colic in 75% Vomiting early and in large amounts in
proximal (gastric,duodenal and small bowel) and later in large bowel

14
RadiologyRadiology
Plain radiographs useful (and easy) CT very useful to assess (new gold standard) Global extent of disease Staging including complications (ischemic bowel) Assist in choice of surgical treatment
*if appropriate and patient is well enough
Plain radiographs useful (and easy) CT very useful to assess (new gold standard) Global extent of disease Staging including complications (ischemic bowel) Assist in choice of surgical treatment
*if appropriate and patient is well enough

15
General approach….General approach….
As with any problem in palliative care, we must consider whether our inquiries or investigations will change the management of the patient.
As with any problem in palliative care, we must consider whether our inquiries or investigations will change the management of the patient.

16
…General approach…General approach
• This is rarely an emergency -take time to :
• Monitor• Investigate appropriately• Provide symptom control
• Remember the overall context…(stage of disease etc)
• This is rarely an emergency -take time to :
• Monitor• Investigate appropriately• Provide symptom control
• Remember the overall context…(stage of disease etc)

17
Care…the right thing for this particular patientCare…the right thing for this particular patient

18
Principles of Care…Principles of Care…
Primary areas of symptom control Pain Nausea Vomiting Thirst
Secondary areas of support Nutrition, including hydration Education Patient & family support
Primary areas of symptom control Pain Nausea Vomiting Thirst
Secondary areas of support Nutrition, including hydration Education Patient & family support

19
…Principles of Care…Management is highly patient specific…Principles of Care…Management is highly patient specific
Stage of illness
Stage of illness
Type of obstruction
Type of obstruction
PrognosisPrognosisPerformance status
Performance status
Goals and choices of
patient
Goals and choices of
patient

20
Active Treatment ApproachesActive Treatment Approaches
Active surgical ResectionBy-passVenting
Colostomy etc Gastrostomy
Active medical
Comfort Care only
Active surgical ResectionBy-passVenting
Colostomy etc Gastrostomy
Active medical
Comfort Care only

21
NormanNorman
Surgery Day 2 Diffuse carcinomatosis Omental caking Not resectable , bypass not possible Moderate symptoms ( N, pain)
Surgery Day 2 Diffuse carcinomatosis Omental caking Not resectable , bypass not possible Moderate symptoms ( N, pain)

22
Active Surgical Active Surgical
Not routine in our patient population, but should be considered in selected patients with mechanical obstruction single site of obstruction reasonable performance status and prognosis
Excellent clinical judgment is necessary. Is it technically feasible and will the patient benefit?
Not routine in our patient population, but should be considered in selected patients with mechanical obstruction single site of obstruction reasonable performance status and prognosis
Excellent clinical judgment is necessary. Is it technically feasible and will the patient benefit?

23
…Surgical …Surgical
25-35% of obstructions due to benign factors or unrelated second primary
Some individuals symptom free for long period after palliative surgery
Operative mortality 10-20%, similar morbidity and complication rate
Median post-op. survival 2.5-11 months Surgical studies rarely look at Quality of Life
25-35% of obstructions due to benign factors or unrelated second primary
Some individuals symptom free for long period after palliative surgery
Operative mortality 10-20%, similar morbidity and complication rate
Median post-op. survival 2.5-11 months Surgical studies rarely look at Quality of Life

24
Poor prognostic factorsPoor prognostic factors Prior failed surgery Widespread carcinomatosis Gross Ascites Multiple levels of obstruction Multiple liver metastases Cachexia Elderly Previous radiotherapy to abdomen
Prior failed surgery Widespread carcinomatosis Gross Ascites Multiple levels of obstruction Multiple liver metastases Cachexia Elderly Previous radiotherapy to abdomen

25
Other Surgical / Interventional Options: decompression techniques
Other Surgical / Interventional Options: decompression techniques
Cecostomy etc Percutaneous Gastrostomy “PEG”
“Venting Gastrostomy” Endoscopic Radiologic
Very effective for persistent nausea and vomiting (up to 92%)
Cecostomy etc Percutaneous Gastrostomy “PEG”
“Venting Gastrostomy” Endoscopic Radiologic
Very effective for persistent nausea and vomiting (up to 92%)

26
Other Surgical / Interventional OptionsOther Surgical / Interventional Options
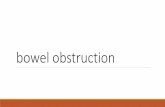
Metal stents placed under endoscopic or fluoroscopic guidance Flexible and self expanding Expensive, not always available in Canada Overall cost effective Technical success rate 90% ( ??) Esophageal, gastro-duodenal, biliary,
colorectal
Metal stents placed under endoscopic or fluoroscopic guidance Flexible and self expanding Expensive, not always available in Canada Overall cost effective Technical success rate 90% ( ??) Esophageal, gastro-duodenal, biliary,
colorectal

27
Stent partially deployedStent partially deployed

NormanNorman
Recurrence of distension, vomiting Still on dexamethasone and haldol Increase steroids, move to PCU Temporary NG tube (his choice)
Recurrence of distension, vomiting Still on dexamethasone and haldol Increase steroids, move to PCU Temporary NG tube (his choice)
28

29
Medical Treatment of Obstruction:symptom relief and possible reversalMedical Treatment of Obstruction:symptom relief and possible reversal
NG tube and rehydration: 30-50% will reverse (but usually takes several days) Temporary – patients choice
Medications: Analgesics Motility agents Antiemetics Antisecretory
NG tube and rehydration: 30-50% will reverse (but usually takes several days) Temporary – patients choice
Medications: Analgesics Motility agents Antiemetics Antisecretory

30
Medical Treatment of Obstruction:AnalgesicsMedical Treatment of Obstruction:Analgesics
Usual opioids by parenteral route (s.c., transdermal etc) anticholinergics for colicky pain Scopolamine hydrobromide 0.4-0.8 mg sc q2-4h
Usual opioids by parenteral route (s.c., transdermal etc) anticholinergics for colicky pain Scopolamine hydrobromide 0.4-0.8 mg sc q2-4h

31
Medical Treatment of Obstruction:Motility agentsMedical Treatment of Obstruction:Motility agents Metoclopramide: 10-40mg sc qid
(Domperidone po only) The classic approach is not to use it in
complete obstruction because it might cause increased cramps. No evidence for this How do you really know complete vs. partial vs.
ileus?
My approach: try it for all and see if increased cramps
Metoclopramide: 10-40mg sc qid(Domperidone po only)
The classic approach is not to use it in complete obstruction because it might cause increased cramps. No evidence for this How do you really know complete vs. partial vs.
ileus?
My approach: try it for all and see if increased cramps

32
Medical Treatment of Obstruction:antinauseantsMedical Treatment of Obstruction:antinauseants Metoclopramide 10-40 sc qid Haloperidol 0.5-2 mg sc/po/iv q12h and prn Metoclopramide 10-40 sc qid Haloperidol 0.5-2 mg sc/po/iv q12h and prn

33
Medical treatment of obstruction: corticosteroidsMedical treatment of obstruction: corticosteroids Dexamethasone 10-20mg daily for trial of five
days (mechanism unknown- helps the nausea, may relieve obstruction by reducing bowel wall edema)
Reduce peritumoral edema Antisecretory : reduce water and salt
secretion
Dexamethasone 10-20mg daily for trial of five days (mechanism unknown- helps the nausea, may relieve obstruction by reducing bowel wall edema)
Reduce peritumoral edema Antisecretory : reduce water and salt
secretion

34
Medical Treatment of Obstruction:Antisecretory…Medical Treatment of Obstruction:Antisecretory…
Octreotide 100-200 mcg sc q 8h Reduce GI secretions Slow intestinal motility Increase absorption of water and electrolytes
Good clinical evidence to support use in malignant bowel obstruction (RCT’s – total vomiting control in 92%)
Use it early in obstruction Rapid and effective
Octreotide 100-200 mcg sc q 8h Reduce GI secretions Slow intestinal motility Increase absorption of water and electrolytes
Good clinical evidence to support use in malignant bowel obstruction (RCT’s – total vomiting control in 92%)
Use it early in obstruction Rapid and effective

35
Grenoble Study JPSM June 2006Grenoble Study JPSM June 2006
Stage 1: NG, hydrate, haldol, scopolamine, steroids, analgesics Stage 2 (after 5 days): still obstructed?
Stop steroids and scopol. , and start octreotide Stage 3 : gastrostomy
Sx control in 90% without ng tube
Stage 1: NG, hydrate, haldol, scopolamine, steroids, analgesics Stage 2 (after 5 days): still obstructed?
Stop steroids and scopol. , and start octreotide Stage 3 : gastrostomy
Sx control in 90% without ng tube

36
Comfort : for all patients Comfort : for all patients
Pain Colic Continuous pain
Nausea & vomiting Mouth Care and Thirst Nutrition Emotional support
Pain Colic Continuous pain
Nausea & vomiting Mouth Care and Thirst Nutrition Emotional support

37
Comfort Care OnlyComfort Care Only
Very advanced stage of disease Multiple medical problems Desire to stay at home In complete obstruction the average
survival is 10-20 days **(often misinformed about a quick
demise)
Very advanced stage of disease Multiple medical problems Desire to stay at home In complete obstruction the average
survival is 10-20 days **(often misinformed about a quick
demise)

38
Norman Norman
Start octreotide 200 tid sc Metoclopramide 20 sc qid Dexamethasone 8 mg sc daily
Settled well, bowels remained open Discharged home day 14 Managed well at home (Gabriola Island) with
sc meds, low residue diet. Died 1 month later at home
Start octreotide 200 tid sc Metoclopramide 20 sc qid Dexamethasone 8 mg sc daily
Settled well, bowels remained open Discharged home day 14 Managed well at home (Gabriola Island) with
sc meds, low residue diet. Died 1 month later at home

39
Overall approachOverall approach1. If urgent (severe Sx) – ng suction2. Start optimal medical management in almost all
patients unless really end stage3. Metoclopramide plus octreotide plus
dexamethasone (+/- haldol) (can combine in one CSCI) is easy and very effective
4. Consider hydration options (may reduce nausea)5. Consider other options/investigations6. Acceptable level of control may be vomiting 1-2
times/day ( as long as nausea is well controlled)
1. If urgent (severe Sx) – ng suction2. Start optimal medical management in almost all
patients unless really end stage3. Metoclopramide plus octreotide plus
dexamethasone (+/- haldol) (can combine in one CSCI) is easy and very effective
4. Consider hydration options (may reduce nausea)5. Consider other options/investigations6. Acceptable level of control may be vomiting 1-2
times/day ( as long as nausea is well controlled)

40

41
References…References…1. Ripamonti et al, Clinical practice recommendations for the
management of bowel obstruction in patients with end-stage cancer. Support Care Cancer (2001) 9: 223-233
2. Ripamonti, C and E. Bruera Palliative Management of Malignant Bowel Obstruction Int J Gynecol Cancer 2002, 12: 135-143
3. Mercadante,S et al. Aggressive Pharmacalogical Treatment for Reversing Malignant Bowel Obstruction J of Pain and Symptom Mgt. 2004, 28: No.4, 412-416
4. Mercadante,S et al Comparison of octreotide and hyoscine butylbromide in controlling GI symptoms due to malignant inoperable bowel obstruction. Support Care Cancer (2000) 8:188-191
5. Dean,Andrew The Palliative effects of Octreotide in Cancer patients Chemotherapy 2001;47 Suppl 2: 54-61
1. Ripamonti et al, Clinical practice recommendations for the management of bowel obstruction in patients with end-stage cancer. Support Care Cancer (2001) 9: 223-233
2. Ripamonti, C and E. Bruera Palliative Management of Malignant Bowel Obstruction Int J Gynecol Cancer 2002, 12: 135-143
3. Mercadante,S et al. Aggressive Pharmacalogical Treatment for Reversing Malignant Bowel Obstruction J of Pain and Symptom Mgt. 2004, 28: No.4, 412-416
4. Mercadante,S et al Comparison of octreotide and hyoscine butylbromide in controlling GI symptoms due to malignant inoperable bowel obstruction. Support Care Cancer (2000) 8:188-191
5. Dean,Andrew The Palliative effects of Octreotide in Cancer patients Chemotherapy 2001;47 Suppl 2: 54-61

42
…References…References
6.Mystakidou,K et al. Comparison of Octreotide Administration vs Conservative Treatment in the Management of Inoperable Bowel Obstruction in Patients with Far Advanced Cancer: a randomized, Double-blind, Controlled Clinical Trial. Anticancer Research 2002 22: 1187-1192
7. Brooksbank, MA et al. Palliative Venting Gastrostomy in Malignant Intestinal Obstruction. Palliative Medicine 2002; 16: 520-526
8. Krouse,RS et al. When the Sun can set on Unoperated Bowel Obstruction: Management of Malignant Bowel Obstruction J Am Coll Surg 2002, 195: No 1 117-128
9. Keymling,M Colorectal Stenting Endoscopy 2003; 35:234-23810. Baron, TH. Expandable Metal Stents for the Treatmentof
Cancerous Obstruction of the GI Tract. NEJM 2001,344:22;1681-1687
6.Mystakidou,K et al. Comparison of Octreotide Administration vs Conservative Treatment in the Management of Inoperable Bowel Obstruction in Patients with Far Advanced Cancer: a randomized, Double-blind, Controlled Clinical Trial. Anticancer Research 2002 22: 1187-1192
7. Brooksbank, MA et al. Palliative Venting Gastrostomy in Malignant Intestinal Obstruction. Palliative Medicine 2002; 16: 520-526
8. Krouse,RS et al. When the Sun can set on Unoperated Bowel Obstruction: Management of Malignant Bowel Obstruction J Am Coll Surg 2002, 195: No 1 117-128
9. Keymling,M Colorectal Stenting Endoscopy 2003; 35:234-23810. Baron, TH. Expandable Metal Stents for the Treatmentof
Cancerous Obstruction of the GI Tract. NEJM 2001,344:22;1681-1687

43
…References…References11. Pothuri, b et al. PEG tube placement in patients with MBO due to
ovarian carcinoma. Gynecologic Oncology 96 (2005) 330-33412.Laval,G. et al. Protocol for the Treatment of Malignant Bowel
Obstruction: A prospective study of 80 cases at Grenoble University Hospital Center. JPSM Vol 31 NO 6. June 2006 p 502-512
13. Mangili, G. et al. Palliative Care for intestinal obstruction in recurrent ovarian cancer: a multivariate analysis. Int Journal of Gynecologic Cancer Vol 15 issue 5 p 830-835
14. Mercadante,S et al. Medical Treatment for Inoperable Malignant Bowel Obstruction: a Qualitative Systematic Review. JPSM Vol 33 No . Feb 2007 p217-223
11. Pothuri, b et al. PEG tube placement in patients with MBO due to ovarian carcinoma. Gynecologic Oncology 96 (2005) 330-334
12.Laval,G. et al. Protocol for the Treatment of Malignant Bowel Obstruction: A prospective study of 80 cases at Grenoble University Hospital Center. JPSM Vol 31 NO 6. June 2006 p 502-512
13. Mangili, G. et al. Palliative Care for intestinal obstruction in recurrent ovarian cancer: a multivariate analysis. Int Journal of Gynecologic Cancer Vol 15 issue 5 p 830-835
14. Mercadante,S et al. Medical Treatment for Inoperable Malignant Bowel Obstruction: a Qualitative Systematic Review. JPSM Vol 33 No . Feb 2007 p217-223